Dissociative identity disorder intimate relationships
The Intimacy Factor and Dissociative Identity Disorder
Intimacy can be such a tabooed and feared topic, especially for those of us with dissociative identity disorder (DID) who have been subjected to years of prolonged abuse and unwanted touch. The very idea of intimacy denotes something very private, closely personal, and not prone to discussion. However, if true healing is to be obtained, those with dissociative identity disorder must discuss concerns of intimacy, closeness, and vulnerability in order to help heal and to have his or her needs met in their relationships.
With that being said, work around intimacy in dissociative identity disorder is difficult and complicated. It is beyond the scope of this post to discuss all aspects of intimacy. Seeking the guidance of a qualified mental health professional to guide you in your healing process is strongly recommended.
What Is Intimacy?
The dictionary defines intimacy as an expression of affection, a loving personal relationship with another, and an amourously familiar act, including, but not limited to, sexual intercourse.
(In fact, there are four types of intimacy. For an even deeper appreciation of what they are and how they can help create intimacy between you and your partner, watch my video below as I discuss the pathway to connectedness.)
In my relationship with my husband, intimacy pertains to a deep, personal connection that fosters feelings of comfort, safety, and security. Without feeling safe and secure in my relationship, intimacy could not be achieved.
Perhaps you agree with these explanations on intimacy or maybe you have a different idea of what intimacy is. Regardless of our personal interpretations, the question we are left with is how do we foster intimacy that will lead to us feeling connected with another while being safe at the same time.
What Helps Foster Intimacy?
For those of us with dissociative identity disorder, most have learned from an early age that touch was unsafe and dangerous, so it might feel more natural for us at the moment to be fearful and to shy away from being vulnerable.
First of all, be gentle with yourself and your expectations. Start with what is easy. One such way is to develop a level of trust and communication. Discussing your relationship with your partner and what the two of you need from each other is a great first step in fostering intimacy. Ths beginning dialogue will help you feel safe, loved, and accepted when expressing your feelings, your needs, your desires, and your wants. Without this basic level of communication, it will be difficult to move forward to a more intimate, and possibly sexual, level in your relationship.
Examples of Intimacy
To start with, intimacy is when you know and trust your partner, For example, intimacy will begin to develop when you both rely on each other to navigate the hardships and good times, when you are responsive to each other's needs, and when you make a permanent commitment to each other.
For me and my husband, communication and understanding have always been key in establishing feelings of safety and in nourishing my desire to be with him. Intimacy for us can be something as gentle as the comfort of holding each other's hand, softly snuggling with each other on the couch, or even laughing at each other's silly jokes.
Intimacy for us can be something as gentle as the comfort of holding each other's hand, softly snuggling with each other on the couch, or even laughing at each other's silly jokes.
What about you and your partner? When was the last time the two of you hugged, danced, or even playfully tickled each other? These are just a few ways to foster and express intimacy toward each other.
Respect Your Partner's Feelings
With that being said, for a long time, I was not comfortable with my husband initiating any form of intimacy with me. Because of the abuse of my past, it was difficult to hold hands or cuddle with him. However, if I wanted to express my love to my husband, I would have to open that door. And while he knew and understood the reasons for my inability to be loving and affectionate in return, there were times he could not help but feel rejected.
When I began writing this post, I asked my husband how he felt when I was not able to reciprocate intimacy. He says:
"I love you, and I understand why you cannot always engage with me, but sometimes I feel rejected.
I would never hurt you, and it makes me feel like one of your abusers when you cannot connect with me. I have in my mind how I want to treat you and make you feel, but things don't always work out that way, and I feel disappointed that I cannot share certain moments with you."
I understand my husband's feelings of discontentment. Even though we with dissociative identity disorder are the ones who have suffered and endured years of abuse, our partners are still allowed to have a reaction when intimacy is not a possibility for us at that moment. Just as I did with my husband, you might need to remind your partner not to take your reaction personally, and reassure your partner he or she did nothing wrong.
Words of Caution
Since lack of intimacy by one partner can cause hurt feelings, it would be appropriate to set up expectations at the beginning of your relationship as to what you will allow. Establish safe boundaries so that your partner will be knowledgable of what you can and cannot do.
But be confident in this: there is no expiration date on intimacy in a relationship. If things are not feeling safe, take a step back and work from the beginning on reestablishing trust and communication. Continue discussing what your needs are. Intimacy is achievable and possible for those with dissociative identity disorder. I wish you a long, safe, and fulfilling intimate relationship with your partner.
APA Reference
Hargis, B. (2019, July 31). The Intimacy Factor and Dissociative Identity Disorder, HealthyPlace. Retrieved on 2022, October 17 from https://www.healthyplace.com/blogs/dissociativeliving/2019/7/the-intimacy-factor-and-dissociative-identity-disorder
Supporting a Spouse With Dissociative Identity Disorder through Treatment and Beyond – BrightQuest Treatment Centers
March 8, 2019, Mary Ellen EllisBrightQuest Treatment Centers
Dissociative identity disorder is a serious condition triggered by trauma that causes the formation of several distinct personalities in one individual. If you have a spouse with this condition, the best way to support them is with professional treatment in a residential facility. Facing the trauma and learning to live with this condition and manage and control the identities requires intensive therapy. Loved ones can help by learning how to support the patient during and after treatment.
If you have a spouse with this condition, the best way to support them is with professional treatment in a residential facility. Facing the trauma and learning to live with this condition and manage and control the identities requires intensive therapy. Loved ones can help by learning how to support the patient during and after treatment.
Dissociative identity disorder is a severe mental illness that causes major disruptions in a person’s life. If your spouse has more than one distinct personality and struggles to function normally because of them, they may be diagnosed with this condition.
What your partner needs from you is support. Ensure they get diagnosed and the necessary, intensive treatment. Therapy in a residential setting is the best way to face the trauma that underlies multiple personalities and to reconsolidate all those identities back into the one person you care about. Learn how to support your spouse through treatment and aftercare.
What Is Dissociative Identity Disorder?
Dissociative identity disorder, or DID, belongs to a class of mental illnesses known as dissociative disorders. These are very serious, highly disruptive conditions that cause a person to become detached from reality in some way. They impact memory, behaviors, perception of oneself and the rest of the world, identity, and emotions.
These are very serious, highly disruptive conditions that cause a person to become detached from reality in some way. They impact memory, behaviors, perception of oneself and the rest of the world, identity, and emotions.
Someone with DID develops and lives with one or more alternative personalities—these are often referred to as alters—and identities in addition to the original, or core, personality. These individual identities may or may not be aware of the others, but when one is in control it can be very different from the others or from the person’s true personality. DID is more often diagnosed in women, but it is still very rare.
The diagnostic symptoms of DID include:
- Having two or more separate and distinct personalities and identities that cause changes in thoughts and behaviors and are obvious to other people
- Memory gap caused by switching between alters
- Significant distress or impairment that is caused by having these different identities
DID and other dissociative conditions are almost always caused by trauma. With DID, a common cause is abuse. If your spouse is struggling with DID, they may be using it to cope with the experience of past trauma and as a defense mechanism against difficult memories. But not consciously. By facing traumatic memories and experiences, your spouse can overcome this damaging condition.
With DID, a common cause is abuse. If your spouse is struggling with DID, they may be using it to cope with the experience of past trauma and as a defense mechanism against difficult memories. But not consciously. By facing traumatic memories and experiences, your spouse can overcome this damaging condition.
How DID Is Treated
As the partner of someone who dissociates and lives as more than one person, life can often feel out of control. You may try to help your husband or wife come back to their own personality or take steps you think will resolve this situation. But the first and most important thing you need to know about DID is that there is nothing you can do personally or at home to heal your spouse.
Once you understand how powerless you are over the condition, instead of giving into despair, realize that you must get your spouse into professional treatment. This is what you can do, along with continuing to support them going through the process. Because DID causes so much functional impairment and intense symptoms, it’s usually necessary for patients to stay in residential facilities for treatment.
The main type of treatment is psychotherapy focused on trauma. This can include trauma-focused cognitive behavioral therapy, dialectical behavior therapy (DBT), eye movement desensitization and reprocessing therapy (EMDR), and others.
Because trauma is the cause of the condition, it is essential to uncover these terrible experiences and face and process the memories in a safe and healing way. The best way to do this is in residential care. It may be hard to let your spouse go for a few months, but it is important for recovery from DID.
Be Available for Your Spouse During Treatment
During residential treatment for DID, your spouse will be facing challenging, difficult memories. Therapy for this condition is the best care, but it isn’t easy. Your spouse will be asked to recall painful traumatic experiences, to talk about them, and to feel all the emotions they trigger.
For some patients, it may be best for loved ones to stay away for a period of time. To best support your spouse during treatment, stay in communication with the professionals in charge of their care. Find out what they need from you. If getting involved and attending some family or couples sessions is helpful or recommended, be available to do that.
To best support your spouse during treatment, stay in communication with the professionals in charge of their care. Find out what they need from you. If getting involved and attending some family or couples sessions is helpful or recommended, be available to do that.
It can be frustrating to be unable to something more active to help someone you love, but sometimes they need to heal without your presence. In the meantime, you can still support your spouse by learning more about DID and trauma. Many facilities offer family psychoeducation programs for loved ones. These educate family members about what the patient is experiencing and how best to support them when they return home.
Begin Your Recovery Journey Today.
619-466-0547Supporting a Spouse with Dissociative Identity Disorder after Treatment
Be patient as your spouse with dissociative identity disorder goes through what can be a lengthy treatment process. This is a complicated mental illness, and depending on the extent of the trauma and the severity of symptoms, it could take several months to heal and be ready to come home. With good treatment, it is possible for someone with DID to manage and minimize alternative identities and to live a normal life again. Here are some things to keep in mind to provide the best support for your loved one after residential care:
With good treatment, it is possible for someone with DID to manage and minimize alternative identities and to live a normal life again. Here are some things to keep in mind to provide the best support for your loved one after residential care:
- Encourage ongoing therapy. Most mental illnesses are not simply cured. They are chronic diseases that can recur in times of stress. To help your spouse maintain good mental health, encourage them to stay in regular therapy.
- Be patient. Identities that came under control in therapy may resurface. Be patient and help your spouse use the strategies they learned in treatment to regain control.
- Don’t play games with the identities. There is no way you can reason your spouse out of an alternative identity. Doing so can make the situation worse. Instead, be honest at all times.
- Try to understand triggers. One thing your spouse will learn in therapy is what things tend to trigger changes in personality.
 Make sure you know what these triggers are and help your spouse be more aware and careful about recognizing them.
Make sure you know what these triggers are and help your spouse be more aware and careful about recognizing them. - Practice good mental hygiene together. Your spouse will have learned some healthy coping strategies in therapy. For instance, if stress triggers their shifts in personality, it’s helpful to have things like meditation or exercise to mitigate stress. Engage in these practices with your spouse to encourage them and help you both.
- Help with memory gaps. You know that your spouse may still have gaps in memory if personalities recur. If they seem confused at times, help them out by backing up and explaining anything they may have missed.
The Need for Self-Care
Living with and loving someone with multiple identities that can appear at any time is stressful and sometimes frightening. It can stir up difficult emotions, like sadness, hopelessness, anxiety, and even anger and resentment. You need care, too, for dealing with this challenging illness.
Few people understand what you are going through, and unlike your spouse, you are not getting months of specialized care. Consider joining a support group for loved ones of people with DID. You may not be able to find one near you, but there are plenty of online groups to give you a chance to connect with others. There also may be more general groups for family members you can join through your spouse’s treatment facility.
Realize that there is no shame and no reason why you shouldn’t get some time away from your spouse occasionally. Taking a little time for yourself is not selfish. In fact, it helps your spouse, because it allows you to maintain good mental health so you can continue to be supportive. Consider taking a few hours here and there, or even a day or two, if you have someone whom you both trust and can be there for your spouse if needed.
Dissociative identity disorder may never truly go away, but by getting your spouse the professional care they need and supporting them during and after treatment you can both heal and learn to manage and live with it.
If you’re concerned about a loved one and believe they may need residential care, we can help. BrightQuest offers long-term treatment for people struggling with complex mental health illnesses and co-occurring disorders. Contact us to learn more about our renowned program and how we can help you or your loved one start the journey toward recovery.
Personality disorder and its treatment: what are the features of manifestations? Schizoid Personality Disorder, Borderline Personality Disorder, Dissociative Personality Disorders
Personality disorders are characterized by a number of characteristic symptoms - this disease has many varieties, and the signs in each case will differ. Narcissistic disorder is characterized by the patient's absolute confidence in his exclusivity, while bipolar disorder is characterized by a change in two opposite phases of mood: mania and depressive disorder. Treatment is prescribed taking into account the results of studies and the individual characteristics of patients.
Submit an application for diagnosis and treatment
I confirm that I accept the terms of consent to the processing of personal data.
Personality disorders can have different manifestations and symptoms - in particular, with bipolar disorder, a person's behavior can change dramatically, while with a schizoid type, a person becomes indifferent to everything and longs for loneliness. Treatment is carried out both medically and psychotherapeutically. Pharmacological therapy is prescribed to relieve acute symptoms, psychotherapeutic correction is carried out to change self-awareness and to teach the patient to control a mental disorder. Group therapy has also been shown to be beneficial for personality disorders.
Personality disorder and its treatment: what are the features of manifestations?
Personality disorder diagnosis
Personality disorder is a collective concept that combines a list of mental disorders. Various stable violations in the commission of actions, thoughts, in the manifestation of feelings - all this is a personality disorder. Symptoms for each type of disease are somewhat different, which requires a separate analysis for each type of disorder.
Various stable violations in the commission of actions, thoughts, in the manifestation of feelings - all this is a personality disorder. Symptoms for each type of disease are somewhat different, which requires a separate analysis for each type of disorder.
Organic Personality Disorders
Organic personality disorders can cause a variety of illnesses, including head trauma, brain tumors, vascular disease, and many others. But more often, epileptic seizures lead to such disorders. According to statistics, the probability of developing organic disorders in people who have been suffering from epileptic seizures for more than ten years is at least 5-10%. Such disorders are characterized by the following symptoms: 1. The presence of strong mood swings, starting with euphoria and ending with complete apathy. 2. The presence of Paranoid ideas (mildly expressed). 3. Changes in sexual behavior. 4. The appearance of difficulties in the process of purposeful activity. 5. The presence of complete anti-sociality. 6. Manifestations of excessive verbosity, the desire to express one's thoughts in an ornate way, or, conversely, manifestations of stupidity, psychological viscosity. Symptoms may develop gradually over six months. Over the past period of time, the patient goes through several stages from mild irritation and some kind of psychological viscosity to a complete organic personality disorder.
5. The presence of complete anti-sociality. 6. Manifestations of excessive verbosity, the desire to express one's thoughts in an ornate way, or, conversely, manifestations of stupidity, psychological viscosity. Symptoms may develop gradually over six months. Over the past period of time, the patient goes through several stages from mild irritation and some kind of psychological viscosity to a complete organic personality disorder.
Dissociative personality disorders
The presented type of psychological disorders indicates that two or more people can get along in the patient. Each of them (the so-called "alter personalities") have their own character, manifestations of their views on the world and ways of interconnection with the surrounding reality. Such diseases are included in the international classification of diseases, and yet, a number of experts question their existence. However, the human brain is a very complex thing, therefore, it is not worth denying a split personality. Here are the symptoms characteristic of this disease: 1. the presence of short-term or long-term amnesia. In some cases, patients forget even very important facts and events that have occurred, for example, the date of their birth, wedding, childbirth. 2. the patient can often lie, although he is sure that he told the whole truth. 3. The patient may not remember how he met someone. Sometimes he may deny that he knew people with whom he had previously had close communication. 4. documents may suddenly appear that are absolutely exactly signed by the patient, however, the calligraphy of the handwriting looks alien. 5. There may be a feeling of derealization in the patient. 6. sometimes the patient may find himself in some places and will not be able to understand how he happened to get here (we are talking about gaps in time). 7. In the patient's personal belongings, items that may not be known can often appear. 8. Various unfamiliar people may call the patient a false name. 9. the patient can hear other people's voices in his head.
Here are the symptoms characteristic of this disease: 1. the presence of short-term or long-term amnesia. In some cases, patients forget even very important facts and events that have occurred, for example, the date of their birth, wedding, childbirth. 2. the patient can often lie, although he is sure that he told the whole truth. 3. The patient may not remember how he met someone. Sometimes he may deny that he knew people with whom he had previously had close communication. 4. documents may suddenly appear that are absolutely exactly signed by the patient, however, the calligraphy of the handwriting looks alien. 5. There may be a feeling of derealization in the patient. 6. sometimes the patient may find himself in some places and will not be able to understand how he happened to get here (we are talking about gaps in time). 7. In the patient's personal belongings, items that may not be known can often appear. 8. Various unfamiliar people may call the patient a false name. 9. the patient can hear other people's voices in his head. 10. as a result, the patient realizes that he is more than one person. In the process of diagnosis, it is imperative to consider whether the patient is taking any substances. Their exposure can cause temporary personality disorders.
10. as a result, the patient realizes that he is more than one person. In the process of diagnosis, it is imperative to consider whether the patient is taking any substances. Their exposure can cause temporary personality disorders.
Borderline Personality Disorder
Borderline Personality Disorder is a very common disorder, it is believed that about 2% of all people on earth are affected in one way or another. It is characterized by characteristic symptoms: 1. A person may be afraid to be alone. The need to stay with yourself can cause quite violent reactions, which can manifest as panic attacks, anger, or even the development of a depressive disorder. 2. Patients cannot adequately evaluate themselves. They often drastically change their minds about certain things, rebuild their plans for the future. 3. Patients often threaten to commit suicide and even suicidal attempts may be made. In addition, patients often engage in self-harm. 4. Patients with this diagnosis are bored virtually all the time. 5. From time to time, patients lose touch with reality. 6. The patient usually has quite difficult and strained relationships with family members and friends. At times there can be a strong rapprochement, but their rejection can immediately begin. 7. Sometimes patients commit very risky acts: they engage in unprotected sex, exceed the speed limit, use drugs. 8. All emotions that patients feel are exaggerated. Usually, all such outbursts of emotionality can last for several hours or several days. 9. It is not uncommon for people with borderline disorder to experience intense, uncontrollable anger. It is necessary to know that such mental personality disorders rarely occur in absolutely healthy families. They usually affect people whose close relatives have a history of the same or other types of personality disorders.
5. From time to time, patients lose touch with reality. 6. The patient usually has quite difficult and strained relationships with family members and friends. At times there can be a strong rapprochement, but their rejection can immediately begin. 7. Sometimes patients commit very risky acts: they engage in unprotected sex, exceed the speed limit, use drugs. 8. All emotions that patients feel are exaggerated. Usually, all such outbursts of emotionality can last for several hours or several days. 9. It is not uncommon for people with borderline disorder to experience intense, uncontrollable anger. It is necessary to know that such mental personality disorders rarely occur in absolutely healthy families. They usually affect people whose close relatives have a history of the same or other types of personality disorders.
Schizoid personality disorder
Schizoid personality disorder is a fairly common disorder. It can be caused by both physiological factors (for example, disorders in the endocrine system or cerebral insufficiency) and psychological factors (difficult childhood, low self-esteem). Symptoms of schizoid disorder: 1. The patient is unable to express his feelings. He is cold and aloof. 2. The patient does not react to any external influences, whether it be praise or criticism, and shows indifference in everything. 3. A patient with such a diagnosis has practically no need for communication. He does not regret making connections, neither friendly nor sexual. 4. The main need of such a person is solitude. Modern medicine has learned to control this disorder. Patients can gradually adapt to the world, make friends, even if they are not very close. Moreover, patients can even achieve significant success in work if it is not related to communication and communication. However, if the disease is left to chance, the patient's condition will worsen, this can lead to some complications. The most common types of complications are alcoholism and drug addiction. Over time, the patient is more and more difficult to treat, as he does not make contact with the attending physician.
Symptoms of schizoid disorder: 1. The patient is unable to express his feelings. He is cold and aloof. 2. The patient does not react to any external influences, whether it be praise or criticism, and shows indifference in everything. 3. A patient with such a diagnosis has practically no need for communication. He does not regret making connections, neither friendly nor sexual. 4. The main need of such a person is solitude. Modern medicine has learned to control this disorder. Patients can gradually adapt to the world, make friends, even if they are not very close. Moreover, patients can even achieve significant success in work if it is not related to communication and communication. However, if the disease is left to chance, the patient's condition will worsen, this can lead to some complications. The most common types of complications are alcoholism and drug addiction. Over time, the patient is more and more difficult to treat, as he does not make contact with the attending physician.
Narcissistic personality disorder
Considering the types of personality disorder, one cannot but pay attention to a very special type - narcissistic disorder. The fact that a person suffers from this disease is indicated by the presence of five or more of the following signs: 1. The patient greatly exaggerates his sense of self-importance. He overestimates his achievements and talents, loves to be recognized as a leader. 2. The patient constantly fantasizes. Fantasies can be about anything, whether it's brilliant business success, ideal love or untold wealth. 3. A person with this diagnosis constantly feels the need to be admired. 4. The patient shamelessly uses other people for his own purposes. 5. He very often feels a strong envy of others. 6. The patient is convinced that he is unique and exceptional, and only other equally unique people can appreciate these advantages. 7. The patient is absolutely sure that he has special rights. 8. The patient is unable to empathize with other people. He is completely devoid of empathy. 9. Man loves to show arrogance. In society, he constantly behaves arrogantly.
The patient is unable to empathize with other people. He is completely devoid of empathy. 9. Man loves to show arrogance. In society, he constantly behaves arrogantly.
Emotional personality disorder
Children who were raised with a lack of attention, or those who had a cruel and domineering father, sometimes grow into people with an emotional personality disorder. The symptoms of this disease are as follows: 1. The patient is very irritable, easily excitable, he has a so-called "explosive" character. 2. On the part of the patient, they characterize him as an evil and vindictive person. 3. The patient cannot adequately assess this or that current situation, this is due to his inability to be reasonable. 4. The patient likes to dramatize everything. He perceives the most banal everyday things with tragedy. 5. A person with this disorder is not able to normally perceive criticism, as well as calmly participate in disputes.
Bipolar personality disorder
Bipolar disorder is characterized by two stages in a person's life: mania and depression. These stages flow from one to another. Statistics say that the risk of getting this disease during the life of each person is approximately one percent. Symptom of the stage of mania:
These stages flow from one to another. Statistics say that the risk of getting this disease during the life of each person is approximately one percent. Symptom of the stage of mania:
- § Hyperactivity, increased energy.
- § Euphoria, slight excitability.
- § Disorder in thoughts and speech (the patient constantly jumps from one idea to another).
- § Extravagance.
- § Increased sexual activity.
- § Insomnia and lack of need for sleep.
- § Addiction to insomnia pills, alcohol and even cocaine.
- § Very aggressive and provocative behavior.
- § Easy distractibility (it is extremely difficult for the patient to concentrate on anything).
- § Complete denial of the problem and unwillingness to be treated.
- Symptoms of depression stage:
- § Sadness, emptiness and anxiety.
- § Profound pessimism.
- § Feelings of guilt before others.
- § Lethargy, lethargy, fatigue.
- § Loss of interest in almost everything, including favorite hobbies and sexual relationships.
- § Drowsiness.
- § Abrupt weight gain or loss.
- § Feeling unwell, including chronic pain.
- § Constant suicidal thoughts, suicidal thoughts.
Episodes of mania and depression alternate throughout the patient's life. However, sometimes between them there are periods of normal health, but even at these moments the patient may feel the residual effects of the disease.
Personality disorder: treatment
The treatment of a particular type of personality disorder is a very complex process. It cannot be cured like a fracture or a cold - once and for all. With this disease, a person has to fight throughout his life. In general, treatment consists of two parts: drug treatment and psychotherapeutic. Medicines are used to relieve symptoms that torment the patient, such as severe anxiety, fear, depression. In addition, there are a number of drugs that relieve outbursts of anger in situations where the patient becomes literally dangerous to others. Psychiatry is used to correct negative character traits. Some traits correct fairly quickly, while others take years to correct. Roughly speaking, behavior changes occur during the first year of treatment, but personality change takes much longer. The type and method of psychotherapy is chosen depending on the type of disorder, but, in any case, the participation of family members in the procedures has a very positive effect on the recovery process. In addition, sometimes doctors use group therapy methods very successfully. It is very important that the attending physician always stays in touch and, in case of emergency, can conduct a treatment session by phone.
In addition, there are a number of drugs that relieve outbursts of anger in situations where the patient becomes literally dangerous to others. Psychiatry is used to correct negative character traits. Some traits correct fairly quickly, while others take years to correct. Roughly speaking, behavior changes occur during the first year of treatment, but personality change takes much longer. The type and method of psychotherapy is chosen depending on the type of disorder, but, in any case, the participation of family members in the procedures has a very positive effect on the recovery process. In addition, sometimes doctors use group therapy methods very successfully. It is very important that the attending physician always stays in touch and, in case of emergency, can conduct a treatment session by phone.
Types of subpersonalities — Knife
Subpersonalities live in each of us, although outwardly we seem to be something monolithic.
Clients usually don't understand the concept of subpersonalities the first time around and say, "No, I only have one 'I'. " I agree with this, though with a caveat: “But there are many versions of it. And my task is to introduce you to them."
" I agree with this, though with a caveat: “But there are many versions of it. And my task is to introduce you to them."
When parts of our "I" change places, one of them comes to the fore, correcting our views and attitudes. Role reversal happens naturally in different circles, places, and circumstances, but as we spend most of our lives on autopilot, we usually don't notice it.
One of your subpersonalities, for example, goes to work and performs official duties. If you think about it, you will notice that at work you feel and behave in a special way. In valuable workers who are praised and rewarded for their work, this part of the personality is very self-confident. Probably, under the control of this part of your "I", you even move differently than in situations related to your private life. Now compare this part of yourself with the one you present to your family. The difference is very noticeable.
My client Mark, after listening to this, said:
— Wow! It seems you are right.
 My family part at work would not have survived at all, and my family part would not have tolerated the work part.
My family part at work would not have survived at all, and my family part would not have tolerated the work part. Mark worked for a Wall Street financial company in a highly competitive environment. In order to survive in such a job, he had to find a subpersonality capable of this. He himself described it as follows: "He does not take prisoners, he has no right to make mistakes and weakness." Realizing for the first time that he had subpersonalities, he laughed:
- Wow, I never thought that I was actually two different people. Colleagues have no idea how plush I am at home with my wife and children.
The idea of subpersonalities disgusts and frightens many people. Some clients think that I am hinting at dissociative identity disorder, but there is nothing in common between it and subpersonalities. Dissociative identity disorder is a mental illness that occurs after physical, emotional or sexual abuse in childhood. Patients also have subpersonalities, but, in addition, they have problems with perception and there is a so-called dissociative amnesia. Such people lose track of time and do not remember what happened to them on a scale incomparable with simple forgetfulness.
Such people lose track of time and do not remember what happened to them on a scale incomparable with simple forgetfulness.
There is an opinion that subpersonalities are not really parts of the "I", but only mood indicators. However, throughout the long history of the development of psychological science, many theorists have successfully applied the concept of subpersonalities to explain the human mental structure. Freud's id, self, and superego, or Jung's complexes, illustrated how the mind processes experiences. Jung described the mind not as a single entity, but as an organism composed of independently acting subpersonalities. Gestalt therapy, transactional analysis, and cognitive behavioral therapy use similar schemas to describe internal processes. The famous psychologist Virginia Satir said that within each individual there is a "private party". Of recent developments, it is worth mentioning Richard Schwartz's model of the inner family.
In it, parts of the "I" are considered as components of a certain system - the inner family. Whatever one may say, we are made up of parts, both old-school specialists and modern researchers agree with this. My task is not to teach you the basics of psychology, but to explain how parts of your personality are arranged and how they affect interaction with a partner.
Whatever one may say, we are made up of parts, both old-school specialists and modern researchers agree with this. My task is not to teach you the basics of psychology, but to explain how parts of your personality are arranged and how they affect interaction with a partner.
Let's take a look at them. You not only go to work and stay at home, you also have other social contacts.
When you feel good, who are you at this time - an introvert or an extrovert? What side do you present in the course of disagreements? Do you fence off and run away or dig in and attack? What part of your personality do you show more often in relationships? Openness, love and compassion - or alienation?
Modern mass culture imposes a rainbow image of love, but everyone who has ever loved knows that it is far from reality. When you love, you open up completely. Love can gut a person and stop him from bleeding, which will require him to awaken all his subpersonalities.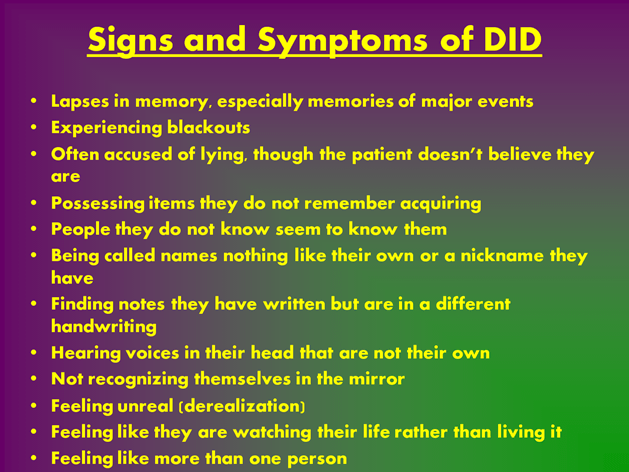 Brené Brown, in The Great Dare, writes about how fragile we feel when we open up to another person: “I define vulnerability as uncertainty, risk, and emotional openness. Let's look at love from this point of view. Waking up every day with a feeling of love for someone in whose reciprocal love and reliability we are not sure who can stay or leave without warning, remain faithful all my life or betray tomorrow - this is vulnerability. In love, you know nothing in advance. This is a huge risk. When we love, we are subject to emotions. Yes, it’s scary, yes, we will probably be hurt later, but is it possible to imagine your life without loving and being loved?”
Brené Brown, in The Great Dare, writes about how fragile we feel when we open up to another person: “I define vulnerability as uncertainty, risk, and emotional openness. Let's look at love from this point of view. Waking up every day with a feeling of love for someone in whose reciprocal love and reliability we are not sure who can stay or leave without warning, remain faithful all my life or betray tomorrow - this is vulnerability. In love, you know nothing in advance. This is a huge risk. When we love, we are subject to emotions. Yes, it’s scary, yes, we will probably be hurt later, but is it possible to imagine your life without loving and being loved?”
Yeah, after such a passage, try not to imagine. The universe has a clearly cynical and twisted sense of humor. You see, love, like nothing else, exposes not only our adult subpersonalities, but also deep old wounds. At the same time, everyone wants to love and be healed of childhood traumas. We are looking for love that we understand, most often the kind that we received from our parents. It doesn't matter what we've experienced - a good relationship or a bad one, attachment or alienation, tenderness or toxicity - the main thing is that it's already familiar. The subconscious desire to be healed leads us to transfer our childhood traumas into romantic relationships.
It doesn't matter what we've experienced - a good relationship or a bad one, attachment or alienation, tenderness or toxicity - the main thing is that it's already familiar. The subconscious desire to be healed leads us to transfer our childhood traumas into romantic relationships.
In response to this, the protective parts of our personality are activated. It is this process that is hidden behind the outer side of problems in a couple. Inside each of us sits the Offended Child, who is desperately protected by other subpersonalities. Let's look at parts of our "I" separately, their tasks and motivations. This is the Offended Child, Protector and Inner Critic.
Offended Child
We are born naked and defenseless and ask, “Am I safe? I am loved? Am I important? Am I good enough?" In early childhood, we ask these questions non-verbally, and as adults, unconsciously, addressing them to parents, relatives and the immediate environment. Answers to them give us the meaning of existence and understanding of our place in the world.
If even one of these questions remains unanswered, there is an inner pain. When this happens time after time, it hurts us. As a result, a subpersonality appears, called the Inner, or Offended, Child.
Offended Child is one or more subpersonalities of a person who have not grown up and continue to suffer. These parts of our "I" are forever stuck in the past and doomed to an endless experience of traumatic experience. When the Offended Child comes to the fore, we feel helpless, we are overwhelmed by emotions.
Even before I started studying to be a psychotherapist, one morning, balancing between sleep and reality, I suddenly came into contact with my Abused Child. I saw how I, seven years old, was sitting in the front seat of the school bus, next to the driver, and my mother was standing on the steps. I can only see her top, but I can hear her voice well. The rest of the children listen in silence. Usually, parents weren't allowed on the bus, and even less often was anyone talking to the driver, Mrs. Johnson, in a raised voice. But that's exactly what my mom did.
Johnson, in a raised voice. But that's exactly what my mom did.
- He will sit in front, with peers, and not in the back with hooligans. They bully him, I won't stand it! If something does not suit you, please contact me, but do not dare to put him back. They are twice as old and behave inappropriately, he is still small," my mother said.
The doors closed, mother remained at the bus stop. Silence reigned in the bus. Mrs. Johnson barked at me:
- March back! - and everyone hooted and cackled. I did not obey, and at her signal, one of her henchmen dragged me by the collar to an empty seat.
“What a weakling,” I muttered in my twenties half asleep. I recalled this incident more than once and always came to the same conclusion. A wave of shame rolled over me, and I thought what misery I was.
The offended Child within us keeps shameful secrets. Regardless of whether we were severely offended or not, when we felt unloved or threatened, seemed to ourselves not good enough or unnecessary, we did not blame our parents for this, but considered ourselves flawed. And now we are ashamed of it. John Bradshaw, in The Shame That Binds You, summed up the Inner Child experience perfectly: “Shame masks hidden secrets and makes us believe we are defective. We feel so terrible that we ourselves are disgusted to look at it, let alone show it to others.
And now we are ashamed of it. John Bradshaw, in The Shame That Binds You, summed up the Inner Child experience perfectly: “Shame masks hidden secrets and makes us believe we are defective. We feel so terrible that we ourselves are disgusted to look at it, let alone show it to others.
Adults do not consider themselves children because they do not want to be weak, helpless and defenseless. But the Offended Child inside us is like an old wound that periodically hurts in bad weather. To some extent, we get used to discomfort. The pain is somewhere nearby, but it is hidden from prying eyes until you stumble upon it. Suppose at the age of six one of the parents stopped paying attention to you or disappeared altogether.
Because of this, your six-year-old subpersonality will always feel abandoned and horrified at the mere thought that a partner can leave or betray. When this part takes over, there is a feeling of defenselessness. Communication with a partner begins to seem fragile and insecure, annoyance appears that your partner may be less interested in a relationship than you. The offended Child warns of potential danger and signals that it is time to take protective measures. Usually we shut ourselves off from the feelings of the Offended Child, and we consider the Protector or Inner Critic to be part of ourselves. Unfortunately, protective measures prevent us from loving, thinking and listening. We shove the Inner Child far away, and he suffers in the dark depths of the subconscious. A traumatic childhood experience is repeated over and over and left unprocessed and unhealed.
The offended Child warns of potential danger and signals that it is time to take protective measures. Usually we shut ourselves off from the feelings of the Offended Child, and we consider the Protector or Inner Critic to be part of ourselves. Unfortunately, protective measures prevent us from loving, thinking and listening. We shove the Inner Child far away, and he suffers in the dark depths of the subconscious. A traumatic childhood experience is repeated over and over and left unprocessed and unhealed.
Liz and John's sexual problems are an example of the Inner Child coming to the fore.
John, an adult, shrunk down to the size of a little boy during a consultation in anticipation of punishment. Liz said so. I think this is not the first time that John reincarnated as a traumatized young version of himself.
John's mother often scolded him and sometimes physically punished him. She lashed out at the kids every day, and as a psychologist, I guess she had borderline personality disorder. John said that she didn’t scream for a reason, but simply if he didn’t come across at the right time, so he tried to be quieter than water below the grass and please her in everything. If the storm could not be prevented, he would shrink and wait for it to pass. He began to avoid conflict at all costs, especially in relations with women. Now childhood trauma has shown itself in his marriage.
John said that she didn’t scream for a reason, but simply if he didn’t come across at the right time, so he tried to be quieter than water below the grass and please her in everything. If the storm could not be prevented, he would shrink and wait for it to pass. He began to avoid conflict at all costs, especially in relations with women. Now childhood trauma has shown itself in his marriage.
A long-standing fear of disappointing the mother, no matter how hard she tried, crept into her and Liz's bedroom. When his wife was offended or angry at the lack of sex, John followed the usual strategy: shrink, freeze and wait for it to be over. Liz's anger awakened in John not only the Offended Child, but also a pleasing subpersonality that helped him avoid suffering. Unfortunately, all this did not help satisfy the wife in bed.
For John, the answer to the question "Am I safe?" never been positive. This led to relationship problems and confrontation between the resentful and protective parts of Liz and John.
Defender
The offended Child has been shaped by childhood trauma, and the Defender's goal is to prevent him from being hurt again. In the process of growing up, we learn self-defense by cultivating the corresponding subpersonalities in ourselves.
The defenders are waiting for the signal from the Offended Child. They realized that some fundamental needs were never satisfied, and their main task and the only purpose of existence is to protect the Offended Child. Defenders act like big brothers we didn't have. When the outside world or our surroundings pose a danger to us, they come out and say, “Stop! Don't you dare offend the Child!" A protector can set boundaries, say no, and help us get out of an unpleasant or risky situation.
Whatever the danger, the Protectors, like bodyguards, shield the Child with themselves. They perform an important task, but their uncontrolled guardianship does not allow us to form close ties.
In the case of Liz and John, the Protectors of both interfere with mutual understanding and greatly complicate the solution of sexual problems. At the consultation, John's Advocate unsuccessfully tried to calm down and not provoke Liz. The more he tried to please her, the more angry she became. John was inadvertently broadcasting to her that her feelings didn't matter, and it blew up her childhood trauma.
At the consultation, John's Advocate unsuccessfully tried to calm down and not provoke Liz. The more he tried to please her, the more angry she became. John was inadvertently broadcasting to her that her feelings didn't matter, and it blew up her childhood trauma.
See also
Hero with a thousand faces. How does a whole family of subpersonalities coexist in each of us?
Liz's parents did not encourage displays of affection. When her emotionality went beyond the unspoken norm, her parents pretended that nothing was happening. Instead of showing interest in the child's living mind and her ability to challenge the unknown, her parents ignored her, ordered her to be quiet, punished her and did not talk to her. Liz learned that no one wanted her feelings. In response to the systematic traumatic treatment, the Offended Child appeared inside Liz. Later, when she matured and became independent, she formed a Protector. He fought for her everywhere, including in his relationship with John.