Mmpi 2 results meaning
How to Trust & Understand your test results
The MMPI-2 Score
The interruption of the MMPI 2 is called the MMPI-2 SCORE. Assigned to each question within the MMPI quiz is a base score of zero which will in total produce a mean score of around 50 for each of the scales being measured. Certain combinations of answers to the questions will add or minus 1 point of your score and at the end your final result is presented.
The score average is around 50 (The test will adjust averages for males and females and a few other different aspects) with a standard deviation of 10 points per deviation Thus, a score of 60 is one standard deviation above the mean, while a score of 30 is two standard deviations below the mean.
MMPI-2 Scoring & Interpretation Meaning
After the MMPI-2 is taken and scored, an interpretive report is constructed by the psychologist. Scores are converted to what are called normalized “T scores” on a scale ranging from 30 to 120. The “normal” range of T scores is from 50 to 65. Anything above 65 and anything below 50 is considered clinically significant and open for interpretation by the psychologist.
Throughout the years and over numerous research studies, a set of standard clinical profiles have emerged on the MMPI-2 which professionals call “codetypes.” A codetype is simply when two scales demonstrate significantly high T scores, with one being higher than the other. For instance, a 2-3 codetype (meaning that both Scale 2 and Scale 3 are significantly elevated) suggests significant depression, lowered activity levels and helplesness; furthermore the person may have become accustomed to their chronic problems and often have physical complaints.
Dozens of clinical codetypes are well-known and understood, as well as T scores that “spike” on a single Scale (such as a “Spike 4”, which would be a sign of a person who shows impulsive behavior, rebelliousness and poor relationships with authority figures). People with little or no psychopathology or personality concerns will not reach significance for any particular codetype. Most people with personality or mental health issues will usually have only one codetype, or a single codetype with a spike on a third scale.
People with little or no psychopathology or personality concerns will not reach significance for any particular codetype. Most people with personality or mental health issues will usually have only one codetype, or a single codetype with a spike on a third scale.
Like all psychological interpretation, scores are analyzed in context of the individual being tested — not in a vacuum. For instance, we might expect a higher score in Hypomania (a measure of energy levels) in a teen, but it might be more unusual to see such a score in a senior citizen. Ideally, the MMPI-2 is being administered as a part of a battery of psychological tests, so that other testing can either confirm or deny the hypotheses the MMPI-2 may suggest.
Cited from psychcentral.com
Understanding Standard Deviation
Standard deviation is a widely used measure of variability or diversity used in statistics and probability theory. It shows how much variation or “dispersion” exists from the average (mean, or expected value). A low standard deviation indicates that the data points tend to be very close to the mean, whereas high standard deviation indicates that the data points are spread out over a large range of values.
A low standard deviation indicates that the data points tend to be very close to the mean, whereas high standard deviation indicates that the data points are spread out over a large range of values.
It is useful for expressing the variability of a population, standard deviation is commonly used to measure confidence in statistical conclusions.
How to Read your Score
1) Identify the T score you want to interpret.
This will come from the results of the test
2) Look at your T score on the normal distribution.
Average is any score between 40-60, A slight issue would be between 30-40 or 60-70. Problem areas with a score below 30 and over 70
3) Compare your score to the average T score.
Different for males and females
4) Look at what the test (and thus the T score) is measuring.
This is in the Scales (found here)
The accurate interpretation of your MMPI results is one of the reasons those who are trained and qualified to administer the MMPI tests like to strongly discourage people attempting to do it themselves.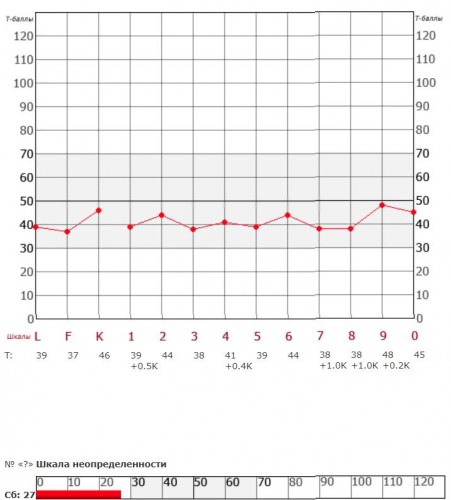 It does take training and knowledge to get a psychological accuracy that is useful for employment or court use of the MMPI.
It does take training and knowledge to get a psychological accuracy that is useful for employment or court use of the MMPI.
Practice the MMPI 2 (Minnesota Multiphasic Personality Inventory) for just $3.99 you can take the MMPI Online (Test & Results only, no analysis or interpretation provided.)
Ativan helps my anxiety immensely http://curtspharmacy.com/ativan
What Is the Minnesota Multiphasic Personality Inventory (MMPI)?
Does taking a personality test give you the jitters? Learn all about the MMPI and how it’s meant to help you.
The Minnesota Multiphasic Personality Inventory (MMPI) is one of the most commonly used psychological tests in the United States.
It’s primarily used to help mental health professionals assess and diagnose mental health conditions, such as schizophrenia, depression, and anxiety.
Lawyers also use the MMPI as forensic evidence in criminal defense and custody disputes. According to the publisher of the MMPI, the University of Minnesota Press, employers sometimes use the test in job screenings for high risk public safety positions, such as:
- police officers
- nuclear power plant personnel
- firefighters
- pilots
- air-traffic controllers
The University of Minnesota first published the test by Starke R. Hathaway and J.C. McKinley in 1942 and currently owns the copyright.
The University of Minnesota Press licenses the test to Pearson Assessments and other companies for sales and distribution.
The MMPI is a protected psychological test. This means the test and its materials are not freely available to the public. You won’t find the test items online, except for a few examples.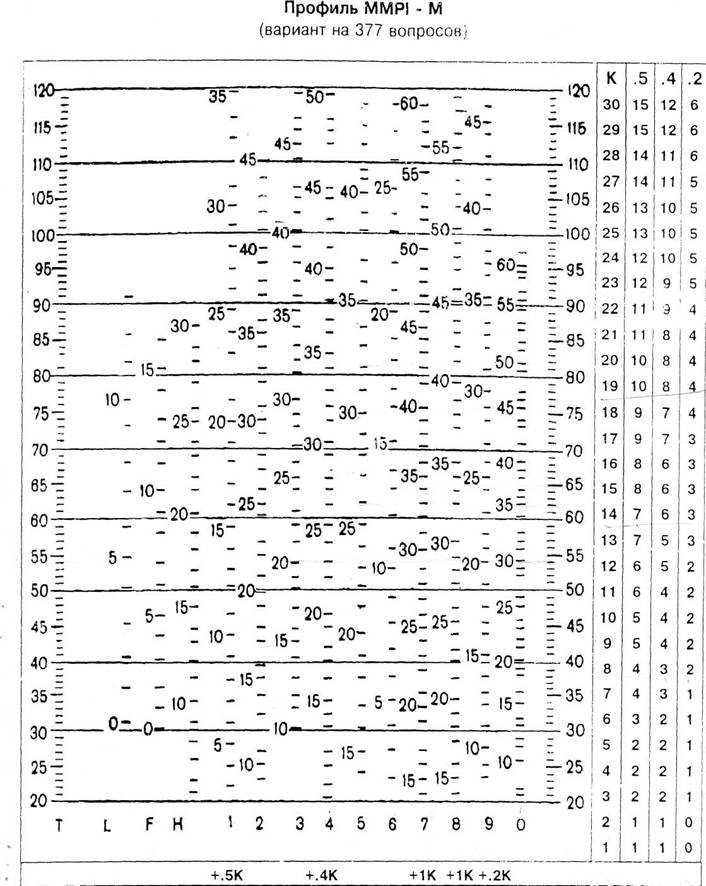
Only professionals who can provide the required credentials can buy the test from Pearson Assessments.
Types of MMPI tests
There are a variety of versions of the MMPI in general use today:
- MMPI-2. This is the standard adult version of the assessment. It was first released in 1989. It contains 567 true/false questions and takes 60 to 90 minutes to complete. It’s been revised to reflect more culturally diverse values than the original 1942 version.
- MMPI-2-Retracted Form. This version, published in 2008, is a shorter version of the MMPI-2. It’s intended for adults and contains 338 true/false items. The MMPI-2-R Ftakes about half the time as the MMPI-2 to complete, about 40 to 50 minutes.
- MMPI-Adolescent. This is a version of the test released in 1992 for adolescents from 14 to 18 years old. The MMPI-A contains 478 items and takes about 60 minutes to complete.
- MMPI-A-RF. This short form of the test for adolescents was released in 2016.
 It contains 241 items and takes 25 to 45 minutes to complete.
It contains 241 items and takes 25 to 45 minutes to complete. - MMPI-3. This is the newest version of the MMPI. It was released in 2020. It has updated items, scales, and norms. It contains 335 items and takes 25 to 50 minutes to complete.
These versions of the test are based on different norms and clinical scales.
A norm is a statistic or set of statistics (such as average, standard deviations, and score ranges) that researchers compare an individual’s score against. This helps researchers determine the baseline “normal,” or typical, result.
A scale is a group of questions that measure a person’s tendency toward a certain mental health condition. They can also measure aspects of mental or social functioning that don’t necessarily indicate a disorder.
Each test version also contains varying content scales, clinical subscales, and supplementary scales.
Interpreting the MMPI is a complex process that is closely protected and monitored.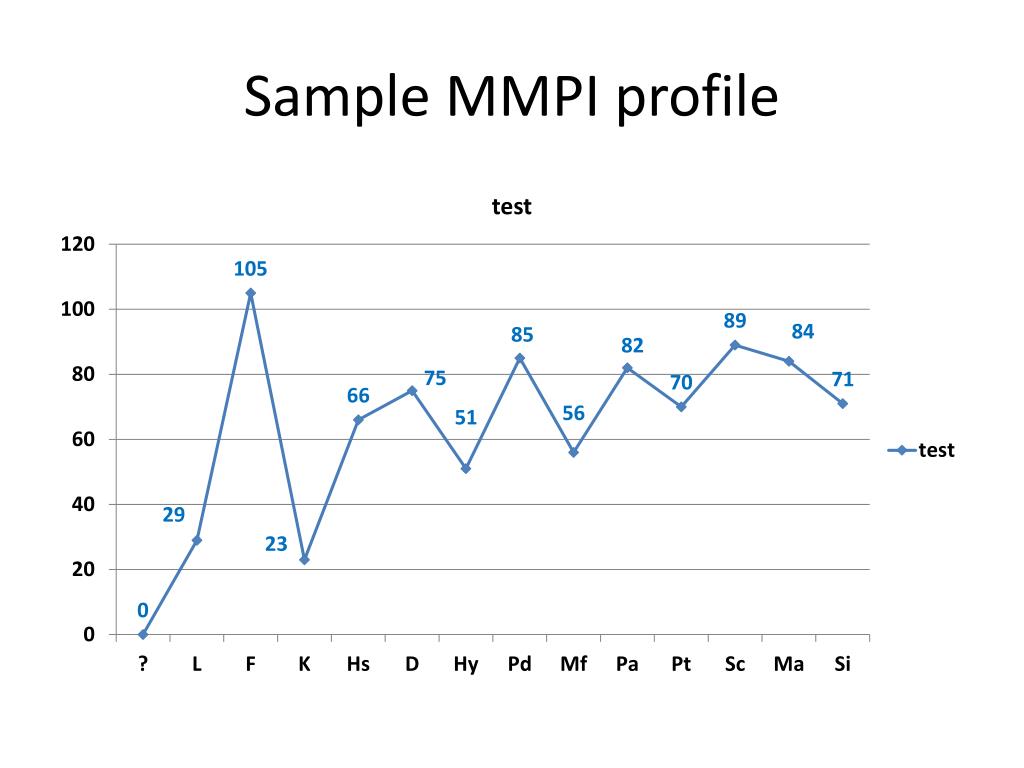 This is because the complex scale requires specific training to accurately interpret the results — and misinterpreting the results can have harmful consequences, leading to unnecessary distress.
This is because the complex scale requires specific training to accurately interpret the results — and misinterpreting the results can have harmful consequences, leading to unnecessary distress.
It’s important to know that the MMPI isn’t a standardized test in the usual sense. It doesn’t use percentile ranks that indicate how well you did on the test. It’s not a test you either pass or fail.
The test is part of a psychological evaluation your clinician will make. The results of the MMPI test will give your clinician a sense of what mental health conditions you might be experiencing.
The MMPI result will be just one factor in the diagnosis the clinician may make and the treatment they’ll recommend. Your mental health and medical history will be considered, along with your experiences.
The MMPI has built-in clinical scales that describe a person’s psychological processes and how they respond to stress.
Each scale is made of a specific group of questions (unknown to the test taker), which the test developer’s field research says indicates a particular psychological condition.
The MMPI also has built-in validity scales designed to identify how a person approached the test, such as whether they attempted to present themselves differently from how they actually view themselves.
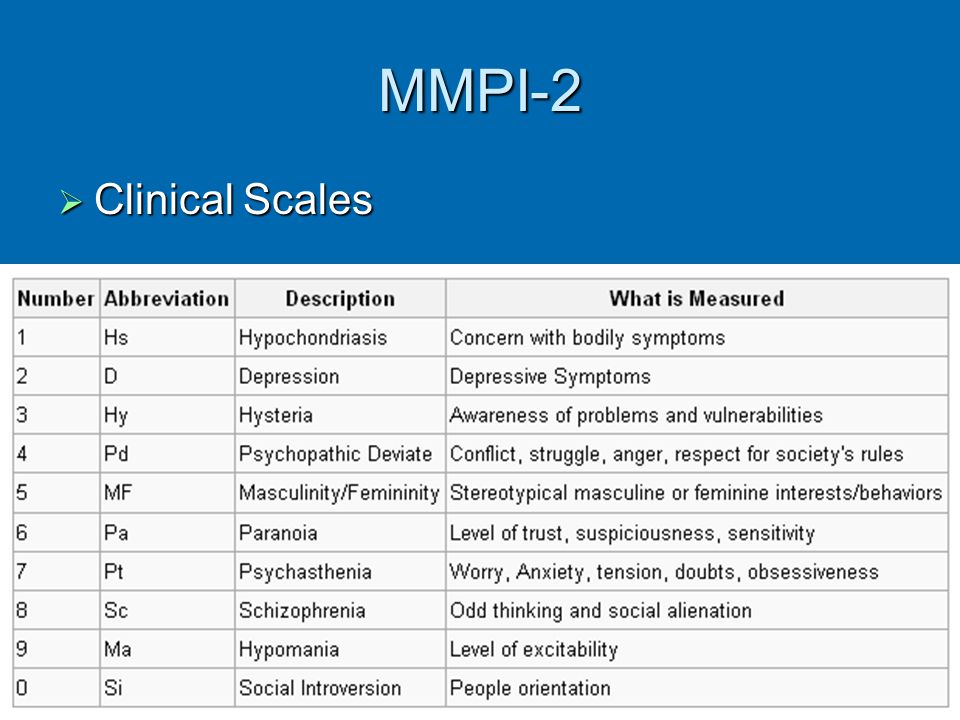
Here are the 10 clinical scales of the MMPI-2, which is still the most widely used version of the MMPI. These scales overlap, but generally, high scale scores point to a high risk of having a mental health disorder.
1. Hypochondriasis (Hs)
The hypochondriasis scale is designed to detect exaggerated concern over one’s health that is unsupported by medical authority. The concerns are usually vague and persist despite not being validated.
2. Depression (D)
The depression scale points to aspects related to clinical depression. The related questions concern low morale, overall dissatisfaction in life, and an absence of hope for the future.
3. Hysteria (Hy)
The hysteria scale tracks five aspects of a person:
- poor physical health
- shyness
- cynicism
- headaches
- neuroticism
A high score on this scale could point to a variety of mental health disorders, such as anxiety, paranoia, or dissociative disorders.
4. Psychopathic deviate (Pd)
This scale points to difficulty with family and authority figures.
It also gauges feelings of alienation from self and society as well as boredom.
5. Masculinity/femininity (Mf)
This scale measures how much a person abides by stereotypical masculine and feminine values and roles.
The questions deal with:
- activity interests
- aesthetic preferences
- personal sensitivities
6. Paranoia (Pa)
The paranoia scale identifies aspects of personality, such as grandiose thinking, suspicion toward other people, and rigid thinking.
It also includes items that might reflect delusions.
7. Psychasthenia (Pt)
This scale gauges a person’s ability to resist certain thoughts or behaviors.
This scale identifies abnormal fears, self-criticism, and concentration difficulty.
8. Schizophrenia (Sc)
This scale identifies tendencies toward bizarre thoughts and social alienation.
Its questions deal with:
- family relationships
- impulse control
- questions of self-worth
- sexual difficulties
9. Hypomania (Ma)
This scale identifies unhealthy overactivity expressed as excitement, elevated and unstable mood, and long strings of ideas.
Also included are feelings of grandiosity and egocentricity.
10. Social introversion (Si)
This scale gauges social introversion, which is the tendency to avoid social interactions or feel awkward and withdraw from them.
These items point to a lack of social skills and a preference to be among small groups or alone.
The validity scales attempt to identify deceptive or inconsistent test results. There are a variety of both intentional and unintentional reasons people might try to present themselves other than what they are.
Intentional deception has been known to occur in situations such as:
- employment screening
- attempts to get costly treatment
- disability evaluations
- personal injury lawsuits
- court-ordered evaluations
- competency hearings
- custody proceedings
- unwillingness to cooperate
Unintentional deception might occur for reasons such as:
- illness
- cultural misunderstanding
- test-taking difficulty
The validity scales vary among MMPI versions, but the MMPI-2 contains three general types of validity scales:
- non-responding or inconsistent responding (CNS, VRIN, TRIN)
- over-reporting, or exaggerating psychological symptoms, popularly called “faking bad” (F, Fb, Fp, FBS)
- under-reporting, or reducing psychological symptoms, popularly called “faking good” (L, K, S)
Here are the validity scales usually used in the MMPI-2 assessment.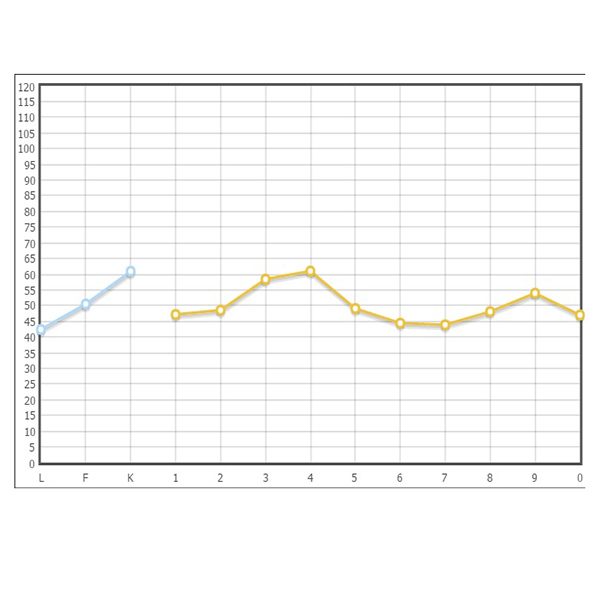 Some have been developed independently from the MMPI-2 test itself.
Some have been developed independently from the MMPI-2 test itself.
- CNS (cannot say). This is a measure of the number of “cannot say” responses.
- VRIN-r (variable response inconsistency). This identifies random responses made without consideration of the content.
- TRIN-r (true response inconsistency). This identifies fixed responding patterns.
- F scale (infrequent responses, 60 items). These are a collection of unlikely and contradictory responses.
- Fb (F back scale). This is the same as the F scale, except it only looks at responses to the second half of the test.
- FBS-r (symptom validity, 43 items). This scale is designed to identify the over-reporting of symptoms. It is popularly referred to as the “faking bad scale” scale.
- L-r (uncommon virtues, 15 items).
 This scale is also called the “lie scale.” It attempts to identify under-reporting of symptoms by test takers to appear in a better light than they actually are.
This scale is also called the “lie scale.” It attempts to identify under-reporting of symptoms by test takers to appear in a better light than they actually are. - K-r (adjustment validity, 30 items). This scale identifies under-reporting by test takers who may be tailoring answers to give the impression of healthy psychological adjustment. It’s also called the “faking good scale.”
- S (superlative self-presentation, 50 items). This scale identifies under-reporting by test takers who are defensive and intentionally distort their responses to try to look better in terms of certain human virtues.
People have always had concerns over the reliability and accuracy of the MMPI ever since it was first published in 1942.
The MMPI has been revised and updated various times to correct gender and racial bias, and to validate the test against new normative samples.
Studies of MMPI accuracy usually focus on specific uses.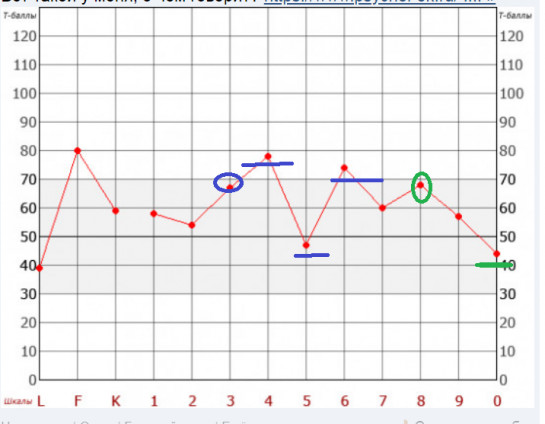 Reports often vary.
Reports often vary.
For example, a 2021 study concluded that the MMPI-2, when results were evaluated through machine learning, provided reliable accuracy in classifying and predicting suicidal ideation and past suicidal attempts.
Researchers recommended that clinicians could use the MMPI to help detect and treat groups with a high risk of suicide.
The MMPI will probably never receive total approval or total disapproval. It’s one tool within a large diagnostic toolbox, and it’s constantly being reviewed and revised.
It will continue to be tweaked and analyzed, and most likely always be a work in progress.
In the book “Of Psychometric Means: Starke R. Hathaway and the Popularization of the Minnesota Multiphasic Personality Inventory,” authors Rebecca Schilling and Stephen T. Casper conclude that the MMPI gives behavioral health professionals a starting point from which to build diagnoses and initiate treatment.
They point out that the MMPI can also help test takers to consider their mental health and better understand their own psychology.
Consider speaking with a doctor or a mental health professional to help you determine which type of MMPI test best aligns with your unique mental health experience.
If you’re going to take the MMPI test, there really is no way to prepare. The best you can do is to be well rested for the test and answer the questions truthfully.
It’s also good to remember the test is designed to be a helping tool, one that can give both you and your mental health professionals a clearer vision of one precious and unique human personality.
Decoding and interpretation of the results of the MMPI test (SMIL)
First, I would like to make a few rather important remarks about working with the MMPI test and its Russian adaptations and derivatives.
First of all, you should not use the Internet interpretation of the results or software versions of the test. You can use online and computer versions of the test only to calculate the results and build a profile. (For example, you can take psychological testing for free on my resource https://datest. ru/ or on https://www.psychol-ok.ru/statistics/mmpi/). The interpretation of the test results should be given by a specialist. The interpretation of the MMPI or SMIL test is primarily given according to the whole profile and according to the profile code, while the interpretation according to individual scales is used only in very specific cases. It has not yet been possible to carry out a decent automated interpretation due to the too great variability of the results. Professional interpretation of the test is hundreds of pages of text manuals with possible options. Both private clients and psychologists can order a professional interpretation of test results.
ru/ or on https://www.psychol-ok.ru/statistics/mmpi/). The interpretation of the test results should be given by a specialist. The interpretation of the MMPI or SMIL test is primarily given according to the whole profile and according to the profile code, while the interpretation according to individual scales is used only in very specific cases. It has not yet been possible to carry out a decent automated interpretation due to the too great variability of the results. Professional interpretation of the test is hundreds of pages of text manuals with possible options. Both private clients and psychologists can order a professional interpretation of test results.
The second problem with the interpretation of the results is the lack of information. There are only a few sources in Russian, and the information presented in them is too laconic. There are a significant number of publications in English on various aspects of the use of the test in various aspects: in clinical practice, in psychological counseling, in forensic psychological examination, professional selection, etc.
The third problem: the preparedness of specialists. Very often one hears from both psychologists and psychiatrists that the test "does not work", that it is "outdated", that it is only "for psychiatric patients", etc. Unfortunately, such judgments stem only from a lack of familiarity with the original literature on MMPI and world experience in the application of the test. I also want to say that it is impossible to fully master the methodology of working with the test without conducting many, many studies, receiving feedback from the subjects. I had to work with the test for three years, doing several thousand examinations, before I could tell myself that I began to understand the nuances of scoring and interpreting the results.
So, let's get down to business! To interpret the profiles of MMPI, SMIL (L.N. Sobchik, 566 questions), MMIL (F.B. Berezin, 377 statements), SKLO (383 questions), MLO (165 statements), it is recommended to perform the following eight steps. Each stage of assessment and interpretation should be carried out taking into account demographic variables such as age, profession, cultural and intellectual level, education, social class.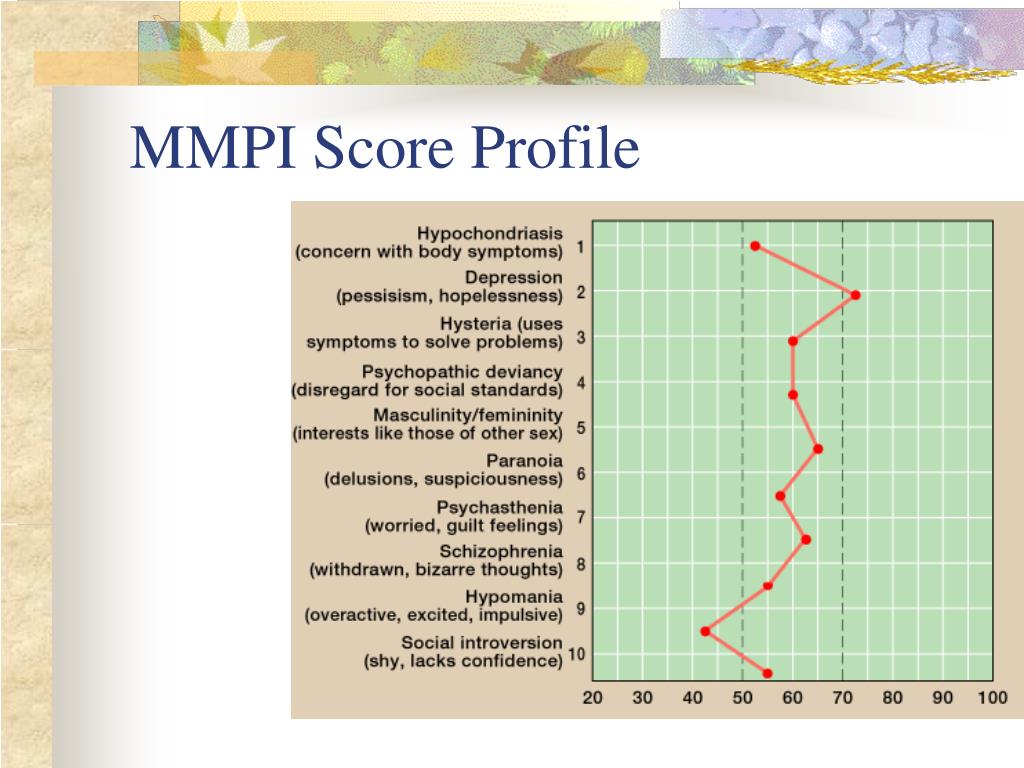
Step 1. Estimate the time spent on the test.
The examiner should note the length of time spent on the MMPI test. For a person over 16 years of age, with at least 8 grades, in a state of moderate excitement with an average IQ, the total time to complete the MMPI or SMIL method should be approximately 90 minutes. The computer version of the tests usually takes 15-30 minutes less (60 to 75 minutes in total). If the subject spends more than 2 hours on the test on the form (more than 1 hour 45 minutes on the computer version), the following aspects should be considered when interpreting the test results:
- Serious psychopathological problems such as severe depression or psychosis.
- Obsessive indecision.
- Below average IQ or poor reading ability as a result of insufficient education.
- Organic lesions of the brain.
If, on the other hand, the subject completes the test in less than an hour, an invalid profile (the subject knows how to "pass" the test), increased impulsivity, a state of hypomania, or a combination of these factors can be suspected.
On blank methods, pay attention to any erasures or pencil dots on the answer sheet. The presence of several of these signs can indicate that the person took the test seriously, which reduces the chance of random answers. A large number of erasures may reflect obsessive-compulsive tendencies.
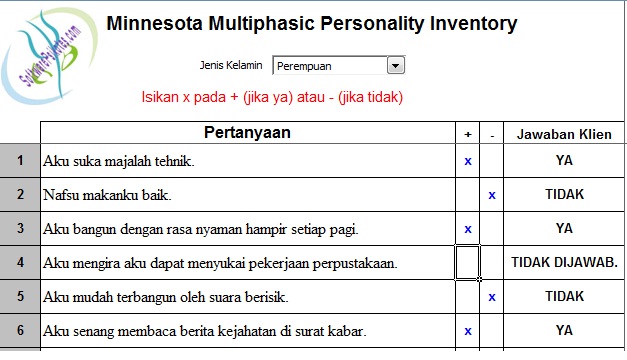
Step 2. Building a profile based on scoring (or obtaining a finished profile during computer testing).
Computer-aided tests may provide information about missing statements, statements for which the answers were changed, or the response time exceeded twice the standard deviation of the mean. On the forms, it is worth paying attention to statements for which the answers were omitted, changed, or the answer contains additional pencil marks. It is important to clarify whether the subject understood the content of these statements, giving answers, or avoiding answers. Discussing with the client or patient the reasons why they chose not to respond to certain statements or why they took so long to answer may shed additional light on how the person functions psychologically and what areas of functioning may be critical for them.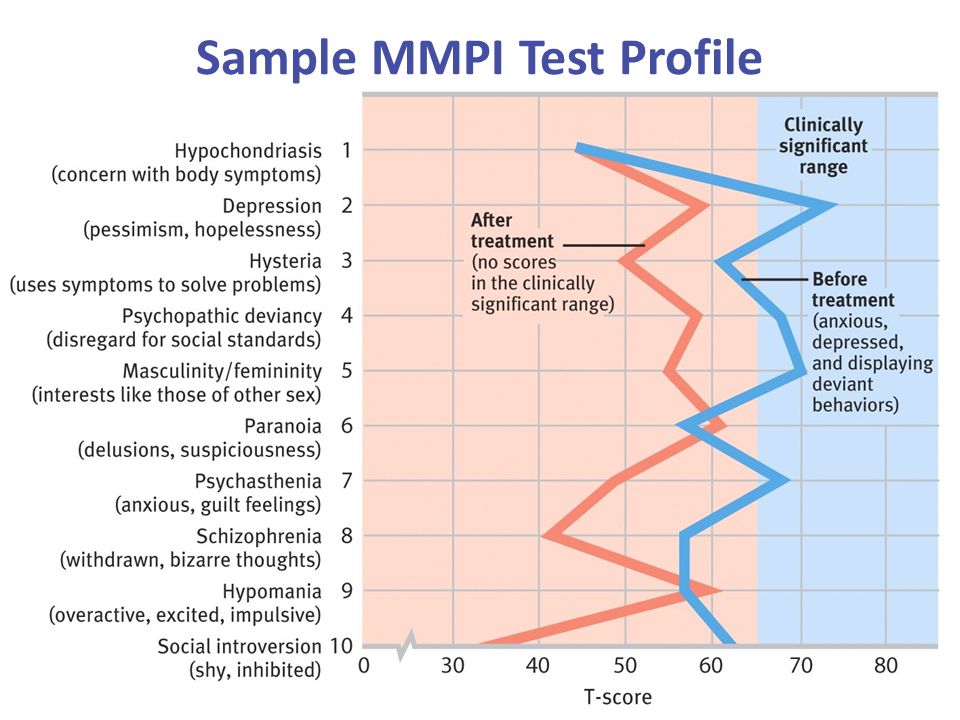
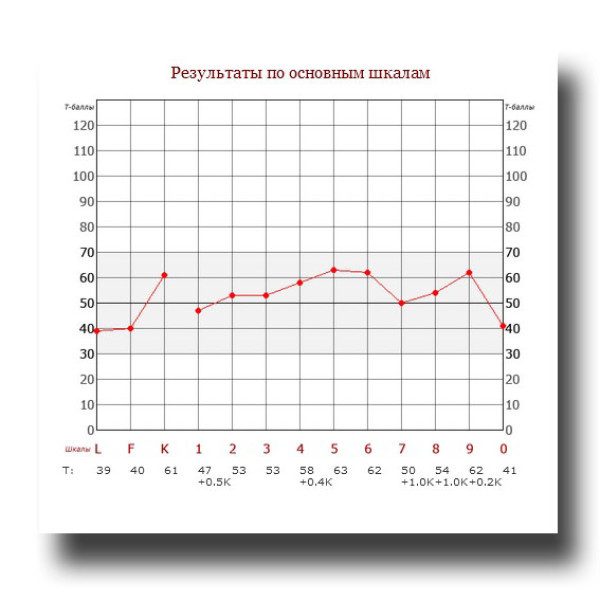
Step 3. Profile evaluation and determination of 1, 2 or 3 peak profile code.
For each of the scales, a T-score value is recorded according to their order (L, F, K, 1, 2, 3, etc.) with their T-scores to the right of those scales. Next, the profile code type is defined. Peaks are considered the highest heights of the scales, except for the 5 MF (masculine-feminine) and 0 SI (social introversion) scales, which are not strictly clinical scales and are not used in determining the type of code. For example, the highest scores in a profile may have scales of 8 and 7, which may give a code type of 87 or 78. The order of the scales in the two- and three-peak code types does not matter (for example, code 13 and code 31 have the same interpretation). Therefore, in the reference part for interpretation, the code type is written as 87/78. With a leading rise of three scales, the code is written as 123/213/231 or 132/312.
Well-differentiated profiles are profiles that have one, two or three scale peaks, with a significant difference between the indicators of other competing scales.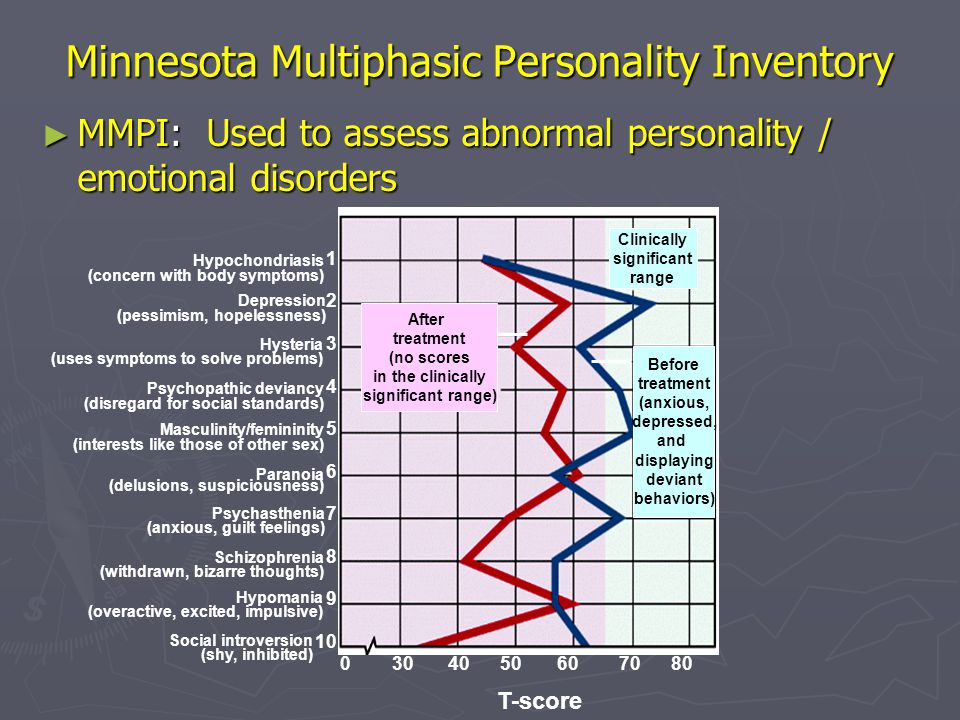
Note that only profiles in which the increase in scale scores exceeds 69 T-points (MMPI, SMIL) or 64 T-points (MMPI-2) can be completely reliably interpreted from the code, and the difference in the scores of the highest scales is at least 5 T-points. Profiles with these scores are more likely to be stable over time (high test-retest reliability).
When scales in well-differentiated code types are elevated (greater than 69 T-scores for MMPI or SMIL, or 64 T-scores for MMPI-2), both symptoms of impairment and personality descriptors are included in the interpretation. It is permissible to take into account the interpretation by two and three peak profile codes if the scale values lie in the area of character accentuations (exceeds 59 T-scores). When scales in well-differentiated types do not exceed the critical level, only personality descriptors, not symptoms, are included in the interpretation. Decryption interpretations must be modified by either lowering the descriptors to a more normal level or removing more extreme descriptors.
Less clearly differentiated profiles should be interpreted by noting each elevated scale and then integrating the values obtained from the various scale descriptors.
An example of deciphering a poorly differentiated profile MMPI.
If the profile is poorly defined due to the presence of additional scales that “compete” with the peak scales in the code type (e.g. code type 27/72, but with scales 1 and 8 also raised almost as high as scales 2 and 7), several strategies need to be used. The safest and most conservative strategy for deciphering and interpreting is to consider the descriptors that occur among all the various elevated scales. For example, anxiety is highly likely to be a common descriptor for elevated scales 1, 2, 7, and 8. Anxiety tendencies are increased if the 7th scale is the most elevated. In addition, the psychologist needs to make an effort to understand and integrate the interpretations given within each of the individual scale descriptions. In addition, it is necessary to take into account and integrate the values of alternative combinations of code types (for example, if all scales 2, 7, 1 and 8 are increased, then the following two-peak code type descriptors must be considered: 27/72, 18/81, 87/78, 12/ 21, 17/71, and another 28/82).
Step 4. Determining the validity of the personality profile.
It is necessary to evaluate the validity of the MMPI profile (MMPI) based on the validity scales. There are a number of indicators that indicate invalid profiles. For example, a frequently encountered defensive (defensive) profile style, in which existing problems are hidden or minimized, is characterized by an increase in the L scale of lies and / or the K scale. A profile in which existing problems are exaggerated is characterized by an increase in the F scale. influence: poor reading comprehension, random answers, psychotic state, high level of infantilism, desire to simulate mental pathology, high level of stress and desire to draw attention to one's problems. In addition, the psychologist must take into account the following factors: the context of the assessment, in order to determine whether, during conversation and observation, the defensive type of responses identified on the scales of validity, the deliberate worsening of results, or the giving of random responses are confirmed. In particular, the assessor must determine the likelihood that the subject would potentially benefit from overestimating or underestimating psychopathology.
In addition, the psychologist must take into account the following factors: the context of the assessment, in order to determine whether, during conversation and observation, the defensive type of responses identified on the scales of validity, the deliberate worsening of results, or the giving of random responses are confirmed. In particular, the assessor must determine the likelihood that the subject would potentially benefit from overestimating or underestimating psychopathology.
Step 5. Determining the general level of adaptation - disadaptation.
Note the number of scales over 64 T-scores (for MMPI-2) or over 69 T-scores (for MMPI, SMIL, MMIL) and the relative height of these scales. The degree of elevation of the F scale can also be an excellent indicator of the degree of pathology, provided that it is not so high as to indicate an invalid profile (95 T-points for men and 99 T-points for women. For psychiatric patients - 120 T-points for men and 119T-scores for women).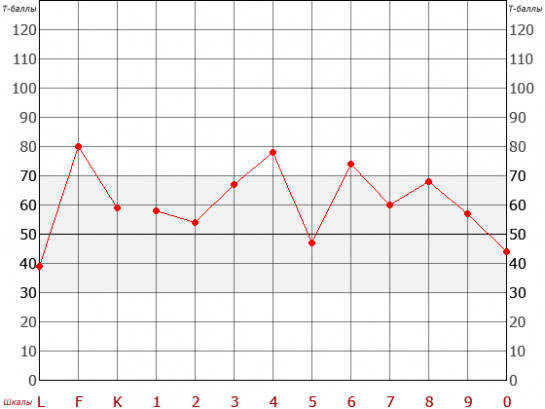 The greater the number and relative height of these scales, the more likely the individual will experience difficulty performing basic duties and experience social and personal discomfort.
The greater the number and relative height of these scales, the more likely the individual will experience difficulty performing basic duties and experience social and personal discomfort.
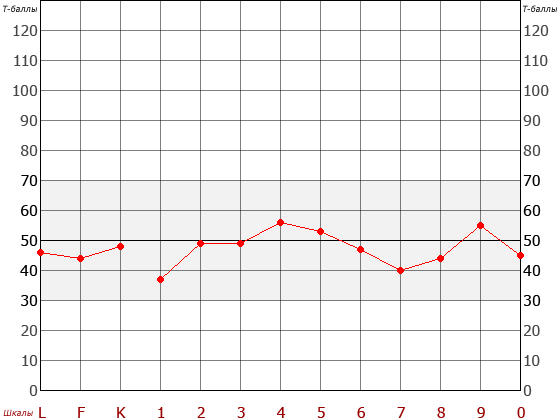
The normal profile of an adapted person is at the average level, and most of the scales lie in the range of 45-65 (70) T-scores.
A low-lying profile, where the main scales lie below the level of 50 T-scores, and is accompanied by low F-scale indicators and an increase in the K-scale, indicates an overstrain of the adaptation system due to the action of a stressful situation. The subject seeks to deny the existing problems or symptoms (especially on scales with a minimum level: one of the most common options is an underestimated 6th scale with the denial of hostility and distrust of people). In the dynamics of the development of the situation, a disruption and breakdown of the adaptation system is very likely if psychological assistance is not provided in time.
Step 6. Description of symptoms, behavior and personality characteristics.

This step is the basic process of transcribing and interpreting the results of the MMPI test.
Moderate rises on the scales (T = 60-65(70)) reflect the sharpening of character traits (personal accentuation) of the subject in the transition zone between mental norm and pathology. Interpretations in these cases should be treated with caution, with more extreme descriptors including psychopathological symptoms removed or rephrased to describe milder characteristics.
An increase in the scales above 65 (70) T-points to a greater extent reflect the characteristic constants for the subject of the main features of the functioning of the personality. However, it can be misleading to base interpretations solely on specific T-scores, as client demographics (age, nationality, educational level, class, occupation) often have a strong influence on results.
Different authors use different criteria to determine high and low profile scores. Some authors use T-score ranges (eg, T = 70-80), others define elevated scores as the top quartile, and still others define upscales as the highest score in the profile, regardless of the specific T-score value.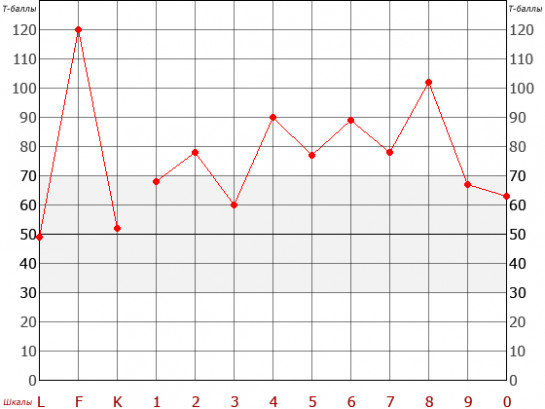 Most often, descriptors are not tied to specific values of T-scores during interpretation. Instead, more general descriptions are given related to high and low scores. The psychologist must independently interpret the accuracy of these potential values, taking into account not only the height of the scales, but also other relevant variables. In addition, each of the scale descriptions is modal. The descriptions should be considered as possible interpretations that will not necessarily apply to all individuals who score on certain scales. These are just hypotheses in theory that need further testing. That is why up to 40% of automated computer interpretations created without the participation of a psychologist evaluating a particular subject are not confirmed. Specific ranges of T-scores are evaluated only for validity scales (L,F,K).
Most often, descriptors are not tied to specific values of T-scores during interpretation. Instead, more general descriptions are given related to high and low scores. The psychologist must independently interpret the accuracy of these potential values, taking into account not only the height of the scales, but also other relevant variables. In addition, each of the scale descriptions is modal. The descriptions should be considered as possible interpretations that will not necessarily apply to all individuals who score on certain scales. These are just hypotheses in theory that need further testing. That is why up to 40% of automated computer interpretations created without the participation of a psychologist evaluating a particular subject are not confirmed. Specific ranges of T-scores are evaluated only for validity scales (L,F,K).
In the process of interpreting the results, one should not just note the values of individual scales, but also study the overall structure or configuration of the profile, noting the relative peaks and troughs in its configuration. Typical configurations, for example, might include a “conversion V,” reflecting possible conversion disorder, or elevated scales of 4 and 9, which reflect a high likelihood of physical aggression. Any scales greater than 65 (70) or reduced below 40 (45) T-scores should be noted as they are particularly important for overall interpretation. When deciphering the meaning of a profile with two or more elevated clinical scales, it is recommended that the psychologist take into account both the descriptors for the individual scales and the corresponding descriptions of the two- and three-peak profile codes. It is also recommended that when interpreting individual scales, the psychologist use not only the values for high and low scores, but also more general information on the corresponding scale. Here you can see information about the specific indicators of the MMPI test and the assessment of the interaction of some scales when deciphering the profile.
Typical configurations, for example, might include a “conversion V,” reflecting possible conversion disorder, or elevated scales of 4 and 9, which reflect a high likelihood of physical aggression. Any scales greater than 65 (70) or reduced below 40 (45) T-scores should be noted as they are particularly important for overall interpretation. When deciphering the meaning of a profile with two or more elevated clinical scales, it is recommended that the psychologist take into account both the descriptors for the individual scales and the corresponding descriptions of the two- and three-peak profile codes. It is also recommended that when interpreting individual scales, the psychologist use not only the values for high and low scores, but also more general information on the corresponding scale. Here you can see information about the specific indicators of the MMPI test and the assessment of the interaction of some scales when deciphering the profile.
Step 7. Providing psychological and medical diagnostic hypotheses
It is not acceptable to use data from only one test to make a psychological diagnosis without confirming or eliminating diagnostic hypotheses by the results of a carefully selected battery of complementary tests and, of course, observation and conversation.
Although MMPI or SMIL test results cannot be directly used to make a medical (psychiatric) diagnosis using pathopsychological research techniques in clinical psychology, they can often make a significant contribution to information related to diagnostic formulations. The current literature on MMPI-2, in describing the types of two- and three-peak profile codes, contains possible DSM-V diagnoses corresponding to each type of profile code. Clinicians can consider these, along with available additional diagnostic information, to make an accurate diagnosis. In non-medical contexts, the formulation of a psychopathological diagnosis would be neither necessary nor appropriate.
Step 8. Forecast of therapy success, feedback and recommendations
Psychodiagnostics in itself is one of the types of psychological assistance provided to a client or patient. Often one of the most valuable services that a psychologist can provide, both for clinicians and for the subject himself, is to predict the likelihood of benefit from a planned intervention. This usually means identifying the strengths and weaknesses of the functioning of the human psyche, the types of psychological protection used, the ability to form a therapeutic alliance, the predicted response to psychotherapy, possible antisocial tendencies and the level of self-awareness.
This usually means identifying the strengths and weaknesses of the functioning of the human psyche, the types of psychological protection used, the ability to form a therapeutic alliance, the predicted response to psychotherapy, possible antisocial tendencies and the level of self-awareness.
Based on the test results, the psychologist can additionally provide suggestions for tailoring specific interventions for the client, based on their profile and the types of problems and difficulties they experience.
In addition, providing the client with clear, relevant feedback describing specific issues of both the current state and previous life experience, as well as suggesting ways for psychological self-help and self-development, has a therapeutic effect.
What information about the subject can be obtained by analyzing the personality profile?
- General level of social and psychological adaptation
- Presence of possible pathopsychological features, their structure, degree of their severity
- Likely complaints
- The need to consult a mental health specialist, provide psychological assistance (issues of psychological support of professional activities to achieve optimal performance and professional longevity).
- Signs of burnout
- Assessment of the level of stress resistance, identification of critical stressors.
- Major sources of stress and frustration
- Basic psychological defenses and coping strategies
- Identification of likely signs of deviant behavior, addictions, the likelihood of disloyal, illegal and criminal behavior.
- The likelihood of counterproductive behavior in the workplace.
- Description of habitual patterns of behavior in normal and critical stress situations.
- The most characteristic personality traits.
- Features of the emotional sphere, dominant emotions,
- Dominant thoughts.
- Characteristic behavioral markers
- Features of education in the parental family
- Probable experienced psychotraumas of childhood and adolescence.
- Possible recent trauma.
- "Strong" (adaptive) sides of personality
- "Weak" (maladaptive) aspects of personality
- Basic needs
- Leading professional qualities
- Missing professionally important qualities
- Optimum suitability by area of engagement
- Unsuitability by areas of interaction
- Recommended occupational tasks
- Recommended and possible occupations
- Occupations not recommended
- Critical areas in professional activity
- Recommendations for interaction in the labor collective
- Recommendations for optimal management style
- Recommendations for optimal working conditions
- Recommended types of psychological assistance, recommendations on the mode of work and rest.

Sample report from my automated testing system.
For private clients interpretation of the results of the MMPI test can help in understanding yourself, see the main internal conflicts and habitual ways of coping with problems, understand the causes of psychological difficulties and problems in communicating with other people, life failures. Recommendations for psychological self-help may be included in the interpretation. Also, interpretation can help to choose the optimal professional activity and work style.
An example of MMPI interpretation for a client (PDF)
For practicing psychologists interpretation allows you to probabilistically assess the presence of certain pathopsychological syndromes in clients, understand the basics of internal conflicts, possible traumas of childhood and adolescence, select the best approaches in therapy, and predict their success and track progress in therapy.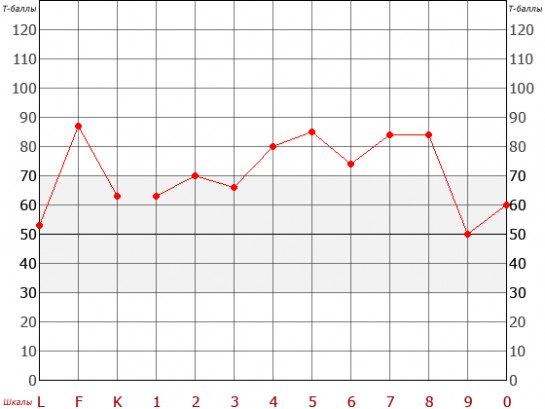
Psychology Test Interpretation Example (PDF)
Description of the MMPI test scales (SMIL)
L - False F - Reliability K - Correction 1 - Hypochondria 2 - Depression 3 - Hysteria 4 - Psychopathy 6 - Paranoia 9 - Psychiasthenia 8 - Introversion
Literature
Groth-Marnat G. Handbook of psychological assessment. John Wiley & Sons, Inc., Hoboken, New Jersey.- 2003.-PP. 231-239.
Andrey Demkin
MMPI®-2 (Minnesota Multifactorial Personality Inventory® - 2) in personality psychodiagnostics. Basic course.
Official recognition of the Russian-language version of MMPI®-2 by the University of Minnesota is a guarantee that its psychometric indicators correspond to the original.
Course requirements
Higher education in psychology or higher medical education with retraining in psychology or psychotherapy.
Rasskazova Elena Igorevna
Author and course leader
Clinical psychologist, Ph. D. Lomonosov, Senior Researcher, Department of Medical Psychology, Mental Health Research Center. Cognitive therapist (Diploma of the Academy of Cognitive Therapy, Philadelphia, USA). Author of more than 200 scientific publications in the field of clinical psychology, health psychology, self-regulation and statistical methods of data processing. Co-leader of the MMPI-2 approbation project in Russia, officially approved by the University of Minnesota.
D. Lomonosov, Senior Researcher, Department of Medical Psychology, Mental Health Research Center. Cognitive therapist (Diploma of the Academy of Cognitive Therapy, Philadelphia, USA). Author of more than 200 scientific publications in the field of clinical psychology, health psychology, self-regulation and statistical methods of data processing. Co-leader of the MMPI-2 approbation project in Russia, officially approved by the University of Minnesota.
Curriculum:
- Scopes and capabilities of different versions of MMPI (MMPI-2, MMPI-A, MMPI-RF, MMPI-A-RF), as well as the reasons for its reliability, validity and reliability when applied to various tasks.
- The structure of the methodology, the content and basics of interpretation of validity scales, main and restructured clinical scales, subscales, content and additional scales, as well as the basis for the analysis of critical sets of items. Features of the practical application of the Russian version of MMPI®-2.
- Possibilities and rules for the use of MMPI®-2 in various areas of personality psychodiagnostics: in clinical and psychological diagnostics, expertise, psychotherapy, psychological counseling, in organizational, sports, military psychology.
- Requirements for the implementation of the methodology, methods for identifying invalid protocols and actions with them.
- Fundamentals of the interpretation of uniform T-scores and their boundary values for diagnosis in clinical and non-clinical settings.
- Basic rules for the interpretation of personality profiles, taking into account profiles on restructured, meaningful and additional scales when conducting psychodiagnostics with different tasks and in different (clinical and non-clinical) conditions.
- Requirements for discussing the results of psychodiagnostics with other professionals (medical professionals, employers, teachers, etc.).
- Methods for discussing the results of psychodiagnostics with clients, patients and their families.
 The use of MMPI®-2 in psychological counseling.
The use of MMPI®-2 in psychological counseling.
The course meets the requirements for practical development and basic application of the three guidelines: "MMPI®-2 (Minnesota Multivariate Personality Inventory® - 2): a guide to application, processing of indicators and interpretation" (Butcher et al., 2001)
-
- Restructured Clinical Scales (RF) MMPI-2: Design, Validity and Interpretation (Tellegen et al., 2008) Porah, Graham, Tellegen, 2009).
After completing the training, you will be given access to your personal account for online purchase and administration of tests.
"Specialist"
17000 ₽
-
Access to course materials for 3 months
-
Certificate of passing the examination test
-
Access to the electronic version of the MMPI-2 test
-
1 free MMPI-2 test
-
Entry into the register of certified specialists on the website giuntipsy.
 ru
ru
-
*Possibility to purchase supervision for an additional fee
Start learning
"Professional"
21000 ₽
-
Access to course materials for 6 months
-
Certificate of passing the examination test
-
Access to the electronic version of the MMPI-2 test
-
2 free MMPI-2 tests
-
Entry into the register of certified specialists on the website giuntipsy.ru
-
1 supervision in a mini-group (3-5 people) with analysis of your case
Start training
"Master"
28000 ₽
-
Access to course materials for 12 months
-
Certificate of passing the examination test
-
Access to the electronic version of the MMPI-2 test
-
3 free MMPI-2 tests
-
Entry into the register of certified specialists on the website giuntipsy.