Mental disorder split personality
Causes, Symptoms, Types & Treatment
Overview
What is delusional disorder?
Delusional disorder is a type of psychotic disorder. Its main symptom is the presence of one or more delusions.
A delusion is an unshakable belief in something that’s untrue. The belief isn’t a part of the person’s culture or subculture, and almost everyone else knows this belief to be false.
People with delusional disorder often experience non-bizarre delusions. Non-bizarre delusions involve situations that could possibly occur in real life, such as being followed, deceived or loved from a distance. These delusions usually involve the misinterpretation of perceptions or experiences. In reality, these situations are either untrue or are highly exaggerated.
Non-bizarre delusions are different from bizarre delusions, which include beliefs that are impossible in our reality, such as believing someone has removed an organ from your body without any physical evidence of the procedure.
People with delusional disorder often continue to socialize and function well, apart from the subject of their delusion. Generally, they don’t behave in an odd or unusual manner. This is unlike people with other psychotic disorders, who might also have delusions as a symptom. In some cases, however, people with delusional disorder might become so preoccupied with their delusions that their lives are disrupted.
What are the types of delusional disorder?
There are different types of delusional disorder, which are determined based on the main theme of the delusions the person experiences. The types of delusional disorder include:
- Erotomanic: People with this type of delusional disorder believe that another person, often someone important or famous, is in love with them. They may attempt to contact the person of the delusion and engage in stalking behavior.
- Grandiose: People with this type of delusional disorder have an overinflated sense of self-worth, power, knowledge or identity.
 They may believe they have a great talent or have made an important discovery.
They may believe they have a great talent or have made an important discovery. - Jealous: People with this type of delusional disorder believe that their spouse or sexual partner is unfaithful without any concrete evidence.
- Persecutory: People with this type of delusional disorder believe someone or something is mistreating, spying on or attempting to harm them (or someone close to them). People with this type of delusional disorder may make repeated complaints to legal authorities.
- Somatic: People with this type of delusional disorder believe that they have a physical issue or medical problem, such as a parasite or a bad odor.
- Mixed: People with this type of delusional disorder have two or more of the types of delusions listed above.
What is the difference between delusional disorder and schizophrenia?
Schizophrenia is a spectrum (or range) of conditions that involve psychotic symptoms, which include:
- Disorganized speech or behavior.

- Negative symptoms (a decrease in emotion in a person’s facial expressions and motivation).
Delusional disorder is different from schizophrenia because there aren’t any other psychotic symptoms other than delusions.
In addition, in contrast to schizophrenia, delusional disorder is relatively rare, and daily functioning isn’t as impaired as it is in schizophrenia.
Who does delusional disorder affect?
Delusional disorder most often occurs in middle to late life, with the average age of onset being 40 years.
The persecutory and jealous types of delusional disorder are more common in people assigned male at birth (AMAB), and the erotomanic type is more common in people assigned female at birth (AFAB).
People who tend to be socially isolated are more likely to develop delusional disorder. These populations include:
- Immigrants who have language barriers.
- People who are deaf.
- People who are visually impaired.
- Elderly people.
How common is delusional disorder?
Although delusions might be a symptom of more common disorders, such as schizophrenia, delusional disorder itself is rather rare. Approximately 0.05% to 0.1% of the adult population has delusional disorder.
What is the most common type of delusional disorder?
The most common type of delusional disorder is the persecutory type — when someone believes others are out to harm them despite evidence to the contrary.
Symptoms and Causes
What are the signs and symptoms of delusional disorder?
The presence of delusions is the most obvious sign of delusional disorder, which vary based on the type.
Another characteristic of this condition is that the person often lacks self-awareness that their delusions are problematic. They’re unable to accept that their delusions are irrational or inaccurate, even if they recognize that other people would describe their delusions this way.
Anger and violent behavior may be present if someone is experiencing persecutory, jealous or erotomanic delusions.
People with delusional disorder may also develop anxiety and/or depression as a result of the delusions.
Early symptoms of delusional disorder may include:
- Feelings of being exploited.
- Preoccupation with the loyalty or trustworthiness of friends.
- A tendency to read threatening meanings into benign remarks or events.
- Persistently holding grudges.
- A readiness to respond and react to perceived slights.
What causes delusional disorder?
As with many other psychotic disorders, researchers don’t yet know the exact cause of delusional disorder. Researchers are, however, looking at the role of various factors that may contribute to the development of the condition, including:
- Genetic factors: The fact that delusional disorder is more common in people who have family members with delusional disorder or schizophrenia suggests there might be a genetic factor involved. Researchers believe that, as with other mental disorders, a tendency to develop delusional disorder might be passed on from parents to their biological children.

- Biological factors: Researchers are studying how abnormalities of certain areas of your brain might be involved in the development of delusional disorder. An imbalance of certain chemicals in your brain, called neurotransmitters, has been linked to the formation of delusional symptoms.
- Environmental and psychological factors: Evidence suggests that delusional disorder can be triggered by stress. Alcohol use disorder and substance use disorder might contribute to the condition. Hypersensitivity and ego defense mechanisms like reaction formation, projection and denial are some psychodynamic theories for the development of delusional disorder. Social isolation, envy, distrust, suspicion and low self-esteem are also some psychological factors that may lead to a person seeking an explanation for these feelings and, thus, forming a delusion as a solution.
Diagnosis and Tests
How is delusional disorder diagnosed?
Healthcare providers — mainly mental health professionals — diagnose delusional disorder when a person has one or more delusions for one month or more that can’t be explained by any other condition. The person must also not have the characteristic symptoms of other psychotic disorders, such as schizophrenia.
The person must also not have the characteristic symptoms of other psychotic disorders, such as schizophrenia.
If someone is experiencing signs and symptoms of delusional disorder, a healthcare provider will perform a complete medical history and physical examination. Although there aren’t any laboratory tests to diagnose delusional disorder, their healthcare provider might use various diagnostic tests — such as imaging tests, a urine drug screen and blood tests — to rule out any physical conditions, medications or substances that could be causing the symptoms.
If their healthcare provider finds no physical reason for the symptoms, a consultation with a psychiatrist or psychologist will likely be made. Psychiatrists and psychologists use specially designed interview and assessment tools to evaluate a person for a psychotic disorder. They’ll ask questions about the delusions and assess the person’s mental status.
The psychiatrist or psychologist may also interview family members and friends so they can provide further details about the person’s delusions and a timeline of the symptoms.
As other mental health conditions can cause delusions, mental health professionals carefully assess the person for other symptoms. Delusional disorder can be misdiagnosed as any of the following conditions:
- Obsessive-compulsive disorder.
- Schizophrenia.
- Delirium/major neurocognitive disorder.
- Bipolar disorder.
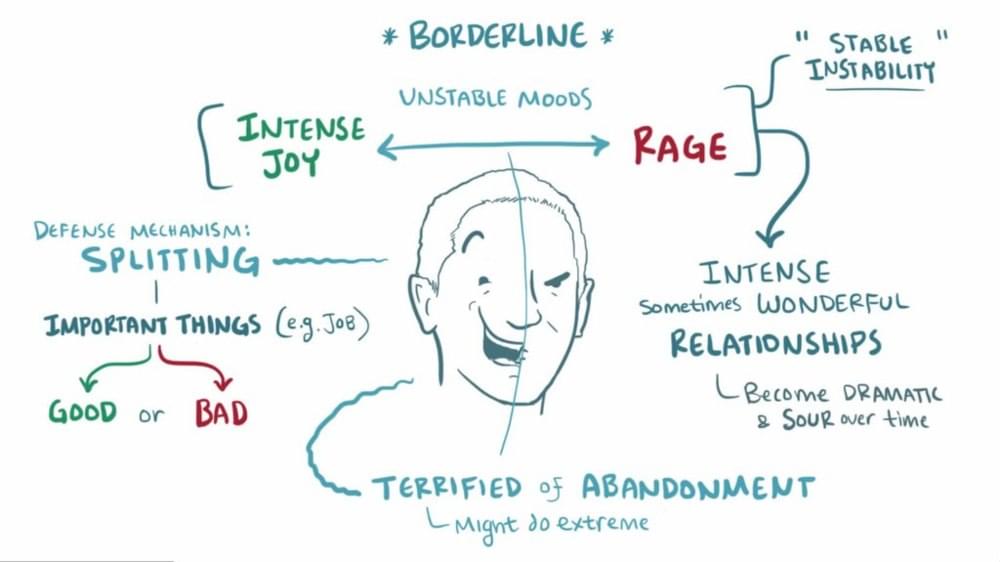
- Personality disorders, especially borderline personality disorder and paranoid personality disorder.
Management and Treatment
How is delusional disorder treated?
Treatment for delusional disorder most often includes psychotherapy (talk therapy) and medication, but delusional disorder is highly resistant to treatment with medication alone.
People with delusional disorder often don’t seek treatment for the condition on their own because most people with delusional disorder don’t realize their delusions are problematic or incorrect. It’s more likely they’ll seek help due to other mental health conditions such as depression or anxiety.
People with severe symptoms or who are at risk of hurting themselves or others might need to be admitted to the hospital until the condition is stabilized.
Psychotherapy for delusional disorder
Psychotherapy is a term for a variety of treatment techniques that aim to help people identify and change troubling emotions, thoughts and behaviors. Working with a mental health professional, such as a psychologist or psychiatrist, can provide support, education and guidance to the person and their family.
Through therapy, people with delusional disorder can learn to manage their symptoms, identify early warning signs of relapse and develop relapse prevention plans. Types of psychotherapy include:
- Individual psychotherapy: This type of therapy can help a person recognize and correct the underlying thinking that has become distorted.
- Cognitive behavioral therapy (CBT): This is a structured, goal-oriented type of therapy.
 A mental health professional helps people take a close look at their thoughts and emotions. They’ll come to understand how their thoughts affect their actions. Through CBT, they can unlearn negative thoughts and behaviors and learn to adopt healthier thinking patterns and habits.
A mental health professional helps people take a close look at their thoughts and emotions. They’ll come to understand how their thoughts affect their actions. Through CBT, they can unlearn negative thoughts and behaviors and learn to adopt healthier thinking patterns and habits. - Family-focused therapy: This therapy can help people with delusional disorder and their families. This treatment involves psychoeducation regarding delusional disorder, communication improvement training and problem-solving skills training.
Medications for delusional disorder
The primary medications used to help treat delusional disorder are called antipsychotics (neuroleptics). Medications include the following:
- First-generation (“typical”) antipsychotics: Healthcare providers have used these medications to treat mental health conditions since the mid-1950s. These medicines work by blocking dopamine receptors in your brain. Dopamine is a neurotransmitter believed to be involved in the development of delusions.
 First-generation antipsychotics include chlorpromazine (Thorazine®), fluphenazine (Prolixin®), haloperidol (Haldol®), thiothixene (Navane®), trifluoperazine (Stelazine®), perphenazine (Trilafon®) and thioridazine (Mellaril®).
First-generation antipsychotics include chlorpromazine (Thorazine®), fluphenazine (Prolixin®), haloperidol (Haldol®), thiothixene (Navane®), trifluoperazine (Stelazine®), perphenazine (Trilafon®) and thioridazine (Mellaril®). - Second-generation (“atypical”) antipsychotics: These newer antipsychotics are also effective in treating the symptoms of delusional disorder. They work by blocking dopamine and serotonin receptors in your brain. These drugs include risperidone (Risperdal®), clozapine (Clozaril®), quetiapine (Seroquel®), ziprasidone (Geodon®) and olanzapine (Zyprexa®). These medications are usually better tolerated than first-generation antipsychotics.
Other medications that healthcare providers might prescribe to treat delusional disorder include anxiolytics and antidepressants. Anxiolytics might help if the person has a very high level of anxiety and/or problems sleeping. Antidepressants can help treat depression, which often occurs in people with delusional disorder.
Prevention
Can delusional disorder be prevented?
There’s no known way to prevent delusional disorder. However, early diagnosis and treatment can help decrease the disruption to the person’s life, family and friendships.
Outlook / Prognosis
What is the prognosis (outlook) for delusional disorder?
The prognosis (outlook) for people with delusional disorder varies depending on a few factors, including:
- The type of delusional disorder.
- The severity of the delusions.
- The person’s life circumstances, including the availability of support and a willingness to stick with treatment.
Delusional disorder doesn’t usually significantly affect a person’s daily functioning, but the severity of the delusion may gradually get worse. Most people with delusional disorder can remain employed as long as their work doesn’t involve things related to their delusions.
The prognosis of delusional disorder is better if the person sticks to their treatment plan. Almost 50% of people have a full recovery, more than 20% of people report a decrease in symptoms and less than 20% of people report minimal to no change in symptoms.
Almost 50% of people have a full recovery, more than 20% of people report a decrease in symptoms and less than 20% of people report minimal to no change in symptoms.
Unfortunately, many people with this condition don’t seek help. It’s often difficult for people with mental health conditions to recognize they’re not well. They also might be too embarrassed or afraid to seek treatment. Without treatment, delusional disorder can be a life-long condition.
What are the possible complications of delusional disorder?
If left untreated, delusional disorder might lead to:
- Depression, often as a consequence of difficulties associated with the delusions.
- Social isolation.
- Legal issues — for example, stalking or harassing the person involved with the delusion could lead to arrest.
- Self-harm or harm to others. This is more common in the jealous and persecutory types.
Living With
How can I help someone with delusional disorder?
If you know someone with delusional disorder, you can help by providing support and encouragement for them to seek help and treatment.
People with delusional disorder who feel pressured or repeatedly criticized by others will likely experience stress, which may worsen their symptoms. Because of this, a positive approach may be more helpful and effective.
The friends and family members of people with delusional disorder often experience stress, depression, grief and isolation. It’s important to take care of your mental health and seek help if you’re experiencing these symptoms.
A note from Cleveland Clinic
It’s important to remember that delusional disorder is a mental health condition. As with all mental health conditions, seeking help as soon as symptoms appear can help decrease the disruptions to life. Mental health professionals can offer treatment plans that can help manage thoughts and behaviors.
Dissociative Identity Disorder (Multiple Personality Disorder): Signs, Symptoms, Treatment
Written by WebMD Editorial Contributors
In this Article
- What Is Dissociative Identity Disorder?
- Who Is At Risk for DID?
- How to Recognize Dissociative Identity Disorder and Its Associated Mental Disorders
- How Is Dissociative Identity Disorder Diagnosed?
- What Other Psychiatric Illnesses Might Occur With DID?
- Are There Famous People With Dissociative Identity Disorder?
- What's the Treatment Plan for Dissociative Identity Disorder?
Dissociative identity disorder (previously known as multiple personality disorder) is thought to be a complex psychological condition that is likely caused by many factors, including severe trauma during early childhood (usually extreme, repetitive physical, sexual, or emotional abuse).
What Is Dissociative Identity Disorder?
Dissociative identity disorder is a severe form of dissociation, a mental process which produces a lack of connection in a person's thoughts, memories, feelings, actions, or sense of identity. Dissociative identity disorder is thought to stem from a combination of factors that may include trauma experienced by the person with the disorder. The dissociative aspect is thought to be a coping mechanism -- the person literally shuts off or dissociates themselves from a situation or experience that's too violent, traumatic, or painful to assimilate with their conscious self.
Who Is At Risk for DID?
Research indicates that the cause of DID is likely a psychological response to interpersonal and environmental stresses, particularly during early childhood years when emotional neglect or abuse may interfere with personality development. As many as 99% of individuals who develop dissociative disorders have recognized personal histories of recurring, overpowering, and often life-threatening disturbances or traumas at a sensitive developmental stage of childhood (usually before age 6).
Dissociation may also happen when there has been persistent neglect or emotional abuse, even when there has been no overt physical or sexual abuse. Findings show that in families where parents are frightening and unpredictable, the children may become dissociative. Studies indicate DID affects about 1% of the population.
How to Recognize Dissociative Identity Disorder and Its Associated Mental Disorders
Dissociative identity disorder is characterized by the presence of two or more distinct or split identities or personality states that continually have power over the person's behavior. With dissociative identity disorder, there's also an inability to recall key personal information that is too far-reaching to be explained as mere forgetfulness. With dissociative identity disorder, there are also highly distinct memory variations, which may fluctuate.
Although not everyone experiences DID the same way, for some the "alters" or different identities have their own age, sex, or race. Each has their own postures, gestures, and distinct way of talking. Sometimes the alters are imaginary people; sometimes they are animals. As each personality reveals itself and controls the individuals' behavior and thoughts, it's called "switching." Switching can take seconds to minutes to days. Some seek treatment with hypnosis where the person's different "alters" or identities may be very responsive to the therapist's requests.
Each has their own postures, gestures, and distinct way of talking. Sometimes the alters are imaginary people; sometimes they are animals. As each personality reveals itself and controls the individuals' behavior and thoughts, it's called "switching." Switching can take seconds to minutes to days. Some seek treatment with hypnosis where the person's different "alters" or identities may be very responsive to the therapist's requests.
Other symptoms of dissociative identity disorder may include headache, amnesia, time loss, trances, and "out of body experiences." Some people with dissociative disorders have a tendency toward self-persecution, self-sabotage, and even violence (both self-inflicted and outwardly directed). As an example, someone with dissociative identity disorder may find themselves doing things they wouldn't normally do, such as speeding, reckless driving, or stealing money from their employer or friend, yet they feel they are being compelled to do it. Some describe this feeling as being a passenger in their body rather than the driver. In other words, they truly believe they have no choice.
In other words, they truly believe they have no choice.
There are several main ways in which the psychological processes of dissociative identity disorder change the way a person experiences living, including the following:
- Depersonalization. This is a sense of being detached from one's body and is often referred to as an "out-of-body" experience.
- Derealization. This is the feeling that the world is not real or looking foggy or far away.
- Amnesia. This is the failure to recall significant personal information that is so extensive it cannot be blamed on ordinary forgetfulness. There can also be micro-amnesias where the discussion engaged in is not remembered, or the content of a meaningful conversation is forgotten from one second to the next.
- Identity confusion or identity alteration. Both of these involve a sense of confusion about who a person is. An example of identity confusion is when a person has trouble defining the things that interest them in life, or their political or religious or social viewpoints, or their sexual orientation, or their professional ambitions.
 In addition to these apparent alterations, the person may experience distortions in time, place, and situation.
In addition to these apparent alterations, the person may experience distortions in time, place, and situation.
It is now acknowledged that these dissociated states are not fully mature personalities, but rather they represent a disjointed sense of identity. With the amnesia typically associated with dissociative identity disorder, different identity states remember different aspects of autobiographical information. There is usually a "host" personality within the individual, who identifies with the person's real name. Ironically, the host personality is usually unaware of the presence of other personalities.
How Is Dissociative Identity Disorder Diagnosed?
Making the diagnosis of dissociative identity disorder takes time. It's estimated that individuals with dissociative disorders have spent seven years in the mental health system prior to accurate diagnosis. This is common, because the list of symptoms that cause a person with a dissociative disorder to seek treatment is very similar to those of many other psychiatric diagnoses. In fact, many people who have dissociative disorders also have coexisting diagnoses of borderline or other personality disorders, depression, and anxiety.
In fact, many people who have dissociative disorders also have coexisting diagnoses of borderline or other personality disorders, depression, and anxiety.
The DSM-5 provides the following criteria to diagnose dissociative identity disorder:
- Two or more distinct identities or personality states are present, each with its own relatively enduring pattern of perceiving, relating to, and thinking about the environment and self.
- Amnesia must occur, defined as gaps in the recall of everyday events, important personal information, and/or traumatic events.
- The person must be distressed by the disorder or have trouble functioning in one or more major life areas because of the disorder.
- The disturbance is not part of normal cultural or religious practices.
- The symptoms cannot be due to the direct physiological effects of a substance (such as blackouts or chaotic behavior during alcohol intoxication) or a general medical condition (such as complex partial seizures).
The distinct personalities may serve diverse roles in helping the individual cope with life's dilemmas. For instance, there's an average of two to four personalities present when the patient is initially diagnosed. Then there's an average of 13 to 15 personalities that can become known over the course of treatment. Environmental triggers or life events cause a sudden shift from one alter or personality to another.
What Other Psychiatric Illnesses Might Occur With DID?
Along with the dissociation and multiple or split personalities, people with dissociative disorders may experience a number of other psychiatric problems, including symptoms:
- Depression
- Mood swings
- Suicidal tendencies
- Sleep disorders (insomnia, night terrors, and sleep walking)
- Anxiety, panic attacks, and phobias (flashbacks, reactions to stimuli or "triggers")
- Alcohol and drug abuse
- Compulsions and rituals
- Psychotic-like symptoms (including auditory and visual hallucinations)
- Eating disorders
Are There Famous People With Dissociative Identity Disorder?
Famous people with dissociative identity disorder include comedienne Roseanne Barr, Adam Duritz, and retired NFL star Herschel Walker.
Walker wrote a book about his struggles with DID, along with his suicide attempts, explaining he had a feeling of disconnect from childhood to the professional leagues. To cope, he developed a tough personality that didn't feel loneliness, one that was fearless and wanted to act out the anger he always suppressed. These "alters" could withstand the abuse he felt; other alters came to help him rise to national fame. Treatment helped Walker realize that these alternate personalities are part of dissociative identity disorder, which he was diagnosed with in adulthood.
What's the Treatment Plan for Dissociative Identity Disorder?
There are currently no formal, evidence-based guldelines to treat DID. Many treatments are based on case reports or are even controversial.
While there's also no "cure" for dissociative identity disorder, long-term treatment can be helpful, if the patient stays committed. Effective treatment includes:
- Psychotherapy: Also called talk therapy, the therapy is designed to work through whatever triggered and triggers the DID.
 The goal is to help “fuse” the separate personality traits into one consolidated personality that can control the triggers. This therapy often includes family members in the therapy.
The goal is to help “fuse” the separate personality traits into one consolidated personality that can control the triggers. This therapy often includes family members in the therapy. - Hypnotherapy. Used in conjunction with psychotherapy, clinical hypnosis can be used to help access repressed memories, control some of the problematic behaviors which accompany DID as well as help integrate the personalities into one.
- Adjunctive therapy. Therapies such as art or movement therapy have been shown to help people connect with parts of their mind that they have shut off to cope with trauma.
There are no established medication treatments for dissociative identity disorder, making psychologically-based approaches the mainstay of therapy. Treatment of co-occurring disorders, such as depression or substance use disorders, is fundamental to overall improvement. Because the symptoms of dissociative disorders often occur with other disorders, such as anxiety and depression, medicines to treat those co-occurring problems, if present, are sometimes used in addition to psychotherapy.
What is Dissociative Identity Disorder?
Dissociative Identity Disorder is a mental disorder characterized by either having two or more personalities, or a state of disconnection from the outside world, one's identity, and an inability to recall certain daily life events and important personal information. This disorder is often mistaken for depression, anxiety, or psychosis. Long before our days, this condition was called possession, and it was treated with exorcism. In the 19th century, this disorder was called hysteria, and in the 20th century it was called multiple personality disorder or multiple personality disorder.
Types of dissociative personality disorder
There are several types of dissociative disorders, which are characterized by different symptoms and manifestations. One of them is dissociative fugue, a disorder in which a person can find himself in a completely unfamiliar place and not remember how he got there. In this case, a person may forget some important information about himself and not even remember his name. At the same time, memory for some information, such as literature, science, and other things, can be preserved. In a state of fugue, a person assumes a different personality and identity with a different character, mannerisms and behavior. While in this identity, a person can lead an outwardly normal life. A dissociative fugue can last for hours or years. After that, a person may find himself in a completely unfamiliar place and at the same time not remember anything that happened to him in a state of fugue.
A person who has a dissociative disorder is actually suffering a lot from their condition.
Another type of dissociative disorder is the presence of several personalities in which a person finds himself in turn or simultaneously. At such moments, he disconnects from himself and stops feeling his own body, and also cannot see himself from the outside. Personalities within a person can have different ages, genders, nationalities, mental abilities, temperaments, and behave in completely different ways. Often these personalities can even have different physiological manifestations. For example, while in one personality, a person can see poorly and wear glasses, and in another, have excellent vision and walk without glasses or lenses (or think that he sees perfectly and does without glasses). Just as in the case of dissociative fugue, when switching, one person cannot remember what happened to the person during immersion in another.
Personalities within a person can have different ages, genders, nationalities, mental abilities, temperaments, and behave in completely different ways. Often these personalities can even have different physiological manifestations. For example, while in one personality, a person can see poorly and wear glasses, and in another, have excellent vision and walk without glasses or lenses (or think that he sees perfectly and does without glasses). Just as in the case of dissociative fugue, when switching, one person cannot remember what happened to the person during immersion in another.
Manifestations of dissociative identity disorder
This disease affects both children (adolescents) and adults and presents with similar symptoms. However, dissociative disorder with multiple personalities in adolescents is quite rare. In old age, dissociation practically does not develop. When a specialist suspects a person of dissociative identity disorder, he usually asks if it happened that the person suddenly found himself in some place and did not understand how he got there. Also, the patient may suddenly speak in a completely different voice, he may have a different handwriting. For example, a person who has one of his personalities as a child may suddenly begin to write in a child's handwriting. Such phenomenal manifestations can be evoked in a patient suffering from dissociative personality disorder, and in a state of hypnosis. That is why the French psychiatrist Jean-Martin Charcot at one time mistakenly believed that hypnosis is a pathological condition that causes hysteria and the manifestation of multiple personalities. However, later it turned out that hypnosis is only superficially similar to dissociative personality disorder, but does not cause it, and the disease itself develops without any connection with hypnosis.
Also, the patient may suddenly speak in a completely different voice, he may have a different handwriting. For example, a person who has one of his personalities as a child may suddenly begin to write in a child's handwriting. Such phenomenal manifestations can be evoked in a patient suffering from dissociative personality disorder, and in a state of hypnosis. That is why the French psychiatrist Jean-Martin Charcot at one time mistakenly believed that hypnosis is a pathological condition that causes hysteria and the manifestation of multiple personalities. However, later it turned out that hypnosis is only superficially similar to dissociative personality disorder, but does not cause it, and the disease itself develops without any connection with hypnosis.
See also
Myths about hypnosis
A person who has a dissociative disorder is, in fact, suffering greatly from his condition. He sees the negative or dismissive attitude of those around him: they look at him strangely, they reject him, no one finds a common language with him, because of him the family can collapse, and so on. At the moment of a dissociative state, a person does not have the opportunity to critically look at himself and his own behavior. That is, in a situation where one of the alternative personalities appears, he is in an inadequate state.
At the moment of a dissociative state, a person does not have the opportunity to critically look at himself and his own behavior. That is, in a situation where one of the alternative personalities appears, he is in an inadequate state.
The main theory about the origin of this disease is based on the fact that in childhood such people experienced a traumatic situation, usually bullying or violence.
Dissociation is one of three conditions in which the patient is exempt from criminal liability, along with psychosis and mental retardation. There were cases when people in a dissociative state committed murder and rape. In such situations, even taking into account the severity of the crimes, patients are not sent to prison, but are sent to a psychiatric hospital or, in extreme cases, to a special ward of the psychiatric department of the prison.
Causes of dissociative identity disorder
Scientists have not yet found the genetic causes of dissociative identity disorder. The main theory about the origin of this disease is based on the fact that in childhood such people experienced a traumatic situation, usually bullying or violence. However, even this theory does not explain all 100% of cases of dissociative states. There are patients who, without an overt or identified traumatic situation in childhood, suffer from dissociative personality disorder. With regard to the physiological manifestations of this disorder, there is an assumption that in such patients certain areas of the brain stop working and others turn on. However, none of the theories suggesting physiological causes of dissociation currently explains all cases of the disease.
The main theory about the origin of this disease is based on the fact that in childhood such people experienced a traumatic situation, usually bullying or violence. However, even this theory does not explain all 100% of cases of dissociative states. There are patients who, without an overt or identified traumatic situation in childhood, suffer from dissociative personality disorder. With regard to the physiological manifestations of this disorder, there is an assumption that in such patients certain areas of the brain stop working and others turn on. However, none of the theories suggesting physiological causes of dissociation currently explains all cases of the disease.
Diagnosis of dissociative identity disorder
Diagnosis of dissociative identity disorder is made through clinical interviews with several specialists. Sometimes the diagnosis requires not one, but several meetings with psychologists and psychiatrists, so that they have the opportunity to identify different aspects of the disorder, look at the patient's condition from several points of view and assemble a consultation. However, the specialist who identifies this disorder must have a great deal of experience and qualifications, since this disease can often be confused with others. In its manifestations, it can be similar to depression, anxiety or psychosis. It is also common for patients with dissociative identity disorder to be diagnosed with schizophrenia. Dissociation is a rare disorder and not every mental health professional can diagnose this disorder.
However, the specialist who identifies this disorder must have a great deal of experience and qualifications, since this disease can often be confused with others. In its manifestations, it can be similar to depression, anxiety or psychosis. It is also common for patients with dissociative identity disorder to be diagnosed with schizophrenia. Dissociation is a rare disorder and not every mental health professional can diagnose this disorder.
Medications do not cure dissociative identity disorder, but only relieve some of the symptoms.
See also
Mental norm and pathology
A separate task for a specialist in the process of diagnosing dissociation in a child is to distinguish diseases from the presence of imaginary friends in a child, which very often appear in perfectly healthy children at a certain age. To do this, a specialist must be highly qualified in the field of developmental psychology and clearly be able to recognize a dissociative disorder not only in adults, but also in children.
Treatment of dissociative identity disorder
The main treatment for dissociative personality disorder is hypnosis. Sometimes specialists connect methods of psychoanalysis or cognitive-behavioral psychotherapy to treatment. Also, in some cases, medication is used to relieve symptoms. Drugs are prescribed if the disorder is accompanied by depression, panic attacks, drug or alcohol addiction. Medications do not cure dissociative identity disorder, but only relieve some of the symptoms. If a child suffers from this disease, then specialists carry out separate work with his parents, provide them with methods of proper communication with the child to improve the results of his treatment.
If you do not treat dissociative personality disorder, but let the disease take its course, then in the case of multiple personalities, a person in an inadequate state can commit some extremely negative actions in relation to others, for example, violent ones. In the case of a dissociative fugue, a person may get lost and never return home - it will simply be impossible to find him.
- Diseases and disorders
Share:
90,000 dissociative identity disorder- MC "Korsakov"
- interviews
- Dissocial identity disorder
in a dissociative reconstruction of the identity of the very cheapness and the most uniform history. Even before the existence of psychology and psychiatry as separate disciplines, people suffering from this condition were "diagnosed" as possessed by some kind of spirit or demon, and treatment was ruthless. And only a few centuries later it became clear that two personalities existing in one person are a disease that needs qualified treatment.
Free consultation now!
Online consultation with a specialist on your issue!
License number: LO-77-01-019036
Causes
In the vast majority of cases, a “split” personality is the result of a severe mental trauma that a person suffered in childhood. This may be the death of a loved one, a tragic incident and the participation of a child as a witness, prolonged family violence, etc. The mechanism for the development of a dissociative disorder should be considered in more detail.
This may be the death of a loved one, a tragic incident and the participation of a child as a witness, prolonged family violence, etc. The mechanism for the development of a dissociative disorder should be considered in more detail.
Not a single child is born as a whole person - this happens in the process of growing up and under the influence of personal experience, external factors, observation of the behavior of others and other circumstances. Under favorable conditions in a child, all aspects are combined into a concept of himself as an integral and unified personality - experience, memories, emotions, perceptions, etc. are integrated into this personality and exist inseparably from it.
But severe mental trauma experienced in childhood can delimit the formation of personality into two phases: “before” and “after” the traumatic event. This leads to the formation of the same two personalities, separated by trauma.
In other cases, the separation of personalities may be formed as a defense mechanism. In this case, the child, trying to isolate himself from the factors that traumatize him, leaves the alternative self “outside”, taking the true self inside - where it is quiet and comfortable.
In this case, the child, trying to isolate himself from the factors that traumatize him, leaves the alternative self “outside”, taking the true self inside - where it is quiet and comfortable.
Although this condition is often referred to as a split personality, in fact, each phase of the formation of the child's mental conception can give rise to a new "I" that "replaces" the original personality at certain events.
COST OF TREATMENT
Symptoms
Dissociative identity disorder has several characteristic manifestations. But their combination is diagnostically informative:
- Multiple identities. They appear in two forms: possessed and unpossessed. The first is noticeable to others - a person behaves differently from what is characteristic of him, he develops habits and inclinations that were previously unusual for him. Everything can change - from intonation and speech to the manner of moving and gastronomic preferences. Such a person can be real (for example, a deceased mother) or "supernatural" (elf, God, devil, etc.
 ). In the unpossessed phase, a person remains normal for others, but he does not feel himself as such. He has a feeling of complete or partial unreality of what is happening, or the impression that he plays the role of a spectator in his own life and is unable to influence everything that happens. The patient may "hear voices" or feel that "someone else is thinking for him."
). In the unpossessed phase, a person remains normal for others, but he does not feel himself as such. He has a feeling of complete or partial unreality of what is happening, or the impression that he plays the role of a spectator in his own life and is unable to influence everything that happens. The patient may "hear voices" or feel that "someone else is thinking for him." - Dissociative amnesia. When identity is split, the patient often does not remember the actions he committed and is surprised or even outraged by the attempts of others to prove that it was he who did it. Moreover, a person with dissociative identity disorder may suddenly lose the skills that he owned a few hours ago. He doesn't know how to use the microwave or how to turn on the TV. Loss of memories can relate to events that happened yesterday or an hour ago, as well as key traumatic events. For example, a person “does not know” about the death of a relative because he does not remember it - here there is a protective mechanism that protects the person’s consciousness from painful memories.
In addition to these obligatory clinical signs, dissociative identity disorder may be accompanied by visual, auditory, tactile and olfactory hallucinations, addiction to self-harm (self-harm or self-mutilation), sexual dysfunction, panic attacks and seizures, etc.
Treatment
Treatment is most effective at an early stage of split personality, when the separation has not yet ended. At this stage, in most cases, it is possible to integrate both (or several) "I" and create conditions for the formation of a whole and unified personality.
Therapy in adulthood may include elements of drug treatment and optionally psychotherapy. It is aimed at:
- stabilization of the human condition;
- increase in the duration of the presence of the "original" personality;
- identifying the relationship between the original and alternative personality and finding solutions for their integration;
- identification of key traumatic factors that led to the splitting of the personality, and the translation of these events into a rational psychological channel, etc.