Criteria for persistent depressive disorder
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.
-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly. Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Medicine, pharmacy and healthcare news
Portal map
- Media - News
- Press Releases
- Pharmacists
- Doctors
- Obstetrics and gynecology
- Allergology
- Gastroenterology
- Hepatology
- Dermatology
- Dietetics
- Infectious diseases
- Research and development
- Cardiology
- Neurology
- Oncology
- Otorhinolaryngology
- Pediatrics
- Psychiatry
- Psychology
- Pulmonology
- Rheumatology
- Dentistry
- Therapy
- Traumatology
- Urology
- Surgery
- Endocrinology
- Health professionals
- Pharmaceutical market
- Industry
- Pharmaceutical industry
- Medical equipment +
- Legal Chronicle
- Analytics
- Legislation
- Documents for pharmacies
- Health records
- Miscellaneous documents
- Medical publications
- Magazines
- Books
- Activities
- Company profile
- About the project
- Advertising
- Contacts
- Search
- English
| Login: | |
| Password: | |
| Remember me | |
| Registration | |
| Forgot your password? | |
Subscription Online
Books Magazines
News
October 14, 2022
Vaccines against COVID-19 can be modified
The Ministry of Health has developed amendments that allow changing the composition of vaccine strains for the prevention of COVID-19.
More
October 14, 2022
A meeting was held at the highest medical level
October 14, 2022
The Russian Ministry of Health has registered a new drug for the treatment of covid
/upload/medialibrary/605/kr_cogn_gl_3.pdf
Doctors
October 14, 2022
Dental anomalies: classification, causes and treatment
The close relationship between oral, systemic and psychological health requires...
More
October 13, 2022
Painful sexual disorder
October 11, 2022
Diagnosis of disorders in the coagulation system, assessment of the risk of hemorrhagic complications in severe cirrhosis/liver diseases according to global screening tests of the hemostasis system and principles for their correction: guidelines
Pharmacists
August 30, 2022
Release of a large number of packages of an OTC drug at once
A customer asked for 20 packs of OTC, but the man following her. ..
..
More
August 9, 2022
Stuffy in the trading floor of the pharmacy - improving working conditions in such a situation
July 13, 2022
Contest #SotexResponsible 2022: second stage
DEPRESSION IN SOMATIC DISEASES (DIAGNOSIS AND TREATMENT)
Dr. A. B. Smulevich - Dr. med. sciences, professor, director of Department borderline mental pathology and Psychomatic Disorders Research Institute Clinical Psychiatry NCPZ RAMS
Dr. M. Yu. Drobizhev - Ph.D. Honey. Sciences, leading researcher of the same branches
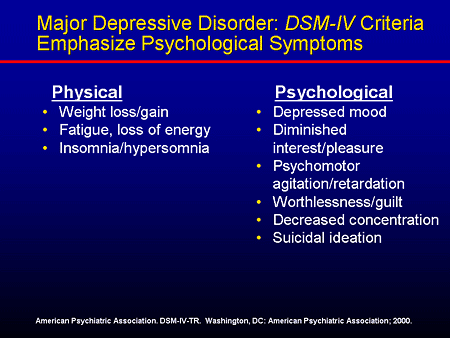
C among mental disorders seen in patients with topical somatic disease (SZ), most common depressive states. According to some authors [11, 17], according to the frequency manifestations, varying from 14 to 46% (Table 1), affective (depressive) syndromes in patients SZ can only be compared with dyssomnic disorders. However, how about evidence from a number of publications related to recent decades, there is also the danger of overdiagnosis depression in patients with SZ [8,14,15]. Traditionally, the composition clinical manifestations of depression includes disorders characteristic and for somatic disease (asthenia, weight loss, sleep disturbances, dizziness, tremor, tachycardia, chest pain cell, dyspnea, dyspeptic disorders - bitterness, dryness in mouth, constipation, flatulence, etc.). Differences in diagnostic approaches to such "common" for affective and somatic pathology symptom complexes in primarily reflected in prevalence rates depression in patients SZ (see diagram).
According to some authors [11, 17], according to the frequency manifestations, varying from 14 to 46% (Table 1), affective (depressive) syndromes in patients SZ can only be compared with dyssomnic disorders. However, how about evidence from a number of publications related to recent decades, there is also the danger of overdiagnosis depression in patients with SZ [8,14,15]. Traditionally, the composition clinical manifestations of depression includes disorders characteristic and for somatic disease (asthenia, weight loss, sleep disturbances, dizziness, tremor, tachycardia, chest pain cell, dyspnea, dyspeptic disorders - bitterness, dryness in mouth, constipation, flatulence, etc.). Differences in diagnostic approaches to such "common" for affective and somatic pathology symptom complexes in primarily reflected in prevalence rates depression in patients SZ (see diagram).
Presented data allow us to state that diagnosis validation depression in patients with current SZ requires clear differential diagnostic criteria 1 . In our opinion, must be taken into account at least at least three circumstances: features of psychopathological disorders, history and hereditary burden, nature of psychosomatic correlations (ratio between expression, dynamics mental disorders and relevant indicators somatic disease - tab. 2).
In our opinion, must be taken into account at least at least three circumstances: features of psychopathological disorders, history and hereditary burden, nature of psychosomatic correlations (ratio between expression, dynamics mental disorders and relevant indicators somatic disease - tab. 2).
Necessary emphasize that the nature of depression, comorbid with topical SZ, heterogeneous. Respectively nosology of depression not limited to somatogenic depression (affective disorder, directly associated with the course of SZ, for example, with atherosclerosis of the cerebral vessels brain). Along with them, there are also nosogenic depressions [4] (depressive reactions to constellation psychogenic and situational factors related to semantic significance of di- agnosia, awareness of danger diseases, physical suffering, quality change life), dysthymia (protracted neurotic depression) endogenous depression. At the same time, as seen from the table. 3, among affective (depressive) disorders predominate nosogenic depressions (depression, hopelessness, anxiety, pessimistic assessment
table 1. Prevalence of depressive conditions (DS) in patients somatic hospital
Prevalence of depressive conditions (DS) in patients somatic hospital
| Authors, year | Volume sample (number of patients) | Frequency DC, % |
| Maguire, et al., 1974 | 230 | 23 |
| Moffic and Paykel, 1975 | 100 | 19 |
| Knights and Folstein, 1977 | 57 | 46 |
| Cavanaugh, 1983 | 335 | 32 | Feidman
| et al., 1985 | 453 | 14. 6 6 |
| Levenson et al., 1987 | 253 | 23 |
| Kathol et al., 1990 | 151 | 44 |
own somatic condition and prospects for improvement in future). The prevalence of the latter over depressions of other genesis confirmed in several studies [15,19].
Turning to basic principles therapy for depression, comorbid current SZ, it is necessary emphasize the expediency use of a wide range therapeutic interventions, including as different methods of psychotherapy, and psychotropic drugs. The use of psychotherapy most appropriate for nosogenic depressions psychogenic/situational conditional disorders (group and individual classes in technology self-regulation" - autogenous exercise, breathing and relaxation therapeutic gymnastics, various techniques neurolinguistic programming) [11].
Among antidepressants, traditionally used in the treatment of depression in somatic patients, point to tricyclic drugs (TCAs): melipramine (imipramine), anafranil, amitriptyline, nortriptyline. Recommending TCAs, many authors [9, 12] indicate not only a high thymoleptic activity, covering the entire spectrum depressive states, observed in the considered patient population (somatogenic, nosogenic depression, dysthymia, endogenous depressive disorders), but also the potential to provide positive therapeutic effect on some symptoms SZ. Thus, it has been shown that imipramine and nortriptyline is effective in ventricular extrasystoles [12]. S. Conolly et al. [9] found that taking imipramine in average therapeutic dose makes it difficult to induce ventricular paroxysm tachycardia with electrophysiological research. Showcased reduction in the frequency of episodes ventricular fibrillation in experimental infarction myocardium against the background of the introduction of TCA and tendency to spontaneous relief of emerging episodes arrhythmias [16]. shown also beneficial effect of TCAs with symptoms of bronchospasm patients with bronchial asthma [13].
shown also beneficial effect of TCAs with symptoms of bronchospasm patients with bronchial asthma [13].
Table 2. Diagnostic criteria depression, comorbid SD
| (1) Mental status |
| Features hypothymia (sadness, anxiety, apathy, anhedonia, intellectual and motor inhibition) whose intensity obeys the circadian rhythm |
| Phenomena alienation in the form depressive anesthesia (feeling sore insensibility) and depression devitalization (weakening or disappearance of vital attraction - attraction to life, self-preservation instinct, somatosensory drives sleep deprivation, appetite) |
| Availability depressive meaningful complex (denotata) |
1. Ideas worthlessness, guilt, damage reflecting self-consciousness disorder form of discontinuity "I" (persistent thinking with negative evaluation of the past, present and prospects for Ideas worthlessness, guilt, damage reflecting self-consciousness disorder form of discontinuity "I" (persistent thinking with negative evaluation of the past, present and prospects for future) |
| 2. Suicidal thoughts |
| 3. Hypochondriacal ideas: dominant ideas about danger (usually exaggerated) somatic illness, unfavorable outcome and futility treatment, negative social consequences; anxiety and fears (up to phobias), not related to the current SZ and relating to functioning of various internal organs and body overall |
| (2) History, premorbid, heredity |
| Depressive and hypomanic states in history |
| Cycloid, hyperthymic, anxious suspicious, hysterical and schizoid constitutional warehouse with reactive lability (tendency to affective disorders) |
| Depressive conditions and suicides in the nearest relatives |
| (3) Violation of psychosomatic correlations |
| Mismatch manifestations of somatovegetative severity disorders and the nature of the SZ (for example, a sharp weight loss and menstrual disorder cycle in hyperthyroidism, despite the slight increase in hormone levels thyroid gland in the blood prolonged algia in the chest cage, uncharacteristic for angina voltage, persistent asthenia unexpressed iron deficiency anemia or prolonged agrypnia in the absence of night asthma attacks, angina). |
| Mismatch dynamics of somatovegetative disorders of the nature of the course CV (for example, persistent nausea, pain in the upper half of the abdomen, no appetite and others gastrointestinal complaints with a healed ulcer stomach or duodenum, asthenia, sleep disorders, decreased libido, anhedonia, persisting in clinical picture, despite the successful treatment of hypothyroidism) |

| Table 3. Nosology of depression in patients somatic hospital | |||
| Diagnosis | Frequency, % | ||
M. E. Stewart et al. [19] E. Stewart et al. [19] | by N. E. Koenig and et al. (15] | own data | |
| Somatogenic depression (organic affective disorder) | - | 1 | 1.4 |
| Depressive reactions: nosogenic other | 17 10 | 14 0.6 | 10 2 |
| Dysthymia | - | 2 | 4 |
| Endogenous depression (major) depressive episode, cyclothymia) | 3 | 9 | 2 |
Table 4. Comparison of fluoxetine and TCA clinical relevance effects on cardiovascular system Comparison of fluoxetine and TCA clinical relevance effects on cardiovascular system | ||
| Symptoms | Fluoxetine | TCA |
| Bradycardia | Moderate | Moderate |
| Decreased blood pressure | Moderate | Moderate |
| Tachycardia | Not specific | Typical |
| Orthostatic hypotension | Not specific | Typical |
| Rhythm disturbances heart and conduction | Not specific | Characteristic |
Table 5. Comparison of fluoxetine and TCA clinical relevance drug interactions, used for the treatment of SZ Comparison of fluoxetine and TCA clinical relevance drug interactions, used for the treatment of SZ | ||
| Preparations, used in therapy | Fluoxetine | TCA. |
| Thyroid hormones | Not interacts | Violations heart rate |
| Methyltestosterone | No data | Disorder consciousness |
| Sympathomimetics | Not interacts | Hypertension |
| Antiarrhythmic class 1 drugs (quinidine, novocainamide, etc.) | Also | Toxic effect |
| Hypotensive preparations | " " | Orthostatic hypotension |
| Cardiac glycosides | " " | Bradycardia |
| Anticholinergics funds | " " | Gain tachycardia, accommodation spasm etc. |
However, the use of TCAs in somatic patients is associated with a number of restrictions associated with pronounced anticholinergic action (Table 4). Introduction of drugs this group is accompanied by side effects: drowsiness during the day, disruption sensorimotor functions (coordination movements, attention, etc.), as well as bradycardia, decreased blood pressure (BP), orthostatic hypotension, dry mucous membranes, urinary retention, constipation. In addition, TCAs are quite often enter into unwanted interactions with somatotropic drugs (Table 5) - thyroid and steroid hormones, antiarrhythmic drugs first class, cordial glycosides, etc. 2 .
In connection with the specified properties TCA is an obvious need introduction to the arsenal of psychotropic drugs used in patients with SD, drugs with minimal behavioral toxicity 3 , whose clinical effect is not accompanied by complications and negative impact on the course of SZ, and interaction with somatotropic drugs is limited character.
Among antidepressants, satisfying the specified requirements, in recent decades are widely distribution inhibitors serotonin reuptake (fluoxetine, sertalin, etc.), polycyclic drugs structures (ludiomil, lerivon, pyrazidol), reversible inhibitors monoamine oxidase (MAO) type A short action [18].
Positive qualities selective inhibitors of the reverse serotonin uptake - no side effects characteristic of TCAs, therapeutically significant interactions with a wide range drugs used in therapy (see Tables 4 and 5). Border guard staff mental illness and Psychosomatic Disorders Research Institute Clinical Psychiatry NTSPZ RAMS tested fluoxetine (Prozac, Eli Lilly) for psychogenic (nosogenic) depressive states of severity not less than 11 on the depression scale Hospital Anxiety Questionnaire and depression [20]. In the study patients participated in aged 21-65 years, who were on inpatient treatment for coronary artery disease (patients predominated with II - III functional class angina, have also been observed patients with acute myocardial infarction myocardium, with unstable and progressive angina) base of the Moscow Medical academy.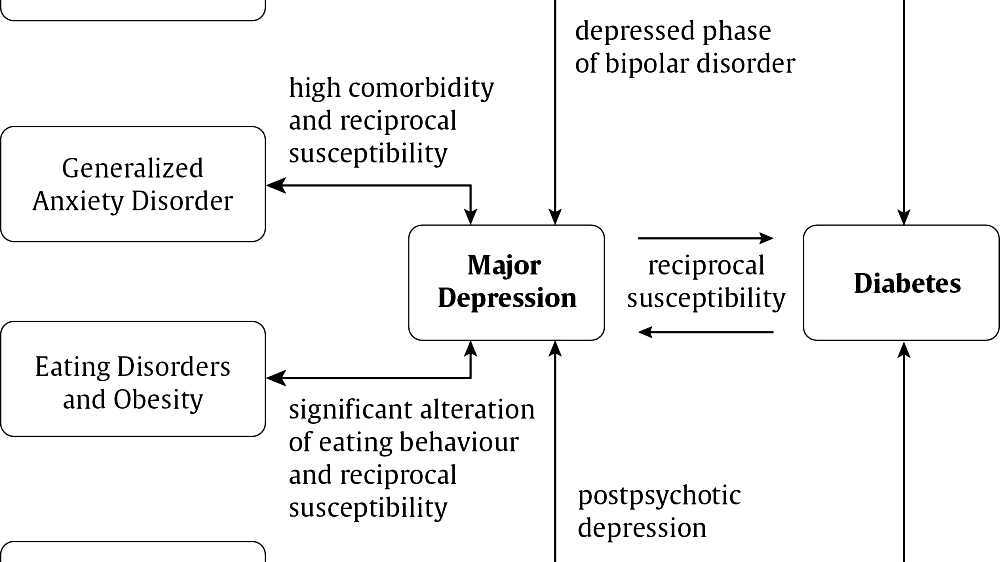 I. M. Sechenova (Department of Coronary Heart Disease, I.M. Sechenov - Head Corresponding Member. RANS prof. A.L. Syrkin). Trial showed high safety and good tolerance of the drug, no adverse interactions with cardiotropic medicines 4 . Not deterioration in somatic state that could be due to the influence of fluoxetine. No significant adverse impact drug on ECG parameters, blood test scores. Not unfavorable interactions with nitrates prolonged action beta blockers, calcium channel blockers, cardiac glycosides, antiarrhythmic drugs.
I. M. Sechenova (Department of Coronary Heart Disease, I.M. Sechenov - Head Corresponding Member. RANS prof. A.L. Syrkin). Trial showed high safety and good tolerance of the drug, no adverse interactions with cardiotropic medicines 4 . Not deterioration in somatic state that could be due to the influence of fluoxetine. No significant adverse impact drug on ECG parameters, blood test scores. Not unfavorable interactions with nitrates prolonged action beta blockers, calcium channel blockers, cardiac glycosides, antiarrhythmic drugs.
A number of general properties of preparations polycyclic structure (ludiomil, larivon, pyrazidol) - insignificant effect on blood pressure [10], intraocular pressure, prostate and etc. - allows to consider such antidepressants as drug of choice for treatment depression in patients with somatic pathology. Especially domestic is preferred the drug pyrazidol, which virtually no effect on blood pressure conduction system of the heart completely devoid of anticholinergic properties (does not cause dryness mucous membranes, spasm accommodation, constipation, etc. ).
).
About prospects use of reversible MAO inhibitors in SD, including glaucoma, prostate adenoma, and also in the physically handicapped patients, the elderly, testify to a short withdrawal period, almost complete lack of clinically significant side effects (noted only mild hypotension) [6]. In a row drugs of the considered group should be called moclobemide (Aurorix, Roche). Orthostatic hypotension while using such a drug is observed even less than placebo (correspondingly 2 - 3% against 5%).
For the treatment of depression, comorbid ST, along with antidepressants within combination therapy widely also use tranquilizers and nootropic drugs - Valium, lexotan, lorazepam, alprazolam, phenazepam, nootropil. Finally, in last decade wide widespread drugs, spectrum of clinical whose actions include affective (depressive) disorders, and manifestations of SD. To such drugs may be assigned derivative adenosylmethionine - Heptral (Knoll), sulpiride (Eglonil, Synthelabo, calcium channel blocker nifedipine [5], verapamil [3].
Heptral not only has thymoleptic properties, but also effective in the syndrome intrahepatic cholestasis, due to cirrhosis of the liver chronic active hepatitis [1], cystic fibrosis 12]. His appointment especially justified in patients with depressive states, comorbid liver diseases. In a study conducted in department of borderline mental pathology and psychosomatic disorders Research Institute of Clinical psychiatry NTsPZ RAMS, drug demonstrated high safety indicators, consistent with literature data [7].
Application of this antidepressant also not accompanied by any hematological and biochemical changes.
Sulpiride along with stimulant and thymoleptic effect improves blood supply to the stomach, intestines, accelerating recovery processes in tissues, suppresses gastric secretion, antiemetic action.
Use of sulpiride indicated for depression comorbid peptic ulcer with localization of the process in the stomach or duodenum (both in acute and in chronic ulcerative process) ulcerative colitis, Crohn's disease and "operated stomach". It should be noted that when taking drug possible violations menstrual cycle, galactorrhea.
It should be noted that when taking drug possible violations menstrual cycle, galactorrhea.
Nifedipine and verapamil, which used for prevention angina attacks, treatment hypertension, as well as as part of combination therapy chronic cardiac deficiencies, have normothymic properties, and, therefore, are drug of choice for secondary prevention of phasic affective (depressive) disorders that develop patients with ST 5 .
Abstract
| Depressive disorders are the most common among mental disorders observing in patients with an urgent somatic disease (SD). The nosological entities of these depressions are not confined to somatogenic depressions (affective disorders directly related to the course of SD, such as with cerebral vascular atherosclerosis). Along with them there are also nosogenic depressions (depressive responses to a constelation of psychogenic and situational factors associated with the symptomatic value of a diagnosis, with the awareness of a risk for the disease, physical sufferings, with changes in the quality of life), dysthymias (chronic neurotic depressions), endogenous depressions.  The differentially diagnostic criteria which validate the diagnosis of depression in SD patients have been proposed. The differentially diagnostic criteria which validate the diagnosis of depression in SD patients have been proposed. These include the specific features of pathophysiological disorders, history and family data, the nature of somatomental correlations (relationships between the severity, dynamics of mental disorders and the relative characteristics of SD). The paper discusses the basic principles of the therapy for depression related to an urgent SD and emphasizes it necessary to use antidepressants of different chemical groups with regard to the profile of their therapeutic effects, the nature of adverse reactions, the interactions with the drugs used in the treatment of SD. |
1 Hereinafter provides data on depression conditions, comorbid current SZ. Wherein affective (depressive) disorders (main diagnosis), flowing "under the mask" somatic disease, called "somatized" depression, the study of which an extensive literature is devoted to this article is not are considered.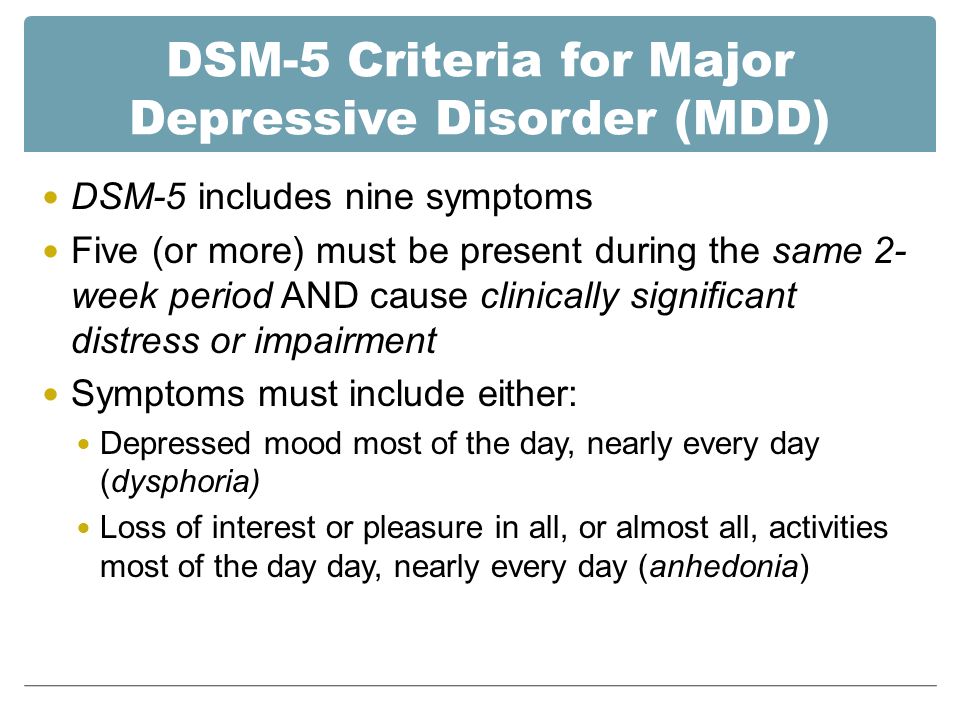
2 Equity for the sake of it should be said that there were new TCAs, distinctive whose features are safety and good portability. One of these drugs-tianeptine (Coaxil, server).
3 I mean overwhelming effect of the drug on daily activity, associated with daytime sleepiness deterioration in memory, attention, slowing down sensorimotor reactions.
4 Preparation also has moderate neuroleptic activity.
5 Lithium salts, widely used for prevention of affective disorders, contraindicated patients with disorder concentration function of the kidneys, thyroid disease, with cardiovascular disease, associated with violation water and electrolyte balance, in individuals with hypertension, on a salt-free diet patients taking cardiac glycosides, beta-blockers, thiazide derivatives.
Literature:
1. Loginov A. S., Ilchenko L. Yu., Petrakov A. V. Treatment of liver damage in drug addicts// Abstracts III Russian National congress "Man and medicine" - RC. "Pharmedinfo" M., 1996.-S. 155-6.
"Pharmedinfo" M., 1996.-S. 155-6.
2. Orlov V. A., Nikitina M. I. The use of heptral (ademetionine) with cystic fibrosis in children // Abstracts reports of the III Russian national congress "Man and medicine" - RC. "Farmedinfo" M., 1996. - S. 177.
3. Panteleeva G. P., Rayushkin V. A., Snedkova L. V. Use as calcium antagonists thymostabilizers// Abstracts reports of the III Russian national congress "Man and medicine" - RC."Pharmedinfo" M., 1996. P.183.
4. Smulevich A. B. Psychic pathology and ischemic disease hearts (to the problem nosogeny)//Mental disorders and cardiovascular pathology / Ed. A. B. Smulevich and A. L. Syrkina. - Libris, M., 1994. - S. 12-19.
5. Snedkova L. V. Application experience calcium channel blocker nifedipine for prophylaxis relapses of affective and schizoaffective psychosis//Journal. Neuropatol. and Psychiatrist. them. S. S. Korsakov. - 1996. -T. 96.-№1.-S. 61-6.
6. Burchard P, Bonetty EP, Daparada M, et al. Pharmacological profile of moclobemide, a shortacting and reversible inhibitor of monoamine oxidase type A//Pharmacol. and Exp. Therap. 1989:284:391-9.
and Exp. Therap. 1989:284:391-9.
7. Carney NWP. Neuropharmacology of S-adenosyl Methionine//Clin. Neuropharmacol 1986:9:235-43.
8. Clark DC, Cavanaugh S. von A., Gibbons R.D. The core symptoms of depression in medical and psychiatric patients//J. Nerv. Ment. Dis. 1983:171:705-13.
9. Connolly SJ, Mitthell B, Swerolow CP, et al. Clinical efficiany electrophisiology of.imipramine for ventricular tachycardia//Am. J. Cardiol 1984:53:516-21.
10. Coopen A, Kopera H. Workshop on the clinical pharmacology and efficacy of mianserin//Brit.J. Clin. Pharmacol. 1978;5.(Suppl.):91-9.
11. Derogatis L.R., Wise T.N. Anxiety and depression disorders in the medical patients//American Psychiatric Press, Inc., Washington D.C., 1989:119.
12. Giardina E.-G.V., Bigger J.I., Glassman A.H. et al. The electrocardigrafic and antiarrythmic effects of imipramine hydrochloride et therapeutic plasma concentration//Circulation. 1979:60:1045-52.
13. Goodman TA, Tupin JP. The psychology of asthma: implications for treatment//Bronchial asthma/Ed. M.E. Gershwin - Orlando, EL. - Grune & Stratton. - 1986:541-60.
M.E. Gershwin - Orlando, EL. - Grune & Stratton. - 1986:541-60.
14. Kathol RG, Noyes R. Jr, Williams J, et al. Diagnosing depression in patients with medical illness//Psychosomatics-1990:31:4:434-40.
15. Koenig HG, Meador KG, Cohen HJ, Blazer DG. Depression in elderly hospitalized patients with medical illness//Arch. Intern. Med. 1988:148:1929-36.
16. Manoach M, Netz H, Varon D, et al. The effect of trycyclic antidepressants on ventricular fibrillation and collatreral blood supply acute coranary occlusion//Heart and vessels - 1986:2:1:36-40.
17. Mayou R, Hawton K. Psychiatric disorders in general hospital//Brit. J. Psychiat. 1986:149:117-90.
18. Rudorfer MV, Potter WZ. Antidepressants: a comparison review of the clinical pharmacology and therapeutic use of the "newer" versus "older" drugs//Drugs. 1989:37:713-38.
19. Stewart MA, Drake F, Winokur G. Depression among medically ill patients//Pract. J. Psychiat. Neurol. 1965:26:8:479-85.
20. Zigmond AS, Snaith RP.