Does effexor cause erectile dysfunction
Effexor Sexual Side Effects Guide
Medically reviewed by Kristin Hall, FNP
Written by Our Editorial Team
Last updated 7/19/2022
Effexor can be a life-changing medication for people suffering from a variety of mood and other disorders, but this medication like most isn’t without its side effects — including Effexor sexual side effects.
From blurred vision and weight gain to withdrawal symptoms like suicidal ideation, antidepressants can cause problems while solving problems.
While Effexor won’t make your eyes melt out of your head or your feet fall off, there are some side effects it has become known for. And f you’ve read about them, you’re probably here to learn more about the risks of Effexor sexual side effects.
To help you understand the relationship between Effexor and your sex life, we’ve answered some of the most common questions people have. Let’s start with the basics.
Does Effexor Cause Sexual Side Effects?
The medication Effexor is a brand-name version of venlafaxine, a serotonin and norepinephrine reuptake inhibitor, also known as an SNRI.
These medications are similar to other antidepressants in that they work to moderate serotonin levels in the brain. But in comparison with SSRIs, SNRIs also moderate another neurotransmitter called norepinephrine.
These antidepressant medications treat major depressive disorder (MDD), but they can also be effective in moderating the symptoms of generalized anxiety disorder (GAD), as well as social anxiety disorder (aptly called SAD) and even panic disorder in certain circumstances. Bipolar disorder patients may also see benefits.
Medications like this often come with side effects, and in the case of venlafaxine, those adverse reactions may include headache, nausea, diarrhea, fatigue, insomnia and, as you probably guessed from the title of this article, some SSRI-induced sexual dysfunction.
online mental health assessment
your mental health journey starts here
Sexual Side Effects of Effexor Explained
Many people become uncomfortable at the idea of hurdles to sexual activity. We get it: sexual functioning is hard enough when you have to be vulnerable and intimate — medication doesn’t need to make it harder.
We get it: sexual functioning is hard enough when you have to be vulnerable and intimate — medication doesn’t need to make it harder.
So, what exactly does antidepressant therapy with venlafaxine do downstairs?
While spontaneous genital combustion isn’t something you’ll have to worry about with Effexor (or any medication that we’re aware of, actually), Effexor can potentially be responsible for some nasty sexual side effects for both men and women.
It’s helpful to understand both because it paints a better portrait of what’s going on down there.
In men, for instance, decreased sex drive, erectile dysfunction, delayed ejaculation or absent ejaculation can be recurring problems while on this medication.
Women can see similar side effects — decreased sex drive and decreased libido can occur, as can problems with delayed orgasm or not being able to orgasm at all.
Which could lead to a perfectly reasonable question: is this medication right for you?
Should You Avoid Effexor?
Many women struggle with orgasm issues. So, a medication that creates an increased risk of already-prevalent sexual problems is certainly something to be wary of when taking or beginning to take this antidepressant medication.
So, a medication that creates an increased risk of already-prevalent sexual problems is certainly something to be wary of when taking or beginning to take this antidepressant medication.
That said, as much as those sexual side effects of Effexor may be a no-go in your head, they do need to be put in context.
Research shows that venlafaxine causes a lower frequency of sexual dysfunction than older antidepressant types like TCAs, for instance.
One study found that venlafaxine actually tended to cause less sexual dysfunction than certain SSRIs in some patients, though more research is necessary to fully understand why.
Still, finding that up to 70 percent of patients using a different drug experienced side effects might rightly make you a little less wary of Effexor.
Furthermore, sexual functioning issues due to Effexor can be moderated in some cases with a reduced daily dose of the medication, or by taking break days from the medication (with the guidance of your healthcare provider, of course).
Avoiding Effexor, in the end, may be a decision not to risk sexual side effects instead of solving mental health symptoms.
Other Treatment Options: Alternatives to Effexor
Antidepressant-induced sexual dysfunction is generally manageable, but if your quality of life suffers from that or any side effect, it’s appropriate to talk to a healthcare provider about other treatment options.
How we treat depressive disorders has evolved greatly in the last few decades, and serotonin-norepinephrine reuptake inhibitors are just one of the tools available today.
A mental health professional might instead prescribe a selective serotonin reuptake inhibitor, or SSRI, which are considered generally well tolerated by the majority of the population.
Antidepressant treatment generally tends to cause sexual problems, and from tricyclic antidepressants to the Effexor XR version of the medication we’ve been talking about, treatment for psychiatric disorders is not without its additional complications.
And with all the talk about pills, it’s important to understand that therapy may also be an effective and necessary tool in dealing with mood disorders.
Cognitive behavioral therapy (CBT), for instance, can be helpful when you’re learning how to deal with negative and intrusive thoughts — something that medication alone can’t stop.
If you’re ready to talk now, consider online therapy with us.
Lifestyle changes — smoking and drinking cutbacks, better dietary habits, getting more exercise and being more socially active — can provide numerous benefits to everyone, but especially people dealing with mood disorders.
psych meds online
psychiatrist-backed care, all from your couch
Effexor and Sexual Health: The Next Steps
Sexual function is an important thing for most people, and when sexual dysfunction is listed as one of the common side effects of a medication, it can give anyone pause — understandably so.
If you’ve found yourself in that pause, take it as a sign that you should have this conversation with a healthcare professional.
Whether you’re worried about sexual side effects or already experiencing them, proper medical advice can help you understand the options, what’s possible, and what’s safe in your unique circumstances.
Have a conversation with a health care provider today so you can get back to living a depression-free, sex-filled life tomorrow.
6 Sources
Hims & Hers has strict sourcing guidelines to ensure our content is accurate and current. We rely on peer-reviewed studies, academic research institutions, and medical associations. We strive to use primary sources and refrain from using tertiary references.
- Singh D, Saadabadi A. Venlafaxine. Updated 2021 Oct 14. In: StatPearls Internet. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535363/.
- Ng, C. W., How, C. H., & Ng, Y. P. (2017). Managing depression in primary care. Singapore medical journal, 58(8), 459–466.
 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5563525/.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5563525/. - Craft, L. L., & Perna, F. M. (2004). The Benefits of Exercise for the Clinically Depressed. Primary care companion to the Journal of clinical psychiatry, 6(3), 104–111. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC474733/
- Kennedy, S. H., Eisfeld, B. S., Dickens, S. E., Bacchiochi, J. R., & Bagby, R. M. (2000). Antidepressant-induced sexual dysfunction during treatment with moclobemide, paroxetine, sertraline, and venlafaxine. The Journal of clinical psychiatry, 61(4), 276–281. https://pubmed.ncbi.nlm.nih.gov/10830148.
- Venlafaxine (Effexor). National Alliance on Mental Illness. (n.d.). https://www.nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Venlafaxine-(Effexor).
- U.S. National Library of Medicine. (n.d.). Venlafaxine: MedlinePlus Drug Information. MedlinePlus. https://medlineplus.gov/druginfo/meds/a694020.
 html.
html.
This article is for informational purposes only and does not constitute medical advice. The information contained herein is not a substitute for and should never be relied upon for professional medical advice. Always talk to your doctor about the risks and benefits of any treatment. Learn more about our editorial standards here.
Antidepressant-induced sexual dysfunction during treatment with moclobemide, paroxetine, sertraline, and venlafaxine
Save citation to file
Format: Summary (text)PubMedPMIDAbstract (text)CSV
Add to Collections
- Create a new collection
- Add to an existing collection
Name your collection:
Name must be less than 100 characters
Choose a collection:
Unable to load your collection due to an error
Please try again
Add to My Bibliography
- My Bibliography
Unable to load your delegates due to an error
Please try again
Your saved search
Name of saved search:
Search terms:
Test search terms
Email: (change)
Which day? The first SundayThe first MondayThe first TuesdayThe first WednesdayThe first ThursdayThe first FridayThe first SaturdayThe first dayThe first weekday
Which day? SundayMondayTuesdayWednesdayThursdayFridaySaturday
Report format: SummarySummary (text)AbstractAbstract (text)PubMed
Send at most: 1 item5 items10 items20 items50 items100 items200 items
Send even when there aren't any new results
Optional text in email:
Create a file for external citation management software
. 2000 Apr;61(4):276-81.
2000 Apr;61(4):276-81.
doi: 10.4088/jcp.v61n0406.
S H Kennedy 1 , B S Eisfeld, S E Dickens, J R Bacchiochi, R M Bagby
Affiliations
Affiliation
- 1 Department of Psychiatry, University of Toronto, Centre for Addiction and Mental Health, Ontario, Canada. [email protected]
- PMID: 10830148
- DOI: 10.4088/jcp.v61n0406
S H Kennedy et al. J Clin Psychiatry. 2000 Apr.
. 2000 Apr;61(4):276-81.
doi: 10.4088/jcp.v61n0406.
Authors
S H Kennedy 1 , B S Eisfeld, S E Dickens, J R Bacchiochi, R M Bagby
Affiliation
- 1 Department of Psychiatry, University of Toronto, Centre for Addiction and Mental Health, Ontario, Canada. [email protected]
- PMID: 10830148
- DOI: 10.4088/jcp.v61n0406
Abstract
Background: Recent reports suggest that adverse effects on sexual function occur in up to 50% of patients who are treated with selective serotonin reuptake inhibitor (SSRI) antidepressants. Previously cited low rates were more likely a function of underreporting than underoccurrence. There is less evidence about rates of dysfunction with serotonin-norepinephrine reuptake inhibitor (SNRI) and reversible inhibitor of monoamine oxidase A (RIMA) antidepressants. The purpose of this report is to evaluate disturbances in sexual drive/desire and arousal/orgasm in 107 patients who met criteria for major depressive disorder and received treatment with either moclobemide, paroxetine, sertraline, or venlafaxine.
Previously cited low rates were more likely a function of underreporting than underoccurrence. There is less evidence about rates of dysfunction with serotonin-norepinephrine reuptake inhibitor (SNRI) and reversible inhibitor of monoamine oxidase A (RIMA) antidepressants. The purpose of this report is to evaluate disturbances in sexual drive/desire and arousal/orgasm in 107 patients who met criteria for major depressive disorder and received treatment with either moclobemide, paroxetine, sertraline, or venlafaxine.
Method: All consenting eligible patients who met DSM-IV criteria for major depressive disorder completed the Sexual Functioning Questionnaire, version 1 (SFQ) and were assessed using the 17-item Hamilton Rating Scale for Depression (HAM-D) prior to and after 8 or 14 weeks of antidepressant therapy. Analyses were carried out to examine the effect of gender, drug type, pretreatment level of sexual dysfunction, and drug response on reported sexual dysfunction.
Results: Compared with women, men experienced a significantly greater level of drug-related impairment in drive/desire (p < .05), whereas there were no statistically significant differences in levels of arousal/orgasm impairment between men and women. The reported impairment in drive/desire items for men ranged from 38% to 50% and from 26% to 32% for women. No differences were found across the 4 antidepressants in men, whereas in women, rates of dysfunction were generally higher with sertraline and paroxetine, but only significantly so in comparison with moclobemide on some measures (p < .03). Rates of sexual dysfunction with venlafaxine tended to fall between those of SSRIs and the RIMA agent. An unexpected relationship was found between favorable drug response and a decreased level of drug-induced sexual dysfunction.
Conclusion: Antidepressant-induced sexual dysfunction occurs in approximately 30% to 70% of patients who are treated with sertraline or paroxetine. Lower rates are reported with moclobemide and venlafaxine. Clinicians should evaluate the various aspects of sexual dysfunction before and during antidepressant therapy.
Lower rates are reported with moclobemide and venlafaxine. Clinicians should evaluate the various aspects of sexual dysfunction before and during antidepressant therapy.
Similar articles
-
Comparison of moclobemide with selective serotonin reuptake inhibitors (SSRIs) on sexual function in depressed adults. The Australian and German Study Groups.
Philipp M, Tiller JW, Baier D, Kohnen R. Philipp M, et al. Eur Neuropsychopharmacol. 2000 Sep;10(5):305-14. doi: 10.1016/s0924-977x(00)00085-7. Eur Neuropsychopharmacol. 2000. PMID: 10974600 Clinical Trial.
-
Prevalence of sexual dysfunction among newer antidepressants.
Clayton AH, Pradko JF, Croft HA, Montano CB, Leadbetter RA, Bolden-Watson C, Bass KI, Donahue RM, Jamerson BD, Metz A.
 Clayton AH, et al. J Clin Psychiatry. 2002 Apr;63(4):357-66. doi: 10.4088/jcp.v63n0414. J Clin Psychiatry. 2002. PMID: 12000211
Clayton AH, et al. J Clin Psychiatry. 2002 Apr;63(4):357-66. doi: 10.4088/jcp.v63n0414. J Clin Psychiatry. 2002. PMID: 12000211 -
Antidepressant side effects in depression patients treated in a naturalistic setting: a study of bupropion, moclobemide, paroxetine, sertraline, and venlafaxine.
Vanderkooy JD, Kennedy SH, Bagby RM. Vanderkooy JD, et al. Can J Psychiatry. 2002 Mar;47(2):174-80. doi: 10.1177/070674370204700208. Can J Psychiatry. 2002. PMID: 11926080
-
SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients.
Montejo-González AL, Llorca G, Izquierdo JA, Ledesma A, Bousoño M, Calcedo A, Carrasco JL, Ciudad J, Daniel E, De la Gandara J, Derecho J, Franco M, Gomez MJ, Macias JA, Martin T, Perez V, Sanchez JM, Sanchez S, Vicens E.
 Montejo-González AL, et al. J Sex Marital Ther. 1997 Fall;23(3):176-94. doi: 10.1080/00926239708403923. J Sex Marital Ther. 1997. PMID: 9292833 Review.
Montejo-González AL, et al. J Sex Marital Ther. 1997 Fall;23(3):176-94. doi: 10.1080/00926239708403923. J Sex Marital Ther. 1997. PMID: 9292833 Review. -
Antidepressant-induced sexual dysfunction.
Gregorian RS, Golden KA, Bahce A, Goodman C, Kwong WJ, Khan ZM. Gregorian RS, et al. Ann Pharmacother. 2002 Oct;36(10):1577-89. doi: 10.1345/aph.1A195. Ann Pharmacother. 2002. PMID: 12243609 Review.
See all similar articles
Cited by
-
Sexual Dysfunction in Remitted Female Patients with Depression on SSRIs: Associated Factors and Relation to Marital Satisfaction and Quality of Life.
Penubarthi S, Kailash SZ, Sureshkumar K, Rajalakshmi AK. Penubarthi S, et al.
 Indian J Psychol Med. 2022 Sep;44(5):452-458. doi: 10.1177/02537176221111954. Epub 2022 Aug 11. Indian J Psychol Med. 2022. PMID: 36157018 Free PMC article.
Indian J Psychol Med. 2022 Sep;44(5):452-458. doi: 10.1177/02537176221111954. Epub 2022 Aug 11. Indian J Psychol Med. 2022. PMID: 36157018 Free PMC article. -
Lidocaine Ineffectiveness Suggests New Psychopharmacology Drug Target.
Mintz M, Badner V, Feldman LK, Mintz P, Saraghi M, Diaz J, Mezhebovsky I, Axelrod I, Gleeson J, Liu C, Smith C, Chow H, Zurakowski D, Segal MM. Mintz M, et al. Psychopharmacol Bull. 2022 Jun 27;52(3):20-30. Psychopharmacol Bull. 2022. PMID: 35815177 Clinical Trial.
-
The antidepressant drug vilazodone is an allosteric inhibitor of the serotonin transporter.
Plenge P, Yang D, Salomon K, Laursen L, Kalenderoglou IE, Newman AH, Gouaux E, Coleman JA, Loland CJ. Plenge P, et al.
 Nat Commun. 2021 Aug 20;12(1):5063. doi: 10.1038/s41467-021-25363-3. Nat Commun. 2021. PMID: 34417466 Free PMC article.
Nat Commun. 2021 Aug 20;12(1):5063. doi: 10.1038/s41467-021-25363-3. Nat Commun. 2021. PMID: 34417466 Free PMC article. -
Prevalence of antidepressant-induced sexual dysfunction among psychiatric outpatients attending a tertiary care hospital.
Al-Nimer MS, Al-Maqbali M. Al-Nimer MS, et al. Neurosciences (Riyadh). 2020 Jul;25(3):238-239. doi: 10.17712/nsj.2020.3.20200047. Neurosciences (Riyadh). 2020. PMID: 32683404 Free PMC article. No abstract available.
-
Selective Serotonin Reuptake Inhibitor-Induced Sexual Dysfunction: Current Management Perspectives.
Atmaca M. Atmaca M. Neuropsychiatr Dis Treat. 2020 Apr 20;16:1043-1050. doi: 10.2147/NDT.S185757. eCollection 2020. Neuropsychiatr Dis Treat.
 2020. PMID: 32368066 Free PMC article. Review.
2020. PMID: 32368066 Free PMC article. Review.
See all "Cited by" articles
Publication types
MeSH terms
Substances
Full text links
Physicians Postgraduate Press, Inc.
Cite
Format: AMA APA MLA NLM
Add to Collections
- Create a new collection
- Add to an existing collection
Name your collection:
Name must be less than 100 characters
Choose a collection:
Unable to load your collection due to an error
Please try again
Send To
Causes of erectile dysfunction - Health Clinic 365 Yekaterinburg
Erectile dysfunction, diagnosis and treatment expressiveness.
Age is not a direct risk factor for erectile dysfunction. Violation of potency at this age is primarily due to the development of diseases, such as cardiovascular and endocrine diseases, which contribute to the appearance of erectile dysfunction. Therefore, the identification and treatment of these diseases is often sufficient to restore potency.
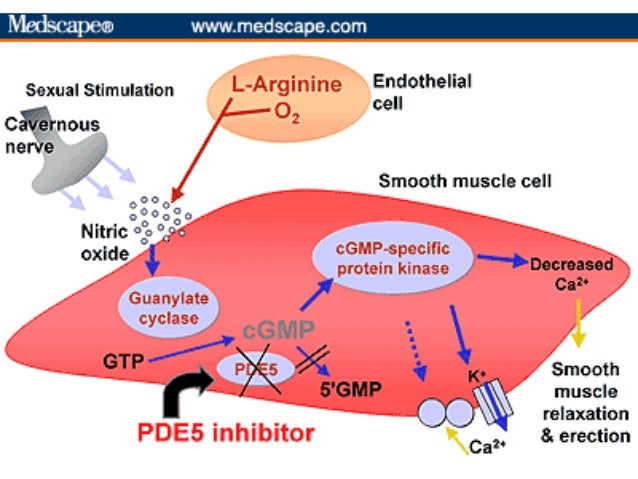
Male sexual arousal is a complex physiological process involving the brain, hormones, emotions, nerves, muscles and blood vessels, and disruption at any of these stages can lead to erectile dysfunction. In addition, stress and mental health problems can cause or worsen erectile dysfunction. In some cases, the cause of erectile dysfunction is a combination of physical and psychological problems. For example, minor physical problems that reduce your sexual response can cause anxiety about maintaining an erection. As a result, a feeling of anxiety can worsen potency.
What is an erection and erectile dysfunction? We often hear that the penis is a special muscle or nerve, but it is not. The penis is a closed hydraulic system (it's easier to say a balloon). The tight filling of this hydraulic system with blood (the creation of blood pressure inside this system of about 100 mm Hg) is an erection. To implement this phenomenon, two components are necessary - the influx of a large amount of blood and the ability of the penis to retain this blood flow during sexual arousal and sexual intercourse.
The penis is a closed hydraulic system (it's easier to say a balloon). The tight filling of this hydraulic system with blood (the creation of blood pressure inside this system of about 100 mm Hg) is an erection. To implement this phenomenon, two components are necessary - the influx of a large amount of blood and the ability of the penis to retain this blood flow during sexual arousal and sexual intercourse.
Blood flow is provided by the expansion of the arteries of the penis at the time of sexual arousal. The retention of blood in the penis is ensured by the complex interaction of the outlet veins, the tunica albuginea and the smooth muscles of the cavernous bodies, like the "nipple" system - "to let everyone in and not to let anyone out." The outflow of blood from the penis is carried out through special veins that penetrate from the inside of the cavernous bodies to the outside through the albuginea at a certain angle. Relaxation of the smooth muscles of the cavernous bodies during sexual arousal causes the expansion and expansion of the cavernous bodies, which leads to the pressing of these veins against the albuginea and blockade of the venous outflow of blood. Thus, the quality of erection depends on the quality of the vessels of the penis (i.e., on the ability of the vessels of the penis to adequately relax at the time of sexual arousal) and on the preservation of the structure of the cavernous bodies, which ensure effective retention of blood by squeezing the veins that penetrate the albuginea.
Thus, the quality of erection depends on the quality of the vessels of the penis (i.e., on the ability of the vessels of the penis to adequately relax at the time of sexual arousal) and on the preservation of the structure of the cavernous bodies, which ensure effective retention of blood by squeezing the veins that penetrate the albuginea.
Based on the above, the reasons for insufficient erection can be:
-
Violations of the erectile mechanism of the penis itself. For example, blockage of the arterial vessels of the penis leads to insufficient blood flow at the time of sexual arousal, and sclerosis of the muscles of the cavernous bodies makes the penis unable to expand and retain blood, i.e., a secondary "venous leak" is formed. The recognized causes of such breakdowns are diabetes mellitus, arterial hypertension, high blood cholesterol, obesity and smoking. In addition, there are often congenital breakdowns of the erectile mechanism, for example, "venous leakage" due to congenital pathologically dilated venous vessels;
-
Impact on the erectile mechanism of the penis pathology of other body systems, such as psycho-emotional, hormonal and nervous.
 A significant effect on the erection of other systems is rare. Consider some forms of such violations:
A significant effect on the erection of other systems is rare. Consider some forms of such violations:
- Psychogenic erectile dysfunction occupies a significant place in the structure of this disease. It should be noted that almost all patients with erectile dysfunction suffer from failure expectation neurosis, and in 40% it is the cause of its occurrence. The reasons for this are both in the peculiarities of the mental organization of a man, and in the influence of the society in which he lives.
- Hormonal erectile dysfunction (age-related deficiency of the male sex hormone). It is recognized that the tissue of the penis is a hormone-dependent tissue. The lack of the male sex hormone testosterone leads to an inadequate response of erectile tissue to sexual stimuli, withering of this tissue. Lack of testosterone is a significant cause of erectile dysfunction. Approximately 20% of men over the age of 50 experience symptoms of insufficiency of the male sex hormone testosterone, which means that erectile dysfunction is also possible.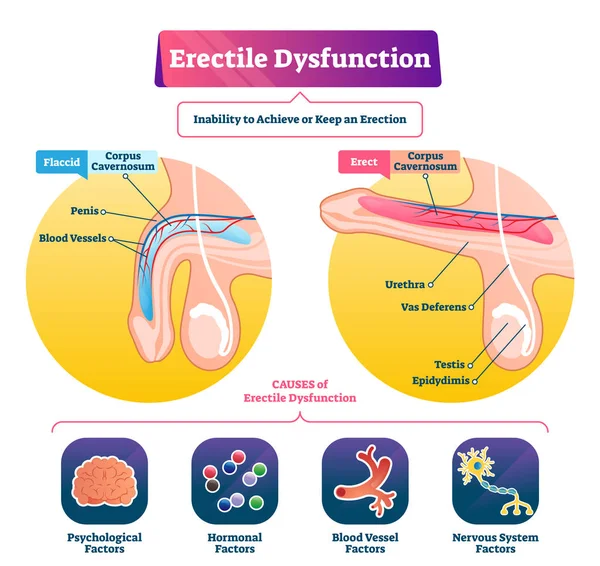
- Neurogenic erectile dysfunction is relatively rare. Mostly it affects people with spinal injury, with severe brain diseases, people suffering from diabetic, alcoholic or toxic neuropathy (dystrophy of nerves in tissues and organs).
So, in most cases, erectile dysfunction is caused by physical causes, including existing or undiagnosed diseases:
- heart disease
- atherosclerosis
- hypertension
- diabetes mellitus
- obesity
- metabolic syndrome
- Parkinson's disease
- multiple sclerosis
- low testosterone
- Peyronie's disease
- use of certain drugs
- smoking
- alcoholism and other substance abuse
- prostate cancer or prostate hyperplasia
- prostatitis
- surgeries or injuries that affect the pelvis or spinal cord.
Psychological Causes of Erectile Dysfunction
The brain plays a key role in triggering a number of physiological processes that cause an erection, starting with feelings of sexual arousal.
Some human conditions interfere with sexual feelings and cause a violation of potency. These include:
-
depression, anxiety or other mental illness
-
stress
-
fatigue
-
relationship problems due to stress, sex, or other problems
Prices
Andrologist - urologist, primary appointment
2100 i
Erectile dysfunction (impotence) - Naedine Medical Center
Term impotence in urological practice was replaced with erectile dysfunction for moral and ethical reasons and as a term that fully reflects the condition of a man with erectile dysfunction.
This is a disease (condition) in which erectile dysfunction occurs in men, leading to the absence or deterioration of sexual life, making it inferior and leading to psycho-emotional disorders and a decrease in the quality of life.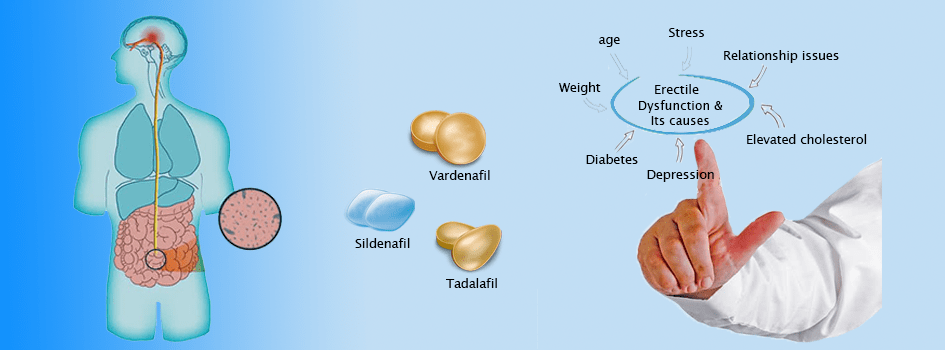 The issue of erectile dysfunction arises when there is an inability to achieve or maintain an erection sufficient for sexual intercourse. As a diagnosis, this disease is considered when the described violations are observed in more than half of the attempts to have sexual intercourse within six months and subject to regular sexual activity.
The issue of erectile dysfunction arises when there is an inability to achieve or maintain an erection sufficient for sexual intercourse. As a diagnosis, this disease is considered when the described violations are observed in more than half of the attempts to have sexual intercourse within six months and subject to regular sexual activity.
Risk factors for this pathology are cardiovascular diseases, diabetes mellitus, arterial hypertension, high blood cholesterol, radiation and chemotherapy, overweight, sedentary lifestyle, smoking, use of drugs and certain drugs and substances, somatic diseases and persons whose work is associated with high physical and psycho-emotional stress. Men with erectile dysfunction experience their condition prone to depression, irritability, withdrawal and anger.
Male erection depends on a number of mental, neurogenic, hormonal, vascular and anatomical factors. Accordingly, making a conclusion from the above, the causes of this disease can be the following:
1) Mental disorders and diseases:
Among the causes of psychogenic erectile dysfunction, there are strict upbringing, religious beliefs, fear of sexual life, sexual perversions (perversions), depression, fear of aging, physical disabilities, a certain sexual preference for a partner, a conflict with a partner, a negative first sexual experience in a man, the expectation of failure in contact with a partner, mental illness and some other conditions.
2) Neurogenic erectile dysfunction occurs as a result of damage to the central nervous system (brain and spinal cord) and or peripheral nerve structures. Tumors, epilepsy, strokes, Parkinson's disease, Alzheimer's disease, multiple sclerosis, cerebrovascular disease can lead to erectile dysfunction due to suppression of sexual desire (libido) or excessive inhibition of the spinal erection centers or impaired nerve conduction at the site of the lesion that is involved in the emergence and maintenance of an erection necessary for the implementation of a full-fledged sexual intercourse. With lesions of the structures of the spine and spinal cord, such as osteochondrosis and herniated disc, tumors, multiple sclerosis, the innervation of the penis may be disturbed, which also leads to erectile dysfunction.
3) Endocrine diseases are the most widespread and often detected in patients with erectile dysfunction. Patients with diabetes mellitus are most often treated. The cause of erectile dysfunction in this case is not so much the main endocrine disease as vascular problems and damage to peripheral nerves.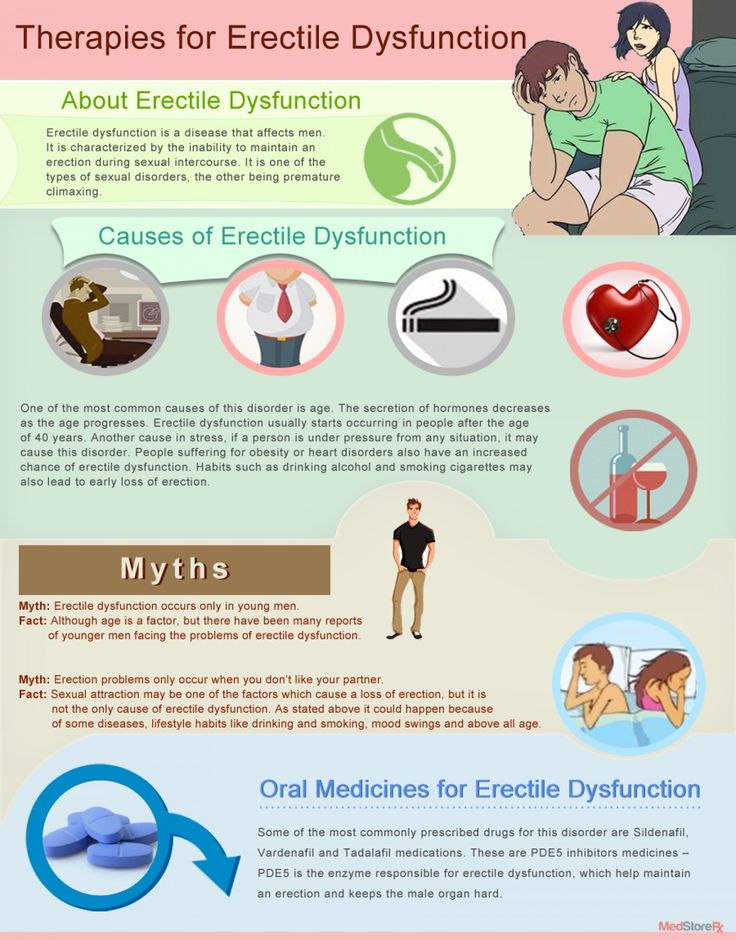 Tumors of the hypothalamus and pituitary gland can also lead to a decrease in sexual desire, a change in the level of hormones that are responsible for erection. In a certain percentage of cases, thyroid diseases directly and indirectly affect a man's ability to have sexual intercourse. Recently, a view on the problem of male aging has been relevant, because. with age, many of the physiological functions of a man fade, and many of this group of patients desire and have the opportunity to live a full sexual life. One of the first terms that appeared to describe age-related changes in men is the term "male menopause", which is currently used quite widely as a description of a set of symptoms that develop in a man after 45-50 years and manifested not only by a decrease in sexual desire, erection in including and morning and discontent in sexual life, but also depression, decreased attention and memory, increased nervousness, fatigue, decreased muscle strength, hot flashes and sweating, sleep disturbances and other symptoms.
Tumors of the hypothalamus and pituitary gland can also lead to a decrease in sexual desire, a change in the level of hormones that are responsible for erection. In a certain percentage of cases, thyroid diseases directly and indirectly affect a man's ability to have sexual intercourse. Recently, a view on the problem of male aging has been relevant, because. with age, many of the physiological functions of a man fade, and many of this group of patients desire and have the opportunity to live a full sexual life. One of the first terms that appeared to describe age-related changes in men is the term "male menopause", which is currently used quite widely as a description of a set of symptoms that develop in a man after 45-50 years and manifested not only by a decrease in sexual desire, erection in including and morning and discontent in sexual life, but also depression, decreased attention and memory, increased nervousness, fatigue, decreased muscle strength, hot flashes and sweating, sleep disturbances and other symptoms. But men do not have a clear age period for the decline in the production of sex hormones, unlike women. Therefore, the use of the term male menopause (from the Latin "climax" means step, ladder) is not correct, because. in men, this condition has a blurred and gradual onset, lasting for years, while in women it has a sharp and spasmodic course. Therefore, the term male menopause should be considered as age-related androgen deficiency. In the absence of contraindications, it is possible to prescribe testosterone replacement therapy to such patients to restore sexual function, erection and improve the quality of life.
But men do not have a clear age period for the decline in the production of sex hormones, unlike women. Therefore, the use of the term male menopause (from the Latin "climax" means step, ladder) is not correct, because. in men, this condition has a blurred and gradual onset, lasting for years, while in women it has a sharp and spasmodic course. Therefore, the term male menopause should be considered as age-related androgen deficiency. In the absence of contraindications, it is possible to prescribe testosterone replacement therapy to such patients to restore sexual function, erection and improve the quality of life.
4) The pathology of the arteries and veins of the small pelvis, the arteries and veins that supply the penis with blood can, to a certain extent, lead to insufficient blood supply to the cavernous bodies with the development of erectile dysfunction. Arterial pathology is most often caused by stenosis or atherosclerotic lesions of the arterial wall, resulting in reduced blood perfusion through the cavernous bodies of the penis with the development of erectile insufficiency.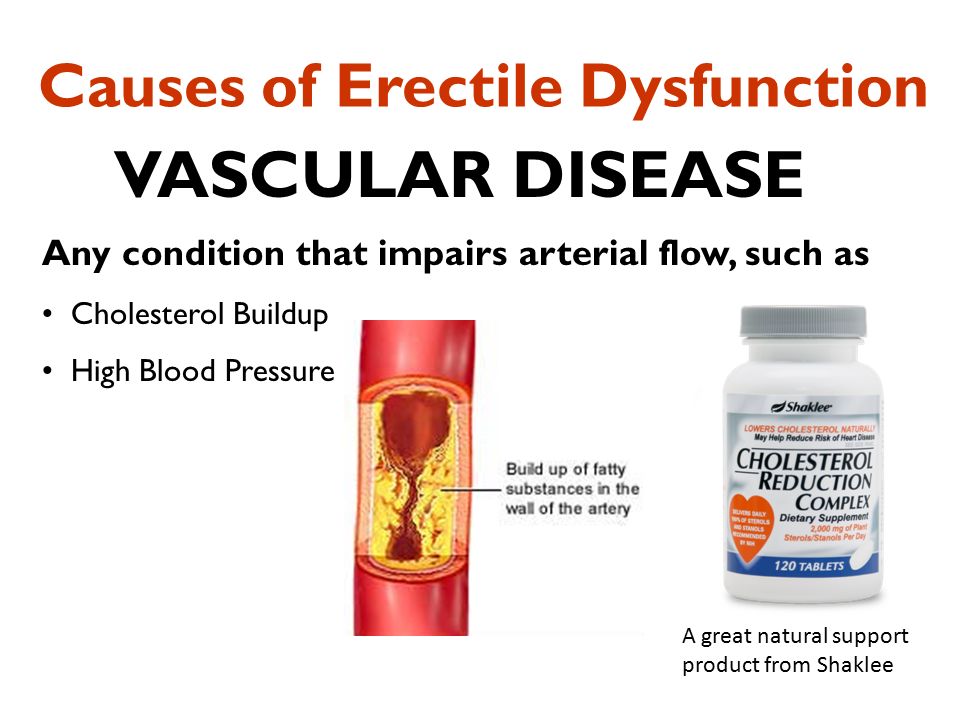 Patients with arterial insufficiency most often note an incomplete erection and difficulty in maintaining it. With pathological venous outflow, patients also note the weakness and rapid disappearance of an erection soon after its onset.
Patients with arterial insufficiency most often note an incomplete erection and difficulty in maintaining it. With pathological venous outflow, patients also note the weakness and rapid disappearance of an erection soon after its onset.
5) Sometimes drugs that are recommended to the patient for another disease can lead to erectile insufficiency. This occurs most often in patients taking sleeping pills, sedatives, antidepressants, hormones and anabolic steroids, blood pressure lowering drugs (diuretics, beta-blockers, ACE inhibitors and Ca-channels) and other drugs. Therefore, such patients need to correct prescriptions by canceling or replacing drugs together with the therapist or cardiologist (if, for example, erectile dysfunction is caused by taking antihypertensive drugs).
In the differential diagnosis of sexual dysfunction, a detailed sexual history of the patient, as well as a thorough laboratory and visual examination, play an important role. Considering that there are many causes of erectile dysfunction, patients are required to prescribe:
-
general analysis of blood and urine,
-
determination of fasting glucose levels,
-
creatinine,
-
urea,
-
testosterone,
-
prolactin and other hormones as needed.