Social pragmatic language disorder
Social Pragmatic Communication Disorder: Symptoms, Treatments & More
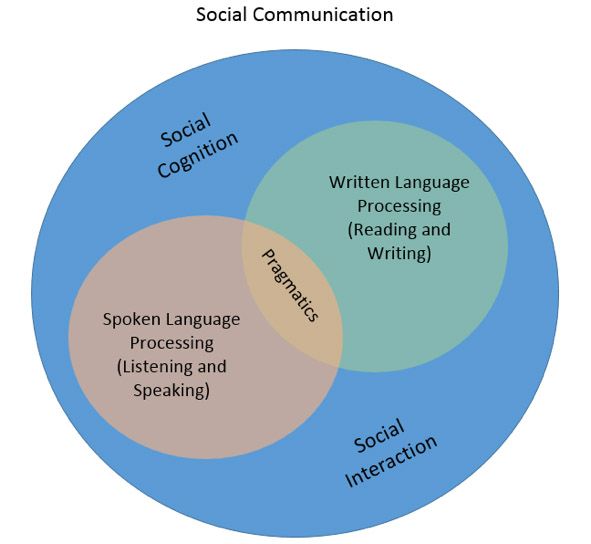
Social pragmatic communication disorder (SPCD) refers to marked challenges with both nonverbal and verbal communication skills used in social settings.
Social-communication difficulties may be associated with other communication disorders. However, as of 2013, SPCD is now considered its own category as defined by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5).
SPCD is also considered separate from certain neurodevelopmental disorders that may also affect communication skills, including autism spectrum disorder (ASD).
Read on to learn more about SPCD, including symptoms, treatment, and how it differs from — or relates to — other conditions that may affect communication skills.
Newly added to the DSM-5’s Communication Disorders section, SPCD refers to a “primary deficit” in both verbal and nonverbal communication used in social situations.
Such difficulties may include:
- inappropriate communication in certain social contexts
- difficulties with using language to socialize
- not knowing how to use and understand both verbal and nonverbal cues
- a lack of understanding regarding nonliteral language
SPCD symptoms may vary in type and intensity between individuals. Below are just some of the signs of SPCD:
- difficulties with adapting communication skills to different social contexts, such as greetings and initiating conversation
- inability to switch between formal and informal language
- problems with taking turns during conversations
- difficulties with using nonverbal communication techniques during social interactions, such as eye contact and hand gestures
- difficulty understanding nonliteral language, such as inferences, sarcasm, metaphors, and idioms made during conversation
- making and/or keeping friends
Having one or more of these symptoms doesn’t automatically mean you have SPCD. To be diagnosed with this communication disorder, the DSM-5 notes that the symptoms must significantly interfere with:
- interpersonal relationships
- your ability to socialize
- work
- school
As of the DSM-5, SPCD is considered a separate condition from ASD.
Some of the symptoms of SPCD may seem to overlap with those associated with ASD, including what is formerly known as Asperger’s. One 2017 study also concluded that SPCD may not seem completely different from ASD, but may include common traits.
One 2017 study also concluded that SPCD may not seem completely different from ASD, but may include common traits.
However, the DSM-5 has placed SPCD in its own category as those that are not caused by any other underlying developmental disorder or medical condition.
Communication difficulties that may be noted in ASD include:
- seeming “lack of attention” in social interactions
- difficulty engaging with back and forth conversations
- talking with others without giving them a chance to respond
SPCD may sometimes be diagnosed with attention-deficit hyperactivity disorder (ADHD). While ADHD may lead to some communication difficulties, the causes and impacts aren’t the same as SPCD.
Communication difficulties that may be seen in ADHD include:
- excessive talking
- inability to concentrate on someone talking with you
- interfering with others’ conversations
- interrupting others who may be talking with you
- having trouble waiting for your turn to talk
While the exact cause is unknown, some researchers believe that SPCD may have a genetic component. It may also run in families who have a history of pragmatic language difficulties.
It may also run in families who have a history of pragmatic language difficulties.
Some of the signs of SPCD may overlap with neurodevelopmental disorders. These include ASD and ADHD.
Prior to the separate classification by DSM-5, SPCD was thought to coexist with ADHD and other genetic or neurological conditions.
However, the DSM-5 considers SPCD its own disorder. This means that it’s not caused by ASD, ADHD, or any other neurodevelopmental condition.
Children must have time to sufficiently develop their language skills before SPCD can be detected. Therefore, a diagnosis of SPCD shouldn’t be made until they are at least 4 to 5 years old.
Because the exact causes of SCPD are unknown, there aren’t any known preventive measures. However, early screening is key to start treatments and provide better outcomes in interpersonal relationships, work, and school.
Other researchers have raised concerns about an SPCD diagnosis versus one of a neurodevelopmental disorder for fear that those affected may not receive the services they need — both at school and in clinical settings.
SPCD may run in families. Other risk factors may include underlying:
- ADHD
- intellectual or developmental disabilities
- other language disorders
- learning disabilities
- hearing loss
- traumatic brain injuries
- dementia
Finding help for social pragmatic communication disorder
If you or a loved one needs help with social pragmatic communication disorder, there are a number of professionals who can help you get started, including your:
- primary care doctor or pediatrician
- teacher
- daycare center
- local health department
Depending on insurance requirements, you may also contact a private speech therapist’s office directly for an assessment and evaluation.
Treatment for SCPD focuses on speech therapy given by a speech-language pathologist (SLP). SLP services are available for children in schools who qualify, and you may also obtain speech therapy in private practices.
While individual, one-on-one sessions are essential, group therapy can also help improve social pragmatic skills. Group therapies are also used in school settings. Some private practices may also offer group social skills classes.
Before you can begin treatment for SPCD, you must be screened and assessed by professionals, such as SLPs. These assessments may be provided in school, private practices, or both.
They will use a combination of:
- interviews (with yourself or parents, depending on your age)
- questionnaires
- self-assessments
- reports from teachers or caregivers
- hearing tests
With early detection and treatment, the outlook for SPCD is positive. You may expect to attend speech therapy and/or social skills classes over the long-term for best results. Teenagers and adults may benefit from life skills groups.
SPCD itself may be lifelong, with some symptoms improving over time. It’s important to monitor progress to also prevent any regressions. With early therapy, however, social-communication skills may be improved, thus decreasing the need for intervention.
With early therapy, however, social-communication skills may be improved, thus decreasing the need for intervention.
SPCD is a type of communication disorder that may adversely affect social interactions. While many of its symptoms can overlap neurodevelopmental disorders such as ADHD, the DSM-5 considers SPCD its own condition. It’s also considered as a separate disorder from ASD.
While it’s important to detect SPCD for early intervention, you shouldn’t self-diagnose this condition. If you suspect you or a loved one is having trouble with social communication, talk with a doctor for help with the next steps.
Social Pragmatic Communication Disorder: Symptoms, Treatments & More
Social pragmatic communication disorder (SPCD) refers to marked challenges with both nonverbal and verbal communication skills used in social settings.
Social-communication difficulties may be associated with other communication disorders. However, as of 2013, SPCD is now considered its own category as defined by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5).
SPCD is also considered separate from certain neurodevelopmental disorders that may also affect communication skills, including autism spectrum disorder (ASD).
Read on to learn more about SPCD, including symptoms, treatment, and how it differs from — or relates to — other conditions that may affect communication skills.
Newly added to the DSM-5’s Communication Disorders section, SPCD refers to a “primary deficit” in both verbal and nonverbal communication used in social situations.
Such difficulties may include:
- inappropriate communication in certain social contexts
- difficulties with using language to socialize
- not knowing how to use and understand both verbal and nonverbal cues
- a lack of understanding regarding nonliteral language
SPCD symptoms may vary in type and intensity between individuals. Below are just some of the signs of SPCD:
- difficulties with adapting communication skills to different social contexts, such as greetings and initiating conversation
- inability to switch between formal and informal language
- problems with taking turns during conversations
- difficulties with using nonverbal communication techniques during social interactions, such as eye contact and hand gestures
- difficulty understanding nonliteral language, such as inferences, sarcasm, metaphors, and idioms made during conversation
- making and/or keeping friends
Having one or more of these symptoms doesn’t automatically mean you have SPCD. To be diagnosed with this communication disorder, the DSM-5 notes that the symptoms must significantly interfere with:
To be diagnosed with this communication disorder, the DSM-5 notes that the symptoms must significantly interfere with:
- interpersonal relationships
- your ability to socialize
- work
- school
As of the DSM-5, SPCD is considered a separate condition from ASD.
Some of the symptoms of SPCD may seem to overlap with those associated with ASD, including what is formerly known as Asperger’s. One 2017 study also concluded that SPCD may not seem completely different from ASD, but may include common traits.
However, the DSM-5 has placed SPCD in its own category as those that are not caused by any other underlying developmental disorder or medical condition.
Communication difficulties that may be noted in ASD include:
- seeming “lack of attention” in social interactions
- difficulty engaging with back and forth conversations
- talking with others without giving them a chance to respond
SPCD may sometimes be diagnosed with attention-deficit hyperactivity disorder (ADHD). While ADHD may lead to some communication difficulties, the causes and impacts aren’t the same as SPCD.
While ADHD may lead to some communication difficulties, the causes and impacts aren’t the same as SPCD.
Communication difficulties that may be seen in ADHD include:
- excessive talking
- inability to concentrate on someone talking with you
- interfering with others’ conversations
- interrupting others who may be talking with you
- having trouble waiting for your turn to talk
While the exact cause is unknown, some researchers believe that SPCD may have a genetic component. It may also run in families who have a history of pragmatic language difficulties.
Some of the signs of SPCD may overlap with neurodevelopmental disorders. These include ASD and ADHD.
Prior to the separate classification by DSM-5, SPCD was thought to coexist with ADHD and other genetic or neurological conditions.
However, the DSM-5 considers SPCD its own disorder. This means that it’s not caused by ASD, ADHD, or any other neurodevelopmental condition.
Children must have time to sufficiently develop their language skills before SPCD can be detected. Therefore, a diagnosis of SPCD shouldn’t be made until they are at least 4 to 5 years old.
Because the exact causes of SCPD are unknown, there aren’t any known preventive measures. However, early screening is key to start treatments and provide better outcomes in interpersonal relationships, work, and school.
Other researchers have raised concerns about an SPCD diagnosis versus one of a neurodevelopmental disorder for fear that those affected may not receive the services they need — both at school and in clinical settings.
SPCD may run in families. Other risk factors may include underlying:
- ADHD
- intellectual or developmental disabilities
- other language disorders
- learning disabilities
- hearing loss
- traumatic brain injuries
- dementia
Finding help for social pragmatic communication disorder
If you or a loved one needs help with social pragmatic communication disorder, there are a number of professionals who can help you get started, including your:
- primary care doctor or pediatrician
- teacher
- daycare center
- local health department
Depending on insurance requirements, you may also contact a private speech therapist’s office directly for an assessment and evaluation.
Treatment for SCPD focuses on speech therapy given by a speech-language pathologist (SLP). SLP services are available for children in schools who qualify, and you may also obtain speech therapy in private practices.
While individual, one-on-one sessions are essential, group therapy can also help improve social pragmatic skills. Group therapies are also used in school settings. Some private practices may also offer group social skills classes.
Before you can begin treatment for SPCD, you must be screened and assessed by professionals, such as SLPs. These assessments may be provided in school, private practices, or both.
They will use a combination of:
- interviews (with yourself or parents, depending on your age)
- questionnaires
- self-assessments
- reports from teachers or caregivers
- hearing tests
With early detection and treatment, the outlook for SPCD is positive. You may expect to attend speech therapy and/or social skills classes over the long-term for best results. Teenagers and adults may benefit from life skills groups.
Teenagers and adults may benefit from life skills groups.
SPCD itself may be lifelong, with some symptoms improving over time. It’s important to monitor progress to also prevent any regressions. With early therapy, however, social-communication skills may be improved, thus decreasing the need for intervention.
SPCD is a type of communication disorder that may adversely affect social interactions. While many of its symptoms can overlap neurodevelopmental disorders such as ADHD, the DSM-5 considers SPCD its own condition. It’s also considered as a separate disorder from ASD.
While it’s important to detect SPCD for early intervention, you shouldn’t self-diagnose this condition. If you suspect you or a loved one is having trouble with social communication, talk with a doctor for help with the next steps.
Social (pragmatic) communication impairment vs. autism: differences and similarities | mental health articles | Emotional & Mental Health center
The symptoms of social (pragmatic) communication disorder will look deceptively familiar to anyone who knows anything about autism - but it's a whole diagnosis.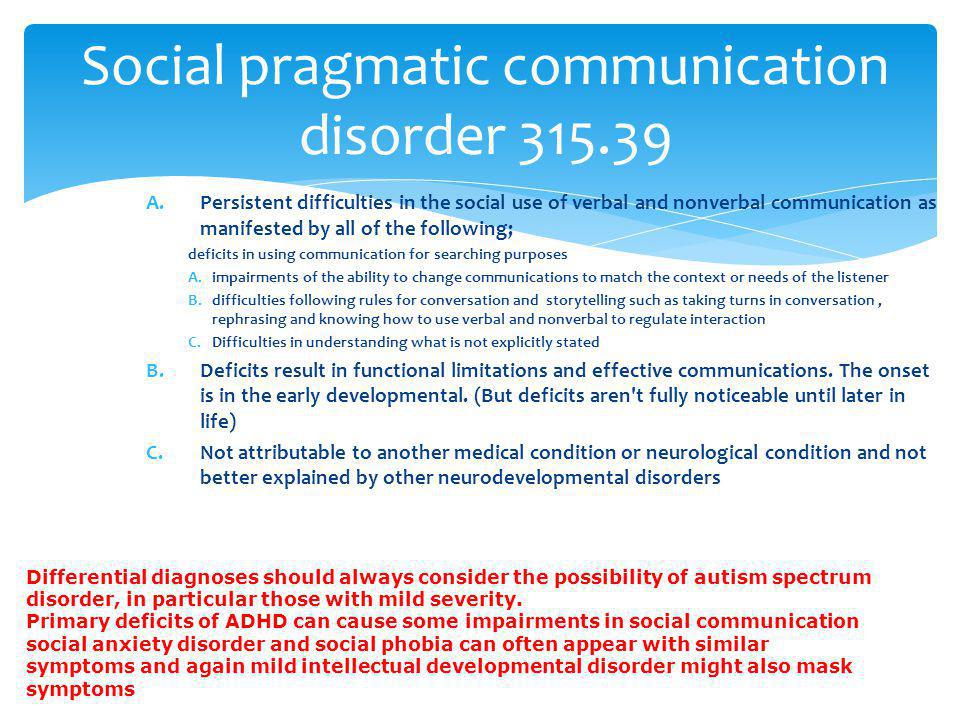
Let's play "guess the diagnosis" game:
- Reduced ability to communicate with other people in a way that most people would consider appropriate to the context. nine0008
- The problem with "code switching", i.e. the inability to change the use of the language according to the situation and, for example, to refer to an authority figure you first met, as well as to a close friend,
- Difficulty understanding and following unspoken rules of communication, such as waiting in line or paraphrasing something that the interlocutor did not understand.
- Find it difficult to "read between the lines" - for example, to understand metaphors, implied meanings and puns. nine0008
Anyone familiar with autism spectrum disorders would probably immediately point their proverbial finger at it, but wonder why this list is incomplete. I'm right? Persistent difficulties in social communication and interaction are, after all, one of the defining characteristics of autism.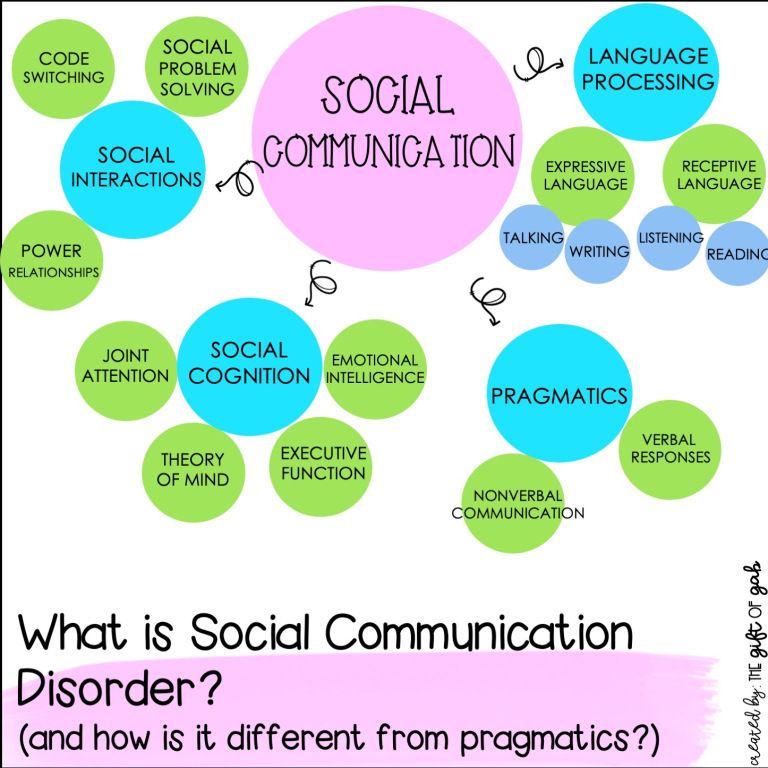
However, this particular set of diagnostic criteria is almost complete, and the only thing we still need to add is that in order for a person to receive this diagnosis, the symptoms must limit the person's life in social, educational and professional areas, they must show in childhood, and that another disorder cannot better explain them. nine0003
We are not looking at autism spectrum disorder but rather social (pragmatic) communication disorder, a diagnosis that was first introduced in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders published in 2013.
What are the differences between social (pragmatic) communication disorder and autism?
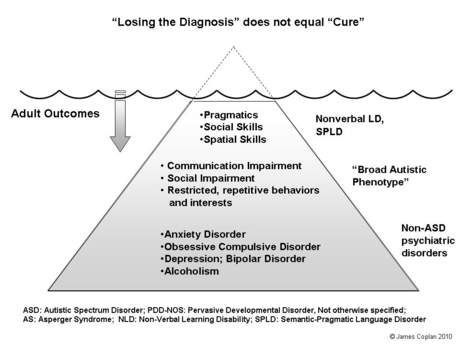
The similarities are clear - and prior to the advent of the DSM-5, many people now diagnosed with social (pragmatic) communication disorder were often diagnosed with pervasive developmental disorder, not otherwise specified, which was considered part of the autism umbrella. nine0003
Unlike social (pragmatic) communication disorder, autism spectrum disorder can be characterized by all of the following:
- Unusual non-verbal social behavior - such as problems making eye contact, comprehension or gestures, even tone of voice, display of objects, and facial expressions, which are unusual.
- Strong preference for and often need sameness and routine, and suffering when faced with even small changes. nine0008
- "Stereotypical" movements and behavior
- Strong and persistent addictions to certain subjects, often to the exclusion of most other things - commonly referred to as "autistic special interests".
- Certain sensory differences. An autistic person can easily become overwhelmed by stimuli such as small sounds, flashing lights, or large crowds, but they can also be less sensitive than most other stimuli. nine0008
Autism can be diagnosed with or without language and intellectual impairments, and the DSM-5 also divides it into several "levels" of severity, depending on the amount of support the autistic person needs to function optimally. Although some autistic people are nonverbal, people with social (pragmatic) communication disorder can speak but have problems with the social aspect of communication.
Together with persistent difficulties in social communication and interaction, stereotyped, repetitive and restrictive interests and behaviors constitute the main features of autism spectrum disorder. In other words, someone with social (pragmatic) communication disorder will show some of the symptoms seen in people with autism, but not all. Rather, their difficulties are limited to the area of social communication. nine0003
In other words, someone with social (pragmatic) communication disorder will show some of the symptoms seen in people with autism, but not all. Rather, their difficulties are limited to the area of social communication. nine0003
Interestingly, autism and social (pragmatic) communication disorder appear to be members of the same extended diagnostic family, with people with a family history of autism being more likely to be diagnosed with this diagnosis. Since SCD is a relatively newly introduced label, research should fill in some of the questions that are currently still "out there" in the future.
How is social (pragmatic) communication diagnosed? nine0023
Parents, grandparents, teachers, family friends, pediatricians, family physicians, and others in the life of a child with symptoms of social (pragmatic) communication disorder are likely to initially suspect that the child is on the autism spectrum. A diagnosis of SCD can only be made after careful evaluation shows that the patterns of repetitive and restricted behavior and interests so characteristic of autism are not present.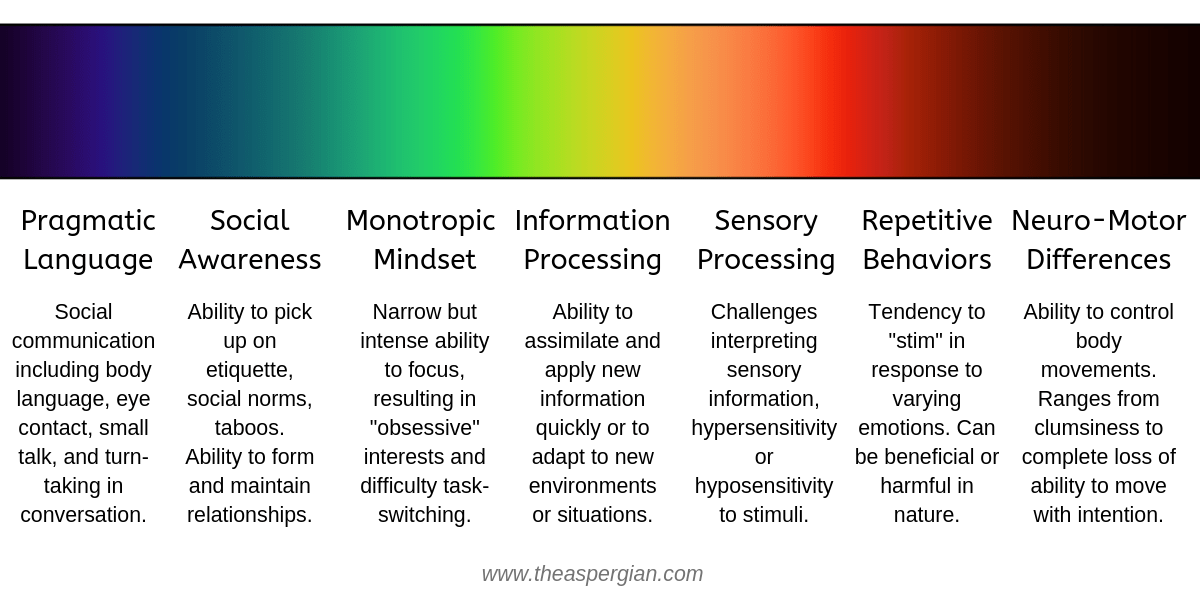
Clinicians will also have to rule out other disorders that may have similar symptoms, such as ADHD, social anxiety, and mental retardation. If another disorder better explains the symptoms seen in a particular person, a diagnosis will be made instead. nine0003
The most important thing parents can do is talk to their child's primary care doctor about the problems they have and the symptoms they notice. If they already suspect that social (pragmatic) communication disorder may be at play because their child doesn't have some of the defining signs of autism, they can certainly report it.
Social (pragmatic) communication disorder: still a bit of a mystery?
Since social (pragmatic) communication disorder has been established as a separate diagnosis relatively recently, little is known about the long-term prognosis or the best ways to help affected people make progress in their communication abilities. All of this should change in the future as the disorder is explored further. At the same time, people diagnosed with the disorder can benefit from the same therapeutic approaches that can help autistic people. nine0003
At the same time, people diagnosed with the disorder can benefit from the same therapeutic approaches that can help autistic people. nine0003
Communication disorder, portal of doctors of the Chelyabinsk region and the city of Chelyabinsk
Communication disorder - any mental disorder, including problems in speech, language and communication. Speech - Expressive reproduction of sounds, includes fluency, articulation, voice and resonant quality. Communication includes any non-verbal or verbal behavior (whether intentional or unintentional) that influences the ideas, behavior or attitudes of another individual. nine0063 The language includes the function, form, and use of the conventional symbol system (ie spoken words, written words, sign language).
Contents
- 1 General definition
- 2 Diagnostics
- 3 See also
- 4 Notes
- 5 Literature
General definition
The types of disorders that are included and excluded from the category of communication disorder may vary depending on the source.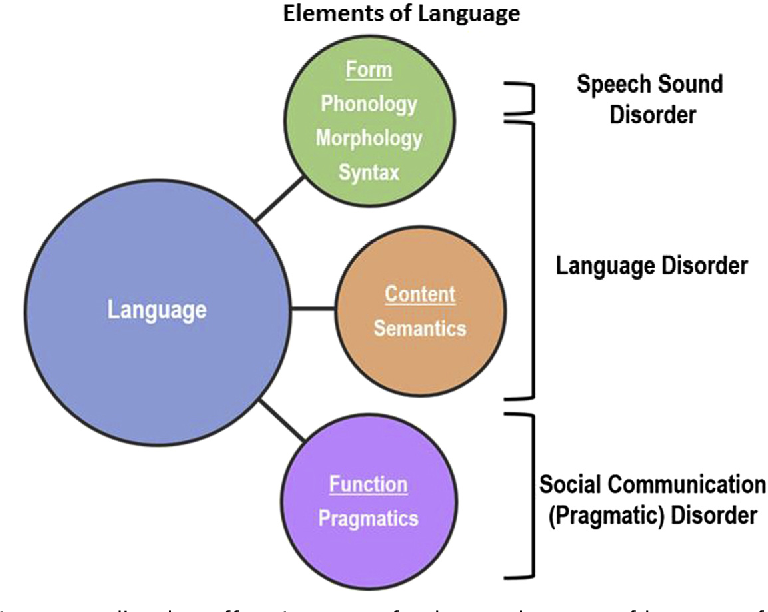 For example, definitions offered by The American Speech-Language-Hearing Association (ASHA) differ from those provided by the Diagnostic and Statistical Manual of Mental Disorders. nine0003
For example, definitions offered by The American Speech-Language-Hearing Association (ASHA) differ from those provided by the Diagnostic and Statistical Manual of Mental Disorders. nine0003
Jean Berko Gleason (2001) defines a communication disorder as a language and speech impairment that causes problems in communication and related areas, such as speech motor function. A deeply rooted auditory distortion can even lead to a loss of desire to listen, which in turn reduces the desire to communicate. Basically, the term communication disorder is used in relation to speech disorders (speech, language or communication) that significantly impede the development of the individual and negatively affect the quality of life. In some communication disorders, a person cannot or can only partially use their own voice as the main communication tool. This is due to the fact that he does not control the various melodic components of the voice - intonation, expressiveness, rhythm, strength, etc. - therefore, the interlocutor perceives his voice as rough, emotionless, devoid of expressiveness.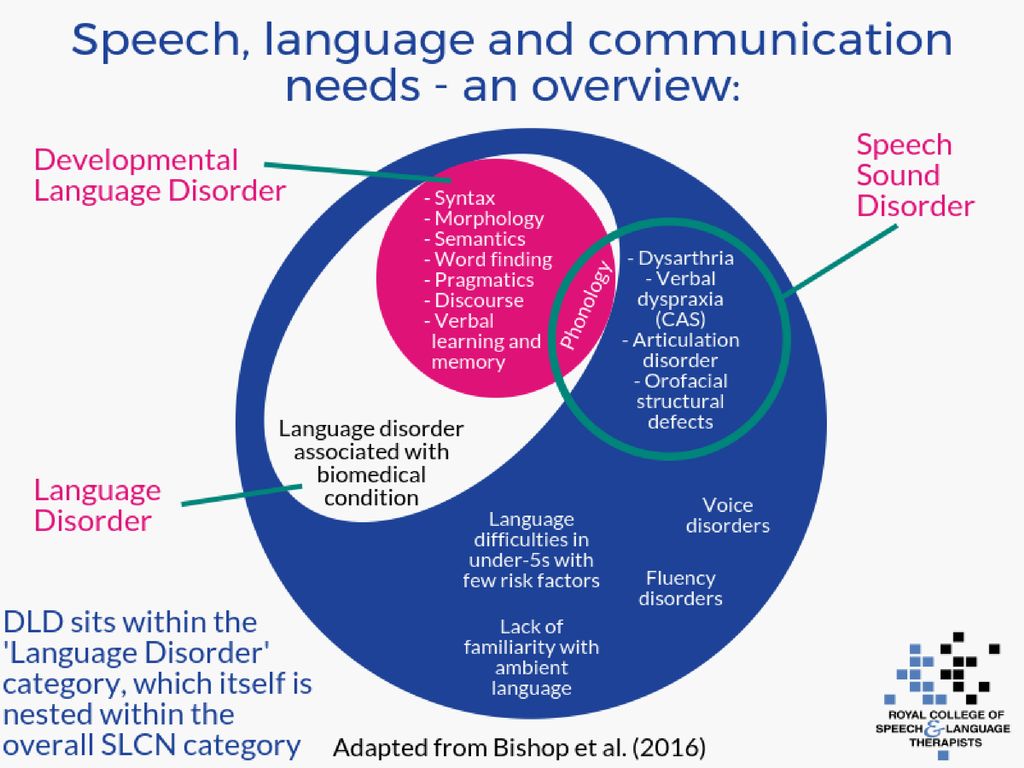 nine0003
nine0003
A person who speaks two or more languages or with a different accent does not have speech disorders if he speaks in a manner appropriate to his usual place of residence or combines his native and foreign languages.
Diagnostics
Communication disorder is most often first diagnosed in childhood or adolescence, although it is not considered exclusively a childhood disorder and may persist into adulthood. Also, this type of disorder may be accompanied by other disorders, such as mental retardation and unwillingness to communicate with others. Diagnosis in the United States involves taking a special DSM test and transcribing its results, which determine if the level is "significantly below" the expected development and whether they significantly interfere with social interaction and mental development. This test can also reveal if development is "deviant" (deviating from the accepted norm) or belated. However, there is a possibility that the individual has problems with social communication, but does not fall into the category of a low level of speech development according to the DSM criteria. nine0003
nine0003
The DSM-IV and DSM-IV-TR definitions of communication disorder included the following diagnoses:
- Stuttering (307.0) is a speech disorder characterized by frequent repetition or prolongation of sounds or syllables or words; or frequent stops or hesitation in speech, breaking its rhythmic flow.
- Expressive speech disorder (315.31) is a disorder characterized by the ability to speak only in simple sentences and constructions, a limited vocabulary. With this violation, the individual understands the language better than he can express himself in it. nine0008
- Mixed expressive-receptive language disorder (315.32) - problems with the perception of what the interlocutor is trying to convey to the individual.
- Phonological disorder (315.39), which is expressed in the form of constant substitutions and mixing of sounds.
- Unspecified communication disorder (307.9)
The Communication Disorders section of the DSM-5 has been significantly revised. Communication disorders in this classification include: nine0003
Communication disorders in this classification include: nine0003
- 315.39 (F80.9) - language disorder (English language disorder) - difficulties in acquiring and using language in different forms (for example, spoken, written, sign language or others), vocabulary is extremely small, sentence structure is limited.
- 315.39 (F80.0) speech sound disorder difficulty in producing speech sounds, unintelligibility of speech which interferes with verbal communication.
- 315.35 (F80.81) Childhood-onset fluency disorder (stuttering). nine0008
- 315.39 (F80.89) social (pragmatic) communication disorder - difficulties in the social use of verbal and non-verbal communication, manifested in the use of communication for social purposes, such as greeting and exchanging information, and also impaired ability to change communication according to the context or needs of the listener, such as speaking differently in class than on the playground, etc. nine0007 307.9 (F80.
 9) unspecified communication disorder
9) unspecified communication disorder In the International Classification of Diseases 10th Revision (ICD-10), section F80 - "specific developmental disorders of speech and language" includes:
- F80.0 - specific disorder of speech articulation.
- F80.1 Expressive speech disorder.
- F80.2 Receptive speech disorder.
- F80.3 - acquired aphasia with epilepsy (Landau-Kleffner syndrome). nine0008
- F80.8 - other developmental disorders of speech and language.
- F80.9 Speech and language development disorders, unspecified.
Alalia (the accepted division of alalia into motor and sensory in ICD-10 corresponds to disorders of expressive F80.1 and receptive speech F80.2) - complete or partial absence of speech in children with good physical hearing, due to underdevelopment or damage to the speech areas of the brain. With sensory alalia, the child does not understand someone else's speech well, moreover, he does not recognize exactly the sounds of speech: he hears what the person is saying, but does not understand what exactly.