Early childhood developmental disorders
Learn about Hemophilia | CDC
Español | Other Languages
Hemophilia
- American Society of Hematology COVID-19 Resources
- National Hemophilia Foundation COVID-19 Vaccines and Bleeding Disorders Frequently Asked Questions
Español (Spanish) | Print
Hemophilia is usually an inherited bleeding disorder in which the blood does not clot properly. People with hemophilia can live full lives and enjoy most of the activities that other people do. If you have hemophilia, or know someone who does, it’s important to learn how to stay as healthy as possible.
What is Hemophilia?
Facts, symptoms, causes, diagnosis, and treatment.
Treatment
Hemophilia treatment centers and blood clotting factor.
Blood Safety
Safety of blood products.
Inhibitors
Diagnosis, treatment, and causes.
Materials & Multimedia
View and use free materials, social media graphics, and videos.
Real Stories
Read real stories about people living with hemophilia.
Research & Surveillance
Community Counts, inhibitor study, CHAMP, and other projects.
Data & Statistics
Data and statistics highlights.
Articles
Scientific articles and key findings.
Training & Education
Continuing education course for providers who are new to hemophilia.
About Us
What CDC is doing about hemophilia.
Plan ahead to help manage bleeding episodes and medical emergencies that occur while away from home.
People with Hemophilia
Women
Healthcare Providers
Partners
The purpose of this series is to provide evidence-based information on new research, interventions, emerging issues of interest in blood disorders, as well as innovative approaches in collaborations and partnerships. We invite you to join us in this series.
A national project to track and learn about hemophilia.
Last Reviewed: November 8, 2022
Source: National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention
CDC.gov Privacy Settings
We take your privacy seriously. You can review and change the way we collect information below.
Performance Cookies Checkbox
These cookies allow us to count visits and traffic sources so we can measure and improve the performance of our site. They help us to know which pages are the most and least popular and see how visitors move around the site. All information these cookies collect is aggregated and therefore anonymous. If you do not allow these cookies we will not know when you have visited our site, and will not be able to monitor its performance.
If you do not allow these cookies we will not know when you have visited our site, and will not be able to monitor its performance.
Functional Cookies Checkbox
Cookies used to make website functionality more relevant to you. These cookies perform functions like remembering presentation options or choices and, in some cases, delivery of web content that based on self-identified area of interests.
Campaign Cookies Checkbox
Cookies used to track the effectiveness of CDC public health campaigns through clickthrough data.
Social Media Cookies Checkbox
Cookies used to enable you to share pages and content that you find interesting on CDC. gov through third party social networking and other websites. These cookies may also be used for advertising purposes by these third parties.
gov through third party social networking and other websites. These cookies may also be used for advertising purposes by these third parties.
Remove all
Confirmed!
Thank you for taking the time to confirm your preferences. If you need to go back and make any changes, you can always do so by going to our Privacy Policy page.
Close
Childhood Developmental Disorders: Types and Symptoms
Our differences make us unique. For some children, individuality may include living with a developmental disorder.
Developmental disorders affect everyone differently. Your child might experience mild impairment, or they may need mechanical assistance during the day.
Living with a lifelong condition doesn’t mean quality of life is absent, however. Children can lead full, happy lives, even when faced with developmental challenges.
Developmental disorders, sometimes referred to as childhood disorders, are physical or brain-based conditions that affect a child’s progress as they grow and develop necessary life skills.
These disorders may impact areas such as:
- mobility
- biological function
- cognition (learning)
- physical or emotional independence
- language
- the five senses and perception
- social skills
Many childhood developmental disorders are present before birth and last throughout life. They may also occur as the result of injury, trauma, or other medical factors during childhood.
What’s the most common childhood developmental disorder?
Childhood developmental disorders can affect anyone of any race, gender, or national origin.
In the United States, approximately 17% of children between the ages of 3 and 17 live with at least one developmental disorder.
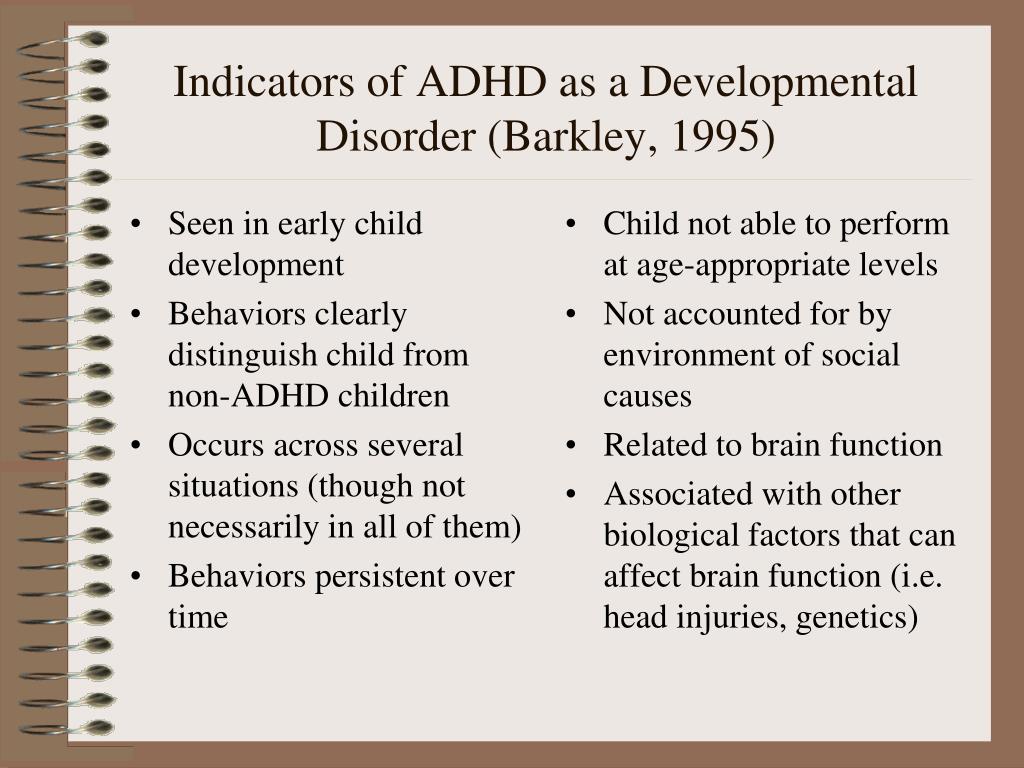
A 2019 review examining studies between 2009 and 2017 revealed that attention deficit hyperactivity disorder (ADHD) was the most commonly seen developmental disorder in children.
Any condition that impacts development in childhood and persists into adulthood may be classified as a childhood developmental disorder.
Not all developmental disorders impact a large number of children. Your child may live with a rare genetic trait or experience an injury that causes long-term, unique effects.
Common developmental disorders include:
- autism spectrum disorder
- learning disorders
- ADHD
- fetal alcohol spectrum disorders
- language disorders
- physical challenges
- other developmental delays
Autism spectrum disorder
While often lumped in under “learning disorders,” autism is a neurodevelopmental disorder and doesn’t always affect your child’s ability to learn.
Instead, behavior, communication, sensory, and social skills challenges may be the most noticeable signs.
While there may also be learning difficulties in some skill areas, many autistic children are gifted.
Learning disorders
There are three main types of learning disorders that can affect how well your child processes information.
These disorders can be present no matter what your child’s intelligence level is. Learning disorders have to do with academic weak spots, not smarts.
Learning disorders have to do with academic weak spots, not smarts.
Reversing letters while reading or difficulty distinguishing left from right could indicate a learning disorder.
Some children may also find math challenging or may have difficulty with writing skills.
Common learning disabilities include:
- dyslexia
- dysgraphia
- dyscalculia
ADHD
Like autism spectrum disorder, ADHD is often incorrectly considered a learning disorder.
Symptoms of ADHD can include hyperactivity and difficulty focusing on the task at hand. These could lead to challenges in a learning environment, but they aren’t a learning disability.
Fetal alcohol spectrum disorders
Fetal alcohol spectrum disorders result from a birthparent consuming alcohol during pregnancy.
Known as FASDs, these conditions may cause a number of side effects for the growing fetus and baby, including:
- low body weight
- non-typical facial features
- vision and hearing problems
- cognitive difficulties
- executive functioning challenges
Common types of FASDs include:
- fetal alcohol syndrome (FAS)
- alcohol-related birth defects (ARBD)
- alcohol-related neurodevelopment disorder (ARND)
- neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE)
Language disorders
If your child experiences challenges related to communication, a language disorder may be the cause.
Language disorders can include symptoms such as:
- stuttering or stammering
- not understanding words
- inability to express themselves
- difficulty speaking words or making sentences
- delayed ability to speak
Common language disorders include:
- auditory processing disorder
- aphasia
Intellectual disorders
Intellectual disorders aren’t the same as learning disorders.
Intellectual disorders are diagnosed when a child has lower capacity for reasoning, learning, and applying skills. This refers to “IQ”, or intelligence quotient.
Lower than average IQ can be reflected in daily functioning and is the primary trait of intellectual disorders.
Your child may experience an intellectual disorder as the result of a different, co-occurring developmental disorder, such as fetal alcohol syndrome.
Physical challenges
Childhood developmental disorders often present as physical challenges.
It may be something obvious, such as a physical difference that requires the use of a wheelchair, or it may be something less visible, such as a change in brain structure.
Common childhood developmental disorders with physical challenges include:
- cerebral palsy
- muscular dystrophy
- spina bifida
Other developmental delays
Not every delay is a disorder. Some children may take longer than others to develop certain skills or hit specific developmental milestones.
Your child may take an extra 3 months to start walking, for example, but this may never develop into something that impacts adult life.
In some cases, your child may present with a developmental disorder that can’t be clearly defined. This doesn’t mean what they’re experiencing isn’t real.
Your child may be living with a developmental disorder that shares traits with many other conditions and can’t be classified as a single diagnosis.
Developmental disorder vs.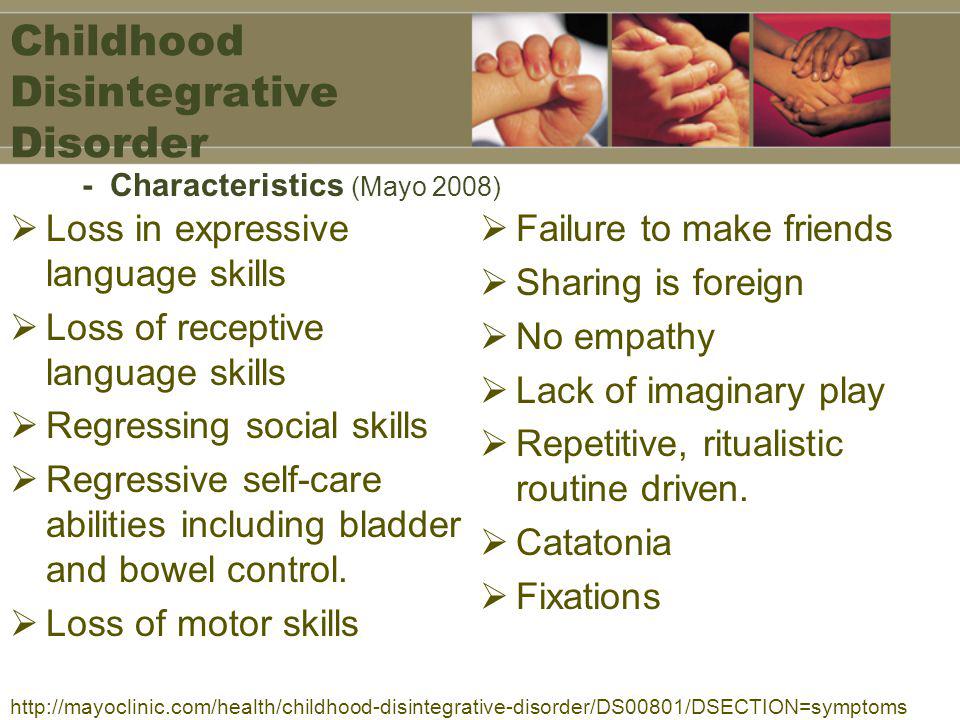 intellectual disability
intellectual disability
Intellectual disabilities are conditions that negatively impact a child’s IQ.
Developmental disorders, on the other hand, don’t necessarily have to do with intelligence.
While they can include intellectual disability, developmental disorders may also only affect behavior, mobility, or other aspects of a child’s development and growth.
The impact of a childhood developmental disorder on adulthood may depend on the type and severity of the condition and the area of development it impacts.
Some conditions, like anxiety or depression, can be treated and managed from childhood through adulthood.
Other conditions, such as those related to language, may be outgrown with the help of targeted therapy and repetition.
Genetic traits or physical challenges that result in a developmental disorder may require mechanical aids, such as prosthetics or mobility chairs.
Many children adapt to life with a developmental disorder. If it’s always been a part of their lives, they often learn early how to accomplish things in their own way. It’s also typical to see them develop additional skills in other areas that help them cope with their challenges.
If it’s always been a part of their lives, they often learn early how to accomplish things in their own way. It’s also typical to see them develop additional skills in other areas that help them cope with their challenges.
When they reach adulthood, new situations may test that ability to adapt.
Adults living with developmental disorders, like learning disabilities, may meet challenges related to:
- employment
- education
- relationships
- independence
Assistance and symptom management are available in all of these areas.
Legislation and community support programs can help adults with developmental disorders gain employment, maintain relationships, and find ways to be independent in daily life.
Many childhood developmental disorders are treatable and can be managed throughout adulthood.
Therapy, medication, and the use of daily assistance will all depend on the disorder and impact it has on daily functioning.
If you suspect your child may be showing signs of a developmental disorder, a health professional can help.
Early diagnosis and intervention can make a difference and help your little one continue a developmental trajectory.
Physical assessments and baseline child development models can let you know how your child’s progress compares to others in their age group.
In most cases, symptom management is possible and helpful.
Every child is unique and will develop at their own pace. However, in some cases, factors like genetics, biology, and injuries may get in the way of them reaching certain milestones.
Developmental disorders can result in specific challenges for a child. These can affect mobility, learning, social interaction, sensory input, and other aspects of growing up.
In most cases, professional intervention and home stimulation can help your child overcome or manage these symptoms.
Delayed physical development of the child symptoms, treatment in Zheleznodorozhny
03/22/2017
Mental retardation is understood as the tempo lag in the development of mental mechanisms, as well as the immaturity of the emotional and volitional activity of children, which can be overcome with the help of specialized training and education.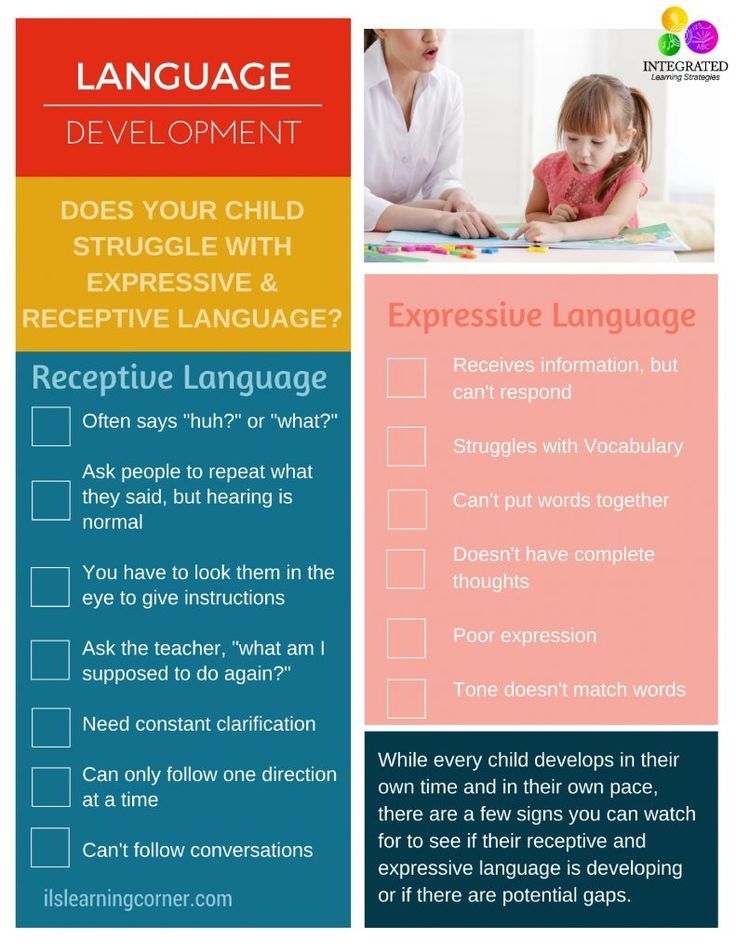 Children with mental retardation are characterized by: an insufficient degree of development of memory, motor skills, thinking, speech, attention, and self-control. In addition, there is a primitive and unstable emotions, poor school performance. Diagnosis of mental retardation must be carried out collegially by a commission, which includes, in addition to medical specialists, psychologists and teachers. Children with established mental retardation need, along with medical care, specially organized correctional and developmental education.
Children with mental retardation are characterized by: an insufficient degree of development of memory, motor skills, thinking, speech, attention, and self-control. In addition, there is a primitive and unstable emotions, poor school performance. Diagnosis of mental retardation must be carried out collegially by a commission, which includes, in addition to medical specialists, psychologists and teachers. Children with established mental retardation need, along with medical care, specially organized correctional and developmental education.
Mental retardation is a reversible violation of the emotional-volitional, as well as intellectual spheres, which are accompanied by certain difficulties in the learning process. About 15-16% of children have some degree of mental retardation. Mental retardation is most often attributed to psychological and pedagogical problems, but it can also be based on organic deviations, in particular neurological diseases. Various mental functions in children develop unevenly, so it is often impossible to diagnose children before they reach 4-5 years of age. In practice, the diagnosis is established mainly at school age.
In practice, the diagnosis is established mainly at school age.
Causes of mental retardation
At the heart of mental retardation may be socio-psychological or biological factors. Biological factors lead to a violation of the formation of various parts of the brain, which is accompanied by partial deviations in the mental maturation of the child. Factors affecting during pregnancy (fetal hypoxia, severe toxicosis, preeclampsia, Rh conflict, intrauterine infection, etc.), during childbirth and after the birth of a child (intracranial trauma, nuclear jaundice of newborns) can have an influence. In early childhood, mental retardation can be caused by severe somatic and infectious diseases, traumatic brain injuries.
Another group of causes includes environmental (social) factors. There is no organic brain damage. The reason can be both neglect on the part of parents, and excessive guardianship, social deprivation, authoritarian upbringing, lack of contact with adults and peers.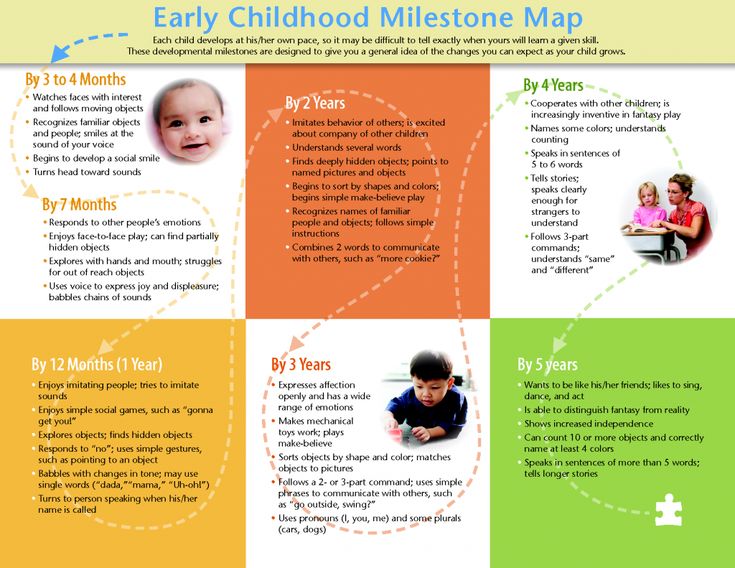
Mental retardation of secondary genesis is often caused by early impairment of vision and hearing, speech defects due to a pronounced lack of sensory information and communication.
Types of mental retardation
Thus, groups of children with mental retardation are heterogeneous. There are several classifications of mental retardation. Consider the etiopathogenetic classification that distinguishes 4 clinical types of mental retardation.
-
ZPR of constitutional genesis is caused by the slow maturation of the central nervous system. It is characterized by harmonious physical and mental infantilism. The behavior and anthropometric data of children do not correspond to age. They are emotionally labile, spontaneous, there is an inability to concentrate, lack of memory. At school age, such children are dominated by playing rather than learning interests.
-
ZPR of somatogenic origin is caused by long-term severe somatic diseases of children at an early age, which inevitably delay the maturation and formation of the central nervous system.
 In the anamnesis of children, chronic diseases of the respiratory system, gastrointestinal tract, cardiovascular system, kidneys, etc. are noted. As a rule, children are in hospitals for a long time, isolated from their peers. ZPR of somatogenic origin can manifest itself in the form of asthenic syndrome, low performance of children, memory loss, superficial attention, hyperactivity or lethargy in case of overwork.
In the anamnesis of children, chronic diseases of the respiratory system, gastrointestinal tract, cardiovascular system, kidneys, etc. are noted. As a rule, children are in hospitals for a long time, isolated from their peers. ZPR of somatogenic origin can manifest itself in the form of asthenic syndrome, low performance of children, memory loss, superficial attention, hyperactivity or lethargy in case of overwork. -
ZPR of psychogenic origin is caused by negative social conditions in which the child is forced to be (neglect, abuse, overprotection). Due to the lack of attention, the child may develop mental instability, intellectual lag, impulsivity. With excessive guardianship, lack of will, lack of initiative, lack of purposefulness, and egocentrism are formed.
-
ZPR of cerebral-organic origin is quite common. It may be due to non-rough organic damage to the brain. Perhaps the defeat of one area or a mosaic lesion of several areas of the brain, violating one or more mental functions.
 The mental retardation of cerebral-organic genesis can be characterized as the lack of formation of the emotional-volitional side and cognitive work: there is no brightness and liveliness of emotions, pronounced suggestibility, poverty of imagination, motor disinhibition, etc.
The mental retardation of cerebral-organic genesis can be characterized as the lack of formation of the emotional-volitional side and cognitive work: there is no brightness and liveliness of emotions, pronounced suggestibility, poverty of imagination, motor disinhibition, etc.
Distinctive features of children with mental retardation
Intellectual disorders in children with mental retardation are characterized by a mild character, but can affect all aspects of intellectual activity: speech, perception, thinking, memory, attention.
A child with mental retardation has a fragmented, inaccurate, slow perception. Some analyzers function fully, but the child has difficulty creating holistic images of the environment. Visual perception is the most developed, auditory - less, in this regard, when explaining academic disciplines to children with mental retardation, it is necessary to use visual materials.
Children with mental retardation have unstable, superficial, short-term attention. The child is distracted and switches attention under the influence of any extraneous stimuli. Situations that are associated with concentration, concentration of attention on something, can cause difficulties. With overwork and increased stress, it is possible to detect signs of hyperactivity syndrome, as well as attention deficit.
The child is distracted and switches attention under the influence of any extraneous stimuli. Situations that are associated with concentration, concentration of attention on something, can cause difficulties. With overwork and increased stress, it is possible to detect signs of hyperactivity syndrome, as well as attention deficit.
Memory is characterized by a mosaic of information memorization, weak selectivity. Visual-figurative memory prevails over verbal. Low mental activity in the process of information reproduction is characteristic. Children with mental retardation have more intact visual-effective thinking; figurative thinking is subjected to greater disturbance due to inaccurate perception. Abstract-logical thinking cannot be achieved without the help of adults. Children with mental retardation are characterized by difficulties with synthesis and analysis, comparison, generalization; they are not able to order events, draw conclusions, formulate conclusions. In addition, children with mental retardation have distorted articulation of most sounds, damage to auditory differentiation, and a sharp limitation in vocabulary.
Diagnostics
To diagnose mental retardation, a comprehensive examination of the child is carried out by a special commission, which includes a child psychologist, speech therapist, child neurologist, defectologist, psychiatrist, pediatrician and, if necessary, other specialists. Collection and study of anamnesis, diagnostic examination of speech, study of living conditions, neuropsychological testing, analysis of medical data are carried out. A conversation is necessarily held with the child, intellectual processes and emotional-volitional qualities are examined.
When an organic pathology is detected, an examination by medical specialists, first of all, a pediatric neurologist and a pediatrician, is necessary. With instrumental diagnostics, instrumental diagnostics can be performed - EEG, MRI of the brain. Differential diagnosis of mental retardation is carried out with autism and oligophrenia.
Correction
To work with children suffering from mental retardation, a multidisciplinary approach is needed, the active participation of child psychologists, neurologists, pediatricians, speech therapists, psychiatrists, defectologists. Correction of mental retardation should begin as early as possible, preferably in the preschool period.
Correction of mental retardation should begin as early as possible, preferably in the preschool period.
Often children need to visit specialized preschool and educational institutions or special groups and correctional classes. It is necessary to dose educational material, rely on clarity, frequent repetition of material, regular change of activities. It is important to pay attention to the development of various cognitive skills (thinking, attention, perception, memory), motor, sensory and emotional spheres, using play therapy, children's art therapy for this. Correction of violations of the speech apparatus is carried out by a speech therapist.
When somatic diseases and organic brain damage are detected, massage, physiotherapy, hydrotherapy, exercise therapy.
Prophylaxis
Children with mental retardation are able to catch up with their peers. They are trainable. With the correct organization of corrective work, a pronounced positive trend is observed in their development. Teachers help them learn new knowledge and skills. They can also, like their peers, enter universities and colleges.
Teachers help them learn new knowledge and skills. They can also, like their peers, enter universities and colleges.
To prevent mental retardation of a child, it is necessary to take great responsibility in planning pregnancy, avoid negative effects on the fetus, prevent somatic and infectious diseases in a child at an early age, and provide favorable living conditions for them. If a child lags behind in psychomotor development, an immediate examination and the beginning of corrective work are necessary.
Methods and techniques for correcting disorders in the development of self-image at an early age
Avdeeva N.N.
Violations in the development of self-image in early childhood can have various causes. First of all, these are violations of the interaction and communication of the child with a close adult. If the baby lacks an interested adult attitude addressed to him as a person, it will be necessary to organize special classes saturated with personality-oriented communication in order to enhance the child's experience of his significance for others, strengthen his positive self-perception, develop self-image.
Corrective classes are conducted by the teacher individually, with each of the children separately, as well as in a group. During individual lessons, emphasis is placed on the personal, subjective manifestations of the child. An adult supports the kid's initiatives, offers him a choice of activities, actions and evaluates the child's personal choice as significant, valuable for himself, emphasizing the child's right to free will.
During classes, an adult talks with a child about friends, a favorite toy, about what the baby saw on a walk, thereby showing personal interest in the life and experiences of the child, showing that the child’s experiences, what happens to him, the events of his life , personal experience - all this is significant for an adult.
In addition to conversation, remedial activities include adult play with a child. Let's take a look at different options for corrective play.
Ball game. The lesson begins with the fact that the kid is invited to choose from a large basket with balls the ball that he likes best. After the child has chosen a certain ball, the adult praises him for his good choice: “What a beautiful ball you have chosen, well done,” and offers to play. For children of the second year of life, an easy task is offered: roll or throw the ball to each other. For children of the third year of life - roll the ball along a certain corridor of cubes or take turns throwing it into the basket.
After the child has chosen a certain ball, the adult praises him for his good choice: “What a beautiful ball you have chosen, well done,” and offers to play. For children of the second year of life, an easy task is offered: roll or throw the ball to each other. For children of the third year of life - roll the ball along a certain corridor of cubes or take turns throwing it into the basket.
As the child copes with the task, it should be made more difficult. For example, the corridor narrows, and the basket moves further and further away.
In the course of the game, the adult praises the child. Praise should refer not only to the specific actions of the child, but also to him as a person: “Well done, how clever you are. You definitely hit the basket." If necessary, the baby should be encouraged, providing him with emotional support. “Look, you are getting better and better,” the adult says with a smile, affectionately hugging the child. Solving more and more difficult tasks, the kid has the opportunity to independently evaluate his successes, his progress in fulfilling the tasks of an adult, which expands and enriches his experience, as well as knowledge about his achievements.
Pyramid. An adult and a child jointly assemble a pyramid. For younger children, you can use the pyramids in the form of "Rooster" or "Bunny", and for older children - "Castle Tower". During the game, the adult gradually attracts the baby to more and more active tasks until the child collects the pyramid completely on his own. At first, the adult himself collects the pyramid, and the kid only gives the rings. Then the adult starts and the child continues. For a while, they act alternately. And then they switch roles: the child acts mainly, and the adult gives the rings and helps with difficulties.
An adult comments on the child's actions, notes progress, progress in mastering actions, compares the child with his level before the start of joint activities, when the child was not yet able to string rings on a pyramid.
Picture stories. Children are offered various pictures depicting objects, animals, seasons. An adult talks about what is shown in the picture in a form accessible to the child. Similarly, children's picture books with simple plots are used. From the story of an adult in the course of classes, a transition is gradually made to the reproduction of the story by a child. Encouraging the baby, asking leading questions, supporting his initiative, the adult more and more involves the child in retelling the plots and describing the pictures, remaining an attentive and interested listener. The child's story is accompanied by praise from an adult, addressed to the specific successes of the baby and the personality as a whole.
Similarly, children's picture books with simple plots are used. From the story of an adult in the course of classes, a transition is gradually made to the reproduction of the story by a child. Encouraging the baby, asking leading questions, supporting his initiative, the adult more and more involves the child in retelling the plots and describing the pictures, remaining an attentive and interested listener. The child's story is accompanied by praise from an adult, addressed to the specific successes of the baby and the personality as a whole.
For example, "What an interesting story you told about a cat about how she catches a mouse." "Well done! He showed all the pictures correctly, remembered all the animals that I told you about last time.
Modeling and drawing. Of course, these two activities are not yet fully available to a small child. However, young children love to sculpt from plasticine and draw with crayons and paints.
An adult asks young children to help him make a figure of a dog, a fox, a bear.
The kid enthusiastically sculpts paws, tail, ears. Older children can independently sculpt balls, balls, rings, etc. The situation unfolds into a game, when what the baby has molded becomes doll food, and the figures molded together are placed in a toy fairy forest or zoo.
Similarly, drawing takes place in the form of a joint activity of an adult and a child passing into play. Particular importance is attached to supporting the initiative of the baby, his activity, creativity. An adult notes the successes, originality and aesthetic qualities of the products of children's creativity, tries to open for the child an understanding of his new capabilities, the ability to independently create something new, interesting, meaningful in the eyes of other people.
Game. An adult organizes a child's game with peers. Traditional games are used: ball, "Mothers and Daughters", "Garage", building a house, etc.
children's attention to the actions of partners encourages the success of each child.
Walk. During a walk, an adult tells the children about the environment, gradually involving them in communication on cognitive and personally significant topics. An adult emphasizes his interest in the child's opinion, the significance of his point of view, his value as a communication partner. In the course of communication, encourages the child to tell about what he observes during a walk, about the events of his life. For example, about where the children were in the summer, who they visited, who visited them, where else they would go, etc. This ability to see oneself in a time perspective is an important point in the development of self-awareness, self-image. The benevolent attention of an adult, his interest in the past, present and future of the child, the encouragement of the ability to correlate events from the life of the baby with a time perspective contributes to the formation of the child's stable ideas about himself, the consolidation of his personality. For this purpose, it is useful to show the baby personal albums with photographs of the child, in which, by years, starting from infancy, the life and growing up of the baby was reflected.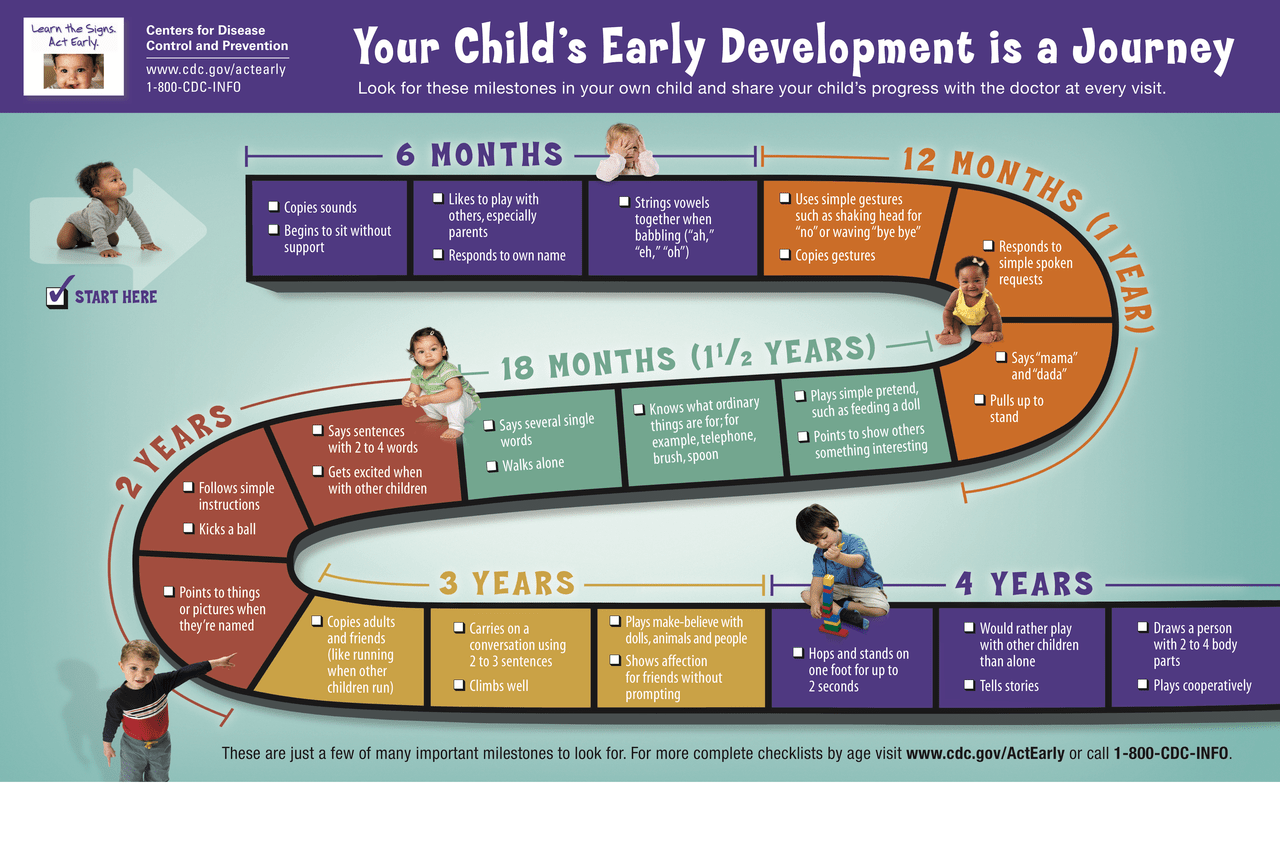
Features of interaction during remedial sessions
Remedial sessions between an adult and a child include some general, basic points of interaction. During classes, an adult treats children affectionately, with a smile, makes tactile contact, often takes the child in his arms. As before (as in infancy), eye contact is important. When communicating with a baby, an adult chooses a position “at eye level”, taking the child in his arms or sitting next to him. In an effort to establish a trusting relationship with the child, an adult pays attention to the mood of the baby, his desires, feelings, calms and encourages frustrated children, and helps in eliminating discomfort.
During a joint game or lesson, an adult addresses the child by name, often uses affectionate words. When teaching a child object actions, age and individual characteristics should be taken into account.
Education is done in a soft way, without violence. For example, when teaching a child to swaddle a doll, start a car, build a high tower of blocks, an adult gently guides his movements with his hand, and then provides an opportunity to perform the action on his own, helping if necessary, but not taking the initiative completely on himself.
The adult responds to any request of the child for joint activities or assistance, and if it is impossible to carry them out calmly, in a friendly tone, explains the reason and asks to wait.
An adult provides children with independence in the choice of toys, activities, partners in the game. If the kid does not want to join the game offered by the adult, does not join the lesson, the adult does not insist, does not blame the child. Children should be encouraged to express their thoughts, feelings, take into account their mood, emotional state.
Of course, all these principles of interaction between adults and children should apply not only to the time of classes with a child, but also to all other situations and moments of relationships and interactions, in particular, those related to the daily routine.
During various regime procedures, adults treat the child attentively, warmly, affectionately. When dressing after sleep and preparing for a walk, they do not forcibly stick the child’s arm into the sleeve, but the leg into tights, trying to dress the baby as soon as possible. An adult offers the child to get dressed, waits for the baby to take the initiative, for example, extends a hand to help him and support his initiative, carefully and affectionately dresses the child. In the third year of life, children are more willing to show independence and adults should encourage them in this.
An adult offers the child to get dressed, waits for the baby to take the initiative, for example, extends a hand to help him and support his initiative, carefully and affectionately dresses the child. In the third year of life, children are more willing to show independence and adults should encourage them in this.
When carrying out routine procedures, adults should take into account the individual characteristics of the child: temperament (they do not push the slow baby with persistence), preferences (they do not force them to eat porridge that is healthy, but not loved by the child), they do not forcefully put them to sleep, they are guided by the child's condition. Such behavior of adults ensures "taking the child into account", orientation to him as a subject in the system of child-adult relations.
Reward and reprimand
The second common point that should be highlighted in the relationship in the family and the preschool children's institution is encouragement and censure.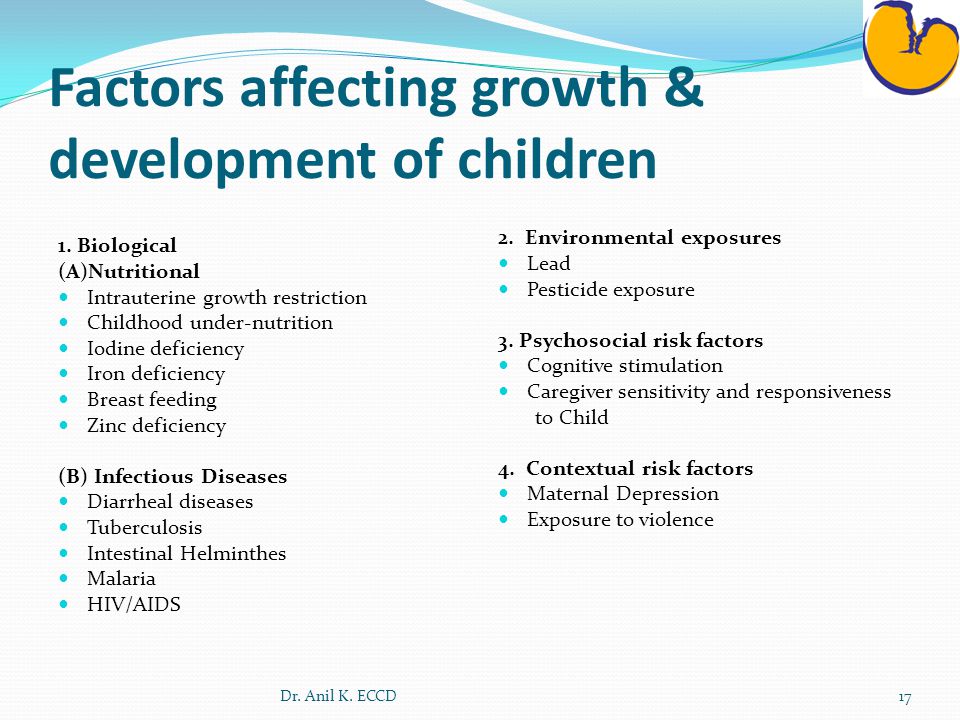 Just as in the first year of life, preference is given to encouragement and praise.
Just as in the first year of life, preference is given to encouragement and praise.
Adults should use the encouragement, support of the child much more often than censure and prohibition. Reprimand can only refer to the specific actions of the baby and never to the child as a person. The failures of the baby in any activity are not recorded specifically by adults, and on this basis no conclusion is made that degrades the dignity of the child. Failures and difficulties are, first of all, a signal to an adult about help, support, teaching a child, opening up new opportunities for him. If the baby himself is emotionally acutely experiencing his failure, you can try to beat the situation that caused him in a playful, humorous way, extinguishing negative emotions. Then the child should be helped to cope with the task, first with an adult, and then on his own, as a positive experience will strengthen his confidence in himself, his abilities, and his competence in interacting with the world.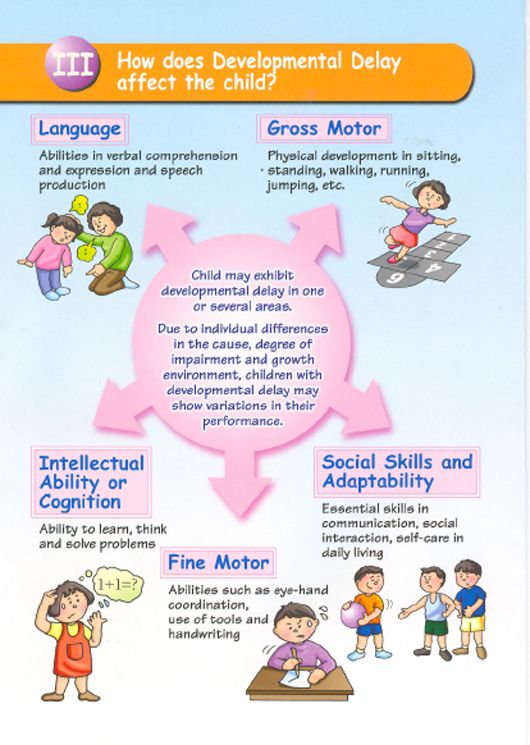
Adults never use physical punishment or other negative discipline that offends, frightens or humiliates a child. For example, when a baby refuses to eat, go to the toilet, go to bed, an adult tries to gently persuade him, translate unwanted actions into a playful form, and in case of failure, give the baby the opportunity to be alone.
In the case when a child expresses obvious disobedience, goes into open conflict, interferes with other children or an adult, offends someone, you should calmly explain why his behavior is undesirable, you can put him on a chair separately from other children or take him to the next room. At the same time, you can’t leave a child alone for a long time, deprive him of your love and attention. After resolving the conflict, the adult should gently hug the baby, tell him about his love for him, express confidence that the unwanted action will not be repeated. It is useful to discuss with the child the causes and consequences of his unwanted behavior, show ways to express their feelings and desires in a socially acceptable way.
Situational-personal communication
The source of a child's knowledge about himself is his individual experience and experience of communication and interaction with adults.
If in diagnostic tests with a mirror the child is not interested in his reflection, turns away from the mirror, shows negative emotions, an urgent correction of his communication with close adults is required, which, first of all, consists in establishing situational emotional-personal communication that is obviously defective in the first year of life .
In corrective work, one should, as it were, go back and repeat or re-build the leading activity and the corresponding form of communication of the previous age period. In communication and interaction with the child, one should activate the exchange of positive emotions, tactile contacts, the expression of love, tenderness, attitude towards the baby as a unique personality, its value for adults. Such behavior of adults will strengthen the positive self-awareness of the child, which was not sufficiently formed in the first year of life, his general positive self-esteem, the basis for the development of his self-image.
Distortions in the formation of the self-image in early childhood can also be caused by an overly long, protracted period of emotional and personal communication. At an early age, the main form of communication between a child and an adult should be practical cooperation, and actions with objects should be the leading activity.
If a child is alone in a family and there are a lot of adults around who “do not have a soul” in him, it often turns out that situational-personal, emotional communication predominates even in the second and third years of life. The kid is protected from independent actions, they strive to do everything for him, not allowing the slightest displeasure, failure of the child in anything.
This leads to the fact that the leading activity is not formed fully and in a timely manner, the child's ideas about his capabilities, abilities, skills do not develop, the development of the self-image is delayed.
Corrective work in case of "stuck" in emotional-personal communication should consist primarily in preparing the conditions for promoting objective actions to the first place in the mental development of the child. To do this, an adult, in the course of emotional, situational-personal communication, must switch the child’s attention from himself to an object: draw the child’s attention to a toy, book, household items, etc., interest the child, demonstrate the capabilities and features of the object, show how it is possible to play, act and offer the child a joint game. At first, it is advisable to perform actions with objects together with the child, helping him to coordinate movements and perform actions correctly. Joint actions and simple games with objects should be cyclical, partners follow the order, the adult adjusts to the child, giving him the opportunity to be a leader. All independent actions of the baby must be supported and approved by an adult. The kid should be encouraged for taking the initiative in the game or inviting an adult to joint actions and practical cooperation (for example, make a bed with an adult, help wash the dishes, wipe the dust, water the flowers, etc.)
To do this, an adult, in the course of emotional, situational-personal communication, must switch the child’s attention from himself to an object: draw the child’s attention to a toy, book, household items, etc., interest the child, demonstrate the capabilities and features of the object, show how it is possible to play, act and offer the child a joint game. At first, it is advisable to perform actions with objects together with the child, helping him to coordinate movements and perform actions correctly. Joint actions and simple games with objects should be cyclical, partners follow the order, the adult adjusts to the child, giving him the opportunity to be a leader. All independent actions of the baby must be supported and approved by an adult. The kid should be encouraged for taking the initiative in the game or inviting an adult to joint actions and practical cooperation (for example, make a bed with an adult, help wash the dishes, wipe the dust, water the flowers, etc.)
Development of the child's idea of himself as an active agent, subject of activity from cubes, etc.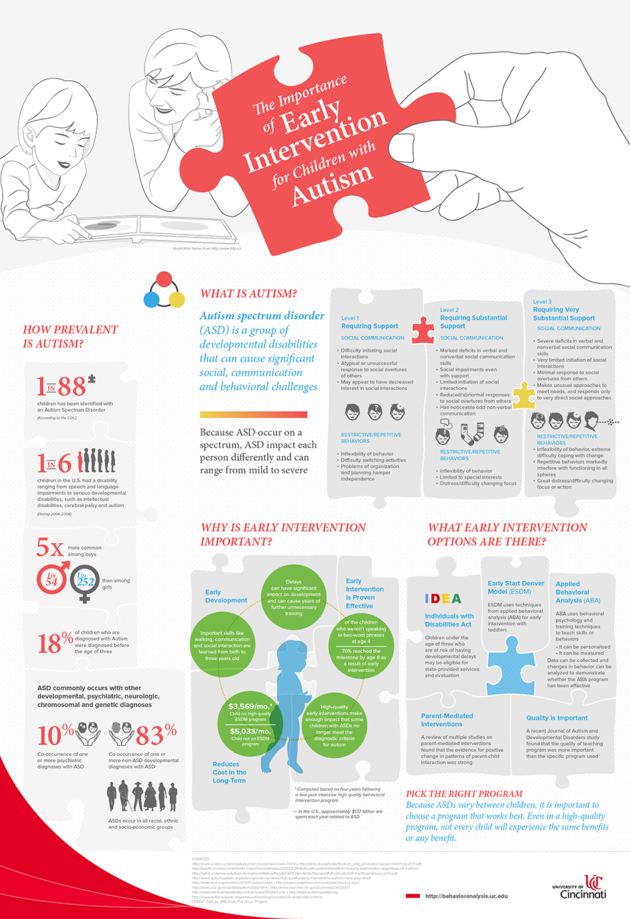 ), one should move on to mastering complex culturally, socially fixed ways of using objects. Here, an adult becomes a role model and the main connoisseur of the child's achievements. An adult demonstrates to the child the rules for handling household items, various actions with toys, simple story games, introduces children's books, teaches them to draw, sculpt, etc. All these actions of an adult allow you to expand the individual experience of the baby, try yourself in new actions, learn about your capabilities, abilities, achievements.
), one should move on to mastering complex culturally, socially fixed ways of using objects. Here, an adult becomes a role model and the main connoisseur of the child's achievements. An adult demonstrates to the child the rules for handling household items, various actions with toys, simple story games, introduces children's books, teaches them to draw, sculpt, etc. All these actions of an adult allow you to expand the individual experience of the baby, try yourself in new actions, learn about your capabilities, abilities, achievements.
Remaining the main connoisseur of a child's skills, an adult often expresses his approval to him, praises him for his achievements, and helps him with difficulties. An adult should provide the child with the opportunity to feel like an active principle, a subject of various actions, which will serve to form a new experience of experiencing confidence in the possibilities of mastering new things, competence in the world around him.
The child should be encouraged to imitate the actions of an adult. If the baby wants to wash the dishes, you can give him an unbreakable plate, a cup, put him on a chair in front of the sink, showing him how to wash dishes with a brush, sponge, praising and directing his actions. Adults should encourage the child's desire for self-service: give them the opportunity to dress themselves, wash themselves, fasten buttons or zippers, pull on mittens, etc.
If the baby wants to wash the dishes, you can give him an unbreakable plate, a cup, put him on a chair in front of the sink, showing him how to wash dishes with a brush, sponge, praising and directing his actions. Adults should encourage the child's desire for self-service: give them the opportunity to dress themselves, wash themselves, fasten buttons or zippers, pull on mittens, etc.
In order to develop a child's knowledge of himself, productive activities should be organized at an early age, such as drawing with a pencil, brush, hand, fingers, crayons, modeling from plasticine, clay, dough, appliqué, writing stories, fairy tales. Musical lessons are also necessary (singing, listening to records, playing musical instruments, dancing), which stimulate the expression of feelings, moods through facial expressions, gestures, movements, speech.
It is useful to support the child's desire for original problem solving, unusual use of objects, creative games and fantasies, writing poems and fairy tales, reproducing familiar stories in the game.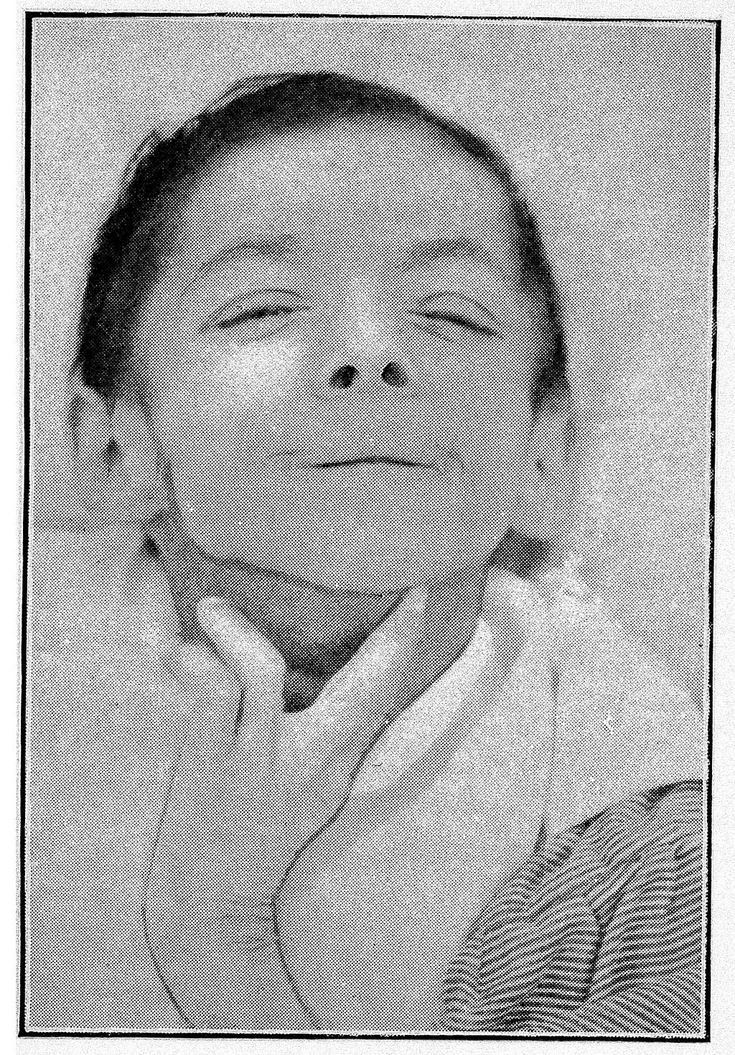
Participation in creative activities will contribute to the development of the child's idea of himself as a creative principle, not only imitating adults, but also generating something new, socially approved and meaningful for other people.
Specific self-assessment
When organizing the subject activity of the child and in the course of practical cooperation with him, conditions should be created for the identification and execution of a specific self-assessment. At an early age, against the background of a general positive self-esteem that has developed under the influence of emotional situational-personal communication between an adult and a child, a specific self-esteem gradually begins to take shape, relating to individual situations, actions, achievements of the baby, and not to his personality as a whole (as happens in the case overall self-esteem).
With the accumulation of individual experience, mastering new actions, as well as the assessment of an adult, the child develops an idea of his achievements, successes, specific skills and abilities. Since an adult is at first the main connoisseur of the achievements of the baby, how the formation of a specific self-esteem will largely depend on his behavior.
Since an adult is at first the main connoisseur of the achievements of the baby, how the formation of a specific self-esteem will largely depend on his behavior.
As we have already said, praise, permission, positive assessments should prevail over censure, prohibition, negative assessments addressed to the child. With properly organized adequate communication and interaction, the assessment of an adult plays an important role in the activity of the baby, guiding the child in relation to the results achieved. When evaluating the actions of the child, an adult, if necessary, can use negative assessments of individual, specific actions of the child, however, such an assessment must be accompanied by a positive assessment of the child as a person. For example, an adult says: "You put the picture of the blocks wrong, but I'm sure if you try, you will get it right, because you are very diligent and already know how to do a lot."
Praise for failure is not allowed. This negatively affects the formation of the child's self-esteem, distorts the criteria for success, and disorients the child. The assessment of an adult should be adequate to the achievements of the child, the result he has received. The assessment should be sufficiently detailed. So, evaluating the baby, the adult gives explanations that set the child the criteria for success and failure in each specific case. At the same time, the adult looks at how the child evaluates himself, doing it on his own, without waiting for the adult's assessment. With an adequate experience of cooperation with an adult and a developed objective activity, a baby in the third year of life does not strive only for a positive assessment of an adult, but independently, in accordance with an achievement or failure, experiences his own success in a specific action. This contributes to the formation of independence, self-control in the implementation of subject-practical activities.
The assessment of an adult should be adequate to the achievements of the child, the result he has received. The assessment should be sufficiently detailed. So, evaluating the baby, the adult gives explanations that set the child the criteria for success and failure in each specific case. At the same time, the adult looks at how the child evaluates himself, doing it on his own, without waiting for the adult's assessment. With an adequate experience of cooperation with an adult and a developed objective activity, a baby in the third year of life does not strive only for a positive assessment of an adult, but independently, in accordance with an achievement or failure, experiences his own success in a specific action. This contributes to the formation of independence, self-control in the implementation of subject-practical activities.
The formation of specific self-esteem ends at the next age stage, in preschool childhood, and does not detract from the value of general self-esteem. a positive attitude towards oneself as a person significant for other people.
a positive attitude towards oneself as a person significant for other people.
Communication with peers
Along with the development of individual experience and communication with adults in an age-appropriate form, communication and interaction of the child with peers should be specially highlighted as another factor in the formation of the self-image. Communication with peers contributes to the development of the baby's ideas about his physical qualities, physical capabilities, and in the third year of life contributes to the child's experience of himself as a creative principle, new opportunities, abilities that are significant for other people.
Without communication with peers, the formation of a child's self-image at an early age will not be complete and adequate. Therefore, adults should create conditions for the development of communication between the child and peers. To do this, first of all, it is necessary to form in children a positive attitude towards peers. By their own behavior, adults demonstrate a respectful attitude towards all children. They draw the attention of kids to each other's emotional states, encourage manifestations of sympathy, empathy for another child. They organize joint games for children, teaching them to coordinate their actions, take into account the desires of each other. Adults also strive to help children resolve emerging conflicts without violence, introduce the principle of priority, switch attention, and emphasize the merits of each child.
By their own behavior, adults demonstrate a respectful attitude towards all children. They draw the attention of kids to each other's emotional states, encourage manifestations of sympathy, empathy for another child. They organize joint games for children, teaching them to coordinate their actions, take into account the desires of each other. Adults also strive to help children resolve emerging conflicts without violence, introduce the principle of priority, switch attention, and emphasize the merits of each child.
You should never compare a child with peers when evaluating his skills, abilities, achievements. Adults, who often use the technique of comparing a baby with other children, thereby belittle and even humiliate either his dignity or the dignity of a peer. You can compare the achievements of the kid only with his own achievements, showing how he has progressed, what he already knows, what he still learns. In this way, adults create a perspective for the positive development of the child and strengthen the image of themselves as a developing whole.
The main lines of formation and correction of the image of oneself at an early age are: organization of communication with adults, peers, as well as promotion of subject-practical actions as the leading activity. When progress along all three lines has been established in correctional work, the following training situations should be included in interaction, communication with an adult.
Developing an idea of one's capabilities, abilities
Adults create conditions for the child to master complex movements, naming them, performing them first together with the child, and then the child independently at the request of an adult. For example, they organize outdoor games with various types of movements: walking, bouncing, squatting, jumping, running, etc. It is helpful to involve your baby in music activities that include simple dance moves.
The same types of movements are practiced in simple physical education classes. The child is taught to perform simple exercises and at the same time name what he is doing. The movements being learned can be repeated with dolls, in games with adults or other children, they can offer to perform a variety of actions. For example, the host shows some movement, calls it and all the participants in the game repeat the movement, the one who makes a mistake becomes the leader.
The movements being learned can be repeated with dolls, in games with adults or other children, they can offer to perform a variety of actions. For example, the host shows some movement, calls it and all the participants in the game repeat the movement, the one who makes a mistake becomes the leader.
From time to time a child is brought to a mirror to examine parts of the body, details of clothing that are usually not visible, correlating the reflection in the mirror with reality. There is no need to be afraid that a child who looks at himself with pleasure in a mirror, plays with his reflection, “flaunts” in new clothes, will grow up narcissistic and spoiled. Psychologically, there is no connection between selfishness and looking at oneself in a mirror at an early age.
But adults who do not like to look at themselves in the mirror, avoid their own reflection, often turn out to be insecure, have underestimated inadequate ideas about themselves, low self-esteem.
In addition to recognizing oneself as a child in a mirror, one should practice recognizing oneself and others in photographs. The kid is shown where mom, dad, grandmother (teacher, familiar adult), other children are, and then they are asked to do it on their own. It is especially interesting for a child to recognize himself in photographs at an early age, compare with the present moment, observe changes in his appearance, physical "I".
The kid is shown where mom, dad, grandmother (teacher, familiar adult), other children are, and then they are asked to do it on their own. It is especially interesting for a child to recognize himself in photographs at an early age, compare with the present moment, observe changes in his appearance, physical "I".
The child's developing sense of ownership should be taken into account. Understanding by the baby that he has his own place at the table, his own play area, his own bed, cup, clothes, etc. testify to the development of self-consciousness, ideas about oneself as the owner of certain things. This is not a manifestation of greed and selfishness, as such behavior of a child is sometimes interpreted by adults, but the development of his knowledge of himself. Therefore, one should respect the child's right to property and at the same time teach him to reckon with similar rights of other people.
Adults should encourage the child to show empathy for the emotional states of others. Praise the baby for trying to comfort a crying, upset person, tell me how best to do it (offer a toy to a crying baby, treat an upset sister with sweets, hug and kiss a tired grandmother, a close adult).
Praise the baby for trying to comfort a crying, upset person, tell me how best to do it (offer a toy to a crying baby, treat an upset sister with sweets, hug and kiss a tired grandmother, a close adult).
Similarly, a child develops the ability to share positive emotions with another person: joy, admiration, a sense of pleasure, etc.
Adults encourage the manifestation of different types of behavior in children in accordance with gender identity. As a rule, adults express more approval, more encourage behavior corresponding to the sex of the child. So, they praise girls when they play with dolls, help their mother with housework (washing clothes, cleaning the room, preparing dinner, etc.), express approval when boys play construction, garage, help grandmother carry a heavy bag, etc. .P. Sex stereotypes of behavior are enshrined in culture. For example, in fairy tales, heroines often have to be rescued from trouble, and male characters have to overcome obstacles and act as a savior. Reading fairy tales, watching cartoons, adults introduce children to different gender role behavior of characters. In everyday life, parents and educators also emphasize the difference between the behavior of boys and girls, gradually forming in children a value system accepted in society, the family, and the child's gender self-identity is formed.
Reading fairy tales, watching cartoons, adults introduce children to different gender role behavior of characters. In everyday life, parents and educators also emphasize the difference between the behavior of boys and girls, gradually forming in children a value system accepted in society, the family, and the child's gender self-identity is formed.
Adults should emphasize the individual differences between children: some boys like to play ball, while others like to build a city out of sand; one child thinks one thing is right, and the other another. Understanding one's difference from others, the right to this difference, as well as the recognition of similar rights of another person, is an important aspect of the development of the child's social "I", the foundations of tolerance, which are laid already in early childhood.
The crisis of the third year of life requires special attention. The behavior of the baby during this period is characterized by obstinacy, uncontrollability, self-will.