Pristiq vs prozac
Pristiq Tapering Help | Desvenlafaxine Weaning & Titration Support
Alternative to Meds News & Blog Articles
Prozac Crossover Method for Pristiq Weaning
The short half-life of Pristiq and the fact that it is an SNRI may warrant considering a crossover to Prozac, and then tapering off the Prozac due to its longer half-life. Pristiq is acting on both serotonin and norepinephrine levels. Prozac only addresses serotonin. So the crossover will involve a dip in norepinephrine support and Prozac will likely provide the serotonin support. In our experience, a sudden norepinephrine drop is much more tolerable than a sudden serotonin drop.
Methods described here including the below need to be talked about with a prescriber sensitive to your situation prior to attempting.
Prozac Crossover Methods Should take into account:
- Medication-sensitive persons may have difficulty switching to a different medication. Stay in close touch with your prescribing physician to avoid complications.
- Before weaning down off Pristiq, your physician may want to induct a small dosage of Prozac to test your tolerance, for example, by cutting the 10mg green elliptical in half to get 5mg.
- Your prescriber may advise you to start 5mg Prozac for one week (one-half tablet) while still taking Pristiq.
- The dosing ranges for Prozac and Pristiq are not equivalent so some guidance from a medical professional is needed to get your situation mapped out. But an example might be if you are taking 50mg Pristiq, drop to 25mg Pristiq, and go up to a total of 10-15mg Prozac.
- You can gauge how long to do this step, by how symptomatic you are after one week or two weeks, etc. If you are still symptomatic, discuss this with your doctor who may advise you to continue for another week at this step.
- Consult with your physician and If the above was tolerated, then discuss if your doctor feels you are ready to convert over to all Prozac (in the example this would be 20-30mg).
 This would be followed by another rest period of 1-2 weeks before any changes.
This would be followed by another rest period of 1-2 weeks before any changes. - From here, look at the Prozac tapering page with your doctor and ask them to use those instructions for your guide
- Your doctor may advise putting you back on your original Pristiq dose if the above is not tolerated. The physician would generally just do a straight taper off the Pristiq in this case.
- Be aware that by switching over to Prozac, you are going from an SNRI to an SSRI. Your physician may agree that generally, Prozac withdrawal is easier to manage than Pristiq as it does not carry the norepinephrine aspect (stimulatory) of Pristiq. This may result in fatigue. But your doctor may advise that Prozac may mitigate harsh effects such as brain zaps that are more associated with Pristiq.
Is Pristiq Prescribed Only to Women?
Although Pristiq (desvenlafaxine) was originally marketed mostly to target women for menstrual or menopausal issues like “hot flashes,” with its pretty-sounding name and cute commercials featuring wind-up dolls, lots of soft pink and pastel colors, and gentle music, prescribing the drug today is not limited to the female market at all.
There are no limits on who may be prescribed Pristiq (desvenlafaxine) except not to children or the under-25 age range due to the high risk of suicide. Among the elderly population, antidepressants are known to be outrageously overprescribed, and the number of complications due to multiple medications, co-occurring disorders, and medical conditions makes the problem exponentially worse.10 It is unfortunate that though general medical practitioners are highly skilled technicians in their bio-physical healing arena, they are less skilled in nutritional aspects of improving health, and are, tragically, wholly untrained in treating mental health issues, let alone within a holistic or drug-free context.
What is Pristiq Prescribed to Treat?
In 2007, the FDA approved Pristiq to treat MDD or major depressive disorder in adults.12
Pristiq has also been prescribed off-label for the following:
- depression in adolescents 13
- Fibromyalgia
- hot flashes for women in menopause
- women’s menstrual difficulties
- chronic pain
- anxiety
- bipolar
- neuropathy associated with diabetes
A wide range of populations and age ranges have been prescribed Pristiq beyond its FDA approval for the treatment of a wide array of conditions. This may have resulted in a significant number of patients for whom Pristiq did not provide the relief they were seeking, with the additional problem of not knowing how to get off Pristiq safely.
This may have resulted in a significant number of patients for whom Pristiq did not provide the relief they were seeking, with the additional problem of not knowing how to get off Pristiq safely.
Side Effects That Lead People to Wanting Pristiq Tapering Help
Pristiq tapering would resolve fears about health issues related to the drug. A 2012 adverse reaction report (among several similar) lists 36 suicides and deaths attributed to Pristiq for that year.1 This report often omits the ages but includes both males and females. The physician attending the patient at death listed Pristiq, and sometimes multiple antidepressants as the cause of death from suicide, renal failure, hepatic failure, thrombocytopenia, and other drug-induced conditions. Cardiac arrest and serotonin syndrome accounted for other deaths reported in the study of adverse reactions to Pristiq and other SNRI antidepressants. These deaths raise concerns.
Except in the case of serotonin syndrome or other medical emergency situations as noted above, Pristiq taper protocols should be as gradual as possible. Only in the case of serotonin syndrome, Stevens-Johnson syndrome, dropping sodium levels, or other major life-threatening reactions such as seizures, skin eruptions, cardiac events, etc., would a physician be justified in calling for immediate Pristiq cessation.
Only in the case of serotonin syndrome, Stevens-Johnson syndrome, dropping sodium levels, or other major life-threatening reactions such as seizures, skin eruptions, cardiac events, etc., would a physician be justified in calling for immediate Pristiq cessation.
Emergency treatment for serotonin syndrome or Steven-Johnson syndrome, or other life-threatening adverse events, is possible only in a hospital setting with an emergency ward, critical or intensive care unit, and trained emergency staff immediately on hand to keep the patient alive if possible.
Those caring for or living with the person should also be apprised of the possibility of these types of worst-case scenarios, and know exactly what to do should they occur. A word of caution: some VOIP phone lines do not have 911 access. It is a good practice to work out an alternative plan so as not to delay access to an ambulance if one is ever needed.
CAUTION: Pristiq Timed-release …
There is an additional complication with exactly how to gradually withdraw from PristiqXR because it is a timed-release medication. Like virtually all other antidepressants, the side effects of Pristiq can be quite uncomfortable and harsh, and extremely hard to tolerate, which may lead to the decision to quit taking it. But trying to quit Pristiq gradually may not be as straightforward as it is for drugs that are not time-release formulations.
Like virtually all other antidepressants, the side effects of Pristiq can be quite uncomfortable and harsh, and extremely hard to tolerate, which may lead to the decision to quit taking it. But trying to quit Pristiq gradually may not be as straightforward as it is for drugs that are not time-release formulations.
The FDA recommends gradual Pristiq cessation whenever possible and acknowledges that abruptly getting off Pristiq or another SNRI medication is associated with potential patient risk. FDA warnings are clear that abrupt Pristiq cessation can have disastrous health impacts.2,7
But no directions are provided as to how exactly to gradually reduce a timed-release pill that only comes in 50mg and 100mg doses, and where the maximum daily dose is 100mg. Clearly, there is an oversight and a huge gap here in giving instruction and guidance to either prescribing physicians or their patients. The task of withdrawal from a timed-release antidepressant is somewhat like figuring out the Rubik’s cube before YouTube.
Alternative to Meds Center’s Physicians Are Trained in How to Quit Pristiq Safely
According to the very apparent absence of available literature, it is clear that there is little direction given to medical practitioners to assist their patients in how to get off Pristiq. Antidepressant tapering and tapering SNRIs or similar medications is not part of the medical training given to doctors in school before they start practicing, nor is it provided by drugmakers or even the FDA, as mentioned above.
Thankfully, Alternative to Meds Center utilizes fully licensed psychiatrists, and other fully licensed and certified doctors, nurses, and practitioners who ARE trained in safe Pristiq tapering protocols. One could say that Alternative to Meds Center has “cracked the code” for how to get off Pristiq with minimum discomfort and maximum comfort and safety. Contact the center for more details on the protocols designed for safe Pristiq tapering.
The Best Solution for Safe Tapering from Pristiq
Alternative to Meds Center provides the finest help with how to get off Pristiq in a nurturing in-patient setting. The center’s Pristiq cessation program (alternatives and withdrawal) has overcome the difficulty of administering gradually reduced dosage and indeed is completely oriented toward patient safety and comfort. For over a decade and a half, Alternative to Meds Center has assisted thousands of clients stopping Pristiq and other medications safely, gently, and comfortably.
The center’s Pristiq cessation program (alternatives and withdrawal) has overcome the difficulty of administering gradually reduced dosage and indeed is completely oriented toward patient safety and comfort. For over a decade and a half, Alternative to Meds Center has assisted thousands of clients stopping Pristiq and other medications safely, gently, and comfortably.
Our programs are administered using techniques that allow for a safe and gradual withdrawal from Pristiq despite it being a timed-release medication. Program steps are individually tailored for each client which benefits the client’s overall personal health. Discovering and eliminating root causes for mental distress, depression, fatigue, sleep issues, insomnia, anxiety, or other undesirable conditions is what makes it possible to elevate and improve natural mental health. That is our prime goal which we offer to our clients, and in so doing, likely reduce or eliminate entirely the need for prescription medications.
Programs implement a blend of many protocols such as neurotoxin testing and removal, nutritional deficiency testing and correction using both oral and IV infusions, and holistic adjunct therapies designed for enhanced patient comfort, a better quality of sleep, more energy, and a brightened mood. We use many additional program components such as restoring the microbiome, life coaching, relaxation therapies, mineral baths, craniosacral massage, nebulized glutathione treatments, prescribed dietary changes, and more, under the oversight of our holistic practitioners including our fully licensed holistic psychiatrist. You are invited to view our services overview pages for more details on the services provided at the center for Pristiq tapering and improving mental health holistically.
Pristiq tapering treatment offered at Alternative to Meds Center is an investment in you for your health-focused and sustainable recovery.
A Guide To Desvenlafaxine Alternatives
Pristiq is an SNRI (serotonin-norepinephrine reuptake inhibitor) that is effective in the treatment of depression and anxiety. While many patients find Pristiq medication effective, some people don’t react to the drug well and require alternatives. Antidepressants that can act as substitutes for desvenlafaxine differ by type and indications. Only a healthcare professional can determine which medication is best for a person. However, it’s always beneficial for the patient to learn about their options.
While many patients find Pristiq medication effective, some people don’t react to the drug well and require alternatives. Antidepressants that can act as substitutes for desvenlafaxine differ by type and indications. Only a healthcare professional can determine which medication is best for a person. However, it’s always beneficial for the patient to learn about their options.
This article will contrast Pristiq vs Effexor and other antidepressants to determine which one can be a suitable substitute. Readers will also discover various factors to consider when switching medications. Finally, other antidepressants that are safe for everyone will be examined.
Alternative Medications To Desvenlafaxine
For some patients, it is necessary to find alternatives to the drug due to the Pristiq side effects or unavailability of the medication. Switching from one antidepressant to another requires continuous medical attention. Patients should always discuss treatment changes with their doctor before implementing them.
The Most Common Alternative Medications to Desvenlafaxine Include:
- Zoloft
- Effexor
- Prozac
- Cymbalta
- Lexapro
- Paxil
- Celexa
- Wellbutrin
- Viibryd
- Fetzima
- Khedezla
- Trintellix
All these drugs have their pros and cons which should be considered before administration. Some drugs may have adverse effects during the withdrawal phase. Therefore, patients should be monitored for signs and symptoms of Pristiq withdrawal. Also, doctors may decide to continue with a particular medication if the side effects are manageable. Thus, patients should not hesitate to report any changes during treatment.
Pristiq vs Effexor
Comparing Pristiq vs Effexor, both medications are SNRIs and have a similar mechanism of action. Also known as Venlafaxine, Effexor works by increasing serotonin in the brain while Pristiq also enhances serotonin levels.
Also known as Venlafaxine, Effexor works by increasing serotonin in the brain while Pristiq also enhances serotonin levels.
The Table Below Compares Pristiq vs Effexor and Summarizes the Similarities and the Differences Between Both Drugs.
| DRUG BRAND NAME | PRISTIQ | EFFEXOR |
| GENERIC NAME | DESVENLAFAXINE | VENLAFAXINE |
| DRUG CLASS | SEROTONIN-NOREPINEPHRINE REUPTAKE INHIBITOR (SNRI) | SEROTONIN-NOREPINEPHRINE REUPTAKE INHIBITOR (SNRI) |
| AVAILABILITY OF GENERIC VERSIONS | YES | YES |
| APPROVED AGE OF USE | 18 YEARS AND ABOVE | 18 YEARS AND ABOVE |
| TREATMENT LENGTH | 4 – 9 MONTHS | 6 – 12 MONTHS |
| PRESCRIPTION FORMS STANDARD DOSAGE | 25 MG TABLETS, 50 MG TABLETS, 100 MG TABLETS | 37. 5 MG CAPSULES, 5 MG CAPSULES, 75 MG CAPSULES, 100MG CAPSULES |
| RISK OF WITHDRAWAL OR OVERDOSE | YES | YES |
| INSURANCE COVERAGE | YES | YES |
Both drugs are not limited to their use as antidepressants but have other off-label functions. Though approved for use in treating depression, Pristiq is used off-label in the treatment of general anxiety disorder. Venlafaxine is also used off-label to treat attention deficit hyperactivity disorder, diabetic neuropathy, complex pain syndrome, etc. However, consult your physician before attempting the off-label uses to avoid any health consequences.
Differences Between Pristiq And Effexor
Effexor is one of the best-known substitutes. Both medicines are made by the same company and are of the same drug class, SNRIs. Thus, they both have similar mechanisms of action – increasing serotonin levels in the brain. However, there are slight differences in their uses. As an antidepressant, Desvenlafaxine’s specialty is treating Major Depressive Disorder. Venlafaxine, on the other hand, treats Major Depressive Disorder, Generalized Anxiety Disorder, panic disorder, and social anxiety disorder. Also, during a clinical trial, it was discovered that both antidepressants were efficacious, but Pristiq users had less nausea.
As an antidepressant, Desvenlafaxine’s specialty is treating Major Depressive Disorder. Venlafaxine, on the other hand, treats Major Depressive Disorder, Generalized Anxiety Disorder, panic disorder, and social anxiety disorder. Also, during a clinical trial, it was discovered that both antidepressants were efficacious, but Pristiq users had less nausea.
Pristiq vs Effexor Side Effects Comparison
Comparing Desvenlafaxine with Effexor it can be concluded that both medications have similar side effects. The side effects of Desvenlafaxine include insomnia, dizziness, excess sweating, nausea, sleepiness, and male sexual problems. Venlafaxine’s side effects include dry mouth, excessive sweating, dizziness, dry mouth, sexual problems, constipation, and decreased appetite. When these side effects occur, report immediately to a health professional for prompt attention.
Switching From Pristiq To Effexor
A doctor may recommend switching between two antidepressants if the initial drug is not effective. Studies indicate that one in three persons responds to depression treatment. So if a patient is treatment-resistant, it is time to either increase the dose or switch medications. Another reason is when the patient reacts adversely to the first antidepressant. Since the main active substance in Effexor is unprocessed, a person can react to the two drugs differently. Some patients report more severe side effects that do not go away after the initial period of adjustment. Also, switching from desvenlafaxine to Effexor requires medical attention to avoid withdrawal symptoms.
Studies indicate that one in three persons responds to depression treatment. So if a patient is treatment-resistant, it is time to either increase the dose or switch medications. Another reason is when the patient reacts adversely to the first antidepressant. Since the main active substance in Effexor is unprocessed, a person can react to the two drugs differently. Some patients report more severe side effects that do not go away after the initial period of adjustment. Also, switching from desvenlafaxine to Effexor requires medical attention to avoid withdrawal symptoms.
Other Desvenlafaxine Alternatives
There are other alternatives of desvenlafaxine that are equally efficient. These medications can treat depression and its symptoms if Pristiq causes adverse reactions or does not work. However, these drugs can have serious side effects as well. So, it is better to consult a health professional to determine which alternative best suits the situation. This is to avoid future health complications. Here are some options of Desvenlafaxine that one can consider:
Here are some options of Desvenlafaxine that one can consider:
Pristiq vs Zoloft
Zoloft is another alternative to Desvenlafaxine. It belongs to the drug class of selective serotonin reuptake inhibitors (SSRIs). It works by increasing serotonin, a naturally occurring chemical in the brain responsible for stabilizing mood and feeling of happiness. Zoloft can be used to treat panic disorder, PTSD, and social anxiety as well as depression while Desvenlafaxine treats major depressive disorder. The side effects of Pristiq vs Zoloft are similar which include nausea, dry mouth, insomnia, fatigue, increased sweating, and restlessness. It is also one of the few Desvenlafaxine pediatric alternatives, available for children under 18 with obsessive-compulsive disorder.
Pristiq vs Lexapro
Lexapro is an antidepressant that treats the symptoms of major depressive disorder and generalized anxiety disorder. It is a selective serotonin reuptake inhibitor that is usually incredibly well-tolerated. Its mechanism of action is to block the reuptake of serotonin into the presynaptic neuron. This leads to an increase in serotonin levels. This drug can become a good substitute for the medication if a person experiences too many adverse effects of desvenlafaxine. Comparing the efficacy of Pristiq vs Lexapro, it was concluded that both medications had no significant advantage over the other. However, Lexapro seems to be a better choice if a patient suffers from depression and anxiety since it is used to treat both conditions. Contrasting the side effects of both drugs, one can conclude that they are similar. These include excessive sweating, headaches, dry mouth, insomnia, fatigue, and restlessness.
Its mechanism of action is to block the reuptake of serotonin into the presynaptic neuron. This leads to an increase in serotonin levels. This drug can become a good substitute for the medication if a person experiences too many adverse effects of desvenlafaxine. Comparing the efficacy of Pristiq vs Lexapro, it was concluded that both medications had no significant advantage over the other. However, Lexapro seems to be a better choice if a patient suffers from depression and anxiety since it is used to treat both conditions. Contrasting the side effects of both drugs, one can conclude that they are similar. These include excessive sweating, headaches, dry mouth, insomnia, fatigue, and restlessness.
Pristiq vs Viibryd
Viibryd can be a substitute for desvenlafaxine in cases when patients don’t react well to the latter. Viibryd has a different mechanism of action than most antidepressants do, combining a selective serotonin reuptake inhibitor and a partial agonist of the 5-HT1A receptor. Desvenlafaxine, on the other hand, is a serotonin-norepinephrine reuptake inhibitor. Both medications are equally potent for treating depression. Comparing the side effects of Pristiq vs Viibryd, both drugs seem to have similar adverse health effects with some differences. Common side effects of both medicines include nausea, dry mouth, vomiting, and insomnia. However, severe side effects of Viibryd are suicidal thoughts, aggressive or violent behavior, seizures or convulsions, etc.
Desvenlafaxine, on the other hand, is a serotonin-norepinephrine reuptake inhibitor. Both medications are equally potent for treating depression. Comparing the side effects of Pristiq vs Viibryd, both drugs seem to have similar adverse health effects with some differences. Common side effects of both medicines include nausea, dry mouth, vomiting, and insomnia. However, severe side effects of Viibryd are suicidal thoughts, aggressive or violent behavior, seizures or convulsions, etc.
Pristiq vs Wellbutrin
Wellbutrin is another effective alternative antidepressant for Desvenlafaxine. However, it belongs to a different group of antidepressants known as norepinephrine-dopamine reuptake inhibitors. Thus, its MOA is different. Wellbutrin treats major depressive disorder by blocking the reuptake of norepinephrine, dopamine, and serotonin. This action leads to the increase of these neurotransmitters which helps to elevate the mood of the patient. Comparing the adverse effects of Pristiq vs Wellbutrin, Wellbutrin causes fewer sexual side effects than other antidepressants and has few to no adverse effects upon withdrawal. This makes Wellbutrin a good option for those who struggle with the withdrawal symptoms of Desvenlafaxine. Also, while desvenlafaxine has the side effect of reducing the appetite, it may be insufficient for people who overeat because of their depression. Contrasting Pristiq vs Wellbutrin, Wellbutrin can help people lose weight effectively, which makes it more suitable for some patients.
This makes Wellbutrin a good option for those who struggle with the withdrawal symptoms of Desvenlafaxine. Also, while desvenlafaxine has the side effect of reducing the appetite, it may be insufficient for people who overeat because of their depression. Contrasting Pristiq vs Wellbutrin, Wellbutrin can help people lose weight effectively, which makes it more suitable for some patients.
If taking any drug makes a patient uncomfortable, it is a first call to talk about this with a doctor.
Fetzima vs Pristiq
Fetzima was approved for treating depression in 2013 by the FDA. The medicine is a selective serotonin-norepinephrine reuptake inhibitor that works by balancing certain chemicals in the brain. In contrasting the efficacy of Fetzima vs Pristiq, there is no available study to indicate which one is more efficacious. It is, therefore, advisable to consult your physician before increasing the dose or switching medicines. When comparing the side effects of Fetzima vs Pristiq, it was discovered that Fetzima can cause significant sexual side effects in men as compared to women. It is also associated with nausea and drops in blood pressure when a person is rapidly sitting or standing up. However, do not stop taking the drug cold turkey as it may lead to complications.
It is also associated with nausea and drops in blood pressure when a person is rapidly sitting or standing up. However, do not stop taking the drug cold turkey as it may lead to complications.
Cymbalta vs Pristiq
Also known as Duloxetine, Cymbalta is a medicine useful in treating depression, anxiety, neuropathic pain, and fibromyalgia. It is a selective serotonin and norepinephrine reuptake inhibitor. Thus it treats depression and its symptoms by increasing the neurotransmitters, serotonin, and norepinephrine, in the brain. When Cymbalta vs Pristiq is compared, it is discovered that Cymbalta has more uses. This is because while Desvenlafxine only treats depression, Cymbalta treats pain as well. Contrasting Cymbalta vs Pristiq, the sexual side effects of the last one are incredibly hindering for many patients. Cymbalta may be a good alternative to desvenlafaxine for people who are strongly affected by sexual dysfunction, resulting from their depression medication. Compared to other antidepressants, Cymbalta is generally well-tolerated and causes fewer sexual side effects.
Compared to other antidepressants, Cymbalta is generally well-tolerated and causes fewer sexual side effects.
Khedezla vs Pristiq
Khedezla can also be a valid alternative. Khedezla is another brand name for desvenlafaxine. Due to the same acting substance, Khedezla doesn’t provide significant benefits over other brands of desvenlafaxine. It is also a serotonin-norepinephrine reuptake inhibitor and works the same way desvenlafaxine does. Khedezla has not been approved for the treatment of depression in children and adolescents. Its side effects include dry mouth, dizziness, suicidal ideation, and constipation. A healthcare professional might prescribe Khedezla if the patient doesn’t find relief in other similar medications.
Trintellix vs Pristiq
Vortioxetine, marketed under the brand name Trintellix, is an antidepressant that is an SSRI. Thus it works by inhibiting serotonin in the brain to treat major depressive disorder. Trintellix can be suitable for patients who don’t respond to desvenlafaxine. Trintellix can be slightly more expensive, and it is known to cause significant sexual side effects in male patients. Trintellix may be more convenient than desvenlafaxine due to its long half-life of 66 hours. The side effects of both medications are similar to the ones mentioned above. They include nausea, vomiting, and constipation. Be sure to consult a physician before switching to Trintellix.
Trintellix can be slightly more expensive, and it is known to cause significant sexual side effects in male patients. Trintellix may be more convenient than desvenlafaxine due to its long half-life of 66 hours. The side effects of both medications are similar to the ones mentioned above. They include nausea, vomiting, and constipation. Be sure to consult a physician before switching to Trintellix.
Pristiq vs Prozac
Prozac (Fluoxetine) is an antidepressant and its use is not restricted to the treatment of depression. The medication can also be used to treat ailments like obsessive-compulsive disorder, panic attacks, bulimia, and premenstrual dysphoric disorder. Therefore comparing the use of Pristiq vs Prozac, Prozac may be preferable due to its treatment of other disorders. Prozac belongs to the class of medications known as selective serotonin reuptake inhibitors. Thus comparing Pristiq vs Prozac, both medications have a similar MOA. Both treat depression by inhibiting the reuptake of serotonin which results in an increase in serotonin. The two medications also share similar side effects which may include vomiting, diarrhea, excessive sweating, seizures, and dryness of mouth.
The two medications also share similar side effects which may include vomiting, diarrhea, excessive sweating, seizures, and dryness of mouth.
Ask Your Doctor Before Taking Antidepressants
Patients may need to find a substitute for desvenlafaxine due to tolerance, discomforting withdrawal symptoms, or persistent side effects. Those who are pregnant or trying to become pregnant might find it beneficial to switch from desvenlafaxine to Cymbalta. Also, such antidepressants as Wellbutrin and Viibryd cause fewer sexual side effects than other medications in this category. Finally, Zoloft might be a suitable alternative for patients who are younger than 18, as this drug is approved for treating obsessive-compulsive disorder in minors.
It is not rare that people misuse their medications, intentionally or unintentionally. In such cases, it is critical to react timely to prevent abuse which may lead to addiction. If the situation goes too far, and the signs of addiction are clear, addiction centers are among the best sites to help recover. Drug abuse treatment is not easy, and not always rapid. In any case, it is worth staying sober.
Drug abuse treatment is not easy, and not always rapid. In any case, it is worth staying sober.
Hope Without Commitment
Find the best treatment options. Call our free and confidential helpline
(888)-772-4219
Most private insurances accepted
Marketing fee may apply
Page Sources
- Clinical Trials. (n.d). 12-week Study of Pristiq (Desvenlafaxine) Social Anxiety Disorder. Clinical Trials. https://clinicaltrials.gov/ct2/show/NCT01316302
- K. Coleman, V. Xavier, T. Palmer, J. Meaney, L. Radalj, et al. (2012). An Indirect Comparison of The Efficacy and Safety of Desvenlafaxine and Venlafaxine Using Placebo as The Common Comparator. PubMed. https://pubmed.ncbi.nlm.nih.gov/22883424/
- D. Singh, A. Saadabadi. (2021). Venlafaxine. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK535363/
- D. Ionescu, MD, J. Rosenbaum, MD, J. Alpert, MD. (2015). Pharmacological Approaches to The Challenge of Treatment-Resistant Depression.
 Dialogues in Clinical Neuroscience. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518696/
Dialogues in Clinical Neuroscience. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518696/ - US Food and Drug Administration. (2008). Zoloft (Sertraline Hydrochloride) Tablets and Oral Concentrate. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019839s070,020990s032lbl.pdf
- National Alliance on Mental Illness. (n.d). Escitalopram (Lexapro). National Alliance on Mental Illness. https://www.nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Escitalopram-(Lexapro)
- Viibryd. (n.d). Side Effects & Safety| Viibryd (vilazodone HCl). Viibryd. https://www.viibryd.com/side-effects
- K. Tourian, MD, C. Leurent, PhD, J. Graepel, PhD, P. Ninan, MD. (2010). Desvenlafaxine and Weight Change in Major Depressive Disorder. The Primary Care Companion to The Journal of Clinical Psychiatry. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2882808/
- Fetzima. (n.d). Safety & Side Effects | Fetzima (levomilnacipran) ER Capsules.
 Fetzima. https://www.fetzima.com/about/antidepressant-side-effects
Fetzima. https://www.fetzima.com/about/antidepressant-side-effects - Prescriber’s Digital Reference. Khedezla (desvenlafaxine) - Drug Summary. Prescriber’s Digital Reference. https://www.pdr.net/drug-summary/Khedezla-desvenlafaxine-3333
- A. D’Agostino, C. English, PharmD, J. Rey, MS. Vortioxetine (Brintellix): A New Serotonergic Antidepressant. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4296590/
- MedlinePlus. (n.d). Fluoxetine. MedlinePlus https://medlineplus.gov/druginfo/meds/a689006.html
- J. Dwyer, MD, M. Bloch, MD. (2019). Antidepressants for Pediatric Use. Current Psychiatry. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6738970/
Published on: February 13th, 2020
Updated on: November 3rd, 2021
About Author
Nena Messina, Ph.D.
Nena Messina is a specialist in drug-related domestic violence. She devoted her life to the study of the connection between crime, mental health, and substance abuse. Apart from her work as management at addiction center, Nena regularly takes part in the educational program as a lecturer.
Medically Reviewed by
Michael Espelin APRN
8 years of nursing experience in wide variety of behavioral and addition settings that include adult inpatient and outpatient mental health services with substance use disorders, and geriatric long-term care and hospice care. He has a particular interest in psychopharmacology, nutritional psychiatry, and alternative treatment options involving particular vitamins, dietary supplements, and administering auricular acupuncture.
Have something to say?
Share your story in our Addiction Treatment Communities
Prozac generation. How the truth about antidepressants was hidden from us - Snob
Thirty years ago, the introduction of Prozac in American pharmacies revolutionized the treatment of depression. Today, however, scientists say we don't know what depression is or whether Prozac actually works. "Snob" cites theses from Quartz's article on why modern approaches to the treatment of depression can be based on misconceptions and what to do for people who suffer from mental illness
Today it is widely believed that depression is the result of biochemical disturbances in the brain. In fact, this is just one of the hypotheses that is so often replicated in the scientific community that it has come to be perceived as a proven truth.
In fact, this is just one of the hypotheses that is so often replicated in the scientific community that it has come to be perceived as a proven truth.
This happened because in medical science psychiatry for a long time did not have the weight of and, as a rule, was associated with the Hippocratic theory of four types of temperament and phrenology (pseudo-science about the connection of the psyche with the shape of the skull). For doctors, Freud's psychoanalytic theory was not convincing either. Under these conditions, the hypothesis that mental illness is a consequence of organic disorders of the brain sounded very attractive. This version was most often discussed as the main one, however, significant studies confirming it have not appeared.
One of the first drugs to "capitalize" the hypothesis of mental illness as a result of biochemical brain disorders was Prozac (fluoxetine). The drug appeared in American pharmacies 30 years ago, and we still do not know how it works and whether it is really effective in treating depression.
Psychiatrists, who benefit from arguing that depression is a disease of the brain and not a mental illness, insist on drug treatment. There are various social factors left behind that can also provoke depression: isolation, poverty, tragic events in life, and much more. Psychotherapy as a method of treatment is secondary to pills. This distorts not only our understanding of depression, but even our experience of it.
Various types of depressive disorders* have been described today. For example, major depressive disorder, drug-induced depressive disorder, organic mood disorders resulting from an organic disease. They all differ in etiology and duration, but the symptoms described are generally the same. Patients with different depressive states are treated with the same drugs, although there is no question of the same violations of the biochemical processes of the brain.
In the 1950s and 1970s, some pretty dangerous drugs were available in American pharmacies to treat depression. Even a slight overdose of these drugs - Butisol (barbiturate) and Valium (diazepam) - could be fatal, which deterred many buyers. The introduction of Prozac made a big difference because it was a new generation of antidepressants, safer and with fewer unpleasant side effects.
Even a slight overdose of these drugs - Butisol (barbiturate) and Valium (diazepam) - could be fatal, which deterred many buyers. The introduction of Prozac made a big difference because it was a new generation of antidepressants, safer and with fewer unpleasant side effects.
Antidepressants that exist today work more or less the same way. So says Anthony Rothschild, Professor of Psychiatry at the University of Massachusetts Medical School. What's more, over the past three decades of Prozac's use in the treatment of depression, the choice of antidepressants in pharmacies has grown significantly. However, nothing more effective than imipramine, the main drug of tricyclic antidepressants, has not been created.
All this time, antidepressant drug manufacturers have been able to claim that depression is a brain disorder that can be corrected with pills: , both Paroxetine and Zoloft (sertraline) were marketed as "chemical rebalancing" drugs. Meanwhile, there are still no convincing, scientifically proven versions of the causes of depression.
Meanwhile, there are still no convincing, scientifically proven versions of the causes of depression.
According to modern research, depression is inherited in 37 percent of cases , so obviously genetics and biology play a significant role. But since neuroscientists still don't have a precise way to determine what brain function is considered "normal" and what is not, it's impossible to test some of the hypotheses.
If serotonin levels were the cause of depression, then SSRIs would work instantly instead of requiring a long cycle of dosing**. In addition, a decrease in the level of serotonin in the brain should provoke depression, but studies show that this is not the case. This does not mean that antidepressants aimed at restoring serotonin levels do not work. But we don't know if they ultimately address the root cause of depression or just combat its effects.
Our ideas about diseases and their nature influence their course. For example, the symptoms of anorexia in patients in Hong Kong have changed as people in the region become more aware of how the disease works in Western countries. It is possible that our current understanding of depression and the medical approach are leading to the fact that the disease covers more people: psychiatry calls mental illness even those conditions that were previously considered stress or emotional decline.
According to this study, the placebo effect in treating depression is almost as good as taking antidepressants. The difference is so small that it practically does not affect the clinical picture. The author of the study, director of the placebo study program at Harvard Medical School, Irwin Kirsch, is a staunch supporter of non-drug treatments for depression. Studies show that pills and psychotherapy are effective in the short term, but patients treated without medication feel better over a longer period of time and have a significantly lower relapse rate. Kirsch, of course, is full of opponents who, on the contrary, are convinced that drugs are necessary.
Kirsch, of course, is full of opponents who, on the contrary, are convinced that drugs are necessary.
The truth, as often happens, is somewhere in between: severely depressed patients who are unable to go to psychotherapy should definitely be prescribed medication. Those who are able to undergo psychotherapy should definitely do this, especially since drug treatment does not help all patients. In the treatment of depression, cognitive-behavioral psychotherapy has also proven itself well, which will cost more than drugs, but the effect of which will be more sustainable.
Depression has become a global epidemic, affecting one in four people worldwide today. It is obvious that the causes are not only in biology, but also around us: poverty, unemployment, sexual violence - it is impossible to stop the epidemic if you do not fight all the causes, many of which - alas - cannot be overcome with pills.
* In DSM-5, 5th edition of the American Diagnostic Manual of Mental Disorders
** SSRIs — Selective Serotonin Reuptake Inhibitors — a group of third-generation antidepressants
What they treat us with: Prozac.
 From depression to bulimia
From depression to bulimia Medicine
16:00, December 14, 2017
Analysis of one of the popular antidepressants how it is customary to treat them and whether the antidepressant Prozac works, read in the new material of the heading “How we are treated”.
Prozac is on the list of the most important, safest and most effective (including from an economic point of view) drugs according to the World Health Organization. However, as we remember after the article with the analysis of Tamiflu, this does not guarantee its effectiveness.
Prozac is prescribed for the treatment of depression, obsessive-compulsive disorders, bulimia nervosa. If you know very well what it is, you can immediately skip to the “from what, from what” part.
When life is not nice
Depression is called depression, loss of interest in what used to make the patient happy. According to the international classification of diseases ICD-10, the main criteria by which such a diagnosis can be made include depressed mood for more than two weeks, loss of strength and consistently high fatigue (more than a month) and anhedonia (the inability to enjoy what used to bring joy). Doctors consider additional criteria for depression to be pessimism, low self-esteem, thoughts of death and suicide, appetite disturbances (weight loss or overeating), sleep problems, constant fears and anxieties, feelings of worthlessness and guilt, inability to concentrate, and a constant sweet taste in the mouth. These symptoms are unlikely to occur simultaneously (for example, fatigue and apathy may predominate in some cases, while anxiety and guilt may prevail in others), therefore, in order to diagnose depression, the patient's condition must meet at least two main criteria and three additional ones. At the same time, according to the definition of the US National Institute of Mental Health, such a state should last quite a long time (more than two weeks).
Doctors consider additional criteria for depression to be pessimism, low self-esteem, thoughts of death and suicide, appetite disturbances (weight loss or overeating), sleep problems, constant fears and anxieties, feelings of worthlessness and guilt, inability to concentrate, and a constant sweet taste in the mouth. These symptoms are unlikely to occur simultaneously (for example, fatigue and apathy may predominate in some cases, while anxiety and guilt may prevail in others), therefore, in order to diagnose depression, the patient's condition must meet at least two main criteria and three additional ones. At the same time, according to the definition of the US National Institute of Mental Health, such a state should last quite a long time (more than two weeks).
Severe depression (clinical) includes a complex set of symptoms called major depressive disorder and may sometimes not be accompanied by low mood at all. However, because of her, the patient is physically unable to live and work normally, and the comments of those around him in the spirit of “he just can’t pull himself together” or “enough to turn sour that he spread snot” sound like a mockery. Such phrases stigmatize depression, blaming a person for his condition, while he himself will not be able to cope and needs treatment. To diagnose major depressive disorder, there is a whole questionnaire of major depression compiled by the World Health Organization. Also, depressive disorders include other conditions accompanied by depression, such as dysthymia (daily low mood and mild symptoms of depression for two years or more).
Such phrases stigmatize depression, blaming a person for his condition, while he himself will not be able to cope and needs treatment. To diagnose major depressive disorder, there is a whole questionnaire of major depression compiled by the World Health Organization. Also, depressive disorders include other conditions accompanied by depression, such as dysthymia (daily low mood and mild symptoms of depression for two years or more).
The causes of depression can be very different: somatic (due to diseases of the body), psychological (after strong dramatic experiences, such as the death of a relative) and iatrogenic (as a side effect of certain drugs). As strange as it would be to provide first aid to a victim of an electric shock without removing the wire from him, it is difficult to cure the symptoms of depression without eliminating its cause or changing the lifestyle that led the patient to such a state. If the patient lacks some essential substances (for example, tryptophan), it is important to make up for their lack, and not just fight the depressed mood with drugs. If he has some kind of psychological trauma, the help of a psychotherapist will be required. And for a person whose depression is provoked by hormonal disorders, neurological diseases, heart disease, diabetes, or even cancer (and this happens), it is more important to cure the disease itself, and symptomatic treatment of depression will be a secondary goal.
If he has some kind of psychological trauma, the help of a psychotherapist will be required. And for a person whose depression is provoked by hormonal disorders, neurological diseases, heart disease, diabetes, or even cancer (and this happens), it is more important to cure the disease itself, and symptomatic treatment of depression will be a secondary goal.
When you can't stop
Obsessive-compulsive disorder, or OCD (also called obsessive-compulsive disorder), consists of two mandatory components: obsessions (obsessive anxious or frightening thoughts) and compulsions (compulsive actions). A classic example is cleanliness-related OCD, where a person is afraid of contamination or contamination by microorganisms. Such thoughts and fears are called obsessions. In order to protect themselves from them, a person will worry too much about cleanliness, such as constantly washing their hands. Any contact with a non-sterile, according to the patient, object, plunges such a person into horror. And if you can’t wash your hands again, he will experience real suffering.
And if you can’t wash your hands again, he will experience real suffering.
You can learn how to deal with medications on your own in the author's online course "How we are treated" by the editor of Indicator.Ru Ekaterina Mishchenko: https://clck.ru/Pnmtk
Such "protective" behavior is called compulsion. The desire for cleanliness can be understood if a person is in conditions of complete unsanitary conditions or, on the contrary, wants to maintain sterile conditions somewhere in the operating room. But if the action loses its true meaning and becomes a mandatory ritual, it becomes a compulsion.
However, OCD can manifest itself not only as a fear of pollution, but also as excessive superstition, fear of losing a necessary object, sexual or religious obsessive thoughts and related actions. Their reasons may lie in several areas: biological and psychological. The first includes diseases and features of the nervous system, lack of neurotransmitters (biologically active substances that ensure the transmission of a nerve impulse from one neuron to another, for example, dopamine or serotonin), genetic predisposition (mutations in the hSERT gene encoding the serotonin carrier protein and located on 17 -th chromosome).
There is also an infectious theory of the development of OCD, associated with the fact that in children it sometimes occurs after infection with streptococcus. This theory is called PANDAS - an abbreviation for the English Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections, which translates as "Children's autoimmune neuropsychiatric disorders associated with streptococcal infections." The cause of this syndrome may be an attack of its own antibodies produced against streptococcus on the patient's nerve cells. However, this theory has not yet been confirmed.
Another group of explanations for the development of OCD is psychological. They go back to the theories of the beginning of the last century (from Freud to Pavlov). Mayakovsky's father died of blood poisoning after being injected with a binder, so it is believed that the poet also showed a pathological love for cleanliness. But you don't have to be a futurist poet to experience the full benefits of OCD: even dogs and cats suffer from it. Only in them this is expressed in the endless licking of wool and attempts to catch their tail.
Only in them this is expressed in the endless licking of wool and attempts to catch their tail.
The Yale-Brown scale is used to diagnose obsessive-compulsive disorder. In the fight against OCD, the method of psychological persuasion can be useful: patients are patiently explained that if they skip the “ritual” once, nothing terrible will happen. But drugs are also used in treatment.
When you are how you eat
Bulimia nervosa (third indication for Prozac) is a binge eating disorder. The main signs of bulimia are uncontrolled eating in large quantities, obsession with excess weight (calorie counting, attempts to induce vomiting after eating, fasting, use of laxatives), low self-esteem, low blood pressure. Other symptoms are sudden changes in body weight, kidney problems and dehydration, enlarged salivary glands, heartburn after eating, and inflammation of the esophagus. Due to provoking vomiting, hydrochloric acid from the stomach constantly enters the oral cavity of patients, which can lead to grinding of tooth enamel and ulcers on the mucous membrane. According to the DSM-5 classification of diseases, uncontrolled consumption of large amounts of food and the simultaneous use of various drastic measures for weight loss is the main criterion for diagnosing bulimia nervosa.
According to the DSM-5 classification of diseases, uncontrolled consumption of large amounts of food and the simultaneous use of various drastic measures for weight loss is the main criterion for diagnosing bulimia nervosa.
Video about bulimia on the educational medical resource Open Osmosis (USA)
The causes of bulimia can be either biological (incorrect levels of hormones or neurotransmitters, including serotonin) or social. The importance of the latter is highlighted, for example, in a high-profile study among teenage girls in Fiji, which showed a sharp increase in cases of intentional bowel cleansing for weight loss in just three years (from 1995 to 1998) after television appeared in the province. Perhaps the desire to be like models from the screens and covers really pushes for such behavior.
Bulimia can often be associated with other psychiatric disorders (depression, anxiety disorders, sleep disorders). According to a study by the New York State Psychiatric Institute and Columbia University, 70% of people with bulimia have ever experienced depression, compared with just over 25% in the general population.
According to a study by the New York State Psychiatric Institute and Columbia University, 70% of people with bulimia have ever experienced depression, compared with just over 25% in the general population.
Bulimia itself is not very common, and it can be more difficult to diagnose than the same anorexia, because changes in body weight in bulimia are less sharp and noticeable. For diagnosis, the food attitude test, developed by the Clark Institute of Psychiatry at the University of Toronto, and other tests based on it, are used. But (as with the tests for OCD and depression above), its result only indicates the likelihood that the patient has developed a disorder, but does not allow for a definitive diagnosis, especially for oneself.
From what, from what
What is a medicine that is prescribed for three types of disorders at once? The active ingredient in Prozac is fluoxetine. The patent for Prozac expired back in 2001, so many generics are available in pharmacies - cheaper copies that use the same active ingredient, but are not as well studied and may differ slightly from the original.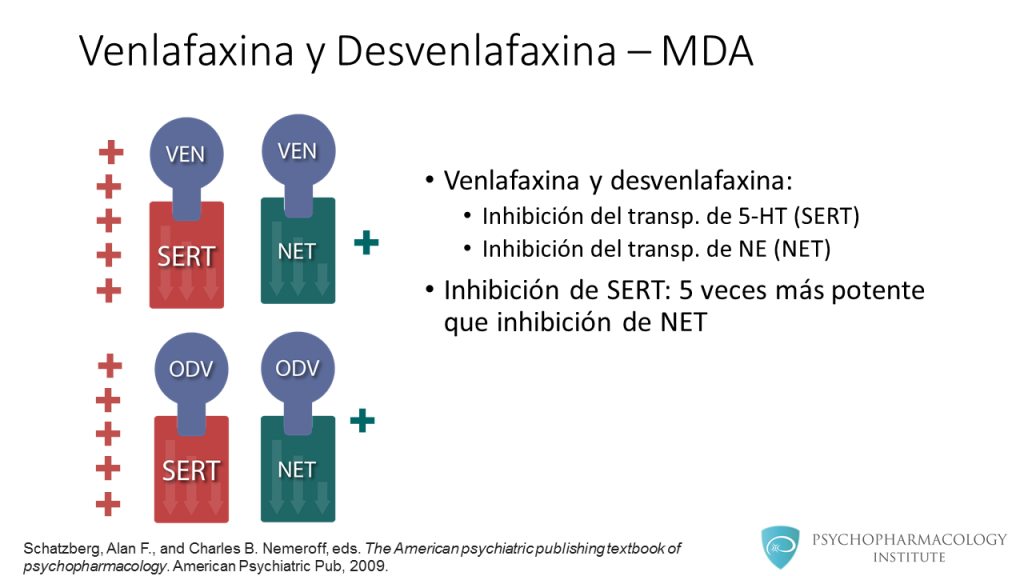 These drugs include Fluoxetine, Prodel, Profluzak, Fluval.
These drugs include Fluoxetine, Prodel, Profluzak, Fluval.
Fluoxetine, discovered and marketed by Eli Lilly and Company, belongs to a group of antidepressants called selective serotonin reuptake inhibitors. This group is considered third-generation antidepressants, fairly well tolerated and without significant side effects.
Fluoxetine is readily absorbed into the blood, can bind to plasma proteins and accumulate in body tissues. It also penetrates the blood-brain barrier, which protects the nervous system and brain from many substances circulating in the blood. There, in the nervous system, it works in the synaptic cleft we have already mentioned, preventing the excess serotonin ejected from the synapse from returning to the neurotransmitter. Because of this, serotonin is longer present in the synaptic cleft and can bind to receptors. How exactly fluoxetine achieves this effect is not clear even to manufacturers, but it is known that it has little effect on the work of other neurotransmitters. However, at high doses, fluoxetine increases adrenaline and dopamine levels, as studies in rat brain tissue show.
However, at high doses, fluoxetine increases adrenaline and dopamine levels, as studies in rat brain tissue show.
Fluoxetine and its metabolite, norfluoxetine, can interfere with each other's actions. Because of this, according to scientists from the Institute of Research Medicine in Barcelona, a constant concentration of fluoxetine in the blood is achieved only after four weeks of taking the drug. Similarly, the effects of taking the medicine do not disappear immediately. Associated with this is the difficulty in selecting the required dose for a particular patient.
Serotonin itself, which is absolutely incorrectly called the “happiness hormone” (hormones are produced in one organ of the body, but perform their function in another, serotonin in this context simply conducts nerve impulses in the brain regions responsible for good mood, and is produced there well), in fact, it performs much more functions. Yes, it affects mood, sleep, and appetite, so some cases of depression, bulimia nervosa, and OCD may be caused by insufficient production of this neurotransmitter and corrected with serotonin reuptake inhibitors. But in addition, platelets can actively capture it and affect blood clotting. Serotonin is also involved in the processes of memorization and learning. At the same time, not only vertebrate animals can produce it: according to a study by Chinese and American scientists, the pain from an insect bite is largely due to the presence of serotonin in the poison, and the dysentery amoeba, according to an article in Science, can cause diarrhea by releasing serotonin in our intestines.
But in addition, platelets can actively capture it and affect blood clotting. Serotonin is also involved in the processes of memorization and learning. At the same time, not only vertebrate animals can produce it: according to a study by Chinese and American scientists, the pain from an insect bite is largely due to the presence of serotonin in the poison, and the dysentery amoeba, according to an article in Science, can cause diarrhea by releasing serotonin in our intestines.
The lists (not) included
But all these are only mechanisms, and besides, they have not been studied to the smallest detail. To understand how this works in real people and how often it helps, let's turn to clinical trials. However, anyone who enters the combination “fluoxetine depression double blind randomized controlled” into the PubMed scientific article database and filters clinical trial (clinical trial) will see more than 558 articles, up to work comparing the effectiveness of Prozac and homeopathy.
Double-blind, randomized, placebo-controlled method is a method of clinical drug research in which the subjects are not privy to important details of the study being conducted. “Double-blind” means that neither the subjects nor the experimenters know who is being treated with what, “randomized” means that the distribution into groups is random, and placebo is used to show that the effect of the drug is not based on autosuggestion and that this medicine helps better than a tablet without active substance. This method prevents subjective distortion of the results. Sometimes the control group is given another drug with already proven efficacy, rather than a placebo, to show that the drug not only treats better than nothing, but also outperforms analogues.
Indicator.Ru
Help
No living person can analyze them within an adequate period of time. And even Cochrane reviews can be found as many as 36 (that's really a lot), although not all of them consider the action of fluoxetine for its direct indications (depression, bulimia and obsessive-compulsive disorder).
The Cochrane Library is a database of the Cochrane Collaboration, an international non-profit organization involved in the development of World Health Organization guidelines. The name of the organization comes from the name of its founder, the 20th-century Scottish medical scientist Archibald Cochrane, who championed the need for evidence-based medicine and the conduct of competent clinical trials and wrote the book Efficiency and Efficiency: Random Reflections on Public Health. Medical scientists and pharmacists consider the Cochrane Database one of the most authoritative sources of such information: the publications included in it have been selected according to the standards of evidence-based medicine and report the results of randomized, double-blind, placebo-controlled clinical trials.
Indicator.Ru
Help
One of them is dedicated to antidepressants used against bulimia nervosa. Although in general the authors note that there is little data on this topic, fluoxetine (for which there were only five randomized double-blind controlled trials in 2003) is recognized as a leader in this direction. However, the authors refuse to recommend this medicine in the conclusion, arguing that not all clinical trial data have been published and are available for consideration.
However, the authors refuse to recommend this medicine in the conclusion, arguing that not all clinical trial data have been published and are available for consideration.
The authors of a 2008 review reviewed the benefits of serotonin reuptake inhibitors (including fluoxetine) in obsessive-compulsive disorder and concluded that they help better than placebo, and the associated side effects are much more significant, among which nausea is most common , insomnia and headache. According to a 2013 review, the usefulness of this same group of drugs in autism and related OCD is unclear, and the data are insufficient to conclude.
The most popular subject of fluoxetine reviews was the fight against depression. But the authors of most of them note the lack of data (for example, in this 2013 review). In a broad inclusion criteria review of 1177 randomized controlled trials of fluoxetine for depression in adults, the authors conclude that it is about as effective as other antidepressants but less toxic. However, they warn against hasty decisions, since most of the studies were conducted on small groups of people (100 or less) and were funded by the manufacturer, which is more profitable to publish only positive results, hiding information about failures. Data on postpartum depression are also found to be insufficient and inconsistent. The same issues are highlighted by a review of articles on the effectiveness of antidepressants against dementia-related senile depression.
However, they warn against hasty decisions, since most of the studies were conducted on small groups of people (100 or less) and were funded by the manufacturer, which is more profitable to publish only positive results, hiding information about failures. Data on postpartum depression are also found to be insufficient and inconsistent. The same issues are highlighted by a review of articles on the effectiveness of antidepressants against dementia-related senile depression.
Indicator.Ru concludes: one of the best stimulant antidepressants is still not perfect
A large number of studies confirm the effectiveness of fluoxetine, a key component of Prozac. But part of the reviews of the Cochrane Collaboration note that not all trial data have been published by manufacturers. And this accusation is not an empty phrase: according to Eli Lilly's internal documents, manufacturers during trials often attributed suicide cases to worsening depression or overdosing on the drug.
As a result, following numerous reports of suicide by patients prescribed this drug, the US Food and Drug Administration (FDA) has issued a warning label to the drug's packaging.
This does not mean that the harm from the medicine always outweighs its benefit, but such dishonest behavior of manufacturers does not allow us to assess the risks more accurately. Given the difficulty with the selection of an individual dose and the slow effect, adjusting the dosage is really not easy.
Prozac is also classified as a serotonin reuptake inhibitor, but if the cause of your condition is something else, you need to pay more attention to finding and eliminating them than fighting depression. As we wrote above, somatic diseases (for example, cirrhosis of the liver, cancer or diabetes), and even a lack of vitamins, can also cause depression. In addition, depression or another disorder may be the result of psychological trauma that will be difficult to deal with without psychotherapy.