What are the side effect of antidepressants
Side effects - Antidepressants - NHS
The side effects of antidepressants can cause problems at first, but they generally improve with time.
It's important to continue treatment, even if you're affected by side effects, as it will take several weeks before you begin to benefit from treatment. With time, you should find that the benefits of treatment outweigh any problems from side effects.
During the first few months of treatment, you'll usually see your doctor or a specialist nurse at least once every 2 to 4 weeks to see how well the medicine is working.
For more information about your specific medicine, see the patient information leaflet that comes with it.
SSRIs and SNRIs
Common side effects of selective serotonin reuptake inhibitors (SSRIs) and serotonin-noradrenaline reuptake inhibitors (SNRIs) can include:
- feeling agitated, shaky or anxious
- feeling and being sick
- indigestion and stomach aches
- diarrhoea or constipation
- loss of appetite
- dizziness
- not sleeping well (insomnia), or feeling very sleepy
- headaches
- loss of libido (reduced sex drive)
- difficulties achieving orgasm during sex or masturbation
- difficulties obtaining or maintaining an erection (erectile dysfunction)
These side effects should improve within a few weeks, although some can occasionally persist.
Tricyclic antidepressants (TCAs)
Common side effects of TCAs can include:
- dry mouth
- slight blurring of vision
- constipation
- problems passing urine
- drowsiness
- dizziness
- weight gain
- excessive sweating (especially at night)
- heart rhythm problems (arrhythmia), such as noticeable palpitations or a fast heartbeat (tachycardia)
The side effects should ease after a couple of weeks as your body begins to get used to the medicine.
Potential health risks
Serotonin syndrome
Serotonin syndrome is an uncommon, but potentially serious, set of side effects linked to SSRIs and SNRIs.
Serotonin syndrome occurs when the levels of a chemical called serotonin in your brain become too high. It's usually triggered when you take an SSRI or SNRI in combination with another medicine (or substance) that also raises serotonin levels, such as another antidepressant or St John's wort.
Symptoms of serotonin syndrome can include:
- confusion
- agitation
- muscle twitching
- sweating
- shivering
- diarrhoea
If you experience these symptoms, you should stop taking the medicine and get immediate advice from your GP or specialist. If this is not possible, call NHS 111.
Symptoms of severe serotonin syndrome include:
- seizures (fits)
- irregular heartbeat (arrhythmia)
- unconsciousness
If you experience symptoms of severe serotonin syndrome, get emergency medical help immediately by dialling 999 to ask for an ambulance.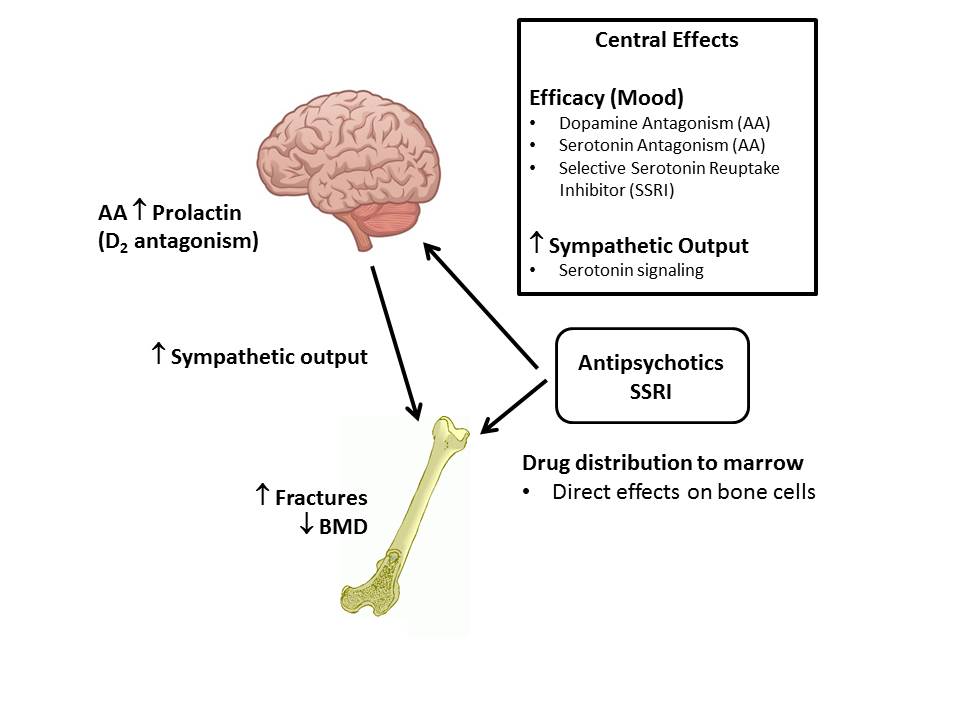
Hyponatraemia
Elderly people who take antidepressants, particularly those who take SSRIs, may experience a severe fall in sodium (salt) levels, known as hyponatraemia. This may lead to a build-up of fluid inside the cells of the body, which can be potentially dangerous.
This can happen because SSRIs can block the effects of a hormone that regulates levels of sodium and fluid in the body. Elderly people are vulnerable because fluid levels become more difficult for the body to regulate as people age.
Mild hyponatraemia can cause symptoms similar to depression or side effects of antidepressants, such as:
- feeling sick
- headache
- muscle pain
- reduced appetite
- confusion
More severe hyponatraemia can cause:
- feeling listless and tired
- disorientation
- agitation
- psychosis
- seizures (fits)
The most serious cases of hyponatraemia can cause you to stop breathing or enter a coma.
If you suspect mild hyponatraemia, you should call your GP for advice and stop taking SSRIs for the time being.
If you suspect severe hyponatraemia, call 999 and ask for an ambulance.
Hyponatraemia can be treated by feeding a sodium solution into the body through an intravenous drip.
Diabetes
Long-term use of SSRIs and TCAs has been linked to an increased risk of developing type 2 diabetes, although it's not clear if the use of these antidepressants directly causes diabetes to develop.
It may be that the weight gain some people using antidepressants experience increases the risk of them developing type 2 diabetes.
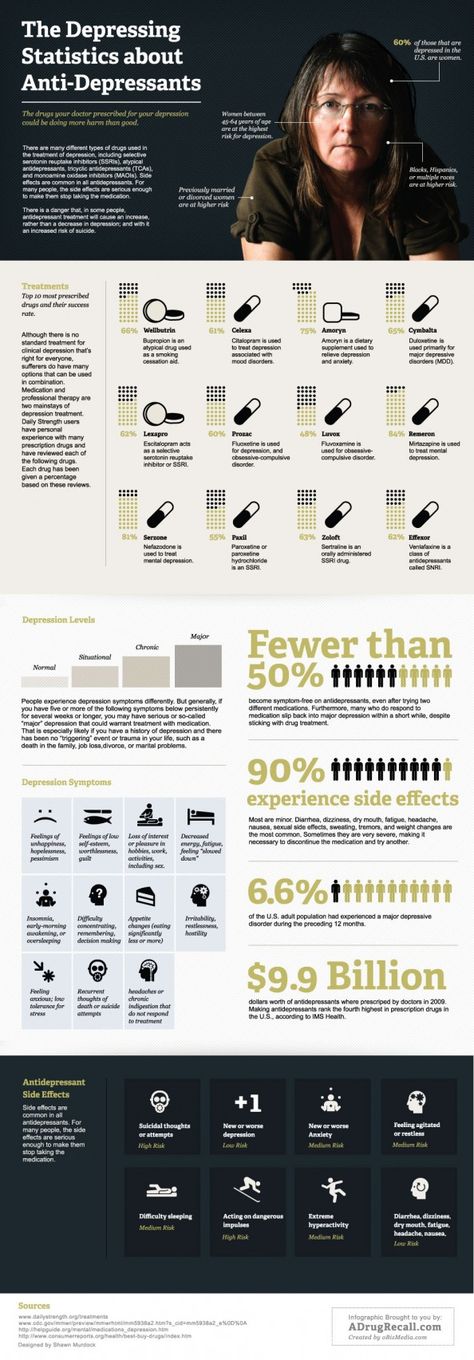
Suicidal thoughts
In rare cases, some people experience suicidal thoughts and a desire to self-harm when they first take antidepressants. Young people under 25 seem particularly at risk.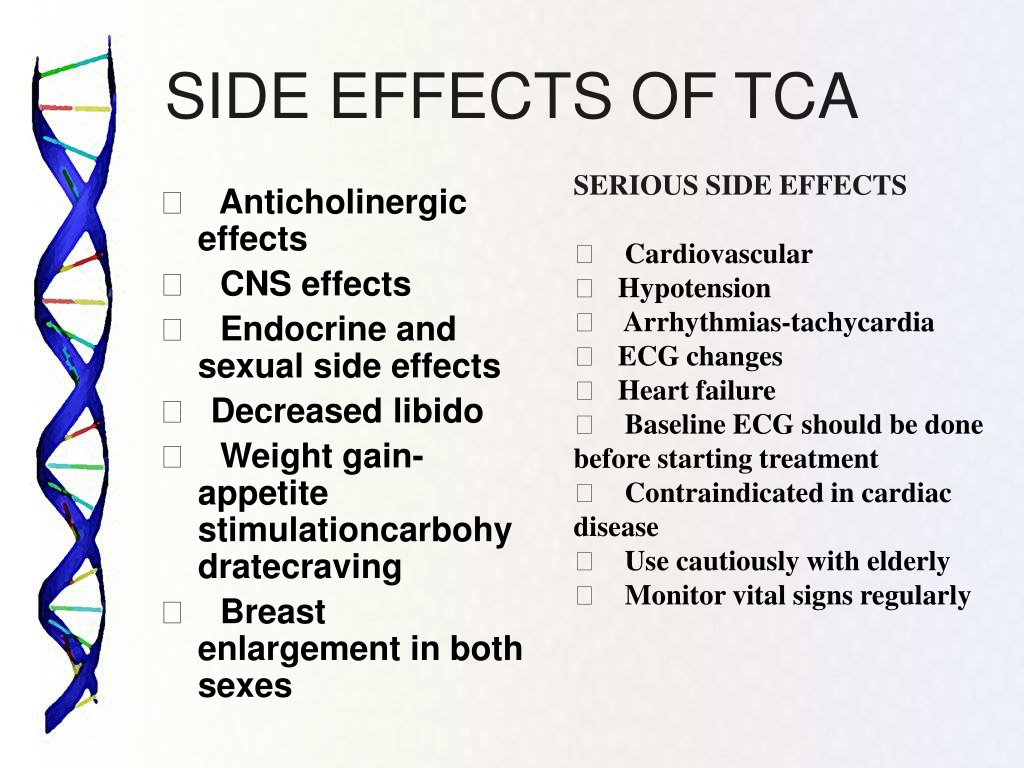
Contact your GP, or go to A&E immediately, if you have thoughts of killing or harming yourself at any time while taking antidepressants.
It may be useful to tell a relative or close friend if you've started taking antidepressants and ask them to read the leaflet that comes with your medicines. You should then ask them to tell you if they think your symptoms are getting worse, or if they're worried about changes in your behaviour.
Page last reviewed: 4 November 2021
Next review due: 4 November 2024
Side effects - Selective serotonin reuptake inhibitors (SSRIs)
The side effects of selective serotonin reuptake inhibitors (SSRIs) can be troublesome at first, but most improve with time.
In general, SSRIs are better tolerated than most other types of antidepressants. The majority of people will only experience a few mild side effects when taking them.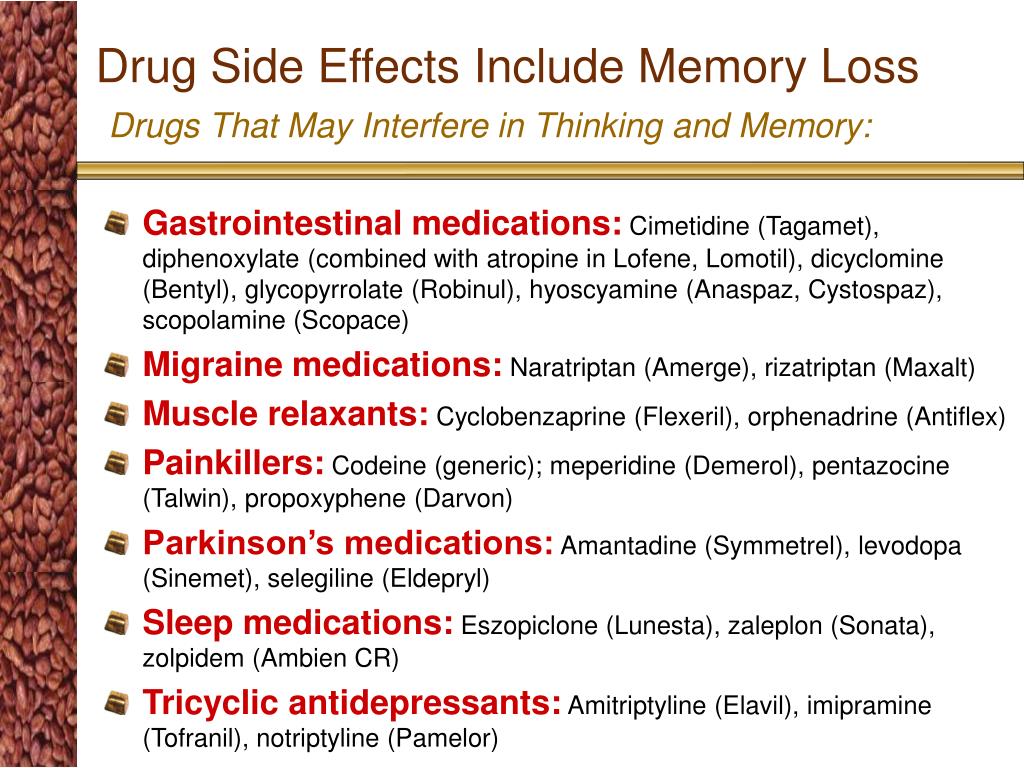
It's important to persist with treatment, even if you're affected by side effects, as it will take several weeks before you begin to benefit from treatment. With time, you should find that the benefits of treatment outweigh problems related to side effects.
You'll usually see your doctor every few weeks when you first start taking SSRIs to discuss how well the medicine is working. However, you can contact your doctor at any point if you experience any particularly troublesome or persistent side effects.
For information about the side effects of a particular SSRI, check the information leaflet that comes with your medicine.
Common side effects
Common side effects of SSRIs can include:
- feeling agitated, shaky or anxious
- feeling or being sick
- indigestion
- diarrhoea or constipation
- loss of appetite and weight loss
- dizziness
- blurred vision
- dry mouth
- excessive sweating
- sleeping problems (insomnia) or drowsiness
- headaches
- loss of libido (reduced sex drive)
- difficulty achieving orgasm during sex or masturbation
- in men, difficulty obtaining or maintaining an erection (erectile dysfunction)
These side effects should improve over time, although some – such as sexual problems – can persist.
Less common side effects
Less common side effects of SSRIs can include:
- bruising or bleeding easily, including vomiting blood or bleeding from your bottom
- confusion
- movement problems, such as stiffness or shaking
- seeing or hearing things that aren't real (hallucinations)
- being unable to pee
Contact 111 or go to A&E immediately if you have any of these symptoms.
Serotonin syndrome
Serotonin syndrome is an uncommon, but potentially serious, set of side effects linked to SSRIs.
Serotonin syndrome occurs when the levels of a chemical in your brain called serotonin become too high. It's usually triggered when you take an SSRI in combination with another medicine (or substance) that also raises serotonin levels, such as another antidepressant or St John's wort.
It's usually triggered when you take an SSRI in combination with another medicine (or substance) that also raises serotonin levels, such as another antidepressant or St John's wort.
Symptoms of serotonin syndrome can include:
- confusion
- agitation
- muscle twitching
- sweating
- shivering
- diarrhoea
If you experience these symptoms, you should stop taking the medicine and seek immediate advice from your GP or specialist. If this isn't possible, call NHS 111.
Symptoms of severe serotonin syndrome include:
- a high temperature of 38C or above
- seizures (fits)
- irregular heartbeat (arrhythmia)
- loss of consciousness
If you or someone you know experiences symptoms of severe serotonin syndrome, seek emergency medical help immediately by dialling 999 and asking for an ambulance.
Hyponatraemia
Elderly people who take SSRIs may experience a severe fall in sodium (salt) levels known as hyponatremia. This may lead to a build-up of fluid inside the body's cells, which can be potentially dangerous.
This side effect occurs because SSRIs can block the effects of a hormone that helps to regulate levels of sodium and fluid in the body. Elderly people are vulnerable because fluid levels become more difficult for the body to regulate.
Mild hyponatremia can cause symptoms similar to depression or side effects of SSRIs, such as:
- feeling sick
- headache
- muscle pain
- reduced appetite
- confusion
More severe hyponatremia can cause the following symptoms:
- feeling listless and tired
- disorientation
- agitation
- psychosis
- seizures (fits)
The most serious cases of hyponatremia can cause you to stop breathing or go into a coma.
If you suspect that you or someone in your care has mild hyponatremia, call your GP or contact 111 for advice and stop taking SSRIs for the time being.
If you suspect severe hyponatremia, call 999 to ask for an ambulance.
Hyponatremia can be treated by feeding a sodium solution into the body through an intravenous drip.
Suicidal thoughts
Some people have suicidal thoughts and a desire to self-harm when they first take SSRIs. Young people under 25 seem particularly at risk.
Contact your GP or go to hospital immediately if you have thoughts of killing or harming yourself at any time while you're taking SSRIs.
It may be useful to tell a relative or close friend that you've started taking antidepressants and ask them to read the leaflet that comes with your medicine.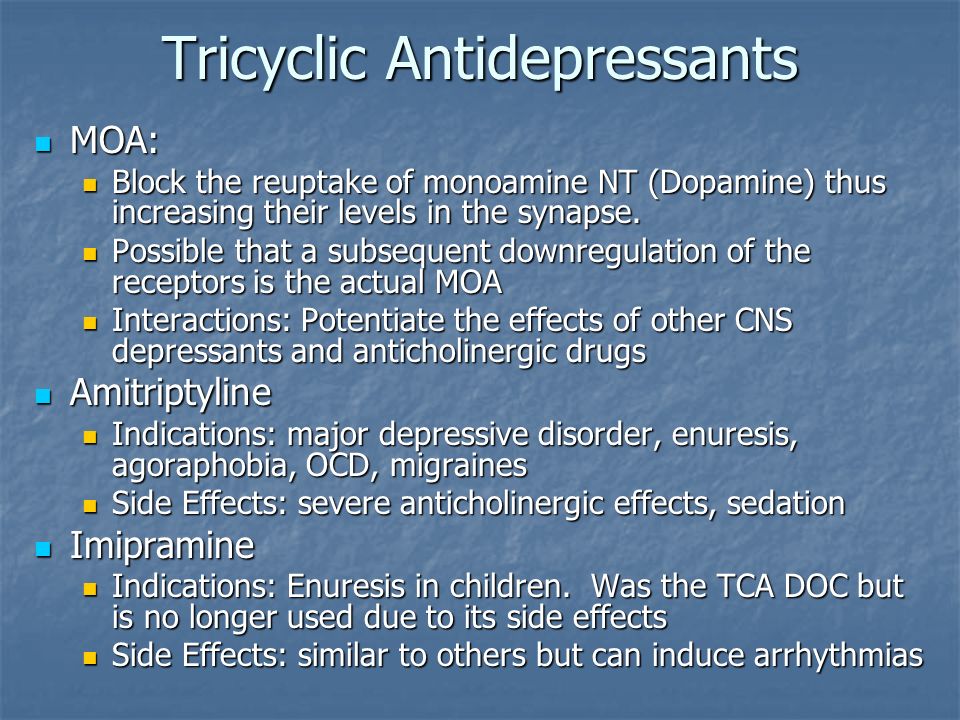 Ask them to tell you if they think your symptoms are getting worse, or if they're worried about changes in your behaviour.
Ask them to tell you if they think your symptoms are getting worse, or if they're worried about changes in your behaviour.
Reporting side effects
The Yellow Card Scheme allows you to report suspected side effects from any type of medicine you're taking. It's run by the medicines safety watchdog, the Medicines and Healthcare products Regulatory Agency (MHRA).
Page last reviewed: 8 December 2021
Next review due: 8 December 2024
SIDE EFFECTS OF ANTIDEPRESSANTS (SSRIs) | Clinical Center "Psychiatry - Narcology"
Currently, the most commonly prescribed antidepressants are drugs from the group of selective serotonin reuptake inhibitors (SSRIs). For most, these medicines are safe and effective, but like all medicines, they can cause side effects. According to statistics, about 40% of patients taking antidepressants also experience side effects, in about 25% of cases they are quite unpleasant.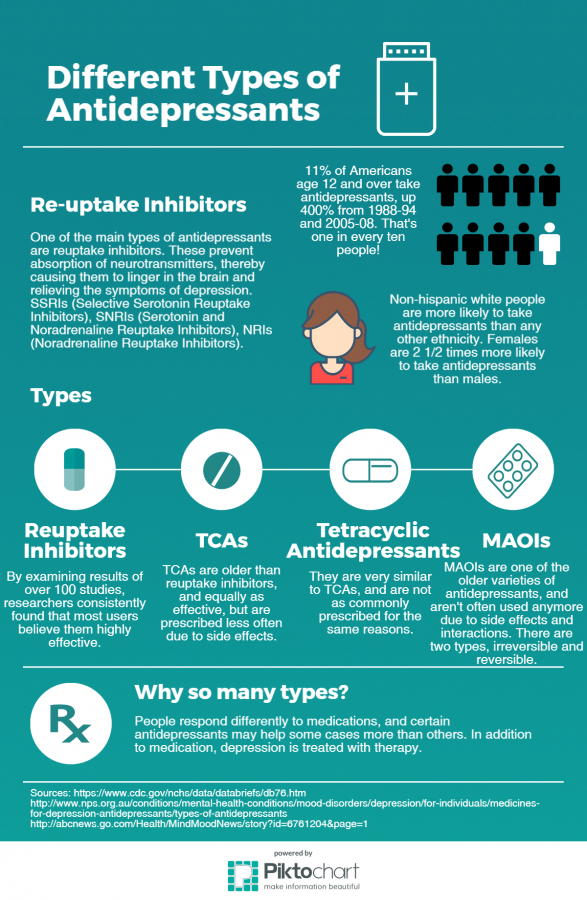 Two of the most common side effects (sexual dysfunction and weight gain) are often the reason people stop taking these medications.
Two of the most common side effects (sexual dysfunction and weight gain) are often the reason people stop taking these medications.
Listed below are the 7 most common side effects of antidepressants that patients should be aware of:
1. SOMATIC SYMPTOMS.
When medications are first prescribed to treat depression, the most common physical symptoms are headache, nausea, joint and muscle pain, rash, and diarrhea. These symptoms are usually mild and temporary. The results of clinical studies have shown that nausea and headache are the most common. As a rule, these symptoms are adaptive in nature, as a rule, they pass on their own, without requiring discontinuation of the drug.
2. SLEEP DISTURBANCE.
Many patients, when first prescribed antidepressants, report problems with sleep: difficulty falling asleep or light sleep with frequent awakenings. Also, against the background of taking SSRIs, nightmares and sleepwalking can be observed. Studies have shown that about 22% of people taking antidepressants experience sleep problems.
Studies have shown that about 22% of people taking antidepressants experience sleep problems.
3. DAY SLEEPNESS .
Sleepiness during the day may be the result of a poor night's sleep, or the direct sedative effect of the antidepressant. In the case when it is a sedative effect, the problem can be solved by transferring the drug to the evening.
4. MIGRAINES
Due to the fact that people who are prone to depression also often suffer from migraines, you need to be careful when taking medications in combination. Medicines; used to treat migraines, triptans, like SSRIs, increase serotonin levels in the brain. If these drugs are used together, it can lead to the development of serotonin syndrome, which manifests itself in the form of headache, heart palpitations, hot flashes. Be sure to discuss with your doctor how to avoid the development of serotonin syndrome if you are prescribed medications of both groups.
5. WEIGHT SET.
WEIGHT SET.
Weight gain is one of the late side effects of antidepressants and is one of the most common reasons for refusing to continue taking or changing the drug. A good prevention of this side effect is moderate physical activity (for example, a 30-minute workout every other day). The likelihood of weight gain also depends on the drug that is prescribed. According to clinical trials, while taking paroxetine, about 25% of patients gain 7% of their weight.
6. SUICIDE .
The risk of suicide while taking antidepressants is currently under extensive investigation. According to most studies, compared with placebo, taking SSRIs or other antidepressants doubles the likelihood of suicidal thoughts. The overall risk of this side effect when taking antidepressants in adolescents and adults is 2 to 4 percent. One of the reasons for suicide while taking antidepressants is that medications increase activity, giving energy for the implementation of a suicidal plan.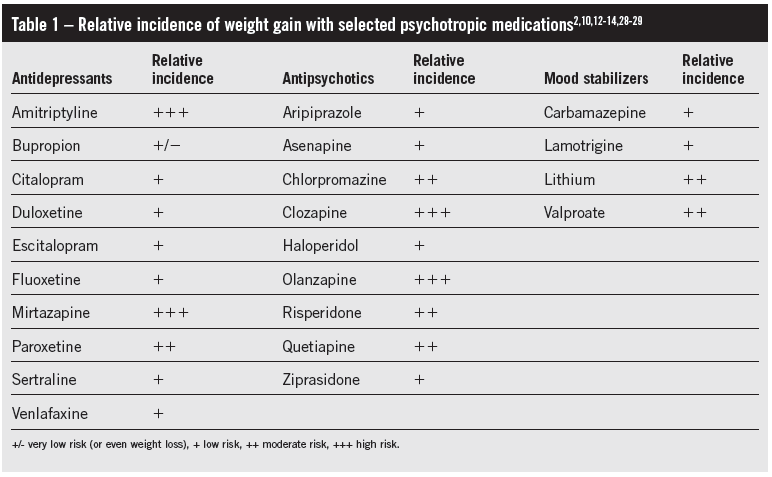 Regular follow-up by a doctor can reduce the risk of this side effect.
Regular follow-up by a doctor can reduce the risk of this side effect.
7. SEXUAL DYSFUNCTION.
Sexual dysfunction is one of the most common long-term side effects of SSRIs. These include decreased sexual desire, delayed ejaculation in men, and inability to achieve orgasm in women. Up to 60% of people taking SSRIs experience one of these side effects. And these are the side effects that patients are not ready to endure.
If you are concerned about any side effects, discuss them with your doctor. As a rule, you can find a solution for any of them. It is not recommended to stop taking medications on your own.
Effects of various antidepressants | Medical Clock
Depression is a serious medical condition most prevalent among adults of all ages worldwide. In recent decades, a significant increase in the frequency of antidepressant use as part of specific therapy among patients with depression has been reported. For example, in the United States of America, 7% of people aged 18 to 39 and 14% of adults aged 40 to 59 are taking antidepressants.
Efficacy and choice of antidepressants
Currently, there are several types of antidepressants with a wide range of possible effects, but the issue of their effectiveness compared with placebo remains debatable. Therefore, when choosing antidepressants, it is necessary to take into account their potential side effects. Many guidelines recommend that selective serotonin reuptake inhibitors be considered as first-line drug therapy for the treatment of patients with depression.
Side effects of antidepressants
Adverse effects have been repeatedly assessed in randomized controlled trials, but these trials are usually performed in selected groups of patients with relatively small sample sizes and rather short duration, so it is not always possible to identify rare but serious side effects. Observational studies have found associations between the use of selective serotonin reuptake inhibitors and an increased risk of fractures and falls, but these studies were either limited to the elderly, or they were dominated by results that already occur quite often at the appropriate age.
There is some evidence that antidepressants may impair driving ability among the elderly, but the evidence for younger drivers is mixed. Similarly, studies have found an increased risk of gastrointestinal bleeding, adverse drug reactions, and all-cause mortality associated with antidepressant use, but again there is insufficient evidence for young and middle-aged individuals, among whom a similar risk may be lower compared with older people due to more frequent comorbidity, interaction with other prescribed drugs and increased susceptibility to adverse effects among the latter.
Objectives of this study
Given the lack of evidence regarding the safety of antidepressants in young and middle-aged people, despite the large number of prescriptions given to this population over fairly long periods, scientists in the UK conducted a large cohort study among patients aged 20-64 years to study the relationship between the use of various antidepressants and the risks of developing some potentially adverse side effects. The results of this work were published on March 8, 2018 in the journal BMC Medicine.
The results of this work were published on March 8, 2018 in the journal BMC Medicine.
Methods and variables
Falls, fractures, upper gastrointestinal bleeding, road traffic accidents, adverse drug reactions, and all-cause mortality were considered as adverse outcomes. At the time of the study, the selected primary care database included the health records of over 12 million patients from over 600 general practitioners in the United Kingdom. Registered information includes patient characteristics, clinical diagnoses, symptoms, and medications prescribed. The study cohort included patients aged 20–64 years with the first reported diagnosis of depression during the period from January 1, 2000 to July 31, 2011.
For the purposes of this study, antidepressants are grouped according to their four major classes according to the British National Formulary: tricyclic and related antidepressants, selective serotonin reuptake inhibitors, monoamine oxidase inhibitors, and other antidepressants.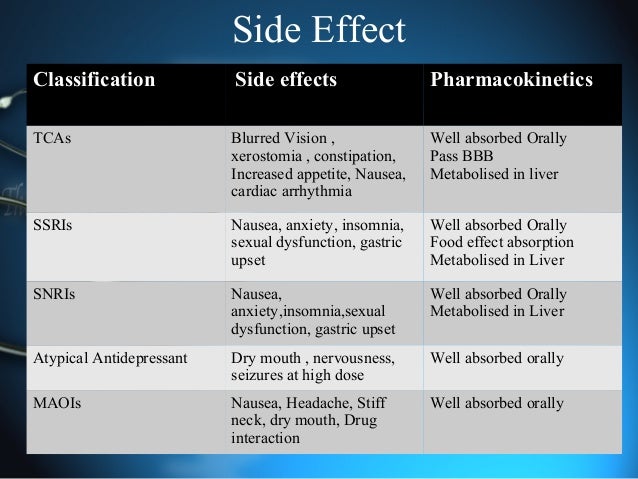 To calculate the daily dose of each drug, scientists used the values provided by the World Health Organization's Collaborating Center for Drug Statistics Methodology.
To calculate the daily dose of each drug, scientists used the values provided by the World Health Organization's Collaborating Center for Drug Statistics Methodology.
Age of patients at baseline and at first diagnosis of depression, gender, smoking and alcohol use status, depression severity, ethnicity, baseline comorbidities (coronary heart disease, stroke or transient ischemic attack, diabetes diabetes, hypertension, cancer, epilepsy or seizures, hypothyroidism, osteoarthritis, rheumatoid arthritis, asthma or chronic obstructive pulmonary disease, osteoporosis, kidney and/or liver disease, obsessive-compulsive disorder) and baseline use of other drugs ( antihypertensive drugs, acetylsalicylic acid, statins, anticoagulants, nonsteroidal anti-inflammatory drugs, anticonvulsants, hypnotics/anxiolytics, antipsychotics, bisphosphonates, oral contraceptives, hormone replacement therapy).
Study results
The initial cohort consisted of 327,235 patients with a first diagnosis of depression during the follow-up period and aged 20 to 64 years.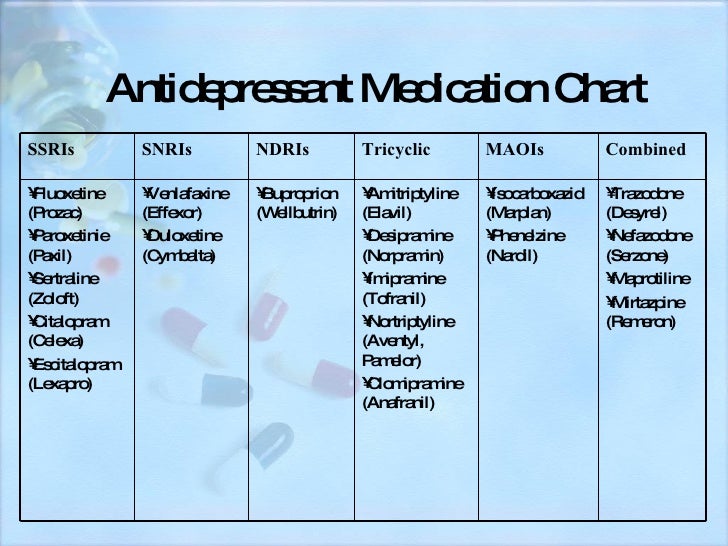 A total of 88,272 (27.0%) patients were excluded due to established inclusion criteria. The final sample consisted of 238,963 patients, of which 146,028 (61%) were female, with a mean age of 39.5 years. The total duration of follow-up was 1,307,326 person-years, with a median of 5.2 years per subject.
A total of 88,272 (27.0%) patients were excluded due to established inclusion criteria. The final sample consisted of 238,963 patients, of which 146,028 (61%) were female, with a mean age of 39.5 years. The total duration of follow-up was 1,307,326 person-years, with a median of 5.2 years per subject.
Most patients (209,476 (87.7%)) were found to be taking antidepressants during follow-up. The median duration of treatment was 221 days, with 36.6% of patients taking drugs for more than 1 year and 5.5% for ≥5 years. Selective serotonin reuptake inhibitors were the most commonly prescribed class of antidepressants (189,968 patients, 2,379,668 prescriptions), followed by tricyclic and related antidepressants (61,901 patients, 533,798 prescriptions), other antidepressants (33,631 patients, 422,079 prescriptions).prescriptions) and monoamine oxidase inhibitors (156 patients, 1791 prescriptions in total). During the same period, 83,784 prescriptions for combination therapy were issued, in which two or more different antidepressants were prescribed for use within one day.
Researchers have found that selective serotonin reuptake inhibitors and the category "other antidepressants" are associated with a significantly increased risk of bone fracture, with all drug groups associated with a significantly increased risk of falls. The use of tricyclic and related antidepressants, as well as other antidepressants, is associated with a slightly higher risk of developing adverse reactions to the use of drugs compared with selective serotonin reuptake inhibitors. Mortality rates were significantly higher with tricyclic and other antidepressants than with selective serotonin reuptake inhibitors during 5 years of follow-up, but not during the first year.
In this cohort of patients aged 20–64 years, the absolute risks of adverse outcomes were mostly < 0.6% per year, and for falls, fractures, gastrointestinal bleeding, and all-cause mortality, they were significantly lower than equivalent risks among the elderly. While the risks associated with the use of antidepressants are low for individuals, given the widespread use of these drugs in adults, the impact at the population level may be greater.