How to know if you have eating disorders
8 Signs You May Have an Eating Disorder
How do we know when disordered eating becomes an eating disorder? Disordered eating does not interfere with one’s ability to function, but may include irregular eating patterns along with judgment around food and/or body. Eating disorders, on the other hand, represent a wide range of behaviors involving food and eating and impair one’s health and ability to function in terms of life goals, relationships, career, and academics. It may be hard to determine whether or not you are experiencing disordered eating or an eating disorder.
First, it may be helpful to reflect on the following questions:
- What are the signs of an eating disorder?
- Are you displaying these signs?
For many individuals with eating disorders, here are some of the more commonly experienced signs and behaviors:
1. Adopting Ritualistic Eating Habits and Rules
Eating a set quantity of a particular food at a certain time in a certain setting may be part of a daily routine. However, when taken to extremes that interfere with everyday life, ritualistic habits and rigid rules may indicate an unhealthy relationship with food. Eliminating whole food groups, limiting food intake, restricting quantities or following inflexible preparation practices may be a sign of an eating disorder.
2. Refusing to Eat With Others
Handling food in social settings can be challenging for those struggling with eating disorders. Individuals may go to great lengths to avoid group events where food is present. They may disengage and disappear from a gathering when food is served.
3. Struggling to Engage with Food in Healthful Ways
Individuals with eating disorders may exhibit unhealthful relationships with food, including avoiding and/or restricting food, purging, and/or eating past the point of fullness. Stress, boredom, grief, joy or other emotions may trigger or intensify eating disordered behaviors.
4. Exercising Excessively to Burn Calories
With an eating disorder, exercise can become more than a means of joyful or healthful movement. Instead, it may become a way to compensate for caloric intake or as a way to punish themselves for “eating too much.” People with eating disorders often become obsessive about tracking the number of calories expended versus the number of those taken in.
Instead, it may become a way to compensate for caloric intake or as a way to punish themselves for “eating too much.” People with eating disorders often become obsessive about tracking the number of calories expended versus the number of those taken in.
5. Obsessing Over Physical Characteristics
Many individuals with eating disorders tend to focus on perceived body image concerns that may or may not be apparent to others. They may obsess over specific parts of their bodies or set weight/size goals that are unhealthy or unrealistic.
6. Hoarding and Stashing Food
Eating disorders can cause people to hide or stash food. In some cases, individuals may hoard select “safe” foods or beverages. They may feel the need to stockpile it, keep it separate or even hide it, so that other family members can’t eat it. For others, the hidden food in question may be triggering to the person, and they may view it as forbidden.
7. Lowered Self-Esteem
Low self-esteem is commonly experienced by those struggling with eating disorders. This can manifest through insecurities over physical characteristics, such as body shape and weight, as well as a generally lowered self-worth – feeling as though you are not worthy or do not measure up to your peers in some way. Oftentimes, disordered eating behaviors are developed as a way to cope with feelings of inadequacy and take back some level of perceived “control” over their life.
This can manifest through insecurities over physical characteristics, such as body shape and weight, as well as a generally lowered self-worth – feeling as though you are not worthy or do not measure up to your peers in some way. Oftentimes, disordered eating behaviors are developed as a way to cope with feelings of inadequacy and take back some level of perceived “control” over their life.
8. Physical Symptoms
There are many physical symptoms associated with eating disorders, oftentimes varying depending on the specific type of eating disorder. Physical symptoms may include gastrointestinal problems, fatigue, high or low blood pressure or fluctuations in weight over relatively short periods of time. Individuals may also experience weakness, dizziness, joint pain or dehydration. For a more detailed breakdown of physical symptoms for each type of eating disorder, visit our pages on Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, ARFID and OSFED.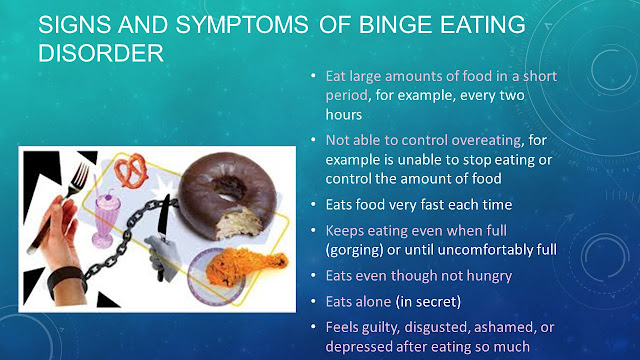
When to Take the Next Step
If you recognize any of the above signs in yourself or in someone you love, it may be time to reach out to us at The Alliance for Eating Disorders Awareness. Here, you’ll find the support and guidance needed to help on the journey to recovery.
To learn more about the eating disorder treatment process, visit our Levels of Care page, which highlights the different types of care one may need. If you’re ready to take the next step in receiving help or support for an eating disorder, visit our national, interactive database to find a provider near you or call us at 866.662.1235 to speak with a specialized and licensed therapist. You are not alone. Help is available and recovery is possible.
Types, Causes, Treatment, and Recovery
Although the term “eating” is in the name, eating disorders are about more than food. They’re complex mental health conditions that often require the intervention of medical and psychological experts to alter their course.
These disorders are described in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) (1).
In the United States alone, an estimated 28 million Americans have or have had an eating disorder at some point in their life (2).
This article describes six of the most common types of eating disorders and their symptoms.
Eating disorders are a range of psychological conditions that cause unhealthy eating habits to develop. They might start with an obsession with food, body weight, or body shape (3).
In severe cases, eating disorders can cause serious health consequences and may even result in death if left untreated. In fact, eating disorders are among the deadliest mental illnesses, second to opioid overdose (4).
People with eating disorders can have a variety of symptoms. Common symptoms include severe restriction of food, food binges, and purging behaviors like vomiting or overexercising.
Although eating disorders can affect people of any gender at any life stage, they’re increasingly common in men and gender nonconforming people. These populations often seek treatment at lower rates or may not report their eating disorder symptoms at all (5, 6).
These populations often seek treatment at lower rates or may not report their eating disorder symptoms at all (5, 6).
Different types of eating disorders have different symptoms, but each condition involves an extreme focus on issues related to food and eating, and some involve an extreme focus on weight.
This preoccupation with food and weight may make it hard to focus on other aspects of life (3).
Mental and behavioral signs may include (7):
- dramatic weight loss
- concern about eating in public
- preoccupation with weight, food, calories, fat grams, or dieting
- complaints of constipation, cold intolerance, abdominal pain, lethargy, or excess energy
- excuses to avoid mealtime
- intense fear of weight gain or being “fat”
- dressing in layers to hide weight loss or stay warm
- severely limiting and restricting the amount and types of food consumed
- refusing to eat certain foods
- denying feeling hungry
- expressing a need to “burn off” calories
- repeatedly weighing oneself
- patterns of binge eating and purging
- developing rituals around food
- excessively exercising
- cooking meals for others without eating
- missing menstrual periods (in people who would typically menstruate)
Physical signs may include (7):
- stomach cramps and other gastrointestinal symptoms
- difficulty concentrating
- atypical lab test results (anemia, low thyroid levels, low hormone levels, low potassium, low blood cell counts, slow heart rate)
- dizziness
- fainting
- feeling cold all the time
- sleep irregularities
- menstrual irregularities
- calluses across the tops of the finger joints (a sign of inducing vomiting)
- dry skin
- dry, thin nails
- thinning hair
- muscle weakness
- poor wound healing
- poor immune system function
Experts believe that a variety of factors may contribute to eating disorders.
One of these is genetics. People who have a sibling or parent with an eating disorder seem to be at an increased risk of developing one (3).
Personality traits are another factor. In particular, neuroticism, perfectionism, and impulsivity are three personality traits often linked to a higher risk of developing an eating disorder, according to a 2015 research review (8).
Other potential causes include perceived pressures to be thin, cultural preferences for thinness, and exposure to media promoting these ideals (8).
More recently, experts have proposed that differences in brain structure and biology may also play a role in the development of eating disorders. In particular, levels of the brain messaging chemicals serotonin and dopamine may be factors (9).
However, more studies are needed before strong conclusions can be made.
Eating disorders are a group of related conditions involving extreme food and weight issues, but each disorder has unique symptoms and diagnosis criteria.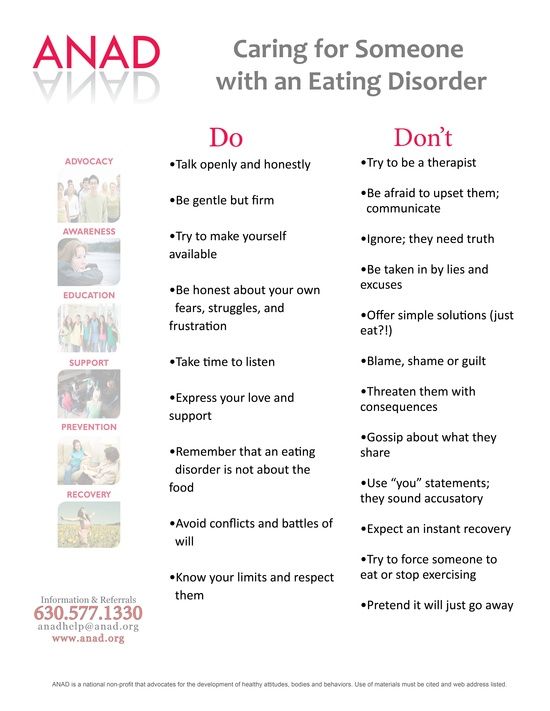 Here are six of the most common eating disorders and their symptoms.
Here are six of the most common eating disorders and their symptoms.
Anorexia nervosa is likely the most well-known eating disorder.
It generally develops during adolescence or young adulthood and tends to affect more women than men (10).
People with anorexia generally view themselves as overweight, even if they’re dangerously underweight. They tend to constantly monitor their weight, avoid eating certain types of foods, and severely restrict their calorie intake.
Common symptoms of anorexia nervosa include (1):
- very restricted eating patterns
- intense fear of gaining weight or persistent behaviors to avoid gaining weight, despite being underweight
- a relentless pursuit of thinness and unwillingness to maintain a healthy weight
- a heavy influence of body weight or perceived body shape on self-esteem
- a distorted body image, including denial of being seriously underweight
However, it’s important to note that weight should not be the major focus of diagnosing someone with anorexia.
Using body mass index as a factor in diagnosis is outdated because people who are categorized as “normal” or “overweight” can have the same risks.
In atypical anorexia, for example, a person may meet the criteria for anorexia but not be underweight despite significant weight loss (7).
Obsessive-compulsive symptoms are also often present. For instance, many people with anorexia are preoccupied with constant thoughts about food, and some may obsessively collect recipes or hoard food.
They may also have difficulty eating in public and exhibit a strong desire to control their environment, limiting their ability to be spontaneous (3).
Anorexia is officially categorized into two subtypes — the restricting type and the binge eating and purging type (1).
Individuals with the restricting type lose weight solely through dieting, fasting, or excessive exercise.
Individuals with the binge eating and purging type may binge on large amounts of food or eat very little. In both cases, after they eat, they purge using activities such as vomiting, taking laxatives or diuretics, or exercising excessively.
In both cases, after they eat, they purge using activities such as vomiting, taking laxatives or diuretics, or exercising excessively.
Anorexia can be very damaging to the body. Over time, individuals living with it may experience thinning of their bones, infertility, and brittle hair and nails.
In severe cases, anorexia can result in heart, brain, or multi-organ failure and death.
Bulimia nervosa is another well-known eating disorder.
Like anorexia, bulimia tends to develop during adolescence and early adulthood and appears to be less common among men than women (10).
People with bulimia frequently eat unusually large amounts of food in a specific period of time.
Each binge eating episode usually continues until the person becomes painfully full. During a binge, the person usually feels that they cannot stop eating or control how much they are eating.
Binges can happen with any type of food but most commonly occur with foods the individual would usually avoid.
Individuals with bulimia then attempt to purge to compensate for the calories consumed and to relieve gut discomfort.
Common purging behaviors include forced vomiting, fasting, laxatives, diuretics, enemas, and excessive exercise.
Symptoms may appear very similar to those of the binge eating or purging subtypes of anorexia nervosa. However, individuals with bulimia usually maintain a relatively typical weight rather than losing a large amount of weight.
Common symptoms of bulimia nervosa include (1):
- recurrent episodes of binge eating with a feeling of lack of control
- recurrent episodes of inappropriate purging behaviors to prevent weight gain
- self-esteem overly influenced by body shape and weight
- a fear of gaining weight, despite having a typical weight
Side effects of bulimia may include an inflamed and sore throat, swollen salivary glands, worn tooth enamel, tooth decay, acid reflux, irritation of the gut, severe dehydration, and hormonal disturbances (11).
In severe cases, bulimia can also create an imbalance in levels of electrolytes, such as sodium, potassium, and calcium. This can cause a stroke or heart attack.
Binge eating disorder is the most prevalent form of eating disorder and one of the most common chronic illnesses among adolescents (12).
It typically begins during adolescence and early adulthood, although it can develop later on.
Individuals with this disorder have symptoms similar to those of bulimia or the binge eating subtype of anorexia.
For instance, they typically eat unusually large amounts of food in relatively short periods of time and feel a lack of control during binges.
People with binge eating disorder do not restrict calories or use purging behaviors, such as vomiting or excessive exercise, to compensate for their binges (12).
Common symptoms of binge eating disorder include (11):
- eating large amounts of food rapidly, in secret, and until uncomfortably full, despite not feeling hungry
- feeling a lack of control during episodes of binge eating
- feelings of distress, such as shame, disgust, or guilt, when thinking about the binge eating behavior
- no use of purging behaviors, such as calorie restriction, vomiting, excessive exercise, or laxative or diuretic use, to compensate for the binge eating
People with binge eating disorder often consume an excessive amount of food and may not make nutritious food choices. This may increase their risk of medical complications such as heart disease, stroke, and type 2 diabetes (13).
This may increase their risk of medical complications such as heart disease, stroke, and type 2 diabetes (13).
Pica is an eating disorder that involves eating things that are not considered food and that do not provide nutritional value (14).
Individuals with pica crave non-food substances such as ice, dirt, soil, chalk, soap, paper, hair, cloth, wool, pebbles, laundry detergent, or cornstarch (11).
Pica can occur in adults, children, and adolescents.
It is most frequently seen in individuals with conditions that affect daily functioning, including intellectual disabilities, developmental conditions such as autism spectrum disorder, and mental health conditions such as schizophrenia (14).
Individuals with pica may be at an increased risk of poisoning, infections, gut injuries, and nutritional deficiencies. Depending on the substances ingested, pica may be fatal.
However, for the condition to be considered pica, the eating of non-food substances must not be a typical part of someone’s culture or religion. In addition, it must not be considered a socially acceptable practice by a person’s peers.
In addition, it must not be considered a socially acceptable practice by a person’s peers.
Rumination disorder is another newly recognized eating disorder.
It describes a condition in which a person regurgitates food they have previously chewed and swallowed, re-chews it, and then either re-swallows it or spits it out (15).
This rumination typically occurs within the first 30 minutes after a meal (16).
This disorder can develop during infancy, childhood, or adulthood. In infants, it tends to develop between 3 and 12 months of age and often disappears on its own. Children and adults with the condition usually require therapy to resolve it.
If not resolved in infants, rumination disorder can result in weight loss and severe malnutrition that can be fatal.
Adults with this disorder may restrict the amount of food they eat, especially in public. This may lead them to lose weight and become underweight (16).
Avoidant/restrictive food intake disorder (ARFID) is a new name for an old disorder.
The term has replaced the term “feeding disorder of infancy and early childhood,” a diagnosis previously reserved for children under age 7 (17).
Individuals with this disorder experience disturbed eating due to either a lack of interest in eating or a distaste for certain smells, tastes, colors, textures, or temperatures.
Common symptoms of ARFID include (11):
- avoidance or restriction of food intake that prevents the person from eating enough calories or nutrients
- eating habits that interfere with typical social functions, such as eating with others
- weight loss or poor development for age and height
- nutrient deficiencies or dependence on supplements or tube feeding
It’s important to note that ARFID goes beyond common behaviors such as picky eating in toddlers or lower food intake in older adults.
Moreover, it does not include the avoidance or restriction of foods due to lack of availability or religious or cultural practices.
In addition to the six eating disorders above, other less known or less common eating disorders also exist.
These include (18):
- Purging disorder. Individuals with purging disorder often use purging behaviors, such as vomiting, laxatives, diuretics, or excessive exercising, to control their weight or shape. However, they do not binge.
- Night eating syndrome. Individuals with this syndrome frequently eat excessively at night, often after awakening from sleep.
- Other specified feeding or eating disorder (OSFED). While it is not found in the DSM-5, this category includes any other conditions that have symptoms similar to those of an eating disorder but don’t fit any of the disorders above.
One disorder that may currently fall under OSFED is orthorexia. Although orthorexia is increasingly mentioned in the media and in scientific studies, the DSM does not yet recognize it as a separate eating disorder (19).
Individuals with orthorexia tend to have an obsessive focus on healthy eating to an extent that disrupts their daily lives. They may compulsively check ingredient lists and nutritional labels and obsessively follow “healthy lifestyle” accounts on social media.
Someone with this condition may eliminate entire food groups, fearing that they’re unhealthy. This can lead to malnutrition, severe weight loss, difficulty eating outside the home, and emotional distress.
Individuals with orthorexia are rarely focused on losing weight. Instead, their self-worth, identity, or satisfaction is dependent on how well they comply with their self-imposed diet rules (19).
If you have an eating disorder, identifying the condition and seeking treatment sooner will improve your chances of recovering. Being aware of the warning signs and symptoms can help you decide whether you need to seek help.
Not everyone will have every sign or symptom at once, but certain behaviors may signal a problem, such as (20):
- behaviors and attitudes that indicate that weight loss, dieting, and control over food are becoming primary concerns
- preoccupation with weight, food, calories, fats, grams, and dieting
- refusal to eat certain foods
- discomfort with eating around others
- food rituals (not allowing foods to touch, eating only particular food groups)
- skipping meals or eating only small portions
- frequent dieting or fad diets
- extreme concern with body size, shape, and appearance
- frequently checking in the mirror for perceived flaws in appearance
- extreme mood swings
If these symptoms resonate with you and you think you may have an eating disorder, it’s important to reach out to a medical professional for help.
Making the decision to start eating disorder recovery might feel scary or overwhelming, but seeking help from medical professionals, eating disorder recovery support groups, and your community can make recovery easier.
If you’re not sure where to start, you can contact the National Eating Disorders Association helpline for support, resources, and treatment options for yourself or someone you know.
To contact, call: (800) 931-2237
Monday–Thursday 11 a.m.–9 p.m. ET
Friday 11 a.m.–5 p.m. ET
Text: (800) 931-2237
Monday–Thursday 3 p.m.–6 p.m. ET
Friday 1 p.m.–5 p.m. ET
Eating disorder treatment plans are specifically tailored to each person and may include a combination of multiple therapies.
Treatment will usually involve talk therapy, as well as regular health checks with a physician (21).
It’s important to seek treatment early for eating disorders, as the risk of medical complications and suicide is high (11).
Treatment options include:
- Individual, group, or family psychotherapy. A type of psychotherapy called cognitive behavioral therapy (CBT) may be recommended to help reduce or eliminate disordered behavior such as binge eating, purging, and restricting. CBT involves learning how to recognize and change distorted or unhelpful thought patterns (11).
- Medications. A doctor may recommend treatment with medications such as antidepressants, antipsychotics, or mood stabilizers to help treat an eating disorder or other conditions that may occur at the same time, such as depression or anxiety (11).
- Nutritional counseling. This involves working with a dietitian to learn proper nutrition and eating habits and may also involve restoring or managing a person’s weight if they have experienced significant weight changes. Studies suggest that combining nutritional therapy with cognitive therapy may significantly improve treatment outcomes (22).

If you think someone in your life has an eating disorder, your best bet is to support and encourage them to seek help from a healthcare professional.
This can be extremely difficult for someone living with an eating disorder, but supporting them in other ways will help them feel cared for and encouraged in their recovery.
Recovering from an eating disorder can take a long time, and this person may have periods of relapsing into old behaviors, especially during times of stress. If you’re close to this person, it’s important to be there for them, and be patient, throughout their recovery (21).
Ways to support someone with an eating disorder include (21):
- Listening to them. Taking time to listen to their thoughts can help them feel heard, respected, and supported. Even if you don’t agree with what they say, it’s important that they know you’re there for them and that they have someone to confide in.
- Including them in activities.
 You can reach out and invite them to activities and social events or ask if they want to hang out one-on-one. Even if they do not want to be social, it’s important to check in and invite them to help them feel valued and less alone.
You can reach out and invite them to activities and social events or ask if they want to hang out one-on-one. Even if they do not want to be social, it’s important to check in and invite them to help them feel valued and less alone. - Trying to build their self-esteem. Make sure they know that they are valued and appreciated, especially for nonphysical reasons. Remind them why you are their friend and why they are valued.
The categories above are meant to provide a better understanding of the most common eating disorders and dispel myths about them.
Eating disorders are mental health conditions that usually require treatment. They can also be damaging to the body if left untreated.
If you have an eating disorder or know someone who might have one, you can seek help from a healthcare professional who specializes in eating disorders.
You can book an appointment with an eating disorder specialist in your area using our Healthline FindCare tool.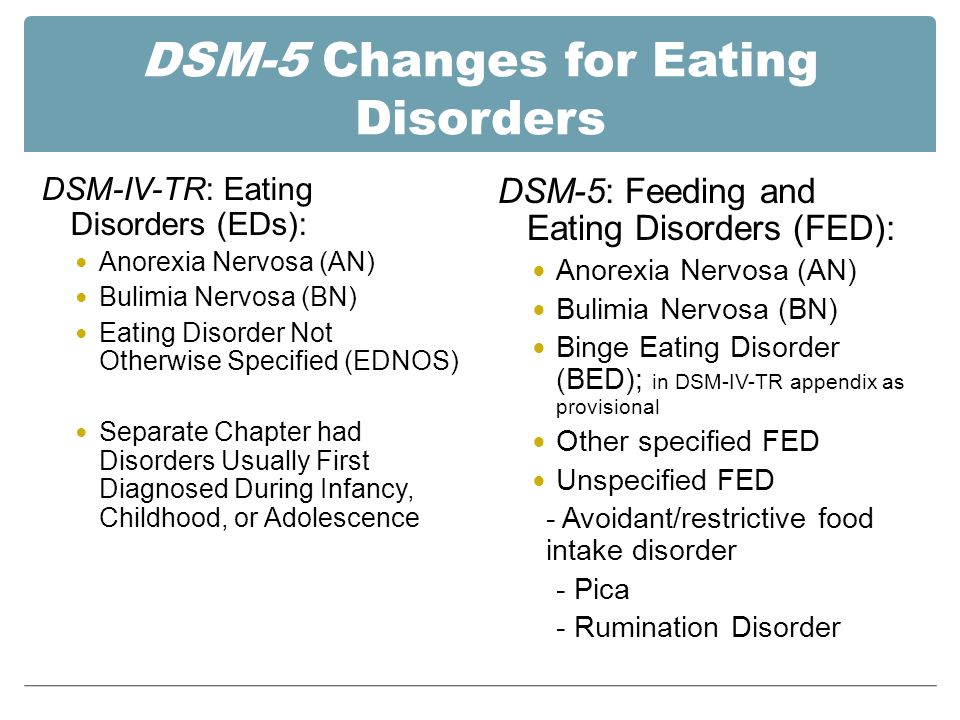
Read this article in Spanish.
Eating disorders | Tervisliku toitumise informatsioon
Eating disorders are psychiatric illnesses that damage a person's physical and mental health and impair their overall quality of life - relationships, work and personal development suffer.
Eating disorders disrupt the connection with one's own body, resulting in highly problematic eating behavior. Weight and body shape are overemphasized, underweight is idealized, and various methods are used to lose weight or prevent weight gain.
Approximately 8% of women and 2% of men will develop an eating disorder during their lifetime. Eating disorders occur in any population, regardless of gender, age, ethnicity, or socioeconomic status. However, they are most common in girls and young women.
Eating disorders are a group of diseases that are distributed differently in different classifications. The most common eating disorders are anorexia ( anorexia nervosa ), bulimia ( bulimia nervosa ) and compulsive overeating ( binge-eating disorder ).
The term "eating disorder" is often erroneously used as a synonym for selective eating disorder, as both are associated with eating disorders. However, the reasons for them are different: an eating disorder is caused by a desire to control weight, while in a selective eating disorder, eating certain foods causes anxiety or fear.
Other eating disorders
Anorexia, bulimia and binge eating disorders are the three most common and well-known eating disorders. However, often not all of the symptoms of a person with an eating disorder correspond to one specific disorder. In such cases, these disorders are referred to as "atypical" or "other eating disorders". A common myth is that in such cases the course of the disease is milder and treatment is treated more lightly. However, this is erroneous, since the name of the disease indicates only its diagnostic criteria, and not the severity or course.
All eating disorders, no matter how they are called or classified, are dangerous conditions that impair quality of life and require treatment.

Causes of Eating Disorders
There is never one single cause of an eating disorder. These are complex diseases, in the development of which a combination of many factors plays an important role. Genetic, biological and environmental factors always play a role. Modern social representations, including the culture of diets and the cult of slimness, contribute to the development of psychological vulnerability, which can become a fertile environment for the formation of eating disorders. Probably for the same reasons, a higher incidence of eating disorders is observed in sports in which weight is of great importance, and among representatives of professions focused on appearance. However, it should be emphasized that browsing social networks or playing a certain sport does not contribute to the development of the disease. There are many factors involved in the development of the disease that are usually beyond the control of the individual. However, it is often more practical and even more important to identify the factors that support the disease, since changing them is associated with better treatment outcomes.
Treatment Options for Eating Disorders
Eating disorders can be life-threatening illnesses with a long and chronic course; they have one of the highest mortality rates of any psychiatric illness. Treating eating disorders is often a lengthy and complex process. However, early intervention is paramount to achieve a good treatment outcome.
Diagnosis and treatment of an eating disorder usually begins with the family doctor. Family sisters can provide advice on healthy eating. Psychiatrists are specialists in the diagnosis and treatment of eating disorders as a psychiatric illness. The participation of a clinical psychologist or psychotherapist is also important.
There are two centers in Estonia that specialize in the treatment of eating disorders: the Department of Eating Disorders of the Mental Health Center of the Tallinn Children's Hospital treats children and adolescents, and the Department of Eating Disorders of the Psychiatric Clinic of the Tartu University Hospital treats adolescents and adults.
For more information about eating disorders and advice on what to do if you suspect a loved one has an eating disorder, visit peaasi.ee.
| 1. I am afraid of the thought that I will put on weight. never |
| 2. I abstain from food when I am hungry. never |
| 3. I find myself preoccupied with thoughts of food. never |
| 4. I have attacks of uncontrolled eating during which I cannot stop myself. never |
| 5. I divide my food into small pieces. never |
| 6. never |
| 7. I especially abstain from high carbohydrate foods (bread, rice, potatoes, etc.). never |
| 8. I feel that others prefer that I eat more. never |
| 9. I vomit after eating. never |
| 10. I experience a heightened sense of guilt after eating. never |
| 11. I am concerned about the desire to lose weight. never |
| 12. never |
| 13. People around me think I'm too thin. never |
| 14. I am preoccupied with thoughts about the fat in my body. never |
| 15. It takes me longer to eat food than other people. never |
| 16. I abstain from food containing sugar. never |
| 17. I eat diet foods. never |
| 18. I feel that issues related to food control my life. never |
| 19. I have self-control in matters related to food. never |
| 20. I feel that others put pressure on me to eat. never |
| 21. I spend too much time and thought on issues related to food. never |
| 22. I feel discomfort after eating sweets. never |
| 23. I am on a diet. never |
| 24. I like the feeling of an empty stomach. never |
| 25.    Copyright © · The Wright Initiative · Articles · Site Map 
|
 I know how many calories are in the food I eat.
I know how many calories are in the food I eat.  When I exercise, I think about burning calories.
When I exercise, I think about burning calories.