Psychologists best define drive states as
11.4 Drive States – Introduction to Psychology
Chapter 11. Emotions and Motivations
Sudeep Bhatia and George Loewenstein
Our thoughts and behaviors are strongly influenced by affective experiences known as drive states. These drive states motivate us to fulfill goals that are beneficial to our survival and reproduction. This module provides an overview of key drive states, including information about their neurobiology and their psychological effects.
Learning Objectives
- Identify the key properties of drive states
- Describe biological goals accomplished by drive states
- Give examples of drive states
- Outline the neurobiological basis of drive states such as hunger and arousal
- Discuss the main moderators and determinants of drive states such as hunger and arousal
What is the longest you’ve ever gone without eating? A couple of hours? An entire day? How did it feel? Humans rely critically on food for nutrition and energy, and the absence of food can create drastic changes, not only in physical appearance, but in thoughts and behaviors. If you’ve ever fasted for a day, you probably noticed how hunger can take over your mind, directing your attention to foods you could be eating (a cheesy slice of pizza, or perhaps some sweet, cold ice cream), and motivating you to obtain and consume these foods. And once you have eaten and your hunger has been satisfied, your thoughts and behaviors return to normal.
Hunger is a drive state, an affective experience (something you feel, like the sensation of being tired or hungry) that motivates organisms to fulfill goals that are generally beneficial to their survival and reproduction. Like other drive states, such as thirst or sexual arousal, hunger has a profound impact on the functioning of the mind. It affects psychological processes, such as perception, attention, emotion, and motivation, and influences the behaviors that these processes generate.
Drive states differ from other affective or emotional states in terms of the biological functions they accomplish. Whereas all affective states possess valence (i.e., they are positive or negative) and serve to motivate approach or avoidance behaviors (Zajonc, 1998), drive states are unique in that they generate behaviors that result in specific benefits for the body. For example, hunger directs individuals to eat foods that increase blood sugar levels in the body, while thirst causes individuals to drink fluids that increase water levels in the body.
Whereas all affective states possess valence (i.e., they are positive or negative) and serve to motivate approach or avoidance behaviors (Zajonc, 1998), drive states are unique in that they generate behaviors that result in specific benefits for the body. For example, hunger directs individuals to eat foods that increase blood sugar levels in the body, while thirst causes individuals to drink fluids that increase water levels in the body.
Different drive states have different triggers. Most drive states respond to both internal and external cues, but the combinations of internal and external cues, and the specific types of cues, differ between drives. Hunger, for example, depends on internal, visceral signals as well as sensory signals, such as the sight or smell of tasty food. Different drive states also result in different cognitive and emotional states, and are associated with different behaviors. Yet despite these differences, there are a number of properties common to all drive states.
Homeostasis
Figure 11.15 The body needs homeostasis and motivates us – through both pleasure and pain – to stay in balance.Humans, like all organisms, need to maintain a stable state in their various physiological systems. For example, the excessive loss of body water results in dehydration, a dangerous and potentially fatal state. However, too much water can be damaging as well. Thus, a moderate and stable level of body fluid is ideal. The tendency of an organism to maintain this stability across all the different physiological systems in the body is called homeostasis.
Homeostasis is maintained via two key factors. First, the state of the system being regulated must be monitored and compared to an ideal level, or a set point. Second, there need to be mechanisms for moving the system back to this set point—that is, to restore homeostasis when deviations from it are detected. To better understand this, think of the thermostat in your own home. It detects when the current temperature in the house is different than the temperature you have it set at (i.e., the set point). Once the thermostat recognizes the difference, the heating or air conditioning turns on to bring the overall temperature back to the designated level.
It detects when the current temperature in the house is different than the temperature you have it set at (i.e., the set point). Once the thermostat recognizes the difference, the heating or air conditioning turns on to bring the overall temperature back to the designated level.
Many homeostatic mechanisms, such as blood circulation and immune responses, are automatic and nonconscious. Others, however, involve deliberate action. Most drive states motivate action to restore homeostasis using both “punishments” and “rewards.” Imagine that these homeostatic mechanisms are like molecular parents. When you behave poorly by departing from the set point (such as not eating or being somewhere too cold), they raise their voice at you. You experience this as the bad feelings, or “punishments,” of hunger, thirst, or feeling too cold or too hot. However, when you behave well (such as eating nutritious foods when hungry), these homeostatic parents reward you with the pleasure that comes from any activity that moves the system back toward the set point.![]() For example, when body temperature declines below the set point, any activity that helps to restore homeostasis (such as putting one’s hand in warm water) feels pleasurable; and likewise, when body temperature rises above the set point, anything that cools it feels pleasurable.
For example, when body temperature declines below the set point, any activity that helps to restore homeostasis (such as putting one’s hand in warm water) feels pleasurable; and likewise, when body temperature rises above the set point, anything that cools it feels pleasurable.
The Narrowing of Attention
As drive states intensify, they direct attention toward elements, activities, and forms of consumption that satisfy the biological needs associated with the drive. Hunger, for example, draws attention toward food. Outcomes and objects that are not related to satisfying hunger lose their value (Easterbrook, 1959). For instance, has anyone ever invited you to do a fun activity while you were hungry? Likely your response was something like: “I’m not doing anything until I eat first.” Indeed, at a sufficient level of intensity, individuals will sacrifice almost any quantity of goods that do not address the needs signaled by the drive state. For example, cocaine addicts, according to Gawin (1991:1581), “report that virtually all thoughts are focused on cocaine during binges; nourishment, sleep, money, loved ones, responsibility, and survival lose all significance. ”
”
Drive states also produce a second form of attention-narrowing: a collapsing of time-perspective toward the present. That is, they make us impatient. While this form of attention-narrowing is particularly pronounced for the outcomes and behaviors directly related to the biological function being served by the drive state at issue (e.g., “I need food now”), it applies to general concerns for the future as well. Ariely and Loewenstein (2006), for example, investigated the impact of sexual arousal on the thoughts and behaviors of a sample of male undergraduates. These undergraduates were lent laptop computers that they took to their private residences, where they answered a series of questions, both in normal states and in states of high sexual arousal. Ariely and Loewenstein found that being sexually aroused made people extremely impatient for both sexual outcomes and for outcomes in other domains, such as those involving money. In another study Giordano et al. (2002) found that heroin addicts were more impatient with respect to heroin when they were craving it than when they were not. More surprisingly, they were also more impatient toward money (they valued delayed money less) when they were actively craving heroin.
More surprisingly, they were also more impatient toward money (they valued delayed money less) when they were actively craving heroin.
Yet a third form of attention-narrowing involves thoughts and outcomes related to the self versus others. Intense drive states tend to narrow one’s focus inwardly and to undermine altruism—or the desire to do good for others. People who are hungry, in pain, or craving drugs tend to be selfish. Indeed, popular interrogation methods involve depriving individuals of sleep, food, or water, so as to trigger intense drive states leading the subject of the interrogation to divulge information that may betray comrades, friends, and family (Biderman, 1960).
Current Controversy
In 2005, the American Psychological Association (APA) issued a report concluding that psychologists could ethically play a role in the interrogation of people captured in Afghanistan and elsewhere. In 2014, following critical media publicity documenting the APA’s involvement in torture, the APA commissioned a law firm to independently investigate APA involvement in interrogation. The firm’s report was damaging to the APA because it suggested that APA leaders colluded with the Department of Defense, CIA, and and other government officials not only to aid in interrogation itself, but to provide justification for government guidelines that defined torture (which is banned by international treaties signed by the U.S.) in a narrow fashion that excluded, for example, so-called “stress positions” and sleep deprivation.Critical Questions
The firm’s report was damaging to the APA because it suggested that APA leaders colluded with the Department of Defense, CIA, and and other government officials not only to aid in interrogation itself, but to provide justification for government guidelines that defined torture (which is banned by international treaties signed by the U.S.) in a narrow fashion that excluded, for example, so-called “stress positions” and sleep deprivation.Critical Questions
1. Do you think that manipulating drive states, such as the need for sleep, constitutes torture?
2. How do you think research on drive states should inform the definition of “torture” and our definition of ethical interrogation techniques? See the full Hoffman Report here – http://www.apa.org/independent-review/APA-FINAL-Report-7.2.15.pdfFor more coverage – http://www.nytimes.com/2015/07/11/us/psychologists-shielded-us-torture-program-report-finds.html
Thus far we have considered drive states abstractly. We have discussed the ways in which they relate to other affective and motivational mechanisms, as well as their main biological purpose and general effects on thought and behavior. Yet, despite serving the same broader goals, different drive states are often remarkably different in terms of their specific properties. To understand some of these specific properties, we will explore two different drive states that play very important roles in determining behavior, and in ensuring human survival: hunger and sexual arousal.
We have discussed the ways in which they relate to other affective and motivational mechanisms, as well as their main biological purpose and general effects on thought and behavior. Yet, despite serving the same broader goals, different drive states are often remarkably different in terms of their specific properties. To understand some of these specific properties, we will explore two different drive states that play very important roles in determining behavior, and in ensuring human survival: hunger and sexual arousal.
Hunger
Figure 11.16 External cues, like the sight and smell of food, can ignite feelings of hunger.Hunger is a classic example of a drive state, one that results in thoughts and behaviors related to the consumption of food. Hunger is generally triggered by low glucose levels in the blood (Rolls, 2000), and behaviors resulting from hunger aim to restore homeostasis regarding those glucose levels. Various other internal and external cues can also cause hunger. For example, when fats are broken down in the body for energy, this initiates a chemical cue that the body should search for food (Greenberg, Smith, & Gibbs, 1990). External cues include the time of day, estimated time until the next feeding (hunger increases immediately prior to food consumption), and the sight, smell, taste, and even touch of food and food-related stimuli. Note that while hunger is a generic feeling, it has nuances that can provoke the eating of specific foods that correct for nutritional imbalances we may not even be conscious of. For example, a couple who was lost adrift at sea found they inexplicably began to crave the eyes of fish. Only later, after they had been rescued, did they learn that fish eyes are rich in vitamin C—a very important nutrient that they had been depleted of while lost in the ocean (Walker, 2014).The
hypothalamus (located in the lower, central part of the brain) plays a very important role in eating behavior. It is responsible for synthesizing and secreting various hormones.
For example, when fats are broken down in the body for energy, this initiates a chemical cue that the body should search for food (Greenberg, Smith, & Gibbs, 1990). External cues include the time of day, estimated time until the next feeding (hunger increases immediately prior to food consumption), and the sight, smell, taste, and even touch of food and food-related stimuli. Note that while hunger is a generic feeling, it has nuances that can provoke the eating of specific foods that correct for nutritional imbalances we may not even be conscious of. For example, a couple who was lost adrift at sea found they inexplicably began to crave the eyes of fish. Only later, after they had been rescued, did they learn that fish eyes are rich in vitamin C—a very important nutrient that they had been depleted of while lost in the ocean (Walker, 2014).The
hypothalamus (located in the lower, central part of the brain) plays a very important role in eating behavior. It is responsible for synthesizing and secreting various hormones. The lateral hypothalamus (LH) is concerned largely with hunger and, in fact, lesions (i.e., damage) of the LH can eliminate the desire for eating entirely—to the point that animals starve themselves to death unless kept alive by force feeding (Anand & Brobeck, 1951). Additionally, artificially stimulating the LH, using electrical currents, can generate eating behavior if food is available (Andersson, 1951).Activation of the LH can not only increase the desirability of food but can also reduce the desirability of nonfood-related items. For example, Brendl, Markman, and Messner (2003) found that participants who were given a handful of popcorn to trigger hunger not only had higher ratings of food products, but also had lower ratings of nonfood products—compared with participants whose appetites were not similarly primed. That is, because eating had become more important, other non-food products lost some of their value.Hunger is only part of the story of when and why we eat. A related process, satiation, refers to the decline of hunger and the eventual termination of eating behavior.
The lateral hypothalamus (LH) is concerned largely with hunger and, in fact, lesions (i.e., damage) of the LH can eliminate the desire for eating entirely—to the point that animals starve themselves to death unless kept alive by force feeding (Anand & Brobeck, 1951). Additionally, artificially stimulating the LH, using electrical currents, can generate eating behavior if food is available (Andersson, 1951).Activation of the LH can not only increase the desirability of food but can also reduce the desirability of nonfood-related items. For example, Brendl, Markman, and Messner (2003) found that participants who were given a handful of popcorn to trigger hunger not only had higher ratings of food products, but also had lower ratings of nonfood products—compared with participants whose appetites were not similarly primed. That is, because eating had become more important, other non-food products lost some of their value.Hunger is only part of the story of when and why we eat. A related process, satiation, refers to the decline of hunger and the eventual termination of eating behavior. Whereas the feeling of hunger gets you to start eating, the feeling of satiation gets you to stop. Perhaps surprisingly, hunger and satiation are two distinct processes, controlled by different circuits in the brain and triggered by different cues. Distinct from the LH, which plays an important role in hunger, the ventromedial hypothalamus (VMH) plays an important role in satiety. Though lesions of the VMH can cause an animal to overeat to the point of obesity, the relationship between the LH and the VMB is quite complicated. Rats with VMH lesions can also be quite finicky about their food (Teitelbaum, 1955).
Whereas the feeling of hunger gets you to start eating, the feeling of satiation gets you to stop. Perhaps surprisingly, hunger and satiation are two distinct processes, controlled by different circuits in the brain and triggered by different cues. Distinct from the LH, which plays an important role in hunger, the ventromedial hypothalamus (VMH) plays an important role in satiety. Though lesions of the VMH can cause an animal to overeat to the point of obesity, the relationship between the LH and the VMB is quite complicated. Rats with VMH lesions can also be quite finicky about their food (Teitelbaum, 1955).
Other brain areas, besides the LH and VMH, also play important roles in eating behavior. The sensory cortices (visual, olfactory, and taste), for example, are important in identifying food items. These areas provide informational value, however, not hedonic evaluations. That is, these areas help tell a person what is good or safe to eat, but they don’t provide the pleasure (or hedonic) sensations that actually eating the food produces. While many sensory functions are roughly stable across different psychological states, other functions, such as the detection of food-related stimuli, are enhanced when the organism is in a hungry drive state.
While many sensory functions are roughly stable across different psychological states, other functions, such as the detection of food-related stimuli, are enhanced when the organism is in a hungry drive state.
After identifying a food item, the brain also needs to determine its reward value, which affects the organism’s motivation to consume the food. The reward value ascribed to a particular item is, not surprisingly, sensitive to the level of hunger experienced by the organism. The hungrier you are, the greater the reward value of the food. Neurons in the areas where reward values are processed, such as the orbitofrontal cortex, fire more rapidly at the sight or taste of food when the organism is hungry relative to if it is satiated.
Sexual Arousal
Figure 11.17 Unlike other drive states the mechanisms that trigger sexual arousal are not the same for men and women.A second drive state, especially critical to reproduction, is sexual arousal. Sexual arousal results in thoughts and behaviors related to sexual activity. As with hunger, it is generated by a large range of internal and external mechanisms that are triggered either after the extended absence of sexual activity or by the immediate presence and possibility of sexual activity (or by cues commonly associated with such possibilities). Unlike hunger, however, these mechanisms can differ substantially between males and females, indicating important evolutionary differences in the biological functions that sexual arousal serves for different sexes.Sexual arousal and pleasure in males, for example, is strongly related to the preoptic area, a region in the anterior hypothalamus (or the front of the hypothalamus). If the preoptic area is damaged, male sexual behavior is severely impaired. For example, rats that have had prior sexual experiences will still seek out sexual partners after their preoptic area is lesioned. However, once having secured a sexual partner, rats with lesioned preoptic areas will show no further inclination to actually initiate sex.
As with hunger, it is generated by a large range of internal and external mechanisms that are triggered either after the extended absence of sexual activity or by the immediate presence and possibility of sexual activity (or by cues commonly associated with such possibilities). Unlike hunger, however, these mechanisms can differ substantially between males and females, indicating important evolutionary differences in the biological functions that sexual arousal serves for different sexes.Sexual arousal and pleasure in males, for example, is strongly related to the preoptic area, a region in the anterior hypothalamus (or the front of the hypothalamus). If the preoptic area is damaged, male sexual behavior is severely impaired. For example, rats that have had prior sexual experiences will still seek out sexual partners after their preoptic area is lesioned. However, once having secured a sexual partner, rats with lesioned preoptic areas will show no further inclination to actually initiate sex. For females, though, the preoptic area fulfills different roles, such as functions involved with eating behaviors. Instead, there is a different region of the brain, the ventromedial hypothalamus (the lower, central part) that plays a similar role for females as the preoptic area does for males. Neurons in the ventromedial hypothalamus determine the excretion of estradiol, an estrogen hormone that regulates sexual receptivity (or the willingness to accept a sexual partner). In many mammals, these neurons send impulses to the periaqueductal gray (a region in the midbrain) which is responsible for defensive behaviors, such as freezing immobility, running, increases in blood pressure, and other motor responses. Typically, these defensive responses might keep the female rat from interacting with the male one. However, during sexual arousal, these defensive responses are weakened and lordosis behavior, a physical sexual posture that serves as an invitation to mate, is initiated (Kow and Pfaff, 1998).
For females, though, the preoptic area fulfills different roles, such as functions involved with eating behaviors. Instead, there is a different region of the brain, the ventromedial hypothalamus (the lower, central part) that plays a similar role for females as the preoptic area does for males. Neurons in the ventromedial hypothalamus determine the excretion of estradiol, an estrogen hormone that regulates sexual receptivity (or the willingness to accept a sexual partner). In many mammals, these neurons send impulses to the periaqueductal gray (a region in the midbrain) which is responsible for defensive behaviors, such as freezing immobility, running, increases in blood pressure, and other motor responses. Typically, these defensive responses might keep the female rat from interacting with the male one. However, during sexual arousal, these defensive responses are weakened and lordosis behavior, a physical sexual posture that serves as an invitation to mate, is initiated (Kow and Pfaff, 1998). Thus, while the preoptic area encourages males to engage in sexual activity, the ventromedial hypothalamus fulfills that role for females.Other differences between males and females involve overlapping functions of neural modules. These neural modules often provide clues about the biological roles played by sexual arousal and sexual activity in males and females. Areas of the brain that are important for male sexuality overlap to a great extent with areas that are also associated with aggression. In contrast, areas important for female sexuality overlap extensively with those that are also connected to nurturance (Panksepp, 2004).
Thus, while the preoptic area encourages males to engage in sexual activity, the ventromedial hypothalamus fulfills that role for females.Other differences between males and females involve overlapping functions of neural modules. These neural modules often provide clues about the biological roles played by sexual arousal and sexual activity in males and females. Areas of the brain that are important for male sexuality overlap to a great extent with areas that are also associated with aggression. In contrast, areas important for female sexuality overlap extensively with those that are also connected to nurturance (Panksepp, 2004).
One region of the brain that seems to play an important role in sexual pleasure for both males and females is the septal nucleus, an area that receives reciprocal connections from many other brain regions, including the hypothalamus and the amygdala (a region of the brain primarily involved with emotions). This region shows considerable activity, in terms of rhythmic spiking, during sexual orgasm. It is also one of the brain regions that rats will most reliably voluntarily self-stimulate (Olds & Milner, 1954). In humans, placing a small amount of acetylcholine into this region, or stimulating it electrically, has been reported to produce a feeling of imminent orgasm (Heath, 1964).
It is also one of the brain regions that rats will most reliably voluntarily self-stimulate (Olds & Milner, 1954). In humans, placing a small amount of acetylcholine into this region, or stimulating it electrically, has been reported to produce a feeling of imminent orgasm (Heath, 1964).
Drive states are evolved motivational mechanisms designed to ensure that organisms take self-beneficial actions. In this module, we have reviewed key properties of drive states, such as homeostasis and the narrowing of attention. We have also discussed, in some detail, two important drive states—hunger and sexual arousal—and explored their underlying neurobiology and the ways in which various environmental and biological factors affect their properties.
There are many drive states besides hunger and sexual arousal that affect humans on a daily basis. Fear, thirst, exhaustion, exploratory and maternal drives, and drug cravings are all drive states that have been studied by researchers (see e. g., Buck, 1999; Van Boven & Loewenstein, 2003). Although these drive states share some of the properties discussed in this module, each also has unique features that allow it to effectively fulfill its evolutionary function.
g., Buck, 1999; Van Boven & Loewenstein, 2003). Although these drive states share some of the properties discussed in this module, each also has unique features that allow it to effectively fulfill its evolutionary function.
One key difference between drive states is the extent to which they are triggered by internal as opposed to external stimuli. Thirst, for example, is induced both by decreased fluid levels and an increased concentration of salt in the body. Fear, on the other hand, is induced by perceived threats in the external environment. Drug cravings are triggered both by internal homeostatic mechanisms and by external visual, olfactory, and contextual cues. Other drive states, such as those pertaining to maternity, are triggered by specific events in the organism’s life. Differences such as these make the study of drive states a scientifically interesting and important endeavor. Drive states are rich in their diversity, and many questions involving their neurocognitive underpinnings, environmental determinants, and behavioral effects, have yet to be answered.
One final thing to consider, not discussed in this module, relates to the real-world consequences of drive states. Hunger, sexual arousal, and other drive states are all psychological mechanisms that have evolved gradually over millions of years. We share these drive states not only with our human ancestors but with other animals, such as monkeys, dogs, and rats. It is not surprising then that these drive states, at times, lead us to behave in ways that are ill-suited to our modern lives. Consider, for example, the obesity epidemic that is affecting countries around the world. Like other diseases of affluence, obesity is a product of drive states that are too easily fulfilled: homeostatic mechanisms that once worked well when food was scarce now backfire when meals rich in fat and sugar are readily available. Unrestricted sexual arousal can have similarly perverse effects on our well-being. Countless politicians have sacrificed their entire life’s work (not to mention their marriages) by indulging adulterous sexual impulses toward colleagues, staffers, prostitutes, and others over whom they have social or financial power. It not an overstatement to say that many problems of the 21st century, from school massacres to obesity to drug addiction, are influenced by the mismatch between our drive states and our uniquely modern ability to fulfill them at a moment’s notice.
It not an overstatement to say that many problems of the 21st century, from school massacres to obesity to drug addiction, are influenced by the mismatch between our drive states and our uniquely modern ability to fulfill them at a moment’s notice.
Image Attributions
Figure 11.14: Jeremy Brooks, https://goo.gl/XrFG2W, CC BY-NC 2.0, https://goo.gl/VnKlK8
Figure 11.15: ashleigh390, https://goo.gl/yXQtEC, CC-BY 2.0, https://goo.gl/BRvSA7
Figure 11.16: Marco Verch, https://goo.gl/c4TC5A, CC BY 2.0, https://goo.gl/BRvSA7
Figure 11.17: Matthew Romack, https://goo.gl/IUbbk0, CC BY 2.0, https://goo.gl/BRvSA7
References
Anand, B. K., & Brobeck, J. R. (1951). Hypothalamic control of food intake in rats and cats. The Yale journal of biology and medicine, 24(2), 123.
Andersson, B. (1951). The effect and localization of electrical stimulation of certain parts of the brain stem in sheep and goats. Acta Physiologica Scandinavica, 23(1), 8–23.
Acta Physiologica Scandinavica, 23(1), 8–23.
Ariely, D., & Loewenstein, G. (2006). The heat of the moment: The effect of sexual arousal on sexual decision making. Journal of Behavioral Decision Making, 19(2), 87–98
Biderman, A. D. (1960). Social-psychological needs and “involuntary” behavior as illustrated by compliance in interrogation. Sociometry, 23(2), 120–147.
Brendl, C. M., Markman, A. B., & Messner, C. (2003). The devaluation effect: Activating a need devalues unrelated objects. Journal of Consumer Research, 29(4), 463–473.
Buck, R. (1999). The biological affects: A typology. Psychological Review, 106, 301–336.
Easterbrook, J. A. (1959). The effect of emotion on cue utilization and the organization of behavior. Psychological Review, 66(3).
Gawin, F. H. (1991). Cocaine addiction: psychology and neurophysiology. Science, 251(5001), 1580–1586.
Giordano, L. A., Bickel, W. K., Loewenstein, G., Jacobs, E. A., Marsch, L., & Badger, G. J. (2002). Mild opioid deprivation increases the degree that opioid-dependent outpatients discount delayed heroin and money. Psychopharmacology, 163(2), 174–182.
K., Loewenstein, G., Jacobs, E. A., Marsch, L., & Badger, G. J. (2002). Mild opioid deprivation increases the degree that opioid-dependent outpatients discount delayed heroin and money. Psychopharmacology, 163(2), 174–182.
Greenberg, D., Smith, G. P., & Gibbs, J. (1990). Intraduodenal infusions of fats elicit satiety in sham-feeding rats. American Journal of Physiology-Regulatory, Integrative, and Comparative Physiology, 259(1), 110–118.
Heath, R. G. (1964). Pleasure response of human subjects to direct stimulation of the brain: Physiologic and psychodynamic considerations. In R. G. Heath (Ed.), The role of pleasure in behavior (pp. 219–243). New York, NY: Hoeber.
Kow, L. M., & Pfaff, D. W. (1998). Mapping of neural and signal transduction pathways for lordosis in the search for estrogen actions on the central nervous system. Behavioural Brain Research, 92(2), 169–180
Olds, J., & Milner, P. (1954). Positive reinforcement produced by electrical stimulation of septal area and other regions of rat brain. Journal of Comparative and Physiological Psychology, 47(6), 419.
Journal of Comparative and Physiological Psychology, 47(6), 419.
Panksepp, J. (2004). Affective neuroscience: The foundations of human and animal emotions (Vol. 4). New York, NY: Oxford University Press U.S.
Rolls, E. T. (2000). The orbitofrontal cortex and reward. Cerebral Cortex, 10(3), 284-294.
Teitelbaum, P. (1955). Sensory control of hypothalamic hyperphagia. Journal of Comparative and Physiological Psychology, 48(3), 156.
Van Boven, L., & Loewenstein, G. (2003). Projection of transient drive states. Personality and Social Psychology Bulletin, 29, 1159–1168.
Walker, P. (2014). Castaway’s sea savvy could have helped him survive year adrift, says expert. The Guardian. Retried from http://www.theguardian.com/world/2014/feb/04/castaway-jose-salvador-alvarenga-survival-expert
Zajonc, R. B. (1998). Emotions. In Gilbert, D. T., Fiske, S. T., & Lindzey, G. (Eds.), The handbook of social psychology (Vols. 1 and 2, 4th ed., pp. 591–632). New York, NY: McGraw-Hill.
1 and 2, 4th ed., pp. 591–632). New York, NY: McGraw-Hill.
Drive States | Noba
By Sudeep Bhatia and George LoewensteinCarnegie Mellon University
Our thoughts and behaviors are strongly influenced by affective experiences known as drive states. These drive states motivate us to fulfill goals that are beneficial to our survival and reproduction. This module provides an overview of key drive states, including information about their neurobiology and their psychological effects.
- Affect
- Homeostatis
- Hunger
- Sexual arousal
Learning Objectives
- Identify the key properties of drive states
- Describe biological goals accomplished by drive states
- Give examples of drive states
- Outline the neurobiological basis of drive states such as hunger and arousal
- Discuss the main moderators and determinants of drive states such as hunger and arousal
What is the longest you’ve ever gone without eating? A couple of hours? An entire day? How did it feel? Humans rely critically on food for nutrition and energy, and the absence of food can create drastic changes, not only in physical appearance, but in thoughts and behaviors. If you’ve ever fasted for a day, you probably noticed how hunger can take over your mind, directing your attention to foods you could be eating (a cheesy slice of pizza, or perhaps some sweet, cold ice cream), and motivating you to obtain and consume these foods. And once you have eaten and your hunger has been satisfied, your thoughts and behaviors return to normal.
If you’ve ever fasted for a day, you probably noticed how hunger can take over your mind, directing your attention to foods you could be eating (a cheesy slice of pizza, or perhaps some sweet, cold ice cream), and motivating you to obtain and consume these foods. And once you have eaten and your hunger has been satisfied, your thoughts and behaviors return to normal.
Hunger is a drive state, an affective experience (something you feel, like the sensation of being tired or hungry) that motivates organisms to fulfill goals that are generally beneficial to their survival and reproduction. Like other drive states, such as thirst or sexual arousal, hunger has a profound impact on the functioning of the mind. It affects psychological processes, such as perception, attention, emotion, and motivation, and influences the behaviors that these processes generate.
Drive states differ from other affective or emotional states in terms of the biological functions they accomplish. Whereas all affective states possess valence (i.e., they are positive or negative) and serve to motivate approach or avoidance behaviors (Zajonc, 1998), drive states are unique in that they generate behaviors that result in specific benefits for the body. For example, hunger directs individuals to eat foods that increase blood sugar levels in the body, while thirst causes individuals to drink fluids that increase water levels in the body.
Whereas all affective states possess valence (i.e., they are positive or negative) and serve to motivate approach or avoidance behaviors (Zajonc, 1998), drive states are unique in that they generate behaviors that result in specific benefits for the body. For example, hunger directs individuals to eat foods that increase blood sugar levels in the body, while thirst causes individuals to drink fluids that increase water levels in the body.
Different drive states have different triggers. Most drive states respond to both internal and external cues, but the combinations of internal and external cues, and the specific types of cues, differ between drives. Hunger, for example, depends on internal, visceral signals as well as sensory signals, such as the sight or smell of tasty food. Different drive states also result in different cognitive and emotional states, and are associated with different behaviors. Yet despite these differences, there are a number of properties common to all drive states.
Homeostasis
Humans, like all organisms, need to maintain a stable state in their various physiological systems. For example, the excessive loss of body water results in dehydration, a dangerous and potentially fatal state. However, too much water can be damaging as well. Thus, a moderate and stable level of body fluid is ideal. The tendency of an organism to maintain this stability across all the different physiological systems in the body is called homeostasis.
Homeostasis is maintained via two key factors. First, the state of the system being regulated must be monitored and compared to an ideal level, or a set point. Second, there need to be mechanisms for moving the system back to this set point—that is, to restore homeostasis when deviations from it are detected. To better understand this, think of the thermostat in your own home. It detects when the current temperature in the house is different than the temperature you have it set at (i.e., the set point). Once the thermostat recognizes the difference, the heating or air conditioning turns on to bring the overall temperature back to the designated level.
Many homeostatic mechanisms, such as blood circulation and immune responses, are automatic and nonconscious. Others, however, involve deliberate action. Most drive states motivate action to restore homeostasis using both “punishments” and “rewards.” Imagine that these homeostatic mechanisms are like molecular parents. When you behave poorly by departing from the set point (such as not eating or being somewhere too cold), they raise their voice at you. You experience this as the bad feelings, or “punishments,” of hunger, thirst, or feeling too cold or too hot. However, when you behave well (such as eating nutritious foods when hungry), these homeostatic parents reward you with the pleasure that comes from any activity that moves the system back toward the set point. For example, when body temperature declines below the set point, any activity that helps to restore homeostasis (such as putting one’s hand in warm water) feels pleasurable; and likewise, when body temperature rises above the set point, anything that cools it feels pleasurable.
The Narrowing of Attention
As drive states intensify, they direct attention toward elements, activities, and forms of consumption that satisfy the biological needs associated with the drive. Hunger, for example, draws attention toward food. Outcomes and objects that are not related to satisfying hunger lose their value (Easterbrook, 1959). For instance, has anyone ever invited you to do a fun activity while you were hungry? Likely your response was something like: “I’m not doing anything until I eat first.” Indeed, at a sufficient level of intensity, individuals will sacrifice almost any quantity of goods that do not address the needs signaled by the drive state. For example, cocaine addicts, according to Gawin (1991:1581), “report that virtually all thoughts are focused on cocaine during binges; nourishment, sleep, money, loved ones, responsibility, and survival lose all significance.”
Drive states also produce a second form of attention-narrowing: a collapsing of time-perspective toward the present. That is, they make us impatient. While this form of attention-narrowing is particularly pronounced for the outcomes and behaviors directly related to the biological function being served by the drive state at issue (e.g., “I need food now”), it applies to general concerns for the future as well. Ariely and Loewenstein (2006), for example, investigated the impact of sexual arousal on the thoughts and behaviors of a sample of male undergraduates. These undergraduates were lent laptop computers that they took to their private residences, where they answered a series of questions, both in normal states and in states of high sexual arousal. Ariely and Loewenstein found that being sexually aroused made people extremely impatient for both sexual outcomes and for outcomes in other domains, such as those involving money. In another study Giordano et al. (2002) found that heroin addicts were more impatient with respect to heroin when they were craving it than when they were not. More surprisingly, they were also more impatient toward money (they valued delayed money less) when they were actively craving heroin.
That is, they make us impatient. While this form of attention-narrowing is particularly pronounced for the outcomes and behaviors directly related to the biological function being served by the drive state at issue (e.g., “I need food now”), it applies to general concerns for the future as well. Ariely and Loewenstein (2006), for example, investigated the impact of sexual arousal on the thoughts and behaviors of a sample of male undergraduates. These undergraduates were lent laptop computers that they took to their private residences, where they answered a series of questions, both in normal states and in states of high sexual arousal. Ariely and Loewenstein found that being sexually aroused made people extremely impatient for both sexual outcomes and for outcomes in other domains, such as those involving money. In another study Giordano et al. (2002) found that heroin addicts were more impatient with respect to heroin when they were craving it than when they were not. More surprisingly, they were also more impatient toward money (they valued delayed money less) when they were actively craving heroin.
Yet a third form of attention-narrowing involves thoughts and outcomes related to the self versus others. Intense drive states tend to narrow one’s focus inwardly and to undermine altruism—or the desire to do good for others. People who are hungry, in pain, or craving drugs tend to be selfish. Indeed, popular interrogation methods involve depriving individuals of sleep, food, or water, so as to trigger intense drive states leading the subject of the interrogation to divulge information that may betray comrades, friends, and family (Biderman, 1960).
Thus far we have considered drive states abstractly. We have discussed the ways in which they relate to other affective and motivational mechanisms, as well as their main biological purpose and general effects on thought and behavior. Yet, despite serving the same broader goals, different drive states are often remarkably different in terms of their specific properties. To understand some of these specific properties, we will explore two different drive states that play very important roles in determining behavior, and in ensuring human survival: hunger and sexual arousal.
Hunger
External cues, like the sight and smell of food, can ignite feelings of hunger. [Image: Marco Verch, https://goo.gl/c4TC5A, CC BY 2.0, https://goo.gl/BRvSA7]Hunger is a classic example of a drive state, one that results in thoughts and behaviors related to the consumption of food. Hunger is generally triggered by low glucose levels in the blood (Rolls, 2000), and behaviors resulting from hunger aim to restore homeostasis regarding those glucose levels. Various other internal and external cues can also cause hunger. For example, when fats are broken down in the body for energy, this initiates a chemical cue that the body should search for food (Greenberg, Smith, & Gibbs, 1990). External cues include the time of day, estimated time until the next feeding (hunger increases immediately prior to food consumption), and the sight, smell, taste, and even touch of food and food-related stimuli. Note that while hunger is a generic feeling, it has nuances that can provoke the eating of specific foods that correct for nutritional imbalances we may not even be conscious of. For example, a couple who was lost adrift at sea found they inexplicably began to crave the eyes of fish. Only later, after they had been rescued, did they learn that fish eyes are rich in vitamin C—a very important nutrient that they had been depleted of while lost in the ocean (Walker, 2014).
For example, a couple who was lost adrift at sea found they inexplicably began to crave the eyes of fish. Only later, after they had been rescued, did they learn that fish eyes are rich in vitamin C—a very important nutrient that they had been depleted of while lost in the ocean (Walker, 2014).
The hypothalamus (located in the lower, central part of the brain) plays a very important role in eating behavior. It is responsible for synthesizing and secreting various hormones. The lateral hypothalamus (LH) is concerned largely with hunger and, in fact, lesions (i.e., damage) of the LH can eliminate the desire for eating entirely—to the point that animals starve themselves to death unless kept alive by force feeding (Anand & Brobeck, 1951). Additionally, artificially stimulating the LH, using electrical currents, can generate eating behavior if food is available (Andersson, 1951).
Activation of the LH can not only increase the desirability of food but can also reduce the desirability of nonfood-related items. For example, Brendl, Markman, and Messner (2003) found that participants who were given a handful of popcorn to trigger hunger not only had higher ratings of food products, but also had lower ratings of nonfood products—compared with participants whose appetites were not similarly primed. That is, because eating had become more important, other non-food products lost some of their value.
For example, Brendl, Markman, and Messner (2003) found that participants who were given a handful of popcorn to trigger hunger not only had higher ratings of food products, but also had lower ratings of nonfood products—compared with participants whose appetites were not similarly primed. That is, because eating had become more important, other non-food products lost some of their value.
Hunger is only part of the story of when and why we eat. A related process, satiation, refers to the decline of hunger and the eventual termination of eating behavior. Whereas the feeling of hunger gets you to start eating, the feeling of satiation gets you to stop. Perhaps surprisingly, hunger and satiation are two distinct processes, controlled by different circuits in the brain and triggered by different cues. Distinct from the LH, which plays an important role in hunger, the ventromedial hypothalamus (VMH) plays an important role in satiety. Though lesions of the VMH can cause an animal to overeat to the point of obesity, the relationship between the LH and the VMB is quite complicated. Rats with VMH lesions can also be quite finicky about their food (Teitelbaum, 1955).
Rats with VMH lesions can also be quite finicky about their food (Teitelbaum, 1955).
Other brain areas, besides the LH and VMH, also play important roles in eating behavior. The sensory cortices (visual, olfactory, and taste), for example, are important in identifying food items. These areas provide informational value, however, not hedonic evaluations. That is, these areas help tell a person what is good or safe to eat, but they don’t provide the pleasure (or hedonic) sensations that actually eating the food produces. While many sensory functions are roughly stable across different psychological states, other functions, such as the detection of food-related stimuli, are enhanced when the organism is in a hungry drive state.
After identifying a food item, the brain also needs to determine its reward value, which affects the organism’s motivation to consume the food. The reward value ascribed to a particular item is, not surprisingly, sensitive to the level of hunger experienced by the organism. The hungrier you are, the greater the reward value of the food. Neurons in the areas where reward values are processed, such as the orbitofrontal cortex, fire more rapidly at the sight or taste of food when the organism is hungry relative to if it is satiated.
The hungrier you are, the greater the reward value of the food. Neurons in the areas where reward values are processed, such as the orbitofrontal cortex, fire more rapidly at the sight or taste of food when the organism is hungry relative to if it is satiated.
Sexual Arousal
Unlike other drive states the mechanisms that trigger sexual arousal are not the same for men and women. [Image: Matthew Romack, https://goo.gl/IUbbk0, CC BY 2.0, https://goo.gl/BRvSA7]A second drive state, especially critical to reproduction, is sexual arousal. Sexual arousal results in thoughts and behaviors related to sexual activity. As with hunger, it is generated by a large range of internal and external mechanisms that are triggered either after the extended absence of sexual activity or by the immediate presence and possibility of sexual activity (or by cues commonly associated with such possibilities). Unlike hunger, however, these mechanisms can differ substantially between males and females, indicating important evolutionary differences in the biological functions that sexual arousal serves for different sexes.
Sexual arousal and pleasure in males, for example, is strongly related to the preoptic area, a region in the anterior hypothalamus (or the front of the hypothalamus). If the preoptic area is damaged, male sexual behavior is severely impaired. For example, rats that have had prior sexual experiences will still seek out sexual partners after their preoptic area is lesioned. However, once having secured a sexual partner, rats with lesioned preoptic areas will show no further inclination to actually initiate sex.
For females, though, the preoptic area fulfills different roles, such as functions involved with eating behaviors. Instead, there is a different region of the brain, the ventromedial hypothalamus (the lower, central part) that plays a similar role for females as the preoptic area does for males. Neurons in the ventromedial hypothalamus determine the excretion of estradiol, an estrogen hormone that regulates sexual receptivity (or the willingness to accept a sexual partner). In many mammals, these neurons send impulses to the periaqueductal gray (a region in the midbrain) which is responsible for defensive behaviors, such as freezing immobility, running, increases in blood pressure, and other motor responses. Typically, these defensive responses might keep the female rat from interacting with the male one. However, during sexual arousal, these defensive responses are weakened and lordosis behavior, a physical sexual posture that serves as an invitation to mate, is initiated (Kow and Pfaff, 1998). Thus, while the preoptic area encourages males to engage in sexual activity, the ventromedial hypothalamus fulfills that role for females.
In many mammals, these neurons send impulses to the periaqueductal gray (a region in the midbrain) which is responsible for defensive behaviors, such as freezing immobility, running, increases in blood pressure, and other motor responses. Typically, these defensive responses might keep the female rat from interacting with the male one. However, during sexual arousal, these defensive responses are weakened and lordosis behavior, a physical sexual posture that serves as an invitation to mate, is initiated (Kow and Pfaff, 1998). Thus, while the preoptic area encourages males to engage in sexual activity, the ventromedial hypothalamus fulfills that role for females.
Other differences between males and females involve overlapping functions of neural modules. These neural modules often provide clues about the biological roles played by sexual arousal and sexual activity in males and females. Areas of the brain that are important for male sexuality overlap to a great extent with areas that are also associated with aggression. In contrast, areas important for female sexuality overlap extensively with those that are also connected to nurturance (Panksepp, 2004).
In contrast, areas important for female sexuality overlap extensively with those that are also connected to nurturance (Panksepp, 2004).
One region of the brain that seems to play an important role in sexual pleasure for both males and females is the septal nucleus, an area that receives reciprocal connections from many other brain regions, including the hypothalamus and the amygdala (a region of the brain primarily involved with emotions). This region shows considerable activity, in terms of rhythmic spiking, during sexual orgasm. It is also one of the brain regions that rats will most reliably voluntarily self-stimulate (Olds & Milner, 1954). In humans, placing a small amount of acetylcholine into this region, or stimulating it electrically, has been reported to produce a feeling of imminent orgasm (Heath, 1964).
Drive states are evolved motivational mechanisms designed to ensure that organisms take self-beneficial actions. In this module, we have reviewed key properties of drive states, such as homeostasis and the narrowing of attention. We have also discussed, in some detail, two important drive states—hunger and sexual arousal—and explored their underlying neurobiology and the ways in which various environmental and biological factors affect their properties.
We have also discussed, in some detail, two important drive states—hunger and sexual arousal—and explored their underlying neurobiology and the ways in which various environmental and biological factors affect their properties.
There are many drive states besides hunger and sexual arousal that affect humans on a daily basis. Fear, thirst, exhaustion, exploratory and maternal drives, and drug cravings are all drive states that have been studied by researchers (see e.g., Buck, 1999; Van Boven & Loewenstein, 2003). Although these drive states share some of the properties discussed in this module, each also has unique features that allow it to effectively fulfill its evolutionary function.
One key difference between drive states is the extent to which they are triggered by internal as opposed to external stimuli. Thirst, for example, is induced both by decreased fluid levels and an increased concentration of salt in the body. Fear, on the other hand, is induced by perceived threats in the external environment. Drug cravings are triggered both by internal homeostatic mechanisms and by external visual, olfactory, and contextual cues. Other drive states, such as those pertaining to maternity, are triggered by specific events in the organism’s life. Differences such as these make the study of drive states a scientifically interesting and important endeavor. Drive states are rich in their diversity, and many questions involving their neurocognitive underpinnings, environmental determinants, and behavioral effects, have yet to be answered.
Drug cravings are triggered both by internal homeostatic mechanisms and by external visual, olfactory, and contextual cues. Other drive states, such as those pertaining to maternity, are triggered by specific events in the organism’s life. Differences such as these make the study of drive states a scientifically interesting and important endeavor. Drive states are rich in their diversity, and many questions involving their neurocognitive underpinnings, environmental determinants, and behavioral effects, have yet to be answered.
One final thing to consider, not discussed in this module, relates to the real-world consequences of drive states. Hunger, sexual arousal, and other drive states are all psychological mechanisms that have evolved gradually over millions of years. We share these drive states not only with our human ancestors but with other animals, such as monkeys, dogs, and rats. It is not surprising then that these drive states, at times, lead us to behave in ways that are ill-suited to our modern lives. Consider, for example, the obesity epidemic that is affecting countries around the world. Like other diseases of affluence, obesity is a product of drive states that are too easily fulfilled: homeostatic mechanisms that once worked well when food was scarce now backfire when meals rich in fat and sugar are readily available. Unrestricted sexual arousal can have similarly perverse effects on our well-being. Countless politicians have sacrificed their entire life’s work (not to mention their marriages) by indulging adulterous sexual impulses toward colleagues, staffers, prostitutes, and others over whom they have social or financial power. It not an overstatement to say that many problems of the 21st century, from school massacres to obesity to drug addiction, are influenced by the mismatch between our drive states and our uniquely modern ability to fulfill them at a moment’s notice.
Consider, for example, the obesity epidemic that is affecting countries around the world. Like other diseases of affluence, obesity is a product of drive states that are too easily fulfilled: homeostatic mechanisms that once worked well when food was scarce now backfire when meals rich in fat and sugar are readily available. Unrestricted sexual arousal can have similarly perverse effects on our well-being. Countless politicians have sacrificed their entire life’s work (not to mention their marriages) by indulging adulterous sexual impulses toward colleagues, staffers, prostitutes, and others over whom they have social or financial power. It not an overstatement to say that many problems of the 21st century, from school massacres to obesity to drug addiction, are influenced by the mismatch between our drive states and our uniquely modern ability to fulfill them at a moment’s notice.
Outside Resources
- Web: An open textbook chapter on homeostasis
- http://en.wikibooks.
 org/wiki/Human_Physiology/Homeostasis
org/wiki/Human_Physiology/Homeostasis - Web: Motivation and emotion in psychology
- http://allpsych.com/psychology101/motivation_emotion.html
- Web: The science of sexual arousal
- http://www.apa.org/monitor/apr03/arousal.aspx
- The ability to maintain homeostasis is important for an organism’s survival. What are the ways in which homeostasis ensures survival? Do different drive states accomplish homeostatic goals differently?
- Drive states result in the narrowing of attention toward the present and toward the self. Which drive states lead to the most pronounced narrowing of attention toward the present? Which drive states lead to the most pronounced narrowing of attention toward the self?
- What are important differences between hunger and sexual arousal, and in what ways do these differences reflect the biological needs that hunger and sexual arousal have been evolved to address?
- Some of the properties of sexual arousal vary across males and females.
 What other drives states affect males and females differently? Are there drive states that vary with other differences in humans (e.g., age)?
What other drives states affect males and females differently? Are there drive states that vary with other differences in humans (e.g., age)?
Vocabulary
- Drive state
- Affective experiences that motivate organisms to fulfill goals that are generally beneficial to their survival and reproduction.
- Homeostasis
- The tendency of an organism to maintain a stable state across all the different physiological systems in the body.
- Homeostatic set point
- An ideal level that the system being regulated must be monitored and compared to.
- Hypothalamus
- A portion of the brain involved in a variety of functions, including the secretion of various hormones and the regulation of hunger and sexual arousal.
- Lordosis
- A physical sexual posture in females that serves as an invitation to mate.
- Preoptic area
- A region in the anterior hypothalamus involved in generating and regulating male sexual behavior.
- Reward value
- A neuropsychological measure of an outcome’s affective importance to an organism.
- Satiation
- The state of being full to satisfaction and no longer desiring to take on more.
References
- Anand, B. K., & Brobeck, J. R. (1951). Hypothalamic control of food intake in rats and cats. The Yale journal of biology and medicine, 24(2), 123.
- Andersson, B. (1951). The effect and localization of electrical stimulation of certain parts of the brain stem in sheep and goats. Acta Physiologica Scandinavica, 23(1), 8–23.
- Ariely, D., & Loewenstein, G. (2006). The heat of the moment: The effect of sexual arousal on sexual decision making. Journal of Behavioral Decision Making, 19(2), 87–98
- Biderman, A. D. (1960). Social-psychological needs and “involuntary” behavior as illustrated by compliance in interrogation.
 Sociometry, 23(2), 120–147.
Sociometry, 23(2), 120–147. - Brendl, C. M., Markman, A. B., & Messner, C. (2003). The devaluation effect: Activating a need devalues unrelated objects. Journal of Consumer Research, 29(4), 463–473.
- Buck, R. (1999). The biological affects: A typology. Psychological Review, 106, 301–336.
- Easterbrook, J. A. (1959). The effect of emotion on cue utilization and the organization of behavior. Psychological Review, 66(3).
- Gawin, F. H. (1991). Cocaine addiction: psychology and neurophysiology. Science, 251(5001), 1580–1586.
- Giordano, L. A., Bickel, W. K., Loewenstein, G., Jacobs, E. A., Marsch, L., & Badger, G. J. (2002). Mild opioid deprivation increases the degree that opioid-dependent outpatients discount delayed heroin and money. Psychopharmacology, 163(2), 174–182.
- Greenberg, D.
 , Smith, G. P., & Gibbs, J. (1990). Intraduodenal infusions of fats elicit satiety in sham-feeding rats. American Journal of Physiology-Regulatory, Integrative, and Comparative Physiology, 259(1), 110–118.
, Smith, G. P., & Gibbs, J. (1990). Intraduodenal infusions of fats elicit satiety in sham-feeding rats. American Journal of Physiology-Regulatory, Integrative, and Comparative Physiology, 259(1), 110–118. - Heath, R. G. (1964). Pleasure response of human subjects to direct stimulation of the brain: Physiologic and psychodynamic considerations. In R. G. Heath (Ed.), The role of pleasure in behavior (pp. 219–243). New York, NY: Hoeber.
- Kow, L. M., & Pfaff, D. W. (1998). Mapping of neural and signal transduction pathways for lordosis in the search for estrogen actions on the central nervous system. Behavioural Brain Research, 92(2), 169–180
- Olds, J., & Milner, P. (1954). Positive reinforcement produced by electrical stimulation of septal area and other regions of rat brain. Journal of Comparative and Physiological Psychology, 47(6), 419.
- Panksepp, J.
 (2004). Affective neuroscience: The foundations of human and animal emotions (Vol. 4). New York, NY: Oxford University Press U.S.
(2004). Affective neuroscience: The foundations of human and animal emotions (Vol. 4). New York, NY: Oxford University Press U.S. - Rolls, E. T. (2000). The orbitofrontal cortex and reward. Cerebral Cortex, 10(3), 284-294.
- Teitelbaum, P. (1955). Sensory control of hypothalamic hyperphagia. Journal of Comparative and Physiological Psychology, 48(3), 156.
- Van Boven, L., & Loewenstein, G. (2003). Projection of transient drive states. Personality and Social Psychology Bulletin, 29, 1159–1168.
- Walker, P. (2014). Castaway's sea savvy could have helped him survive year adrift, says expert. The Guardian. Retried from http://www.theguardian.com/world/2014/feb/04/castaway-jose-salvador-alvarenga-survival-expert
- Zajonc, R. B. (1998). Emotions. In Gilbert, D. T., Fiske, S. T., & Lindzey, G. (Eds.), The handbook of social psychology (Vols.
 1 and 2, 4th ed., pp. 591–632). New York, NY: McGraw-Hill.
1 and 2, 4th ed., pp. 591–632). New York, NY: McGraw-Hill.
Authors
Creative Commons License
Drive States by Sudeep Bhatia and George Loewenstein is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.How to cite this Noba module using APA Style
Bhatia, S. & Loewenstein, G. (2022). Drive states. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/pjwkbt5hHow does the libido work?
The term libido is commonly used to describe sexual desire or desire for sexual activity. Modern medicine recognizes the importance of libido as one of the key indicators of overall health and quality of life. In the article we understand how the libido works, why it is for a person and why sometimes the libido changes.
Content
- Evolution and libido
- Which hormones regulate libido in women
- What governs male libido
- Neurotransmitters: libido in the head
- Why libido increases
- Why libido can decrease
- Note
Evolution and Libido
Although the libido today is influenced by many factors, from psychological to cultural, its nature is evolutionary in origin.
Sex drive is a common trait in the reproduction of mammals and birds. The sexual activity of many species varies depending on the sexual cycle, that is, from periodically repeating changes in the body of females from one ovulation to another. nine0025
The fact is that the probability of conception is not uniform, but varies depending on the phase of the cycle. Man, for example, belongs to polyestrous animals, that is, species in which sexual cycles are repeated throughout the year. And although a person can conceive offspring on any day, the probability of fertilization is higher precisely on the days of ovulation. Libido these days is also, as a rule, increased.
Fluctuating libido is a mechanism that allows you to increase the frequency of sexual intercourse on the most favorable days for conception. Libido is an important force of natural selection, which encourages us to reproduce with maximum efficiency and pass our genetic material to the next generations, that is, to win the evolutionary lottery. nine0025
nine0025
What hormones regulate libido in women
The main hormones that regulate sexual desire are sex hormones: estrogen, progesterone and testosterone. All three hormones are present in both male and female bodies. However, women have significantly less testosterone than men. Conversely, estrogen and progesterone are mostly female sex hormones.
In the first (follicular) phase of the menstrual cycle, several follicles grow and mature in the ovaries at once, the level of estrogen in the blood also increases. About a week before ovulation, a single dominant follicle is determined and continues to grow. The remaining follicles stop in their development and undergo the opposite - atresia. At the same time, the concentration of estrogen in the blood grows further, due to the production of the hormone by the dominant follicle. In the middle of the cycle, the follicle bursts, ovulation occurs - the release of the egg into the uterus through the fallopian tubes. After ovulation, estrogen levels gradually decrease. nine0025
nine0025
Experiments have shown that both men and women rate photographs of women's faces taken before ovulation as more attractive than photographs of the same women after ovulation.
Women's libido is also strongest around ovulation, when estrogen is at its peak.
In addition, estrogen plays an important role in women's health, energizes and enhances attractiveness.
After ovulation comes the second (luteal) phase of the menstrual cycle. In place of the bursting follicle, a corpus luteum is formed, which releases progesterone. If fertilization does not occur, then by the end of the menstrual cycle, the corpus luteum disintegrates, and progesterone levels fall. nine0025
Low estrogen levels and high progesterone levels at the end of the cycle lead to a decrease in libido. With the onset of menstruation, sexual desire increases again.
However, due to the fact that both progesterone and estrogen levels simultaneously decrease approximately one week before the end of the cycle, PMS symptoms may occur: swelling, bloating, lethargy, mood swings.
In women who take hormonal contraceptives, hormone fluctuations are less pronounced, so changes in libido are not so noticeable. nine0025
Some women who take oral contraceptives may not notice any change in sex drive, while others report decreased libido as an unwanted side effect.
What governs male libido
The main male sex hormone is testosterone. Its fluctuations can affect the level of sexual desire. Thus, a decrease in testosterone is associated with low libido.
But if in women hormonal fluctuations are extended for a long period (about a month), then in men changes occur more often: testosterone levels are usually elevated in the morning, and decrease in the evening. Therefore, sexual desire is also often higher in the morning and lower late in the evening. In addition to daily fluctuations, testosterone levels also change throughout life, reaching a maximum in adolescence with a gradual decrease after 30 years. nine0025
nine0025
Testosterone is not the only fuel that fuels the male libido. Estradiol, the predominant form of estrogen, also affects sex drive.
In addition to testosterone, estradiol levels also affect libido. This is partly due to the fact that estradiol affects the areas of the brain that control sexual behavior, and partly due to the role of the hormone in the regulation of testosterone levels.
Sex hormones, their receptors and the aromatase enzyme are in a complex balance that regulates sexual behavior, erection, libido, as well as mood and mental state. nine0025
Neurotransmitters: libido in the head
The exact role of neurotransmitters, active brain chemicals, in sexual desire is not fully understood. But it can be noted that one of the “controlling” libido is a neurotransmitter and the hormone oxytocin. Oxytocin is called the hormone of love and affection because it is responsible for the positive emotions that a person experiences during the period of falling in love and at the peak of sexual desire. Oxytocin rises with arousal and orgasm.
Oxytocin rises with arousal and orgasm.
nine0024 Oxytocin is the hormone of love and affection. In women, nipple stimulation can cause a surge of oxytocin followed by arousal. In experiments on male rats, oxytocin has been shown to cause erection and ejaculation, and also increase sperm count.
One study showed that treating a patient with oxytocin nasal spray had a positive effect on libido, erection and orgasm. A little later, the successful experiment was repeated on 29 heterosexual couples. Participants reported that the introduction of the "love hormone" increased the intensity of orgasm and the satisfaction of partners after intercourse. In addition, participants were able to better share sexual desires and empathize with partners. nine0025
The effects were more pronounced in men. Men also noted higher levels of sexual satiety. However, the effect of treatment varied from small to moderate.
Another neurotransmitter that can influence libido is dopamine. Dopamine plays an important role in emotional behavior, attention, memory, reward and pleasure. Dopamine can affect testosterone levels, and testosterone can affect dopamine.
Dopamine plays an important role in emotional behavior, attention, memory, reward and pleasure. Dopamine can affect testosterone levels, and testosterone can affect dopamine.
The neurotransmitter dopamine also affects libido. Sex hormones create conditions for increasing the synthesis of dopamine, and its release leads to an increase in sexual desire, by activating the right areas of the brain. nine0025
In men, one of the key areas of the brain responsible for sexual behavior is the medial preoptic area. Injections of substances that mimic the effects of dopamine into such an area in rats lead to an increase in sexual activity.
An increase in libido can also occur after administration of the dopamine precursor, L-DOPA. Conversely, the introduction of molecules that block the work of dopamine leads to a decrease in libido.
Why libido increases
Hypersexuality due to various causes is diagnosed in approximately 2% of the population. An excessively high libido can be caused by:
An excessively high libido can be caused by:
- High levels of mood-regulating neurotransmitters such as dopamine and serotonin.
- A side effect of certain drugs (including those that affect dopamine levels).
- Damage to areas of the brain involved in sexual behavior (particularly in epilepsy).
Persistent sexual arousal that causes discomfort is a sign of hypersexual disorder. nine0025
There is a noticeable difference between high and too high libido. The cause for concern is the increase in sexual desire to a level that is out of control and interferes with daily life.
Why libido can decrease
A decrease in sexual desire is more common than an increase in it. Clinical criteria for diagnosing low libido have not been established, as there is a wide range of what is considered "low": normal sexual desire for one person may seem high or low for another. However, the following symptoms are commonly mentioned:
- Loss of desire for a partner.

- Disinterest in masturbation.
- Few or no sexual fantasies.
- Anxiety about lack of interest in sex.
Persistent reluctance to have sex may be a sign of hypoactive sexual desire disorder - anaphrodisia.
Hormonal disorders are a common cause of anaphrodisia. Libido may decrease in response to changes in estrogen, progesterone, and testosterone levels. Testosterone is the prime suspect. nine0025
In the absence of testosterone in men, libido is low, while treatment of testosterone deficiency leads to normalization of libido.
Women may also experience decreased sexual desire due to low testosterone, but decreased estrogen is more likely to be the cause. This is what happens during menopause. In a 2008 study, 27% of premenopausal women and 52% of menopausal women experienced low sex drive.
In addition to hormonal fluctuations, anaphrodisia can be caused by:
- Stress,
- Diabetes,
- High blood pressure,
- Certain medications, especially antidepressants,
- Alcohol abuse,
- Smoking,
- Underuse of drugs
In most cases, restoring libido can be achieved by making healthier lifestyle changes and reducing stress levels. Sometimes drug therapy is required to normalize hormonal balance. nine0025
Sometimes drug therapy is required to normalize hormonal balance. nine0025
Note
- Libido has an evolutionary origin. It helps mammals, including humans, maximize the chance of having offspring.
- The female libido is mainly dependent on progesterone and estrogen. In the first phase of the cycle before ovulation, there is a lot of estrogen, and little progesterone - libido is increased. In the second phase, estrogen becomes less and progesterone increases, so libido decreases.
- Taking oral contraceptives may affect a woman's libido. nine0008
- Male libido is primarily controlled by testosterone. The highest level of the hormone is in adolescence, and after 30 years it gradually decreases. Following testosterone, libido may also decrease.
- In addition to hormones, sexual desire is influenced by neurotransmitters: dopamine and oxytocin.
- Increased or decreased libido are relative concepts. There are no single indicators for determining the "normality" of a libido: what is a "normal" sexual desire for one person may seem high or low for another.
 nine0008
nine0008 - Decreased libido - anaphrodisia - may be associated with stress, hormonal imbalance, bad habits, taking certain medications.
- Increased libido may be a symptom of a hypersexual disorder or may occur after certain drugs, brain injury or damage, or neurotransmitter imbalance.
- If the change in libido causes discomfort, you should consult a doctor.
Quality of life, high libido, good mood are in many cases indicators of good health. The Atlas Genetic Test helps you take care of yourself, understand your predisposition to multifactorial diseases, and improve your health with personalized test results. nine0182
Atlas Blog Articles about attraction:
A conversation with an expert. How to enjoy sex?
Sleep, diet and giving up your smartphone: what habits will make you happier?
- Roslan et al. The Bio-Psycho-Social Dimension in Women's Sexual Desire: 'Argumentum ad novitatem'.
 2019
2019 - Motta-Mena, Puts. Endocrinology of human female sexuality, mating, and reproductive behavior. 2016
- Roberts et al. Female facial attractiveness increases during the fertile phase of the menstrual cycle. 2004
- Rastrelli et al.Testosterone and sexual function in men.2018
- Oti et al. Systemic effects of oxytocin on male sexual activity via the spinal ejaculation generator in rats.2021
- MacDonald, Feifel. Dramatic improvement in sexual function induced by intranasal oxytocin. 2012
- Shoemaker. Male Libido, Testosterone, & Neurotransmitters. 2019
- Grazzotin. Libido: the biological scenario. 2000
- Montjero et al. Sexual side effects of antidepressant and antipsychotic drugs. 2015
- Shulster et al. The role of estradiol in male reproductive function. 2016
- Tuijl et. al. Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior? 2020
- West et.
 al. Prevalence of low sexual desire and hypoactive sexual desire disorder in a nationally representative sample of US women.2008
al. Prevalence of low sexual desire and hypoactive sexual desire disorder in a nationally representative sample of US women.2008 - Behnia et. al. Differential effects of intranasal oxytocin on sexual experiences and partner interactions in couples. 2014
- Dominguez, Hull. Dopamine, the medial preoptic area, and male sexual behavior.2005
What is libido and how to increase it
Libido is a sexual desire, a desire for some kind of sexual activity. These may include thoughts, fantasies of a sexual nature, and a desire for sex. It may precede sexual contact or occur during the process.
Often people who experience difficulties with a lack or excess of libido find themselves alone with the problem and do not dare to start solving it. We asked an endocrinologist and a psychotherapist to talk about libido in such a way that it was clear how to approach this issue. nine0025
.
Advertising on RBC www.adv.rbc.ru
Georgy Mskhalaya, endocrinologist, andrologist at the European Medical Center
Natalya Rivkina, psychiatrist, psychotherapist, head of the clinic for psychiatry and psychotherapy at the European Medical Center Freud. According to Freud, the libido is the drive to life, the drive to change and continue, it is the very manifestation of life. The second concept of this theory is mortido. Mortido is the force that limits the libido, the drive towards a static state, towards death as the primary state from which the inanimate was introduced into the state of life. nine0025
According to Freud, the libido is the drive to life, the drive to change and continue, it is the very manifestation of life. The second concept of this theory is mortido. Mortido is the force that limits the libido, the drive towards a static state, towards death as the primary state from which the inanimate was introduced into the state of life. nine0025
The main idea of the theory is that a person has an energy that is primarily and naturally realized through libido, that is, a person strives for life and its continuation. But if this energy is not realized through libido, then it turns into mortido and the opposite effect begins, the desire for death. Later, destrudo mechanisms were described - patterns of behavior that realize the desire for death and destroy a person.
How to measure libido
George Mskhalaya: As such, there is no test for libido in endocrinology. Usually we ask our patients at the reception how often they have sexual intercourse, whether there is a sexual desire, how often a person becomes the initiator of sexual relations. For example, it may be that a person has sexual contact regularly three times a week, but in 100% of cases the partner is the initiator. This is important. Another significant aspect when we talk about libido is getting an orgasm. We ask whether there are orgasms at all, how often, whether a person considers his orgasms to be bright, whether there is a decrease in the intensity of orgasms. The answers to these questions help us understand whether we are dealing with endocrinological disorders. nine0025
For example, it may be that a person has sexual contact regularly three times a week, but in 100% of cases the partner is the initiator. This is important. Another significant aspect when we talk about libido is getting an orgasm. We ask whether there are orgasms at all, how often, whether a person considers his orgasms to be bright, whether there is a decrease in the intensity of orgasms. The answers to these questions help us understand whether we are dealing with endocrinological disorders. nine0025
© Shutterstock
Natalya Rivkina: In our practice, we use clinical interviews to assess libido, collect a patient's history and analyze it.
Methods for assessing female libido and sexuality in psychotherapy can be used:
- vector scale for determining the sexual constitution, developed and tested for women by Irina Botneva from the Moscow Research Institute of Psychiatry;
- questionnaire of sex attitudes of the psychologist Hans Eysenck; nine0008
- Sexual Temperament Questionnaire by Eric Jansen and John Bancroft of the Kinsey Institute;
- Sexual Addiction Test by Patrick Karnes, a specialist in the study of sexually addictive behavior.
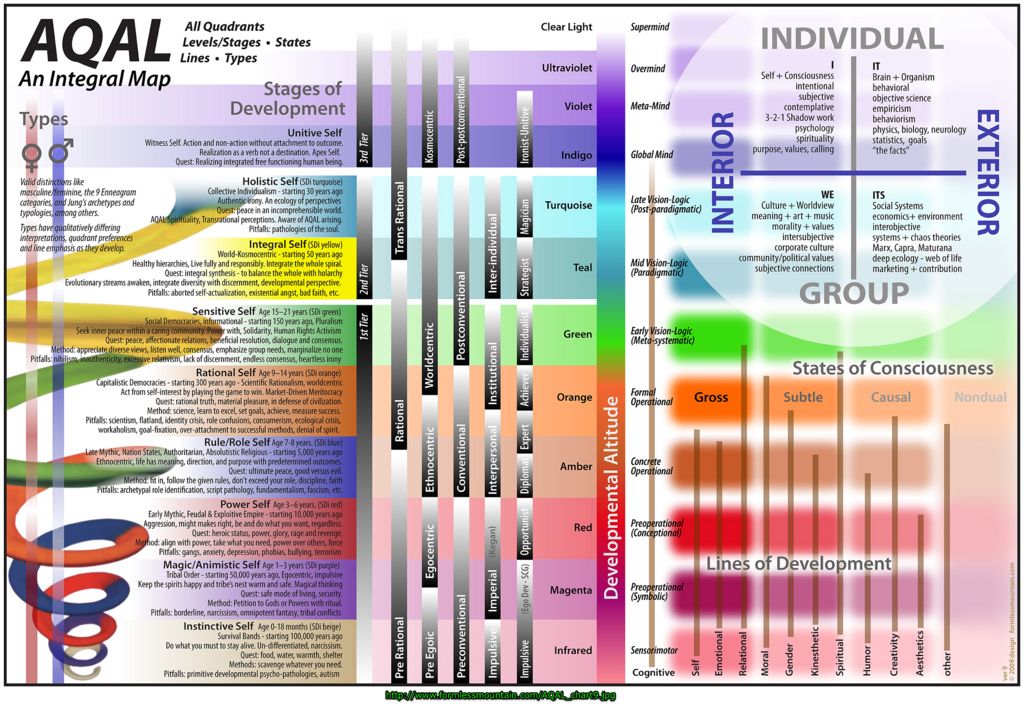
For men:
- vector scale for determining the sexual constitution, developed and tested for men by one of the first domestic sexologists Georgy Vasilchenko from the Moscow Research Institute of Psychiatry; nine0008
- questionnaire of sex attitudes of the psychologist Hans Eysenck;
- Sexual Addiction Test by Patrick Carnes.
What affects libido
George Mskhalaya: Sexual desire is a multifactorial process: hormones, lifestyle, and psychology are involved here. Of course, the role of hormones in the formation of attraction is great: first of all, these are testosterone and estrogens. Both of these hormones are important for both men and women. It is necessary to understand the mechanism of synthesis of these hormones: all female sex hormones (estrogens) are formed in our body from male (androgens). nine0025
Female hormones are not directly synthesized in the body. Therefore, if the synthesis of male hormones is disrupted, then the synthesis of female hormones is automatically disrupted, since they have nothing to form from. It is a mistake to believe that only testosterone is responsible for attraction. There are studies and data that show that if we artificially block the transition of male sex hormones to female ones, then this negatively affects libido. That is, testosterone is high, estrogens are low, and against this background, there is a decrease in sexual desire. Therefore, we always evaluate the level of all sex hormones, regardless of the gender of patients. nine0025
It is a mistake to believe that only testosterone is responsible for attraction. There are studies and data that show that if we artificially block the transition of male sex hormones to female ones, then this negatively affects libido. That is, testosterone is high, estrogens are low, and against this background, there is a decrease in sexual desire. Therefore, we always evaluate the level of all sex hormones, regardless of the gender of patients. nine0025
Prolactin, a pituitary hormone, is also extremely important: its increase above the reference values will reduce libido. In addition, we evaluate the level of thyroid hormones. Lack of thyroid hormones provokes an increase in prolactin levels, which in turn will negatively affect libido.
© Shutterstock
We definitely look for some general somatic pathology: for example, iron deficiency anemia, which can make you feel unwell, chronic fatigue, fatigue, loss of energy, which will definitely also affect libido. nine0025
Natalia Rivkina: A person's psychological well-being and comfort have a strong influence on libido. By well-being we mean a complex of factors of human interaction with oneself, the world around and people. For example, a man may be hormonally and erection-free, but his libido is reduced or even absent because he has severe work stress or personality problems with his current partner. Or, with absolutely normal organic indicators, a girl may have a reduced libido as a result of a depressive state. nine0025
By well-being we mean a complex of factors of human interaction with oneself, the world around and people. For example, a man may be hormonally and erection-free, but his libido is reduced or even absent because he has severe work stress or personality problems with his current partner. Or, with absolutely normal organic indicators, a girl may have a reduced libido as a result of a depressive state. nine0025
Here is a list of psychological causes leading to a decrease in libido that I encounter in my practice:
- mental and physical overwork;
- prolonged sexual abstinence;
- depressive or depressed emotional state;
- failure to meet key human needs;
- avoiding, tabooing the topics of sex and intimacy during the period of a person's growing up on the part of his parents; nine0007 distrust of the partner;
- disappointment in a partner;
- low self-esteem;
- fear of not pleasing a partner;
- bad sexual experience;
- excessive expectations from sexual contact that are not justified;
- negative experience of past relationships, fear of emotional attachment to a partner;
- loss of thrill from sex is typical for couples who have been together for a long time; nine0008
- acute conflict situations with a partner.
How to increase libido
George Mskhalaya: First of all, you need to contact a specialist, to exclude the natural causes of a decrease in libido. For example, a chronic sleep disorder that prevents a person from recovering will have an extremely negative effect on libido. Working at night can disrupt the circadian rhythm of hormone production, which can also cause complaints. There are no folk methods to increase sexual desire. From what does not require doctor's prescriptions, the recommendations will be quite standard: get enough sleep, reduce stress, increase physical activity. nine0025
Natalia Rivkina: Decreased desire can become a symptom of depression, stress, mental and physical strain, intrapersonal problems, interpersonal conflicts. To correct a reduced libido caused by psychological factors, a psychotherapist can use the methods of cognitive-behavioral psychotherapy, systemic psychotherapy, body-oriented therapy, psychoanalysis and emotionally focused therapy.
© Shutterstock
Are there products that increase libido
George Mskhalaya: This is pure myth. There is no proven effectiveness for any products in combating reduced libido. Eat oysters, avocados and ginger for pleasure, but if there is a task to adjust the level of sexual desire, then it is better to immediately contact a specialist.
How to reduce libido
George Mskhalaya: If a person has a consistently high libido, he is satisfied with it and finds ways to realize his sexual desire, then there is no need to reduce anything. This is not a pathology. If a person has a hypertrophied sexual desire that he cannot control, it gives him discomfort and reduces the quality of life, then he should consult a psychiatrist. nine0025
Natalya Rivkina: Abnormally increased libido may indicate some mental disorders and conditions, for example:
- inferiority complex, neurotic experiences;
- manic syndrome;
- Concealed homosexuality;
- pathology of the brain: traumatic brain injury, tumors of the hypothalamic region, lesions of diencephalic structures;
- hormonal dysfunctions.
 nine0021
nine0021
It is important to note that the decrease or increase in attraction must be considered in dynamics and take into account episodes of abrupt changes in attraction and their context. If a person is prone to low temperament, then this does not indicate the presence of symptoms of depression or problems, and vice versa. It is not considered a problem to lose attraction to a particular partner, but to maintain attraction in general. Normally, libido does not cause inconvenience to a person and his partner, does not have sharp rises or falls and corresponds to the external situation. nine0025
Can libido go away forever? The main thing is to act not with oysters, but with scientific methods.
When libido returns after childbirth
George Mskhalaya: Everything is very individual. Not all libido decreases after childbirth. But this is not uncommon either. During pregnancy and after childbirth, there is an active production of prolactin, a hormone that stimulates lactation in mothers.