Difference between positive and negative symptoms in schizophrenia
Symptoms - Schizophrenia - NHS
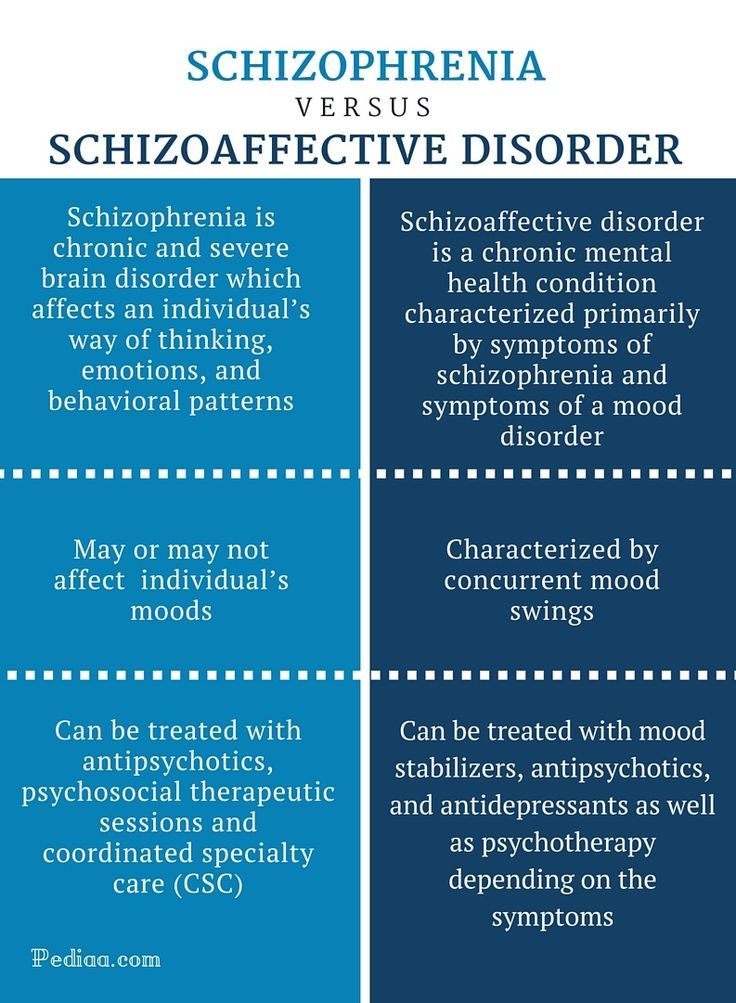
Schizophrenia changes how a person thinks and behaves.
The condition may develop slowly. The first signs can be hard to identify as they often develop during the teenage years.
Symptoms such as becoming socially withdrawn and unresponsive or changes in sleeping patterns can be mistaken for an adolescent "phase".
People often have episodes of schizophrenia, during which their symptoms are particularly severe, followed by periods where they experience few or no symptoms. This is known as acute schizophrenia.
Positive and negative symptoms
The symptoms of schizophrenia are usually classified into:
- positive symptoms – any change in behaviour or thoughts, such as hallucinations or delusions
- negative symptoms – where people appear to withdraw from the world around then, take no interest in everyday social interactions, and often appear emotionless and flat
Hallucinations
Hallucinations are where someone sees, hears, smells, tastes or feels things that do not exist outside their mind. The most common hallucination is hearing voices.
Hallucinations are very real to the person experiencing them, even though people around them cannot hear the voices or experience the sensations.
Research using brain-scanning equipment shows changes in the speech area in the brains of people with schizophrenia when they hear voices. These studies show the experience of hearing voices as a real one, as if the brain mistakes thoughts for real voices.
Some people describe the voices they hear as friendly and pleasant, but more often they're rude, critical, abusive or annoying.
The voices might describe activities taking place, discuss the hearer's thoughts and behaviour, give instructions, or talk directly to the person. Voices may come from different places or 1 place, such as the television.
Delusions
A delusion is a belief held with complete conviction, even though it's based on a mistaken, strange or unrealistic view. It may affect the way the person behaves. Delusions can begin suddenly or may develop over weeks or months.
Delusions can begin suddenly or may develop over weeks or months.
Some people develop a delusional idea to explain a hallucination they're having. For example, if they have heard voices describing their actions, they may have a delusion that someone is monitoring their actions.
Someone experiencing a paranoid delusion may believe they're being harassed or persecuted. They may believe they're being chased, followed, watched, plotted against or poisoned, often by a family member or friend.
Some people who experience delusions find different meanings in everyday events or occurrences.
They may believe people on TV or in newspaper articles are communicating messages to them alone, or that there are hidden messages in the colours of cars passing on the street.
Confused thoughts (thought disorder)
People experiencing psychosis often have trouble keeping track of their thoughts and conversations.
Some people find it hard to concentrate and will drift from one idea to another.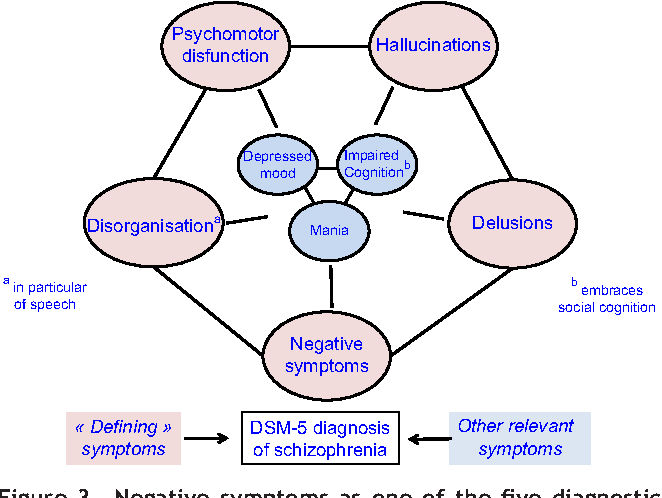 They may have trouble reading newspaper articles or watching a TV programme.
They may have trouble reading newspaper articles or watching a TV programme.
People sometimes describe their thoughts as "misty" or "hazy" when this is happening to them. Thoughts and speech may become jumbled or confused, making conversation difficult and hard for other people to understand.
Changes in behaviour and thoughts
A person's behaviour may become more disorganised and unpredictable.
Some people describe their thoughts as being controlled by someone else, that their thoughts are not their own, or that thoughts have been planted in their mind by someone else.
Another feeling is that thoughts are disappearing, as though someone is removing them from their mind.
Some people feel their body is being taken over and someone else is directing their movements and actions.
Negative symptoms of schizophrenia
The negative symptoms of schizophrenia can often appear several years before somebody experiences their first acute schizophrenic episode.
These initial negative symptoms are often referred to as the prodromal period of schizophrenia.
Symptoms during the prodromal period usually appear gradually and slowly get worse.
They include the person becoming more socially withdrawn and increasingly not caring about their appearance and personal hygiene.
It can be difficult to tell whether the symptoms are part of the development of schizophrenia or caused by something else.
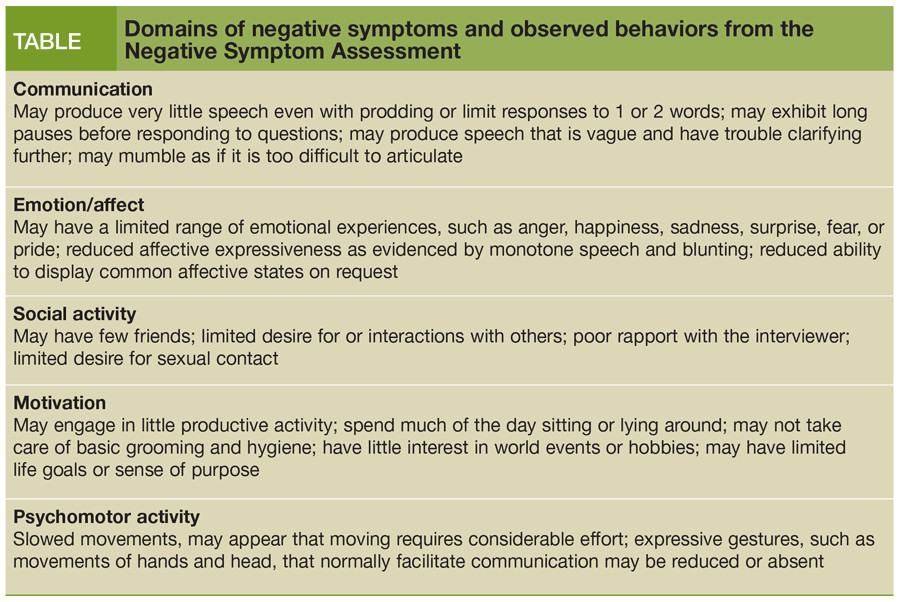
Negative symptoms experienced by people living with schizophrenia include:
- losing interest and motivation in life and activities, including relationships and sex
- lack of concentration, not wanting to leave the house, and changes in sleeping patterns
- being less likely to initiate conversations and feeling uncomfortable with people, or feeling there's nothing to say
The negative symptoms of schizophrenia can often lead to relationship problems with friends and family as they can sometimes be mistaken for deliberate laziness or rudeness.
Psychosis
Schizophrenia is often described by doctors as a type of psychosis.
A first acute episode of psychosis can be very difficult to cope with, both for the person who is ill and for their family and friends.
Drastic changes in behaviour may occur, and the person can become upset, anxious, confused, angry or suspicious of those around them.
They may not think they need help, and it can be hard to persuade them to visit a doctor.
Read more about understanding psychotic experiences.
Difference Between Positive and Negative Symptoms of Schizophrenia
Tanya J. Peterson
Among schizophrenia’s many types of symptoms—cognitive, neurological, behavioral, and emotional—are categories known as positive symptoms of schizophrenia and negative symptoms of schizophrenia. Most schizophrenia symptoms in the DSM-5 fall into these two categories, and it’s the positive symptoms and negative symptoms that are the defining features of the mental illness we call schizophrenia.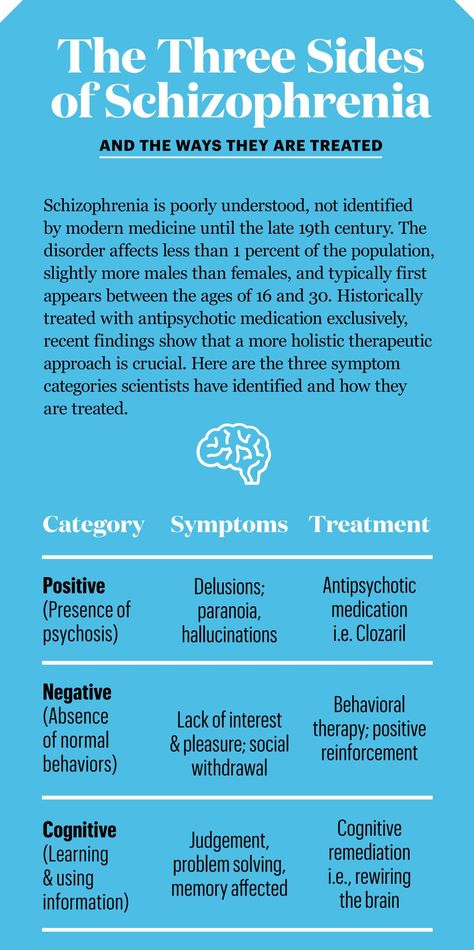
Schizophrenia is an illness of the brain with a whole constellation of characteristics. The symptoms represent a range of experiences someone living with this serious mental illness can face. Everyone will possess some combination of symptoms, but no one has all of them (Are Schizophrenia Symptoms in Males and Females Different?).
By definition, schizophrenia involves having some positive symptoms and some negative symptoms. The positive and the negative symptoms exist together and comprise this serious mental illness.
Positive and Negative Symptoms of Schizophrenia Can Be Confusing
The terms “positive” and “negative” can be misleading. They sound like judgments, as if the positive symptoms are good and the negative symptoms are bad. This isn’t the case, however. “Positive” symptoms refer to characteristics that are added to someone’s state of being. “Negative” symptoms, in contrast, are characteristics that are removed from the person’s state of being.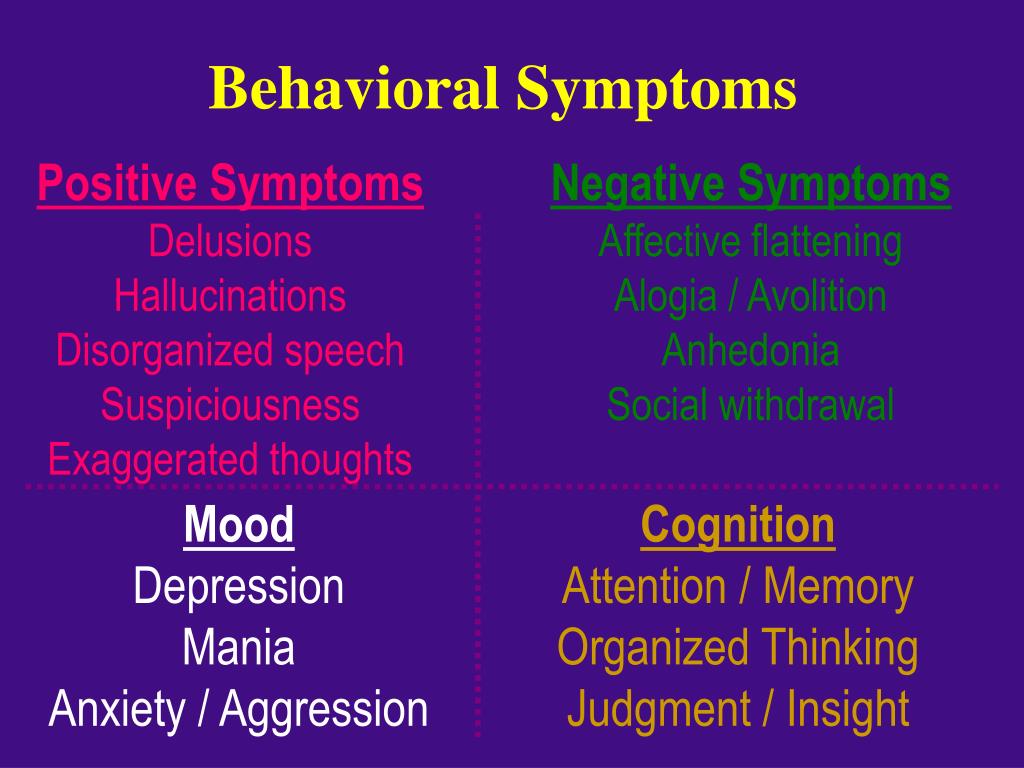
The difference between positive and negative symptoms of schizophrenia is what they do to the person who is living with schizophrenia. Both types of symptoms impact the way he interacts with the world around him and within him. Schizophrenia positive symptoms create distortions and new ways of experiencing the world, while schizophrenia negative symptoms take things away.
Schizophrenia Positive Symptoms
The positive symptoms of schizophrenia involve hallucinations, delusions, disorganized speech, and disorganized or catatonic behavior.
- Hallucinations add things to sensory perceptions. Someone with schizophrenia might see, hear, feel, smell, or taste things that aren’t real.
- Delusions add distortions to someone’s thoughts. She will think and believe things that aren’t logical or real.
- Disorganized speech means that someone’s speech is difficult to follow or understand. He might get off track during a conversation or respond in ways that don’t make sense.
 Processes added to what usually happens in the brain cause this disorganization and difficulty in communication.
Processes added to what usually happens in the brain cause this disorganization and difficulty in communication. - Disorganized behavior can be erratic, inappropriate, or bizarre. Patterns of interacting with the world are added to her “normal” patterns of interaction.
- Catatonic behavior is withdrawn, can involve unusual positioning of the body, sitting in silence, staring at nothing. As with disorganized behavior, a different behavior pattern has been added to the person’s way of being in the world.
Schizophrenia Negative Symptoms
The negative symptoms of schizophrenia diminish the brain’s ability to process certain experiences and to respond or behave in particular ways. This can lead to:
- Flat affect, where someone can’t show emotion and even the ability to smile is taken away
- Decreased motivation and goal-driven behavior
- Inability to make and pursue goals
- Slowed reaction to other people, events, and happenings
- Diminished speech (instead of disorganized, it is barely there; known as alosia)
- Loss of ability to fully care about people or events (apathy)
- Loss of ability to feel pleasure or happiness (anhedonia)
Someone with schizophrenia experiences some combination of both positive and negative symptoms.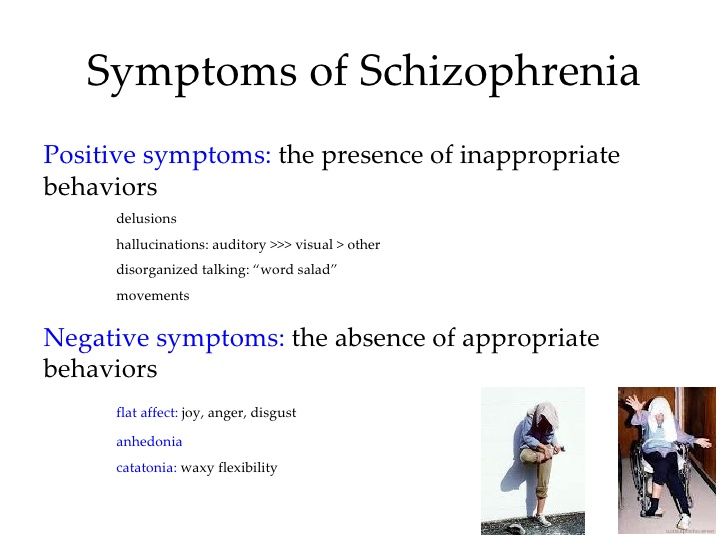 Whether they’re positive symptoms of schizophrenia, adding unwanted and unnecessary experiences and characteristics to the person or are negative symptoms of schizophrenia, removing desirable features, these symptoms greatly disrupt someone’s life, how he experiences it, and how he lives it.
Whether they’re positive symptoms of schizophrenia, adding unwanted and unnecessary experiences and characteristics to the person or are negative symptoms of schizophrenia, removing desirable features, these symptoms greatly disrupt someone’s life, how he experiences it, and how he lives it.
APA Reference
Peterson, T. (2018, March 28). Difference Between Positive and Negative Symptoms of Schizophrenia, HealthyPlace. Retrieved on 2023, February 3 from https://www.healthyplace.com/thought-disorders/schizophrenia-symptoms/difference-between-positive-and-negative-symptoms-of-schizophrenia
Last Updated: April 7, 2018
Medically reviewed by Harry Croft, MD
More Info
Schizophrenia Risk Factors: What Ups the Risk of Schizophrenia?
Schizoaffective Disorder and Hearing Voices
Coping With Psychosis: Some Thoughts From a Psychologist With Paranoid Schizophrenia
Someone You Know is Mentally Ill
Alternative Treatments for Schizoaffective Disorder
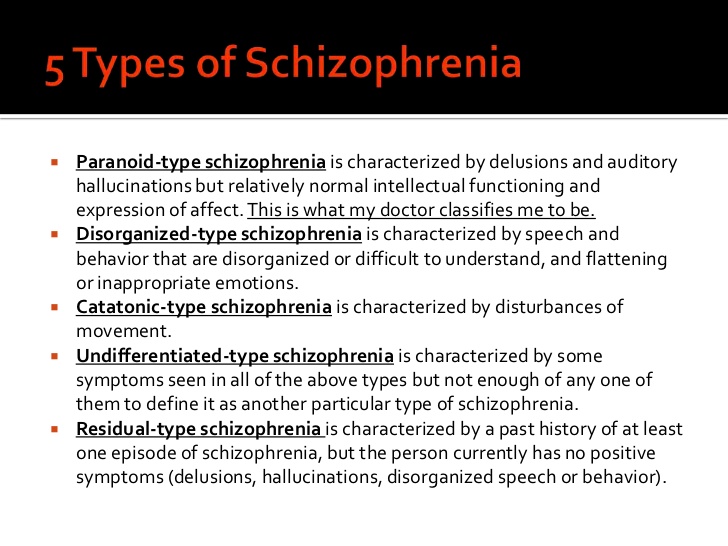
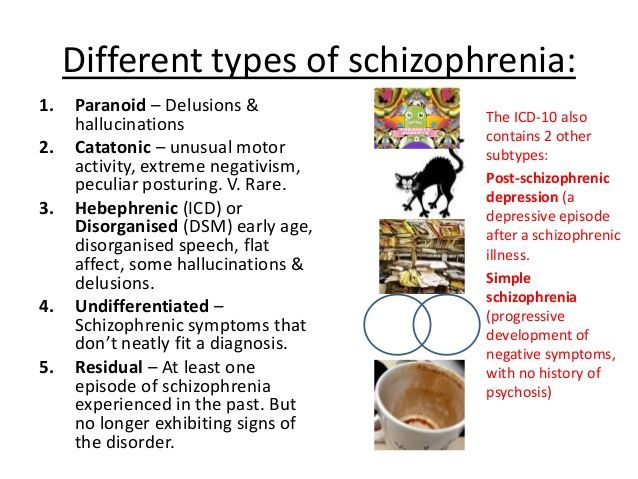
Types of Schizophrenia
Schizophrenia Facts, Schizophrenia Statistics
Negative symptoms: detailed information
- Negative symptoms are the main symptom complex of schizophrenia spectrum disorders.
 It leads to social maladjustment, the prerequisites for the formation of which are a violation of the motivational, cognitive, emotional sphere.
It leads to social maladjustment, the prerequisites for the formation of which are a violation of the motivational, cognitive, emotional sphere. - Although patients may appear sad, withdrawn, and immersed in anxiety, the negative symptoms of schizophrenia are not the same as symptoms of depression. On the contrary, they are symptoms that occur regardless of the presence or absence of depressive manifestations, positive symptoms, cognitive impairment and behavioral disorganization.
- Five conditions are considered to be the key manifestations of the negative symptoms of schizophrenia: flattened affect, alogia, anhedonia, asociality and abulia. These conditions are grouped depending on the leading type of disorders: symptoms associated with a decrease in expression (blunted affect, alogia), symptoms caused by a violation of motivation and the inability to enjoy pleasure (anhedonia, asociality, abulia).
In this section
Main symptom complex of schizophrenia
Negative symptoms - symptoms of a violation of the patient's usual daily functioning.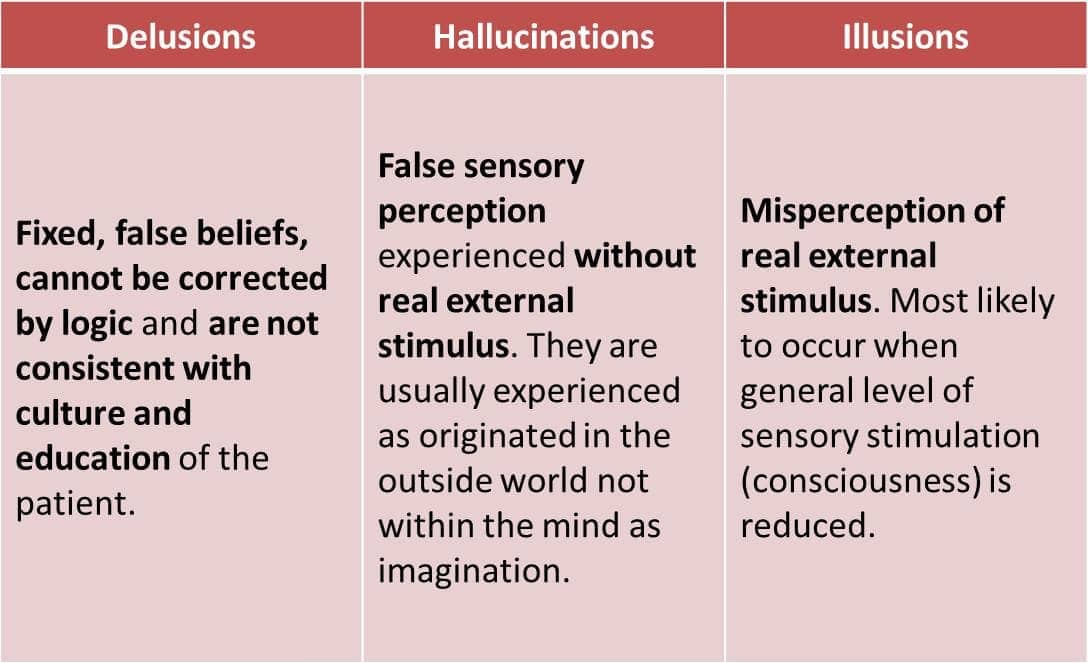 They arise against the background of changes in the motivational and emotional sphere, which leads to schizophrenia.
They arise against the background of changes in the motivational and emotional sphere, which leads to schizophrenia.
At the moment, there is no common understanding of the etiology and pathophysiology of the appearance of negative and positive symptoms of schizophrenia. Research has also shown that negative symptoms of schizophrenia can occur independently of positive, cognitive symptoms, depression, or disorganization 1.2 .
Negative symptoms are associated with low motivation, flattening of affect, impaired social and interpersonal interaction 3 .
Negative symptoms are recognized as a key manifestation of schizophrenia. Eugen Bleuler (1857-1939) was the first to speak about them. In a 1950 edition of his work, the negative symptoms are described as:
“Indifference to everything—friends and relatives, work or pleasure, duties or rights, good or bad luck…
The face (of the patient) is inexpressive, the posture is stooped. An image of indifference…
An image of indifference…
the ability to work, to serve oneself is reduced…
Such people lose their desire to do something on their own initiative or at the direction of others” 4 .
It is important to note that negative symptoms can be difficult to recognize, especially if they are mild. But they should not be confused with sadness or just a bad mood 5.6 .
Five key negative symptoms of schizophrenia (5 "A")
Flattened affect alogia, anhedonia, asociality, abulia - five key negative symptoms of schizophrenia 7 .
The ability to express emotions
(noticeable to others)
Acted affect - This is a decrease in the expressiveness of verbal and non -verbal communications (monotony of speech, inexpressiveness of facial expressions and troops).
Studies of vocal expression showed that in patients with schizophrenia, compared with healthy volunteers, there was a violation of tonality, speed, volume, and modulation of speech. Changes were recorded both during spontaneous and arbitrary speech.
Changes were recorded both during spontaneous and arbitrary speech.
Non-verbal behavior of patients with schizophrenia is smoothed out, becomes inexpressive, not aimed at communication. These manifestations complicate the process of the patient's interaction with society, since it is expressive facial expressions, gestures, postures that are an important component of interpersonal communication 7 .
Alogia - poverty of speech, a decrease in the number of words used during a conversation, a violation of the spontaneity of speech.
Alogia revealed during clinical interview. Estimated spontaneity of speech, sentence structure. Patients are characterized by a violation of spontaneity, short answers, lack of need to independently reveal the topic of conversation.
A meta-analysis of studies showed that patients, unlike healthy people, speak with large pauses, build short sentences, their speech is not smooth.
At the same time, the scarcity of speech, the need to use a large number of words, use long sentences that do not carry a semantic load, does not belong to the concept of alogia 7 .
Reduced motivation and ability to enjoy (what the patient feels)
Asociality - lack of need for interpersonal contacts, communication.
The patient has no desire, no strength to initiate or maintain communication with others.
This state should be distinguished from the limitations of social interaction associated with positive symptoms: delusions, hallucinations. The patient may refuse to communicate because of a bad mood, fear of harming others, due to the appearance of suspicion, fears characteristic of a delusional episode.
Also, the patient may be in forced social isolation, and simply not be able to communicate with people. This is not equivalent to asociality 7 .
Anhedonia , that is, a decrease in the ability to enjoy, experience positive emotions.
Traditionally regarded as a core feature of both depression and schizophrenia.
The anhedonia component can be divided into two components:
Reduced ability to experience pleasure during potentially pleasurable activities - consummatory anhedonia.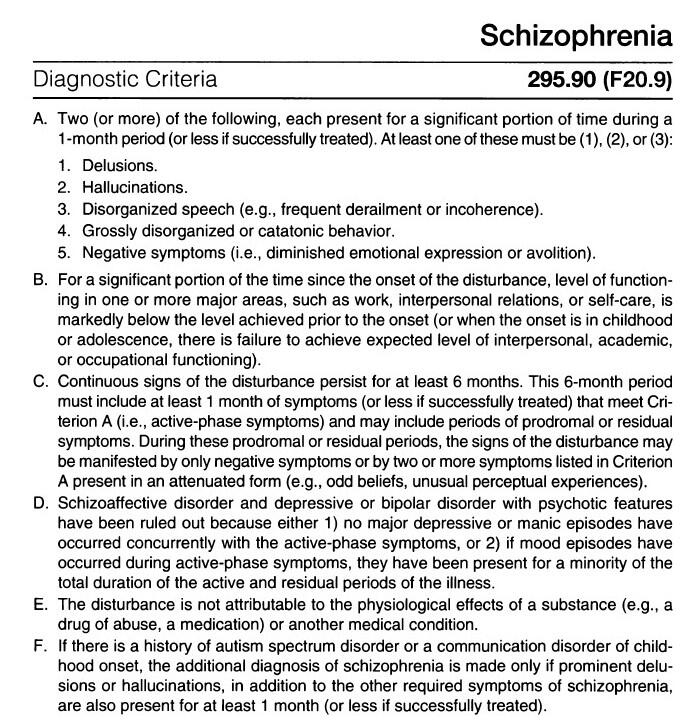 In schizophrenia remains relatively unaffected;
In schizophrenia remains relatively unaffected;
Reduced ability to anticipate future pleasure - anticipatory anhedonia. It is characteristic of patients with schizophrenia and is considered a hallmark of negative symptoms.
Anticipatory anhedonia results in an inability to anticipate rewards and reduces the patient's motivation for hedonic experiences 7.8 .
Studies have shown that schizophrenic patients with consummatory anhedonia do not differ from healthy controls in their ability to experience subjective responses to emotionally charged stimuli. With anticipatory anhedonia, the differences are pronounced.
The mechanisms underlying anhedonia can be explained as violations of the motivational component - no expectation of reward, positive reinforcement, no desire for action, and also considered from the point of view of cognitive dysfunction. When episodic memory impairments make it difficult to remember and recall hedonistic experiences 7 .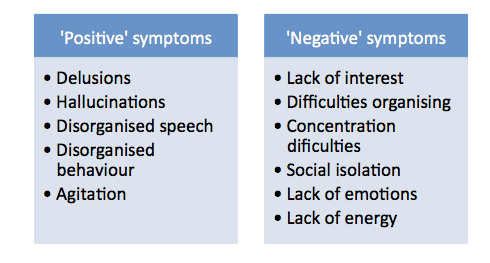
Abulia is an inability to purposeful activity. There is a decrease in involvement in work, study, hobbies, household chores. The ability to self-care is impaired.
There is no consensus on the degree of overlap between the terms abulia, decreased aspiration, lack of motivation, and apathy, and they are often considered interchangeable.
Abulia in schizophrenia is characterized by a weakening of interest in any activity: the patient does not initiate and does not support business activity. He has no such need as such. At the same time, the patient does not experience discomfort, feelings of guilt due to unfulfilled obligations.
A decrease in activity can also be a secondary manifestation associated with a depressed state (a general feeling of sadness, guilt, characteristic of abulia), due to the lack of opportunities for activity.
And yet, there is an opinion that a violation in the incentive-reward system is a key aspect of aboulia 7 .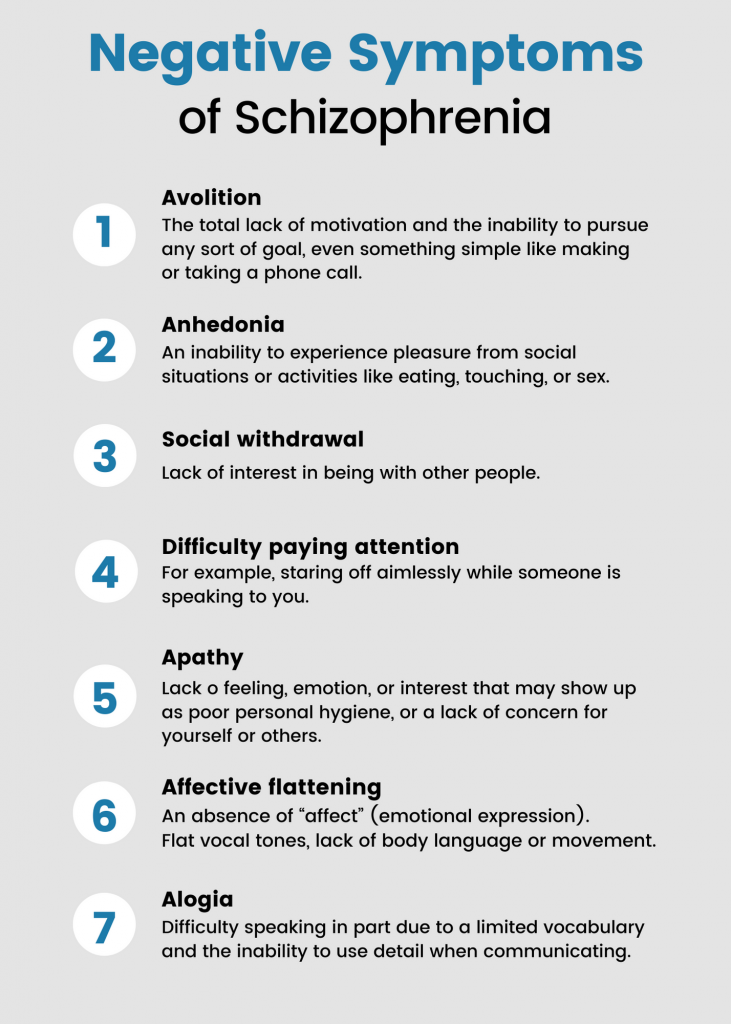
In general, studies show that of the five negative symptoms of schizophrenia listed, patients most often show a lack of social motivation, followed by a decrease in expressiveness (flattened affect) and alogia 9-11 .
Two groups of negative symptom complexes
(factors within negative symptoms)
Factor analyzes of negative symptoms demonstrated that the structure of these symptoms is not one-dimensional. The number of identified factors ranged from 2 to 5.
Usually, the division is based on how often certain combinations of symptoms occur in the clinical picture of the disease.
The most reproducible and stable structure includes two factors 12 :
A group of symptoms associated with a decrease in emotional expression (flattened affect, alogia).
A group of symptoms associated with a decrease in motivation for activity and inability to enjoy pleasure (anhedonia, asociality, abulia).
The co-occurrence of certain negative symptoms can be explained by: neurobiological pathologies and psychosocial causes (13).
For example, flattening of affect/alogia can be associated with a non-social, neuropsychological aspect (14). At the same time, aboulia/apathy is directly related to the social interaction of the patient (3).
Characteristics of negative symptoms
Negative symptoms can also be divided according to their appearance: primary, secondary; according to the degree of manifestation on: pronounced, predominant; by duration of exposure: persistent.
| Negative symptom definition | |
| Primary | Considered to be the main symptoms of schizophrenia that persist during the period of stabilization of the disease |
Primary negative symptoms of schizophrenia are considered the main symptoms of the disease, which persist even during the stabilization of the patient's condition.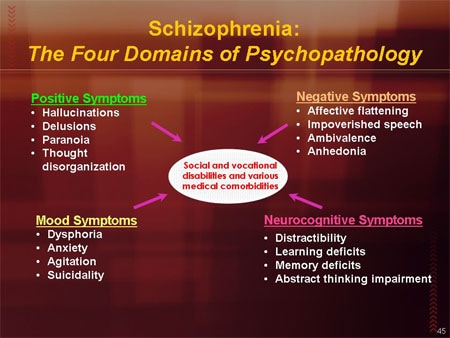 Their pathophysiology is specific to schizophrenia 15 .
Their pathophysiology is specific to schizophrenia 15 .
In contrast to primary symptoms, secondary negative symptoms appear as a consequence of positive symptoms, as neurological side effects of drug therapy, as a response to negative environmental factors 16.17 .
Characteristics "severe" and "predominant" describe the degree of manifestation of negative symptoms in a particular patient.
Symptoms may be considered "severe" if the patient has more negative symptoms than positive symptoms.
Criteria:
1. Baseline score ≥4 on at least 3 items or ≥5 on at least 2 items on the PANSS Negative Symptom Subscale;
2. Score >3 on item 1 and item 6 on the PANSS Negative Symptom Subscale and at least one-third of items scoring >3 and no more than two items scoring >3 on the Positive Symptom Subscale) 18.19 .
Persistent negative symptoms are defined by the PANSS as the presence of at least one moderate or severe negative symptom (not affected by depression or parkinsonism) at baseline and one year after treatment 20 . Presence of at least one negative symptom of moderate or severe severity for more than one year 20 .
Presence of at least one negative symptom of moderate or severe severity for more than one year 20 .
For purposes of clinical trials, data is required for periods longer than 6 months 19 .
Sources:
- Kirkpatrick, B., Fenton, W. S., Carpenter, W. T. & Marder, S. R. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr. Bull . 32, 214–219 (2006).
- Wallwork, R. S., Fortgang, R., Hashimoto, R., Weinberger, D. R. & Dickinson, D. Searching for a consensus five-factor model of the Positive and Negative Syndrome Scale for schizophrenia. Schizophr. Res . 137, 246–250 (2012).
- Foussias, G., Agid, O., Fervaha, G. & Remington, G. Negative symptoms of schizophrenia: Clinical features, relevance to real world functioning and specificity versus other CNS disorders. EUR. Neuropsychopharmacol . 24, 693–709 (2014).
- Bleuler, E. Dementia praecox or the group of schizophrenias. Dementia praecox or the group of schizophrenias (1950).

- National Institutes of Mental Health (NIMH). Schizophrenia . (2017). Available at: https://www.nimh.nih.gov/health/publications/schizophrenia-booklet/index.shtml.
- Fischer, B. A. & Buchanan, R. W. Schizophrenia: Clinical Manifestations, Course, Assessment and Diagnosis. UpToDate (2017). Available at: www.up-to-date/schizophrenia.
- Marder, S. R. & Galderisi, S. The current conceptualization of negative symptoms in schizophrenia. World Psychiatry 16, 14–24 (2017).
- Strauss, G. P., Waltz, J. A. & Gold, J. M. A review of reward processing and motivational impairment in schizophrenia. Schizophr. Bull . 40, S107-116 (2014).
- Lyne, J. et al. Prevalence of item level negative symptoms in first episode psychosis diagnoses. Schizophr. Res . 135, 128–133 (2012).
- Peralta, V. & Cuesta, M. J. Dimensional structure of psychotic symptoms: An item-level analysis of SAPS and SANS symptoms in psychotic disorders.
 Schizophr. Res . 38, 13–26 (1999).
Schizophr. Res . 38, 13–26 (1999). - Selten, J. P., Wiersma, D. & Van den Bosch, R. J. Distress attributed to negative symptoms in schizophrenia. Schizophr. Bull . 26, 737–744 (2000).
- Fleischhacker, W. et al. The efficacy of cariprazine in negative symptoms of schizophrenia: Post hoc analyzes of PANSS individual items and PANSS-derived factors. EUR. Psychiatry 58, 1–9 (2019).
- Bucci, P. & Galderisi, S. Categorizing and assessing negative symptoms. Curr. Opin. Psychiatry 30, 201–208 (2017).
- Liemburg, E. et al. Two subdomains of negative symptoms in psychotic disorders: Established and confirmed in two large cohorts. J. Psychiatr. Re s. 47, 718–725 (2013).
- Mucci, A., Merlotti, E., Üçok, A., Aleman, A. & Galderisi, S. Primary and persistent negative symptoms: Concepts, assessments and neurobiological bases. Schizophr. Res . 186, 19–28 (2017).
- Carpenter, W.
 T., Heinrichs, D. W. & Alphs, L. D. Treatment of negative symptoms. Schizophr. Bull . 11, 440–452 (1985).
T., Heinrichs, D. W. & Alphs, L. D. Treatment of negative symptoms. Schizophr. Bull . 11, 440–452 (1985). - Hasan, A. et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Schizophrenia, Part 1: Update 2012 on the acute treatment of schizophrenia and the management of treatment resistance. World J. Biol. Psychiatry 13, 318–378 (2012).
- Rabinowitz, J. et al. Negative symptoms in schizophrenia – the remarkable impact of inclusion definitions in clinical trials and their consequences. Schizophr. Res . 150, 334–338 (2013).
- European Medicines Agency. Guideline on clinical investigation of medicinal products, including depot preparation in the treatment of schizophrenia. (2012).
- Galderisi, S. et al. Persistent negative symptoms in first episode patients with schizophrenia: Results from the European First Episode Schizophrenia Trial. Eur. Neuropsychopharmacol .
 23, 196–204 (2013).
23, 196–204 (2013).
Acta Psychiatrica Scandinavica
Negative symptoms of schizophrenia: an unresolved problem
Stahl SM, Buckley PF.
Acta Psychiatr Scand. 2007; 115:4-11.
« Negative symptoms can make the patient reserved, inert. He does not disturb others. Therefore, relatives and carers of the patient consider such a condition as a positive aspect of the disease, and not as a dangerous factor that worsens the patient's quality of life.
Negative symptoms of schizophrenia: what are they?
Negative symptoms can be grouped into 2- or 5-factor patterns: decreased emotional expressiveness (flattened affect, alogia) and decreased motivation to work and inability to enjoy (anhedonia, asociality, abulia).
Download
Negative symptoms of schizophrenia: primary and secondary
Negative symptoms of schizophrenia: primary and secondary.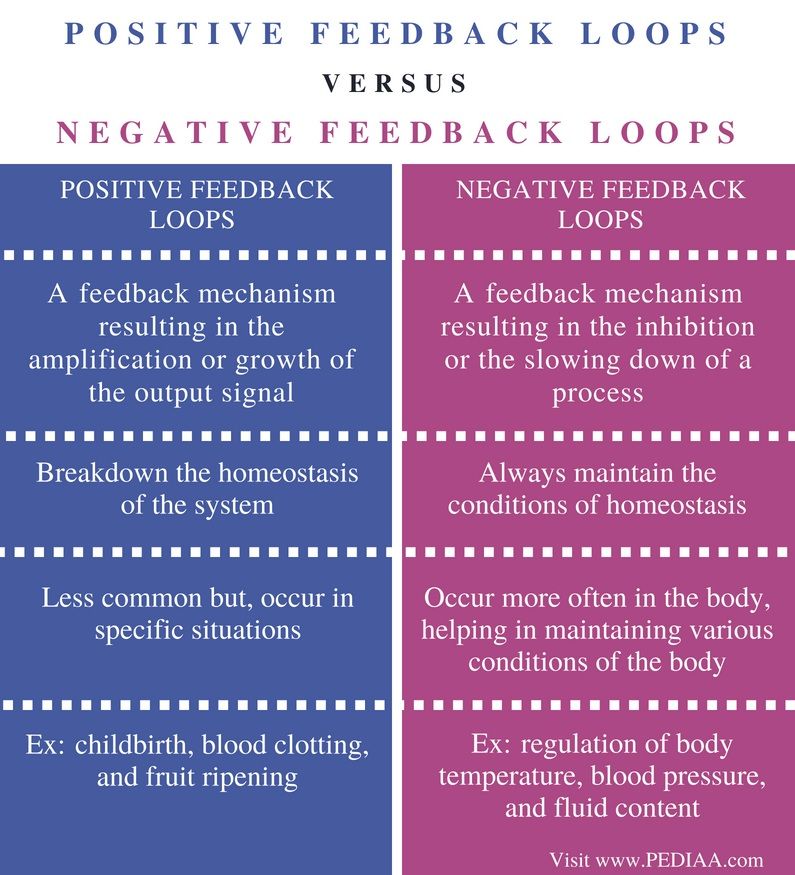
More…
Login to Unlock
Reagila: daily control… Reagila: daily control…
(Reagila® RU: LP-005405 dated 03/18/2019) In this case, treatment Relief of the negative symptoms of schizophrenia should be accompanied by an improvement in the patient's quality of life, in which case the treatment can be considered successful (2). Resistant
More…
Please confirm your consent to the use of cookies
Yes, I agree
No, I refuse
Please confirm that you are a health worker
Showing 0 result(s).
Please log in to see 0 more result(s).
Risperidone versus placebo in schizophrenia
Survey Question
Is risperidone (tablet form) more effective than placebo in treating symptoms of schizophrenia or similar illnesses?
Relevance
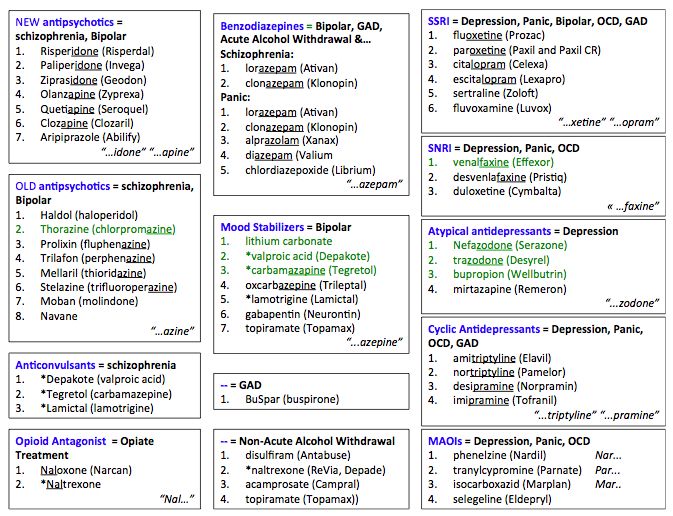
People with schizophrenia often hear voices and see things that do not exist (hallucinations) and believe in strange phenomena (manias). These are called "positive symptoms". Mental illness at the same time causes fatigue, apathy, emotional impoverishment (emotional dullness) and detachment. These are called "negative symptoms". The main treatment for these symptoms of schizophrenia are antipsychotic medications (neuroleptics). Antipsychotic drugs can be divided into traditional (old) and non-traditional (new) drugs. Traditional neuroleptics such as chlorpromazine (chlorpromazine) and haloperidol have been and remain the mainstay of treatment for decades, and are effective in reducing the positive symptoms of schizophrenia. Negative symptoms however are quite resistant to treatment. In addition, drug treatment is associated with unpleasant side effects that encourage people to stop taking their medication, which in turn can lead to relapse. There is an opinion that atypical antipsychotics such as risperidone are more effective than traditional antipsychotics because they reduce positive symptoms but cause fewer side effects.
These are called "positive symptoms". Mental illness at the same time causes fatigue, apathy, emotional impoverishment (emotional dullness) and detachment. These are called "negative symptoms". The main treatment for these symptoms of schizophrenia are antipsychotic medications (neuroleptics). Antipsychotic drugs can be divided into traditional (old) and non-traditional (new) drugs. Traditional neuroleptics such as chlorpromazine (chlorpromazine) and haloperidol have been and remain the mainstay of treatment for decades, and are effective in reducing the positive symptoms of schizophrenia. Negative symptoms however are quite resistant to treatment. In addition, drug treatment is associated with unpleasant side effects that encourage people to stop taking their medication, which in turn can lead to relapse. There is an opinion that atypical antipsychotics such as risperidone are more effective than traditional antipsychotics because they reduce positive symptoms but cause fewer side effects.
Study profile
High quality randomized clinical trials were searched in 2008, 2013 and 2015. We included 15 studies involving 2428 people. In the studies, participants with schizophrenia or related illnesses (inpatient and outpatient) were randomly assigned to treatment groups for oral risperidone or placebo.
Main results
Results from limited data suggest that risperidone is more effective than placebo in reducing overall symptoms of schizophrenia, and participants taking risperidone were more likely to adhere to treatment. However, like the old traditional antipsychotics, risperidone caused serious side effects such as parkinsonism.
Quality of evidence
The evidence was of very low quality. Information and data were limited, poorly presented and possibly biased (biased by bias) for risperidone. Nearly half of the included clinical trials were funded by pharmaceutical companies. It is difficult to draw firm conclusions based on the results of this review.