How long does it take to be diagnosed with depression
NIMH » Depression
What is depression?
Everyone feels sad or low sometimes, but these feelings usually pass with a little time. Depression (also called major depressive disorder or clinical depression) is different. It can cause severe symptoms that affect how you feel, think, and handle daily activities, such as sleeping, eating, or working. It is an illness that can affect anyone—regardless of age, race, income, culture, or education. Research suggests that genetic, biological, environmental, and psychological factors play a role in depression.
Depression may occur with other mental disorders and other illnesses, such as diabetes, cancer, heart disease, and chronic pain. Depression can make these conditions worse, and vice versa. Sometimes medications taken for these illnesses cause side effects that contribute to depression symptoms.
What are the different types of depression?
Two common forms of depression are:
- Major depression, which includes symptoms of depression most of the time for at least 2 weeks that typically interfere with one’s ability to work, sleep, study, and eat.
- Persistent depressive disorder (dysthymia), which often includes less severe symptoms of depression that last much longer, typically for at least 2 years.
Other forms of depression include:
- Perinatal depression, which occurs when a woman experiences major depression during pregnancy or after delivery (postpartum depression).
- Seasonal affective disorder, which comes and goes with the seasons, typically starting in late fall and early winter and going away during spring and summer.
- Depression with symptoms of psychosis, which is a severe form of depression where a person experiences psychosis symptoms, such as delusions (disturbing, false fixed beliefs) or hallucinations (hearing or seeing things that others do not see or hear).
Individuals diagnosed with bipolar disorder (formerly called manic depression or manic-depressive illness) also experience depression.
What are the signs and symptoms of depression?
Common symptoms of depression include:
- Persistent sad, anxious, or “empty” mood
- Feelings of hopelessness or pessimism
- Feelings of irritability, frustration‚ or restlessness
- Feelings of guilt, worthlessness, or helplessness
- Loss of interest or pleasure in hobbies or activities
- Decreased energy, fatigue, or being “slowed down”
- Difficulty concentrating, remembering, or making decisions
- Difficulty sleeping, early morning awakening, or oversleeping
- Changes in appetite or unplanned weight changes
- Aches or pains, headaches, cramps, or digestive problems without a clear physical cause and that do not ease even with treatment
- Suicide attempts or thoughts of death or suicide
If you or someone you know is in immediate distress or is thinking about hurting themselves,
call the National Suicide Prevention Lifeline toll-free at 1-800-273-TALK (8255). You also can text the Crisis Text Line (HELLO to 741741) or use the Lifeline Chat on the National Suicide Prevention Lifeline website.
You also can text the Crisis Text Line (HELLO to 741741) or use the Lifeline Chat on the National Suicide Prevention Lifeline website.
How is depression diagnosed?
To be diagnosed with depression, an individual must have five depression symptoms every day, nearly all day, for at least 2 weeks. One of the symptoms must be a depressed mood or a loss of interest or pleasure in almost all activities. Children and adolescents may be irritable rather than sad.
If you think you may have depression, talk to your health care provider. Primary care providers routinely diagnose and treat depression and refer individuals to mental health professionals, such as psychologists or psychiatrists.
During the visit, your provider may ask when your symptoms began, how long they last, how often they occur, and if they keep you from going out or doing your usual activities. It may help to make some notes about your symptoms before your visit. Certain medications and some medical conditions, such as viruses or a thyroid disorder, can cause the same depression symptoms. Your provider can rule out these possibilities by doing a physical exam, interview, and lab tests.
Your provider can rule out these possibilities by doing a physical exam, interview, and lab tests.
Read NIMH’s Tips for Talking With Your Health Care Provider to help prepare for and get the most out of your visit. For additional resources, visit the Agency for Healthcare Research and Quality website.
Does depression look the same in everyone?
Depression can affect people differently, depending on their age.
Children with depression may be anxious, cranky, pretend to be sick, refuse to go to school, cling to a parent, or worry that a parent may die.
Older children and teens with depression may get into trouble at school, sulk, be easily frustrated‚ feel restless, or have low self-esteem. They also may have other disorders, such as anxiety and eating disorders, attention-deficit hyperactivity disorder, or substance use disorder. Older children and teens are more likely to experience excessive sleepiness (called hypersomnia) and increased appetite (called hyperphagia). In adolescence, females begin to experience depression more often than males, likely due to the biological, life cycle, and hormonal factors unique to women.
In adolescence, females begin to experience depression more often than males, likely due to the biological, life cycle, and hormonal factors unique to women.
Younger adults with depression are more likely to be irritable, complain of weight gain and hypersomnia, and have a negative view of life and the future. They often have other disorders, such as generalized anxiety disorder, social phobia, panic disorder, and substance use disorders.
Middle-aged adults with depression may have more depressive episodes, decreased libido, middle-of-the-night insomnia, or early morning awakening. They also may more frequently report having gastrointestinal symptoms such as diarrhea or constipation.
Older adults with depression commonly experience sadness or grief or may have other less obvious symptoms. They may report a lack of emotions rather than a depressed mood. Older adults also are more likely to have other medical conditions or pain that may cause or contribute to depression. In severe cases, memory and thinking problems (called pseudodementia) may be prominent.
In severe cases, memory and thinking problems (called pseudodementia) may be prominent.
How is depression treated?
Depression treatment typically involves medication, psychotherapy, or both. If these treatments do not reduce symptoms, brain stimulation therapy may be another treatment option. In milder cases of depression, treatment might begin with psychotherapy alone, and medication added if the individual continues to experience symptoms. For moderate or severe depression, many mental health professionals recommend a combination of medication and therapy at the start of treatment.
Choosing the right treatment plan should be based on a person’s individual needs and medical situation under a provider’s care. It may take some trial and error to find the treatment that works best for you. You can learn more about the different types of treatment, including psychotherapy, medication, and brain stimulation therapies on the NIMH's depression webpage. For information on finding a mental health professional and questions to ask when considering therapy, visit NIMH’s psychotherapies webpage.
For information on finding a mental health professional and questions to ask when considering therapy, visit NIMH’s psychotherapies webpage.
Medications
Antidepressants are medications commonly used to treat depression. They take time to work—usually 4 to 8 weeks—and symptoms such as problems with sleep, appetite, or concentration often improve before mood lifts. It is important to give medication a chance before deciding whether or not it works.
Please Note: Some individuals—especially children, teenagers, and young adults—may experience an increase in suicidal thoughts or behavior when taking antidepressants, particularly in the first few weeks after starting or when the dose is changed. All patients taking antidepressants should be watched closely, especially during the first few weeks of treatment.
Information about medications changes frequently. Visit the U.S. Food and Drug Administration (FDA) website for the latest warnings, patient medication guides, and newly approved medications.
Treatment-resistant depression occurs when a person doesn’t get better after trying at least two antidepressants. Esketamine is a newer FDA-approved medication for treatment-resistant depression delivered as a nasal spray in a doctor’s office, clinic, or hospital. It often acts rapidly—typically within a couple of hours—to relieve depression symptoms. Individuals usually continue to take an oral antidepressant to maintain the improvement in depression.
Another option for treatment-resistant depression is to add a different type of medication that may make an antidepressant more effective, such as an antipsychotic or anticonvulsant medication or bupropion, an antidepressant that works differently from most.
Medications prescribed by your health care provider for depression can have side effects, but these may lessen over time. Talk to your provider about any side effects that you have. Do not stop taking medications without the help of a health care provider. If you abruptly stop taking your medicine, you may experience severe withdrawal symptoms.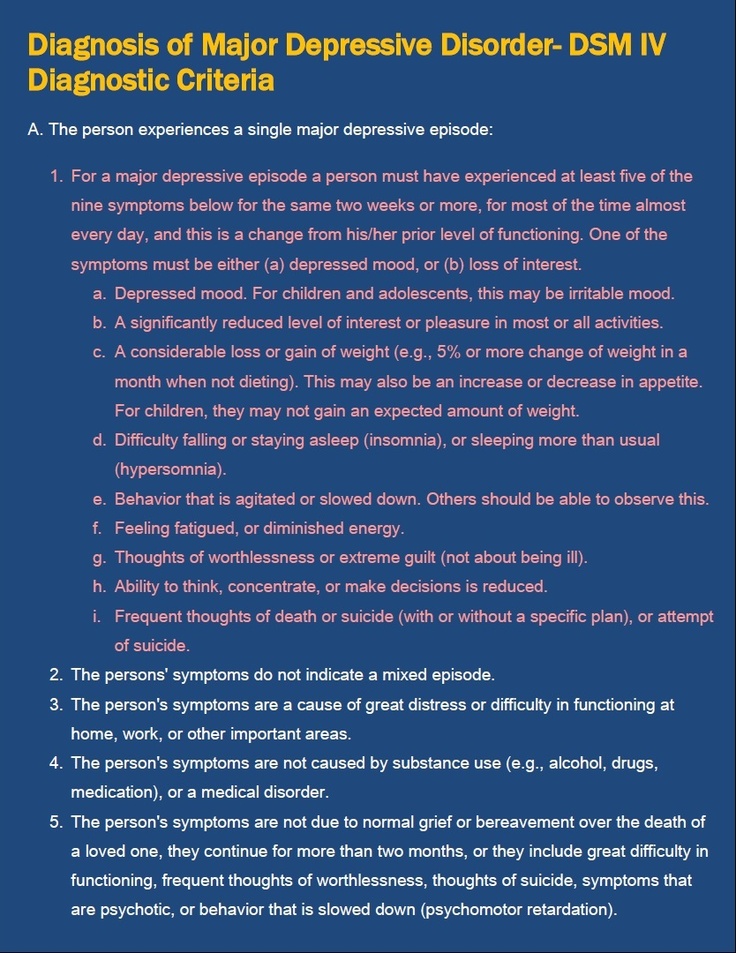
FDA has not approved any natural products for depression. While research is ongoing, some people find natural products, including vitamin D and the herbal dietary supplement St. John’s wort, to help depression. Do not use St. John’s wort or other dietary supplements for depression before talking to your provider. For more information, visit the National Center for Complementary and Integrative Health website.
Psychotherapy
Psychotherapy (also called “talk therapy” or “counseling”) teaches individuals with depression new ways of thinking and behaving and helps with changing habits that contribute to depression. Most psychotherapy occurs with a licensed, trained mental health professional in one-on-one sessions or with other individuals in a group setting. Two effective psychotherapies to treat depression include cognitive behavioral therapy (CBT) and interpersonal therapy (IPT). The use of older forms of psychotherapy, such as dynamic therapy, for a limited time also may help some people with depression.
With CBT, people learn to challenge and change unhelpful thinking patterns and behavior to improve their depressive and anxious feelings. Recent advances in CBT include introducing mindfulness principles and the development of specialized forms of therapy targeting particular symptoms, such as insomnia.
IPT focuses on interpersonal and life events that impact mood and vice versa. The goal of IPT is to help people improve their communication skills within relationships, establish social support networks, and develop realistic expectations to help them deal with crises or other issues that may be contributing to or worsening their depression.
Brain Stimulation Therapy
Brain stimulation therapy, which involves activating or inhibiting the brain directly with electricity or magnetic waves, is another option for some people when other depression treatments have not been effective.
The most common forms of brain stimulation therapy include electroconvulsive therapy and repetitive transcranial magnetic stimulation. Other brain stimulation therapies are newer and, in some cases, still experimental.
Other brain stimulation therapies are newer and, in some cases, still experimental.
How can I find help?
The Substance Abuse and Mental Health Services Administration provides the Behavioral Health Treatment Services Locator, an online tool for finding mental health treatment and support groups in your area. For additional resources, visit NIMH's Help for Mental Illnesses webpage.
How can I take care of myself?
Once you begin treatment, you should gradually start to feel better. Go easy on yourself during this time. Try to do things you used to enjoy. Even if you don’t feel like doing them, they can improve your mood. Other things that may help:
- Try to get some physical activity. Just 30 minutes a day of walking can boost mood.
- Try to maintain a regular bedtime and wake-up time.
- Eat regular, healthy meals.
- Do what you can as you can. Decide what must get done and what can wait.
- Try to connect with other people, and talk with people you trust about how you are feeling.
- Postpone important life decisions until you feel better.
- Avoid using alcohol, nicotine, or drugs, including medications not prescribed for you.
How can I help a loved one who is depressed?
If someone you know has depression, help them see a health care provider or mental health professional. You also can:
- Offer support, understanding, patience, and encouragement.
- Invite them out for walks, outings, and other activities.
- Help them stick to their treatment plan, such as setting reminders to take prescribed medications.
- Make sure they have transportation to therapy appointments.
- Remind them that, with time and treatment, the depression will lift.
Take comments about suicide seriously, and report them to your loved one’s health care provider or therapist. If they are in immediate distress or thinking about hurting themselves, call 911 for emergency services or go to the nearest hospital emergency room.
Where can I find clinical trials for depression?
Clinical trials are research studies that look at new ways to prevent, detect, or treat diseases and conditions. Although individuals may benefit from being part of a clinical trial, participants should be aware that the primary purpose of a clinical trial is to gain new scientific knowledge so others may receive better help in the future.
Researchers at the National Institute of Mental Health (NIMH) and around the country conduct many studies with patients and healthy volunteers. Talk to your health care provider about clinical trials, their benefits and risks, and whether one is right for you. For more information, visit NIMH's clinical trials information.
Reprints
This publication is in the public domain and may be reproduced or copied without permission from NIMH. Citation of NIMH as a source is appreciated. To learn more about using NIMH publications, please contact the NIMH Information Resource Center at 1-866‑615‑6464, email nimhinfo@nih. gov, or refer to our reprint guidelines.
gov, or refer to our reprint guidelines.
For More Information
MedlinePlus (National Library of Medicine) (en español)
ClinicalTrials.gov (en español)
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
National Institutes of Health
NIH Publication No. 21-MH-8079
Revised 2021
Depression Diagnosis and Screening: What Doctors Look For
Written by Debra Fulghum Bruce, PhD
In this Article
- How Is Depression Diagnosed?
- Diagnosing Depression and the Physical Exam
- Depression Screening Tests
- What Does the Doctor Look for to Make a Depression Diagnosis?
- How Can Depression Symptoms Lead to a Depression Diagnosis?
- Are There Physical Signs of Depression?
- How Can I Help the Doctor Make a Proper Diagnosis?
- How Do I Know When to Seek Help?
How Is Depression Diagnosed?
Depression is often diagnosed through a combination of lab tests and simply talking to a patient.
To effectively diagnose and treat depression, the doctor must hear about specific symptoms of depression. They may use a series of standard questions to screen for depression. While a physical examination will reveal a patient's overall state of health, by talking with a patient, a doctor can learn about other things that are relevant to making a depression diagnosis. A patient, for example, can report on such things as daily moods, behaviors, and lifestyle habits.
A depression diagnosis is often difficult to make because clinical depression can show up in so many different ways. For example, some clinically depressed people seem to withdraw into a state of apathy. Others may become irritable or even agitated. Eating and sleeping patterns can be exaggerated. Clinical depression may cause someone to sleep or eat to excess, or almost eliminate those activities.
Observable or behavioral symptoms of clinical depression also may sometimes be minimal despite profound inner turmoil. Depression can be an all-encompassing disorder, and it affects a person's body, feelings, thoughts, and behaviors in varying ways.
Depression can be an all-encompassing disorder, and it affects a person's body, feelings, thoughts, and behaviors in varying ways.
Types of depression your doctor may look for
It used to be that all mood disorders were lumped together. Now, a doctor will make a distinction about the particular disorder or subtype of depression that a patient has. For example, a doctor will determine whether a patient has major depression, chronic depression including dysthymia, seasonal affective disorder (SAD), bipolar disorder, or some other type of clinical depression.
Diagnosing Depression and the Physical Exam
Your doctor may include standard tests as part of the initial physical exam. Among them may be blood tests to check electrolytes, liver function, toxicology screening, and kidney function. Because the kidneys and liver are responsible for the elimination of depression medications, impairment to either of these two organs may cause the drugs to accumulate in the body.
Other tests may sometimes include:
- CT scan or MRI of the brain to rule out serious illnesses such as a brain tumor
- Electrocardiogram (EKG) to diagnose some heart problems
- Electroencephalogram (EEG) to record electrical activity of the brain
Depression Screening Tests
After discussing your mood and the way it affects your life, your doctor may also ask you questions that are used specifically to screen for depression. The inventories and questionnaires the doctor may use are just one part of the medical process of diagnosing depression. These tests, however, can sometimes give your doctor better insight into your mood. They can use them to make a diagnosis with more certainty.
One example of a screening test is a two-part questionnaire that has been shown to be highly reliable in identifying the likelihood of depression. When you take this test, you will be asked to answer two questions:
- During the past month, have you been bothered by feeling down, depressed, or hopeless?
- During the past month, have you been bothered by little interest or pleasure in doing things?
Your answer to the two questions will determine what the doctor does next. The doctor may ask you additional questions to help confirm a diagnosis of depression. Or if your answers indicate you do not have depression, the doctor may review your symptoms again to continue the effort to find the cause. Studies show that these two questions, especially when used with another test as part of the assessment process, are highly effective tools for detecting most cases of depression.
The doctor may ask you additional questions to help confirm a diagnosis of depression. Or if your answers indicate you do not have depression, the doctor may review your symptoms again to continue the effort to find the cause. Studies show that these two questions, especially when used with another test as part of the assessment process, are highly effective tools for detecting most cases of depression.
Your doctor may use other depression screening instruments that measure the presence and severity of depression symptoms. Examples include:
- The Patient Health Questionnaire-9 (PHQ-9), a nine-item, self-administered diagnostic screening and severity tool based on current diagnostic criteria for major depression
- Beck Depression Inventory (BDI), a 21-question, multiple-choice self-report that measures the severity of depression symptoms and feelings
- Zung Self-Rating Depression Scale, a short survey that measures the level of depression, ranging from normal to severely depressed
- Center for Epidemiologic Studies-Depression Scale (CES-D), an instrument that allows patients to evaluate their feelings, behavior, and outlook from the previous week
- Hamilton Rating Scale for Depression (HRSD), also known as the Hamilton Depression Rating Scale (HDRS) or HAM-D, a multiple-choice questionnaire that doctors may use to rate the severity of a patient's depression
When you take a test or inventory, you may feel uncomfortable responding honestly to questions or statements that are made.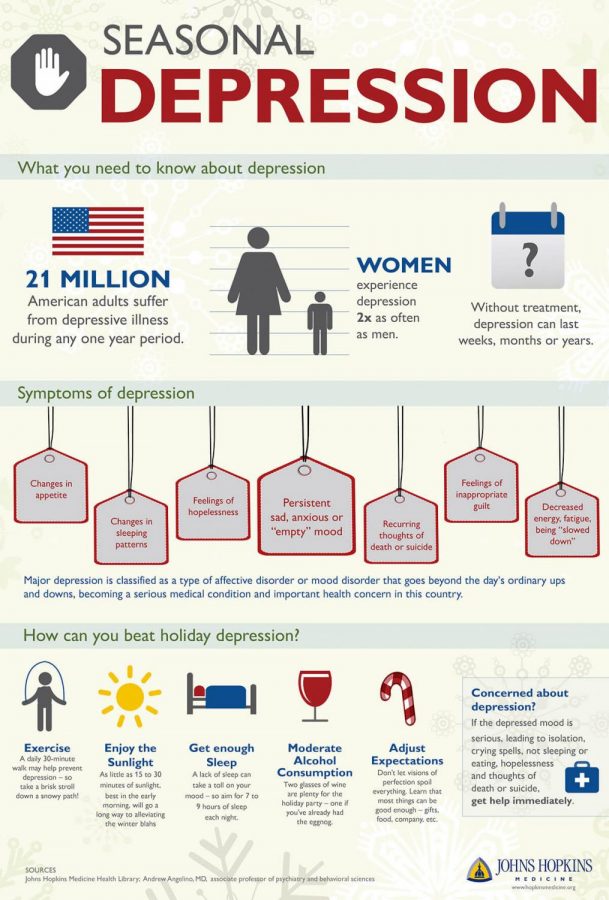 The person who administers the test will be asking about depression and mood, depression and cognition, and the physical feelings of depression such as lack of energy, sleep disturbance, and sexual problems. Be as honest as you can when assessing your symptoms. Questionnaires and screening tools can help a mental health professional in making a diagnosis, but rating scales in themselves are not a substitute for a clinical diagnosis made from a thorough interview. Once your doctor has made an accurate diagnosis, they can then prescribe an effective treatment.
The person who administers the test will be asking about depression and mood, depression and cognition, and the physical feelings of depression such as lack of energy, sleep disturbance, and sexual problems. Be as honest as you can when assessing your symptoms. Questionnaires and screening tools can help a mental health professional in making a diagnosis, but rating scales in themselves are not a substitute for a clinical diagnosis made from a thorough interview. Once your doctor has made an accurate diagnosis, they can then prescribe an effective treatment.
What Does the Doctor Look for to Make a Depression Diagnosis?
Your doctor will evaluate your symptoms, including how long you've had them, when they started, and how they were treated. They'll ask about the way you feel, including whether you have any symptoms of depression such as:
- Sadness or depressed mood most of the day or almost every day
- Loss of enjoyment in things that were once pleasurable
- Major change in weight (gain or loss of more than 5% of weight within a month) or appetite
- Insomnia or excessive sleep almost every day
- Physical restlessness or sense of being run-down that others can notice
- Fatigue or loss of energy almost every day
- Feelings of hopelessness or worthlessness or excessive guilt almost every day
- Problems with concentration or making decisions almost every day
- Recurring thoughts of death or suicide, suicide plan, or suicide attempt
How Can Depression Symptoms Lead to a Depression Diagnosis?
To be diagnosed with major depression, you must have at least five of the symptoms listed above with at least one of the first two nearly daily for at least 2 weeks.
Depression symptoms can last weeks, months, or sometimes years. They can affect personality and interfere with social relationships and work habits, potentially making it difficult for others to have empathy for you. Some symptoms are so disabling that they interfere significantly with your ability to function. In very severe cases, people with depression may be unable to eat, maintain their hygiene, or even get out of bed.
Episodes may happen only once in a lifetime or may be recurrent, chronic, or longstanding. In some cases, they seem to last forever. Symptoms may appear to be precipitated by life crises. At other times, they may seem to happen at random.
Clinical depression commonly goes along with other medical illnesses such as heart disease or cancer and worsens the prognosis for these illnesses.
Are There Physical Signs of Depression?
Yes. In fact, a great many people with depression come to their doctor first with only physical issues. You might notice:
- Back pain
- Headaches
- Joint pain
- Limb pain
- Gut problems (digestion issues and belly pain)
- Constant tiredness
- Sleep problems
- Slowing of physical movement and thinking
You might notice these symptoms even before you notice the mental health symptoms of depression, or you might notice them at the same time. Your doctor can help you figure out the source of your symptoms.
Your doctor can help you figure out the source of your symptoms.
How Can I Help the Doctor Make a Proper Diagnosis?
Before your appointment, write down your concerns about depression and specific symptoms of depression you might have. It’s also helpful to get an in-depth family history from relatives before meeting with your doctor. This information can help the doctor make an accurate diagnosis and ensure effective treatment. Before your visit, think about and write down:
- Your mental and physical health concerns
- Symptoms you've noticed
- Unusual behaviors you've had
- Past illnesses
- Your family history of depression
- Medications you’re taking now and in the past, including both prescribed and over-the-counter medications
- Unusual side effects of medications you are taking or have taken
- Natural dietary supplements you’re taking
- Your lifestyle habits (exercise, diet, smoking, alcohol consumption, drug use)
- Your sleep habits
- Causes of stress in your life (marriage, work, social)
- Questions you have about depression and depression medications
How Do I Know When to Seek Help?
The biggest hurdle to diagnosing and treating depression is recognizing that someone has it. Unfortunately, about half of the people who have depression never get diagnosed or treated. And not getting treatment can be life threatening: More than 10% of people who have depression take their own lives.
Unfortunately, about half of the people who have depression never get diagnosed or treated. And not getting treatment can be life threatening: More than 10% of people who have depression take their own lives.
When depression is hurting your life, such as causing trouble with relationships, work issues, or family disputes, and there isn't a clear solution to these problems, you should seek help to keep things from getting worse, especially if these feelings last for any length of time.
If you or someone you know is having suicidal thoughts or feelings, call 911 or go to the emergency room right away.
Depression Guide
- Overview & Causes
- Symptoms & Types
- Diagnosis & Treatment
- Recovering & Managing
- Finding Help
Treatment of depression: a psychotherapist on how to identify the disease and why take pills
Health
Together with the scientific director of the psychological center "Quality of Life", psychotherapist, Ph.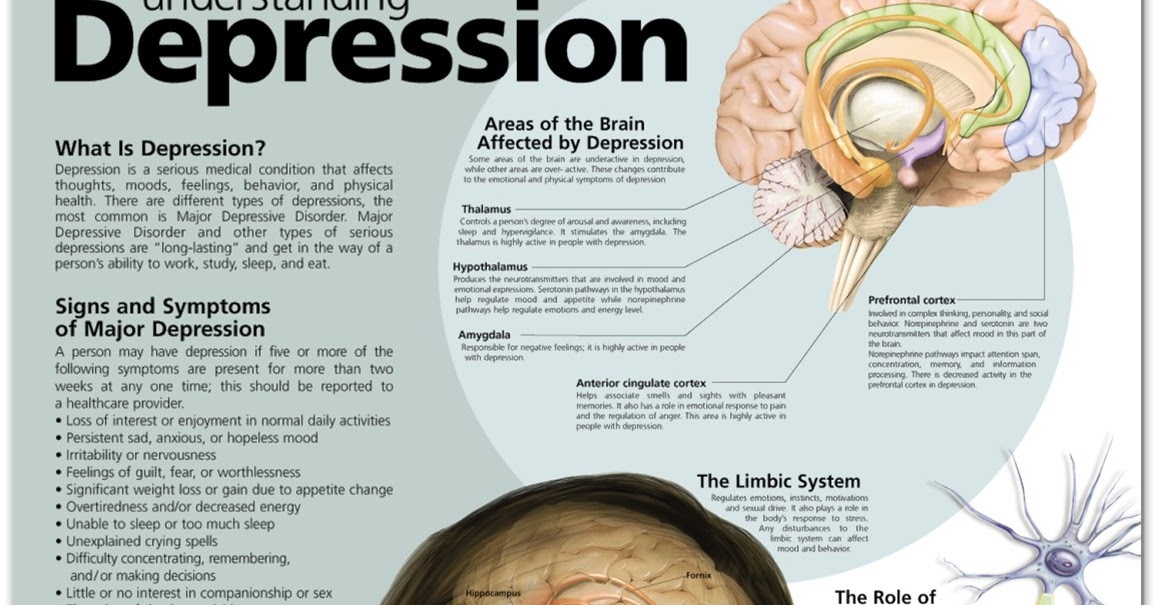 D. Alexander Erichev understands why depressive disorders occur and which of us is more prone to them, in which cases antidepressants can help (and what they do to the body), and in which - talking with a doctor, and can a feeling of depression haunt you for years?
D. Alexander Erichev understands why depressive disorders occur and which of us is more prone to them, in which cases antidepressants can help (and what they do to the body), and in which - talking with a doctor, and can a feeling of depression haunt you for years?
How do I know if I'm depressed?
From a medical point of view, depression is called when there is a low mood for at least two weeks in a row. And a number of other symptoms: negative thoughts about the present and the future, impaired concentration, impaired appetite (more often a decrease, but women may, on the contrary, jam), sleep disturbance. It often happens that a person wakes up early and can no longer fall asleep. Sometimes, on the contrary, in a depressive state, classic insomnia occurs: it is difficult to fall asleep, unpleasant thoughts come into your head, often against this background, a person begins to lose weight. Depression is dangerous, including the fact that a person can seriously think about suicide. This is not to prove anything to anyone. It’s just that during depression it seems to him that there is nowhere to wait for help, but there is no way out. Of course, it is impossible to independently diagnose a depressive disorder, but everyone is able to suspect its presence. For example, you can use the Depression Test developed by Aaron Beck.
This is not to prove anything to anyone. It’s just that during depression it seems to him that there is nowhere to wait for help, but there is no way out. Of course, it is impossible to independently diagnose a depressive disorder, but everyone is able to suspect its presence. For example, you can use the Depression Test developed by Aaron Beck.
Is it true that depression is a characteristic disease of our time? And that far fewer people suffered from it before?
If we are talking about anxiety and depression, then over the past hundred years there has indeed been a multiple increase in these manifestations. The fact is that a hundred years ago, in principle, little attention was paid to mild manifestations of mental illness. But the quality of life is improving, and we began to think about conditions that are already different from the norm, but not quite terrible. The increase in the incidence is observed, including for this reason.
There is one more hypothesis (namely, hypotheses) why more and more anxiety-depressive disorders appear in modern society. This is explained by the fact that social ties between people are weakening, and the pace of life and information load are increasing. You can have thousands of friends on Facebook, but at the same time, a lack of live warm communication and support from others. This is indeed considered one of the factors influencing the rise in depressions.
This is explained by the fact that social ties between people are weakening, and the pace of life and information load are increasing. You can have thousands of friends on Facebook, but at the same time, a lack of live warm communication and support from others. This is indeed considered one of the factors influencing the rise in depressions.
Why does depression occur at all? Is it true that some people are predisposed to them initially?
Some time ago, in psychotherapy, endogenous depressions (that is, more due to biological prerequisites) and neurotic depressions (in which a person's intrapersonal conflict is "to blame") were singled out separately. For endogenous depressions, for example, seasonality is characteristic. Autumn has come or spring has come - the mood has suddenly decreased. Also characterized by early awakenings, appetite disturbances, more pronounced weight loss, bad mood in the morning and some improvement in the evenings.
In case of neurotic depression, the symptoms manifest themselves differently: it is usually difficult for a person to fall asleep, loss of appetite and body weight is less pronounced. Often there is no inhibition, which, with endogenous depressions, can be serious in a person. Clinicians try to take into account these differences. Because the closer depression is to endogenous, the more points of application for drug treatment. And the more depression is associated with external factors, the more attention is paid to psychotherapy. However, now more and more often they refuse such a division, because they believe that in any depression there is a contribution from both a biological component and a psychological one.
Often there is no inhibition, which, with endogenous depressions, can be serious in a person. Clinicians try to take into account these differences. Because the closer depression is to endogenous, the more points of application for drug treatment. And the more depression is associated with external factors, the more attention is paid to psychotherapy. However, now more and more often they refuse such a division, because they believe that in any depression there is a contribution from both a biological component and a psychological one.
Up to 20% of women and up to 10% of men experience depression (they seek help less often)
Can you understand that you are biologically predisposed to depression?
We can talk about predisposition again at the level of a hypothesis. For example, if a number of my close relatives suffered from severe depression, then it is more likely that I am also at risk.
How can you know for sure that depression is caused by processes in the body?
There is no device that will show the presence of endogenous depression. Yes, studies are now being published from the series “which areas of the brain in people with long-term depression change and which connections are broken”, but this is all just research so far. Perhaps someday there will be clearer instrumental criteria by which it would be possible to diagnose depression. But so far it is impossible to say according to one biological parameter: “My friend, you have biological depression!” The most important thing here is a structured questioning of a specialist.
Yes, studies are now being published from the series “which areas of the brain in people with long-term depression change and which connections are broken”, but this is all just research so far. Perhaps someday there will be clearer instrumental criteria by which it would be possible to diagnose depression. But so far it is impossible to say according to one biological parameter: “My friend, you have biological depression!” The most important thing here is a structured questioning of a specialist.
Can my genes be to blame for my depressive disorder?
Yes, certainly genetics makes a significant contribution. However, the latest research also plays an important role in epigenetics: it turned out that in certain periods of time our body is much more sensitive to external influences. And it is capable of launching serious changes, which will then accompany a person throughout his life. Such exposure may be an early stressful experience. For example, separation from mother, child neglect, physical and sexual abuse, emotional rejection. There are a number of studies that show that traumatic events in childhood can seriously increase the risk of anxiety-depressive disorders in adulthood.
There are a number of studies that show that traumatic events in childhood can seriously increase the risk of anxiety-depressive disorders in adulthood.
In general, if we take any of us, then everyone has a chance of developing depression. Could it be that the stress might be too high for us? May be. Maybe that the protective forces are not enough to cope with it? Of course. In many respects, the role is played by what kind of stress we experienced. If a particular person's main fear is loneliness and rejection, then the loss of warm meaningful relationships will more provoke the development of depression, and then go into depression. Others have a different value system, and the most important points for them are status, financial condition. And the same dismissal or bankruptcy can play a cruel joke on such a person.
So depression is triggered by a specific stressful situation?
Everyone is different. Depressions are very versatile. You know how to say you have a cough. But behind a cough as a symptom, allergies, smoker's bronchitis, and tuberculosis can be hidden. Same here. Of course, the psychotherapist is more often treated by people whose depression occurs against the background of stressful events. One of the most emotionally complex reasons for conversion in psychotherapeutic practice is the reaction of loss. If a loved one dies, they say that depression is a retribution for love. And the more you loved, the more you were attached, the more likely it is that an acute state of depression will develop.
But behind a cough as a symptom, allergies, smoker's bronchitis, and tuberculosis can be hidden. Same here. Of course, the psychotherapist is more often treated by people whose depression occurs against the background of stressful events. One of the most emotionally complex reasons for conversion in psychotherapeutic practice is the reaction of loss. If a loved one dies, they say that depression is a retribution for love. And the more you loved, the more you were attached, the more likely it is that an acute state of depression will develop.
Not strong, but prolonged stress can lead to depression
Stressful events can be not only momentary, but also chronic. For example, a woman lives with an alcoholic husband and tries to control him. This story has no beginning and no end. She tenses all the time - why there is no money at home, why the family is not as we would like, why the husband does not change. And the likelihood that this will eventually lead her to depression is very high. The same factors include constant conflicts at work. It's one thing when a person comes to work and generally understands why he does it. Yes, it can be difficult for him. Yes, sometimes he struggles with tasks. But in general, he feels that the team supports him, and he himself does the right thing and approaches his goals. Another thing is when he comes to work every day thinking that he is not liked here, that nothing good can be expected from colleagues, that his work does not make sense. Such a perception of one's activity and the emotions associated with it will make a serious contribution to the treasury of depression. Prolonged stress (even if not very strong) can destroy psychological well-being slowly but steadily.
The same factors include constant conflicts at work. It's one thing when a person comes to work and generally understands why he does it. Yes, it can be difficult for him. Yes, sometimes he struggles with tasks. But in general, he feels that the team supports him, and he himself does the right thing and approaches his goals. Another thing is when he comes to work every day thinking that he is not liked here, that nothing good can be expected from colleagues, that his work does not make sense. Such a perception of one's activity and the emotions associated with it will make a serious contribution to the treasury of depression. Prolonged stress (even if not very strong) can destroy psychological well-being slowly but steadily.
When to take antidepressants and what they do to the body
If we are talking about the treatment of depression, then there are three options - psychotherapy, drug treatment, or both. In what cases and what should be resorted to?
If we are talking about moderate or severe depression (in which, for example, a person loses a lot of weight, behaves inhibitedly, he has suicidal thoughts and a pronounced feeling of guilt gnaws at him), then in this case, medication becomes a priority. therapy. And it is very important to start with medicines so that a person does not burrow further in his condition. Yes, psychotherapy is also needed. But at the initial stage, it will just complement drug therapy, gradually increasing its share in the treatment process more and more.
therapy. And it is very important to start with medicines so that a person does not burrow further in his condition. Yes, psychotherapy is also needed. But at the initial stage, it will just complement drug therapy, gradually increasing its share in the treatment process more and more.
The question is more difficult when a person has a slight degree of mood depression. Variations are possible here, because even in different countries there are different treatment protocols. For example, in England it was decided that psychotherapy is used first in mild stages. And only if it turns out to be ineffective, then they switch to antidepressants. But they have made significant progress in increasing the availability of psychotherapeutic care for the population.
At the same time, there can also be stratification in the camp of specialists: each sandpiper praises his own swamp and his own approach. The closer a person is to biological psychiatry, the more often he advocates for the prescription of medicinal help. The closer to the format of the implementation of psychotherapeutic assistance, the more often it begins to lobby for its endless use. The truth, as always, is somewhere in the middle (especially since modern guidelines most often recommend a combination of psychotherapy and medication).
The closer to the format of the implementation of psychotherapeutic assistance, the more often it begins to lobby for its endless use. The truth, as always, is somewhere in the middle (especially since modern guidelines most often recommend a combination of psychotherapy and medication).
There are also paradoxical cases with the patients themselves. For example, a person has all the manifestations of biological depression, but he is tuned only to psychotherapy. And the specialist has to explain that this may not be enough. At the same time, a person may come who has all the symptoms of a slight decrease in mood due to life's adversities, which, from a professional point of view, are still within the framework of a bad mood. But he demands to urgently prescribe him pills, because his neighbor took them and it helped him a lot.
How long should I take antidepressants?
Generally, antidepressants are prescribed for at least 6 months. And this is from the moment of improvement.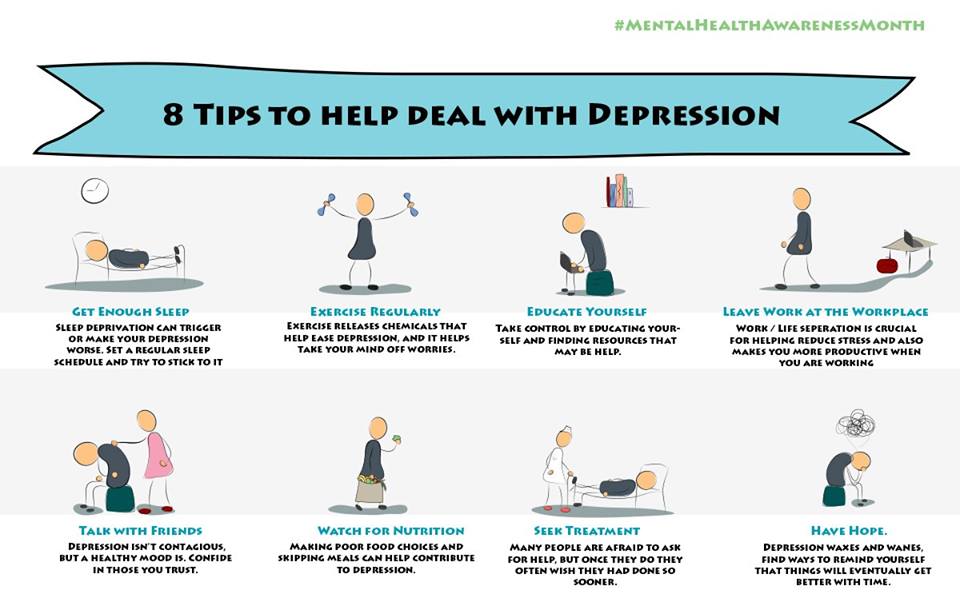 Usually, the effect of this group of drugs begins to develop 3-4 weeks after the start of treatment. These are not the drugs that are used as "ambulance". If we compare the effect of antidepressants with the effect of alcohol, then we can say that this is such alcohol, drinking which a person gets an effect (normalization of mood) after a few weeks and gently and gradually. If this were the case with alcohol, then there would be much fewer dependent people. Therefore, myths about dependence on antidepressants in most cases do not correspond to reality.
Usually, the effect of this group of drugs begins to develop 3-4 weeks after the start of treatment. These are not the drugs that are used as "ambulance". If we compare the effect of antidepressants with the effect of alcohol, then we can say that this is such alcohol, drinking which a person gets an effect (normalization of mood) after a few weeks and gently and gradually. If this were the case with alcohol, then there would be much fewer dependent people. Therefore, myths about dependence on antidepressants in most cases do not correspond to reality.
It is important to understand that there are many drugs and it is not always possible to choose the right one the first time. Yes, sometimes it happens that the doctor prescribed drug therapy and the person felt better after 3-4 weeks. He is already cheerful, goes to work, takes one pill a day and does not think about anything bad. Maybe there are some side effects, but usually they are not pronounced.
An antidepressant is an alcohol, the effect of which you get in a few weeks
Another option (fortunately, more rare) - a person comes for help to a specialist, he is prescribed therapy.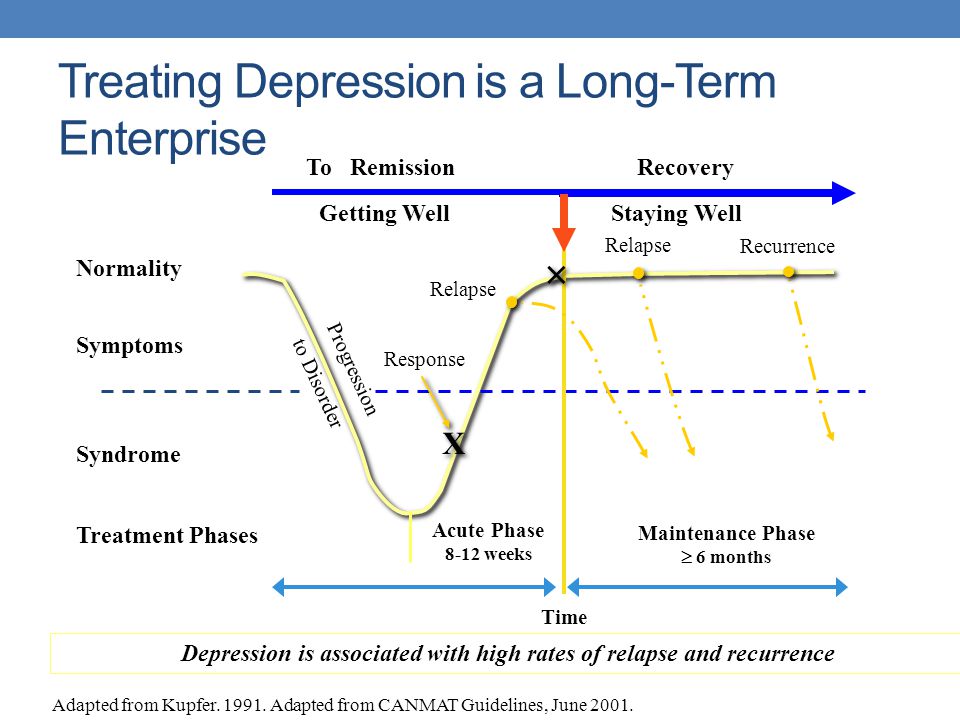 One and the same drug, first at a low dosage, then at an average, then at a high one. The response is insufficient. Change to another drug, then to the third. And it happens that a person manages to help only on the third or fourth attempt. The selection of the drug can take quite a long time.
One and the same drug, first at a low dosage, then at an average, then at a high one. The response is insufficient. Change to another drug, then to the third. And it happens that a person manages to help only on the third or fourth attempt. The selection of the drug can take quite a long time.
In medicine, there is now a large selection of antidepressants, different groups, with different dosing regimens and their own characteristics. Everyone has a different chemical structure and different tolerability. At the same time, one person from the drug may not have any side effects at all, while another person of the same age may experience difficulties.
According to the action, antidepressants can be conditionally divided into stimulating, sedative and balanced. Stimulants are needed when a person is dominated by lethargy, apathy and reduced performance. Sedatives are well suited for combinations of depression and anxiety, as well as for correcting sleep disorders.
Many people are afraid of antidepressants, among other things, because after withdrawal they may feel worse again.
On the one hand, antidepressants are a cast under which a fracture can heal. And it is logical that if the plaster is removed, and the fracture did not have time to grow together, then it makes sense to impose it for a longer period of time. Therefore, sometimes the course of treatment with them can take a long period of time. On the other hand, there are cases when a person, taking medication, does not particularly change his style and way of life, does not learn to better cope with stress, does not fight the habit of catastrophizing events. With the abolition of drug therapy in any case, the condition may worsen, but this is more likely to occur when a person does not master the skills to cope with the emotional burden.
By the way, how should a person on antidepressants feel? If there are moments of euphoria - is it bad?
Episodes when the mood is too high (especially if sleep began to decrease significantly, because the person is too good, his activity is much higher than usual) - this is not a very good signal and it is necessary to report it to the supervising specialist. For a number of people, not only downturns are characteristic, but also pronounced upswings in mood.
For a number of people, not only downturns are characteristic, but also pronounced upswings in mood.
About the return of depression and long-term depression
Is it true that if depression was once, then it can happen again?
Everything is different here. If we are talking about depression, which is closer to endogenous (biological) with its roots, then relapses are of course more likely. And if a person has already suffered three or four episodes, then the risk that there will be a fifth is much higher than if it happened once. Another thing is that some people experience a decrease in mood after traumatic stressful events. Further, such injuries do not happen to him, and depression does not bother him either.
Have you met people who were depressed for several years?
Of course, there is such a term as dysthymia - when a person has little pleasure, he has a chronically depressed mood, which leads to significant discomfort, but still allows him to cope with the basic requirements of everyday life.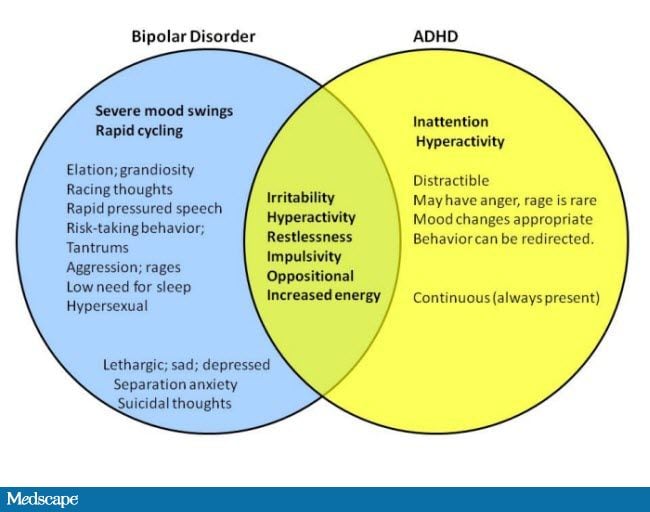
Does it happen that a person with depression cannot be helped at all?
Whatever we say, depressive disorders are currently treated fairly well. If a person is properly treated, then the probability of coping with current problems is very high. Problems are more likely to arise when people refuse help, isolate themselves, self-medicate, and so on. The state when nothing can be helped at all is an exclusive, a rarity. There are resistant depressions that are very difficult to correct. But, fortunately, this is not so common.
About whether depression can be cured by talking to a psychotherapist
Why do you think many people with depression do not get to specialists?
The first reason is that people themselves do not always understand that they have depression and need help. Secondly, there is no support and understanding from loved ones. Some people think that anxiety-depressive disorder is some kind of whim. Now, if there were no hands, it would be a problem. And here is some depression. In addition, the accusation of a person that he himself is to blame for his condition may begin.
Now, if there were no hands, it would be a problem. And here is some depression. In addition, the accusation of a person that he himself is to blame for his condition may begin.
Thirdly, unfortunately, in society there is an idea of psychotherapeutic assistance as something focused only on patients with schizophrenia and other severe mental disorders.
Depression?! Now, if there were no hands, it would be a problem.
Fourth, the idea that quality care is unavailable. There is an opportunity to get both paid and free help. In the city there is a Clinic of neuroses named after. I.P. Pavlova, urban psychotherapeutic centers, in each district there is a psycho-neurological dispensary, where psychotherapists also work. The question is how a person seeks help for himself.
How many psychotherapy sessions would it take to get a person out of this state?
For each individual. A number of studies show that cognitive behavioral therapy can often be effective within 10-12 sessions. That is, this is work for three to four months, if classes are held once a week. But it happens that a mood disorder is combined with underlying disorders and personality conflicts. Then the course of psychotherapy can take much longer.
That is, this is work for three to four months, if classes are held once a week. But it happens that a mood disorder is combined with underlying disorders and personality conflicts. Then the course of psychotherapy can take much longer.
All psychotherapists work differently. Is it important for a person to understand what method the doctor uses, to which he has reached?
The main thing is that only a certified psychotherapist or psychiatrist should be involved in the diagnosis and pharmacological treatment of depression. When it comes to psychotherapy itself, it is useful to imagine what method a particular specialist owns. When the development of a psychotherapist goes in a particular direction, he is a member of specialized communities, grows, undergoes his own supervision, regularly studies (and so on throughout his professional life!) and so on. In terms of large international studies, there are methods whose effectiveness is better researched and justified. For example, the same cognitive-behavioral psychotherapy for depression.
For example, the same cognitive-behavioral psychotherapy for depression.
How, for example, in the case of CBT, how to understand that this is it?
These are, first of all, structured homework assignments. With depression, work with mental chewing gum (ruminations) most often begins, so that a person learns to stop and postpone it. Ruminations significantly impair the quality of life, so learning to deal with them is an important task. At the initial stages, behavioral activation is also often used - when a person, together with a specialist, plans small pleasant things and learns to implement them. Indeed, even with a relatively unstable decrease in mood, a person refuses something good, because it seems to him that it will not bring pleasure. Thus, he drives himself more and more into the corner of a joyless existence. Perfectionism and the closely related procrastination are also important targets for collaboration. Cognitive therapists work with thoughts and beliefs about themselves, about the future, with distortions in the perception of events. Quite often, diary entries are used. That is, a person analyzes when his mood changed and in connection with what. The relationship in cognitive behavioral therapy is similar to the coach-athlete model. The patient actively participates in the process and becomes more psychotherapeutic towards himself.
Quite often, diary entries are used. That is, a person analyzes when his mood changed and in connection with what. The relationship in cognitive behavioral therapy is similar to the coach-athlete model. The patient actively participates in the process and becomes more psychotherapeutic towards himself.
Doctor's advice
Try to notice the pleasant moments in life and move towards your own goals and values. Spend time on warm communication with those people with whom you feel good. If something goes wrong, then the most important thing is not to despair. Even if you have developed depression, there is always a way out of it.
Follow our news on Telegram
Author:
Katerina Reznikova,
reasons, how to understand that you have depression, how long it lasts, is it possible to get out of it on your own
Please explain in simple words what depression is. For example, how long can it last? How can I tell if I or someone close to me has depression?
For example, how long can it last? How can I tell if I or someone close to me has depression?
Is it possible to cope with depression without the help of a specialist? Can depression go away on its own?
Are there any official data for the world and Russia, how many people are in a state of depression? How many have been there?
Does depression depend on gender, age, nationality, faith, sexual orientation and place of residence, or are they unrelated to each other?
If there is an addiction, then who is more susceptible to depression: men or women, children or adults, Russians or Americans, Christians or Muslims, heterosexuals or homosexuals, Muscovites or Omsk residents, city dwellers or villagers?
Yana Shagova
psychologist
Author profile
Depression is a mental disorder. Its main manifestations are as follows: decreased mood, inability to enjoy life, severe apathy, pessimism, lack of strength. And the most disturbing symptom is suicidal thoughts.
And the most disturbing symptom is suicidal thoughts.
It is often difficult for a depressed person to maintain full-fledged relationships even with those closest to him, to do household chores, to take care of himself. And also - to study and work productively, since depression often negatively affects cognitive abilities and brain function in general.
According to the currently main hypothesis of the occurrence of depression - the monoamine theory - during this disease, malfunctions of neurotransmitters occur. These are substances with the help of which brain cells exchange information with each other, in particular monoamines: serotonin, dopamine and norepinephrine.
Understanding Depression - American Psychiatric Association
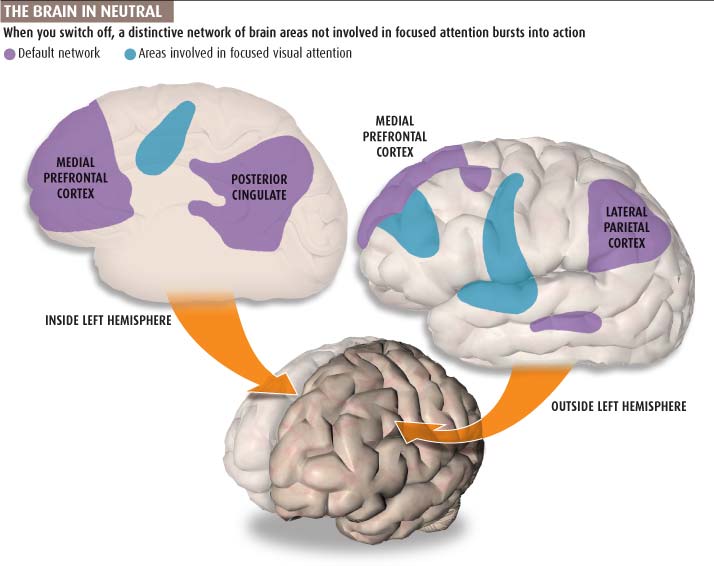
Depression is also known to alter some parts of the brain, such as the hippocampus, which is responsible for memory and emotional regulation, the prefrontal cortex, which processes information from the hippocampus, and the amygdala, which plays a role in the formation of fear and other emotions.
Go see a doctor
Our articles are written with love for evidence-based medicine. We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
What causes depression
Predisposition to depression is determined by various factors. One of the most important is genetics. People whose immediate family members have had the disorder may be more likely to develop it.
Genetic Causes of Major Depressive Disorder - Psychological Medicine
Other significant risk factors are psychological and social.
Psychological factors include, for example, the conditions in which a person grows up and how others treat him during this period. If a child receives a lot of love and support, they are less likely to suffer from depression as an adult. Conversely, those who are often abused and humiliated in childhood have a higher risk of developing this disease.
Conversely, those who are often abused and humiliated in childhood have a higher risk of developing this disease.
Social factors that can trigger depression are, for example, low income and the city and region where the person lives. I will tell you more about this below.
Community 08/24/21
How to get rid of the idea that there is not enough money?
Another common cause is somatic diseases: hormonal failure or an acute deficiency of some substances. In addition, depression can be provoked by severe stress caused, for example, by the loss of a loved one or the loss of a job.
How long depression can last
According to a study by Dutch doctors, in 50% of cases, a depressive episode lasted three months. At the same time, more than 20% of the symptoms of the disease did not go away even after two years.
Duration of episodes of major depressive disorder in the Dutch population - British Journal of Psychiatry
Duration of illness depends on the severity and severity of symptoms, individual characteristics and other factors. In addition, some people experience relapses: there is evidence that in 50% of cases depression returns and needs to be treated again.
In addition, some people experience relapses: there is evidence that in 50% of cases depression returns and needs to be treated again.
How to tell if you have depression
You can tell if a person is depressed by looking at their characteristic signs. The main one is a long-term decrease in mood. It can appear with different intensity. Someone due to depression feels a slight melancholy. Someone - an acute unwillingness to live.
In addition, you should be wary if you lost interest in your favorite activities for a long time - more than a month ago - and nothing brings you joy. For example, you absolutely do not want to go for a walk, play sports, see friends and relatives. Or if the feeling of boredom and routine does not leave. Or you are tormented by thoughts about your own uselessness and that you don’t know how and why to live. And the future seems exceptionally gloomy, full of troubles and troubles.
Another important symptom is a constant feeling of physical weakness. Especially if it makes it difficult to force yourself to get out of bed, get dressed, take a shower and brush your teeth. And I want only one thing - to lie down, looking at one point.
Especially if it makes it difficult to force yourself to get out of bed, get dressed, take a shower and brush your teeth. And I want only one thing - to lie down, looking at one point.
Sleep and eating disorders can also signal depression. For example, insomnia or unusually long - 10-12 hours - sleep. And also a lack of appetite or, conversely, a strong craving for sweet and fatty foods, which provokes frequent overeating.
/insomnia/
How to deal with insomnia
Depressed people often suffer from memory and concentration problems, as well as the ability to process information and make decisions. If you notice that you often cannot choose products in the store, you begin to be late everywhere, forget about things, do your work more slowly, there is a reason to consult a doctor. Especially if all of the above is accompanied by a bad mood and gloomy thoughts.
Complete list of signs of depression
According to the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, a diagnosis of depression can be made if a person has five or more symptoms of depression within two weeks:
- Low mood or persistent irritability.

- Significant reduction in pleasure or interest in all or nearly all activities.
- Decrease or, conversely, increase in weight and appetite.
- Insomnia or too much sleep.
- Psychomotor agitation or inhibition.
- Decreased energy and increased fatigue.
- Feelings of worthlessness and low self-esteem or inadequate guilt.
- Inhibited thinking or reduced alertness.
- Suicidal thoughts.
Online self-diagnosis questionnaires for depression, such as the well-known Beck test, are not worth using: they are very inaccurate.
Is it possible to cope with depression on your own
In theory, you can cope with depression on your own. But in extremely rare cases - with its mild and short form. The problem is that a person is usually unable to assess the severity and severity of their symptoms and establish the cause of their occurrence.
Therefore, if you suspect a mental disorder, it is better to contact a specialist.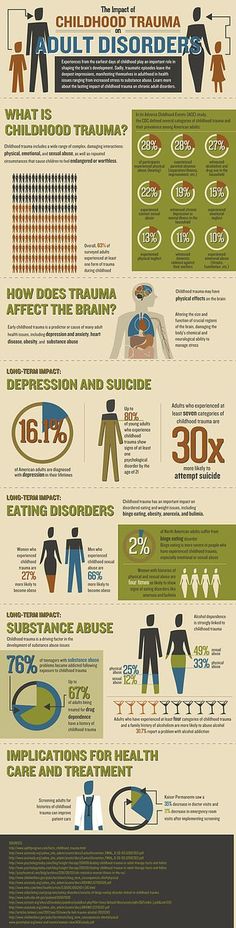 It is not so important who it will be at the initial stage: a psychologist, psychotherapist or psychiatrist. You will be helped to understand how to proceed further and whether treatment is necessary.
It is not so important who it will be at the initial stage: a psychologist, psychotherapist or psychiatrist. You will be helped to understand how to proceed further and whether treatment is necessary.
/postpartum-depression-treatment/
Dealing with postpartum depression
Depression is treated with specific medications. Often - in combination with psychotherapy. It has been proven that a combination of approaches gives the best effect. Other methods - mindfulness practices, yoga, physical activity - are useful and effective, but are of an auxiliary nature.
According to the rules in force in Russia, only psychiatrists and psychotherapists can decide on the appointment of drug therapy, select drugs, their dosage and adjust it in the course of treatment. Psychologists without a medical education are not entitled to do this.
A very small number of cases can be dispensed with without medication: when depression is mild, short-lived, and its symptoms are not pronounced.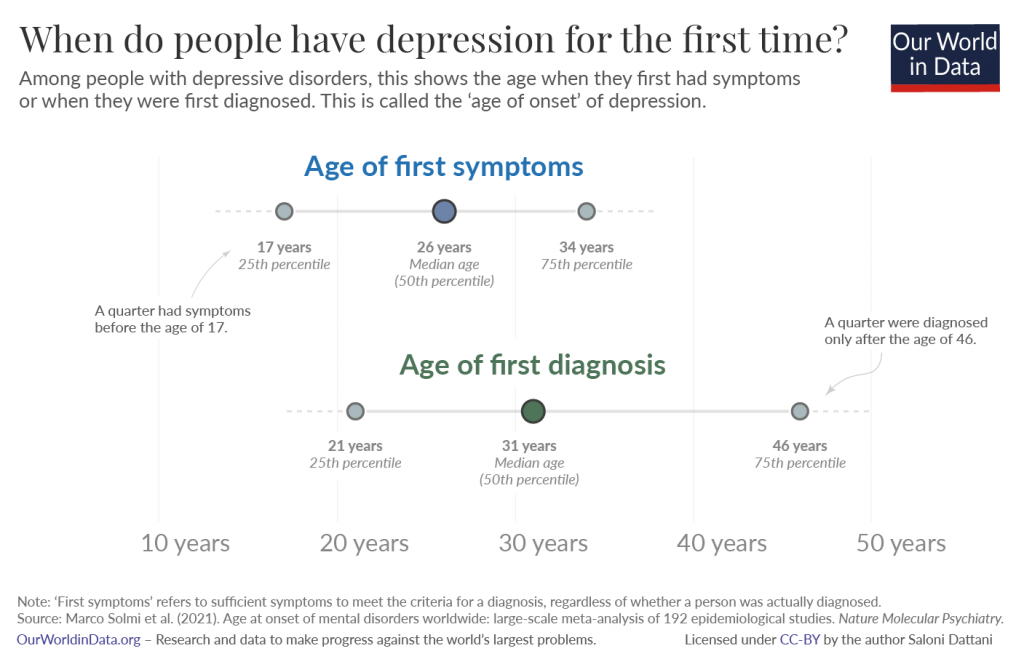 But again, the decision about this should be made by the doctor. I note that the side effects of modern drugs are much less inconvenient than the symptoms of depression, and they pass quite quickly. Therefore, you should not resist taking medication with all your might.
But again, the decision about this should be made by the doctor. I note that the side effects of modern drugs are much less inconvenient than the symptoms of depression, and they pass quite quickly. Therefore, you should not resist taking medication with all your might.
Treatment of depressive disorders with and without medication - Pharmacopsychiatry
And another important point. Sometimes depression is not an independent disease, but is part of other mental disorders. For example, bipolar affective or schizoaffective. They are treated differently than depression. Therefore, it is very important to make an accurate diagnosis at the very beginning: incorrectly prescribed therapy can aggravate the symptoms of the disease.
How many people suffer from depression
According to the World Health Organization, approximately 5% of the world's inhabitants suffer from depression. The top five countries in terms of the prevalence of depression are Ukraine, the USA, Estonia, Australia and Brazil. In them, this disease affects 5.7-6.3% of the population.
In them, this disease affects 5.7-6.3% of the population.
Russia - in eleventh place. According to WHO, more than 8 million - 5.5% - of the country's inhabitants have depression.
Most likely, these estimates are lower than the real numbers. Especially in less developed countries, where medicine is not so well prepared to diagnose and treat mental disorders. In addition, even in developed countries, depression is often not detected. Source: World Population Review, WHO data Most likely, these estimates are lower than the real numbers. Especially in less developed countries, where medicine is not so well prepared to diagnose and treat mental disorders. In addition, even in developed countries, depression is often not detected. Source: World Population Review, WHO dataWhat affects predisposition to depression
Place of residence. Residents of large cities are thought to be more likely to suffer from mental disorders, including depression. They are constantly exposed to stress due to noise pollution and strong lighting, crowded population, lack of full communication with loved ones and high pace of life.
Urbanization and Mental Disorders - Industrial Psychiatry Journal
But it cannot be argued that life in the countryside is better for the psyche: there is no data on this. In addition, the state of the psyche determines not only the place of residence, but also other factors. It is impossible to separate them from each other.
If a person lives in a small town and does not experience financial difficulties, communicates enough with relatives, plays sports, then we can assume that he is more likely to be mentally healthy than a conventional city dweller.
Nationality. There is no connection between nationality and predisposition to depression. On the other hand, the unfavorable socio-economic situation in the country of residence - poverty or political instability - seriously affects the development of any mental disorders.
Sexuality is also not directly related to depression. But the so-called minority stress that LGBT people experience in modern society makes them more vulnerable to mental disorders.
Community 07/27/21
What is the difference between sex and gender?
Gender and age. But gender may be a risk factor: women are twice as likely to be diagnosed with depression. This is explained not only by physiology, but also by the peculiarities of the social status: women are more often subjected to violence and earn less. They have to balance work, childcare and domestic work, and their career options are limited.
Why depression is more common among women - Journal of Psychiatry and Neuroscience
In addition, there is a hypothesis that men are simply less likely to seek medical and psychological help. Therefore, they are less likely to be diagnosed with depression.
By the way, depression is not as common in children of both sexes as it is in adults. It affects 3.2% of the general child population. And most often, depression is diagnosed in adults 18-25 years old.
Religion. A significant link between depression and religious beliefs has not yet been found: the results of studies on this subject are contradictory. On the one hand, there is evidence that believers and atheists experience fewer symptoms of depression than those who occupy an intermediate position in relation to religion.
A significant link between depression and religious beliefs has not yet been found: the results of studies on this subject are contradictory. On the one hand, there is evidence that believers and atheists experience fewer symptoms of depression than those who occupy an intermediate position in relation to religion.
On the other hand, a large study by scientists from Latin America showed that religious women over 65 years of age have an increased tendency to depression. But the reasons for this are unclear. The issue still needs to be studied.
/list/antidepressant-myths/
8 myths about antidepressants
What is the result
Depression is a mental disorder that, according to statistics, affects 5% of people in the world. It may not go away for years. The predisposition to depression is genetic. But a dysfunctional childhood, severe stress in adulthood, and some somatic disorders increase the likelihood of its occurrence.