Does zoloft give you headaches
12 Zoloft Side Effects - SSRI Uses & Common Interactions To Know
Remember the original Zoloft commercial? The one where a sad little blob rolled around on screen with a rain cloud hovering over its head?
That commercial first debuted back in 2001, and since then Zoloft, or Sertraline hydrochloride, has become one of the top psychiatric drugs used by American adults, according to one recent study.
“Zoloft is one of the first-line antidepressant medications prescribed for both depression and anxiety, meaning it’s one of the most likely to work,” says Alison Hermann, MD, a clinical psychiatrist at Weill Cornell Medicine and New York-Presbyterian Hospital.
Zoloft is part of a class of drugs called SSRIs, or selective-serotonin reuptake inhibitors. “Their main effect has to do with changing the signaling of one of the main neurotransmitters in the brain, serotonin, which modulates mood,” explains James Murrough, MD, the director of the Mood and Anxiety Disorders Program at the Icahn School of Medicine at Mount Sinai.
“These medicines tend to increase the availability of serotonin in the brain, which can help boost your mood.”
And that’s the goal, right?
In general, antidepressants are well tolerated. But, like with all drugs, there are Zoloft side effects—some of which are merely annoying and some of which can actually be dangerous. “I generally start my patients on the lowest milligram pill and have them cut it in half for the few few doses just to make sure you’re tolerating it before bumping it up,” says Dr. Hermann.
So if you’re prescribed Zoloft, here’s what to look out for.
1
Changes in Weight or Appetite
People taking Zoloft gained nearly two pounds over the course of a year, according to one study published in the journal JAMA Psychiatry. It’s not the only SSRI linked with weight gain, but if that’s a concern for you, talk to your doctor about your options.
It’s not the only SSRI linked with weight gain, but if that’s a concern for you, talk to your doctor about your options.
2
GI Effects
“Interestingly, there’s actually a lot of serotonin in the gastrointestinal tract, so people on Zoloft can experience changes in GI function,” says Dr. Murrough. “That could mean an upset stomach, nausea, or changes in bowel habits like constipation or diarrhea.” Dr. Murrough suggests starting on the lowest possible dose to avoid these issues, then increasing the dosage as your system acclimates to the extra serotonin.
3
Sexual Side Effects
This is one of those side effects no one wants to talk about, but it can affect at least a third of patients on SSRIs, says Dr. Murrough. “We don’t know why drugs like Zoloft have sexual side effects, but people can experience things like difficulty orgasming, a lack of sex drive, or the inability to get or maintain an erection. ” For some people, the benefits of the medicine will outweigh the negative effects on their sex life; for others, a change in medication may be necessary.
” For some people, the benefits of the medicine will outweigh the negative effects on their sex life; for others, a change in medication may be necessary.
4
Increased Anxiety
Another one of the more common Zoloft side effects is called akathisia. “It’s like feeling amped up or restless, like you need to move, or like you’re unable to calm down,” explains Dr. Hermann. In some cases, akathisia can even feel like a panic attack. But akathisia can be mitigated by starting on a really low dose and slowly working your way up, she adds.
5
Mood or Behavior Changes
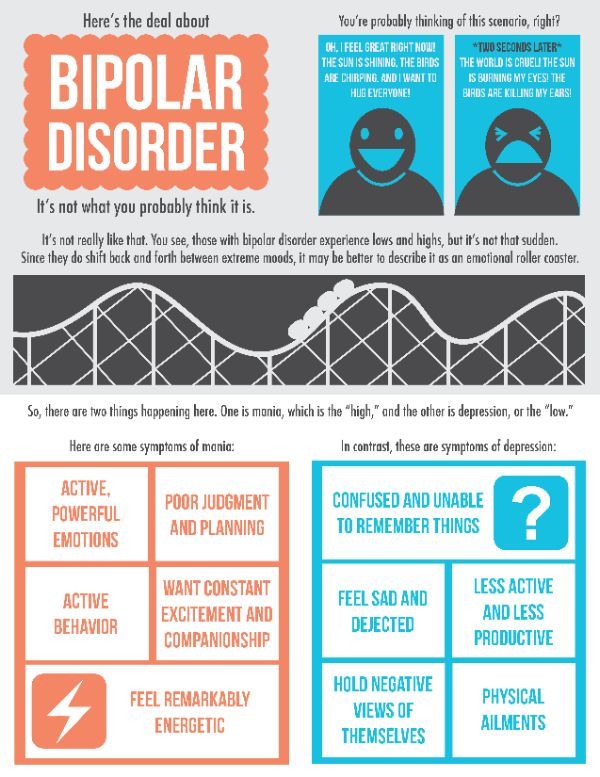
Obviously, you want your mood to change while taking an antidepressant or anti-anxiety drug. “But the mood or behavior change that we’re most worried about as mental health professionals is increased depression or suicidal thoughts or a switch from depression to mania,” says Dr. Hermann. “Any antidepressant intervention has the potential to flip someone who’s vulnerable, who has bipolar disorder rather than depression, into a mania, which is why it’s so important to make sure you have the right diagnosis before starting medication.”
Hermann. “Any antidepressant intervention has the potential to flip someone who’s vulnerable, who has bipolar disorder rather than depression, into a mania, which is why it’s so important to make sure you have the right diagnosis before starting medication.”
6
Night Sweats
“Nighttime sweating is a common side effects of SSRIs, and Zoloft is one of the drugs where it’s more common,” says Dr. Hermann. “It’s not dangerous at all, provided that the person is seeing an internist regularly and has had a physical exam and lab work within the year to indicate there’s nothing else responsible for it.” It is uncomfortable, though, so Hermann recommends wearing sweat-wicking materials to bed and keeping your bedroom cool enough at night.
7
Serotonin Syndrome
“This is a catch-all term for what happens when there’s too much serotonin in the body,” says Dr. Murrough. “It affects your blood pressure, can cause severe GI symptoms, and can even lead to confusion, fevers, and seizures—in extreme cases, it’s life-threatening.”
Murrough. “It affects your blood pressure, can cause severe GI symptoms, and can even lead to confusion, fevers, and seizures—in extreme cases, it’s life-threatening.”
The risk is very low for people who are just taking one medication, but if someone is on several medications that affect serotonin levels, the risk level rises. “Sometimes, people describe this as a bad flu—so on the off chance that happens, call your doctor right away,” says Dr. Murrough. “The treatment is to simply stop the medication.”
8
Trouble Sleeping
In most cases, antidepressants and anti-anxiety meds help people sleep better. But, occasionally, “people report unusual dreams, restlessness during sleep, or feeling like their sleep is altered in some way,” says Dr. Hermann.
This is a potential risk of taking something that affects your brain, says Dr. Hermann, and if it’s disruptive enough to your life, your doctor might try you on a different drug.
9
Rashes
Sometimes people can develop rashes or increased skin sensitivity while taking Zoloft, says Naema Qureshi, MD, a psychiatrist at Brooklyn Minds. It’ll usually go away on its own, and you can find relief in the mean time with an over-the-counter anti-itch cream.
“However, if you show signs of an allergic reaction, such as hives, itchiness, or throat swelling shortly after you start Zoloft, you should stop taking it and report these symptoms to your doctor immediately,” says Dr. Qureshi.
10
Headaches
Headaches are common when you first start taking Zoloft, or when you increase the dose, says Dr. Qureshi.
“For most people, headaches go away after a week or two as your body adjusts to the medication,” she explains. “If you experience occasional headaches while starting the medication, you can try common over-the-counter pain relievers such as Tylenol.![]() ”
”
If your headaches are persistent, Dr. Qureshi recommends talking to your doctor, as it’s possible you may tolerate a different medication better.
11
Dry Mouth
Dry mouth is another common side effect of Zoloft which can sometimes persist, says Dr. Qureshi.
“It's important to pay attention to dry mouth because it can increase your risk of cavities and other oral issues,” she says. “In addition to maintaining good oral hygiene and hydration, you could consider trying a toothpaste or mouthwash specifically designed for dry mouth.”
12
Rare Side Effects
While most people tolerate Zoloft well, patients can experience rare but serious side effects such as vision changes, seizures, confusion, and dizziness while taking it, says Dr. Qureshi. Talk to your doc about any underlying conditions you have before you start any new meds, how Zoloft might interact with anything you're already taking, and seek immediate help if you start experiencing any of these uncommon side effects.
Ashley Mateo Ashley Mateo is a writer, editor, and UESCA- and RRCA-certified running coach who has contributed to Runner’s World, Bicycling, Women's Health, Health, Shape, Self, and more.
Emilia Benton Emilia Benton is a Houston-based freelance writer and editor.
Zoloft (Sertraline) & Headaches: Does It Cause or Treat Headaches?
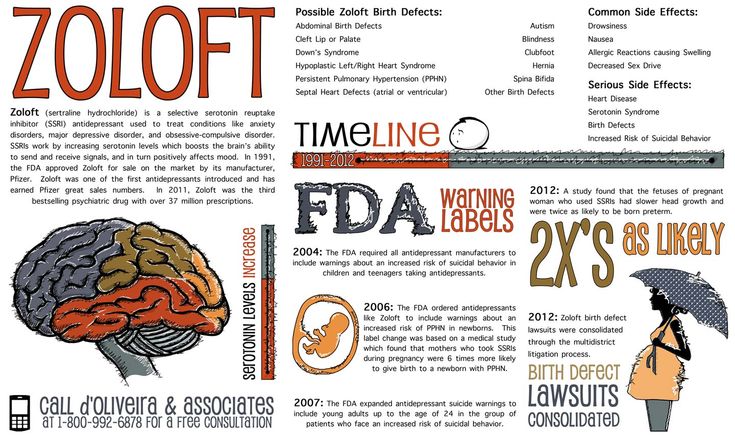
Zoloft (Sertraline), is an SSRI (selective serotonin reuptake inhibitor) prescribed for the treatment of major depressive disorder, OCD (obsessive-compulsive disorder), panic disorder, and social anxiety disorder. It was approved by the FDA in 1991 and initially marketed by the pharmaceutical company Pfizer. In 2013, Zoloft became the single most popular antidepressant medication in the United States with over 41 million prescriptions filled throughout the year.
If compared to other antidepressant medications, evidence suggests that Zoloft is similar in both effectiveness and tolerability. Through its ability to inhibit the reuptake of serotonin within the brain, Zoloft can treat a variety of neuropsychiatric conditions. Additionally, there’s preliminary evidence suggesting that Zoloft may prove useful as a treatment for headaches.
Additionally, there’s preliminary evidence suggesting that Zoloft may prove useful as a treatment for headaches.
Conversely, many individuals claim that Zoloft actually causes them to experience bad headaches as a side effect. It seems as though whether Zoloft helps to treat headaches or causes headaches as a side effect is subject to significant individual variation. This article will discuss why Zoloft might help treat headaches in a subset of persons, yet cause headaches in others.
How often do headaches occur as a Zoloft side effect?
Research suggests that headache is one of the most common side effects of Zoloft (along with nausea, diarrhea, dry mouth, insomnia, somnolence, tremor, headache, and sexual dysfunction). According to data compiled by Murdoch & McTavish (1992), the aforementioned side effects (one of which is headaches) will occur in 10% to 20% of patients. That said, the percentage of patients that specifically end up with headaches as a side effect remains unknown.
According to research from Cipriani, La Ferla, Furukawa, et al. (2009), sertraline is associated with approximately 1.6-fold increased likelihood of headache as a side effect compared to tricyclic antidepressants. The finding that sertraline increases odds of headache compared to tricyclic antidepressants was derived from 5 trials with 1090 participants in which sertraline was compared to amitriptyline. However, because amitriptyline is used as first-line agent to treat headaches, this finding shouldn’t be surprising.
- Source: https://www.ncbi.nlm.nih.gov/pubmed/1281075
- Source: https://www.ncbi.nlm.nih.gov/pubmed/19370626
Zoloft (Sertraline) & Headaches: Possible Causes of this Side Effect
If you experience headaches while taking Zoloft, listed below are some potential causes. That said, you should know that the specific causes of headache on Zoloft will be subject to significant individual variation. A subset of Zoloft users might experience headaches specifically as a result of medication-induced changes in cerebral blood flow, whereas other individuals might experience headaches as a result of changes in the neurotransmission of serotonin – or a combination of blood flow and neurotransmitter changes.
- Adaptation to Zoloft: Many individuals may experience headaches as a transient Zoloft side effect in the first few months after treatment commencement. During the first few weeks or months of treatment, the brain and central nervous system are undergoing adaptation to the presence of Zoloft and its neurochemical effects. While undergoing adaptation, there may be changes in neurotransmitter levels, receptor densities, regional blood flow, and regional activation – each of which, or the combination of which, could potentially induce headaches. If you just started taking Zoloft, this adaptation phase of treatment might account for your headaches. Continuing to use Zoloft for several months may cause the headaches to abate if they were initially related to lack of physiologic adaptation to the medication.
- Administration timing: It’s possible that the timing at which you administer Zoloft might be culpable for triggering headaches as a side effect as a result of an interaction with circadian biology.
 It is understood that circadian biology influences the production of hormones and neurotransmitters throughout the body at different times of day. This considered, it’s reasonable to speculate that individualized circadian rhythms may increase or decrease likelihood of headaches as a side effect of Zoloft based on its timing of administration. For one person, administering Zoloft before bed might increase likelihood of headaches, yet for another person taking Zoloft before bed may decrease odds of headaches – largely due to medication-circadian biology interactions.
It is understood that circadian biology influences the production of hormones and neurotransmitters throughout the body at different times of day. This considered, it’s reasonable to speculate that individualized circadian rhythms may increase or decrease likelihood of headaches as a side effect of Zoloft based on its timing of administration. For one person, administering Zoloft before bed might increase likelihood of headaches, yet for another person taking Zoloft before bed may decrease odds of headaches – largely due to medication-circadian biology interactions. - Cerebral blood flow: It is documented that SSRI antidepressants like Zoloft can alter cerebral blood flow in throughout the brains of users. Evidence suggests that Zoloft and other SSRIs often significantly increase cerebral blood flow in the prefrontal cortex. Moreover, some individuals may experience decreased cerebral blood flow as a result of SSRI-induced vasoconstriction; this is a rare adverse effect.
 Because significant changes in cerebral blood flow can induce headache and migraine, it’s possible that Zoloft-mediated cerebral blood flow change is a cause of headache.
Because significant changes in cerebral blood flow can induce headache and migraine, it’s possible that Zoloft-mediated cerebral blood flow change is a cause of headache. - Dosage adjustments: Anytime you increase or decrease your Zoloft dosage, it takes time for your brain and body to adapt to the new dose. If you increase the dosage, you’re ingesting a greater quantity of sertraline, which in turn, alters brain activity to a greater extent than lower dosages. More specifically, alterations in neurotransmission and cerebral blood flow due to lack of adaptation to the increased dosage may explain the headaches. Oppositely, if the Zoloft dosage was recently decreased, neurophysiologic adjustments may take place such that headache occurs as a symptom of withdrawal from the larger dose.
- Interaction effects: If you’re using Zoloft with other medications and/or supplements or mixing Zoloft and alcohol, there’s a chance that Zoloft might be interacting with the other substance(s) to cause your headache.
 Zoloft might interact with the other substance(s) during metabolism (i.e. pharmacokinetically) or within the body (i.e. pharmacodynamically) to increase likelihood of headache. For example, if Zoloft and another substance synergistically alter cerebral blood flow or neurotransmission, the synergistic effects might be the cause of your headaches.
Zoloft might interact with the other substance(s) during metabolism (i.e. pharmacokinetically) or within the body (i.e. pharmacodynamically) to increase likelihood of headache. For example, if Zoloft and another substance synergistically alter cerebral blood flow or neurotransmission, the synergistic effects might be the cause of your headaches. - Missed doses: If you accidentally skip a dose of Zoloft or mistime your dosing, you may experience headaches as a result of withdrawal. The effects of a single Zoloft pill are suggested last for a total of 24 hours. If you forget to take your Zoloft dose, your body enters an early stage of Zoloft withdrawal whereby headache can occur as a withdrawal symptom. Resuming your medication as soon as possible and adhering to a dosing schedule can minimize likelihood of headache throughout treatment.
- Neural connectivity: Evidence from neuroimaging studies suggests that SSRIs like Zoloft can alter brain connectivity within just 3 hours of treatment.
 Specifically, SSRI medications appear to decrease neural connections in most regions of the brain with the exception of the thalamus and cerebellum. In the thalamus and cerebellum, connectivity significantly increases after antidepressant administration. Other research indicates that SSRIs substantially modulate functional connectivity in the anterior cingulate cortex (ACC) and limbic regions. Based on the fact that Zoloft changes the connections within your brain, we must consider that this is another potential cause of headache.
Specifically, SSRI medications appear to decrease neural connections in most regions of the brain with the exception of the thalamus and cerebellum. In the thalamus and cerebellum, connectivity significantly increases after antidepressant administration. Other research indicates that SSRIs substantially modulate functional connectivity in the anterior cingulate cortex (ACC) and limbic regions. Based on the fact that Zoloft changes the connections within your brain, we must consider that this is another potential cause of headache. - Neurotransmitter levels: Zoloft is understood to function as a selective-serotonin reuptake inhibitor whereby it increases serotonin levels extracellularly. Research suggests that the neurotransmitter serotonin is implicated in the pathogenesis of many types of headaches, including migraine and tension-type. It’s possible that, for a subset of persons, using Zoloft could alter serotonergic transmission throughout the brain in ways that increase susceptibility to headache.
- Oxidative stress increase: Some research suggests that high-dose Zoloft administration significantly increases levels of oxidative stress. It is known that high oxidative stress may play a role in headache or migraine pathogenesis. For this reason, it’s fair to suspect that Zoloft-induced oxidative stress could trigger headaches in susceptible individuals.
- Regional activity: In addition to modifying neural connectivity, Zoloft and other SSRIs appear to alter activation of various brain regions. It is understood that antidepressants increase activation of the prefrontal cortex, a brain region that’s often underactive among persons with depression. Additionally, antidepressants also appear to decrease hyperactivity or overactivation within the limbic regions of the brain. That said, the regional activity changes induced by Zoloft might cause headaches for a subset of users.
- Side effects: Even if Zoloft doesn’t directly cause headaches, it’s possible that other Zoloft side effects might provoke or increase likelihood that headaches will occur.
 For example, insomnia is a common side effect of Zoloft that might interfere with your sleep quality. If you’re getting less sleep or worse sleep while using Zoloft as a result of insomnia (as a side effect), this might indirectly provoke headaches.
For example, insomnia is a common side effect of Zoloft that might interfere with your sleep quality. If you’re getting less sleep or worse sleep while using Zoloft as a result of insomnia (as a side effect), this might indirectly provoke headaches. - Withdrawal from Zoloft: If you’re tapering off of Zoloft or withdrawing from Zoloft, you may experience headaches as a Zoloft withdrawal symptom. During withdrawal from the medication, headaches can be triggered by many things, including: neurotransmitter adjustments, blood flow changes, poor sleep, electrolyte imbalances, high anxiety, hormone changes, etc.
Note: Experiencing headaches while taking Zoloft might also be a coincidence rather than a side effect. For example, if while taking Zoloft you: are exposed to high stress, aren’t getting proper sleep, are dehydrated, aren’t eating enough calories, or aren’t consuming a nutritious diet – these could explain your headache. If you aren’t living a healthy lifestyle, it may be difficult to know whether your headaches are legitimately attributable to Zoloft.
- Source: https://www.ncbi.nlm.nih.gov/pubmed/8588061
- Source: https://www.ncbi.nlm.nih.gov/pubmed/15641869
- Source: https://www.ncbi.nlm.nih.gov/pubmed/26412065
- Source: https://www.ncbi.nlm.nih.gov/pubmed/24610613
How Zoloft Might Treat Headaches…
Not everyone will experience headaches as a side effect of Zoloft. In fact, preclinical evidence suggests that Zoloft may prove efficacious as a treatment for tension-type headaches, regardless of comorbid neuropsychiatric conditions. In other words, some individuals will find that Zoloft prevents or reduces the frequency and/or severity of headache or migraine. Though the exact mechanism(s) by which Zoloft might treat headaches is unknown, below are a few possibilities.
- Anxiety reduction: One obvious way in which Zoloft may treat or prevent headaches is by reducing anxiety and stress. As a selective-serotonin reuptake inhibitor, Zoloft upregulates concentrations of extracellular serotonin to treat anxiety disorders.
 Untreated anxiety disorders and/or stress increase one’s risk of experiencing tension-type headaches and migraine. High anxiety can disrupt electrolyte, neurotransmitter, and hormone levels, as well as alter blood flow within the brain to trigger headaches. Assuming Zoloft effectively treats your anxiety, this may be reason as to why it also alleviates headaches.
Untreated anxiety disorders and/or stress increase one’s risk of experiencing tension-type headaches and migraine. High anxiety can disrupt electrolyte, neurotransmitter, and hormone levels, as well as alter blood flow within the brain to trigger headaches. Assuming Zoloft effectively treats your anxiety, this may be reason as to why it also alleviates headaches. - Brain activation changes: As was mentioned, ongoing Zoloft treatment alters many aspects of brain activity, including: cerebral blood flow, neural connectivity, neurotransmission, and regional activation. It’s possible that brain activity changes attributable to Zoloft administration might protect against headache.
- Blood flow: Treatment with Zoloft can alter blood flow within the brain. Modulation of blood flow to certain regions of the brain might prevent or minimize the severity of headaches.
- Neural connectivity: Treatment with Zoloft can alter neural connectivity (connections between brain regions).
 Modulation of neural connectivity in certain areas of the brain might help treat headaches.
Modulation of neural connectivity in certain areas of the brain might help treat headaches. - Neurotransmission: Zoloft functions by inhibiting the reuptake of serotonin within the brain. Because serotonin irregularities may play a role in headache and/or migraine, normalizing serotonin levels with Zoloft might help treat headaches.
- Regional activation: Zoloft can increase activity in certain regions of the brain and decrease activity in others. It’s possible that modulation of regional activity via Zoloft could help reduce headache frequency and/or severity.
- Depression treatment: Untreated depression is associated with increased risk of experiencing tension-type headaches. Some evidence also suggests that depressive disorders may increase risk of migraine. If you have headaches with comorbid depression and Zoloft effectively treats your depressive symptoms, this could be the way in which it is alleviating your headache.
 In other words, mood enhancement might be the reason you’re experiencing fewer headaches on Zoloft than pre-treatment.
In other words, mood enhancement might be the reason you’re experiencing fewer headaches on Zoloft than pre-treatment. - Inflammation reduction: Unmanaged neuroinflammation is thought to play a role in the pathogenesis of headache and migraine. This considered, it’s fair to speculate that reducing inflammation might reduce the frequency and/or severity of headaches. Evidence suggests that taking Zoloft for 12 weeks can decrease systemic inflammation to a significant extent, as evidenced by serum reductions in CRP (C-Reactive Protein) – a biomarker of inflammation. If your systemic inflammation decreases while using Zoloft, this anti-inflammatory effect may be how the medication is treating your headaches.
- Sleep enhancement: If before using Zoloft your sleep quality was poor or duration was suboptimal for physiological needs, this may have been reason as to why you were experiencing headaches. Poor sleep can increase inflammation, increase the stress response, modify hormone secretion, and alter many facets of brain activity.
 If after taking Zoloft for a while your sleep improves in terms of quality and/or duration, this may be reason as to why you’re experiencing fewer or less severe headaches than usual.
If after taking Zoloft for a while your sleep improves in terms of quality and/or duration, this may be reason as to why you’re experiencing fewer or less severe headaches than usual.
Using Zoloft for Headaches: A Potential Treatment (Research)
It is known that Zoloft was once considered an investigational medication for the treatment of headaches. In other words, if Zoloft would’ve shown significant promise in managing headaches, perhaps it would’ve undergone clinical trials for the treatment of headaches. If approved, we might see Zoloft being marketed as a headache medication. Nevertheless, included below are studies in which the efficacy of Zoloft was examined or discussed for the management of headaches.
2003: Sertraline versus amitriptyline in the prophylactic therapy of non-depressed chronic tension-type headache patients.
Boz, Altunayoglu, Velioglu, et al. noted that individuals with chronic tension-type headache (CTTH) are usually the most challenging to treat. First-line treatments for chronic tension-type headaches consist primarily of tricyclic antidepressants (TCAs), however, many individuals find them difficult to tolerate due to anticholinergic side effects. For this reason, the aforementioned researchers sought to determine if sertraline, an SSRI, may prove useful in the prevention of chronic tension-type headaches in non-depressed persons.
First-line treatments for chronic tension-type headaches consist primarily of tricyclic antidepressants (TCAs), however, many individuals find them difficult to tolerate due to anticholinergic side effects. For this reason, the aforementioned researchers sought to determine if sertraline, an SSRI, may prove useful in the prevention of chronic tension-type headaches in non-depressed persons.
A parallel-group randomized study was organized in which the efficacy of sertraline was compared to that of amitriptyline for the prophylaxis of chronic tension-type headaches. Study participants were monitored for a 4-week baseline period, then were assigned to receive either: 50 mg sertraline (41 patients) or 25 mg amitriptyline (44 patients) – for a 12-week treatment phase. The efficacies of each intervention were determined based on headache diaries in which the following were documented: occurrence; number; intensity; and duration – of headaches.
Results indicated that both sertraline and amitriptyline significantly decreased headache symptoms and need to use analgesic medications in the first, second, and third months of treatment – compared to baseline recordings. That said, amitriptyline was significantly superior in reducing headache symptoms and need to use analgesic medications in the second and third months of the study. In terms of tolerability, recipients of sertraline experienced fewer debilitating side effects.
That said, amitriptyline was significantly superior in reducing headache symptoms and need to use analgesic medications in the second and third months of the study. In terms of tolerability, recipients of sertraline experienced fewer debilitating side effects.
It was concluded that both sertraline and amitriptyline are effective in the management of chronic tension-type headache. However, when efficacies are compared, amitriptyline seems to be more effective. While sertraline may not be as effective as amitriptyline, it still might be of therapeutic value in treating chronic tension-type headaches.
- Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3452139/
2002: Sertraline in chronic tension-type headache.
Singh and Misra conducted a randomized, double-blinded, placebo-controlled study to evaluate the efficacy of sertraline for the treatment of chronic tension-type headache (CTTH). The researchers recruited a total of 50 patients who were diagnosed with chronic tension-type headache to participate in a 10-week study. The first 2 weeks of the study consisted of a run-in phase, the next 4 weeks were the treatment phase, and the final 4 weeks served as a follow-up phase.
The first 2 weeks of the study consisted of a run-in phase, the next 4 weeks were the treatment phase, and the final 4 weeks served as a follow-up phase.
The effectiveness of sertraline was determined based upon: headache index scores, analgesic usage (per week), and percentage (%) reduction in headache frequency. Results indicated that recipients of sertraline exhibited significant reductions in weekly analgesic intakes from ~4.34 to ~1.07 tablets per week, whereas recipients of the placebo did not exhibit significant reductions in weekly analgesic intakes. That said, headache index scores and percentage reductions in headache frequency did not significantly change among recipients of sertraline.
Researchers concluded that, based on significant reductions in weekly analgesic intakes among sertraline recipients, sertraline may prove therapeutic in the management of chronic tension-type headache. More specifically, it was stated that sertraline may be a viable alternative to amitriptyline among persons who find amitriptyline to be ineffective or intolerable.
- Source: https://www.ncbi.nlm.nih.gov/pubmed/12126338
1999: Selective serotonin reuptake inhibitors for migraine prophylaxis.
Landy, McGinnis, Curlin, and Laizure sought to determine the therapeutic potential of sertraline in the prevention of migraine. Researchers organized a study in which 27 adults with a history of migraine participated. The study begun with a 4-week baseline phase in which migraine frequency and severity were monitored among participants without treatment.
Thereafter, participants were assigned at random to receive either: sertraline or a placebo in double-blinded manner – for a duration of 8 weeks. The effectiveness of sertraline as a migraine prophylactic was determined based upon daily diaries in which migraine: occurrence, severity, and degree of impairment – were recorded. Researchers utilized the diary data to determine changes in “headache index” scores or composite scores calculated based upon migraine frequency and severity.
Results indicated that headache index scores did not significantly improve from baseline (~20.8) through week 8 (~17.6) or week 12 (~16.7). Researchers noted that the finding in this study was similar to findings in which other SSRIs (fluoxetine, fluvoxamine, and paroxetine) were evaluated for migraine prophylaxis. It was concluded that SSRIs may lack efficacy in migraine prophylaxis, but may offer some therapeutic value among individuals with refractory or treatment-resistant migraine and comorbid depression.
Although this study didn’t find sertraline (Zoloft) to be effective for migraine prevention, there were some serious limitations, including the small sample size (just 6 participants used Zoloft for the full 12-week duration). Moreover, it’s possible that dosages of sertraline may have been inadequate to effectively prevent migraine. Due to the small sample size, it’s difficult to confirm that sertraline lacks efficacy in migraine prophylaxis.
- Source: https://www.
 ncbi.nlm.nih.gov/pubmed/15613191
ncbi.nlm.nih.gov/pubmed/15613191
Based on the research, is Zoloft an effective treatment for headaches?
Possibly. As of current, data derived from studies in which the efficacy of Zoloft for headache was investigated – are limited. Moreover, all studies are limited by small sample sizes. For this reason, it’s difficult to elucidate whether Zoloft is of legitimate therapeutic value in the treatment of headache and/or migraine.
Searching through PubMed, I was only able to dig up 3 studies in which Zoloft was evaluated for the treatment of headache: 2 studies testing it for tension-type headache and 1 study for migraine prevention (i.e. prophylaxis). If data from existing studies are accurate, it would seem as though administration of Zoloft at 50 mg per day for 4-12 weeks might prove useful in treating chronic tension-type headache – especially among those who respond poorly to first-line interventions. However, it does not seem as though Zoloft would be useful as a migraine prophylactic.
- Boz et al. (2003): A study by Boz et al. concluded that sertraline (50 mg per day) was effective in the management of chronic tension-type headache over a 12-week period in patients without depression. Yet when compared to amitriptyline, (a tricyclic antidepressant commonly used to treat headache), Zoloft was significantly less effective.
- Singh and Misra (2002): A 10-week study by Singh and Misra discovered that ongoing sertraline treatment reduced analgesic intakes from ~4 tablets per week (at baseline) to ~1 tablet per week among individuals with chronic tension-type headache. This finding suggested that Zoloft may be of value in preventing or reducing the severity of chronic tension-type headache.
- Landy et al. (1999): A well-designed yet very small-scale study by Landy et al. discovered that Zoloft was ineffective as a migraine prophylactic over a 12-week span. However, in this study there were only 6 individuals in the treatment group (using Zoloft for the full 12 weeks).
Using Zoloft for headache or migraine treatment (Possible scenarios)
There are a few scenarios where it may be worth testing the efficacy of Zoloft as a treatment for headache and/or migraine. The most obvious scenario would be if an individual presented headache plus comorbid anxiety and/or depressive symptoms. Another scenario might be if an individual reacted poorly to first-line headache medications (in terms of effect or tolerability) – or if the headache is classified as refractory (difficult-to-treat).
- Comorbid anxiety and/or depression: If you have comorbid anxiety and/or depression with headache or migraine, it may be worth trying Zoloft. Zoloft is frequently prescribed as a first-line intervention for major depressive disorder and anxiety disorders. If Zoloft is effective for anxiety and/or depression – plus headache – you may be able to use just one medication to manage all of your symptoms rather than using one drug for headache, another for depression, and/or another for anxiety – (which could get difficult to manage and/or increase likelihood of adverse interactions).
- Chronic tension-type headache: There’s evidence to suggest that Zoloft at a dosage of 50 mg per day may be effective in the treatment of chronic tension-type headache in non-depressed adults. One study found that daily Zoloft administration lead to significant decreases in headache frequency and severity, as well as the need to use analgesic medications (for headache relief) over a 12-week span.
- Poor response to first-line therapies: If you’ve tested all first-line headache therapies and find them to be ineffective, suboptimally effective, or intolerable – you may need to explore other options like Zoloft. A few studies suggest that Zoloft may be useful as a headache medication among persons who respond poorly to first-line headache therapies.
- Refractory headache or migraine: If you’ve tested every clinically-recommended medication for the treatment of headache and migraine, yet you aren’t getting symptomatic relief – you may have refractory headache or migraine.
 Refractory means that your headache or migraine is difficult-to-treat and isn’t responding to conventional therapies. In this case, you may want to try Zoloft as an off-label intervention based on preliminary evidence suggesting that it might help.
Refractory means that your headache or migraine is difficult-to-treat and isn’t responding to conventional therapies. In this case, you may want to try Zoloft as an off-label intervention based on preliminary evidence suggesting that it might help.
Variables that may influence Zoloft-induced headaches or Zoloft’s efficacy as a headache treatment
There are several variables that may influence whether Zoloft ends up causing headaches, treating headaches, or having zero impact on headaches throughout treatment. These variables include: concurrent substance use; genetics; lifestyle; duration of Zoloft use; Zoloft dosage; and comorbid medical conditions. It is the combination of these variables that probably determines whether someone will experience headaches on Zoloft – or get headache relief from it.
- Concurrent substance use: If you’re using other substances (medications and/or supplements) along with Zoloft, there’s a chance that the headaches you’re experiencing during treatment might stem from synergistic physiologic effects (induced by Zoloft and another substance).
 It’s also possible that some sort of pharmacokinetic or pharmacodynamic interaction effect between Zoloft and another medication is to blame for your headaches. Additionally, if you’re using other substances with Zoloft, it’s possible that the other substance(s) are more culpable for your headache than the Zoloft. Another possibility is that other substances are the sole reason for your headaches (that you’ve mistakenly assumed are from Zoloft).
It’s also possible that some sort of pharmacokinetic or pharmacodynamic interaction effect between Zoloft and another medication is to blame for your headaches. Additionally, if you’re using other substances with Zoloft, it’s possible that the other substance(s) are more culpable for your headache than the Zoloft. Another possibility is that other substances are the sole reason for your headaches (that you’ve mistakenly assumed are from Zoloft). - Genetics: It is understood that a person’s genetics and epigenetics might determine their risk for headache and migraine. If you do a bit of research, you’ll see that certain genes and phenotypes are associated with increased risk of headache and migraine – whereas others may be protected against headache and migraine. If you are at high risk of experiencing headaches based on your genes, you might be more likely to experience headaches as a side effect of Zoloft than another user.
- Lifestyle & environment: Various lifestyle and environmental factors might also influence whether Zoloft is likely to cause headaches – or its efficacy as a treatment for headaches.
 Examples of lifestyle and environmental factors include: diet (vitamin/nutrient intake), sleep (quality/quantity), sunlight exposure, artificial light exposure, pollution, exercise, stressors, etc. Someone living a high stress lifestyle who’s exposed to air pollution and/or noise pollution may experience headaches regardless of the Zoloft. Oppositely, a low stress lifestyle in an environment devoid of pollution may protect against headaches on Zoloft – or increase its efficacy as a treatment.
Examples of lifestyle and environmental factors include: diet (vitamin/nutrient intake), sleep (quality/quantity), sunlight exposure, artificial light exposure, pollution, exercise, stressors, etc. Someone living a high stress lifestyle who’s exposed to air pollution and/or noise pollution may experience headaches regardless of the Zoloft. Oppositely, a low stress lifestyle in an environment devoid of pollution may protect against headaches on Zoloft – or increase its efficacy as a treatment. - Duration of Zoloft use: The total duration over which you’ve used Zoloft might determine whether some individuals experience headaches as a side effect – or find the drug effective in treating headaches. If you’ve only used Zoloft for a short-term, headaches might occur as an adaptation-related side effect. Moreover, short-term use probably isn’t enough time to derive therapeutic benefit from Zoloft for headache treatment.
- Zoloft dosage: Certain dosages of Zoloft might increase odds of experiencing headaches as a side effect – or increase odds that the drug effectively treats headaches.
 Evidence suggests that a dosage of 50 mg per day seems to be useful in the treatment of tension-type headache. That said, it is understood that high doses of Zoloft (e.g. above 50 mg) can increase oxidative stress which might provoke headaches. There’s usually individual variation in terms of dose-responses to Zoloft for the treatment of headaches – and sometimes the occurrence of headaches as a side effect (e.g. headaches might only occur at very high doses for some persons).
Evidence suggests that a dosage of 50 mg per day seems to be useful in the treatment of tension-type headache. That said, it is understood that high doses of Zoloft (e.g. above 50 mg) can increase oxidative stress which might provoke headaches. There’s usually individual variation in terms of dose-responses to Zoloft for the treatment of headaches – and sometimes the occurrence of headaches as a side effect (e.g. headaches might only occur at very high doses for some persons). - Medical conditions: If you have a history of headache and/or migraine, you’ll probably be at increased risk of experiencing headaches during Zoloft treatment. Other medical conditions may also increase your risk of experiencing headache on Zoloft, including OCD. Some literature suggests that persons with OCD (obsessive-compulsive disorder) tend to experience headaches more frequently while using SSRIs than those without OCD. Ask your doctor whether preexisting medical conditions may increase or decrease your risk of headache while using Zoloft.
Possible ways to minimize headaches on Zoloft
Though headache is a common side effect of Zoloft, a majority Zoloft users will not experience frequent or severe headaches as a result of the medication. That said, if you end up with frequent or debilitating headaches while using Zoloft, below are some potential strategies for minimizing their occurrence. Understand that you should always inform a medical doctor of headaches that you’re experiencing while taking Zoloft. Moreover, you should never implement any of these headache mitigation strategies without first consulting a medical doctor and verifying that they’re safe and/or potentially useful.
- Administration timing: Some individuals may end up with headaches as a side effect of Zoloft because they fail to administer Zoloft at the same time each day. Zoloft is intended to be taken once per day (24-hour period) at the exact same time each day. If you forget to take your daily dose or mistime your dosing, you may experience headaches as a result of a temporary or mini withdrawal.
 Strict adherence to a dosing schedule (e.g. taking Zoloft every day at ~8:00 AM) may help minimize headaches. Moreover, if you’re experiencing headaches while taking Zoloft in the morning, you may want to try shifting its administration timing to the afternoon or night to see if a different time might help (via circadian-medication interactions).
Strict adherence to a dosing schedule (e.g. taking Zoloft every day at ~8:00 AM) may help minimize headaches. Moreover, if you’re experiencing headaches while taking Zoloft in the morning, you may want to try shifting its administration timing to the afternoon or night to see if a different time might help (via circadian-medication interactions). - Adjust your lifestyle: If you’re living a high-stress lifestyle and aren’t attempting to stay healthy, this could be why you’re experiencing headaches on Zoloft. Focus on eating a nutritious diet, stay hydrated, minimize your stress, get some exercise each day, get natural light, avoid excessive artificial light, and get plenty of sleep each night. Living a healthy lifestyle might completely attenuate your headaches.
- Dosage adjustment: If your headaches have become an annoying Zoloft side effect, you may want to ask your psychiatrist about dosage adjustments. Sometimes decreasing your Zoloft dosage or titrating down to the “minimal effective dose” might alleviate your headaches.
 In other cases, you might need to increase your dose to better treat conditions like anxiety and/or depression – each of which might be responsible for causing your headaches.
In other cases, you might need to increase your dose to better treat conditions like anxiety and/or depression – each of which might be responsible for causing your headaches. - Concurrent medications: If you’re using other substances (medications and/or supplements) along with Zoloft, it is recommended that you review them with your doctor. Concurrent substance use might be the chief reason that you’re experiencing headaches. If a substance that you’re using is interacting with Zoloft, this interaction effect might be the reason you’re experiencing headaches. Another possibility is that concurrently administered substances are causing headaches as a side effect – and you’ve mistakenly blamed the headaches on Zoloft. For this reason, you may want to discontinue all medically-unnecessary substances for a while and see if your headaches abate. Another option might be to add another medication or supplement to your daily regimen to prevent and/or treat headaches.
- Use for a longer-term: If you’re a new Zoloft user and are experiencing headaches, you may want to try using it for a longer-term. Sometimes headaches are merely a transient side effect due to lack of physiologic adjustment to Zoloft. If the headaches you’re experiencing are a side effect stemming from lack of physiologic adaptation to the medication, the headaches may dissipate within 4 to 8 weeks of treatment.
Note: If you find it difficult to cope with headaches while using Zoloft, you may want to ask your doctor about Zoloft withdrawal and/or switching to another antidepressant medication. Understand that, if you decide to discontinue Zoloft treatment, headaches may worsen or persist for a while until your neurochemistry rebalances.
Conclusion: Does Zoloft cause headaches or treat headaches?
As was mentioned earlier, Zoloft may cause headaches in a subset of users and prevent or reduce the frequency and/or severity of headaches in others. Individual variables will determine who is most at risk of experiencing Zoloft-induced headaches.
Individual variables will determine who is most at risk of experiencing Zoloft-induced headaches.
If you’ve used Zoloft for a reasonable length of time, share a comment below mentioning whether you’ve experience headaches as a side effect of treatment. Included below is a list of questions that you may want to answer to help others understand your experience with headaches while using Zoloft.
- If you’ve noticed more headaches or severe headaches while using Zoloft, do you believe the headaches are directly caused by Zoloft? (Or is it possible that your lifestyle and/or concurrent substance use (medications or supplements) might be triggering your headaches?)
- Assuming you experience headaches while using Zoloft, are they severe enough to warrant withdrawal or switching to another medication?
- If you have a medical history of headaches, have you noticed a reduction in headache frequency or severity since initiating treatment with Zoloft?
- Moreover, document the type of headaches that you usually experience such as: migraine, chronic tension-type headaches, etc.
- To help others get a better understanding of your situation, mention things like your: Zoloft dosage, primary reason for using Zoloft (e.g. to treat depression), and how long you’ve used it (in total).
Why does it hurt? Hidden Meanings of Pain Medical On Group St. Petersburg
Pain is an important signal that a failure has occurred in some of the body's systems. But often with pain, the brain signals a hidden emotional overload. Acute stress can lead to a surge and release of emotions and end fairly quickly, however, if the situation does not change, then stress becomes chronic and may well “leave in the body”, manifesting itself in different ways.
These can be pains in the heart, increased pressure, indigestion, spasms of the stomach or biliary tract, depending on the body - it always tears where it is thin. And many nations have figurative descriptions of psychosomatic disorders - in Russia, for example, the expressions “bilious person”, “I earned an ulcer at this work”, “my heart is breaking from all this” are quite often used. All this quite accurately describes the sensations that a person experiences during prolonged stress.
All this quite accurately describes the sensations that a person experiences during prolonged stress.
And even if the body copes with the load, avoiding the development of an organic disease such as pancreatitis, gastritis or hypertension, functional disorders can poison a person's life for a very long time. At the same time, the brain gets used to considering chronic pain as the norm, and adapts to it, closing a vicious circle. And in the end, it turns out that the pain is born in the head, and it manifests itself, for example, by contracting with or without the gallbladder.
What are the shapes:
- tension headache (spasms of the neck muscles),
- neurogenic bronchial asthma,
- vegetative-vascular dystonia with cardialgia (broken heart syndrome on ECG),
- hypertensive crises (stress vasospasm),
- stress-induced gastric ulcer,
- irritable bowel syndrome (diarrhea and constipation),
- neurogenic gastrostasis (stopping stomach contractions),
- psychogenic erectile dysfunction, anorgasmia, painful intercourse,
- neurogenic bladder (urination every half an hour).

By and large, all these diseases come down to the desynchronization of contractions: the alternation of spasms and excessive relaxation leads to the “pot, don’t boil” effect - for a certain time, physiological fluids accumulate, and then splash out in a short period, which the body is unable to cope with. And when a person is nervous, sometimes without noticing it, the flow of stomach acid, bile, blood, bronchial mucus and other substances is disturbed, the well-coordinated system of organs fails, and pain appears.
About the work of the psyche
Each person has his own character traits and his own unique experience that make him react to life situations in one way or another. It can be said about many that they have “cockroaches in their heads” (the main thing is that the interlocutors have them of the same breed). Everyone has their own accentuations, specific personality traits, which become much more pronounced under the influence of stress: the more hassle, the stronger the accentuations, and such an increase in instability must be interrupted in time. It is best to do this at the stage of manifesting symptoms in the body (pain, spasms, hypertension, etc.), when the body is already signaling an overload, but still coping with it.
It is best to do this at the stage of manifesting symptoms in the body (pain, spasms, hypertension, etc.), when the body is already signaling an overload, but still coping with it.
How to treat it?
Influence the nervous system, primarily the central one (the brain), which will send normalized signals to the body (vegetative). This is done with the help of drugs “for nerves”, which are divided into three large groups - antidepressants of various principles of work, anxiolytics and antipsychotics. But the names of these groups are rather conditional: the systematization was created quite a long time ago; medicine has since stepped far forward, and it turned out that the names have remained old, and it is not easy to come up with new ones because of the versatility of the effects and mechanisms of new drugs. As a rule, they act on different groups of receptors simultaneously and exhibit a number of effects, which makes it possible to choose one pill to correct several disorders at once.
These drugs have a remarkable property: they do not cure, but cure, and due to the specifics of their work, it is impossible to get addicted to them, like drugs. The essence of the work of such drugs is the gradual "growing" on neurons of a larger number of receptors - zones that are sensitive to neurotransmitters (a kind of signal transmitters), and fixing this mechanism as a norm. After the drug is discontinued, the effect persists, and the nervous system itself, without outside help, continues to work correctly. But treatment takes time: for digestive disorders, the course lasts from three to six months, for any chronic pain - at least a year.
The selection of the drug and its dose is a separate art. If with inflammatory processes such as ulcers or hepatitis, the selection is based on the results of tests, then with psychotropic therapy this is not possible. Changes in the regulation of the work of human nerve cells are very multifaceted and subtle, and so far it has not been possible to create a coherent system of assessment tools. Therefore, the choice of drugs comes, first of all, from the characteristics of the patient's personality and statistical data. In 80% of cases, the drug can be selected on the first try, but sometimes, according to the results of individual tolerance, a replacement may be required, and this is completely normal. Sometimes a doctor may prescribe two pills at once, if their combination gives exactly the cocktail that the suffering brain needs. This is also normal.
Therefore, the choice of drugs comes, first of all, from the characteristics of the patient's personality and statistical data. In 80% of cases, the drug can be selected on the first try, but sometimes, according to the results of individual tolerance, a replacement may be required, and this is completely normal. Sometimes a doctor may prescribe two pills at once, if their combination gives exactly the cocktail that the suffering brain needs. This is also normal.
Everything has side effects, including this kind of drugs. Yes, they may appear, but they will either pass quickly enough, or the doctor will replace the drug. In addition, for the treatment of psychosomatic disorders, dosages are prescribed much lower than for the treatment of mental disorders, and in such doses, drugs almost do not cause side effects and do not have a clear effect on the mental sphere - for example, the notorious “inhibitory” effect.
Science is constantly evolving, some drugs are becoming obsolete, and new ones are taking their place. For example, due to high toxicity, Aminazine and Amitriptyline are practically no longer prescribed, Teraligen has a safer and more effective successor, and a number of drugs like Quentiapine are used only under dispensary observation. And, of course, the drug market cannot do without “fuflomycins”, which do not have any evidence base; the most popular of them are Phenibut, Afobazol, Tenoten, Adaptol, Novopassit.
For example, due to high toxicity, Aminazine and Amitriptyline are practically no longer prescribed, Teraligen has a safer and more effective successor, and a number of drugs like Quentiapine are used only under dispensary observation. And, of course, the drug market cannot do without “fuflomycins”, which do not have any evidence base; the most popular of them are Phenibut, Afobazol, Tenoten, Adaptol, Novopassit.
Effective drugs for the normalization of the nervous system of the body:
- Grandaxin is a daytime anxiolytic, works in a complex manner, does not cause drowsiness;
- Atarax - a mild anxiolytic, relieves anxiety and itching;
- Eglonil, Sonapax - antipsychotics, stabilize mood swings;
- Trittiko - an atypical antidepressant for anxiety and depressive disorders, improves sleep;
- Paxil - antidepressant, relieves anxiety depressions and panic attacks;
- Zoloft is an invigorating antidepressant, good for apathy and general weakness;
- Duloxent is an antidepressant used to treat chronic pain.

All these drugs are prescribed on special prescription forms, only a doctor can choose the medicine and the regimen. If you need to remove chronic pain or other disruption of the organs, a therapist, cardiologist, urologist or gastroenterologist can give a prescription. If there are obvious mental symptoms - depression, anxiety, guilt, sleep disturbances - it is better to consult a psychotherapist (namely, a psychotherapist, because a psychologist is not a doctor and does not prescribe medications).
Enjoy life, take care of yourself and be healthy!
Zoloft instructions for use: Side effects, analogues, contraindications
POSSIBLE SIDE EFFECTS. A SPECIALIST'S CONSULTATION IS REQUIRED.
Author of the article
Khokhrina Kristina Sergeevna,
pharmacist
All authorsContent of the article
- Zoloft: active substance
- Zoloft: Side effects
- Zoloft: Contraindications
- Zoloft and alcohol
- Zoloft: overdose
- Zoloft: How to stop drinking it
- ALLOFT: Analogs
- Related articles
WHO estimates that 3. 8% of the total population, or 280 million people, suffer from depression. Among them, 5% of adults and 5.7% of persons over 60 years of age. More than 700,000 people die each year from suicide due to depression. Depression is treatable with medication.
8% of the total population, or 280 million people, suffer from depression. Among them, 5% of adults and 5.7% of persons over 60 years of age. More than 700,000 people die each year from suicide due to depression. Depression is treatable with medication.
Doctors prescribe antidepressants. Zoloft is one of them. We asked pharmacist Kristina Khokhrina to tell us in more detail: what side effects it can cause, what active ingredient, contraindications, overdose, is the drug compatible with alcohol and how to stop drinking it.
All products Zoloft26 reviews
Zoloft: active ingredient
Zoloft contains the active ingredient - sertraline in the form of hydrochloride. It is produced in tablets with a dosage of 50 mg and 100 mg. Zoloft is an antidepressant. It is used to treat and prevent depression caused by various causes. And also when:
- obsessive-compulsive disorders
- panic disorders
- post-traumatic stress disorder
- social phobias
How Zoloft works
Zoloft helps to eliminate depressive manifestations:
- relieves anxiety
- normalizes sleep
- reduces somatic manifestations: palpitations, disruption of the gastrointestinal tract, increased excitability.
Zoloft does not cause dependence on the drug and does not lead to weight gain in humans.
Zoloft side effects
Watch your condition carefully while using the medicine. If you experience side effects that are not described or if symptoms worsen, contact your doctor immediately.
Zoloft: side effects
- flatulence, nausea, vomiting, diarrhea, constipation, abdominal pain, dry mouth
- increased heart rate, increased blood pressure
- arthralgia, muscle cramps
- gait disturbance, teeth grinding, drowsiness, syncope, headache, migraine, tremor, insomnia, anxiety, hallucinations, psychosis, nightmares, decreased libido, suicide, coma
- yawning, bronchospasm
- Bedwetting, urinary retention during the day
- hepatitis, jaundice
- decreased potency, disruption of the reproductive system, disruption of the menstrual cycle in women
- visual impairment
- thyroid disorder
- urticaria, pruritus, anaphylactic shock
- flushing, tinnitus, loss of appetite and others
Zoloft: contraindications
- hypersensitivity to any component of the preparation
- concomitant use of monoamine oxidase inhibitors and pimozide
- pregnancy and lactation
- children under 6 years of age
Caution must be taken in: mental retardation, epilepsy, renal and/or hepatic insufficiency, marked reduced body weight.
Zoloft and alcohol
Alcohol is not recommended to be taken with the medicine. Its action can increase side effects and lead to overdose.
Learn how to recognize depression in the article "The Beck Test for Depression"
Zoloft: Overdose
Overdose of Zoloft occurs when used simultaneously with alcohol or other incompatible drugs. With such combinations, severe poisoning can occur, up to coma and death. Overdose symptoms are:
- nausea
- vomiting
- drowsiness
- increased heart rate
- dizziness
- psychomotor agitation
- diarrhea
- excessive sweating
Hospital observation and constant monitoring of vital signs will be required. When first aid is not recommended to induce vomiting, it is better to give activated charcoal.
Zoloft: how to stop drinking it
"Withdrawal" syndrome is rare. Nevertheless, it is necessary to discuss with the doctor a decrease in the dosage of the drug. Since the termination of treatment is possible:
Nevertheless, it is necessary to discuss with the doctor a decrease in the dosage of the drug. Since the termination of treatment is possible:
- symptoms of depression
- hallucinations
- aggression
- anxiety
- psychosis
Particular attention should be paid to the fact that after the end of the use of Zoloft, within 14 days, you should not take drugs related to monoamine oxidase inhibitors.
Zoloft: analogues
Zoloft has about 10 names of analogues of the active substance. All medicines are prescribed and prescribed by a doctor. Therefore, to choose a remedy or replace your own, consult your doctor first.
Zoloft and Atarax: compatibility
The combination of these drugs increases the side effects. This manifests itself in the form of dizziness, drowsiness and confusion. Elderly people have difficulty in thinking and coordinating movements.
Do you want to understand the analogues of drugs in order to skillfully select drugs for your budget? Our manual from expert pharmacists "Analogues of popular drugs" will help you with this! Getting a training manual is easy: subscribe to our social networks and write “analogues” in the messages.
Megapharmacy in social networks: VKontakte, Telegram, OK
Summary
- Zoloft is an antidepressant that is taken to prevent and treat depression and other disorders.
- Zoloft may have a significant number of side effects.
- The active substance is sertraline, dosage in tablets of 50 mg or 100 mg.
- Zoloft has contraindications that should be taken into account when prescribing it.
- The use of alcohol in conjunction with Zoloft is not recommended to avoid overdose symptoms.
- An overdose of the drug occurs when used simultaneously with certain drugs and alcohol.
Learn more