Bipolar disorder mood stabilizers
Bipolar disorder - Diagnosis and treatment
Diagnosis
To determine if you have bipolar disorder, your evaluation may include:
- Physical exam. Your doctor may do a physical exam and lab tests to identify any medical problems that could be causing your symptoms.
- Psychiatric assessment. Your doctor may refer you to a psychiatrist, who will talk to you about your thoughts, feelings and behavior patterns. You may also fill out a psychological self-assessment or questionnaire. With your permission, family members or close friends may be asked to provide information about your symptoms.
- Mood charting. You may be asked to keep a daily record of your moods, sleep patterns or other factors that could help with diagnosis and finding the right treatment.
- Criteria for bipolar disorder. Your psychiatrist may compare your symptoms with the criteria for bipolar and related disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Diagnosis in children
Although diagnosis of children and teenagers with bipolar disorder includes the same criteria that are used for adults, symptoms in children and teens often have different patterns and may not fit neatly into the diagnostic categories.
Also, children who have bipolar disorder are frequently also diagnosed with other mental health conditions such as attention-deficit/hyperactivity disorder (ADHD) or behavior problems, which can make diagnosis more complicated. Referral to a child psychiatrist with experience in bipolar disorder is recommended.
Care at Mayo Clinic
Our caring team of Mayo Clinic experts can help you with your bipolar disorder-related health concerns Start Here
More Information
- Bipolar disorder care at Mayo Clinic
- Bipolar in children
- Urinalysis
Treatment
Treatment is best guided by a medical doctor who specializes in diagnosing and treating mental health conditions (psychiatrist) who is skilled in treating bipolar and related disorders. You may have a treatment team that also includes a psychologist, social worker and psychiatric nurse.
You may have a treatment team that also includes a psychologist, social worker and psychiatric nurse.
Bipolar disorder is a lifelong condition. Treatment is directed at managing symptoms. Depending on your needs, treatment may include:
- Medications. Often, you'll need to start taking medications to balance your moods right away.
- Continued treatment. Bipolar disorder requires lifelong treatment with medications, even during periods when you feel better. People who skip maintenance treatment are at high risk of a relapse of symptoms or having minor mood changes turn into full-blown mania or depression.
- Day treatment programs. Your doctor may recommend a day treatment program. These programs provide the support and counseling you need while you get symptoms under control.
-
Substance abuse treatment. If you have problems with alcohol or drugs, you'll also need substance abuse treatment.
 Otherwise, it can be very difficult to manage bipolar disorder.
Otherwise, it can be very difficult to manage bipolar disorder. - Hospitalization. Your doctor may recommend hospitalization if you're behaving dangerously, you feel suicidal or you become detached from reality (psychotic). Getting psychiatric treatment at a hospital can help keep you calm and safe and stabilize your mood, whether you're having a manic or major depressive episode.
The primary treatments for bipolar disorder include medications and psychological counseling (psychotherapy) to control symptoms, and also may include education and support groups.
Medications
A number of medications are used to treat bipolar disorder. The types and doses of medications prescribed are based on your particular symptoms.
Medications may include:
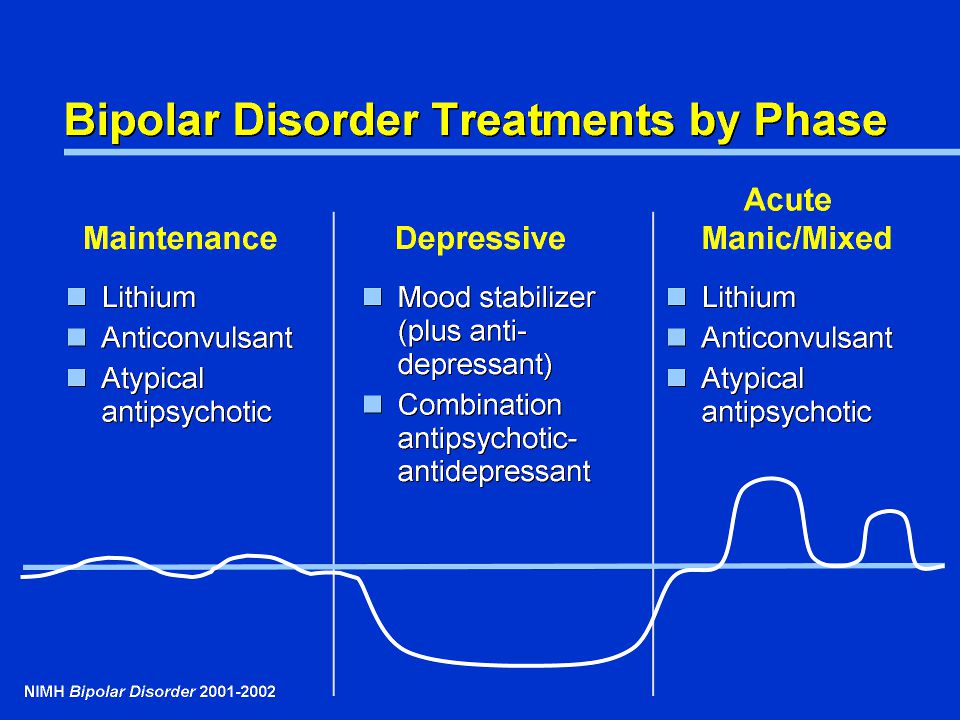
- Mood stabilizers. You'll typically need mood-stabilizing medication to control manic or hypomanic episodes. Examples of mood stabilizers include lithium (Lithobid), valproic acid (Depakene), divalproex sodium (Depakote), carbamazepine (Tegretol, Equetro, others) and lamotrigine (Lamictal).
- Antipsychotics. If symptoms of depression or mania persist in spite of treatment with other medications, adding an antipsychotic drug such as olanzapine (Zyprexa), risperidone (Risperdal), quetiapine (Seroquel), aripiprazole (Abilify), ziprasidone (Geodon), lurasidone (Latuda) or asenapine (Saphris) may help. Your doctor may prescribe some of these medications alone or along with a mood stabilizer.
- Antidepressants. Your doctor may add an antidepressant to help manage depression. Because an antidepressant can sometimes trigger a manic episode, it's usually prescribed along with a mood stabilizer or antipsychotic.
- Antidepressant-antipsychotic. The medication Symbyax combines the antidepressant fluoxetine and the antipsychotic olanzapine. It works as a depression treatment and a mood stabilizer.
- Anti-anxiety medications. Benzodiazepines may help with anxiety and improve sleep, but are usually used on a short-term basis.
Finding the right medication
Finding the right medication or medications for you will likely take some trial and error. If one doesn't work well for you, there are several others to try.
This process requires patience, as some medications need weeks to months to take full effect. Generally only one medication is changed at a time so that your doctor can identify which medications work to relieve your symptoms with the least bothersome side effects. Medications also may need to be adjusted as your symptoms change.
Side effects
Mild side effects often improve as you find the right medications and doses that work for you, and your body adjusts to the medications. Talk to your doctor or mental health professional if you have bothersome side effects.
Don't make changes or stop taking your medications. If you stop your medication, you may experience withdrawal effects or your symptoms may worsen or return. You may become very depressed, feel suicidal, or go into a manic or hypomanic episode.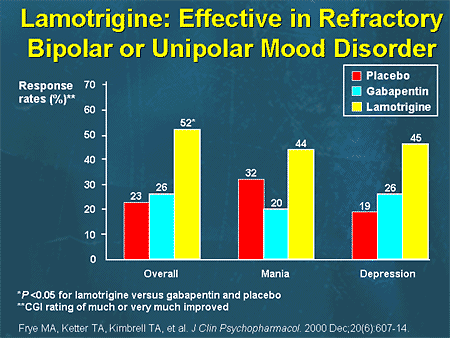 If you think you need to make a change, call your doctor.
If you think you need to make a change, call your doctor.
Medications and pregnancy
A number of medications for bipolar disorder can be associated with birth defects and can pass through breast milk to your baby. Certain medications, such as valproic acid and divalproex sodium, should not be used during pregnancy. Also, birth control medications may lose effectiveness when taken along with certain bipolar disorder medications.
Discuss treatment options with your doctor before you become pregnant, if possible. If you're taking medication to treat your bipolar disorder and think you may be pregnant, talk to your doctor right away.
Psychotherapy
Psychotherapy is a vital part of bipolar disorder treatment and can be provided in individual, family or group settings. Several types of therapy may be helpful. These include:
- Interpersonal and social rhythm therapy (IPSRT). IPSRT focuses on the stabilization of daily rhythms, such as sleeping, waking and mealtimes.
 A consistent routine allows for better mood management. People with bipolar disorder may benefit from establishing a daily routine for sleep, diet and exercise.
A consistent routine allows for better mood management. People with bipolar disorder may benefit from establishing a daily routine for sleep, diet and exercise. - Cognitive behavioral therapy (CBT). The focus is identifying unhealthy, negative beliefs and behaviors and replacing them with healthy, positive ones. CBT can help identify what triggers your bipolar episodes. You also learn effective strategies to manage stress and to cope with upsetting situations.
- Psychoeducation. Learning about bipolar disorder (psychoeducation) can help you and your loved ones understand the condition. Knowing what's going on can help you get the best support, identify issues, make a plan to prevent relapse and stick with treatment.
- Family-focused therapy. Family support and communication can help you stick with your treatment plan and help you and your loved ones recognize and manage warning signs of mood swings.
Other treatment options
Depending on your needs, other treatments may be added to your depression therapy.
During electroconvulsive therapy (ECT), electrical currents are passed through the brain, intentionally triggering a brief seizure. ECT seems to cause changes in brain chemistry that can reverse symptoms of certain mental illnesses. ECT may be an option for bipolar treatment if you don't get better with medications, can't take antidepressants for health reasons such as pregnancy or are at high risk of suicide.
Transcranial magnetic stimulation (TMS) is being investigated as an option for those who haven't responded to antidepressants.
Treatment in children and teenagers
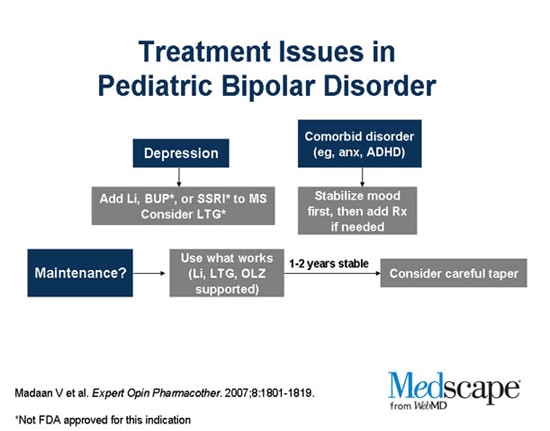
Treatments for children and teenagers are generally decided on a case-by-case basis, depending on symptoms, medication side effects and other factors. Generally, treatment includes:
- Medications. Children and teens with bipolar disorder are often prescribed the same types of medications as those used in adults. There's less research on the safety and effectiveness of bipolar medications in children than in adults, so treatment decisions are often based on adult research.
- Psychotherapy. Initial and long-term therapy can help keep symptoms from returning. Psychotherapy can help children and teens manage their routines, develop coping skills, address learning difficulties, resolve social problems, and help strengthen family bonds and communication. And, if needed, it can help treat substance abuse problems common in older children and teens with bipolar disorder.
- Psychoeducation. Psychoeducation can include learning the symptoms of bipolar disorder and how they differ from behavior related to your child's developmental age, the situation and appropriate cultural behavior. Understanding about bipolar disorder can also help you support your child.
- Support. Working with teachers and school counselors and encouraging support from family and friends can help identify services and encourage success.
More Information
- Bipolar disorder care at Mayo Clinic
- Bipolar medications and weight gain
- Bipolar treatment: I vs.
 II
II - Cognitive behavioral therapy
- Electroconvulsive therapy (ECT)
- Family therapy
- Psychotherapy
- Transcranial magnetic stimulation
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which
information is beneficial, we may combine your email and website usage information with
other information we have about you. If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Lifestyle and home remedies
You'll probably need to make lifestyle changes to stop cycles of behavior that worsen your bipolar disorder. Here are some steps to take:
- Quit drinking or using recreational drugs. One of the biggest concerns with bipolar disorder is the negative consequences of risk-taking behavior and drug or alcohol abuse. Get help if you have trouble quitting on your own.
- Form healthy relationships. Surround yourself with people who are a positive influence. Friends and family members can provide support and help you watch for warning signs of mood shifts.
- Create a healthy routine.
 Having a regular routine for sleeping, eating and physical activity can help balance your moods. Check with your doctor before starting any exercise program. Eat a healthy diet. If you take lithium, talk with your doctor about appropriate fluid and salt intake. If you have trouble sleeping, talk to your doctor or mental health professional about what you can do.
Having a regular routine for sleeping, eating and physical activity can help balance your moods. Check with your doctor before starting any exercise program. Eat a healthy diet. If you take lithium, talk with your doctor about appropriate fluid and salt intake. If you have trouble sleeping, talk to your doctor or mental health professional about what you can do. - Check first before taking other medications. Call the doctor who's treating you for bipolar disorder before you take medications prescribed by another doctor or any over-the-counter supplements or medications. Sometimes other medications trigger episodes of depression or mania or may interfere with medications you're taking for bipolar disorder.
- Consider keeping a mood chart. Keeping a record of your daily moods, treatments, sleep, activities and feelings may help identify triggers, effective treatment options and when treatment needs to be adjusted.
Alternative medicine
There isn't much research on alternative or complementary medicine — sometimes called integrative medicine — and bipolar disorder. Most of the studies are on major depression, so it isn't clear how these nontraditional approaches work for bipolar disorder.
Most of the studies are on major depression, so it isn't clear how these nontraditional approaches work for bipolar disorder.
If you choose to use alternative or complementary medicine in addition to your physician-recommended treatment, take some precautions first:
- Don't stop taking your prescribed medications or skip therapy sessions. Alternative or complementary medicine is not a substitute for regular medical care when it comes to treating bipolar disorder.
- Be honest with your doctors and mental health professionals. Tell them exactly which alternative or complementary treatments you use or would like to try.
- Be aware of potential dangers. Alternative and complementary products aren't regulated the way prescription drugs are. Just because it's natural doesn't mean it's safe. Before using alternative or complementary medicine, talk to your doctor about the risks, including possible serious interactions with medications.
Coping and support
Coping with bipolar disorder can be challenging. Here are some strategies that can help:
- Learn about bipolar disorder. Education about your condition can empower you and motivate you to stick to your treatment plan and recognize mood changes. Help educate your family and friends about what you're going through.
- Stay focused on your goals. Learning to manage bipolar disorder can take time. Stay motivated by keeping your goals in mind and reminding yourself that you can work to repair damaged relationships and other problems caused by your mood swings.
- Join a support group. Support groups for people with bipolar disorder can help you connect to others facing similar challenges and share experiences.
- Find healthy outlets. Explore healthy ways to channel your energy, such as hobbies, exercise and recreational activities.
- Learn ways to relax and manage stress.
 Yoga, tai chi, massage, meditation or other relaxation techniques can be helpful.
Yoga, tai chi, massage, meditation or other relaxation techniques can be helpful.
Preparing for your appointment
You may start by seeing your primary care doctor or a psychiatrist. You may want to take a family member or friend along to your appointment, if possible, for support and to help remember information.
What you can do
Before your appointment, make a list of:
- Any symptoms you've had, including any that may seem unrelated to the reason for the appointment
- Key personal information, including any major stresses or recent life changes
- All medications, vitamins, herbs or other supplements you're taking, and the dosages
- Questions to ask your doctor
Some questions to ask your doctor may include:
- Do I have bipolar disorder?
- Are there any other possible causes for my symptoms?
- What kinds of tests will I need?
- What treatments are available? Which do you recommend for me?
- What side effects are possible with that treatment?
- What are the alternatives to the primary approach that you're suggesting?
- I have these other health conditions.
 How can I best manage these conditions together?
How can I best manage these conditions together? - Should I see a psychiatrist or other mental health professional?
- Is there a generic alternative to the medicine you're prescribing?
- Are there any brochures or other printed material that I can have?
- What websites do you recommend?
Don't hesitate to ask other questions during your appointment.
What to expect from your doctor
Your doctor will likely ask you a number of questions. Be ready to answer them to reserve time to go over any points you want to focus on. Your doctor may ask:
- When did you or your loved ones first begin noticing your symptoms?
- How frequently do your moods change?
- Do you ever have suicidal thoughts when you're feeling down?
- Do your symptoms interfere with your daily life or relationships?
- Do you have any blood relatives with bipolar disorder or depression?
- What other mental or physical health conditions do you have?
- Do you drink alcohol, smoke cigarettes or use recreational drugs?
- How much do you sleep at night? Does it change over time?
- Do you go through periods when you take risks that you wouldn't normally take, such as unsafe sex or unwise, spontaneous financial decisions?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
Mood Stabilizers as a Treatment for Bipolar Mania
Written by WebMD Editorial Contributors
In this Article
- Which Bipolar Medicine Is Best?
- What Is Mood-Stabilizing Medication?
- Other Mood-Stabilizing Medicines
- Medicines for Bipolar Depression
- Will the Medicine Work for Me?
- Medication Tips
- Side Effects of Bipolar Drugs
- Stick to Your Treatment
If you have bipolar disorder, the right medications can be like a pair of eyeglasses. Bipolar disorder distorts your view of yourself and the world, but the medications can help you to see things clearly again.
Bipolar disorder distorts your view of yourself and the world, but the medications can help you to see things clearly again.
Medications are an essential part of a treatment plan. They won’t cure you, but they will help you keep your moods in balance so you can do the things you need and want to do.
Which Bipolar Medicine Is Best?
Doctors use many types of drugs to treat bipolar disorder. Some fight the extreme highs of mania and others treat the lows of depression. You might take one drug at a time or a few at the same time.
The best bipolar medicine is the one that works best for you. Work with your doctor to decide on the medication plan that helps you the most.
You may keep taking these medications for years or decades, even if it’s been a long time since your last manic or depressive episode. This is called maintenance therapy and helps prevent recurrence of symptoms.
What Is Mood-Stabilizing Medication?
Mood stabilizers are medicines that treat and prevent highs (mania) and lows (depression).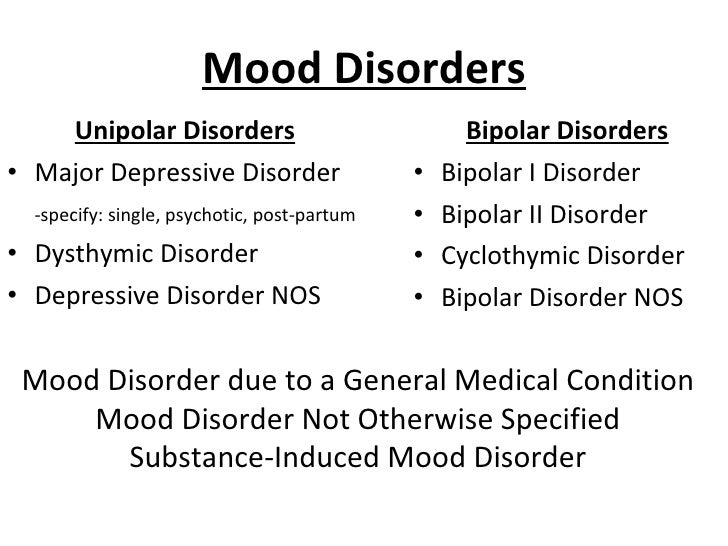 They also help to keep your moods from interfering with work, school, or your social life.
They also help to keep your moods from interfering with work, school, or your social life.
Examples include:
- Carbamazepine (Carbatrol, Epitol, Equetro, Tegretol)
- Divalproex sodium (Depakote)
- Lamotrigine (Lamictal)
- Lithium
- Valproic acid (Depakene)
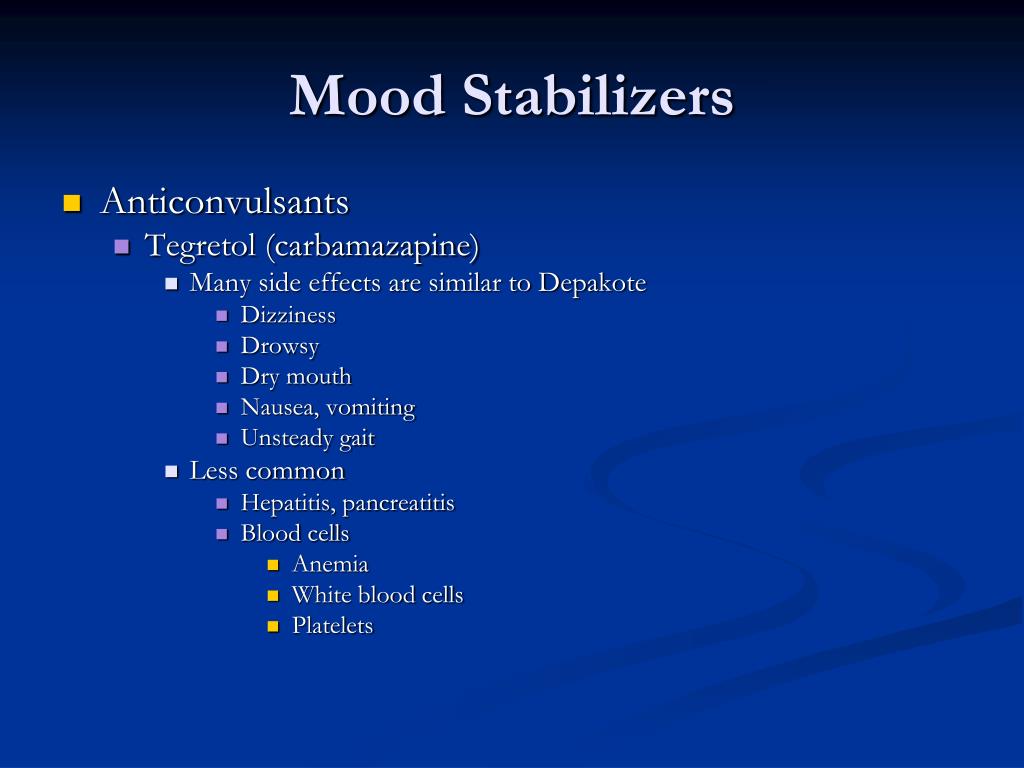
Some of these drugs are known as anticonvulsants, which are also used to treat seizure disorders, including carbamazepine, lamotrigine, and valproic acid.
Not all of these drugs have the same effects, though. Some (such as lithium) are better at treating mania. Others (such as lamotrigine) may be more useful for depression.
Keep in mind that the term "mood stabilizer" can be misleading. If you take one, your mood can still change during the day. These medicines treat full episodes of mania or depression that last for several days or weeks at a time.
Other Mood-Stabilizing Medicines
Drugs called antipsychotic medications are also common in bipolar treatment plans.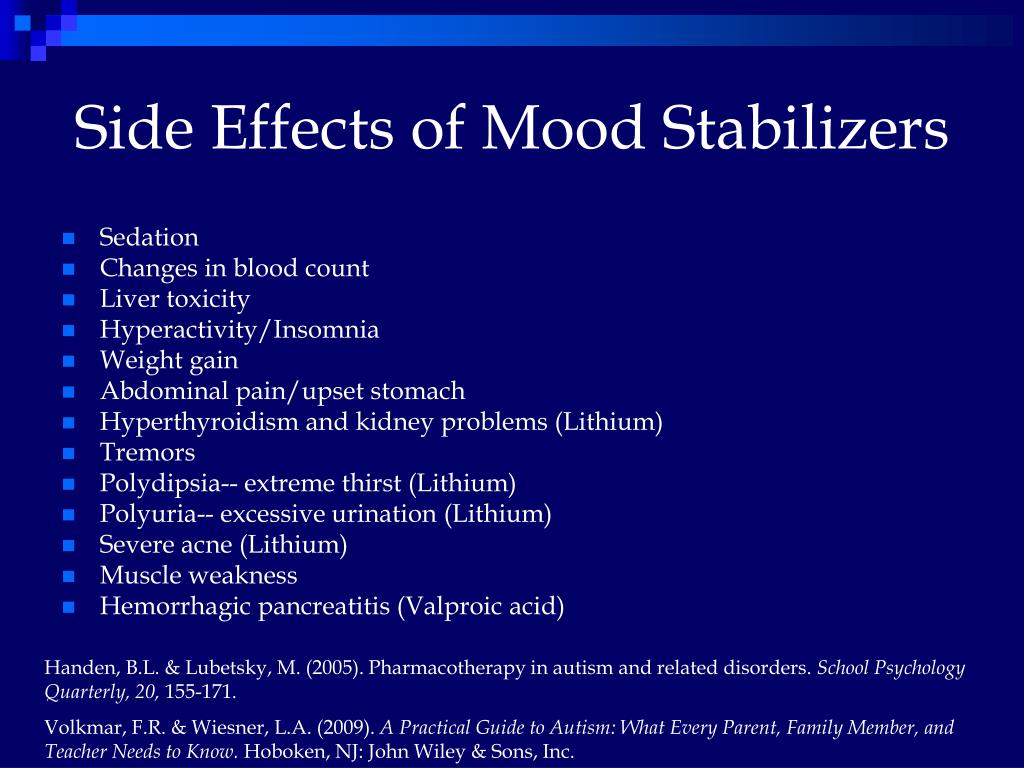 You can take them alone or with mood stabilizers to help with symptoms of mania. These drugs include:
You can take them alone or with mood stabilizers to help with symptoms of mania. These drugs include:
- Haloperidol (Haldol)
- Loxapine (Loxitane) or loxapine inhaled (Adasuve)
Today, doctors may prescribe newer antipsychotic drugs, including:
- Aripiprazole (Abilify)
- Asenapine (Saphris)
- Cariprazine (Vraylar)
- Lumateperone (Caplyta)
- Lurasidone (Latuda)
- Olanzapine (Zyprexa)
- Olanzapine/samidorphan (Lybalvi)
- Quetiapine fumarate (Seroquel)
- Risperidone (Risperdal)
- Ziprasidone (Geodon)
Medicines for Bipolar Depression
Most of the time, doctors will start bipolar disorder treatment by prescribing a mood-stabilizing drug like lithium. But the FDA has approved some medicines for bipolar depression, too:
- Fluoxetine combined with olanzapine (Symbyax)
- lumateperone (Caplyta)
- Lurasidone (Latuda). You might take it alone or with lithium or valproic acid.
- Quetiapine fumarate (Seroquel)
For some people, traditional antidepressants may trigger a manic episode. Because of this risk, your doctor should keep track of you closely if you take one.
Will the Medicine Work for Me?
Your doctor can’t predict how well a particular bipolar medication will work for you. You may need to try several different kinds and different doses to figure out the right approach. And that can take time.
It can be frustrating, but don't give up. Eventually, you and your doctor should be able to find a prescription that works for you.
Medication Tips
If you have bipolar disorder, taking your medication should be part of your routine. Take it at the same time every day. It's easier to remember if you do it along with another daily activity, like brushing your teeth, eating breakfast, or getting into bed. A weekly pillbox can help you see if you've missed a dose.
Be sure to talk to your pharmacist or doctor about the best time of day to take your bipolar medications. Some are best if you take them in the morning or at bedtime and others with meals or after meals.
Some are best if you take them in the morning or at bedtime and others with meals or after meals.
Make sure you know what to do if you accidentally miss a dose. Ask your doctor. Don't assume that doubling up is a good idea.
Side Effects of Bipolar Drugs
Like any drug, bipolar medicines can cause some side effects. They vary depending on which medications you use. These side effects can include:
- Nausea
- Tremors
- Hair loss
- Sexual problems
- Weight gain
- Liver damage
- Kidney damage
- Diarrhea
- Belly pain
- Skin reaction
Some medications can affect how well your liver works or the amount of white blood cells or platelets you have. You may need regular tests to make sure that you're staying healthy. The antipsychotic drug ziprasidone (Geodon) is linked to a rare but serious skin reaction called DRESS syndrome (drug reaction with eosinophilia and systemic symptoms).
Many side effects will go away after a few weeks of treatment. If you still feel bad after that, see your doctor. Don't assume you have to just live with the side effects. Your doctor may be able to change your dose, give you another medicine to control the side effects, or try a different medication altogether.
If you still feel bad after that, see your doctor. Don't assume you have to just live with the side effects. Your doctor may be able to change your dose, give you another medicine to control the side effects, or try a different medication altogether.
Stick to Your Treatment
Medications for bipolar disorder are powerful drugs, and you must take them exactly as your doctor recommends. Don't stop taking a medicine without your doctor's approval. It can be dangerous.
When you're feeling good, you might decide that you want to stop taking your medication. But that's a bad idea unless your doctor agrees. Treatment only during mood episodes may not be enough to prevent symptoms from coming back. In most people, maintenance treatment between mood episodes makes mania and depression happen less often and makes them less severe. If you're feeling good now, that's likely because your medication is working. So stick with it.
Bipolar Disorder Guide
- Overview
- Symptoms & Types
- Treatment & Prevention
- Living & Support
Valproate as a maintenance treatment for people with bipolar disorder after episodes of mood disorder
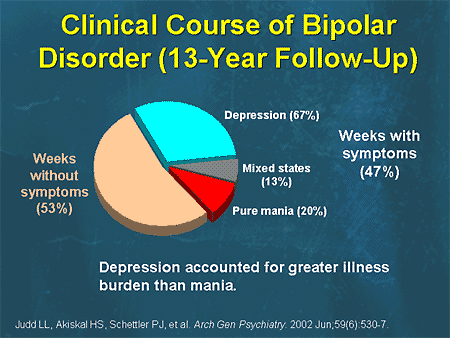
Bipolar disorder is a disorder that manifests itself in the form of manic and depressive states, and sometimes mixed.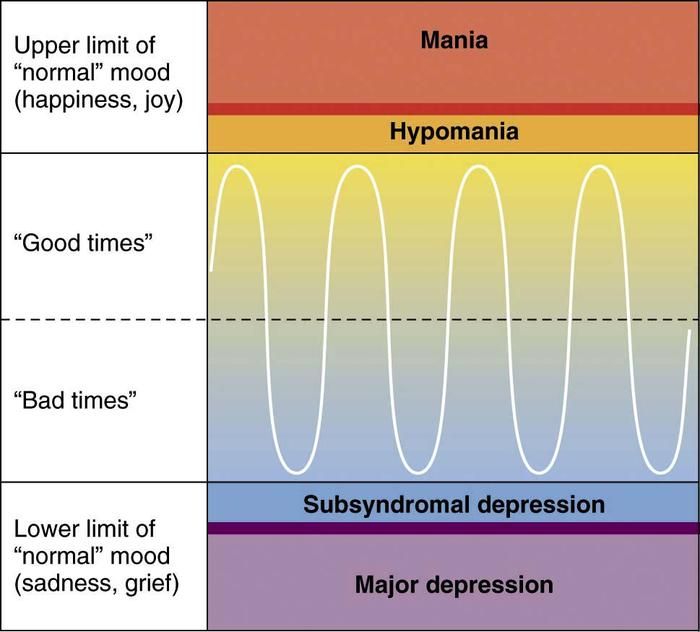 Depression is characterized by a decline in mood and energy, as well as an inability to experience joy, often in combination with other problems, such as sleep disturbance. Mania is the opposite - there is "too" a lot of energy, as well as problems with a good mood or irritability. In mixed states, the symptoms of depression and mania are combined. These episodes of mood disorder usually occur several times in a person's life, so long-term treatment (supportive care) can play a very important role in preventing relapses. Since valproate is a drug that may be useful in the treatment of the acute phase of bipolar disorder, in this review we wanted to answer the following question: is valproate useful as a maintenance agent in bipolar disorder? nine0003
Depression is characterized by a decline in mood and energy, as well as an inability to experience joy, often in combination with other problems, such as sleep disturbance. Mania is the opposite - there is "too" a lot of energy, as well as problems with a good mood or irritability. In mixed states, the symptoms of depression and mania are combined. These episodes of mood disorder usually occur several times in a person's life, so long-term treatment (supportive care) can play a very important role in preventing relapses. Since valproate is a drug that may be useful in the treatment of the acute phase of bipolar disorder, in this review we wanted to answer the following question: is valproate useful as a maintenance agent in bipolar disorder? nine0003
We searched for relevant studies (randomized controlled trials or RCTs) of long-term treatment of people with bipolar disorder with valproate or any other mood stabilizer, antipsychotic, or placebo. Three of us looked at RCTs to make sure the experiments were scientific. We extracted data from studies, put all the evidence together, and performed statistical analysis to find significant results. nine0003
We extracted data from studies, put all the evidence together, and performed statistical analysis to find significant results. nine0003
We searched up to 11 January 2013 and found six studies with 876 participants. The quality of the studies in terms of design was not very good, which means that the effects of some drugs may have been overestimated. The pooled studies suggest that valproate may help prevent the recurrence of bipolar disorder, especially depressive episodes. However, due to limited evidence, conclusions regarding valproate versus placebo and lithium (or other active agents) cannot be made with any reasonable degree of certainty. Lithium is an important drug to compare with valproate as it is known to be effective in preventing the recurrence of bipolar disorder. When we pooled the results of all studies that compared valproate with lithium, the evidence did not support superiority of valproate or lithium in terms of efficacy. People who took valproate for a long time were more likely to continue taking their prescribed medications than patients who were given lithium.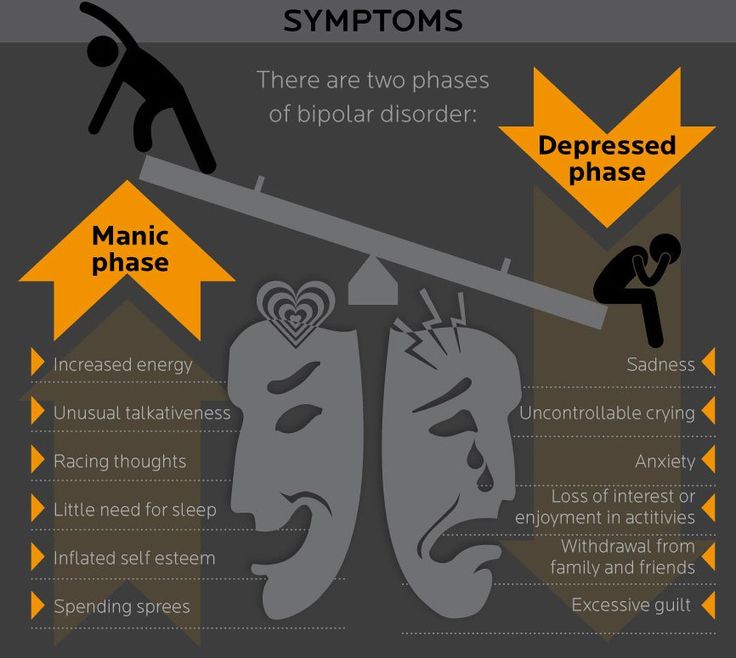 Clinicians and patients should be aware of the side effects of valproate, including alopecia, tremor, and weight gain. nine0003
Clinicians and patients should be aware of the side effects of valproate, including alopecia, tremor, and weight gain. nine0003
We also found a study comparing valproate monotherapy with combination therapy (taking two drugs at the same time). This study compared people who took only lithium or valproate with those who took valproate and lithium at the same time. There is no evidence that the use of valproate and lithium, compared with lithium alone, provided greater patient adherence to the prescribed treatment.
Translation notes:
Translation: Lilianna Lenarovna Mullina. Editing: Kukushkin Mikhail Evgenievich. Project coordination for translation into Russian: Cochrane Russia - Cochrane Russia (branch of the Northern Cochrane Center on the basis of Kazan Federal University). For questions related to this translation, please contact us at: [email protected]; [email protected] by: Ekaterina Yudina
symptoms of bipolar disorder, how it proceeds, how to find a psychiatrist, diagnosis and treatment
Victoria K.
lives with bipolar disorder
The first signs of the disease appeared in my teenage years, and the psychiatrist diagnosed bipolar disorder at the age of 26.
According to WHO, 45 million people worldwide suffer from bipolar disorder. This disease greatly reduces the quality of life: in some periods you are overly energetic and do things that you can regret, in other periods you are not able to get off the couch to do everyday things. nine0003
I will tell you how I have BAD and what I do to cope with the disorder and live like all ordinary people.
Go see a doctor
Our articles are written with love for evidence-based medicine. We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you. nine0003
What is Bipolar Affective Disorder?
Bipolar Affective Disorder, or BAD, is a mental disorder with alternating emotional ups and downs in mood.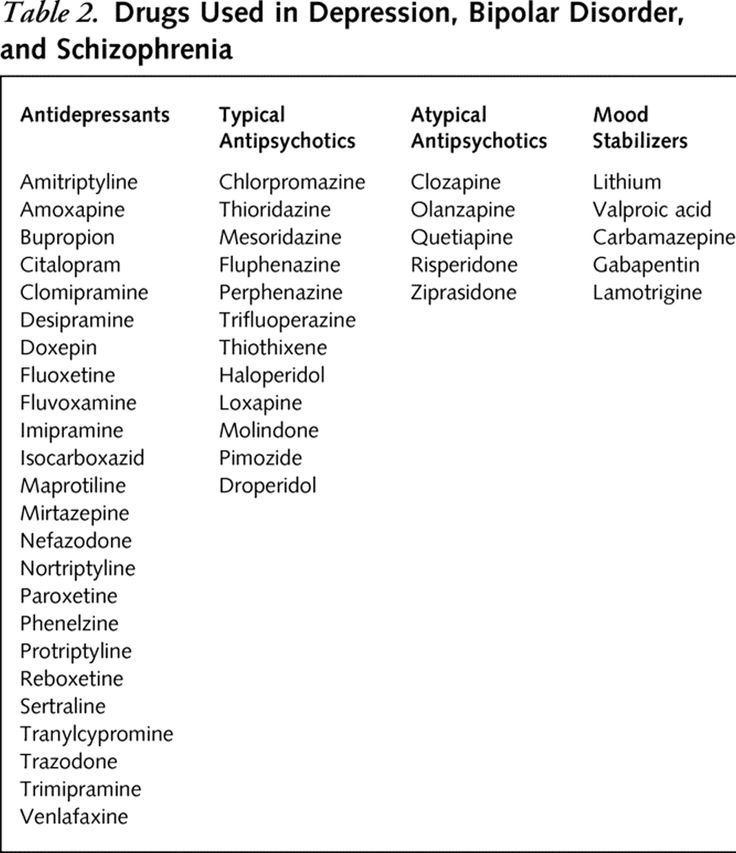 It is affective just because it is associated with violations of the emotional state, that is, mood - in psychiatry, the manifestation and experience of emotions is called affect. Previously, this disease was called manic-depressive psychosis.
It is affective just because it is associated with violations of the emotional state, that is, mood - in psychiatry, the manifestation and experience of emotions is called affect. Previously, this disease was called manic-depressive psychosis.
Bipolar Disorders - A Physician's Handbook MSD
Why BAD develops is not exactly known. Among the reasons are heredity, traumatic events, violations of the production of neurotransmitters - substances due to which signals are transmitted between brain neurons. The disease often manifests itself in adolescence or in the period between 20 and 30 years.
How Bipolar Disorder Manifests
BAD usually starts abruptly, followed by periods without symptoms and periods of exacerbations. The peculiarity of the disease is that during periods of exacerbations there are episodes, or phases, with different emotional states that can replace each other in an arbitrary order. nine0003
Bipolar Disorder - Mayo Clinic Blog Article
For example, when the illness escalates, the following conditions may occur.
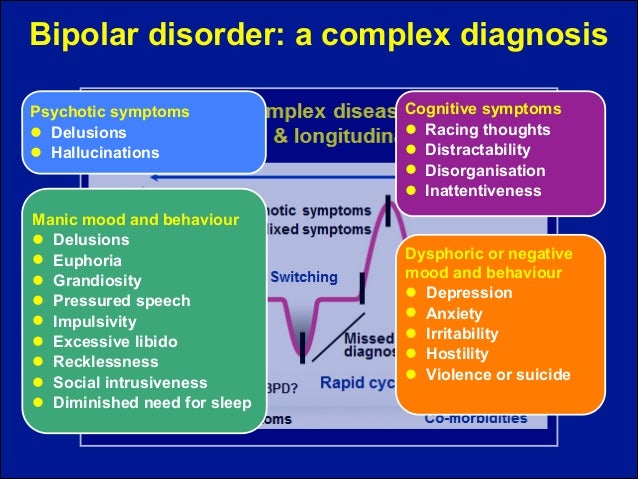
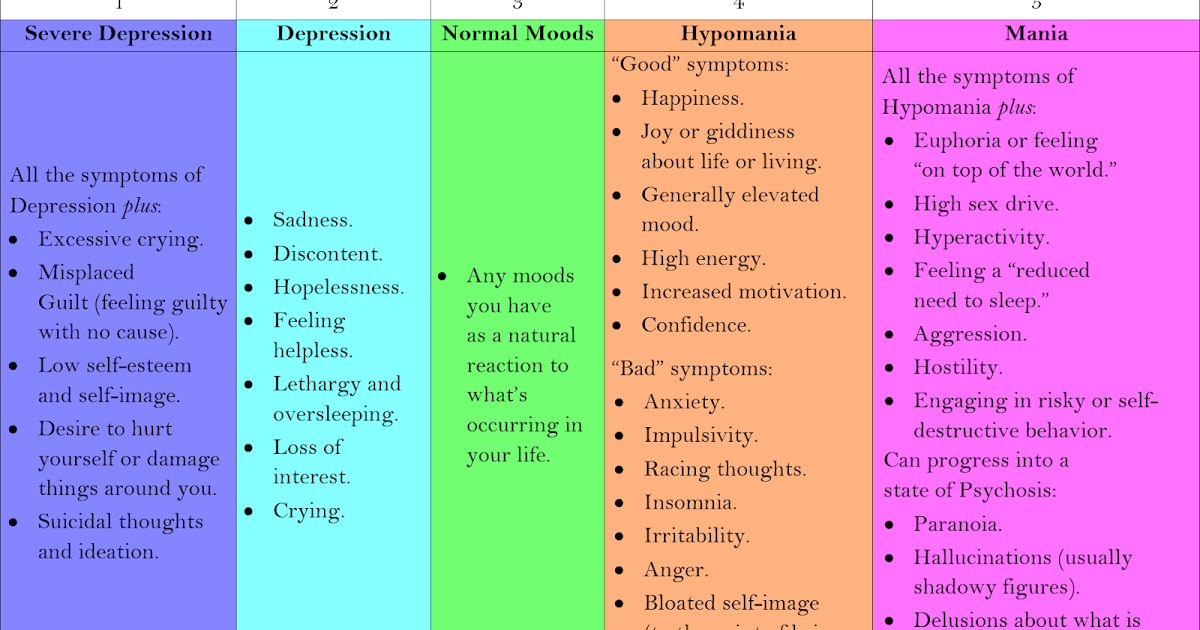
Mania - a state of elevated or irritable mood. The person feels energetic, actively engaged in something, such as finding a new hobby or even trying to open a business. As a rule, he sleeps little, is self-confident, talkative, he has a lot of ideas, often crazy. Risk sensitivity may decrease - for example, a person invests all the money in a hopeless business or gets into a loan. Hobbies for gambling, extreme sports are not uncommon. At the same time, a person feels great, but often cannot concentrate on one thing, work productively. nine0003
The extreme degree of mania is manic psychosis, when delusions of persecution, hallucinations, excessive activity develop, a person can become dangerous to himself or others.
Hypomania is a kind of mild mania. A person is in a state of emotional uplift, but this uplift is not so pronounced. However, the mood still improves, the need for sleep decreases, the person is creative, relaxed, feels euphoric, and his productivity increases.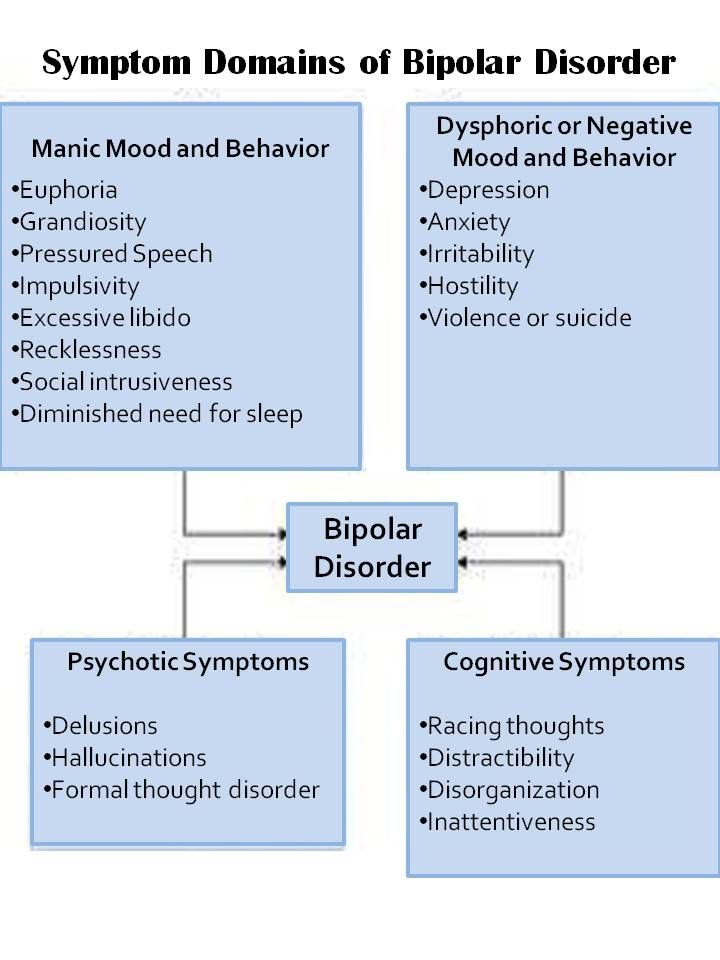 Although in some people such periods may be accompanied by irritability and a decrease in concentration. nine0003
Although in some people such periods may be accompanied by irritability and a decrease in concentration. nine0003
Depression - low mood, loss of interest in life, fatigue, guilt, indecision, decreased concentration. Sleep and appetite disturbances may occur. Sometimes there are thoughts of suicide, the futility of one's own life.
/bye-depression/
“It reminded me of a strict regime sanatorium”: how much I spent on treating depression
Between exacerbations, a person can return to normal, although it happens that his performance is still reduced. nine0003
Manifestations of the phases of bipolar disorder, according to the National Institute of Mental Health USA
| Parameter | Mania | Depression |
|---|---|---|
| Mood | Excitement, joy, irritability, resentment | Sadness, depression, emptiness, anxiety, hopelessness |
| Sleep | Reduced need for sleep | Trouble falling asleep, getting up early or sleeping too much |
| Appetite | Loss of appetite | Often increased appetite, weight gain |
| Communication | Talkativeness | Slow speech, forgetfulness |
| Concentration | Sensation of jumping thoughts, multitasking | Problems with attention and decision making, distraction |
| Behavior | Risk appetite, runaway spending, promiscuous sex | Lack of pleasure and interest in anything, decreased libido |
| Subjective feelings | Feeling of self-importance, talent and power | Feelings of worthlessness, suicidal thoughts, suicide attempts |
Mood
Excitement, joy, irritability, resentment
Sleep
Decreased need for sleep
Appetite
Loss of appetite
Communication
Talking
Concentration
The feeling of jumping of thoughts, multitasking
behavior
Risk, unbridled sex
Subjective sensations
Feeling and power
Depression 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 Mood
Sadness, depression, emptiness, anxiety, hopelessness
Sleep
Trouble falling asleep, getting up early or sleeping too much
Appetite
often increased appetite, weight gain
Communication
Slow speech, forgetfulness
Concentration
Problems with attention and making decisions, Dispersibility
behavior
Lack of pleasure and interest in something, decrease in libido
Subjective feelings
Feelings of worthlessness, suicidal thoughts, suicide attempts
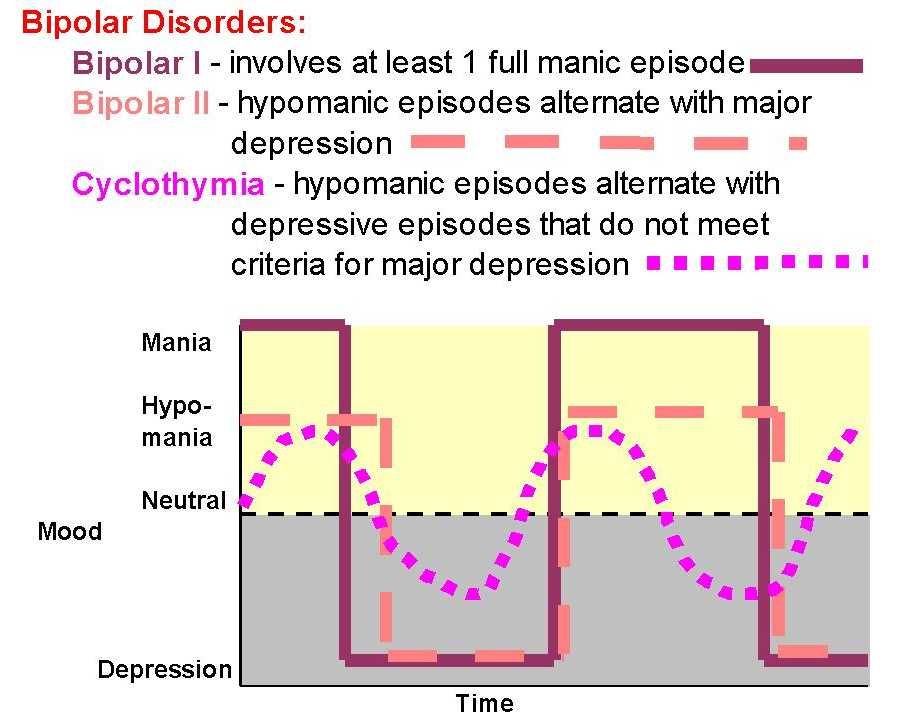
There are two main types of bipolar disorder according to how the disease manifests itself:
- When there was at least one manic episode and depressive episodes recur.

- When there are periods of depression and at least one episode of hypomania, but without full mania.
Bipolar Disorder - National Institute of Mental Health USA
I just have bipolar affective disorder type 2. This means that there are no full-fledged manias, but there are hypomanias and severe depressions.
Hypomania is a very cool time for me. You can do everything: get a second degree, run a marathon, learn English, go on an unplanned trip. And so for several months during which you do not sleep, do not eat, acquire new friends, start novels, end old relationships. You feel all sensations in the maximum range. During the day, it can throw several times from tears and the desire to die to incredible happiness. nine0003 This is what mania looks like in BAD. Source: Twitter
After hypomania comes depression. And immediately there is not enough strength not only for what was started during the previous phase, but also for ordinary things. The most understandable image of depression for me is “pressed down by a concrete slab.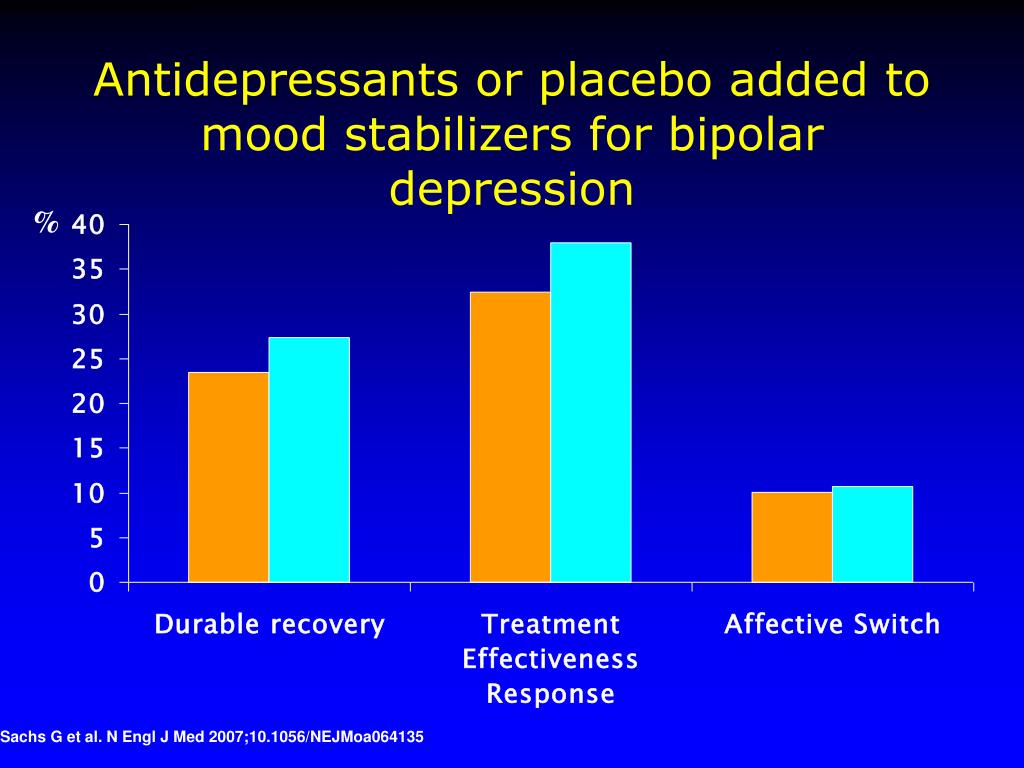 ” It becomes hard to do the simplest things: wash the dishes, change clothes, go to the store.
” It becomes hard to do the simplest things: wash the dishes, change clothes, go to the store.
Unfortunately, the brighter the hypomania goes, the worse the depression gets later — that's why, with experience, I stopped enjoying the active phase. nine0216 Now it's even more difficult for me: I understand what is happening with my brain, but I can't control it.
As I remember now, my first hypomania happened at the age of 12. Then there were periods of exacerbations clearly in a year and a half: hypomania lasts 2-3 months, usually May - July, depression - 5-6 months, usually in October - March, in between remission occurs when I feel normal. If I am in a long-term remission, then I hardly notice phase changes: mood swings are smoothed out with the help of medications or psychotherapy. nine0003
10 podcasts about health and medicine
The usual course of bipolar affective disorder
Viktor Lebedev
psychiatrist, science journalist
During an exacerbation of bipolar disorder, episodes of mania or hypomania and depression may alternate.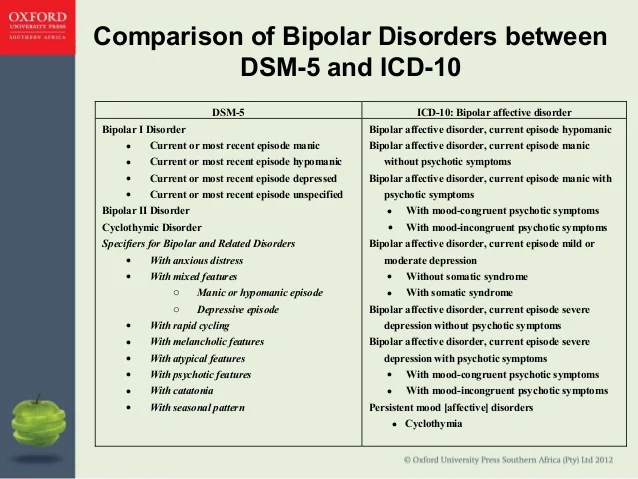 There is a clear separation of phases: first a hypomanic or manic episode, then a depressive episode, it happens that there are recurring episodes of depression, then hypomania. In the latter case, hypomanic phases are sometimes not noticed, a person may be diagnosed with recurrent, that is, recurring depression, and may be prescribed the wrong treatment. nine0003
There is a clear separation of phases: first a hypomanic or manic episode, then a depressive episode, it happens that there are recurring episodes of depression, then hypomania. In the latter case, hypomanic phases are sometimes not noticed, a person may be diagnosed with recurrent, that is, recurring depression, and may be prescribed the wrong treatment. nine0003
In fact, in BAD, the phases can alternate in any order, the diagnosis is made if there is any combination of manic and depressive episodes. The first time the disease usually begins with an episode of mania or hypomania, which develops into depression. Less commonly, it starts with depression, then mania or hypomania occurs. But in any case, there must be affective disturbances, that is, mood disturbances.
The exacerbation of the disease lasts from several weeks to several months. This also depends on whether the person is receiving medical treatment. If you respond quickly to an exacerbation, you can sometimes return to normal health in a week.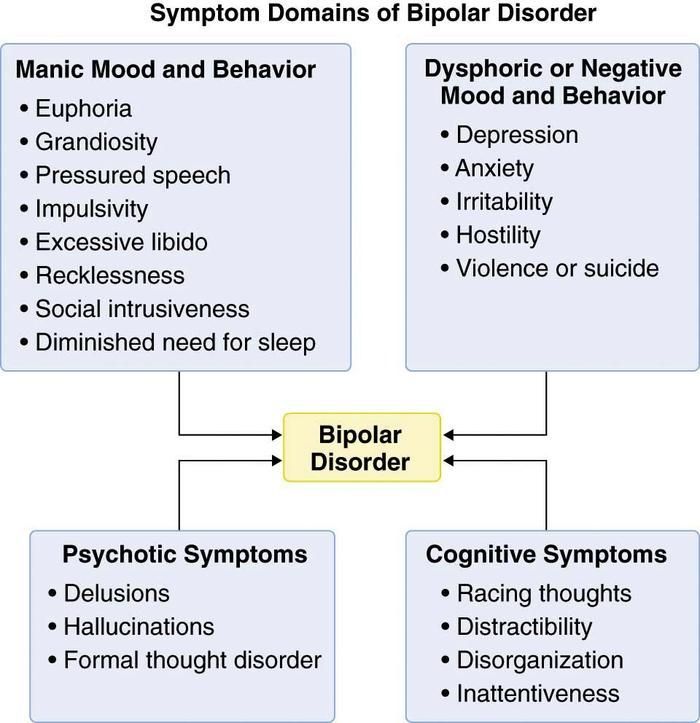 If not treated, the exacerbation can last for several months - especially the depressive phases, episodes of hypomania and mania usually pass faster. nine0003
If not treated, the exacerbation can last for several months - especially the depressive phases, episodes of hypomania and mania usually pass faster. nine0003
Seasonality of phases, when there is a connection between the manifestations of the disease and the change of seasons, occurs, but not all patients with bipolar disorder notice it.
How I suspected I had BAR
The first time I thought I was going crazy was when I was 18 years old. Painful relationships ended, obsessive thoughts and images swirled in my head, I listened to the same song in the player, walked for hours and could not stop. This went on for so long and was so unbearable that I almost decided to go to a psychiatrist. However, they didn’t talk about mental disorders then, so I didn’t even know where to turn. Then this state passed by itself. nine0003
I did not see a psychiatrist until seven years later, when I again had a similar severe condition: obsessive thoughts, inability to control emotions, self-harm, sleep and appetite disturbances. Before that, I had three episodes of hypomania every two years, but after them there was no severe depression, and therefore no reason to seek help.
Before that, I had three episodes of hypomania every two years, but after them there was no severe depression, and therefore no reason to seek help.
Then I just went to the district polyclinic - it turned out that a psychotherapist was there. She checked my symptoms on the Beck scale, diagnosed me with an anxiety-depressive disorder, and prescribed a common antidepressant that is often prescribed for depression. nine0003
Beck Depression Scale - online test
It seemed to me that antidepressants helped me immediately: my mood improved, I got energy, I talked a lot with friends, hung out, worked. Now I know this is a bad sign. Antidepressants usually take a long time to work: it takes about three weeks for the effect to appear, and I got better after a few days. In addition, in bipolar affective disorder, antidepressants can cause hypomania if not mitigated by other drugs. nine0003 This meme is well understood by those who were not immediately given the correct diagnosis. If you add Mentos to Coca-Cola, you get a foamy fountain that will splash out of the bottle. Antidepressants, in particular SSRIs - selective serotonin reuptake inhibitors - have the same effect on the mood of people with BAD
If you add Mentos to Coca-Cola, you get a foamy fountain that will splash out of the bottle. Antidepressants, in particular SSRIs - selective serotonin reuptake inhibitors - have the same effect on the mood of people with BAD
I went to this psychotherapist several more times, but she did not track my sharp mood swings, and I had one of the most severe hypomanias . I drank and smoked a lot, I had incredible emotional swings, I ruined my relationship with my best friend, I stopped eating and sleeping. nine0003
After a couple of months, my condition stabilized a little, but I continued to take antidepressants: I knew that they should not be stopped abruptly. Before canceling, I went for a consultation with another doctor, already at a paid clinic. She turned out to be a good specialist: she asked questions about mood swings, found out if I had previously had mood swings, ups and downs, depressions. Then everything was fine because of taking antidepressants, so I denied everything.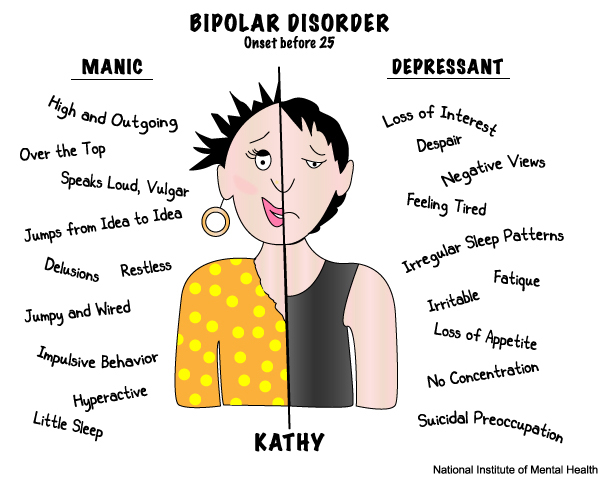
A year later, as the doctor ordered, I smoothly stopped taking antidepressants, and a few months later I was overcome by one of the most severe depressions. If last time I could attribute depression to circumstances - burnout, relationship difficulties, fatigue - now there was no reason for it. I had a job I loved, a great relationship with my husband, financial stability, a new city. And I wanted to die. nine0003
/psychotherapy-search/
How to choose a psychotherapist
This moment became a turning point in the diagnosis. I already knew that there is such a disease as bipolar affective disorder, what are its symptoms and features. Information about BAR appeared in the media field: I read articles and blog posts, watched videos on YouTube.
I was able to describe the last 10 years of my life in phases: there was a strong rise, followed by a decline. For example, in the hypomania of 2012, I worked two jobs, passed the state exams, wrote a diploma, hung out with friends until the middle of the night and completely took care of the life of the family. In hypomania in 2014, she entered the magistracy, graduated from a driving school, traveled, and also ran a marathon. nine0003
In hypomania in 2014, she entered the magistracy, graduated from a driving school, traveled, and also ran a marathon. nine0003
Every upswing was followed by a downturn: I stopped running, didn't pass the exam in the traffic police, and dropped out of the master's program. Each such exacerbation generally lasts a year and a half, and then repeats.
How I searched for a suitable psychiatrist
After collecting information about BAD, I decided to find a psychiatrist to confirm or deny my diagnosis. It didn't happen right away.
First I went to a psychiatrist on the advice of a friend, he helped her with depression. The doctor saw me in a paid clinic, the appointment cost about 3000 R. The consultation was unsuccessful: the doctor was clearly not interested in my condition, he indifferently asked questions about depression and prescribed antidepressants. And not the ones that were assigned to me last time, but others. I was too depressed to stand my ground, so I just started looking for another doctor.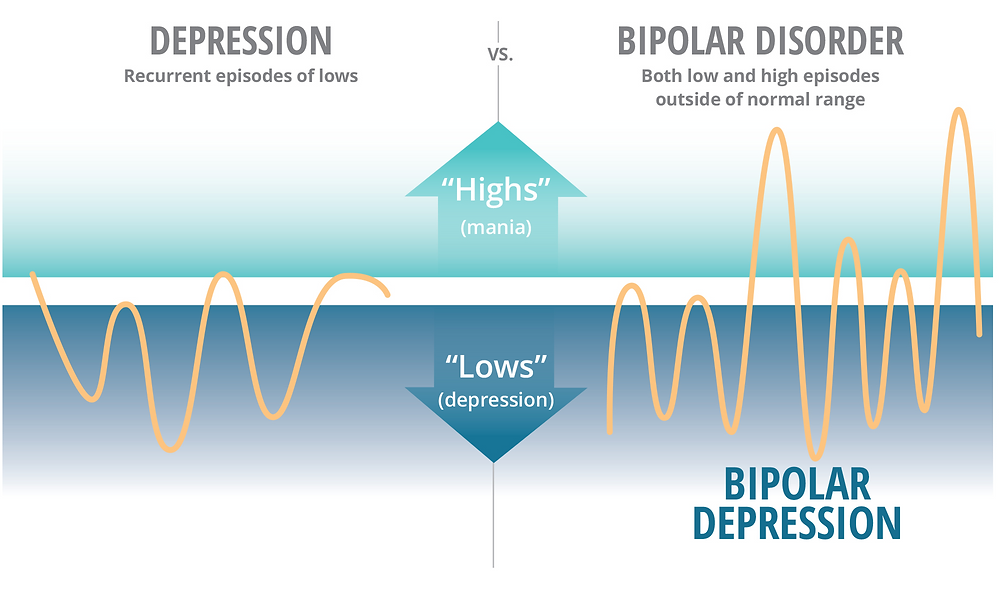 nine0003
nine0003
6 useful services for finding a psychotherapist
The second doctor was in a state clinic, she was recommended to me on Facebook. At first, I waited a long time for an appointment - the doctor was half an hour late, then I started asking about birth injuries and vascular dystonia. This consultation didn't work for me either. I paid 2,000 rubles for her.
The third appointment was successful: I found a psychiatrist, whom I still go to. She works at the State Institute of Psychiatry, but I see her for a fee. One consultation costs 2500 R.
2500 Р
I pay a psychiatrist for one appointment
The institute where the doctor sees, I was advised somewhere in the comments on the Internet. I called the reception and asked to sign me up for a doctor specializing in affective disorders as soon as possible.
The search for a suitable psychiatrist took about a month, so I went to see a doctor in a completely crushed state, in tears and hysteria.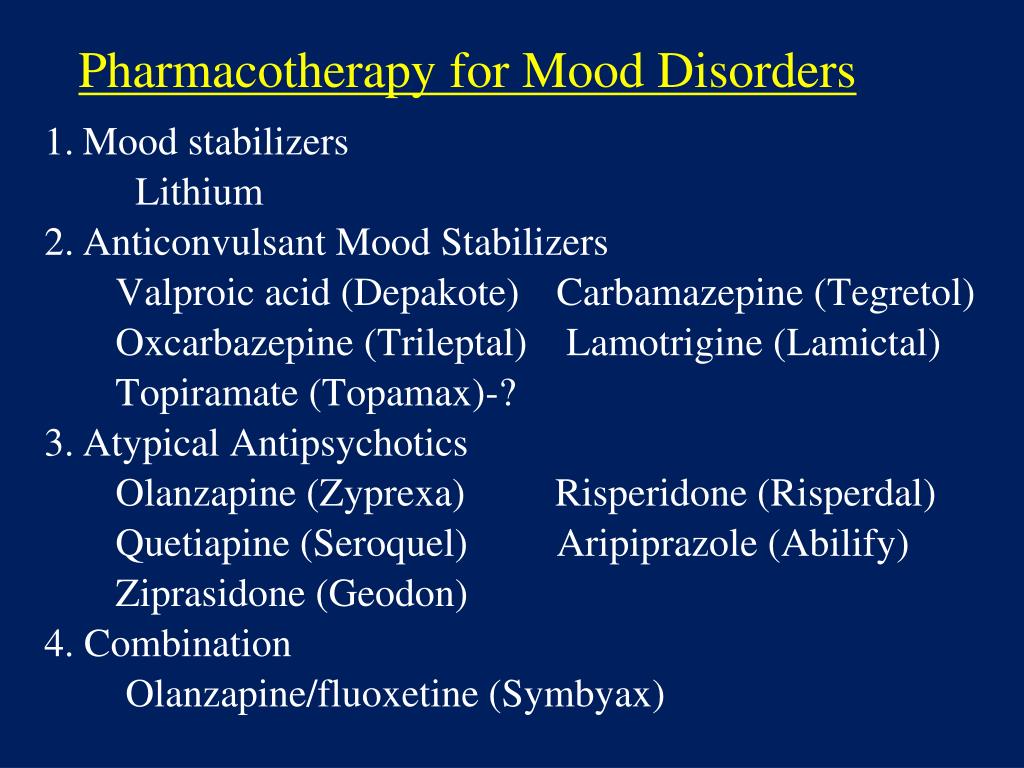 The psychiatrist asked me about the illness, listened to me and offered free hospitalization. However, I refused: I felt that I was controlling myself so as not to commit suicide, and my husband was also nearby, who understood the seriousness of the situation. As a result, I continued the treatment at home. nine0003
The psychiatrist asked me about the illness, listened to me and offered free hospitalization. However, I refused: I felt that I was controlling myself so as not to commit suicide, and my husband was also nearby, who understood the seriousness of the situation. As a result, I continued the treatment at home. nine0003
When hospitalization is needed for bipolar disorder
Viktor Lebedev
psychiatrist, science journalist
Hospitalization for bipolar affective disorder may be necessary if during a manic episode the patient develops strong arousal, he completely loses a critical attitude to his condition, and hallucinations appear rave. Such a condition can end badly for the patient himself or his relatives. In a depressive episode, indications for hospitalization will be suicidal thoughts or suicide attempts. nine0003
Inpatient treatment may also be needed in case of a severe decrease in working capacity.
If you suspect you have bipolar disorder, but are not in the acute phase of the disease, help is not urgent, it is better to spend time looking for a psychiatrist who specializes in bipolar disorder or affective disorders in general. Such a doctor is likely to quickly make the correct diagnosis and select the best treatment.
Such a doctor is likely to quickly make the correct diagnosis and select the best treatment.
Before taking, it is worth writing down all the symptoms that bother you, and also, if possible, make a retrospective graph of the expected phases - mania and depression, write down when they occurred and how long they lasted. This will help the doctor understand if this is BAD or something else. nine0003 This is how the BAR phase sequence looks like in my case
BAD treatment
Consultations with a psychiatrist and drug therapyThe psychiatrist first wrote me a prescription for several drugs: antidepressants and mood stabilizers. They are usually prescribed to people with affective disorders.
As explained to me, treatment is, among other things, checking for the correctness of the diagnosis, a way to distinguish depression from bipolar disorder. If the prescribed drugs help, the diagnosis is correct. nine0216 About two months later, my diagnosis was officially confirmed: bipolar affective disorder type 2.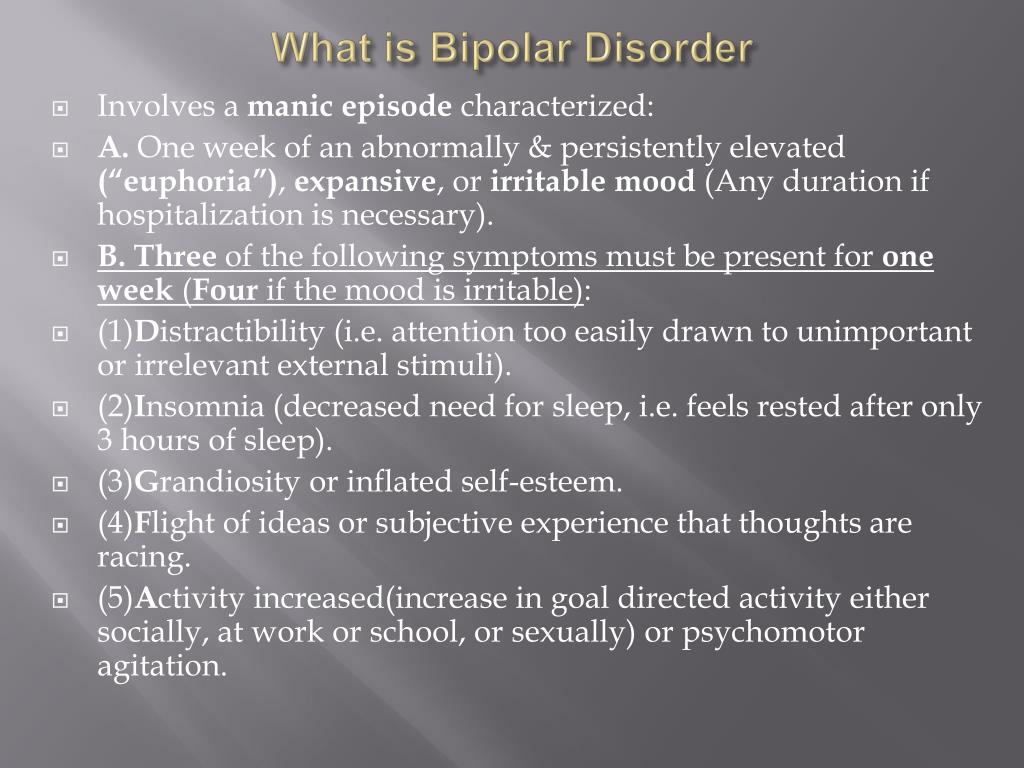
How bipolar disorder is diagnosed
Viktor Lebedev
psychiatrist, science journalist
Bipolar affective disorder is diagnosed by what problems a person is worried about. His story should contain a description of typical mood and behavioral disorders, usually there is an alternation of phases of the disease.
Complaints and a history of the disease are enough for diagnosis, sometimes the testimonies of relatives are also taken into account, which can tell about a person's behavior. It happens that a doctor can send you to a clinical psychologist for a psychological examination, but usually an ordinary psychodiagnostic conversation is enough. nine0003
You can suspect the disease on your own, although with hypomania or mania, criticality to one's condition often decreases, that is, a person does not understand that something is wrong with him. Sometimes relatives of the patient come for help, and not he himself. It is better to apply for a diagnosis to a specialist who has worked with BAD, knows what the manifestations of the disease look like.
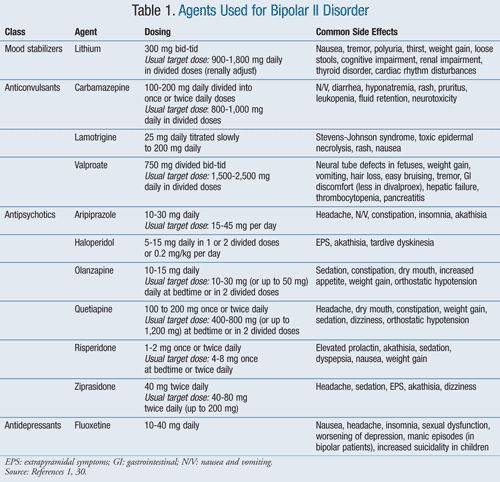
In general, drug therapy for bipolar disorder consists of several types of drugs that relieve different manifestations of the disease. These are normotimics that stabilize mood, antidepressants that help to cope with depression, antipsychotics that relieve excessive arousal. nine0003
Medication for Bipolar Disorders - MSD Handbook
Bipolar Disorder in Adults: Choice of Therapy - Article for Physicians Uptodate
The doctor selects the type of medication and dosage based on the phase the patient is in. Antidepressants are usually used in depressive phases and in combination with mood stabilizers. Antipsychotics - only in manic episodes and also together with normotimics.
In severe cases, a person with bipolar disorder may take up to six different drugs. But you need to strive to get by with one or two. nine0003
I started taking prescribed antidepressants and mood stabilizers immediately after seeing a psychiatrist. This time, the process of getting out of depression was long and smooth.
How therapy is selected for bipolar affective disorder
Viktor Lebedev
psychiatrist, scientific journalist
The psychiatrist selects treatment individually, taking into account the clinical picture: in the depressive phase - some drugs, in the hypomanic phase - others, in mania - still others.
It is important to combine drugs correctly. So, if a patient with bipolar disorder is prescribed only antidepressants, this can worsen the situation, even if he is depressed. Antidepressants can "disperse" his condition to hypomania or even mania. It is necessary to normalize a person’s well-being, and not throw him into a state with the opposite sign, so therapy includes normotimics. nine0003
The fact is that depression in BAD is not the same depression as usual, they are not always similar even in external manifestations, there are differences from a biological point of view, that is, in how processes in the brain change.
I visit my psychiatrist regularly: she adjusts the doses of drugs and monitors my condition. In the first year, I visited her six times - it cost me 15,000 R. Now I go to the doctor only during an exacerbation or a presumptive phase change - about four times a year, once every three to four months. It costs 10,000 R per year. In total, I have been seeing a doctor for three years now. nine0003
In the first year, I visited her six times - it cost me 15,000 R. Now I go to the doctor only during an exacerbation or a presumptive phase change - about four times a year, once every three to four months. It costs 10,000 R per year. In total, I have been seeing a doctor for three years now. nine0003
For two years, until recently, I took antidepressants and mood stabilizers in the minimum dosage. A pack of antidepressants for a month cost about 400 R, mood stabilizers - 600 R. That is, during the period of remission, the pills took 1000 R per month.
1000 R
I spend on pills a month in remission
My prescriptions for drugs However, a few months ago I had an exacerbation, I went into hypomania, so the regimen and dose of drugs had to be changed on the go. Within two weeks, my psychiatrist and I canceled antidepressants, significantly increased the dose of mood stabilizers - 2.5 times, and added antipsychotics. During the exacerbation, which lasted two months, 4000 R per month was spent on tablets. Now 2000 R will go away - the dose of mood stabilizers has been reduced by one and a half times and neuroleptics by half, antidepressants have been removed. nine0003
Now 2000 R will go away - the dose of mood stabilizers has been reduced by one and a half times and neuroleptics by half, antidepressants have been removed. nine0003
It is interesting to observe how quickly drug therapy changes the state of the body and how it then returns to normal. Often, drugs do not fit the first time, so you need to regularly visit a psychiatrist and monitor your well-being. But after choosing the right therapy, you can live almost as before, except that you need to be more attentive to yourself.
/obsessive-compulsive-disorder/
How I live with obsessive-compulsive disorder
BAD treatment cannot be found once and for all
Each patient who is responsible for the treatment of bipolar disorder and is in contact with the doctor has his own scheme for changing the dosage or types of medications, taking into account well-being. For example, if you cannot sleep for more than a few days and stop eating, you add an antipsychotic. If you fall into an abyss of self-hatred and don’t swim for more than a week, an antidepressant will help.
If you fall into an abyss of self-hatred and don’t swim for more than a week, an antidepressant will help.
Of course, this does not cancel regular meetings with a psychiatrist, because the process of choosing drugs and dosages is very complicated. Now I can regulate a lot myself, depending on how I feel, but I still see a specialist. nine0003
At the same time, bipolar affective disorder cannot be cured once and for all - you can only go into a long remission. As my doctor told me, this is five years without pronounced phases. In my case, I lasted two years without episodes, and now I need to start the countdown again.
Also, as far as I know from my experience and the experience of people with the same diagnosis, at some point there is an illusion that everything is cool, there is no illness, it seemed to you that you are doing great. At this point, people stop taking pills - this is a bad decision, never do this. If you feel good, first of all, you should check if this is the beginning of hypomania. And secondly, be glad that you have entered remission. nine0003
And secondly, be glad that you have entered remission. nine0003
During these three years, I once stopped drinking pills - I got depressed, once I did not pay attention to the symptoms - I got severe hypomania, now I'm trying to go into remission again.
BAD treatment
PsychotherapyThe effectiveness of treatment of bipolar affective disorder can be increased by combining drug therapy with psychotherapy. Cognitive behavioral therapy is often used for bipolar disorder. It teaches you how to cope with stress factors, monitor your condition, manage the symptoms of the disease. Even during the sessions, together with the doctor, they work out trigger situations, that is, what can provoke an exacerbation of the disease. nine0003
Bipolar affective disorder and supportive psychotherapy - article on the Uptodate physician website
For example, I have trouble admitting my own mistakes. Every mistake for me is a tragedy, and it seems to me that those around her will never forget. It is difficult for me to admit my own mistakes, oversights cause great anxiety. I also have an ideal image of what I should be: read a lot, earn money, keep my house perfectly clean, have six-packs, study, know two foreign languages, go to exhibitions. Obviously, this is impossible, but a persistent desire to reach an unattainable height is also stressful. I work through all this with a psychotherapist. nine0003
It is difficult for me to admit my own mistakes, oversights cause great anxiety. I also have an ideal image of what I should be: read a lot, earn money, keep my house perfectly clean, have six-packs, study, know two foreign languages, go to exhibitions. Obviously, this is impossible, but a persistent desire to reach an unattainable height is also stressful. I work through all this with a psychotherapist. nine0003
I started therapy only six months ago, on the advice of a doctor, before that I thought that I could cope on my own. At first she was in therapy with a psychotherapist, whom she found through the Inhale project, which helps burnt out employees from the charitable field. I worked with her on this project, then continued after completion.
We looked at situations that increase my anxiety, including fear of making mistakes and being judged, as well as difficulties in life in general. The cost within the project was 400 R per meeting, there were about ten of them in total, then, already outside the project, the price increased to 2400 R.
/prl/
How much does it cost to treat borderline personality disorder
Now I went to another psychotherapist - she has a more applied approach, we look for my cognitive distortions and try to remove them. For example, we work with my excessive anxiety about the impression I make on other people, and the fear that I cannot control it.
The cost of sessions with this specialist is 2500 R per visit. Now I go to her every 10-14 days, that is, 2-3 times a month. In general, I have been working with my condition on my own for quite a long time, so the therapist only directs me in the right direction. nine0003
Is psychotherapy mandatory for bipolar disorder
Viktor Lebedev
psychiatrist, science journalist
Cognitive behavioral therapy is most commonly prescribed for bipolar disorder. This is an optional therapy, that is, an auxiliary method of treatment, you only need to take medication. However, psychotherapy can greatly improve the quality of life: it complements the action of drugs well, helps to control and change those things that pills do not work on. First of all, cognitive-behavioral therapy helps to control emotions, better cope with your illness. nine0003
First of all, cognitive-behavioral therapy helps to control emotions, better cope with your illness. nine0003
Many also benefit from support groups for people with bipolar disorder. I tried to go to such a meeting, but it didn’t work for me: I don’t want to define myself through illness, this is part of my life - but not me.
The largest project holding such meetings is Sunday BAR. They support not only people with bipolar disorder, but also their loved ones. Meetings are held online and offline.
List of support groups in different cities for people with BAD and other disordersPDF, 275 KB
BAD treatment
LifestyleUniversal advice given for bipolar disorder and more includes: sleep and work-life balance, eat right, avoid alcohol, exercise.
All this really helps, but in fact, organizing your life is difficult: meetings with friends, vacations, unexpected work do not fit into the routine, you want to work more, and alcohol looks like a great way to cope with anxiety, although in fact it can lead to depression. nine0003
nine0003
I try to keep the correct regimen to the best of my ability. True, according to my feelings, depression comes by itself, without any triggers from the outside, and I cannot influence it. But hypomania is fueled by new projects, loves, and other emotions. For example, even a small amount of falling in love causes hypomania, which, in turn, increases falling in love. It doesn't end well.
/shizofreniya/
How much does it cost to support a relative with a mental disorder
I lived in St. Petersburg for quite a long time, there during the white nights you don’t feel like sleeping at all - and this provokes hypomania. One of the psychiatrists even forbade me to go to St. Petersburg for some time.
Now I have an established sleep and eating regime, I quickly notice its violation - this is a signal that an exacerbation has begun. Unfortunately, sometimes the regime is knocked down by external circumstances, then it is more difficult to notice the exacerbation of BAD.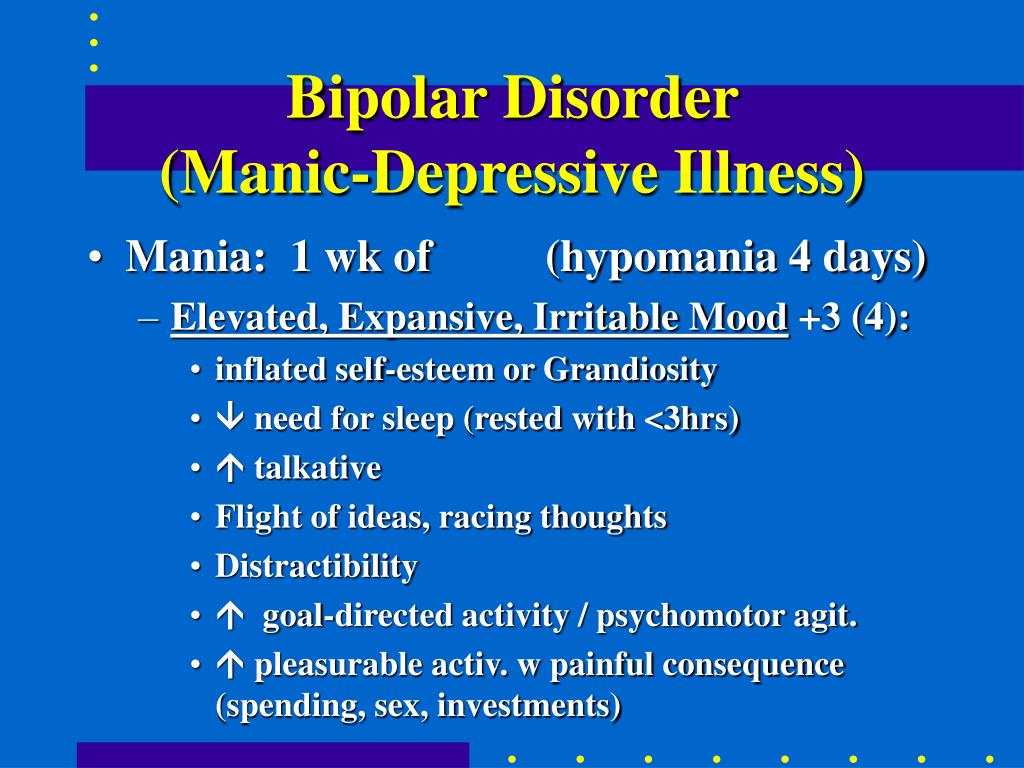
Sleep is very important to me, it is my priority. I try not to hang out until the middle of the night, and if I didn’t manage to get enough sleep, then I try to sleep in the afternoon. I usually go to bed around midnight, get up at 8-9hours of the morning is a comfortable mode for me and my work. I very rarely stay awake at night or wake up later than 10 am.
I have a fitness bracelet that tracks the phases and amount of sleep - it helps to see the dynamics and notice deviations. When I see a sleep disorder, I start drinking light tranquilizers and antipsychotics to return to a comfortable mode.
| Sleeping less than seven hours on pills indicates an episode of hypomania, without drugs in this phase I would sleep less than four hours | And sleep for more than seven hours is already the normalization of the state after the addition of other tablets |
Everything is more difficult with food: I have a difficult relationship with my own body, so I perceive a decrease in appetite with enthusiasm.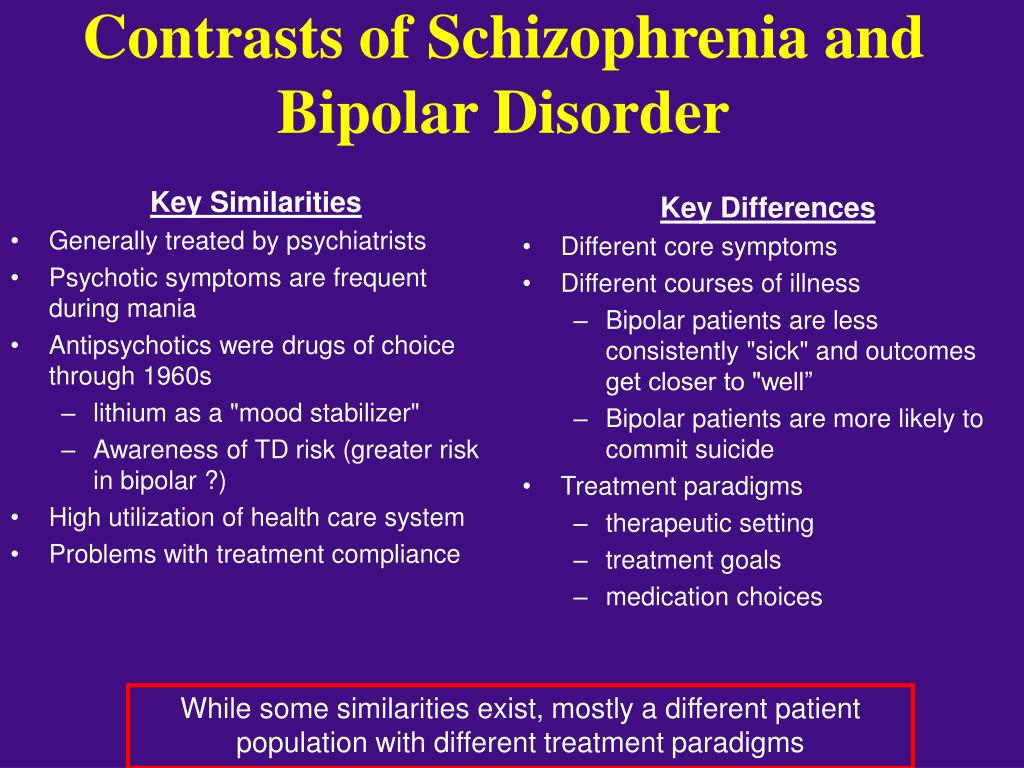 I am working on the problem with a psychotherapist, how to solve it, until I figured it out. My psychiatrist believes that first sleep, and then everything else, and my experience confirms this: sleep disturbances have a stronger effect on well-being. I also keep a record of alcohol consumption in the Alcogram application - abuse negatively affects my condition. When I see how many sober days there were, it motivates me to control myself. nine0003
I am working on the problem with a psychotherapist, how to solve it, until I figured it out. My psychiatrist believes that first sleep, and then everything else, and my experience confirms this: sleep disturbances have a stronger effect on well-being. I also keep a record of alcohol consumption in the Alcogram application - abuse negatively affects my condition. When I see how many sober days there were, it motivates me to control myself. nine0003
I am lucky that I take my job seriously: it is responsible and resource-intensive, it is important for me to be productive, it disciplines and helps me to keep the regime.
What to do to reduce the frequency of exacerbations
Viktor Lebedev
psychiatrist, science journalist
In BAD, it is important to have a daily routine that allows you to maintain normal behavior. This reduces the frequency of exacerbations, sometimes helps to completely avoid the recurrence of episodes of the disease. In addition to quality sleep and proper nutrition, you need to avoid overwork, work in an exhausted state, give yourself a rest. Doctors usually insist on the exclusion of alcohol, drugs are also dangerous, especially stimulants, which can cause psychosis in a healthy person. nine0003
Doctors usually insist on the exclusion of alcohol, drugs are also dangerous, especially stimulants, which can cause psychosis in a healthy person. nine0003
Exacerbations of the disease can occur on their own, without the influence of external factors, or they can be caused by external events, both tragic, such as the death of a loved one or a break in relationships, and joyful. Therefore, it is important to learn to recognize your emotions, to identify in time what provokes a new episode, both independently and with the help of psychotherapy.
How I live with BAD now
Accepting the diagnosis was not easy: on the one hand, it finally became clear what was happening to me and that it could be regulated. On the other hand, this is a diagnosis for life. You need to constantly monitor your condition, take pills, consult with doctors. nine0003
The most difficult thing for me was the inability to separate myself as a person from the disease. What of what I did in life was the result of my choice, and what was a symptom of the disease? Moving from city to city, changing jobs, partners, hobbies - what if all this is just a disease, and I'm not behind it? Three years have passed - and I still cannot separate myself from BAD, it seems impossible.
Now life has become easier: now I know what to expect in the near future, because the phase schedule is still respected. It is clear when to slow down with the pace of life, and when to add antidepressants. nine0003
My work is related to people. Of course, the disease affects my mood and state: in depression I have less strength and the ability to give out emotions, in hypomania, on the contrary, there are a lot of emotions, but there is not enough concentration. It's good that work allows you to vary the load depending on the phase: in depression I can work a little less, and in hypomania - a little more.
At the time of my first diagnosed depression, I had an unloved job, it took the entire resource. I cried in the mornings, afternoons and evenings because it was difficult for me to keep working. Now I really love my job, it gives me more resources than it takes. nine0003
I continue to take medication, see a psychiatrist several times a year and a psychotherapist several times a month.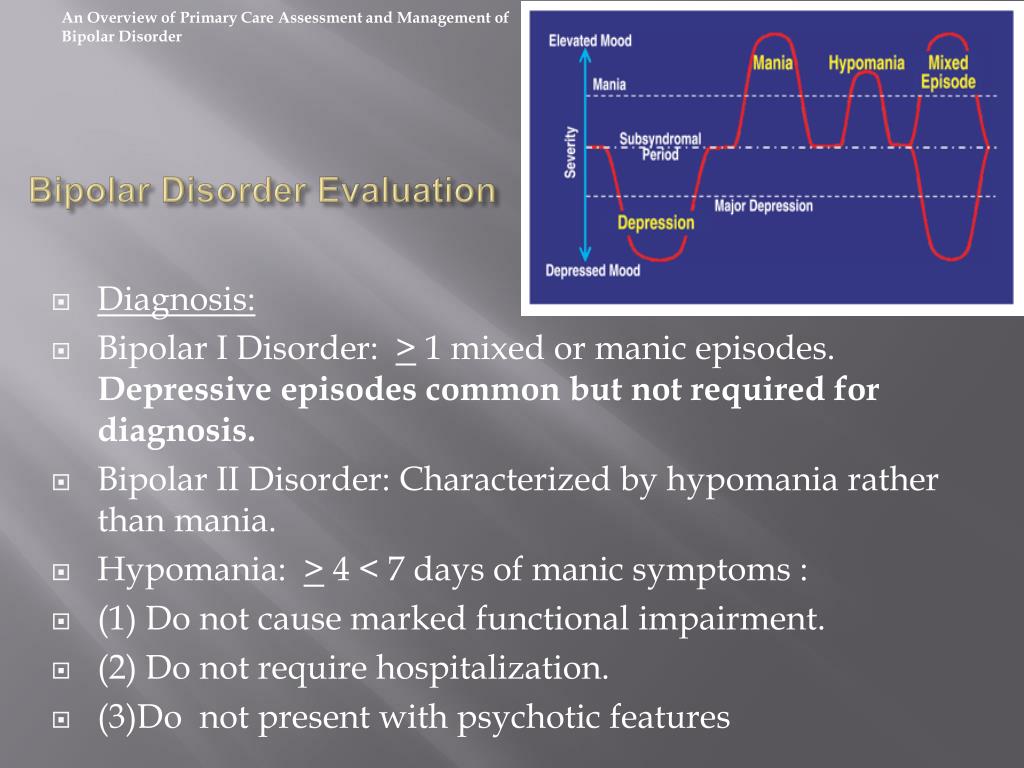 In March, at the most difficult moment of the exacerbation, I spent on medicines, an appointment with a psychiatrist and three meetings with a psychologist 13,000 R.
In March, at the most difficult moment of the exacerbation, I spent on medicines, an appointment with a psychiatrist and three meetings with a psychologist 13,000 R.
13,000 R
I go into remission and spend about 8,000-10,000 R per month on medications, a psychologist, and periodic appointments with a psychiatrist. A significant amount, but it allows me to remain in a resourceful and efficient state. nine0003
The unobvious difficulty of living with bipolar disorder is the need to strictly control one's financial situation. In hypomania, money flies away easily, you make decisions instantly - for example, you can decide in a minute to fly to Spain and buy tickets. When you are depressed, you spend less, but it is also difficult to earn money. I try to keep a financial cushion in case of an aggravation, and also take into account all expenses in the application so as not to get into debt. Fortunately, so far my financial anxiety is stronger than bipolar, so there has never been a credit card debt. nine0003
nine0003
I spent 58,800 rubles on BAD treatment in a year
| Treatment | Price |
|---|---|
| Psychiatric appointment | 10 000 R, total 4 receptions of 2500 R |
| Psychotherapist appointment | 25 000 R, total 10 receptions of 2500 R |
| Antidepressants | 4800 R, 12 packs of 400 R |
| Antipsychotics | 7000 R, 7 packs of 1000 R |
| Normotimics | 12000 R, 15 packs of 800 R |
Reception of a psychiatrist
10 000 R, total 4 receptions of 2500 r
Reception of a psychotherapist
25 000 r, total 10 doses of 2500 r
antidepressants
4800 r, 12 packages of 400 p
neuroleptic neuroleptic
7000 R, 7 packs of 1000 R
Normotimics
12000 R, 15 packs of 800 R
Books I recommend reading about bipolar affective disorder
The most famous book about living with bipolar disorder is The Restless Mind.