Antidepressants that do not cause erectile dysfunction
Sexual dysfunction in selective serotonin reuptake inhibitors (SSRIs) and potential solutions: A narrative literature review
1. Kim WK, Shin D, Song WO. . Depression and Its comorbid conditions more serious in women than in men in the United States. J Womens Health (Larchmt). 2015; 24 12: 978- 85. DOI: 10.1089/jwh.2014.4919. PubMed PMID: 26131726. [PubMed] [Google Scholar]
2. Olfson M, Marcus SC. . National patterns in antidepressant medication treatment. Arch Gen Psychiatry. 2009; 66 8: 848- 56. DOI: 10.1001/archgenpsychiatry.2009.81. PubMed PMID: 19652124. [PubMed] [Google Scholar]
3. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder, 3rd ed. Arlington (VA): The Association; 2010. [Google Scholar]
4. Rosenber KP, Bleiberg KL, Koscis J, Gross C. . A survey of sexual side effects among severely mentally ill patients taking psychotropic medications: impact on compliance. J Sex Marital Ther. 2003; 29 4: 289- 96. PubMed PMID: 14504017. [PubMed] [Google Scholar]
5. Waldinger MD. . Psychiatric disorders and sexual dysfunction. Handb Clin Neurol. 2015; 130: 469- 89. DOI: 10.1016/B978-0-444-63247-0.00027-4. PubMed PMID: 26003261. [PubMed] [Google Scholar]
6. Huang XK, Lu YP, Luo SW, Wang F, Xiet ZY, Wang XD. . Efficacy and safety of selective serotonin re-uptake inhibitors in the treatment of premature ejaculation: a systematic evaluation. Zhonghua Nan Ke Xue. 2009; 15 3: 248- 55. Chinese. PubMed PMID: 19452699. [PubMed] [Google Scholar]
7. Stimmel GL, Gutierrez MA. . Counseling patients about sexual issues. Pharmacotherapy. 2006; 26 11: 1608- 15. DOI: 10.1592/phco.26.11.1608. PubMed PMID: 17064206. [PubMed] [Google Scholar]
8. Kennedy SH, Dickens SE, Eisfeld BS, Bagby RM. . Sexual dysfunction before antidepressant therapy in major depression. J Affect Disord. 1999; 56 2-3: 201- 8. DOI: 10.1016/S0165-0327(99)00050-6. PubMed PMID: 10701478. [PubMed] [Google Scholar]
9. Stahl SM. . Mechanism of action of serotonin selective reuptake inhibitors. Serotonin receptors and pathways mediate therapeutic effects and side effects. J Affect Disord. 1998; 51 3: 215- 35. DOI: 10.1016/S0165-0327(98)00221-3. PubMed PMID: 10333979. [PubMed] [Google Scholar]
Stahl SM. . Mechanism of action of serotonin selective reuptake inhibitors. Serotonin receptors and pathways mediate therapeutic effects and side effects. J Affect Disord. 1998; 51 3: 215- 35. DOI: 10.1016/S0165-0327(98)00221-3. PubMed PMID: 10333979. [PubMed] [Google Scholar]
10. Montejo-Gonzales AL, Llorca G, Izquierdo JA, Ledesma A, Bousono M, Calcedo A, et al.. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther. 1997; 23 3: 176- 94. PubMed PMID: 9292833. [PubMed] [Google Scholar]
11. Safa M, Sadr S, Talischi F, . Ghasem Boroujerdi F. Study of effects of selective serotonin reuptake inhibitors on stages of sexual function in Iranian patients with major depressive disorder. Ther Adv Psychopharmacol. 2013; 3 6: 306- 13. DOI: 10.1177/2045125313488906. PubMed PMID: 24294483. [PMC free article] [PubMed] [Google Scholar]
12. Keltner NL, McAfee KM, Taylor CL. . Mechanisms and treatments of SSRI-induced sexual dysfunction. Perspect Psychiatr Care. 2002; 38 3: 111- 6. PubMed PMID: 12385082. [PubMed] [Google Scholar]
. Mechanisms and treatments of SSRI-induced sexual dysfunction. Perspect Psychiatr Care. 2002; 38 3: 111- 6. PubMed PMID: 12385082. [PubMed] [Google Scholar]
13. Sidi H, Asmidar D, Hod R, Guan NC. . Female sexual dysfunction in patients treated with antidepressant-comparison between escitalopram and fluoxetine. J Sex Med. 2012; 9 5: 1392- 9. DOI: 10.1111/j.1743-6109.2011.02256.x. PubMed PMID: 21477024. [PubMed] [Google Scholar]
14. Waldinger MD, Zwinderman AH, Schweitzer DH, Olivier B. . Relevance of methodological design for the interpretation of efficacy of drug treatment of premature ejaculation: a systematic review and meta-analysis. Int J Impot Res. 2004; 16 4: 369- 81. DOI: 10.1038/sj.ijir.3901172. PubMed PMID: 14961051. [PubMed] [Google Scholar]
15. Hirschfeld RM. . Long-term side effects of SSRIs: sexual dysfunction and weight gain. J Clin Psychiatry. 2003; 64 Suppl 18: 20- 4. PubMed PMID: 14700451. [PubMed] [Google Scholar]
16. Arlas F, Padin JJ, Rivas MT, Sánchez A. . Sexual dysfunctions induced by serotonin reuptake inhibitors. Aten Primaria. 2000; 26 6: 389- 94. Spanish. PubMed PMID: 11111311. [PMC free article] [PubMed] [Google Scholar]
. Sexual dysfunctions induced by serotonin reuptake inhibitors. Aten Primaria. 2000; 26 6: 389- 94. Spanish. PubMed PMID: 11111311. [PMC free article] [PubMed] [Google Scholar]
17. Waldinger MD, Zwinderman AH, SSRIs Olivier B.. and ejaculation: a double-blind, randomized, fixed-dose study with paroxetine and citalopram. J Clin Psychopharmacol. 2001; 21 6: 556- 60. DOI: 10.1097/00004714-200112000-00003. PubMed PMID: 11763001. [PubMed] [Google Scholar]
18. Keltner NL, McAfee KM, Taylor CL. . Mechanisms and treatments of SSRI-induced sexual dysfunction. Perspect Psychiatr Care. 2002; 38 3: 111- 6. PubMed PMID: 12385082. [PubMed] [Google Scholar]
19. Gelenberg AJ, McGahuey C, Laukes C, Okayli G, Moreno F, Zentner L, et al.. Mirtazapine substitution in SSRI-induced sexual dysfunction. J Clin Psychiatry. 2000; 61 5: 356- 60. PubMed PMID: 10847310. [PubMed] [Google Scholar]
20. Gelenberg AJ, Dunner DL, Rothschild AJ, Pedersen R, Dorries KM, Ninan PT. . Sexual functioning in patients with recurrent major depressive disorder enrolled in the PREVENT study. J Nerv Ment Dis. 2013; 201 4: 266- 73. DOI: 10.1097/NMD.0b013e318288d298. PubMed PMID: 23538970. [PubMed] [Google Scholar]
J Nerv Ment Dis. 2013; 201 4: 266- 73. DOI: 10.1097/NMD.0b013e318288d298. PubMed PMID: 23538970. [PubMed] [Google Scholar]
21. Safarinejad MR. . The effects of the adjunctive bupropion on male sexual dysfunction induced by a selective serotonin reuptake inhibitor: a double-blind placebo-controlled and randomized study. BJU Int. 2010; 106 6: 840- 7. DOI: 10.1111/j.1464-410X.2009.09154.x. PubMed PMID: 20067456. [PubMed] [Google Scholar]
22. DailyMed.NLM.NIH.gov [Internet]. Bethesda (MD): U.S. National Library of Medicine [Updated October 29, 2015]. Label: Effexor XR- venlafaxine hydrochloride capsule, extended release. Available from: http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=53c3e7ac-1852-4d70-d2b6-4fca819acf26.
23. Thase ME, Clayton AH, Haight BR, Thompson AH, Modell JG, Johnston JA. . A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability. J Clin Psychopharmacol. 2006; 26 5: 482- 8. DOI: 10.1097/01.jcp.0000239790.83707.ab. PubMed PMID: 16974189. [PubMed] [Google Scholar]
DOI: 10.1097/01.jcp.0000239790.83707.ab. PubMed PMID: 16974189. [PubMed] [Google Scholar]
24. Clayton AH, Warnock JK, Kornstein SG, Pinkerton R, Sheldon-Keller A, McGarvey EL. . A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry. 2004; 65 1: 62- 7. DOI: 10.4088/JCP.v65n0110. PubMed PMID: 14744170. [PubMed] [Google Scholar]
25. Ashton AK, Rosen RC. . Bupropion as an antidote for serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry. 1998; 59 3: 112- 5. DOI: 10.4088/JCP.v59n0304. PubMed PMID: 9541153. [PubMed] [Google Scholar]
26. Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F. . Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients. Spanish Working Group for the Study of Psychotropic-Related Sexual Dysfunction. J Clin Psychiatry. 2001; 62 Suppl 3: 10- 21. PubMed PMID: 11229449. [PubMed] [Google Scholar]
[PubMed] [Google Scholar]
27. Schwartz TL, Siddiqui UA, Stahl SM. . Vilazodone: a brief pharmacological and clinical review of the novel serotonin partial agonist and reuptake inhibitor. Ther Adv Psychopharmacol. 2011; 1 3: 81- 7. DOI: 10.1177/2045125311409486. PubMed PMID: 23983930. [PMC free article] [PubMed] [Google Scholar]
28. Clayton AH, Gommoll C, Chen D, Nunez R, Mathews M. . Sexual dysfunction during treatment of major depressive disorder with vilazodone, citalopram, or placebo: results from a phase IV clinical trial. Int Clin Psychopharmacol. 2015; 30 4: 216- 23. DOI: 10.1097/YIC.0000000000000075. PubMed PMID: 26039688. [PMC free article] [PubMed] [Google Scholar]
29. Jacobsen PL, Mahableshwarkar AR, Palo WA, Chen Y, Dragheim M, Clayton AH. . Treatment-emergent sexual dysfunction in randomized trials of vortioxetine for major depressive disorder or generalized anxiety disorder: a pooled analysis. CNS Spectr. 2015; 17: 1- 12. PubMed PMID: 26575433. [PubMed] [Google Scholar]
30. Taylor MJ, Rudkin L, Bullemor-Day P, Lubin J, Chukwujekwu C, Hawton K. . Strategies for managing sexual dysfunction induced by antidepressant medication. Cochran Database Syst Rev. 2013; 5:CD003382. DOI: 10.1002/14651858.CD003382.pub3. PubMed PMID: 23728643. [PubMed]
Taylor MJ, Rudkin L, Bullemor-Day P, Lubin J, Chukwujekwu C, Hawton K. . Strategies for managing sexual dysfunction induced by antidepressant medication. Cochran Database Syst Rev. 2013; 5:CD003382. DOI: 10.1002/14651858.CD003382.pub3. PubMed PMID: 23728643. [PubMed]
31. Modabbernia A, Sohrabi H, Nasehi AA, Raisi F, Saroukhani S, Jamshidi A, et al.. Effect of saffron on fluoxetine-induced sexual impairment in men: randomized double-blind placebo-controlled trial. Psychopharmacology (Berl). 2012; 223 4: 381- 8. DOI: 10.1007/s00213-012-2729-6. PubMed PMID: 22552758. [PubMed] [Google Scholar]
32. Wang Y, Han T, Zhu Y, Zheng CJ, Ming QL, Rahman K, et al.. Antidepressant properties of bioactive fractions from the extract of Crocus sativus L. J Nat Med. 2010; 64 1: 24- 30. DOI: 10.1007/s11418-009-0360-6. PubMed PMID: 19787421. [PubMed] [Google Scholar]
33. Kashani L, Raisi F, Saroukhani S, Sohrabi H, Modabbernia A, Nasehi AA, et al.. Saffron for treatment of fluoxetine-induced sexual dysfunction in women: randomized double-blind placebo-controlled study. Hum Psychopharmacol. 2013; 28 1: 54- 60. DOI: 10.1002/hup.2282. PubMed PMID: 23280545. [PubMed] [Google Scholar]
Hum Psychopharmacol. 2013; 28 1: 54- 60. DOI: 10.1002/hup.2282. PubMed PMID: 23280545. [PubMed] [Google Scholar]
Antidepressants: Which cause the fewest sexual side effects?
Sexual side effects are common with antidepressants in both men and women, so your concern is understandable. Effects on sexual function can include:
- A change in your desire for sex
- Erectile problems
- Orgasm problems
- Problems with arousal, comfort and satisfaction
The severity of sexual side effects depends on the individual and the specific type and dose of antidepressant. For some people, sexual side effects are minor or may ease up as their bodies adjust to the medication. For others, sexual side effects continue to be a problem.
Antidepressants with the lowest rate of sexual side effects include:
- Bupropion (Wellbutrin XL, Wellbutrin SR)
- Mirtazapine (Remeron)
- Vilazodone (Viibryd)
- Vortioxetine (Trintellix)
Antidepressants most likely to cause sexual side effects include:
- Selective serotonin reuptake inhibitors (SSRIs), which include citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), paroxetine (Paxil, Pexeva) and sertraline (Zoloft).

- Serotonin and norepinephrine reuptake inhibitors (SNRIs), which include venlafaxine (Effexor XR), desvenlafaxine (Pristiq) and duloxetine (Cymbalta).
- Tricyclic and tetracyclic antidepressants, such as amitriptyline, nortriptyline (Pamelor) and clomipramine (Anafranil).
- Monoamine oxidase inhibitors (MAOIs), such as isocarboxazid (Marplan), phenelzine (Nardil) and tranylcypromine (Parnate). However, selegiline (Emsam), an MAOI that you stick on your skin as a patch, has a low risk of sexual side effects.
If you're taking an antidepressant that causes sexual side effects, your doctor may recommend one or more of these strategies:
- Waiting several weeks to see whether sexual side effects get better.
- Adjusting the dose of your antidepressant to reduce the risk of sexual side effects. But always talk with your doctor before changing your dose.

- Switching to another antidepressant that may be less likely to cause sexual side effects.
- Adding a second antidepressant or another type of medication to counter sexual side effects. For example, the addition of the antidepressant bupropion may ease sexual side effects caused by another antidepressant.
- Adding a medication to improve sexual function, such as sildenafil (Viagra), tadalafil (Cialis) or vardenafil (Levitra, Staxyn). These medications are approved by the Food and Drug Administration only to treat sexual problems in men. Limited research suggests that sildenafil may improve sexual problems caused by antidepressants in some women, but more information is needed on its effectiveness and safety in women.
Stopping medication because of sexual side effects is a common problem, and for most people this means depression returns. Work with your doctor to find an effective antidepressant or combination of medications that will reduce your sexual side effects and keep your depression under control.
If you're pregnant or trying to become pregnant, tell your doctor, as this may affect the type of antidepressant that's appropriate.
Be patient. Everyone reacts differently to antidepressants, so it may take some trial and error to identify what works best for you.
Last Updated: January 25th, 2020
© 1998-2022 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved.
Terms of Use
Sexual dysfunction due to antidepressants
… this problem is widely underestimated and very rarely addressed by specialists in consultations.
Unfortunately …
Major depressive disorder (MDD) affects about 6% of men and 18% of women. The lifetime risk of the disease is 7-12% for men and 20-25% for women. In somatic patients, the prevalence of depression reaches 20-35% and is comparable to the prevalence of arterial hypertension or even exceeds it.![]() The risk of depression is highest in patients with medical conditions (eg, cardiovascular disease, diabetes mellitus and other endocrine disorders, cancer, HIV/AIDS, and hepatitis C). Targeted screening reveals depression in 45 to 95% (average - 69%) of patients seeking medical help for somatic symptoms. It is the sole reason for 10 - 20% of visits to general practitioners. The prevalence of depression among patients with severe somatic diseases reaches 20-60%. In the global structure of the disease burden (death + disability), MDD is 4.4% and is in fourth place among all pathologies. It is predicted that by 2020 they will move to second place after coronary artery disease. One should also keep in mind such widespread diseases in the population as panic disorder, adjustment disorder, anxious depression, phobic and anxiety disorder, chronic pain (chronic pain disorder), etc., which are also accompanied by depressive symptoms and have some common etio-pathogenetic ( neurotransmitter) mechanisms with MDD.
The risk of depression is highest in patients with medical conditions (eg, cardiovascular disease, diabetes mellitus and other endocrine disorders, cancer, HIV/AIDS, and hepatitis C). Targeted screening reveals depression in 45 to 95% (average - 69%) of patients seeking medical help for somatic symptoms. It is the sole reason for 10 - 20% of visits to general practitioners. The prevalence of depression among patients with severe somatic diseases reaches 20-60%. In the global structure of the disease burden (death + disability), MDD is 4.4% and is in fourth place among all pathologies. It is predicted that by 2020 they will move to second place after coronary artery disease. One should also keep in mind such widespread diseases in the population as panic disorder, adjustment disorder, anxious depression, phobic and anxiety disorder, chronic pain (chronic pain disorder), etc., which are also accompanied by depressive symptoms and have some common etio-pathogenetic ( neurotransmitter) mechanisms with MDD.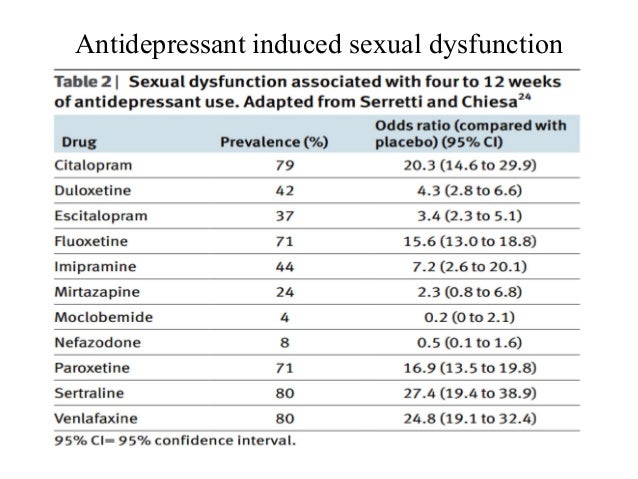
Fortunately …
Doctors have at their disposal drugs that can stop or significantly reduce the manifestations of depressive symptoms - antidepressants depressive disorder). The effectiveness of antidepressants in major depression has been proven in numerous placebo-controlled studies, in the aggregate covering tens of thousands of patients (on average, antidepressants are effective in 55-65% of patients). Antidepressants have a selective effect on depression (and anxiety symptoms), that is, they improve mood, reduce or relieve melancholy, lethargy, apathy, anxiety and emotional stress, increase mental activity, normalize the phase structure and duration of sleep, appetite. The main effect of antidepressants is that they block the breakdown of monoamines (serotonin, norepinephrine, dopamine, phenylethylamine, etc.) under the action of monoamine oxidases (MAO) or block the neuronal reuptake of monoamines, as a result of which the concentration of these mediators in the synaptic cleft increases, due to this, their effects are enhanced (according to modern concepts, one of the leading mechanisms for the development of depression is the lack of monoamines in the synaptic cleft - especially serotonin and dopamine).
Unfortunately …
For most antidepressants, more or less pronounced disorders of sexual function (sexual dysfunction - SDP) are described: decreased and loss of libido, impotence, erectile dysfunction, priapism, lubrification disorders, clitoral disorders, retention or inhibition of ejaculation / orgasm, painful retrograde ejaculation, anorgasmia, partial or complete, dyspareunia and vaginismus, vaginal or penile anesthesia, decreased sexual satisfaction, etc. For example, tricyclic antidepressants (TCAD), having a wide range of effects on neurotransmitter systems and their receptors (serotonin-, norepinephrine- and dopaminergic, blocking α1-adrenergic and h2-histamine receptors, anticholinergic effect on peripheral and central Ach M1 receptors) mainly reduce sexual arousal, as well as desire, cause anorgasmia (delayed or painful ejaculation), and selective inhibitors Serotonin reuptake ryers (SSRIs), by increasing the content of serotonin in the blood, reduce sexual activity, cause anorgasmia and delayed ejaculation. Mood stabilizers - lithium salts - have negative effects on sexual function due to the development of hypothyroidism, weight gain, slowing down of thought processes. Trazodone inhibits serotonin reuptake and acts as a 5-HT2a and 5-HT2c receptor antagonist. It has very few undesirable effects on sexual function, but can sometimes be the cause of priapism.
Mood stabilizers - lithium salts - have negative effects on sexual function due to the development of hypothyroidism, weight gain, slowing down of thought processes. Trazodone inhibits serotonin reuptake and acts as a 5-HT2a and 5-HT2c receptor antagonist. It has very few undesirable effects on sexual function, but can sometimes be the cause of priapism.
However, it should be taken into account that assessment of the true contribution of antidepressants to the development of PDD is difficult, since depressive disorder is classically associated with sexual dysfunction. For example, depression is characterized by a loss of the ability to experience joy (anhedonia) in almost all areas of life, including libido. Loss of interest in sexuality has been reported in approximately 70% of patients with unipolar depression and in approximately 75% of patients with bipolar disorder.
Fortunately …
Currently, there are a number of methods that can limit the adverse effects of drugs, including antidepressants, on sexual function. Important questions such as general satisfaction with sexual life and the nature of sexual problems (decreased desire, problems with erection/lubrification, orgasm, ejaculation, frequency of sexual intercourse and/or masturbation) should be clarified with the patient before prescribing treatment aimed at eliminating PDP. In patients receiving antidepressants for whom sexual function is essential, treatment must be carefully selected. If possible, antidepressants that do not activate the serotonin system should be prescribed; in this case, bupropion, mirtazapine, or trazodone may be the first choice. If the therapeutic effect on serotonin receptors is important, duloxetine is prescribed.
Important questions such as general satisfaction with sexual life and the nature of sexual problems (decreased desire, problems with erection/lubrification, orgasm, ejaculation, frequency of sexual intercourse and/or masturbation) should be clarified with the patient before prescribing treatment aimed at eliminating PDP. In patients receiving antidepressants for whom sexual function is essential, treatment must be carefully selected. If possible, antidepressants that do not activate the serotonin system should be prescribed; in this case, bupropion, mirtazapine, or trazodone may be the first choice. If the therapeutic effect on serotonin receptors is important, duloxetine is prescribed.
The following approaches are available for treating sexual side effects of antidepressants:
► 1 . Wait out the period of adaptation to the side effects of the drug. Improved mood may be associated with a more satisfying sex life. This approach is rarely used due to the fact that only 10% of patients develop tolerance to the side effects of antidepressants; usually ineffective against anorgasmia induced by TCAD; can be applied to patients with low frequency of sexual activity.
► 2 . Reduce dose. This approach is almost never used. The main problem is to find a dose that will reduce the side effects on the sexual sphere without causing symptoms of depression.
► 3 . Plan sexual activity before taking an antidepressant. This means that the drug is prescribed immediately after sexual activity, for example, before bedtime. This tactic may only be useful for antidepressants with a short half-life.
► 4 . Temporarily stop the drug. You can partially reduce the dose of the antidepressant or stop taking it for several days (for example, from Friday evening to Sunday morning) and consider sexual activity at the end of this period. This approach may be effective for drugs with a short half-life (eg, paroxetine, sertraline) and not at all effective for drugs with a long half-life, such as fluoxetine (Prozac).
► 5 . Change antidepressant. This tactic has been described as the most successful. SSRIs can be replaced by bupropion or mirtazapine, which rarely cause PDP. However, changing the antidepressant does not always achieve such a therapeutic effect and is associated with other side effects, such as weight gain. For patients with anxiety, an alternative would be to switch to duloxetine, an antidepressant that responds to depression with anxiety and causes the least negative effect on sexual function.
However, changing the antidepressant does not always achieve such a therapeutic effect and is associated with other side effects, such as weight gain. For patients with anxiety, an alternative would be to switch to duloxetine, an antidepressant that responds to depression with anxiety and causes the least negative effect on sexual function.
► 6 . Apply correctors. The use of corrective treatment is by far the most commonly used tactic in clinical practice. Various types of antidotes have been proposed to balance the effect of antidepressants on different types of neurotransmitters (see table). In general, data on these correctors come from small clinical trials and need further study. Currently, effectiveness - in the treatment of side effects of antidepressants on the genital area - has been proven only for bupropion, buspirone and some phosphodiesterase inhibitors (sildenafil, tadalafil).
Please note! Even realizing that antidepressants cause PDP, this problem cannot be solved in isolation or taking into account only its pharmacological component. A comprehensive treatment plan should take into account psychological factors and the normal evolution of personal sexual functioning. Patients should be advised to lead a healthy lifestyle: weight loss, balanced diet, exercise, quit smoking and other bad habits, treatment of addictions.
A comprehensive treatment plan should take into account psychological factors and the normal evolution of personal sexual functioning. Patients should be advised to lead a healthy lifestyle: weight loss, balanced diet, exercise, quit smoking and other bad habits, treatment of addictions.
Medicines that can cause erectile dysfunction: 9 types | Cavalcanti Institute of Andrology
There are several factors that can affect a man's sexual potency, including medications that can cause erectile dysfunction.
Read in this text which types of drugs can interfere with male sexual activity.
What can cause impotence in a man?
If a man suffers from erection problems, the explanation may be a careful study of his medication list.
We can classify as erectile dysfunction when a man is unable to achieve or maintain an erection for full penetrative intercourse. This is usually a problem that men over 40 begin to face.
There are many causes of sexual potency problems other than aging, such as comorbidities (such as diabetes, hypertension, and heart disease), obesity, sedentary lifestyle, or hormonal imbalances.
What many men don't know, however, is that certain medications can also alter sexual potency, affecting not only desire but also blood flow and even neurotransmitter stimuli.
Second Harvard Health Special Report titled "Erectile Dysfunction: How Medications, Lifestyle Changes, and Other Treatments Can Help You Overcome This Nagging Problem", about 25% of all cases of erectile dysfunction are the result of exposure to some type of drugs such as medicines. .
Without even realizing it, after they start taking certain drugs, men begin to experience weak erections, or even not achieve a hardness suitable for sex at all.
What drugs can cause erectile dysfunction?
In addition to organic causes, some classes of drugs have a greater side effect on erection. Some of these remedies may or may not be available without a prescription, and the list is quite long. Discover the main ones:
1 - Antihypertensives
Hypertension can cause erectile dysfunction because it hardens and narrows the arteries. However, drugs that control blood pressure can also affect a man's sexual potency. This class of drugs causes the most erection problems.
However, drugs that control blood pressure can also affect a man's sexual potency. This class of drugs causes the most erection problems.
One explanation for this fact is that, while lowering blood pressure in general, they can also affect blood flow to the penis.
The drugs most commonly associated with sexual problems are thiazide diuretics, but beta-blockers can also affect erections.
2 - Antidepressants and psychiatric drugs
Some antidepressants, anxiolytics, sedatives and antipsychotics can interfere with a man's sex life, not only by affecting desire but also delaying ejaculation.
Even while altering hormones such as serotonin, which is the feel-good hormone, these antidepressants are mixed with testosterone, which regulates sexual function by stimulating libido and achieving an erection.
The main antidepressants that affect libido are selective serotonin reuptake inhibitors, norepinephrine inhibitors and tricyclic antidepressants because they alter the neurotransmitter system.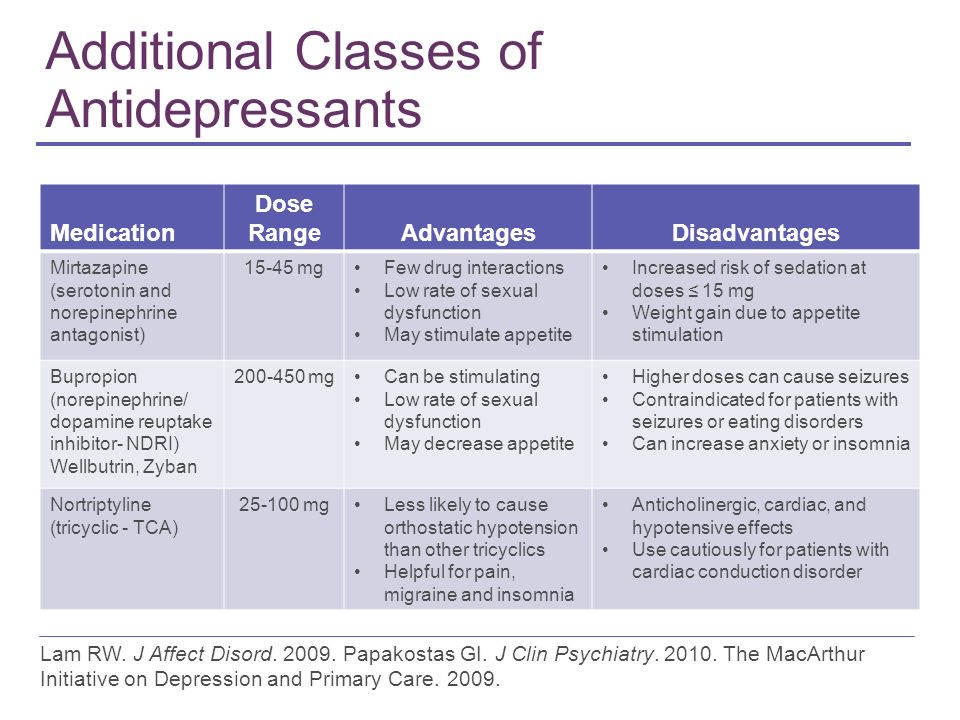
3 - Immunosuppressants
Among the drugs that cause impotence in men, there are also immunosuppressants.
These medicines help treat an autoimmune disease or even prevent organ rejection after a transplant. They reduce the activity of the immune system, as a result, sexual function often suffers.
4 - Antiandrogens
Antiandrogens are used for various problems, for example in the treatment of prostate cancer.
These drugs suppress the function of these hormones that are associated with male characteristics, so they can affect sexual performance, especially if taken for many years, and eventually lead to incomplete erections.
Despite this, these drugs often cannot be stopped, but an alternative medicine can be tried.
5 - Antihistamines
Medicines classified as H2 blockers, which treat allergies, heartburn and nausea, block the action of histamine, which is a substance that affects sexual arousal, helping to relax the smooth muscles of the penis, allowing the blood vessels to fill with blood and make the penis hard.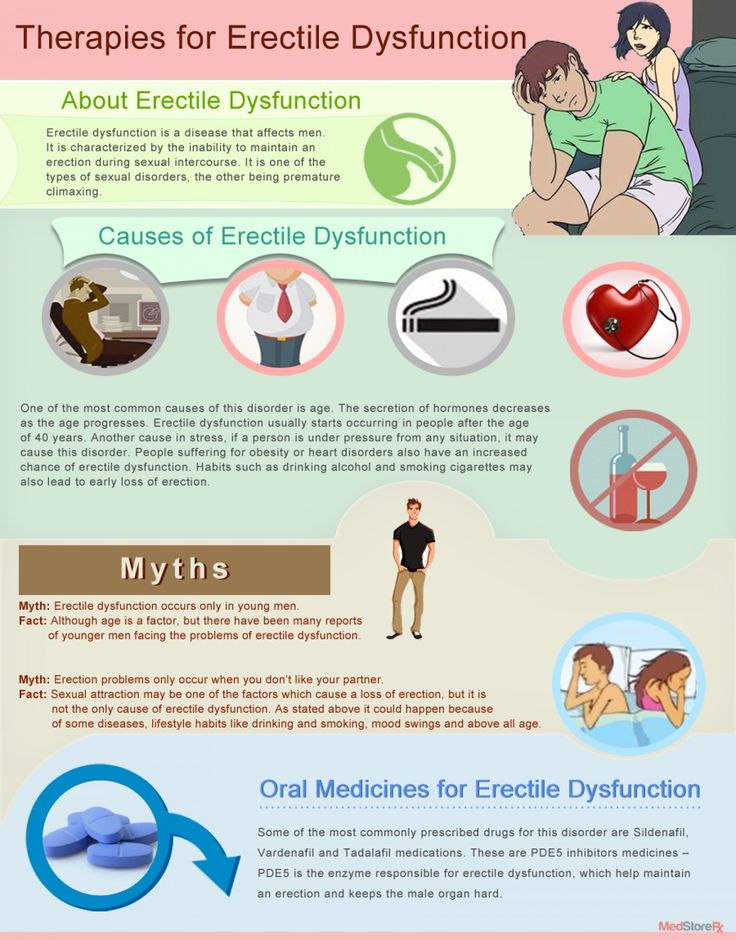
With constant use and frequent blocking of the action of histamine in the body, many men can develop erectile dysfunction.
6 - Hormonal drugs and chemotherapy
Among the drugs that can cause erectile dysfunction are cancer drugs that include hormone therapy to slow the progression of the disease.
Some of these drugs have an anti-androgenic effect, that is, they reduce the effect of testosterone and thus affect a man's sex life, changing not only sexual desire, but also fertility.
7 - Opioids
Among drugs that can cause erectile dysfunction, are opioids such as codeine and morphine. This class of drugs is commonly prescribed to treat pain.
These drugs can cause erectile dysfunction because they interfere with signaling between the pituitary, hypothalamus, and testicles, causing a very dramatic drop in testosterone levels.
8 - Hair loss medications
Some alopecia medications can lower dihydrotestosterone, which is also essential for erectile function as it directly affects libido.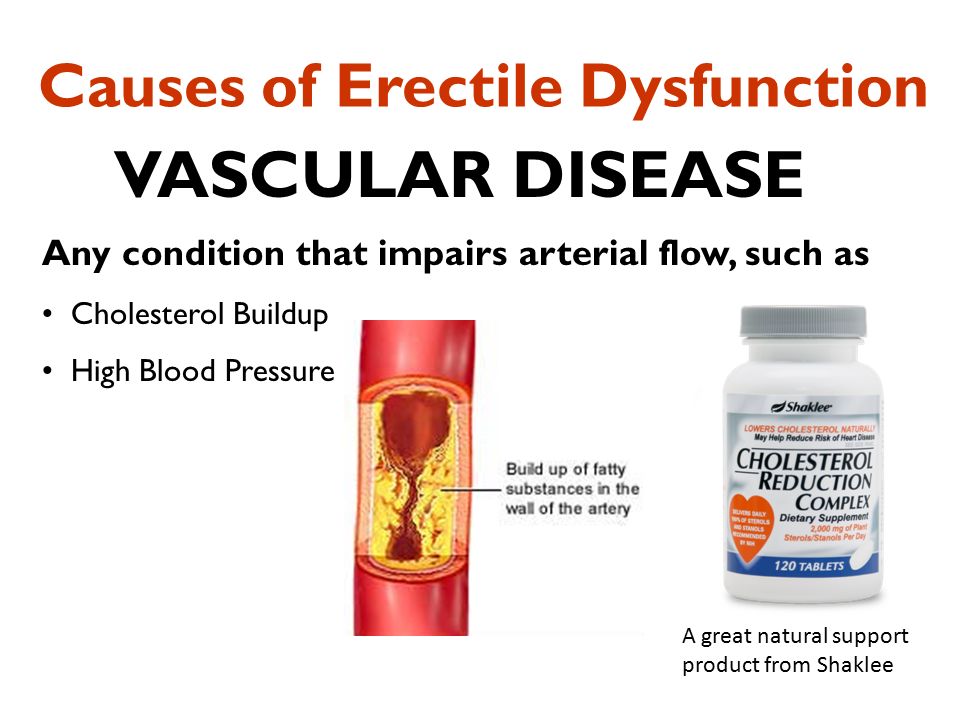 Among them is finasteride, a molecule similar to steroid hormones.
Among them is finasteride, a molecule similar to steroid hormones.
About 10% of men who undergo these hair treatments may suffer in their sex life.
Watch a video about finasteride:
9 - Antiepileptic drugs
These drugs, which help prevent epileptic seizures, can also change a man's ability to orgasm.
Medicines that can cause erectile dysfunction: what to do?
To find out more about the lack of reaction of the body during sex, you need to see a urologist or andrologist who will check if erectile dysfunction may be due to factors other than medication.
If the urologist finds that the drugs are causing erectile dysfunction, the drugs can be changed or even the dosage changed so as not to compromise the original treatment.