Emdr therapy explained
What is EMDR? – EMDR Institute – EYE MOVEMENT DESENSITIZATION AND REPROCESSING THERAPY
Eye Movement Desensitization and Reprocessing (EMDR) is a psychotherapy treatment that was originally designed to alleviate the distress associated with traumatic memories (Shapiro, 1989a, 1989b). Shapiro’s (2001) Adaptive Information Processing model posits that EMDR therapy facilitates the accessing and processing of traumatic memories and other adverse life experience to bring these to an adaptive resolution. After successful treatment with EMDR therapy, affective distress is relieved, negative beliefs are reformulated, and physiological arousal is reduced. During EMDR therapy the client attends to emotionally disturbing material in brief sequential doses while simultaneously focusing on an external stimulus. Therapist directed lateral eye movements are the most commonly used external stimulus but a variety of other stimuli including hand-tapping and audio stimulation are often used (Shapiro, 1991).
Shapiro (1995, 2001) hypothesizes that EMDR therapy facilitates the accessing of the traumatic memory network, so that information processing is enhanced, with new associations forged between the traumatic memory and more adaptive memories or information. These new associations are thought to result in complete information processing, new learning, elimination of emotional distress, and development of cognitive insights. EMDR therapy uses a three pronged protocol: (1) the past events that have laid the groundwork for dysfunction are processed, forging new associative links with adaptive information; (2) the current circumstances that elicit distress are targeted, and internal and external triggers are desensitized; (3) imaginal templates of future events are incorporated, to assist the client in acquiring the skills needed for adaptive functioning.
FOR LAYPEOPLE
EMDR (Eye Movement Desensitization and Reprocessing) is a psychotherapy that enables people to heal from the symptoms and emotional distress that are the result of disturbing life experiences. Repeated studies show that by using EMDR therapy people can experience the benefits of psychotherapy that once took years to make a difference. It is widely assumed that severe emotional pain requires a long time to heal. EMDR therapy shows that the mind can in fact heal from psychological trauma much as the body recovers from physical trauma. When you cut your hand, your body works to close the wound. If a foreign object or repeated injury irritates the wound, it festers and causes pain. Once the block is removed, healing resumes. EMDR therapy demonstrates that a similar sequence of events occurs with mental processes. The brain’s information processing system naturally moves toward mental health. If the system is blocked or imbalanced by the impact of a disturbing event, the emotional wound festers and can cause intense suffering. Once the block is removed, healing resumes. Using the detailed protocols and procedures learned in EMDR therapy training sessions, clinicians help clients activate their natural healing processes.
Repeated studies show that by using EMDR therapy people can experience the benefits of psychotherapy that once took years to make a difference. It is widely assumed that severe emotional pain requires a long time to heal. EMDR therapy shows that the mind can in fact heal from psychological trauma much as the body recovers from physical trauma. When you cut your hand, your body works to close the wound. If a foreign object or repeated injury irritates the wound, it festers and causes pain. Once the block is removed, healing resumes. EMDR therapy demonstrates that a similar sequence of events occurs with mental processes. The brain’s information processing system naturally moves toward mental health. If the system is blocked or imbalanced by the impact of a disturbing event, the emotional wound festers and can cause intense suffering. Once the block is removed, healing resumes. Using the detailed protocols and procedures learned in EMDR therapy training sessions, clinicians help clients activate their natural healing processes.
More than 30 positive controlled outcome studies have been done on EMDR therapy. Some of the studies show that 84%-90% of single-trauma victims no longer have post-traumatic stress disorder after only three 90-minute sessions. Another study, funded by the HMO Kaiser Permanente, found that 100% of the single-trauma victims and 77% of multiple trauma victims no longer were diagnosed with PTSD after only six 50-minute sessions. In another study, 77% of combat veterans were free of PTSD in 12 sessions. There has been so much research on EMDR therapy that it is now recognized as an effective form of treatment for trauma and other disturbing experiences by organizations such as the American Psychiatric Association, the World Health Organization and the Department of Defense. Given the worldwide recognition as an effective treatment of trauma, you can easily see how EMDR therapy would be effective in treating the “everyday” memories that are the reason people have low self-esteem, feelings of powerlessness, and all the myriad problems that bring them in for therapy. Over 100,000 clinicians throughout the world use the therapy. Millions of people have been treated successfully over the past 33 years.
Over 100,000 clinicians throughout the world use the therapy. Millions of people have been treated successfully over the past 33 years.
EMDR therapy is an eight-phase treatment. Eye movements (or other bilateral stimulation) are used during one part of the session. After the clinician has determined which memory to target first, he asks the client to hold different aspects of that event or thought in mind and to use his eyes to track the therapist’s hand as it moves back and forth across the client’s field of vision. As this happens, for reasons believed by a Harvard researcher to be connected with the biological mechanisms involved in Rapid Eye Movement (REM) sleep, internal associations arise and the clients begin to process the memory and disturbing feelings. In successful EMDR therapy, the meaning of painful events is transformed on an emotional level. For instance, a rape victim shifts from feeling horror and self-disgust to holding the firm belief that, “I survived it and I am strong. ” Unlike talk therapy, the insights clients gain in EMDR therapy result not so much from clinician interpretation, but from the client’s own accelerated intellectual and emotional processes. The net effect is that clients conclude EMDR therapy feeling empowered by the very experiences that once debased them. Their wounds have not just closed, they have transformed. As a natural outcome of the EMDR therapeutic process, the clients’ thoughts, feelings and behavior are all robust indicators of emotional health and resolution—all without speaking in detail or doing homework used in other therapies.
” Unlike talk therapy, the insights clients gain in EMDR therapy result not so much from clinician interpretation, but from the client’s own accelerated intellectual and emotional processes. The net effect is that clients conclude EMDR therapy feeling empowered by the very experiences that once debased them. Their wounds have not just closed, they have transformed. As a natural outcome of the EMDR therapeutic process, the clients’ thoughts, feelings and behavior are all robust indicators of emotional health and resolution—all without speaking in detail or doing homework used in other therapies.
TREATMENT DESCRIPTION
EMDR therapy combines different elements to maximize treatment effects. A full description of the theory, sequence of treatment, and research on protocols and active mechanisms can be found in F. Shapiro (2001) Eye movement desensitization and reprocessing: Basic principles, protocols and procedures (2nd edition) New York: Guilford Press.
EMDR therapy involves attention to three time periods: the past, present, and future. Focus is given to past disturbing memories and related events. Also, it is given to current situations that cause distress, and to developing the skills and attitudes needed for positive future actions. With EMDR therapy, these items are addressed using an eight-phase treatment approach.
Focus is given to past disturbing memories and related events. Also, it is given to current situations that cause distress, and to developing the skills and attitudes needed for positive future actions. With EMDR therapy, these items are addressed using an eight-phase treatment approach.
Phase 1: The first phase is a history-taking session(s). The therapist assesses the client’s readiness and develops a treatment plan. Client and therapist identify possible targets for EMDR processing. These include distressing memories and current situations that cause emotional distress. Other targets may include related incidents in the past. Emphasis is placed on the development of specific skills and behaviors that will be needed by the client in future situations.
Initial EMDR processing may be directed to childhood events rather than to adult onset stressors or the identified critical incident if the client had a problematic childhood. Clients generally gain insight on their situations, the emotional distress resolves and they start to change their behaviors. The length of treatment depends upon the number of traumas and the age of PTSD onset. Generally, those with single event adult onset trauma can be successfully treated in under 5 hours. Multiple trauma victims may require a longer treatment time.
The length of treatment depends upon the number of traumas and the age of PTSD onset. Generally, those with single event adult onset trauma can be successfully treated in under 5 hours. Multiple trauma victims may require a longer treatment time.
Phase 2: During the second phase of treatment, the therapist ensures that the client has several different ways of handling emotional distress. The therapist may teach the client a variety of imagery and stress reduction techniques the client can use during and between sessions. A goal of EMDR therapy is to produce rapid and effective change while the client maintains equilibrium during and between sessions.
Phases 3-6: In phases three to six, a target is identified and processed using EMDR therapy procedures. These involve the client identifying three things:
1. The vivid visual image related to the memory
2. A negative belief about self
3. Related emotions and body sensations.
In addition, the client identifies a positive belief. The therapist helps the client rate the positive belief as well as the intensity of the negative emotions. After this, the client is instructed to focus on the image, negative thought, and body sensations while simultaneously engaging in EMDR processing using sets of bilateral stimulation. These sets may include eye movements, taps, or tones. The type and length of these sets is different for each client. At this point, the EMDR client is instructed to just notice whatever spontaneously happens.
The therapist helps the client rate the positive belief as well as the intensity of the negative emotions. After this, the client is instructed to focus on the image, negative thought, and body sensations while simultaneously engaging in EMDR processing using sets of bilateral stimulation. These sets may include eye movements, taps, or tones. The type and length of these sets is different for each client. At this point, the EMDR client is instructed to just notice whatever spontaneously happens.
After each set of stimulation, the clinician instructs the client to let his/her mind go blank and to notice whatever thought, feeling, image, memory, or sensation comes to mind. Depending upon the client’s report, the clinician will choose the next focus of attention. These repeated sets with directed focused attention occur numerous times throughout the session. If the client becomes distressed or has difficulty in progressing, the therapist follows established procedures to help the client get back on track.
When the client reports no distress related to the targeted memory, (s)he is asked to think of the preferred positive belief that was identified at the beginning of the session. At this time, the client may adjust the positive belief if necessary, and then focus on it during the next set of distressing events.
Phase 7: In phase seven, closure, the therapist asks the client to keep a log during the week. The log should document any related material that may arise. It serves to remind the client of the self-calming activities that were mastered in phase two.
Phase 8: The next session begins with phase eight. Phase eight consists of examining the progress made thus far. The EMDR treatment processes all related historical events, current incidents that elicit distress, and future events that will require different responses
History of EMDR – EMDR Institute – EYE MOVEMENT DESENSITIZATION AND REPROCESSING THERAPY
Shapiro then conducted a case study4 and a controlled study1 to test the effectiveness of EMD. In the controlled study, she randomly assigned 22 individuals with traumatic memories to two conditions: half received EMD, and half received the same therapeutic procedure with imagery and detailed description replacing the eye movements. She reported that EMD resulted in significant decreases in ratings of subjective distress and significant increases in ratings of confidence in a positive belief. Participants in the EMD condition reported significantly larger changes than those in the imagery condition.
In the controlled study, she randomly assigned 22 individuals with traumatic memories to two conditions: half received EMD, and half received the same therapeutic procedure with imagery and detailed description replacing the eye movements. She reported that EMD resulted in significant decreases in ratings of subjective distress and significant increases in ratings of confidence in a positive belief. Participants in the EMD condition reported significantly larger changes than those in the imagery condition.
Shapiro wrote “a single session of the procedure was sufficient to desensitize subjects’ traumatic memories, as well as dramatically alter their cognitive assessments
6.” Unfortunately, Shapiro has often been erroneously cited as claiming that “EMDR can cure [posttraumatic stress disorder] PTSD in one session (F. Shapiro, 1989).”7 Shapiro never made this statement; what she actually wrote was that the EMD procedure "serves to desensitize the anxiety … not to eliminate all PTSD-related symptomatology and complications, nor to provide coping strategies for the victims8” and reported "an average treatment time of five sessions"8 to comprehensively treat PTSD.
1989 was the first year that controlled studies investigating the treatment of PTSD were published. Besides Shapiro’s article, three other studies9,10,11 were published. The Brom et al.9 study compared the results of psychodynamic therapy, hypnotherapy, and desensitization and provided an average of 16 sessions. It found clinically significant treatment effects for 60% of the civilian participants, with no differences between the conditions. The Cooper and Clum10 study compared flooding to standard care in a Veterans Administration Hospital. They reported moderate clinical effects after 6-14 sessions, with a 30% patient drop-out rate. The Keane et al.11 (1989) study compared flooding to a wait-list control for veteran participants and reported moderate clinical effects after 14-16 sessions. [See Comparison of EMDR and Cognitive Behavioral Therapies for more information.
Shapiro continued to develop this treatment approach, incorporating feedback from clients and other clinicians who were using EMD. In 1991 she changed the name to Eye Movement Desensitization and Reprocessing12 (EMDR) to reflect the insights and cognitive changes that occurred during treatment, and to identify the information processing theory that she developed to explain the treatment effects.
In 1991 she changed the name to Eye Movement Desensitization and Reprocessing12 (EMDR) to reflect the insights and cognitive changes that occurred during treatment, and to identify the information processing theory that she developed to explain the treatment effects.
Because EMDR therapy was an effective treatment, achieving results very quickly for many clients, Shapiro felt an ethical obligation to teach other clinicians so that individuals suffering from PTSD could find relief. However, EMDR was still experimental since it had not received independent confirmation through other controlled studies. She attempted to resolve this ethical dilemma by teaching EMDR only to licensed clinicians, and by ensuring that everyone who learned the approach was trained by the EMDR Institute in the same model. That way safeguards would be in place, clinicians would be taught to inform clients of its status, and a feedback system would allow everyone that was trained to get the most up to date information. In 1995, after other controlled studies had been published, the label “experimental” and the training restrictions were removed and a textbook of procedures was published13 . Shapiro has been severely criticized by some for her method of dissemination, because she initially restricted training and because she taught an experimental procedure. However, these critics ignore the APA ethics code mandated responsibilities of an innovator to determine training practices and the fact that even as late as 1998, there were no treatments for PTSD that were designated as well-established and empirically validated15. At that time, independent reviewers for the Clinical Psychology Division of the American Psychological Association identified three treatments with “probable efficacy.” These were EMDR, exposure therapy, and stress inoculation therapy.
In 1995, after other controlled studies had been published, the label “experimental” and the training restrictions were removed and a textbook of procedures was published13 . Shapiro has been severely criticized by some for her method of dissemination, because she initially restricted training and because she taught an experimental procedure. However, these critics ignore the APA ethics code mandated responsibilities of an innovator to determine training practices and the fact that even as late as 1998, there were no treatments for PTSD that were designated as well-established and empirically validated15. At that time, independent reviewers for the Clinical Psychology Division of the American Psychological Association identified three treatments with “probable efficacy.” These were EMDR, exposure therapy, and stress inoculation therapy.
Since the initial studies were published in 1989, hundreds of case studies have been published, and there have been numerous controlled outcome studies16 . These studies have demonstrated EMDR’s effectiveness in PTSD treatment and EMDR is now recognized as efficacious in the treatment of PTSD [See Efficacy of EMDR and Summary of PTSD Studies].
These studies have demonstrated EMDR’s effectiveness in PTSD treatment and EMDR is now recognized as efficacious in the treatment of PTSD [See Efficacy of EMDR and Summary of PTSD Studies].
A professional association, independent from Shapiro and the EMDR Institute was founded in 1995 to establish standards for training and practice. The EMDR International Association (EMDRIA) declares that its primary objective is “to establish, maintain and promote the highest standards of excellence and integrity in Eye Movement Desensitization and Reprocessing (EMDR) practice, research and education.” Information about EMDRIA is available at www.emdria.org
Despite its demonstrated effectiveness, similar to most new approaches in psychotherapy, EMDR has been surrounded by controversy. While some critics have labeled EMDR a “pseudoscience” others have commented that these conclusions are based on misinterpretations of the literature [see "Confusion, Misinformation, and Charges of "Pseudoscience"]. Another area of debate is the role of eye movements in EMDR [See Eye Movements and Alternate Dual Attention Stimuli and What has research determined about EMDR's eye movement component? In the Commonly Asked Questions section.
Another area of debate is the role of eye movements in EMDR [See Eye Movements and Alternate Dual Attention Stimuli and What has research determined about EMDR's eye movement component? In the Commonly Asked Questions section.
1Shapiro, F. (1989). Efficacy of the eye movement desensitization procedure in the treatment of traumatic memories. Journal of Traumatic Stress, 2, 199-223.
2Shapiro, F. & Forrest, M. (1997). EMDR The Breakthrough Therapy for Overcoming Anxiety, Stress and Trauma. New York: Basic Books
5Shapiro, F. (1989). Eye movement desensitization: A new treatment for post-traumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry, 20, 211-217.
6Shapiro, F. (1989). Efficacy of the eye movement desensitization procedure in the treatment of traumatic memories. Journal of Traumatic Stress, 2, 199-223
7Lohr, J. M., Tolin, D. F., & Lilienfeld, S. O. (1998). Efficacy of eye movement desensitization and reprocessing: Implications for behavior therapy. Behavior Therapy, 29, 123-156.
M., Tolin, D. F., & Lilienfeld, S. O. (1998). Efficacy of eye movement desensitization and reprocessing: Implications for behavior therapy. Behavior Therapy, 29, 123-156.
8Shapiro, F. (1989). Efficacy of the eye movement desensitizatioin procedure in the treatment of traumatic memories. Journal of Traumatic Stress, 2, 199-223.
9Brom, D., Kleber, R. J., & Defares, P. B. (1989). Brief psychotherapy for posttraumatic stress disorders. Journal of Consulting and Clinical Psychology, 57, 607-612
10Cooper, N.A., & Clum, G.A. (1989). Imaginal flooding as a supplementary treatment for PTSD in combat veterans: A controlled study. Behavior Therapy, 20, 381-391.
11Keane, T.M., Fairbank, J.A., Caddell, J.M., & Zimmering, R.T., (1989). Implosive (flooding) therapy reduces symptoms of PTSD in Vietnam combat veterans. Behavior Therapy, 20, 245-260.
Behavior Therapy, 20, 245-260.
12Shapiro, F., (1991). Eye movement desensitization & reprocessing procedure: From EMD to EMD/R-a new treatment model for anxiety and related traumata. Behavior Therapist, 14, 133-135.
13Shapiro, F. (1995). Eye Movement Desensitization and Reprocessing: Basic Principles, Protocols and Procedures (1st edition). New York: Guilford Press
15Chambless, D.L., Baker, M.J., Baucom, D.H., Beutler, L.E., Calhoun, K.S., Crits-Christoph, P., Daiuto, A., DeRubeis, R., Detweiler, J., Haaga, D.A.F., Bennett Johnson, S., McCurry, S., Mueser, K.T., Pope, K.S., Sanderson, W.C., Shoham, V., Stickle, T., Williams, D.A., & Woody, S.R. (1998) . Update on empirically validated therapies, II., The Clinical Psychologist, 51, 3-16.
16For complete listing see See Shapiro, F., (2001). Eye Movement Desensitization and Reprocessing: Basic Principles, Protocols and Procedures (2nd edition). New York: Guilford Press
New York: Guilford Press
EMDR THERAPY: A Review of Development and Mechanisms of Action
Udy Oren, Roger Solomon
This article presents the history and development of EMDR from the original discovery of Dr. Francine Shapiro in 1987 to current results, as well as future directions for research and clinical practice. . EMDR is an integral psychotherapy that considers dysfunctionally stored memories as a core element in the development of psychopathology.
Key words: psychotherapy method, EMDR, eye movement desensitization and processing, effective psychotherapy.
Eye Movement Densitization and Processing (EMDR) is a therapeutic approach based on the Adaptive Information Processing (API) model. From the point of view of this integrative psychotherapeutic approach, dysfunctionally stored memories are considered to be the primary basis of clinical pathology. Processing these memories and integrating them into larger adaptive networks of memories allows them to be transformed and the system to function again.
Over the past 25 years, enough clinical research has been conducted on EMDR therapy to lead to widespread acceptance of this approach as an effective treatment for psychic trauma. The history of therapy, the API model, clinical application and elements of the procedure itself are described in various literature (European EMDR Association: http://www.emdr-europe.org/), which also describes studies confirming two main theories explaining the mechanisms of action of bilateral stimulation (BLS) used during EMDR therapy.
EMDR is an integrative psychotherapeutic approach whose procedural elements fit well with most other types of psychotherapy (F. Shapiro, 2001, 2002). The therapy is based on the API model, which emphasizes the role of our brain's information processing system in the development of both healthy human functioning and pathology. Within the IPA model, insufficiently processed memories of uncomfortable or traumatic experiences are considered as the primary source of any psychopathology not caused by organic disorders.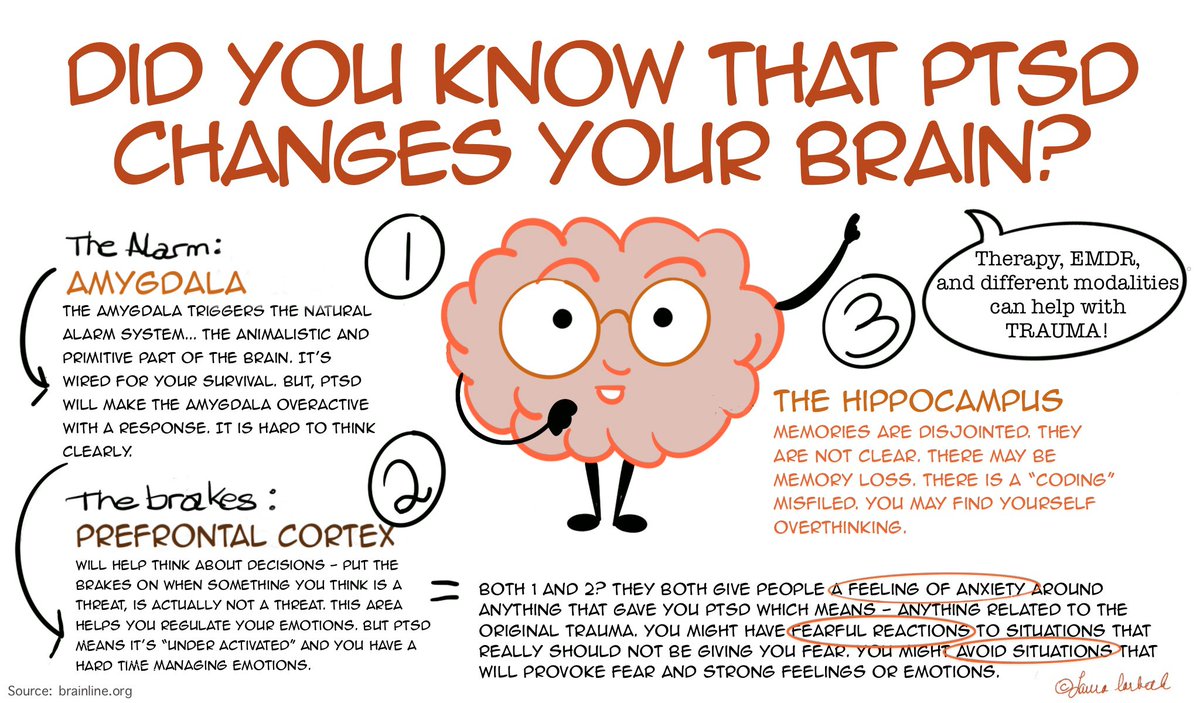 The processing of these memories leads to a resolution of the problem by rebuilding the system and assimilating the memory data into larger adaptive memory networks. EMDR is an 8-phase therapy that includes a three-part protocol focusing on:
The processing of these memories leads to a resolution of the problem by rebuilding the system and assimilating the memory data into larger adaptive memory networks. EMDR is an 8-phase therapy that includes a three-part protocol focusing on:
- memories behind current problems;
– situations in the present and triggers that need to be dealt with separately in order to bring the client into a stable state of psychological health;
- as well as the integration of positive memory scripts for more adaptive behavior in the future.
One of the distinguishing features of EMDR is the use of bilateral stimulation, in particular side-to-side eye movements, alternating knee tapping, or alternating auditory stimulation, using standardized procedures and protocols to work with all aspects of the target memory network.
History of occurrence.
The history of EMDR began in 1987 when F. Shapiro discovered the effects of eye movements on disturbing memories. Based on this, she developed a therapy protocol she called Eye Movement Desensitization (EMD). Since initially F. Shapiro adhered to behavioral views, she first decided that the effect of eye movements was similar to systematic desensitization, and decided that it was based on the body's natural relaxation reaction.
Based on this, she developed a therapy protocol she called Eye Movement Desensitization (EMD). Since initially F. Shapiro adhered to behavioral views, she first decided that the effect of eye movements was similar to systematic desensitization, and decided that it was based on the body's natural relaxation reaction.
She also suggested that the EMD process is related to the phenomenon of REM sleep and its effects on humans.
Shapiro's first studies were randomized clinical trials and showed promising results in the treatment of victims of sexual violence and war veterans (Shapiro, 1989).
Shapiro continued to develop and improve EMD procedures beyond the behavioral paradigm and in 1991 changed the name of the therapy to EMDR. The decision to add the word "processing" was due to the realization that desensitization is only one of the results of therapy, in fact, has a deeper effect, which can be better understood from the theory of information processing.
Early 1990s EMDR is experiencing a period of rapid growth and, at the same time, fierce discussions. The support of Joseph Wolpe, author of the method of systematic desensitization, as well as the publication of the results of several studies (Marquis, 1991; Wolpe & Abrams, 1991) led to the assertion that EMDR is a very promising form of psychotherapy. On the other hand, opponents of EMDR questioned the role of eye movements themselves (Lohr et al., 1992) and saw no scientific reason to add them to what they considered to be a type of exposure therapy (McNally, 1999). This criticism was recognized as erroneous (see review in Perkins & Rouanzoin, 2002), but the presence of opponents did not prevent F. Shapiro and her colleagues from continuing their work and conducting additional research. As empirical data was collected, EMDR therapy training programs began throughout the US, as well as in Europe, Australia, and Central and South America.
The support of Joseph Wolpe, author of the method of systematic desensitization, as well as the publication of the results of several studies (Marquis, 1991; Wolpe & Abrams, 1991) led to the assertion that EMDR is a very promising form of psychotherapy. On the other hand, opponents of EMDR questioned the role of eye movements themselves (Lohr et al., 1992) and saw no scientific reason to add them to what they considered to be a type of exposure therapy (McNally, 1999). This criticism was recognized as erroneous (see review in Perkins & Rouanzoin, 2002), but the presence of opponents did not prevent F. Shapiro and her colleagues from continuing their work and conducting additional research. As empirical data was collected, EMDR therapy training programs began throughout the US, as well as in Europe, Australia, and Central and South America.
The faculty of the EMDR Institute (www.emdr.com) have made a commitment from the very beginning to provide philanthropic education in hot spots and disaster areas around the world. At 1995 after the Oklahoma bombing, the EMDR community responded by creating the EMDR Humanitarian Assistance Program (EMDR-HAP).
At 1995 after the Oklahoma bombing, the EMDR community responded by creating the EMDR Humanitarian Assistance Program (EMDR-HAP).
The EMDR-HAP Program (www.emdrhap.org) and its affiliates around the world have continued to run hundreds of charity trainings in areas such as war-torn Bosnia, Nicaragua, Northern Ireland, Mexico City, post-quake Istanbul, Southeast Asia after the tsunami, in Israel, Palestine, Haiti after the earthquake, and at the request of many US government agencies.
Since 1995, when the first EMDR association (www.emdria.org) was founded in the USA, many other state and regional associations have appeared, including EMDR Asia (www.emdr-asia.org), EMDR Ibero-America (www.emdria.org). .emdriberoamerica.org), as well as the EMDR Europe Association (www.emdreurope.org), which has over 20 national associations and over 8,000 members (24,000 members in 2017. editor's note).
Due to the large amount of empirical research accumulated over the past 20 years, EMDR therapy is recognized as an effective therapy for trauma and is included in the clinical guidelines of many professional organizations and recommended by the ministries of health in different countries. In Europe, these include the Clinical Resource Efficiency Support Committee of the Department of Health Northern Ireland (CREST, 2003), the Guidance for the Delivery of Mental Health Services of the National Committee of the Netherlands (2003), the Study of the French State Institute of Medicine and Health (INSERM, 2004), UK Government Collaborating Center for Mental Health (NICE, 2005), Swedish Council for Technology Evaluation (2001), and UK Department of Health. In the United States, such organizations include the American Psychiatric Association (2004), the American Psychological Association (Chambles et al., 1998), State Institute of Mental Health (2007), and Department of Veterans Affairs and Department of Defense (2004). EMDR is also included in the recommendations of the International Traumatic Stress Society (ISTSS) (Foa, Keane & Friedman, 2009) (http://www.emdreurope.org/info.asp?CategoryID=15).
In Europe, these include the Clinical Resource Efficiency Support Committee of the Department of Health Northern Ireland (CREST, 2003), the Guidance for the Delivery of Mental Health Services of the National Committee of the Netherlands (2003), the Study of the French State Institute of Medicine and Health (INSERM, 2004), UK Government Collaborating Center for Mental Health (NICE, 2005), Swedish Council for Technology Evaluation (2001), and UK Department of Health. In the United States, such organizations include the American Psychiatric Association (2004), the American Psychological Association (Chambles et al., 1998), State Institute of Mental Health (2007), and Department of Veterans Affairs and Department of Defense (2004). EMDR is also included in the recommendations of the International Traumatic Stress Society (ISTSS) (Foa, Keane & Friedman, 2009) (http://www.emdreurope.org/info.asp?CategoryID=15).
Clinical studies.
Numerous practice guidelines and meta-analyses (Bisson & Andrew, 2007) show that EMDR has a therapeutic effect that is equal in strength and duration to that of the most extensively studied CBT techniques.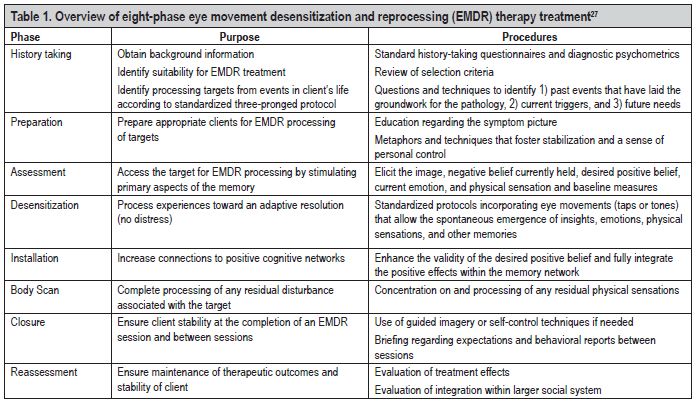 The results of about 20 controlled studies have confirmed the effectiveness of EMDR therapy: for the treatment of PTSD; in the treatment of a wide range of disorders, including phobias (de Jongh, Ten Broeke & Renssen, 1999; de Jongh, van den Oord & Ten Broeke, 2002), panic disorder (Goldstein et al., 2000; Fernandez & Faretta, 2007), generalized anxiety disorder (Gauvreau & Bouchard, 2008), problems with self-control and self-esteem (Soberman, Greenwald & Rule, 2002), complicated cases of mourning (Solomon & Rando, 2007), dysmorphia (Brown, McGoldrick & Buchanan, 1997), olfactory disorder syndrome (McGoldrick, Begum & Brown, 2008), sexual dysfunction (Wernik, 1993), pedophilia (Ricci et al., 2006), fear of failure (Barker & Barker, 2007), chronic pain (Grant & Threlfo, 2002), migraines (Marcus, 2008), and phantom pain in amputees (Schneider et al., 2008; Tinker & Wilson, 2006; de Roos, Veenstra et al., 2010). Most studies evaluate the effectiveness of EDMR with adults, however, there are several studies showing unusually positive results with children (Greenwald, 1998; Ahmad & SundelinWahlsten, 2008; Chemtob, Nakashima & Carlson, 2002; de Roos & de Jongh, 2008; Jaberghaderi, Greenwald, Rubin, Dolatabadim & Zand, 2004).
The results of about 20 controlled studies have confirmed the effectiveness of EMDR therapy: for the treatment of PTSD; in the treatment of a wide range of disorders, including phobias (de Jongh, Ten Broeke & Renssen, 1999; de Jongh, van den Oord & Ten Broeke, 2002), panic disorder (Goldstein et al., 2000; Fernandez & Faretta, 2007), generalized anxiety disorder (Gauvreau & Bouchard, 2008), problems with self-control and self-esteem (Soberman, Greenwald & Rule, 2002), complicated cases of mourning (Solomon & Rando, 2007), dysmorphia (Brown, McGoldrick & Buchanan, 1997), olfactory disorder syndrome (McGoldrick, Begum & Brown, 2008), sexual dysfunction (Wernik, 1993), pedophilia (Ricci et al., 2006), fear of failure (Barker & Barker, 2007), chronic pain (Grant & Threlfo, 2002), migraines (Marcus, 2008), and phantom pain in amputees (Schneider et al., 2008; Tinker & Wilson, 2006; de Roos, Veenstra et al., 2010). Most studies evaluate the effectiveness of EDMR with adults, however, there are several studies showing unusually positive results with children (Greenwald, 1998; Ahmad & SundelinWahlsten, 2008; Chemtob, Nakashima & Carlson, 2002; de Roos & de Jongh, 2008; Jaberghaderi, Greenwald, Rubin, Dolatabadim & Zand, 2004).
When looking at the results of studies comparing the effectiveness of EMDR and cognitive behavioral therapy (CBT), it is important to remember that EMDR therapy does not require the 30 to 100 hours of homework that most forms of cognitive behavioral therapy do. However, with EMDR it is possible to achieve the same therapeutic effect with less psychological trauma to the client, as well as by working exclusively in sessions. As a result, the therapy is gentler, more tolerable by both clients and therapists (Arabia, Manca & Solomon, 2011), and is also able to produce positive results when sessions are carried out over several days in a row (Wesson & Gould, 2009).
One of the elements of EMDR, bilateral stimulation, has attracted the most attention from both clinicians and scientists. Several theories have been put forward to explain the action of BLS, but the mechanisms of action are still being studied. An early component analytic study assessing the role of eye movements produced conflicting results. However, critics have found a flaw in this study due to the use of an incorrectly selected patient group and insufficient duration of therapy (Chemtob, Tolin, van der Kolk & Pitman, 2000). On the other hand, specific physiological effects of eye movement during EMDR therapy sessions have been identified (Propper et al., 2007; Elofsson, von Scheele, Theorell & Sondergaard, 2008; Sack, Lempa, Steinmetz, Lamprecht & Hofmann, 2008; Wilson , Silver, Covi & Foster, 1996). Scientists believe that eye movements lead to an increase in parasympathetic activity and a decrease in psychophysiological arousal. Similar physiological results were obtained in a study where a patient experienced a decrease in pulse rate and galvanic skin reflex after one session of EMDR (Aubert-Khalfa, Roques & Blin, 2008).
However, critics have found a flaw in this study due to the use of an incorrectly selected patient group and insufficient duration of therapy (Chemtob, Tolin, van der Kolk & Pitman, 2000). On the other hand, specific physiological effects of eye movement during EMDR therapy sessions have been identified (Propper et al., 2007; Elofsson, von Scheele, Theorell & Sondergaard, 2008; Sack, Lempa, Steinmetz, Lamprecht & Hofmann, 2008; Wilson , Silver, Covi & Foster, 1996). Scientists believe that eye movements lead to an increase in parasympathetic activity and a decrease in psychophysiological arousal. Similar physiological results were obtained in a study where a patient experienced a decrease in pulse rate and galvanic skin reflex after one session of EMDR (Aubert-Khalfa, Roques & Blin, 2008).
Two theories enjoy the greatest support from scientists. One concerns the orienting reflex, which, in their opinion, is directly related to the processes that take place during REM sleep (Stickgold, 2002, 2008). This theory is also supported by those randomized studies in which it was found that eye movements improve the functioning of event memory (Christman, Garvey, Propper & Phaneuf, 2003), increase the flexibility of attention focus (Kuiken, Bears, Miall & Smith, 2002; Kuiken, Chudleigh & Racher, 2010) and enhance the ability to recognize true information (Parker & Dagnall, 2007; Parker, Relph & Dagnall, 2008; Parker, Buckley & Dagnall, 2009). The orienting reflex hypothesis has also been evaluated in studies showing decreased levels of arousal (MacCulloch & Feldman, 1996; Barrowcliff, Gray, MacCulloch, Freeman & MacCulloch, 2003; Barrowcliff, Gray, Freeman & MacCulloch, 2004; Schubert, Lee & Drummond, 2011).
This theory is also supported by those randomized studies in which it was found that eye movements improve the functioning of event memory (Christman, Garvey, Propper & Phaneuf, 2003), increase the flexibility of attention focus (Kuiken, Bears, Miall & Smith, 2002; Kuiken, Chudleigh & Racher, 2010) and enhance the ability to recognize true information (Parker & Dagnall, 2007; Parker, Relph & Dagnall, 2008; Parker, Buckley & Dagnall, 2009). The orienting reflex hypothesis has also been evaluated in studies showing decreased levels of arousal (MacCulloch & Feldman, 1996; Barrowcliff, Gray, MacCulloch, Freeman & MacCulloch, 2003; Barrowcliff, Gray, Freeman & MacCulloch, 2004; Schubert, Lee & Drummond, 2011).
The second dominant hypothesis is that eye movements and other forms of dual focus stimulation (such as tapping and auditory stimulation) disrupt the habitual functioning of short-term memory. Randomized trials of this theory show that eye movements reduce the saturation and/or emotional charge of memories and frightening images (Andrade, Kavanagh & Baddeley, 1997; Engelhard, van Uijen & van den Hout, 2010; Engelhard et al. , 2011; Gunter & Bodner, 2008; Kavanagh, Freese, Andrade & May, 2001; Maxfield, Melnyk & Hayman, 2008; Sharpley, Montgomery & Scalzo, 1996; van den Hout, Muris, Salemink & Kindt, 2001; van den Hout et al., 2011). At the moment, it is not known when exactly the change in saturation and emotional charge occurs - before or after the decrease in physiological arousal, whether these two phenomena are closely related or whether they represent independent elements of the process (Sack et al., 2007, 2008a, b).
, 2011; Gunter & Bodner, 2008; Kavanagh, Freese, Andrade & May, 2001; Maxfield, Melnyk & Hayman, 2008; Sharpley, Montgomery & Scalzo, 1996; van den Hout, Muris, Salemink & Kindt, 2001; van den Hout et al., 2011). At the moment, it is not known when exactly the change in saturation and emotional charge occurs - before or after the decrease in physiological arousal, whether these two phenomena are closely related or whether they represent independent elements of the process (Sack et al., 2007, 2008a, b).
Ten randomized trials support both hypotheses. Therefore, there is good reason to believe that both theories are correct and that both processes described contribute to the therapeutic effect of EMDR. All of these findings collectively tell us that while previous component analyzes have failed to confirm the importance of bilateral pacing for EMDR, there is little doubt that the next generation of component analyzes of diagnosed patients will add to our knowledge base—provided, of course, that they are done well.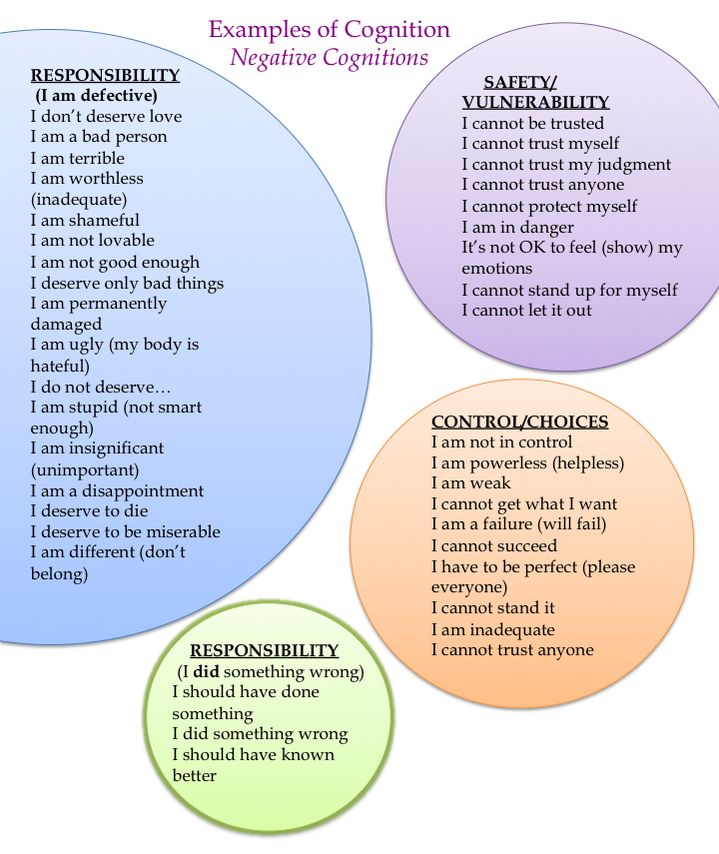 research work (F. Shapiro, 2001).
research work (F. Shapiro, 2001).
Model of adaptive information processing (API).
Behind the transformation of EMD into EMDR was primarily the API model, which is the theoretical basis for the entire clinical practice of EMDR (F. Shapiro, 1995, 2001). According to this model, networks of memories that store all previous experience are the basis for both human health and the emergence of pathology. New experience is an endless stream of conscious and unconscious elements of information that are processed by the brain with the help of an information processing system within these networks of memories. This system is inherently adaptive in that it is capable of using information to support human growth and development through learning when it functions normally. Relevant sensory, cognitive, emotional and somatic information is stored in memory networks, which in the future will be used to enable a person to adaptively respond to the world around him.
Apparently, some stressful negative events lead to an overload of the information processing system, as a result of which they cannot be assimilated adaptively. Such an event is stored in memory along with disturbing emotions, physical sensations and fears experienced at the time of the event. These situations can sometimes represent serious traumas, but more often they are everyday negative events that happen to people at home, in relationships, at school, at work, and so on, such as humiliation, rejection, and failure. In such situations, information regarding the negative event is stored in isolation from adaptive memory networks. Current situations in the present may trigger earlier memories, whereby the individual may experience some or all of the sensory, cognitive, emotional, and somatic aspects of events, resulting in maladaptive or symptomatic behavior.
Such an event is stored in memory along with disturbing emotions, physical sensations and fears experienced at the time of the event. These situations can sometimes represent serious traumas, but more often they are everyday negative events that happen to people at home, in relationships, at school, at work, and so on, such as humiliation, rejection, and failure. In such situations, information regarding the negative event is stored in isolation from adaptive memory networks. Current situations in the present may trigger earlier memories, whereby the individual may experience some or all of the sensory, cognitive, emotional, and somatic aspects of events, resulting in maladaptive or symptomatic behavior.
The API model considers negative beliefs, behaviors, and personality traits as a consequence of dysfunctionally stored memories (F. Shapiro, 2001). From this point of view, any negative self-belief (e.g., "I'm stupid"), any negative emotional reaction (e.g., fear in the presence of an authority figure), any negative somatic reaction (e. g., abdominal pain before an exam) are symptoms rather than the cause of current problems. The reason is considered to be memories of unprocessed events from the patient's life that are activated in the present. This view of psychological pathology is the main theoretical basis of EMDR therapy and helps the clinician understand the client, formulate a treatment plan, and select appropriate therapeutic interventions.
g., abdominal pain before an exam) are symptoms rather than the cause of current problems. The reason is considered to be memories of unprocessed events from the patient's life that are activated in the present. This view of psychological pathology is the main theoretical basis of EMDR therapy and helps the clinician understand the client, formulate a treatment plan, and select appropriate therapeutic interventions.
During an EMDR session, standardized procedures and protocols are used to access the memory associated with the current difficulty, which also uses brief bilateral stimulation (eye movements, tactile and auditory stimulation). Recordings of sessions (F. Shapiro, 2001, 2002; Shapiro & Forrest, 1997) show that processing mainly occurs due to the rapid establishment of intrapsychic connections between emotions, insights, sensations and memories that arise during the session, which change after each next set of bilateral stimulation. According to the API model, this process is seen as establishing a connection between the target memory and adaptive information, which allows the client to move forward, passing through the necessary stages of affect and awareness related to topics such as (1) the right degree of responsibility, (2) safety in present moment, and (3) the possibility of making choices in the future.
EMDR processing is understood as an inducement to the emergence of new associations and connections, which makes further learning possible and leads to the preservation of memories in a new, adaptive form. Once this has happened, the client can look at the disturbing event and at himself from a new, adaptive perspective. This new point of view does not carry the negative cognitions, affect and somatic sensations that were previously at the center of his maladaptive perception of this event. Consequently, the event ceases to have a negative impact on the client's personality, his worldview, as well as his emotional and somatic experience. This reworking, leading to new learning, is a central element of the EMDR model and therapy. The three-part protocol used in EMDR therapy works and recycles the positive experiences and new information/education needed to overcome any lack of knowledge or skills.
8-phase therapeutic approach.
EMDR Integrative Psychotherapy uses an 8-phase protocol to guide the therapist in dealing with current psychological difficulties stemming from past negative events.![]()
Phase 1 - History taking. The therapist collects general psychological data, focusing on current strengths and difficulties, past events that are related to current problems, present situations that cause problems, and positive goals for the future.
Phase 2 - Preparation. The therapist prepares the client for reprocessing by establishing a therapeutic alliance, providing psychological preparation for the client's difficulties, as well as explaining the EMDR process, and teaching the client specific types of relaxation techniques to help the client maintain a "dual focus" during a series of reprocessing sessions.
Phase 3 – Evaluation. The therapist will help the client clarify the details of the target memory, including the central picture, current negative cognition, desired positive cognition, current emotions and physical sensations, and some basic scale measurements.
Phase 4 - Desensitization. The therapist follows the client in guiding the processing of a disturbing memory from a past or current target event. At a later stage, positive scenarios for future behavior are also processed. Processing includes changes in sensory, cognitive, emotional and somatic information. The purpose of this phase is to reduce the anxiety associated with the memory to the lowest possible level and to promote personal growth through gaining insight and new perspectives, resulting in a new sense of self and worldview.
At a later stage, positive scenarios for future behavior are also processed. Processing includes changes in sensory, cognitive, emotional and somatic information. The purpose of this phase is to reduce the anxiety associated with the memory to the lowest possible level and to promote personal growth through gaining insight and new perspectives, resulting in a new sense of self and worldview.
Phase 5 - Installation. The therapist helps the client identify the currently desired positive self-belief about the processed memory and reinforces it, facilitating the integration of the memory into adaptive memory networks.
Phase 6 - Body scan. The therapist helps the client to discover and process any residual somatic sensations, striving for a complete somatic resolution.
Phase 7 - Completion. The therapist gives the client feedback about the session and what to expect after the session is over. The client is asked to keep brief notes of psychological reactions between sessions. If necessary, the therapist may use relaxation techniques to help the client stabilize before the session ends.
If necessary, the therapist may use relaxation techniques to help the client stabilize before the session ends.
Phase 8 - Reassessment. The therapist evaluates the client at the start of the next session, paying special attention to the effect of the therapy and assessing what has happened between sessions. This step also includes a re-evaluation of the previously redesigned target to assess the persistence of the therapy effect, as well as to identify other aspects that potentially need further processing. The therapist uses this information to determine the next step(s) in the course of therapy.
Three-part protocol (past, present, future).
Upon completion of therapy planning (Phase 1) and preparation and stabilization (Phase 3), EMDR therapy includes a three-part protocol that addresses past, present, and future relevant memories/scripts. In this approach, the therapist helps the client identify the details of each memory/script (phase 3) and process it (phases 4, 5, 6). Based on the API model, the client is first asked to process past experiences (both earlier and more recent) related to current difficulties. Reprocessing then focuses on current situations that are causing maladaptive responses in the present (including negative thoughts, emotions, feelings, and behaviors). Once memories from the past and present have been processed, the client is asked to imagine adaptive behaviors that will be used as a memory script for the future. This is done in relation to each of the previously identified situations in the present that cause dysfunctional reactions. Then the scenarios, which include cognitive, somatic and behavioral information, are processed, which contributes to their integration into the adaptive network of memories. The client may then be asked to face a particular problematic situation and then provide the therapist with feedback that will help him decide whether to continue therapy.
Based on the API model, the client is first asked to process past experiences (both earlier and more recent) related to current difficulties. Reprocessing then focuses on current situations that are causing maladaptive responses in the present (including negative thoughts, emotions, feelings, and behaviors). Once memories from the past and present have been processed, the client is asked to imagine adaptive behaviors that will be used as a memory script for the future. This is done in relation to each of the previously identified situations in the present that cause dysfunctional reactions. Then the scenarios, which include cognitive, somatic and behavioral information, are processed, which contributes to their integration into the adaptive network of memories. The client may then be asked to face a particular problematic situation and then provide the therapist with feedback that will help him decide whether to continue therapy.
Mechanisms of action.
As with any form of psychotherapy, the neurophysiological nature of the effects of EMDR is currently unknown, but several mechanisms of action may contribute to the therapeutic effect. Scientists propose a range of possible mechanisms of action that distinguish EMDR from traditional CBT practices. One of these mechanisms concerns "suppression" (extinction) and "recovery" (reconsolidation). EMDR therapy proposes, among other mechanisms of action, the assimilation of adaptive information found in other memory networks that come into contact with the network containing the previously isolated anxiety event (Solomon & Shapiro, 2008). After the successful completion of therapy, it is assumed that the memory is no longer isolated, as it appears to be properly integrated into the larger memory network. This idea is quite consistent with recent neurobiological theories about memory retrieval (Cahill & McGaugh, 1998; Suzuki et al., 2004) who suggest that once a memory is accessed, it can become labile and then re-stored in an altered form. The process of EMDR associated with the attachment of new associations to previously isolated memory networks can indeed activate the recovery process.
Scientists propose a range of possible mechanisms of action that distinguish EMDR from traditional CBT practices. One of these mechanisms concerns "suppression" (extinction) and "recovery" (reconsolidation). EMDR therapy proposes, among other mechanisms of action, the assimilation of adaptive information found in other memory networks that come into contact with the network containing the previously isolated anxiety event (Solomon & Shapiro, 2008). After the successful completion of therapy, it is assumed that the memory is no longer isolated, as it appears to be properly integrated into the larger memory network. This idea is quite consistent with recent neurobiological theories about memory retrieval (Cahill & McGaugh, 1998; Suzuki et al., 2004) who suggest that once a memory is accessed, it can become labile and then re-stored in an altered form. The process of EMDR associated with the attachment of new associations to previously isolated memory networks can indeed activate the recovery process.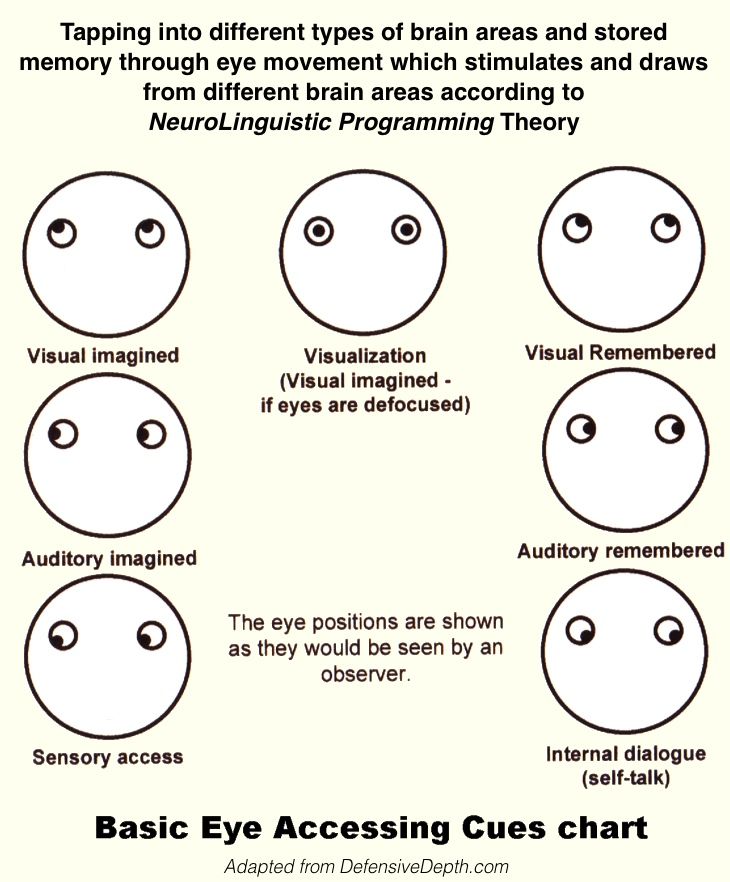 Therefore, EMDR may have different mechanisms of action than the main mechanism of action of various types of exposure therapy, namely "repression" (Craske, 1999; Lee, Taylor & Drummond, 2006; Rogers & Silver, 2002). It is believed that "restoration" changes the original memory, and "stopping", in turn, creates a new memory that begins to compete with the old one.
Therefore, EMDR may have different mechanisms of action than the main mechanism of action of various types of exposure therapy, namely "repression" (Craske, 1999; Lee, Taylor & Drummond, 2006; Rogers & Silver, 2002). It is believed that "restoration" changes the original memory, and "stopping", in turn, creates a new memory that begins to compete with the old one.
During the evaluation phase of EMDR therapy, there are also additional mechanisms that help bring together the various fragments of memory. When undergoing exposure therapy, the client is asked to describe the memory in the most detailed way, while in EMDR therapy there are no such requirements. Rather, during the appraisal phase, the therapist helps the client isolate the negative memory image, identify the current negative belief and desired positive belief, associated emotions, and bodily sensations. Experience that has not been reworked enough can be stored in fragments (van der Kolk & Fisler, 1995). Therefore, the systematization of memory components as an element of the procedure stimulates the process of processing.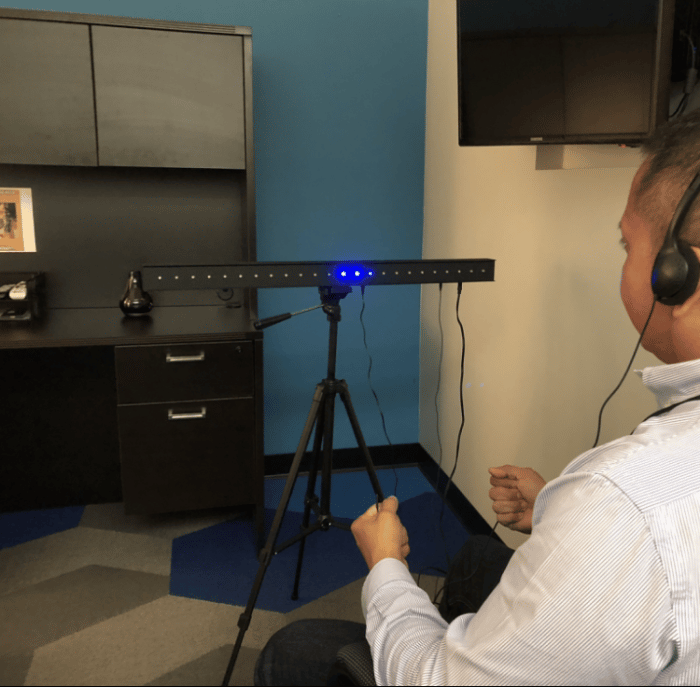 This procedure activates memory networks containing other aspects of the negative experience, potentially enabling the client to reconnect parts of the experience, make sense of it, and facilitate the process of retaining the memory in narrative memory.
This procedure activates memory networks containing other aspects of the negative experience, potentially enabling the client to reconnect parts of the experience, make sense of it, and facilitate the process of retaining the memory in narrative memory.
Cognitive restructuring is another element of the procedure that can explain the effectiveness of EMDR. However, in traditional types of cognitive therapy, it is customary to identify some irrational belief about oneself (negative cognition), and then deliberately question it, restructure and reframe this belief, turning it into an adaptive belief about oneself (positive cognition) (Beck, Rush, Shaw & Emery, 1979). The assessment phase in EMDR differs from cognitive restructuring methods in that there is no deliberate attempt by the therapist to change or reframe the client's current belief. It is assumed that the belief will change spontaneously in the process of subsequent processing. However, from the point of view of the API, the preliminary formation of an association between negative cognition and more adaptive information that contradicts negative experiences can contribute to further processing, since it activates the corresponding adaptive networks.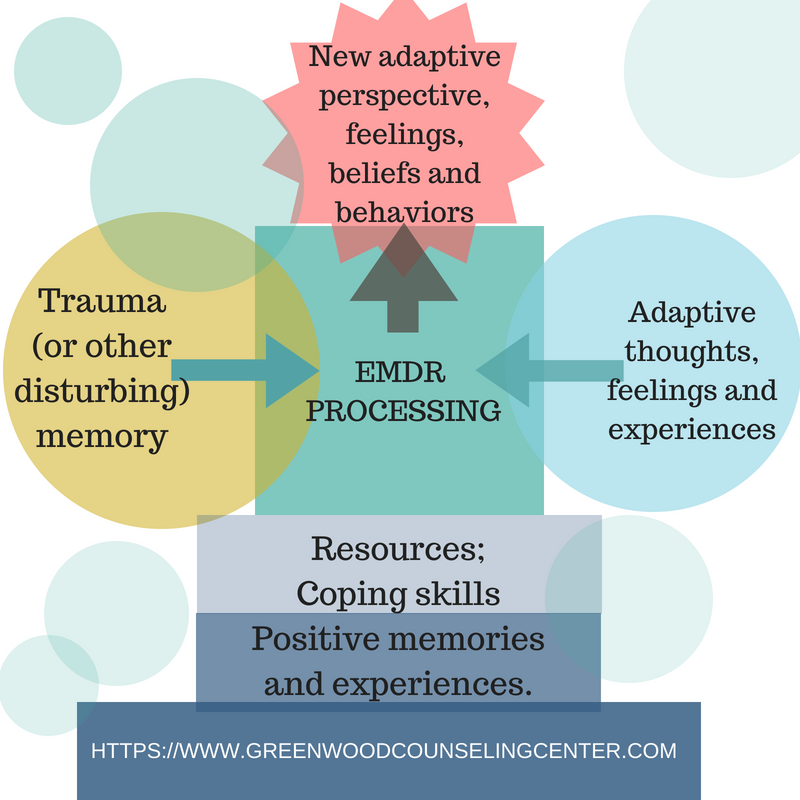
The desensitization and installation phases have different mechanisms of action. One of the possible mechanisms of action is awareness. During the desensitization phase of EMDR, clients are instructed to "let whatever happens" and "just pay attention" to whatever comes up (F. Shapiro, 1989, 1995, 2001). This is quite consistent with the principles of mindfulness practice (Siegel, 2007). Instructions like this reduce excessive demands on themselves and perhaps help clients to observe without judgment what they are feeling and thinking. Research confirms that the adoption of the paradigm that sees negative thoughts and feelings as transient mental phenomena rather than as aspects of the personality (Teasdale, 1997; Teasdale et al., 2002) has a beneficial therapeutic effect. However, while meditation techniques most often ask participants to return to their original focus of attention (Tzan-Fu, Ching-Kuan & Nien-Mu, 2004), in EMDR therapy clients are asked to simply "notice" various associations as they occur.
Perceived mastery may be another important procedural element that makes EMDR an effective therapy. Whereas exposure techniques require concentration and do not encourage distraction from the incident in order to prevent avoidance, EMDR therapy uses only momentary attention to the various associations that occur within the client during sets of eye movements. Therefore, during EMDR, clients may experience an increase in the sense of being able to switch between experiencing the event, paying attention to what is happening, and communicating the change to the therapist. The client's ability to use coping strategies more effectively can improve along with their ability to cope with stress, anxiety and depression in dangerous situations. (Bandura, 2004). From an API perspective, this sense of ability and efficiency is encoded in the brain as adaptive information available to connect with memory networks containing dysfunctionally stored information.
Finally, exposure therapy maintains a high level of anxiety by initially focusing on the disturbing event, as mentioned above, while the eye movements used in EMDR seem to increase parasympathetic arousal and reduce the intensity and emotionality of negative material, as well as to increase the flexibility of attention. It is possible that such effects allow information from other memory systems to connect to a target network that contains dysfunctionally stored information (Shapiro, 1995, 2001) leading to transformation and then retrieval of the memory (Cahill & McGaugh, 1998; Suzuki et al., 2004). Further clinical studies are required to explore these hypotheses and better understand the specific, side-effects, and interactive effects of different factors on EMDR performance.
It is possible that such effects allow information from other memory systems to connect to a target network that contains dysfunctionally stored information (Shapiro, 1995, 2001) leading to transformation and then retrieval of the memory (Cahill & McGaugh, 1998; Suzuki et al., 2004). Further clinical studies are required to explore these hypotheses and better understand the specific, side-effects, and interactive effects of different factors on EMDR performance.
Conclusions.
EMDR is one of the pioneering arts of psychotherapy. Primarily, this therapy is part of the evidence-based therapy group, which combines the clinical and scientific aspects of psychotherapy for decades after the establishment of recommendations for evidence-based treatments according to the Boulder Model (Fagan & Warden, 1996). Since the inception of EMDR, practitioners have always supported the development of clinical research, as evidenced by more than 30 randomized trials of trauma therapy. The API model forms the theoretical basis for EMDR, however, it is clear that the answers to the questions surrounding EMDR (and other therapies) lie in the human brain. As a result, more than ten studies have been devoted to the study of the neurobiological aspects of therapy, and their results indicate that psychotherapy and brain research should develop in tandem (Bossini, Fagiolini & Castrogiovanni, 2007; Pagani et al., 2007; Richardson et al. ., 2009).
As a result, more than ten studies have been devoted to the study of the neurobiological aspects of therapy, and their results indicate that psychotherapy and brain research should develop in tandem (Bossini, Fagiolini & Castrogiovanni, 2007; Pagani et al., 2007; Richardson et al. ., 2009).
EMDR is an integrative form of psychotherapy that includes elements that are compatible with a variety of approaches. The central place in therapy here is occupied by the body, however, the cognitive, emotional and behavioral aspects retain their importance. One of the most important advantages of EMDR is that it can also be used as a highly focused, short-term form of psychotherapy (in cases of single trauma: Shapiro, 1989; Jarero, Artigas & Luber, 2011; Kutz, Resnik & Dekel, 2008), and as a long-term, integrative, more widely applicable form of therapy (in cases of complex trauma, Korn, 2009). Along with positive psychology, EMDR is a form of humanistic therapy that believes in the client's inner resources and their ability to use those resources for personal growth. The working premise of EMDR is that the client heals himself with proper stimulation from the therapist, which leads to improved functioning of the internal information processing system (Shapiro, 1995, 2001). And finally, in all corners of the world, in dozens of countries, therapists of all cultures and professional orientations are successfully trained in EMDR. The very fact that EMDR has been successfully used in various cultures (Kim et al., 2010; Kavakcı, Kaptanog lu, Kug u & Dog an, 2010; Konuk et al., 2006; Uribe & Ramirez, 2006) indicates that EMDR makes a huge contribution to the development of the world of psychotherapy and to the well-being of mankind.
The working premise of EMDR is that the client heals himself with proper stimulation from the therapist, which leads to improved functioning of the internal information processing system (Shapiro, 1995, 2001). And finally, in all corners of the world, in dozens of countries, therapists of all cultures and professional orientations are successfully trained in EMDR. The very fact that EMDR has been successfully used in various cultures (Kim et al., 2010; Kavakcı, Kaptanog lu, Kug u & Dog an, 2010; Konuk et al., 2006; Uribe & Ramirez, 2006) indicates that EMDR makes a huge contribution to the development of the world of psychotherapy and to the well-being of mankind.
In summary, EMDR sees current problems as primarily related to dysfunctionally stored memories. There is direct work with past experience that has not been adequately processed and integrated into adaptive networks. EMDR is an evidence-based psychotherapeutic approach effective in trauma therapy. However, EMDR can be used to treat a wide range of disorders due to the fact that dysfunctionally stored memories are present in clients with all kinds of clinical diagnoses. (Mol et al., 2005; Obradovicˇı, Bush, Stamperdahl, Adler & Boyce, 2010). The EMDR integrative psychotherapeutic approach uses an eight-phase, three-stage (past, present, future) protocol that aims to free the client from the influence of experience that lays the foundation for the current pathology, as well as embedding a wide variety of elements of experience and memories into a common system in order to lead the client to a state of mental health.
(Mol et al., 2005; Obradovicˇı, Bush, Stamperdahl, Adler & Boyce, 2010). The EMDR integrative psychotherapeutic approach uses an eight-phase, three-stage (past, present, future) protocol that aims to free the client from the influence of experience that lays the foundation for the current pathology, as well as embedding a wide variety of elements of experience and memories into a common system in order to lead the client to a state of mental health.
Although the exact mechanisms behind these changes are unknown to us, a large number of randomized trials confirm that the eye movements used in EMDR correlate with the desensitization effect. Given the results of studies that show that eye movements per se lead to increased attentional flexibility and memory retrieval, it can be hypothesized that decreased arousal levels allow adaptive information from other memory networks to connect with the network that stores dysfunctionally stored information. This may lead to adaptive memory retrieval. However, as with other forms of psychotherapy, further brain research is needed to determine the exact biological basis for the therapeutic effect. Additional research is also needed to determine the neurobiological basis of eye movements and the interactive effects of various components of the EMDR therapy process. Given that homework is not used in EMDR therapy, daily therapy can easily validate the results of these studies, reducing the time frame that is usually required for other forms of therapy.
However, as with other forms of psychotherapy, further brain research is needed to determine the exact biological basis for the therapeutic effect. Additional research is also needed to determine the neurobiological basis of eye movements and the interactive effects of various components of the EMDR therapy process. Given that homework is not used in EMDR therapy, daily therapy can easily validate the results of these studies, reducing the time frame that is usually required for other forms of therapy.
Literature
1. Besser-Siegmund, K. EMDR in coaching / K. Besser-Siegmund, X Siegmund; per. with him N. Gust. - St. Petersburg: Werner Regen Publishing House, 2007. - 160 p.
2. Shapiro, F. Psychotherapy of emotional trauma using eye movements: basic principles, protocols and procedures /F. Shapiro; per. from English. A.S. Rigina - M .: Independent firm "Class" - 1998 - 496 p.
3. Perkins, B.R., & Rouanzoin, C.C. A critical evaluation of current views regarding eye movement desensitization and reprocessing (EMDR): Clarifying points of confusion. Journal of Clinical Psychology, 58 - 2002 - pp. 77–97.
Journal of Clinical Psychology, 58 - 2002 - pp. 77–97.
4. Shapiro, F. Eye movement desensitization and reprocessing: Basic principles, protocols and procedures (2nd ed.). New York: Guilford Press - 2001 - 450 p.
5. Shapiro, F. Paradigms, processing, and personality development. In F. Shapiro (Ed.), EMDR as an integrative psychotherapy approach: Experts of diverse orientations explore the paradigm prism. Washington, DC: American Psychological Association Books - 2002 - pp. 3–26
6. Shapiro, F. EMDR, Adaptive Information Processing, and Case Conceptualization / F. Shapiro // Journal of EMDR Practice and Research, Volume 1, Number 2 – 22007 – pp. 68-87
EMDR (Eye Movement Desensitization and Reprocessing)
August 26, 2022
What is EMDR
EMDR (Eye Movement Desensitization and Reprocessing) or EMDR (Eye Movement Desensitization and Reprocessing) is a short-term therapy that has been developed to treat post-traumatic disorders. This approach uses sensory information to help a person process traumatic experiences and emotional stress.
How EMDR works
Our brain has a natural way of recovering from traumatic memories and events. Eye movements activate the information processing mechanism in the nervous system. This can be seen, for example, in REM sleep ("rapid eye movement phase"). Being in this phase, we see dreams in which thoughts, emotions and events are processed.
When a traumatic event occurs to a person, the brain may not be able to fully process it. Therefore, the memory, as it were, "gets stuck" in the memory. A person feels constant anxiety, guilt and pain, sees nightmares, suffers from obsessive thoughts, and having met a “trigger”, he reacts as if he is re-experiencing this situation.
An EMDR therapist uses visual stimuli to artificially trigger the processing of traumatic memories, making them less vivid.
How an EMDR session works
In EMDR therapy, work is carried out according to protocols that the specialist selects based on the client's request. The preparatory phase is devoted to the collection of anamnesis, screening of the client and therapy planning. The specialist explains the principles of work, teaches relaxation techniques, and together with the client creates a “safe place”.
The specialist explains the principles of work, teaches relaxation techniques, and together with the client creates a “safe place”.
After that, the sessions of desensitization and reprocessing of memories begin directly. During the session, a person under the guidance of a specialist focuses on negative experiences, making eye movements from side to side.
To enhance the effect, the therapist may suggest that the client alternately tap himself on the left and right sides of the body (for example, on the knees or forearms), this is called bilateral (bilateral) stimulation. Holding dual attention allows the brain to process memories of the traumatic experience.
Is EMDR hypnosis
EMDR is not a form of hypnosis. The therapist guides the client, creates external stimuli, but you will always be awake and in control. You can stop the session at any time if you wish.
What problems does the method work with
EMDR is successfully used for the following problems:
- experiencing single traumatic events (accident, violence, death certificate, loss)
- PTSD and CPTSD
- childhood psychological trauma
- depression
- phobias
- anxiety disorders
- panic attacks
- eating disorders
- relationship problems
- obsessions
- avoidance behavior
What are the contraindications
EMDR is not applicable for:
- brain diseases
- epilepsy
- decrease in memory or intelligence
- psychotic states
How many appointments may be needed
EMDR refers to short-term therapy. To work with an active stressful experience, 3-7 sessions are needed. If the experience is in a chronic phase and lasts for many years, up to 10-12 sessions may be needed. However, a measurable reduction in anxiety and anxiety can be observed after the first EMDR session.
To work with an active stressful experience, 3-7 sessions are needed. If the experience is in a chronic phase and lasts for many years, up to 10-12 sessions may be needed. However, a measurable reduction in anxiety and anxiety can be observed after the first EMDR session.
Some customers require a lengthy EMDR preparation before it is possible to proceed directly to processing. To determine the possible duration of therapy, a preliminary assessment and psychodiagnostics are necessary.
## Scientific validity of the method EMDR is one of the few therapies that has been scientifically proven to be effective. The method was developed in 1987 by Francine Shapiro, a psychologist and researcher at the Institute for Psychical Research, (USA). While walking in the park after chemo, Frances noticed how her anxious thoughts left her after she moved her eyes quickly and actively. Through research into this phenomenon, it has been proven that eye movements alternately turn on the right and left hemispheres of the brain, thus allowing strong feelings to decrease down to neutral ones.