Screening for eating disorders
Learn about the Different Screening Options for Detecting Eating Disorders
Screening for eating disorders can help a person get the right diagnosis and treatment. Learn about the different screening options for detecting eating disorders.
With so many different health trends and dietary requirements, it can be hard to tell what is healthy and what may signal a more serious problem. It’s not always easy to spot an eating disorder since they’re not always associated with low weight and certain behaviors can seem like a normal part of dieting.
Eating disorder screening tools and questionnaires can help identify signs and symptoms that indicate a person has an eating disorder. Tools that screen for eating disorders can help identify a person who is struggling and allow them to get appropriate treatment.
The SCOFF Questionnaire
The SCOFF questionnaire is a short and easy-to-use tool for assessing the presence of anorexia and bulimia. The questionnaire includes five questions related to self-control, weight loss, body image and the role of food in a person’s life.
The questions included in the SCOFF questionnaire are scored one for “yes” answers and zero points are given for answering “no” to a question. A cut-off point of two points or greater out of five suggests an eating disorder. The SCOFF Questionnaire is helpful for identifying potential cases of eating disorders, but shouldn’t be used on its own to formally diagnose a condition.
Eating Disorder Screening for Primary Care
Eating disorder screening for primary care (ESP) is a set of five questions taken from other questionnaires. It is a quick-and-easy tool that doctors can use in their general practice to get a sense of whether an eating disorder may be present.
The ESP asks about eating behaviors and the patient’s family and personal history of eating disorders. While this tool can be a helpful first step, it should be followed up by a full psychological test if an eating disorder is suspected. If an eating disorder seems likely after completing an ESP, a doctor will often refer a patient onwards to a psychiatrist for more complete testing and diagnosis.
Eating Attitudes Test
The Eating Attitudes Test (EAT-26) is a 26-question screening tool that asks questions that fall into three general categories. These categories include distorted body image, body weight, bulimic behavior and self-control. This questionnaire allows for a complete picture of symptoms and behaviors.
A score of 11 is considered to suggest the presence of an eating disorder.
Questionnaire for Eating Disorder Diagnosis
The Questionnaire for Eating Disorder Diagnosis (Q-EDD) was designed to capture the diagnostic criteria for eating disorders included in the Diagnostic and Statistical Manual of Mental Disorders (DSM), 4th edition.
Initial testing of this questionnaire showed that it is a reliable test, and compares well against a diagnostic interview by a clinician. However, since the update to the DSM-5 in 2013, the questionnaire does not necessarily reflect the most current diagnostic criteria.
For example, the DSM-5 includes revised new eating disorders like binge eating disorder or eating disorder not otherwise specified (EDNOS). Using the Q-EDD for eating disorder screening may fail to capture all of the currently recognized eating disorders, so it’s best to use a questionnaire that reflects the recent diagnostic changes.
Using the Q-EDD for eating disorder screening may fail to capture all of the currently recognized eating disorders, so it’s best to use a questionnaire that reflects the recent diagnostic changes.
Eating Disorder Examination
The Eating Disorder Examination (EDE) is a diagnostic interview that reflects the current DSM-5 diagnostic criteria for eating disorders. It is also available in The Eating Disorder Examination Questionnaire (EDE-Q). Both are considered gold-standard screening tools.
The examination and questionnaires are delivered slightly differently. The EDE is delivered by a clinician, like a psychiatrist, in an interview. The EDE-Q can be completed by a patient on their own, but having a clinician nearby to explain concepts or answer questions can be helpful.
Both the interview and questionnaire include four subscales or categories related to symptoms of eating disorders. These categories include restraint, eating concern, shape concern and weight concern. This screening tool also asks questions about eating disorder behaviors, like using laxatives, how often binge eating occurs or whether a patient exercises excessively. This information can help clinicians provide a more specific and accurate diagnosis.
This screening tool also asks questions about eating disorder behaviors, like using laxatives, how often binge eating occurs or whether a patient exercises excessively. This information can help clinicians provide a more specific and accurate diagnosis.
The EDE and EDE-Q are the best options for eating disorder screenings.
The Importance of Screening for Eating Disorders
Screening for eating disorders can help tell the difference between healthy behavior and a serious disorder that requires treatment.
Importantly, screening for eating disorders can help make sure a patient gets the right diagnosis. Getting the correct diagnosis is important for determining the best treatment and can improve a patient’s chances of recovery.
People who are worried about their eating behaviors or think they may have an eating disorder can complete a simple questionnaire. A questionnaire is a helpful first step in assessing whether or not your symptoms might suggest an eating disorder. However, it’s important to receive a full assessment from a trained professional. A formal diagnosis usually requires a combination of physical assessment and a psychological interview.
However, it’s important to receive a full assessment from a trained professional. A formal diagnosis usually requires a combination of physical assessment and a psychological interview.
Screening for eating disorders is an important first step in identifying a problem and asking for help. If you are struggling with an eating disorder related to a substance use disorder, The Recovery Village can help. Reach out today to take the first step toward a healthier future.
Editor – Thomas Christiansen
With over a decade of content experience, Tom produces and edits research articles, news and blog posts produced for Advanced Recovery Systems. Read more
Medically Reviewed By – Dr. Sarah Dash, PHD
Dr. Sarah Dash is a postdoctoral research fellow based in Toronto. Sarah completed her PhD in Nutritional Psychiatry at the Food and Mood Centre at Deakin University in 2017. Read more
Siervo, M; et al. “Application of the SCOFF, Eating Attitud[…]eeking diet-therapy. ” Eating Weight Disord, 2005. Accessed September 23, 2019.
” Eating Weight Disord, 2005. Accessed September 23, 2019.
Orbitello, B. “The EAT-26 as screening instrument for c[…]tion unit attenders.” International Journal of Obesity, 2006. Accessed September 23, 2019.
Morgan, J F; et al. “The SCOFF questionnaire: a new screening[…]or eating disorders.” The Western Journal of Medicine, 2000. Accessed September 23, 2019.
Berg, Kelly C; et al. “Psychometric evaluation of the eating di[…]w of the literature.” The International Journal of Eating Disorders, 2012. Accessed September 24, 2019.
Cotton, Mary-Anne; et al. “Four simple questions can help screen for eating disorders.” Journal of General Internal Medicine, 2003. Accessed September 24, 2019.
Medical Disclaimer
The Recovery Village aims to improve the quality of life for people struggling with substance use or mental health disorder with fact-based content about the nature of behavioral health conditions, treatment options and their related outcomes. We publish material that is researched, cited, edited and reviewed by licensed medical professionals.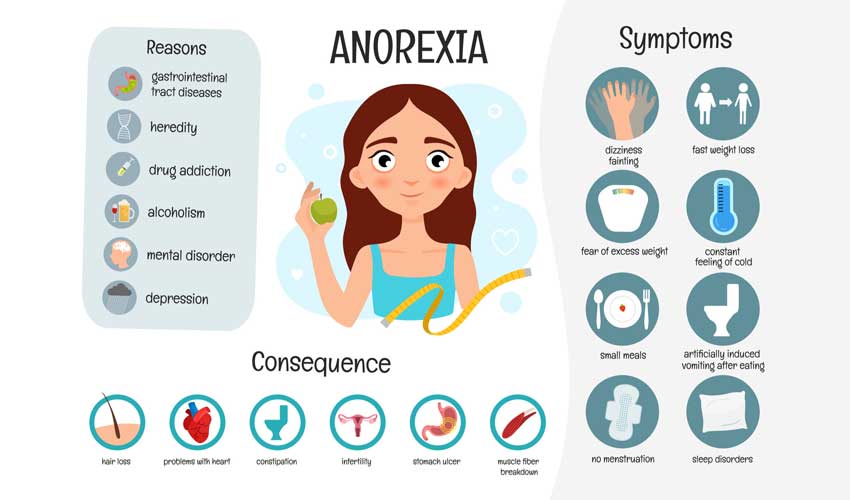 The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare providers.
The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare providers.
Eating Disorders: Screening & Assessment
CAMH logo- Eating Disorders
- Screening & Assessment
- Diagnosis
- Treatment
- Resources
Back to top
Text below adapted from The patient who has an eating disorder, Psychiatry in primary care, by David S. Goldbloom, (CAMH, 2019).
Goldbloom, (CAMH, 2019).
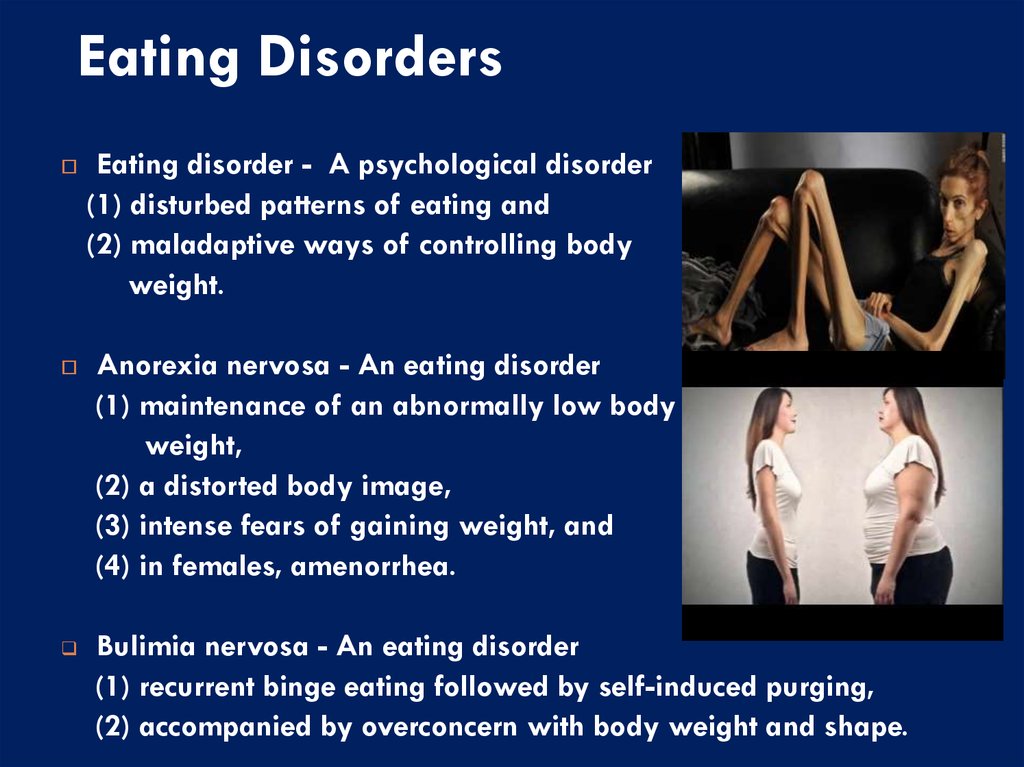
Symptoms
No other psychiatric disorder has as many physical signs and laboratory findings as the eating disorders. Obesity is not one of those signs because most people who are overweight do not have a formal eating disorder. It is more likely to be normal-weight or underweight women who present for help with an undiagnosed eating disorder. The chief complaint is rarely “I think I have an eating disorder”; rather, the patient may ask for help with:
- constipation, bloating or fluid retention
- weight loss, despite being at a normal weight
- mood instability, anxiety, sleep or concentration problems.
The following physical signs and laboratory findings are also common:
- marked weight loss
- bradycardia and hypotension
- amenorrhea or light, irregular periods
- impaired temperature regulation
- acrocyanosis
- delayed gastric emptying
- hair loss, dry skin and growth of lanugo hair
- hypokalemic, hypochloremic metabolic alkalosis
- elevated salivary amylase
- parotid hypertrophy
- anemia
- EKG findings of low voltage, T-wave inversion, prolonged QTc interval
- osteoporosis at a young age.

Screening and Assessment
The SCOFF is a brief five-question screening test for eating disorders, similar to the CAGE screen for alcohol dependence. The name of the questionnaire is somewhat controversial because the word “scoff” means to eat greedily. The SCOFF has been evaluated and compared with other measures in specialty clinics and in primary care in England and the United States. In the British version, the “O” represents “one stone” of weight and “sick” is understood to be “vomit.” The American version is provided below, using language more familiar to Canadians.
SCOFF Questionnaire
- Do you make yourself vomit (Sick) because you feel uncomfortably full?
- Do you worry that you have lost Control over how much you eat?
- Have you recently lost more than 15 pounds (One stone) in a 3-month period?
- Do you believe you are Fat when others say you are too thin?
- Would you say that Food dominates your life?
Give 1 point for every “yes. ” Scoring 2 or higher indicates a likely case of anorexia nervosa or bulimia.
” Scoring 2 or higher indicates a likely case of anorexia nervosa or bulimia.
Reproduced with permission from “The SCOFF questionnaire: Assessment of a new screening tool for eating disorders,” by J.F. Morgan et al., 1999, BMJ, 319, p. 1467. © 1999 BMJ Publishing Group.
In Eating Disorders:
- Introduction
- The Primary Care Practitioner Role
- Screening & Assessment
- Diagnosis
- Treatment
- Psychotherapy
- Pharmacotherapy
- Resources & References
Eating Disorders Home
Diagnosis
Dr. David Goldbloom, Senior Medical Advisor at CAMH, goes through a series of scenarios for primary care practitioners.
Active listening
Psychiatric interviewing scenarios for primary care practitioners
Read More
Asking items on a checklist
Psychiatric interviewing scenarios for primary care practitioners
Read More
Asking about substance use
Psychiatric interviewing scenarios for primary care practitioners
Read More
Asking about trauma/sexual abuse
Psychiatric interviewing scenarios for primary care practitioners
Read More
Talking about involving family members
Psychiatric interviewing scenarios for primary care practitioners
Read More
Referring a patient
Psychiatric interviewing scenarios for primary care practitioners
Read More
Normal eating behavior.
 Screening - Eating Disorders and Body Image
Screening - Eating Disorders and Body Image Normal eating behavior…
⠀
… screening…
⠀
On the paper, mark + or - in front of each of the 12 items, agreeing or disagreeing with each of them.
⠀1. You eat when you are hungry and are able to stop when you are full.
⠀
2. You stop eating because you think that “enough” and “time to stop”, and not because you are full.
⠀
3. You choose food that is delicious for you personally.
⠀
4. If you are on a diet or have not eaten enough, then you are physically ill (nausea, dizziness, weakness).
⠀
5. Your diet is a combination of healthy and tasty food.
⠀
6. You eat according to a certain pattern. For example, always 3 times a day or strictly at a certain moment of the day.
⠀
7. You believe that if you eat when you are hungry and stop when you are full, then you will not get better.
⠀
8. You feel guilty if you overeat.
⠀
9. You can balance thoughts about weight, food, nutrition with thoughts about other aspects of your life.
You can balance thoughts about weight, food, nutrition with thoughts about other aspects of your life.
⠀
10. In a cafe you watch what other people eat, then decide what you will eat.
⠀
11. You are able to leave a few cookies on your plate because you know that you can finish them tomorrow.
⠀
12. You choose food based on calories.
⠀
🔹 You can find out the transcript of the screening at the consultation
🔹 If you have 4-8 or 9-12 points, then URGENTLY WRITE me a direct to sign up for a free consultation. On it, I will help you find ways to solve your problem.
Book a consultation
Progressive Muscle Relaxation
Under stress, muscles tense up to run, attack, survive. For two weeks, most of us did not run or attack anywhere, but froze and sank
Read more»
Prolonged stress eating
If you cope with negative experiences through food, in the face of uncertainty, the symptoms may increase. sedative effect, it's okay to use it sometimes. Remember how
sedative effect, it's okay to use it sometimes. Remember how
Read more»
Before and after photo danger in eating disorder
A trigger in marketing is content that after interacting with which the consumer tends to behave and feel in a certain way. ⠀ BEFORE/AFTER photos are triggers, they are great
Read more»
Toxic shame in eating disorders
Shame is a social emotion. It is useful for its regulatory properties. It works when there is a possibility of being in a socially unacceptable situation. And if you are already in it
Read more»
The quality and duration of sleep is one of the factors of weight stability
The quality and duration of sleep is one of the factors of weight stability. ⠀ I propose to get acquainted with the essence of the first choice therapy in the treatment of insomnia (insomnia), comorbid with others
Read more»
Lose weight for health
What to do if the doctor suggested a diet to lose weight? ⠀ First, figure out how you gained weight and whether weight is really a threat to your
Read more»
Eating disorders in boys - symptoms and stereotypes
«If you were a girl, I would say that you suffer from anorexia». These words were told to 17-year-old Andy by a pediatrician who has been with him since birth. Andy did not eat snacks and sweets, but ate mostly huge amounts of grilled chicken breasts, vegetables and protein shakes, lifting weights and running for two hours a day. By the time he came to me for help in mid-March, he was very exhausted, his hair was falling out, and he barely had the strength to keep his head upright.
These words were told to 17-year-old Andy by a pediatrician who has been with him since birth. Andy did not eat snacks and sweets, but ate mostly huge amounts of grilled chicken breasts, vegetables and protein shakes, lifting weights and running for two hours a day. By the time he came to me for help in mid-March, he was very exhausted, his hair was falling out, and he barely had the strength to keep his head upright.
Andy's pediatrician suggested that he might be depressed and advised him to "walk more". Fortunately, Andy's worried mother, who suspected that her son was suffering from more than just depression, took him to a clinic for teens with eating disorders. I diagnosed Andy with anorexia nervosa. As it turned out, his depressed mood was secondary to the underlying diagnosis, and he returned to his cheerful, energetic self a few months after starting treatment for the eating disorder.
Andy was the first boy I treated with an eating disorder, but certainly not the last. Since then, I have seen dozens of boys and young men with bulimia nervosa, selective eating, binge eating, and anorexia nervosa. Thankfully, a lot has changed for the better in the 15 years that have passed since I had the privilege of working with Andy. Health professionals and the general public have become more aware that eating disorders affect both men and women. However, boys face some barriers to treatment and recovery.
Since then, I have seen dozens of boys and young men with bulimia nervosa, selective eating, binge eating, and anorexia nervosa. Thankfully, a lot has changed for the better in the 15 years that have passed since I had the privilege of working with Andy. Health professionals and the general public have become more aware that eating disorders affect both men and women. However, boys face some barriers to treatment and recovery.
The stereotype that eating disorders are exclusively a “girl problem” causes men with eating disorders to face even more stigma than women. And because everyone associates eating disorders with girls and young women, health care providers may be less likely to ask males screening questions about eating disorders, and less likely to make a correct diagnosis. Delay in diagnosis causes the disease to become more entrenched over time. By the time a boy arrives for specialized treatment for an eating disorder, months or even years after the onset of symptoms, he may be much more severely ill.
The main symptoms of eating disorders tend to be the same in men and women: a pervasive pattern of food restriction, overeating and/or purging that adversely affects physical and psychological health; severe anxiety about food and weight; and, often, body image disturbance. In my experience, eating disorders for men and women are more similar than they are different. However, there are some key gender differences among symptoms.
Men are often preoccupied with achieving and maintaining a lean, muscular physique. To this end, boys with eating disorders often eat massive amounts of protein and take supplements or even steroids to increase their musculature.
Boys with bulimia or other types of eating disorders can hide their symptoms from themselves and others quite easily. Parents, siblings and peers may find it amusing to watch teenage boys eat massive amounts of food uncontrollably, unaware of the suffering they are experiencing.
Eating disorders in men can result in bradycardia, hypotension and hypothermia, as well as low testosterone, low vitamin D and osteopenia. Many boys with eating disorders consume excessive amounts of protein in an attempt to build muscle. A diet too high in protein can lead to problems with the digestive system and cause damage to the liver and kidneys.
Many boys with eating disorders consume excessive amounts of protein in an attempt to build muscle. A diet too high in protein can lead to problems with the digestive system and cause damage to the liver and kidneys.
The prevalence of eating disorders in men is higher than we think. However, according to the National Eating Disorders Association, almost a third of people with eating disorders are men. Unfortunately, to this day, men are far less likely than women to seek treatment for an eating disorder, so it is likely that there are millions of undiagnosed boys and men.
In closing, I would like to share an inspirational quote from a former teenage patient I treated for an eating disorder a few years ago. Having fully recovered, he told me in his last session: “I am used to seeing the enemy in my body; something that I had to defeat in order to subdue him. But now my body is my companion. We work together and help each other. We are on the same team.