Therapeutic safety plan
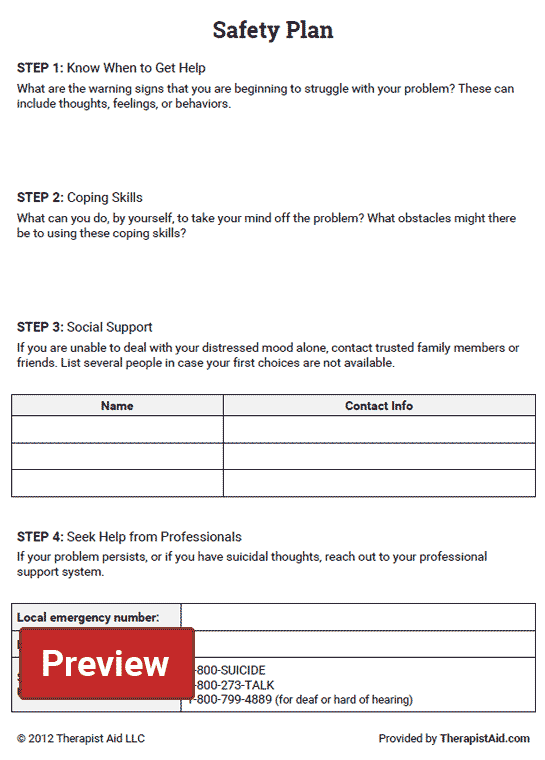
6 Steps to Develop a Safety Plan
Suicide is the 10th leading cause of death in the Unites States. Every year, more than 44,000 Americans die by suicide. While there is no “one size fits all” treatment for someone experiencing suicidal thoughts, evidence shows that protective factors can help lessen the likelihood of suicide among adults.
At Skyland Trail, clients learn to identify protective factors through our evidence-based treatment model. As part of their treatment plan, clients work with our clinical team to discuss and develop protective factors such as a safety plan that can help decrease suicidal thoughts and behaviors.
Family and friends can encourage a loved one to create a safety plan when he or she is not experiencing suicidal thoughts and can think clearly. A safety plan identifies a set of strategies and support systems that your loved one can use when he or she experiences warning signs of a crisis.
1. Identify warning signs.- What are my thoughts, mood or behaviors during times of crisis?
- What do you experience when you feel extremely distressed?
What can I do to take my mind of my problems without contacting another person?
- Practice a relaxation technique such as meditation
- Engage in a physical activity or hobby like going on a walk or knitting
Who or what social setting will help take your mind off your problems at least for a little while?
Who helps you feel better when you socialize with them?
Example: My friend Bob likes to watch football. When I’m feeling down, I can go watch football with him. It will provide a distraction and I can enjoy the company of a friend without having to talk about my feelings.
Name_____________________________ Phone____________________
Place _____________________________
4. Have a list of people you can ask for helpList family members or friends who you can contact during crisis.
Name_____________________________ Phone____________________
Name_____________________________ Phone____________________
5. Make a list of professionals or agencies to contact during a crisis.- Clinician Name and Phone Number
- Emergency Contacts
- Urgent Care Services
- Suicide Prevention Lifeline Phone: 1-800-273-TALK (8255)
- Crisis Line in Georgia: 1-800-715-4225
Encourage your loved one to complete a safety plan and keep it handy – maybe save it on his or her phone or keep a print out in a purse or wallet. And ensure that you have a copy too. The safety plan is designed to build a person’s sense of internal locus of control and is a helpful resource for both you and your loved one during times of crisis.
Safety Plan FAQ: What It Is and How It Can Help High-Risk Clients
A safety plan is a clinical document that a mental health provider creates to help a client maintain safety. Some clients may never require a safety plan, but you should always be prepared to develop one if safety concerns arise.
Some clients may never require a safety plan, but you should always be prepared to develop one if safety concerns arise.
In this article, we’ll go over:
- What is a safety plan?
- Why is a safety plan important?
- What is included in a safety plan?
- When should I use a safety plan with a client?
- Free templates and resources
What is a safety plan?
A safety plan is a collaboration between a client and therapist. It is a clinical document that outlines strategies for helping a client maintain safety. Sometimes individuals such as a parent, guardian, or partner may participate in the development of the document, as they may play an active part in the plan. A copy of the plan should always be dated and given to the client. The original should be kept in your records.
Why is a safety plan important?
A safety plan is helpful for a client because it reminds them of their coping skills and support system when experiencing unsafe thoughts or behaviors. Examples of unsafe thoughts or behaviors can include:
Examples of unsafe thoughts or behaviors can include:
- Urges to engage in self-harm
- Thoughts of hurting someone else
- Thoughts of suicide
- Experiencing internal voices telling a client to act in a dangerous manner
A safety plan acknowledges what risk factors a client is experiencing, what they can do on their own to maintain safety, who to contact for help, and where to go if they cannot be safe. It also provides a client with resources if they are unable to maintain safety on their own.
If you are aware of a client experiencing unsafe thoughts or behaviors, and a client engages in such behaviors that cause injury or death, you could be held responsible. While a safety plan does not guarantee a client will be safe, it demonstrates that a provider has assessed for risk and addressed the concern to the best of their ability. This is helpful for a provider because it can protect you from potential legal action.
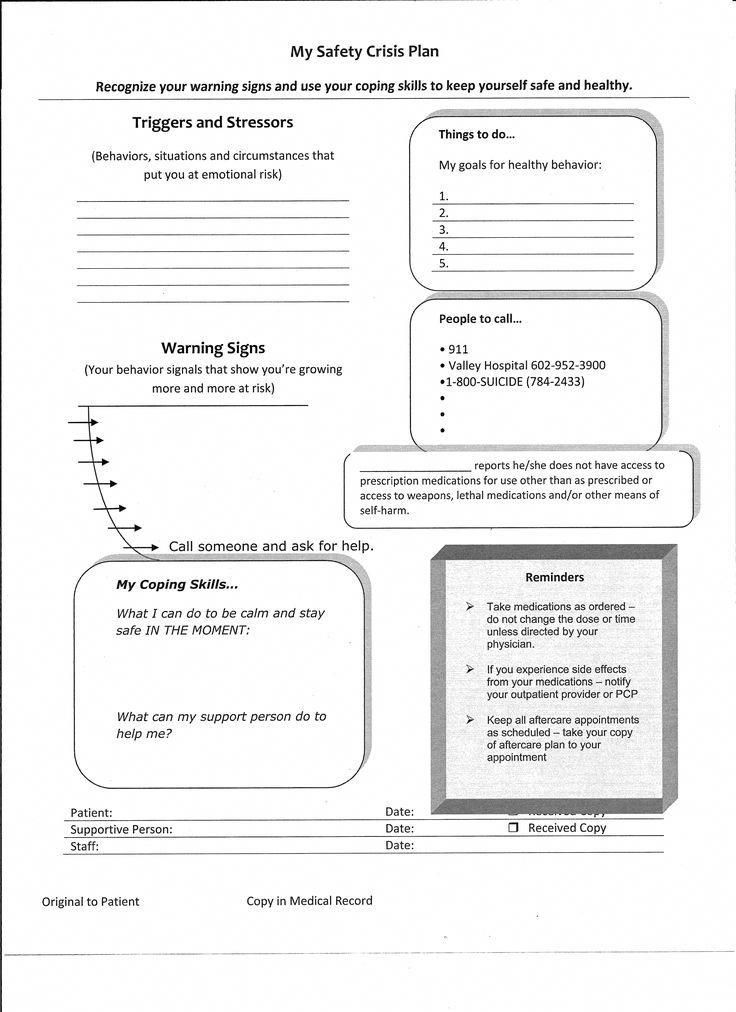
What is included in a safety plan?
✓
TriggersSituations, people, or things that make a client feel upset, angry, sad, anxious, or uncomfortable.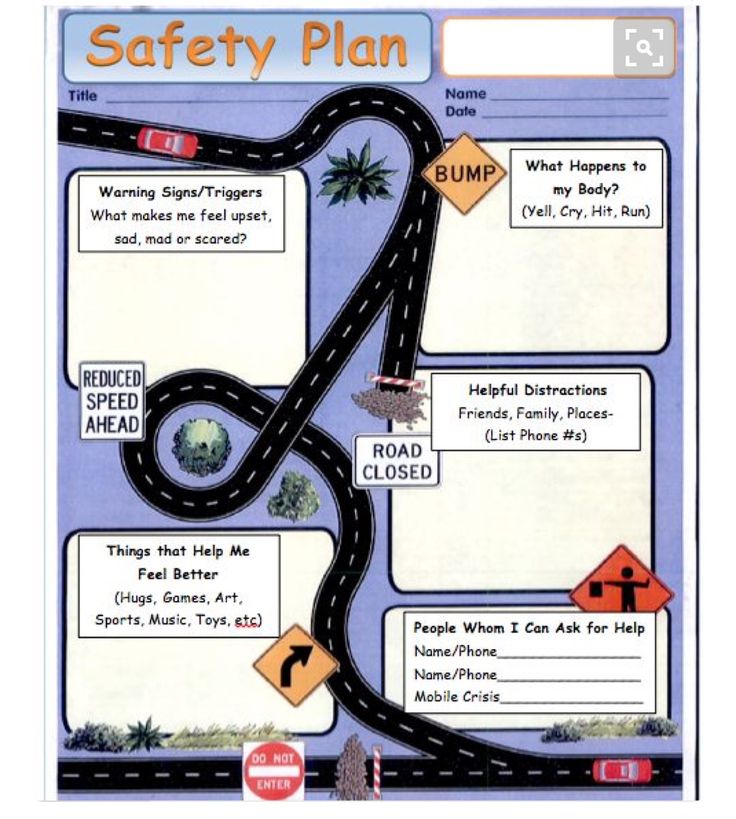
✓
Warning signsThoughts, images, situations, behaviors that indicate a client is experiencing or about to experience unsafe thoughts or behaviors.
✓
Coping skillsThings a client has identified that they can do on their own to self-soothe.
✓
Support systemSomeone a client has identified that they can ask for help.
✓
Professional supportResources a client can use if they are unable to maintain their safety on their own.
✓
AcknowledgmentA copy of the plan is dated and given to the client. The original is kept in your records.
When should I create a safety plan with a client?
Completing a safety plan for a client deemed as high-risk is a best clinical practice. Examples of a high-risk client include, but are not limited to:
- Your client expresses thoughts or feelings about harm to themselves or others
- Your client engages in potentially dangerous behaviors that may result in harm to self or others
- Your client steps down from a higher level of care to outpatient therapy care
- Your client’s response to PHQ-9 question #9, which asks about thoughts related to suicidal ideation
Free templates and resources
- Safety Plan Template: Adult
- Safety Plan Template: Child and adolescent
- Emergency resources
- National Suicide Prevention Lifeline: (800) 273-8255
- For SonderMind providers: CE Webinar: Helping Kids and Adolescents with Self-Harm and Suicidal Thoughts (1.
 5 CEs)
5 CEs)
Get access to more resources
Join SonderMind, and our evidence-based approach to care will give you the additional tools you need to provide the best possible support to even more people in need. Get access to free trainings, case consultation, and an exclusive online forum for SonderMind therapists. See all continuing education and training opportunities available to SonderMind providers here.
Join a community of mental health providers committed to changing the future of mental healthcare.
Join SonderMind
**Disclaimer: This document is intended for educational purposes only. Please check with your legal counsel or state licensing board for specific requirements.
SonderMind Inc.© 2022
On the side of life: a security plan //Psychological newspaper
In my practice, I meet clients with suicidal intentions and actions, and I know that in such cases, colleagues often enter into anti-suicidal contracts, which, in my opinion, are ineffective and are designed to protect the psychologist rather than the client. What are the alternatives? Why is the anti-suicidal contract bad, and when can it still be used? And what is a "safety plan"?
What are the alternatives? Why is the anti-suicidal contract bad, and when can it still be used? And what is a "safety plan"?
nine0005 Anti-Suicide Contract is a written agreement specifying that a person undertakes to preserve his life and not harm himself. Such contracts were first used by American psychiatrists in 1973 and came into general practice from transactional analysis.
It seems that the goal is clear - to protect the client from harm to his health and to transfer the responsibility to save his life. Why then do I say they are ineffective? nine0003
Imagine yourself in the place of the client: the psychologist heard that you were thinking about suicide and quickly asked you to sign a paper that you would not do anything to yourself. In whose interests does the psychologist act then? It looks like an attempt to save not the client, but yourself: from feelings of guilt, responsibility, undesirable consequences or a lawsuit. Especially if all actions are done formally: "Here is a piece of paper, sign it, you are free. "
"
How will you feel?
Most likely abandoned, abandoned, deceived. nine0003
The client must be treated as an equal. The task is to negotiate, not to force or suppress.
An anti-suicidal contract is appropriate if it is not a formality, but part of a therapeutic agreement between two people, based on trust. And trust must be earned.
Ask how the client feels? What are the reasons to live? How did he come up with the idea of suicide? How long is he willing to not commit suicide to give himself time to change? Come to an agreement together. nine0003
Asking to sign a contract without agreement and discussion is like asking a client to formulate a contract like “I promise to feel important this week.” Not very doable, you say?
More importantly, this contract should be not only (and even not so much) with the therapist, but with yourself. People often deceive others, but very rarely deceive themselves.
Another feature of the contract is that it does not prevent anything. You can't sign an anti-suicidal contract for 40 years, or 10, or even a year. The task of the contract is to delay suicidal actions and give a little time. nine0003
You can't sign an anti-suicidal contract for 40 years, or 10, or even a year. The task of the contract is to delay suicidal actions and give a little time. nine0003
In suicidal clients, opposite desires coexist at the same time: "I want to die" and "I do not want to die", they are both strong and fight with each other. If there was only one desire, then the person would either be dead after a short period of time, or would not have suicidal thoughts at all. At the same time, a struggle of life and death takes place in a person. As in the parable of the two wolves: “And which wolf wins in the end?” "The one you feed." The task of the therapist is to give the “white” wolf strength and a little time to get stronger. nine0003
Therefore, the meaning and necessity of the anti-suicidal contract lies in two things:
1) buy time if suicidal intentions appear;
2) buy time to establish a therapeutic relationship.
As an alternative to suicide contracts, I suggest using security plans.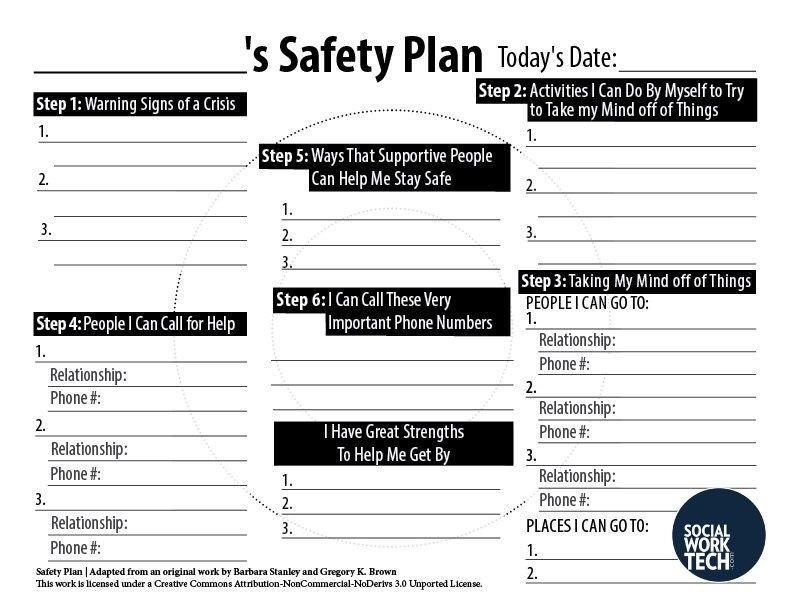
Safety Plan is a series of steps to follow until you feel safe. nine0003
The anti-suicide contract focuses on what the client should NOT do. A safety plan is about the things you should do to help yourself.
It is compiled together with the client, right at the session. The plan is made while the client feels well and can think clearly, do not wait for suicidal thoughts to turn into action.
The safety plan is written in such a way that it does not need to be memorized and memorized, all steps are designed to give the client hope that other people will take care of him, give specific alternative actions that can be taken instead of hurting yourself. nine0003
Its tasks are much broader than those of the anti-suicide contract, and include:
- specific signs that mean that a person can move from thoughts to suicidal actions;
- reasons for which it is worth living;
- a list of people to contact in such a case;
- steps you can take to cope and/or distract yourself when you feel hopeless or insecure; nine0049
- contacts of hotlines, crisis centers and specialists.
Put it in writing and let the client keep it where he can easily get it in case of need.
Even before the end of the session, ask the client to share this plan with another person, one of the people to whom the client can turn in case of need to prevent a suicide attempt.
Cognitive Behavioral Psychologists A. Wenzel and S. Jaeger-Hiemen offer the following plan steps:
1. Specify when the plan should be used.
When you experience any situations, images, thoughts, feelings or behaviors, you have suicidal urges. List them. For example: “If I stop taking care of my health and isolate myself, this is a wake-up call for me.”
2. What are your reasons for living?
As Frankl wrote in his book Saying Yes to Life: “If a person has a why, he can bear any how. When you're feeling down, it's easy to get caught up in pain and forget the positives in your life.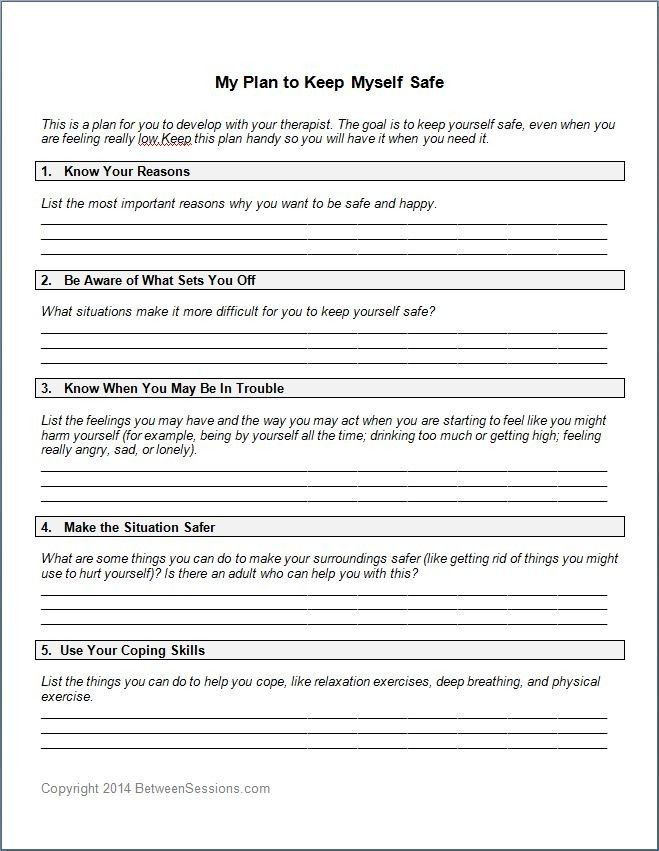 This list will help you redirect your attention to the reasons why it is worth living until your suicidal thoughts go away. For example: your parents, travel, children, work, your pet.
This list will help you redirect your attention to the reasons why it is worth living until your suicidal thoughts go away. For example: your parents, travel, children, work, your pet.
3. What can be done to calm down?
What usually calms you personally when you are upset? For example: taking a hot bath, listening to music, exercising, walking, meditating. Create an action list for yourself or use existing practices (breathing exercises or phone apps to deal with stress, such as Headspace, Whats up, etc.).
4. Who can you talk to?
Create a list of contacts you can talk to if self-help measures aren't working. List names, phone numbers, social media links, and other contact information. nine0003
5. Which professional can you talk to?
Contacts of hotlines, crisis centers, helplines, psychologist and psychiatrist. Save phone numbers, addresses and other contact information. Be sure to agree with your psychologist what method of communication you use when a critical situation arises. For example, it is not always possible to answer a phone call, but it is much easier to answer a written message in a messenger. nine0003
Be sure to agree with your psychologist what method of communication you use when a critical situation arises. For example, it is not always possible to answer a phone call, but it is much easier to answer a written message in a messenger. nine0003
6. How can you make your environment secure?
For example, remove from the house (or secure) all objects with which you can harm yourself. Or, in the event of an attack, leave the house until the urge passes. Example: "When I feel like hurting myself, I go to a public place like the mall, restaurant or library to distract myself."
7. What else can you do if you still don't feel safe? nine0006
If all else fails, go to the nearest emergency room and ask for help. Make a list of the nearest hospitals, their addresses and phone numbers in advance. If you don't feel you can safely get to the hospital on your own, call 911 and ask to be taken to the hospital.
And remember: there is no shame in asking for help. As well as taking care of yourself in different ways.
As well as taking care of yourself in different ways.
38. Evaluation of drug safety. Therapeutic index and standard safety margins. nine0001
Rating security is carried out on two levels:
a) preclinical (obtaining information about drug toxicity, effects on reproductive functions, embryotoxicity and teratogenicity, long-term effects)
b) clinical (further assessment efficacy and safety of drugs)
If after reaching a plateau effect, the dose of drugs will continue to increase, then after a certain period of time its toxic effects will start to show action. addiction toxic action on the dose (concentration) of the drug is the same character as its useful effect and can be described by a gradient or quantum curves. On these curves value can also be determined nine0124 TD 50 or TS 50 - toxic dose (concentration) of drugs, which causes a toxic effect, equal to 50% of the maximum (for quantum curve - toxic effect in 50% of persons in populations). Sometimes, instead of TD 50 use indicator LD 50 - lethal dose , which causes the death of 50% of objects in populations.
Sometimes, instead of TD 50 use indicator LD 50 - lethal dose , which causes the death of 50% of objects in populations.
Grade drug safety is characterized by based on grade or quantum curves "dose-effect" and the following indicators:
a) therapeutic index is ratio between toxic and effective doses of drugs that cause the appearance of a half-maximal effect: TI=TD 50 /ED 50 . The greater the therapeutic value index, the more secure is medicine.
b) therapeutic latitude (therapeutic window) is the dose range between the minimum therapeutic and minimal toxic doses of drugs. Is more correct indicator of drug safety, because allows you to take into account the degree of growth unwanted effects on the curve "dose-effect". nine0003
c) reliable factor security – is the ratio of the minimum toxic doses to the maximum effective (FNB=TD 1 /ED 99 ), shows how many times the therapeutic dose of the drug was exceeded without the risk of developing intoxication (unwanted effects).
d) therapeutic corridor is effective concentration range drug substance in the blood needs to be created and maintained body in order to achieve desired therapeutic effect. nine0003
39. Pharmacokinetic interaction of drugs
Interaction LS is a change the severity and nature of the effects simultaneous or prior the use of several drugs.
a) pharmacokinetic
1) At the stage of absorption.
introduction per os interaction determine:
1. medium acidity
2. direct interaction in the gastrointestinal tract
Tetracyclines interact with calcium, aluminum, iron, magnesium with the formation of chelate complexes. Cholestyramine breaks absorption of acid derivatives, drugs calcium, varvarin, digoxin, digitoxin, fat-soluble vitamins, trimethoprim, clindamycin, cephalexin, tetracycline. Iron supplements are better absorbed from vitamin C. Iron preparations with carbonates, tetracyclines are absorbed.