Depression more common in women
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
Alcohol, Tobacco, and Other Drugs
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Misusing alcohol, tobacco, and other drugs can have both immediate and long-term health effects.The misuse and abuse of alcohol, tobacco, illicit drugs, and prescription medications affect the health and well-being of millions of Americans. NSDUH estimates allow researchers, clinicians, policymakers, and the general public to better understand and improve the nation’s behavioral health. These reports and detailed tables present estimates from the 2021 National Survey on Drug Use and Health (NSDUH).
Alcohol
Data:
- Among the 133.1 million current alcohol users aged 12 or older in 2021, 60.0 million people (or 45.1%) were past month binge drinkers.
 The percentage of people who were past month binge drinkers was highest among young adults aged 18 to 25 (29.2% or 9.8 million people), followed by adults aged 26 or older (22.4% or 49.3 million people), then by adolescents aged 12 to 17 (3.8% or 995,000 people). (2021 NSDUH)
The percentage of people who were past month binge drinkers was highest among young adults aged 18 to 25 (29.2% or 9.8 million people), followed by adults aged 26 or older (22.4% or 49.3 million people), then by adolescents aged 12 to 17 (3.8% or 995,000 people). (2021 NSDUH) - Among people aged 12 to 20 in 2021, 15.1% (or 5.9 million people) were past month alcohol users. Estimates of binge alcohol use and heavy alcohol use in the past month among underage people were 8.3% (or 3.2 million people) and 1.6% (or 613,000 people), respectively. (2021 NSDUH)
- In 2020, 50.0% of people aged 12 or older (or 138.5 million people) used alcohol in the past month (i.e., current alcohol users) (2020 NSDUH)
- Among the 138.5 million people who were current alcohol users, 61.6 million people (or 44.4%) were classified as binge drinkers and 17.7 million people (28.8% of current binge drinkers and 12.8% of current alcohol users) were classified as heavy drinkers (2020 NSDUH)
- The percentage of people who were past month binge alcohol users was highest among young adults aged 18 to 25 (31.
 4%) compared with 22.9% of adults aged 26 or older and 4.1% of adolescents aged 12 to 17 (2020 NSDUH)
4%) compared with 22.9% of adults aged 26 or older and 4.1% of adolescents aged 12 to 17 (2020 NSDUH) - Excessive alcohol use can increase a person’s risk of stroke, liver cirrhosis, alcoholic hepatitis, cancer, and other serious health conditions
- Excessive alcohol use can also lead to risk-taking behavior, including driving while impaired. The Centers for Disease Control and Prevention reports that 29 people in the United States die in motor vehicle crashes that involve an alcohol-impaired driver daily
Programs/Initiatives:
- STOP Underage Drinking interagency portal - Interagency Coordinating Committee on the Prevention of Underage Drinking
- Interagency Coordinating Committee on the Prevention of Underage Drinking
- Talk. They Hear You.
- Underage Drinking: Myths vs. Facts
- Talking with your College-Bound Young Adult About Alcohol
Relevant links:
- National Association of State Alcohol and Drug Abuse Directors
- Department of Transportation Office of Drug & Alcohol Policy & Compliance
- Alcohol Policy Information Systems Database (APIS)
- National Institute on Alcohol Abuse and Alcoholism
Tobacco
Data:
- In 2020, 20.
 7% of people aged 12 or older (or 57.3 million people) used nicotine products (i.e., used tobacco products or vaped nicotine) in the past month (2020 NSDUH)
7% of people aged 12 or older (or 57.3 million people) used nicotine products (i.e., used tobacco products or vaped nicotine) in the past month (2020 NSDUH) - Among past month users of nicotine products, nearly two thirds of adolescents aged 12 to 17 (63.1%) vaped nicotine but did not use tobacco products. In contrast, 88.9% of past month nicotine product users aged 26 or older used only tobacco products (2020 NSDUH)
- Tobacco use is the leading cause of preventable death, often leading to lung cancer, respiratory disorders, heart disease, stroke, and other serious illnesses. The CDC reports that cigarette smoking causes more than 480,000 deaths each year in the United States
- The CDC’s Office on Smoking and Health reports that more than 16 million Americans are living with a disease caused by smoking cigarettes
Electronic cigarette (e-cigarette) use data:
- In 2021, 13.2 million people aged 12 or older (or 4.7%) used an e-cigarette or other vaping device to vape nicotine in the past month.
 The percentage of people who vaped nicotine was highest among young adults aged 18 to 25 (14.1% or 4.7 million people), followed by adolescents aged 12 to 17 (5.2% or 1.4 million people), then by adults aged 26 or older (3.2% or 7.1 million people).
The percentage of people who vaped nicotine was highest among young adults aged 18 to 25 (14.1% or 4.7 million people), followed by adolescents aged 12 to 17 (5.2% or 1.4 million people), then by adults aged 26 or older (3.2% or 7.1 million people). - Among people aged 12 to 20 in 2021, 11.0% (or 4.3 million people) used tobacco products or used an e-cigarette or other vaping device to vape nicotine in the past month. Among people in this age group, 8.1% (or 3.1 million people) vaped nicotine, 5.4% (or 2.1 million people) used tobacco products, and 3.4% (or 1.3 million people) smoked cigarettes in the past month. (2021 NSDUH)
- Data from the Centers for Disease Control and Prevention’s 2020 National Youth Tobacco Survey. Among both middle and high school students, current use of e-cigarettes declined from 2019 to 2020, reversing previous trends and returning current e-cigarette use to levels similar to those observed in 2018
- E-cigarettes are not safe for youth, young adults, or pregnant women, especially because they contain nicotine and other chemicals
Resources:
- Tips for Teens: Tobacco
- Tips for Teens: E-cigarettes
- Implementing Tobacco Cessation Programs in Substance Use Disorder Treatment Settings
- Synar Amendment Program
Links:
- Truth Initiative
- FDA Center for Tobacco Products
- CDC Office on Smoking and Health
- National Institute on Drug Abuse: Tobacco, Nicotine, and E-Cigarettes
- National Institute on Drug Abuse: E-Cigarettes
Opioids
Data:
- Among people aged 12 or older in 2021, 3.
 3% (or 9.2 million people) misused opioids (heroin or prescription pain relievers) in the past year. Among the 9.2 million people who misused opioids in the past year, 8.7 million people misused prescription pain relievers compared with 1.1 million people who used heroin. These numbers include 574,000 people who both misused prescription pain relievers and used heroin in the past year. (2021 NSDUH)
3% (or 9.2 million people) misused opioids (heroin or prescription pain relievers) in the past year. Among the 9.2 million people who misused opioids in the past year, 8.7 million people misused prescription pain relievers compared with 1.1 million people who used heroin. These numbers include 574,000 people who both misused prescription pain relievers and used heroin in the past year. (2021 NSDUH) - Among people aged 12 or older in 2020, 3.4% (or 9.5 million people) misused opioids in the past year. Among the 9.5 million people who misused opioids in the past year, 9.3 million people misused prescription pain relievers and 902,000 people used heroin (2020 NSDUH)
- According to the Centers for Disease Control and Prevention’s Understanding the Epidemic, an average of 128 Americans die every day from an opioid overdose
Resources:
- Medication-Assisted Treatment
- Opioid Overdose Prevention Toolkit
- TIP 63: Medications for Opioid Use Disorder
- Use of Medication-Assisted Treatment for Opioid Use Disorder in Criminal Justice Settings
- Opioid Use Disorder and Pregnancy
- Clinical Guidance for Treating Pregnant and Parenting Women With Opioid Use Disorder and Their Infants
- The Facts about Buprenorphine for Treatment of Opioid Addiction
- Pregnancy Planning for Women Being Treated for Opioid Use Disorder
- Tips for Teens: Opioids
- Rural Opioid Technical Assistance Grants
- Tribal Opioid Response Grants
- Provider’s Clinical Support System - Medication Assisted Treatment Grant Program
Links:
- National Institute on Drug Abuse: Opioids
- National Institute on Drug Abuse: Heroin
- HHS Prevent Opioid Abuse
- Community Anti-Drug Coalitions of America
- Addiction Technology Transfer Center (ATTC) Network
- Prevention Technology Transfer Center (PTTC) Network
Marijuana
Data:
- In 2021, marijuana was the most commonly used illicit drug, with 18.
 7% of people aged 12 or older (or 52.5 million people) using it in the past year. The percentage was highest among young adults aged 18 to 25 (35.4% or 11.8 million people), followed by adults aged 26 or older (17.2% or 37.9 million people), then by adolescents aged 12 to 17 (10.5% or 2.7 million people).
7% of people aged 12 or older (or 52.5 million people) using it in the past year. The percentage was highest among young adults aged 18 to 25 (35.4% or 11.8 million people), followed by adults aged 26 or older (17.2% or 37.9 million people), then by adolescents aged 12 to 17 (10.5% or 2.7 million people). - The percentage of people who used marijuana in the past year was highest among young adults aged 18 to 25 (34.5%) compared with 16.3% of adults aged 26 or older and 10.1% of adolescents aged 12 to 17 (2020 NSDUH)
- Marijuana can impair judgment and distort perception in the short term and can lead to memory impairment in the long term
- Marijuana can have significant health effects on youth and pregnant women.
Resources:
- Know the Risks of Marijuana
- Marijuana and Pregnancy
- Tips for Teens: Marijuana
Relevant links:
- National Institute on Drug Abuse: Marijuana
- Addiction Technology Transfer Centers on Marijuana
- CDC Marijuana and Public Health
Emerging Trends in Substance Misuse:
- Methamphetamine—In 2019, NSDUH data show that approximately 2 million people used methamphetamine in the past year.
 Approximately 1 million people had a methamphetamine use disorder, which was higher than the percentage in 2016, but similar to the percentages in 2015 and 2018. The National Institute on Drug Abuse Data shows that overdose death rates involving methamphetamine have quadrupled from 2011 to 2017. Frequent meth use is associated with mood disturbances, hallucinations, and paranoia.
Approximately 1 million people had a methamphetamine use disorder, which was higher than the percentage in 2016, but similar to the percentages in 2015 and 2018. The National Institute on Drug Abuse Data shows that overdose death rates involving methamphetamine have quadrupled from 2011 to 2017. Frequent meth use is associated with mood disturbances, hallucinations, and paranoia. - Cocaine—In 2019, NSDUH data show an estimated 5.5 million people aged 12 or older were past users of cocaine, including about 778,000 users of crack. The CDC reports that overdose deaths involving have increased by one-third from 2016 to 2017. In the short term, cocaine use can result in increased blood pressure, restlessness, and irritability. In the long term, severe medical complications of cocaine use include heart attacks, seizures, and abdominal pain.
- Kratom—In 2019, NSDUH data show that about 825,000 people had used Kratom in the past month. Kratom is a tropical plant that grows naturally in Southeast Asia with leaves that can have psychotropic effects by affecting opioid brain receptors.
 It is currently unregulated and has risk of abuse and dependence. The National Institute on Drug Abuse reports that health effects of Kratom can include nausea, itching, seizures, and hallucinations.
It is currently unregulated and has risk of abuse and dependence. The National Institute on Drug Abuse reports that health effects of Kratom can include nausea, itching, seizures, and hallucinations.
Resources:
- Tips for Teens: Methamphetamine
- Tips for Teens: Cocaine
- National Institute on Drug Abuse
More SAMHSA publications on substance use prevention and treatment.
Last Updated: 01/05/2023
Features of depressive disorders in women and men
It is known that depressive disorders occupy a leading position among all mental illnesses. In the countries of the European Union, their share in women is about 30%, in men - 23% [1]. At the same time, it was found that women suffer from depression 2 times more often than men [2, 3], and have twice the risk of developing depression compared to men, starting from adolescence, i.e. from the moment the menstrual cycle begins [2] . Women go to the doctor more often and have a higher detection rate of depressive disorders [4, 5]. Men, on the other hand, more often hide their emotional experiences from the doctor and those around them, considering them a manifestation of weakness of character. Men are fond of extreme sports, gambling, “go” to work in order to arouse in themselves the lost interest in life. Some men try to alleviate mental conditions with the use of alcohol and psychoactive substances [6]. The higher frequency of depression in women is explained by their special position in the family and society, their social role, the negative impact of socio-economic, religious, cultural and other factors. In many countries, women are still unequal with men, despite the fact that a woman can be highly valued as a mother, wife, or professional specialist [3]. Depression in women may be associated with purely female socio-psychological and family problems, such as loneliness, divorce, infertility, illness and troubles in the family, while in men depression often occurs against the background of troubles and failures at work [3, 7].
Men, on the other hand, more often hide their emotional experiences from the doctor and those around them, considering them a manifestation of weakness of character. Men are fond of extreme sports, gambling, “go” to work in order to arouse in themselves the lost interest in life. Some men try to alleviate mental conditions with the use of alcohol and psychoactive substances [6]. The higher frequency of depression in women is explained by their special position in the family and society, their social role, the negative impact of socio-economic, religious, cultural and other factors. In many countries, women are still unequal with men, despite the fact that a woman can be highly valued as a mother, wife, or professional specialist [3]. Depression in women may be associated with purely female socio-psychological and family problems, such as loneliness, divorce, infertility, illness and troubles in the family, while in men depression often occurs against the background of troubles and failures at work [3, 7]. Some studies [8] have noted a relationship between mood and psychosocial factors (stress, physical and mental health) [8].
Some studies [8] have noted a relationship between mood and psychosocial factors (stress, physical and mental health) [8].
In addition to psychosocial factors, neurohormonal changes in the body play an important role in the development of depressive disorders in women (during puberty, during pregnancy and the postpartum period, during perimenopause) [8—16]. Cyclic changes in a woman's body, caused by the menstrual cycle, are also reflected in the emotional sphere in the form of premenstrual mood deterioration [17-19].
Thus, it can be noted that the development of depression in women and men is influenced by both sex-role and social factors, defined by the concept of "gender", and purely biological ones, such as the presence in women of menstrual-generative function associated with the cyclic release of hormones, regulated by the neuroendocrine system.
In general, the symptoms of depression are the same in women and men, but there are certain differences in their frequency and prevalence in the structure of depression. In women, depressive episodes are longer and recur more frequently than in men [20]. Atypical depression and somatic symptoms of depression are more common in women [21]. In the study by B. Silverstein et al. [22] found that classical depression is comparable in the frequency of prevailing symptoms in women and men, but anxious depression with somatic symptoms occurs 2 times more often in women. C. Lai [23], in a study of 146 Taiwanese patients, showed that women with anxious depression had increased appetite, hypersomnia, and loss of sensitivity; women were more likely than men to report a violation of sexual desire, women showed a higher frequency of sleep disturbances (difficulty falling asleep, altered sleep duration), somatic complaints (loss of appetite, chest pain, headache), melancholy and anxiety; men reported more episodes with alcohol and substance use. In a study conducted by the Canadian Epidemiological Society [24], it was found that atypical symptoms of depression were observed in only 11% of cases.
In women, depressive episodes are longer and recur more frequently than in men [20]. Atypical depression and somatic symptoms of depression are more common in women [21]. In the study by B. Silverstein et al. [22] found that classical depression is comparable in the frequency of prevailing symptoms in women and men, but anxious depression with somatic symptoms occurs 2 times more often in women. C. Lai [23], in a study of 146 Taiwanese patients, showed that women with anxious depression had increased appetite, hypersomnia, and loss of sensitivity; women were more likely than men to report a violation of sexual desire, women showed a higher frequency of sleep disturbances (difficulty falling asleep, altered sleep duration), somatic complaints (loss of appetite, chest pain, headache), melancholy and anxiety; men reported more episodes with alcohol and substance use. In a study conducted by the Canadian Epidemiological Society [24], it was found that atypical symptoms of depression were observed in only 11% of cases. Women predominated in the groups of both typical and atypical depression (77 and 75%, respectively). When examining twin pairs [25], a higher frequency of atypical symptoms was found in women, such as increased appetite, weight gain, hypersomnia, and fatigue. These patients also had ideas of guilt, tearfulness, diurnal mood swings with a predominant deterioration in the morning hours, and lethargy. Women also had younger onset of depression and longer duration of depressive episodes than men.
Women predominated in the groups of both typical and atypical depression (77 and 75%, respectively). When examining twin pairs [25], a higher frequency of atypical symptoms was found in women, such as increased appetite, weight gain, hypersomnia, and fatigue. These patients also had ideas of guilt, tearfulness, diurnal mood swings with a predominant deterioration in the morning hours, and lethargy. Women also had younger onset of depression and longer duration of depressive episodes than men.
But, summarizing the available literature on the issue under consideration, we can note the sufficient inconsistency and ambiguity of the results obtained; this is probably due to the difference in samples and diagnostic criteria for depression, which is the basis for further research.
The purpose of this work is to study the clinical features of depression in women compared with men.
Material and methods
The study was conducted from 2014 to 2017 in the outpatient and inpatient settings of the Clinic of Psychiatry. S.S. Korsakov First Moscow State Medical University. THEM. Sechenov. 120 women aged 18 to 65 years and 67 men of the same age suffering from recurrent depressive disorder - RDD (F33 according to ICD-10) were examined by clinical and clinical follow-up methods.
S.S. Korsakov First Moscow State Medical University. THEM. Sechenov. 120 women aged 18 to 65 years and 67 men of the same age suffering from recurrent depressive disorder - RDD (F33 according to ICD-10) were examined by clinical and clinical follow-up methods.
The study did not include women and men with a first or single episode of depression, as well as those suffering from decompensated somatic and neurological diseases, pregnant women.
A special questionnaire card was developed for the study. The MADRS (Montgomery-Asberg Depression Rating Scale) was also used to assess the severity of depression.
The average age of women was 45.0 [32.5; 54.0] years, male age — 47.0 [40.5; 54.0] years ( p \u003d 0.254). The duration of the disease in the group of women was 8.0 [4.0; 16.0] years, in men — 6.0 [2.5; 12.0] years ( p = 0.161). The severity of depression in women was 27.0 [26.0; 28.0] points, in men — 27.0 [26.0; 27.5] points on the MADRS scale ( p = 0. 704). Thus, the groups did not differ significantly in age, disease duration, or severity of depression.
704). Thus, the groups did not differ significantly in age, disease duration, or severity of depression.
Statistical processing of the obtained results was carried out using the program Statistica for Windows 6.0 (StatSoft Inc.). Qualitative features are presented as absolute and relative (%) indicators.
The analysis of the correspondence of the distribution of attribute values to the characteristics of the normal distribution was carried out using the Kolmogorov-Smirnov method. Since most of the quantitative characteristics did not comply with the laws of normal distribution, they were described using the median (Me) and quartiles (Me [25%; 75%]), and nonparametric statistical methods were used to assess the statistical significance of differences between groups: when comparing two independent groups according to quantitative indicators, the Mann-Whitney method was used; more than two independent groups - the Kruskal-Wallis method. When comparing independent groups in terms of quality indicators, the χ 9 method was used0035 2 , bilateral if necessary - Fisher's exact test.
The confidence level was accepted as sufficient at p <0.05; in the case of multiple comparisons, the Bonferroni correction was used, in this case p was defined as p = 0.05/ n , where n is the number of pairwise comparisons on the same data set.
Results and discussion
When comparing women and men, a number of significant differences were found. When assessing the socio-demographic indicators, it was found (Table 1), Table 1. Socio-demographic indicators in the female and male groups of patients that there were more married women than married men, and there were slightly more divorced and unmarried men than the corresponding status of women . The number of working men is significantly higher, which is probably due not only to illness, but also to the social status of a housewife, as well as a lower retirement age. The level of education is approximately the same in the two groups and does not differ statistically significantly. Thus, men are more busy with work and are less adapted in family terms.
Thus, men are more busy with work and are less adapted in family terms.
When assessing the course of depression, it was found that in women, depression generally begins at an earlier age compared to men (Table 2). Table 2. Characteristics of the course of depression in women and men At the same time, in 71.7% of women, depression manifests itself during periods of hormonal adjustment (puberty, postpartum, perimenopause). The duration of the disease in them was 8.0 [4.0; 16.0] years, for men — 6.0 [2.5; 12.0] years. The number of depressive episodes in women was also significantly higher than in men. The average duration of depressive episodes in men and women did not differ significantly, however, the duration of remission was significantly longer in the group of women, which, with a larger number of episodes, could probably be associated with an earlier onset of depression in them. However, complete remission was more often achieved in men — 79.1%, compared with women - 48. 3%, which may be due to the presence of premenstrual syndrome in 65% of patients, in which there was a deterioration in the mental state. The severity of depression on the MADRS scale, the presence of seasonality did not significantly differ in the compared groups. However, seasonality in the course of depression in women was significantly more common in those patients (20.9%) whose manifestation of depression was not associated with periods of hormonal changes.
3%, which may be due to the presence of premenstrual syndrome in 65% of patients, in which there was a deterioration in the mental state. The severity of depression on the MADRS scale, the presence of seasonality did not significantly differ in the compared groups. However, seasonality in the course of depression in women was significantly more common in those patients (20.9%) whose manifestation of depression was not associated with periods of hormonal changes.
When comparing the clinical picture of depression in women and men, it was found (Table 3), Table 3. Clinical features of depression in women and men Note. BP - blood pressure. that in women the leading affect was anxiety, in men it was melancholy. Apathetic depression was the most rare in both women and men, but significantly more common in women. For women, a decrease in appetite was more characteristic (an increase in appetite was quite rare and only in women), the presence of diurnal mood swings with deterioration in most cases in the morning, suicidal thoughts, lack of strength, energy, and a constant feeling of fatigue compared to men. Men were characterized by a change in motor activity in the form of lethargy, while women were characterized by arousal. Decreased libido was presented approximately equally in men and women. Sleep disturbances characteristic of depression (early awakenings, shortened sleep) were equally present in the structure of depression in women and men, but women significantly more often complained of disturbed falling asleep and lack of a sense of sleep. Among the symptoms in women, ideas of self-accusation and self-abasement, avoidance of contact with other people were significantly more common. A decrease in motivation was significantly more often observed in men. Anhedonia and suffering from loneliness are presented approximately equally in both groups of patients.
Men were characterized by a change in motor activity in the form of lethargy, while women were characterized by arousal. Decreased libido was presented approximately equally in men and women. Sleep disturbances characteristic of depression (early awakenings, shortened sleep) were equally present in the structure of depression in women and men, but women significantly more often complained of disturbed falling asleep and lack of a sense of sleep. Among the symptoms in women, ideas of self-accusation and self-abasement, avoidance of contact with other people were significantly more common. A decrease in motivation was significantly more often observed in men. Anhedonia and suffering from loneliness are presented approximately equally in both groups of patients.
According to the results of the assessment of somatic symptoms observed in depression, women complained of constipation and tachycardia significantly less frequently. The men were characterized by panic attacks along with other somatic symptoms.
Comorbidity with alcohol abuse in the group of men is significantly higher than in women (34.3% vs. 10.0%; p <0.001).
When evaluating concomitant somatic diseases, data were obtained, according to which men have a significantly higher number of cardiovascular, pulmonary diseases and diseases of the genitourinary system (Table 4). Table 4. Concomitant diseases in women and men The predominance of concomitant cardiovascular and pulmonary diseases in men may be determined by their significantly higher presence of bad habits compared to women (74.6% vs. 22.7%; p <0.001).
The data obtained in this study indicate that the clinical picture of recurrent depression and its course have certain gender differences. The earlier onset of the disease with more seizures and less quality remissions in women is due to the relationship and mutual influence of the menstrual-generative (reproductive) function and depression. Symptoms typical of endogenous depression, such as anhedonia, early morning awakenings, diurnal mood swings with worsening in the morning, were characteristic of most women and men. In the structure of depression in women, anxiety, ideas of self-blame, suicidal thoughts, avoidance of contact with others, weakness, fatigue, decrease and increase in appetite, sleep disturbance and lack of a sense of sleep were more often noted. In men, symptoms such as melancholy, motor retardation, decreased motivation, somatic symptoms of depression (constipation, tachycardia, increased blood pressure), comorbid panic attacks and concomitant diseases of the cardiovascular, respiratory and genitourinary systems were more often observed. The revealed gender features in the structure and course of recurrent depression will allow for more accurate diagnosis and prescribing adequate therapy.
In the structure of depression in women, anxiety, ideas of self-blame, suicidal thoughts, avoidance of contact with others, weakness, fatigue, decrease and increase in appetite, sleep disturbance and lack of a sense of sleep were more often noted. In men, symptoms such as melancholy, motor retardation, decreased motivation, somatic symptoms of depression (constipation, tachycardia, increased blood pressure), comorbid panic attacks and concomitant diseases of the cardiovascular, respiratory and genitourinary systems were more often observed. The revealed gender features in the structure and course of recurrent depression will allow for more accurate diagnosis and prescribing adequate therapy.
The authors declare no conflict of interest.
*e-mail: [email protected]
https://orcid.org/0000-0002-0013-5031
Spin straw into gold: why women are more likely to suffer from depression
Sad but true: in all countries of the world, women suffer from depression twice as often as men. Psychologist Ursula Nuber believes that women take on too much: the blame for failed relationships, caring for parents and children, career, life. Forbes Woman publishes an excerpt from Nuber's book "Who am I without you? Why women are more likely to suffer from depression and how they find themselves, which is published by the Alpina publishing house
Psychologist Ursula Nuber believes that women take on too much: the blame for failed relationships, caring for parents and children, career, life. Forbes Woman publishes an excerpt from Nuber's book "Who am I without you? Why women are more likely to suffer from depression and how they find themselves, which is published by the Alpina publishing house
In an attempt to understand the general increase in depression among men and women, experts are increasingly looking at causes that are outside the person. First of all, on social changes, because of which everyday life has become so tense and tiring. Today, most of us suffer from colossal lack of time, have to do several things at the same time, experience stress even in our free time, and increasingly feel that life is out of control.
The idea that the social structure of our time contributes to depression is credited to the French sociologist Alain Ehrenberg, who in his book Tired of Being Oneself (La Fatigue d'être soi) showed that modern conditions of life and the various problems associated with them pose a serious risk to mental health.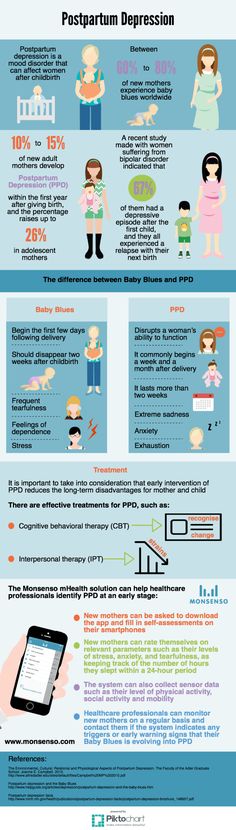 He argues that people today are overwhelmed and morally capitulate to the demands of society. “Whatever area we turn to (be it work, school or family), the world dictates new rules to us,” writes Ehrenberg. - They no longer include humility, discipline and adherence to morality, but flexibility, willingness to change, quick reaction, etc. Self-control, mental and affective flexibility, the ability to act: a person has to constantly adapt to a world that is losing its constancy, to an unstable and temporary world, consisting of multidirectional flows and trajectories. The clear rules of the social and political game have been lost. Such institutional transformations give the impression that each of us, even the most ordinary and weakest, is obliged to make his own choice and make decisions on all issues.
He argues that people today are overwhelmed and morally capitulate to the demands of society. “Whatever area we turn to (be it work, school or family), the world dictates new rules to us,” writes Ehrenberg. - They no longer include humility, discipline and adherence to morality, but flexibility, willingness to change, quick reaction, etc. Self-control, mental and affective flexibility, the ability to act: a person has to constantly adapt to a world that is losing its constancy, to an unstable and temporary world, consisting of multidirectional flows and trajectories. The clear rules of the social and political game have been lost. Such institutional transformations give the impression that each of us, even the most ordinary and weakest, is obliged to make his own choice and make decisions on all issues.
Self-sufficiency is the first commandment of our time. And at the same time, trying to rely only on ourselves, we are constantly faced with limitations. How can you handle family and work responsibilities equally when there are not enough child care places, full-time schools, or part-time jobs? How can personal happiness be achieved when the need to make a choice among many options is crushing and the ability to understand what could make us personally happy and what is the meaning of our life is lost? Such overloads, according to Ehrenberg, cause the depletion of our "I" and lead to depressive disorders. After all, a person who believes that he cannot cope, does not meet his own requirements and the (real or perceived) expectations of others, is at risk of becoming a victim of depression. The sociologist paints a grim picture of the future: “Psychotropic drugs, which improve mood, increase self-control and, who knows, perhaps even alleviate the horror of existence, will occupy an increasing place in our lives.”
How can you handle family and work responsibilities equally when there are not enough child care places, full-time schools, or part-time jobs? How can personal happiness be achieved when the need to make a choice among many options is crushing and the ability to understand what could make us personally happy and what is the meaning of our life is lost? Such overloads, according to Ehrenberg, cause the depletion of our "I" and lead to depressive disorders. After all, a person who believes that he cannot cope, does not meet his own requirements and the (real or perceived) expectations of others, is at risk of becoming a victim of depression. The sociologist paints a grim picture of the future: “Psychotropic drugs, which improve mood, increase self-control and, who knows, perhaps even alleviate the horror of existence, will occupy an increasing place in our lives.”
Psychoanalyst Marianne Leuzinger-Boleber puts forward similar arguments. She also believes that the spread of this disease has primarily social prerequisites. “Depression is a disease of the meaning and joy of life. Both — the meaning and joy of life — are harder to find in our time than ever before. Just look at the political situation in Germany: unemployment is rising, the welfare state is collapsing, old recipes are outdated, old ties are falling apart. All of these factors can cause depression. The person falling into it reacts sharply to the current state of disorientation.
She also believes that the spread of this disease has primarily social prerequisites. “Depression is a disease of the meaning and joy of life. Both — the meaning and joy of life — are harder to find in our time than ever before. Just look at the political situation in Germany: unemployment is rising, the welfare state is collapsing, old recipes are outdated, old ties are falling apart. All of these factors can cause depression. The person falling into it reacts sharply to the current state of disorientation.
A few years ago, Dutch scientists found evidence that often, when women seek to equalize the balance in relationships, they literally run into a blank wall.
Inexorably high demands, lack of meaning and joy in life - the norms of life in modern society equally oppress both sexes and, therefore, do not explain why women fall ill with depression much more often than men. However, when investigating the causes of this disease, it is necessary to take into account the significance of such a stimulus as stress. After all, apparently, in addition to those social conditions that exhaust both those and others equally, additional specific stress factors put pressure on women.
However, when investigating the causes of this disease, it is necessary to take into account the significance of such a stimulus as stress. After all, apparently, in addition to those social conditions that exhaust both those and others equally, additional specific stress factors put pressure on women.
Elena works four hours a day as a cashier at a gas station. The gas station is 50 km from her house, so she has to wind 100 km back and forth every day, spending from 50 minutes to nearly two hours, depending on traffic. And it would be nothing if her working day ended there. But she still has to work as a cleaner in two or three places. After all, she has four children from 8 to 15 years old, and the woman barely makes ends meet. When she returns home late at night, the children are already looking forward to dinner. Her husband is at home all day, as he works mainly on the night shift at the factory, and sometimes he can cook something. But this does not happen so often, because he needs to get enough sleep. In addition, in the evening Elena makes sure that the children do their homework. For a long time she coped well with the daily chores. But lately she has been suffering from insomnia. It is rarely possible to spend the night calmly without waking up, and in the morning it is insanely hard to get out of bed. She feels overwhelmed, and it seems that a weight of lead is pulling her to the ground.
But this does not happen so often, because he needs to get enough sleep. In addition, in the evening Elena makes sure that the children do their homework. For a long time she coped well with the daily chores. But lately she has been suffering from insomnia. It is rarely possible to spend the night calmly without waking up, and in the morning it is insanely hard to get out of bed. She feels overwhelmed, and it seems that a weight of lead is pulling her to the ground.
Even if a woman receives a lot of support from her partner or relatives, household chores take a lot of her energy. Her daily routine is often determined by the needs of other people. No matter how emancipated today's women may be, they are still caught in the vise of the continuous cycle of "women's" affairs: raising children, housekeeping, doing homework, ironing, washing, cleaning, caring for sick and elderly relatives - all these tasks are heavily burdened mainly on the shoulders of women and are never completed. In addition, the performance of the functions in question usually does not bring women much respect or recognition. They can never be sure that they have done everything right and as expected of them. There are no clear criteria by which one can determine whether enough has been done and whether it has turned out well. So women try to be guided by an imaginary, mostly extremely high standard - and this gives them an oppressive feeling that they are not good enough. After all, society addresses them with a ruthless message. It convinces them that they can have everything - a job, a partner, a family, but is silent about the price they will have to pay for this, and does not warn that the main burden will fall on their shoulders. As a result, women believe that in life it is possible to succeed in all areas at once, and blame themselves if their hopes are not met.
In addition, the performance of the functions in question usually does not bring women much respect or recognition. They can never be sure that they have done everything right and as expected of them. There are no clear criteria by which one can determine whether enough has been done and whether it has turned out well. So women try to be guided by an imaginary, mostly extremely high standard - and this gives them an oppressive feeling that they are not good enough. After all, society addresses them with a ruthless message. It convinces them that they can have everything - a job, a partner, a family, but is silent about the price they will have to pay for this, and does not warn that the main burden will fall on their shoulders. As a result, women believe that in life it is possible to succeed in all areas at once, and blame themselves if their hopes are not met.
That this is impossible to achieve, even with great effort, is obvious when one pays attention to the special stressors that occur predominantly in the lives of women. Women's stress is significantly different from men's. Do not underestimate the difficulties of men. But there are many stressors that affect women exclusively, threaten their health - and can cause depression.
Women's stress is significantly different from men's. Do not underestimate the difficulties of men. But there are many stressors that affect women exclusively, threaten their health - and can cause depression.
The scourge of the digital society: how we were all struck by the fear of missed opportunities and what to do about it
Stress factor: time
Compared to men, women experience stress much longer. They spend significantly more time working in the office and around the house, raising children and caring for elderly relatives than men. Numerous studies confirm that cooking, cleaning and laundry are still perceived as predominantly women's activities, in addition, women have the main responsibility for raising children. If anyone thinks that men in our time are aware of this imbalance (and appreciate their wives for their overtime work), then a survey organized by the GfK market research institute will help dispel this misconception. Parents of preschool children answered questions about how actively they participate in housework and childcare. According to the survey data, the majority of fathers were of the opinion that equality reigns in their family in relation to everyday tasks. About 40% of the surveyed fathers of children under six years of age said they do exactly the same amount of housework as their spouse. However, women assessed the situation somewhat differently: only about 26% of the mothers surveyed indicated that the husband participates in household chores as much as they do. This gap is also confirmed by other studies: at the latest after the birth of the first child, marriage, previously based on partnership, turns into a traditional one, and a once equal, emancipated woman becomes either a tangled “working mother”, balancing double workload with great difficulty, or an unfortunate housewife who gave up her career for the sake of her family.
Parents of preschool children answered questions about how actively they participate in housework and childcare. According to the survey data, the majority of fathers were of the opinion that equality reigns in their family in relation to everyday tasks. About 40% of the surveyed fathers of children under six years of age said they do exactly the same amount of housework as their spouse. However, women assessed the situation somewhat differently: only about 26% of the mothers surveyed indicated that the husband participates in household chores as much as they do. This gap is also confirmed by other studies: at the latest after the birth of the first child, marriage, previously based on partnership, turns into a traditional one, and a once equal, emancipated woman becomes either a tangled “working mother”, balancing double workload with great difficulty, or an unfortunate housewife who gave up her career for the sake of her family.
It has been proven that married men are much less likely to become depressed than single men.Married women, on the other hand, are more likely to develop depression than unmarried women.
Often there is a reproach - and often from the women themselves, that it is they who are to blame for such a bias: they should simply involve their husbands in housework and childcare more often. They could see to it that the men did their part. Many women object to this “I am not his teacher” or point out that all their attempts have not been successful. Their typical complaints are: “How many times do I have to tell him that he has to cook too?”, “How many times do I have to tell him that he has to come home from work early to put the kids to bed?”, “How many times do I tell him that At the end of a long day, would I like to have a quiet conversation with him?”
If women don't get any response to this, they feel they can't bring about any change and resign themselves to the situation. From the outside, such women seem to be happy with everything, but inside they still experience tension and stress.
From the outside, such women seem to be happy with everything, but inside they still experience tension and stress.
A few years ago, Dutch scientists found confirmation that often, when women seek to equalize the balance in relationships, they literally run into a blank wall. It turned out that the reason why women are so bad at defending their interests, wishes and needs is related, among other things, to the strategies they use to achieve change. Because they avoid open conflict and don't want to cause trouble (see more on this in the section "As long as they don't cause trouble"), they resort to less successful indirect methods. Careful maneuvering, accurate criticism, transparent hints are called upon to bring about the necessary changes in the long run. Most women seek to avoid quarrels and try to "write out" their wishes to a partner in homeopathic doses. Another female strategy is waiting. Women expect to achieve change through patience alone, but to no avail.
Smiling depression. How dangerous is the desire to be no worse than others
Men also use the strategy of waiting - and achieve in their own way much more success than women. They simply behave passively and by their inaction ensure that everything remains the same. One of the study participants admitted: “I don’t do anything. I sit quietly for myself, and then she has no choice but to look after the children herself. I just don't react. She usually puts up with it." And another said: “When my mother got angry, I didn’t say anything. I just did my own thing. And I do the same with my wife. I just don't react. I don't want to hear what she says, and I can't hear it."
Men have another effective strategy - argumentation. Many of them try to convince women that the current situation is completely normal. Using strong arguments, they clearly demonstrate to the woman that there are clear advantages in her position, her demands are unfounded and she has no reason to be dissatisfied. But at the same time, the man does not take into account the feelings of the woman, so that she becomes confused. We see examples of this in the aforementioned Dutch survey: “He thinks I get everything wrong. Reminds me of different events, and then I think: “Well, yes, he is right!” But then I notice that my feelings, in which he is not at all interested, tell me something else, and that his words do not agree with the facts. But then I think it's all about me."
Using strong arguments, they clearly demonstrate to the woman that there are clear advantages in her position, her demands are unfounded and she has no reason to be dissatisfied. But at the same time, the man does not take into account the feelings of the woman, so that she becomes confused. We see examples of this in the aforementioned Dutch survey: “He thinks I get everything wrong. Reminds me of different events, and then I think: “Well, yes, he is right!” But then I notice that my feelings, in which he is not at all interested, tell me something else, and that his words do not agree with the facts. But then I think it's all about me."
Stress from a lot of things, chronic lack of time and constant overwork does not necessarily lead to depression. When a woman receives recognition of her achievements from a partner or other significant people, when her legitimate requirements are heeded and she meets care and respect in a relationship, she is quite able to find the strength to perform various tasks. But if she gets the impression that she is talking to the wall and no one pays attention to her, or that her efforts are taken for granted, then there is almost no chance of recharging dead batteries. If at the same time she feels cut off from other people and abandoned to her fate and thinks that she cannot truly rely on anyone in the world, then an overabundance of stress can result in a full-fledged depression. At a certain point, the feeling of loss of control over life and defenselessness in the face of circumstances becomes overwhelming, and the woman is overcome by helplessness. And helplessness, in turn, is one of the main signs of depression.
But if she gets the impression that she is talking to the wall and no one pays attention to her, or that her efforts are taken for granted, then there is almost no chance of recharging dead batteries. If at the same time she feels cut off from other people and abandoned to her fate and thinks that she cannot truly rely on anyone in the world, then an overabundance of stress can result in a full-fledged depression. At a certain point, the feeling of loss of control over life and defenselessness in the face of circumstances becomes overwhelming, and the woman is overcome by helplessness. And helplessness, in turn, is one of the main signs of depression.
Study: women are more likely than men to experience severe stress at work and less satisfied with themselves
Stress factor: being married
It has been proven that married men are much less likely to become depressed than single men. Married women, on the other hand, are more likely to develop depression than unmarried women. Married women very often complain of friction and dissatisfaction with their relationship with their spouse. Quarrels, betrayal or misunderstanding on the part of a partner mean more stress for women than for men. Women seem to suffer from conflict and lingering relationship problems more than their partners. Research has repeatedly shown that there is a measurable relationship between relationship stress and physical symptoms. As mentioned above, happily married women are much less likely and to a lesser extent than unhappy women to have premenstrual syndrome. A failed marriage can also pose a significant danger to a woman's mental health: being unhappy in a marriage, women are much more likely than men to fall into depression. Thus, marriage appears to offer some protection to men, but not to women.
Married women, on the other hand, are more likely to develop depression than unmarried women. Married women very often complain of friction and dissatisfaction with their relationship with their spouse. Quarrels, betrayal or misunderstanding on the part of a partner mean more stress for women than for men. Women seem to suffer from conflict and lingering relationship problems more than their partners. Research has repeatedly shown that there is a measurable relationship between relationship stress and physical symptoms. As mentioned above, happily married women are much less likely and to a lesser extent than unhappy women to have premenstrual syndrome. A failed marriage can also pose a significant danger to a woman's mental health: being unhappy in a marriage, women are much more likely than men to fall into depression. Thus, marriage appears to offer some protection to men, but not to women.
Men are more likely than women to report that they feel that their spouse understands, supports and cares for them. For married men, the wife is often the only close person. How strong the need for men to have a wife nearby is shown by a series of longitudinal studies conducted in different countries: widowers are more likely to die than married men. For widows, such a dependence could not be established. Researchers Henk Schutt and Margarethe and Wolfgang Ströbe, who have been working on this topic for many years, found that "widowers are indeed at significantly greater risk than widows." Scientists explain this surprising finding by the fact that stable relationships have a protective effect on men. They receive emotional support and care mainly from their wife - and when she disappears from their lives, there is a palpable emptiness left behind. Among women, on the contrary, few people ever claim that they have the opportunity to rely on their legal spouse. They fail to find in their husband the readiness to lend a shoulder, to listen, to show the understanding they need. Apparently, therefore, the breakup or even death of a partner - despite all the suffering that such a blow of fate naturally causes - is not an equally strong stress factor for women and does not cause heavy damage to their health.
For married men, the wife is often the only close person. How strong the need for men to have a wife nearby is shown by a series of longitudinal studies conducted in different countries: widowers are more likely to die than married men. For widows, such a dependence could not be established. Researchers Henk Schutt and Margarethe and Wolfgang Ströbe, who have been working on this topic for many years, found that "widowers are indeed at significantly greater risk than widows." Scientists explain this surprising finding by the fact that stable relationships have a protective effect on men. They receive emotional support and care mainly from their wife - and when she disappears from their lives, there is a palpable emptiness left behind. Among women, on the contrary, few people ever claim that they have the opportunity to rely on their legal spouse. They fail to find in their husband the readiness to lend a shoulder, to listen, to show the understanding they need. Apparently, therefore, the breakup or even death of a partner - despite all the suffering that such a blow of fate naturally causes - is not an equally strong stress factor for women and does not cause heavy damage to their health.
Stress factor: motherhood
Research results confirm that the need to care for a small child in itself is a significant factor in the development of female depression. In many cases, the reason for this can be deep disappointment. Most couples form a family, firmly believing that they will share all responsibilities equally, as partners. However, reality looks different. After the birth of a child, the old traditional distribution of roles comes into force. The woman stays at home, the man becomes the sole breadwinner. New mothers are forced to put their career and life goals on hold indefinitely - and they often feel like they have to take care of their children alone, and it takes all their strength.
In addition, modern women believe that they must be ideal mothers. They strive to do everything right and perfect, as they are convinced that the well-being, success and mental health of the child depend solely on them. Of course, a mother (like a father) is largely responsible for her children and their development. However, the requirements that mothers make of themselves are sometimes overstated and unattainable: to be an impeccable "super mom" for a "super child" and prove to themselves and the whole world that they have everything under control.
Of course, a mother (like a father) is largely responsible for her children and their development. However, the requirements that mothers make of themselves are sometimes overstated and unattainable: to be an impeccable "super mom" for a "super child" and prove to themselves and the whole world that they have everything under control.
A mother of two teenage children and two grown-up children returned to work after a long break. She likes her work, but she notices that she has forgotten how to stand up for herself in the professional world. She lacks the former fighting fuse, she sees that she is not keeping up with her colleagues. She does not want to fight with them for a place in the sun, she does not like it. But at the same time, she wonders: is she setting a good example for her children? Maybe she should have made her way more actively, behaved in a combative way? Less retreat and more successful in defending your interests, despite resistance? At the same time, she worries more about her children than about herself. They have just reached the age at which it is time to start building a career. How will they succeed if their mother isn't their role model, she wonders. Can she instill in them the grip they need? The father of the children - he could, but he left the family many years ago. She feels that she cannot do this task alone, but she believes that she is obliged to do it.
They have just reached the age at which it is time to start building a career. How will they succeed if their mother isn't their role model, she wonders. Can she instill in them the grip they need? The father of the children - he could, but he left the family many years ago. She feels that she cannot do this task alone, but she believes that she is obliged to do it.
From the very beginning, motherhood has high expectations from women, expectations that were not there in the past. As the French writer and philosopher Elisabeth Badenter argues, women today need more time and energy to raise two children than it took a mother of six years ago. “Immediately after the birth of a child, feats are expected from her. Nowadays, a good mother should be ready to breastfeed her baby whenever he demands it. This means that from the very beginning she is at the disposal of the baby at any time of the day or night, and the child takes a place in the parental bed between the adults.
Women are afraid of making the slightest mistake in upbringing and are very passionate about early development. It is now rare that young children are sent outside to play or left unsupervised for hours in the company of siblings or neighborhood children. Today, mothers are expected to closely monitor their child's academic progress, actively participate in his life and play the role of a chauffeur with him. Otherwise, how can he get into all his circles (football training, music school, tutoring, fencing lesson ...)?
Motherhood has become a profession that requires a lot of knowledge and skills, but brings almost no recognition. What mothers do is taken for granted by others. To make matters worse, most women tend to do this work alongside their main job—and this leads to internal divisions and constant remorse. Many working mothers constantly lack energy and time, and they think that they cannot fully cope with either raising a child or with professional responsibilities.