Beta blockers depression
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.
-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly. Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
beta-blockers do not cause depression but may cause sleep disturbances uMEDp
The American Heart Association (AHA) has assessed the psychological side effects of taking beta-blockers. It turned out that taking this group of drugs does not lead to depressive disorders, increased anxiety or hallucinations. Depression appeared in patients taking beta-blockers no more often than in other people.
The study was conducted by scientists from the Berlin Institute for Health Research. They conducted a meta-analysis of 258 studies with over 50,000 participants.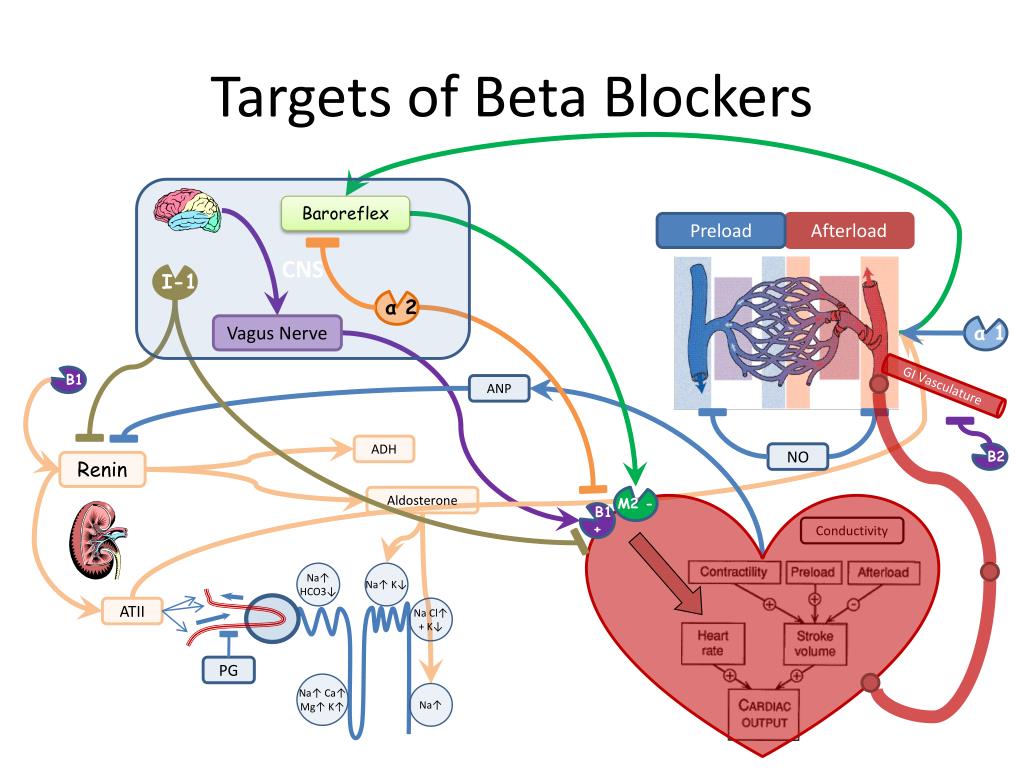 They published the results of their work in the journal Hypertension.
They published the results of their work in the journal Hypertension.
Most often, when taking beta-blockers, patients reported the development of depression in them. However, depression was diagnosed both among patients taking this group of drugs and among participants in the placebo group.
The experts also found that depression caused patients to stop treatment with both beta-blockers and other drugs. The most common mental health reason for not taking beta-blockers was feeling tired.
Also, German scientists noted that the appearance of nightmares and insomnia may be associated with the intake of beta-blockers. However, they were unable to track how long patients experienced these side effects.
In addition, experts emphasize that patients after a heart attack or stroke may be more likely to experience side effects from taking beta-blockers. Scientists have not found a causal relationship between taking drugs and the development of mental complications in this group of patients, but they believe that such patients should be under special supervision.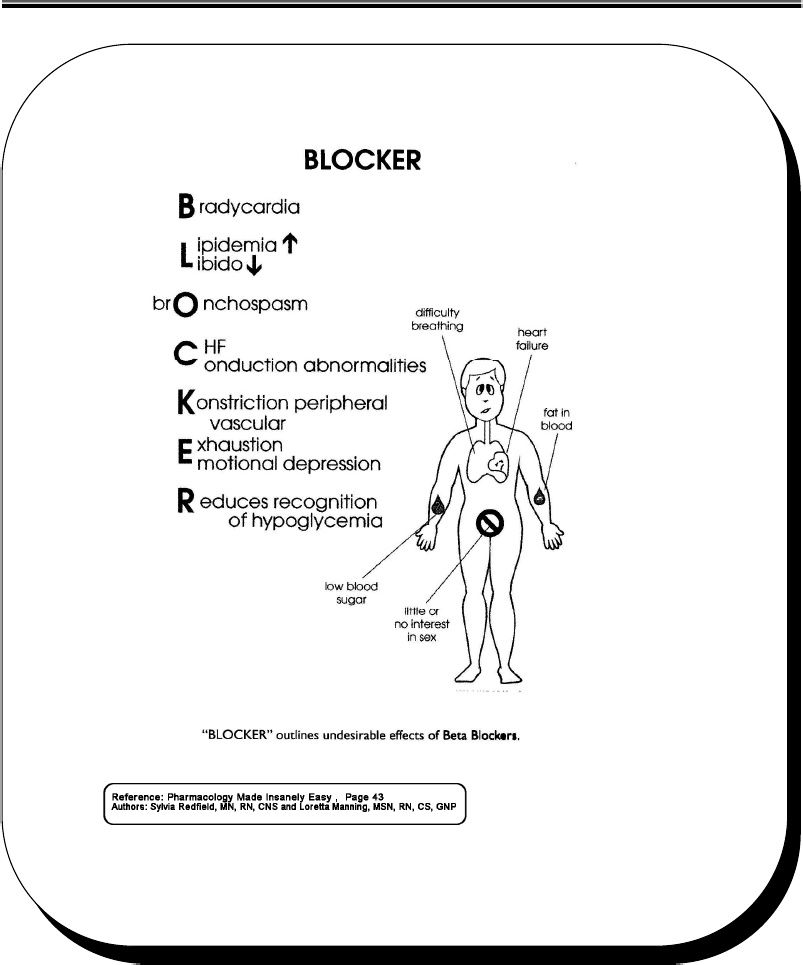
Beta-blockers are used to treat cardiovascular conditions, including heart failure, arrhythmias, angina, and hypertension. Previously, scientists suspected that beta-blockers could cause side effects such as depression, anxiety, drowsiness, insomnia, hallucinations and nightmares.
“The possible mental health side effects of beta-blockers have been discussed in the scientific community for decades. The results of our study showed that beta-blockers are not responsible for many of these negative side effects,” said Reinhold Kreutz, head of the study, professor at the Berlin Institute of Health and the Institute of Clinical Pharmacology and Toxicology.
It is worth noting that the scientists stated a significant limitation during the meta-analysis of the data. The main drawback of their study is that they analyzed data from 20 years ago, when the description of side effects was not universal. In addition, the authors stated that they only considered randomized, double-blind clinical trials. It turns out that they did not look at other studies that could provide more information about long-term treatment with beta-blockers.
It turns out that they did not look at other studies that could provide more information about long-term treatment with beta-blockers.
photo: freepik.com
The results of the detection of depression in patients with glaucoma when using beta-blockers or travatan | Lysenko O.I., Malyshev A.V.
Summary Objective: to establish the presence and characteristics of depressive disorders in two groups of patients with glaucoma: those who use BAB to reduce IOP and those who use Travatan 0.004%.
Objective: to establish the presence and characteristics of depressive disorders in two groups of patients with glaucoma: those who use BAB to reduce IOP and those who use Travatan 0.004%.
Methods: patients were divided into two groups of equal size. 1st group to reduce IOP used BAB, 2nd - travatan 0.004%. The severity of depressive symptoms was assessed using the A.T. Beck (1961). A score of 0 to 9 was defined as no depression, 10–15 as mild depression, 16–19 as moderate depression, and 20 or more as severe depression.
Results: 98 people aged 56 to 75 years old (mean age 64±4.56 years) were examined. In the 1st group, depression was detected in 15 (30.6%) patients, in the group that used travatan 0.004% - only 5 (10.2%). The average score of depression on the Beck scale was 16.4±0.05 in the 1st group, 8.4±0.02 in the 2nd group.
Conclusion: such patients try to disguise the change in the psycho-emotional state with the help of somatic complaints. Therefore, special attention should be paid to patients taking BAB in all dosage forms, regardless of the duration of their use.
Key words: beta-blockers, depression, travoprost.
Abstract
Results of a definition of depressive status in patients with glaucoma treated with beta-blockers or travoprost
O.I. Lysenko, A.V. Malyshev
Kuban State Medical University, Krasnodar
Purpose: to define the presence and peculiarities of depressive disorders in patients with glaucoma treated with beta-blockers or travoprost 0. 004%.
004%.
Methods: 2 groups of patients were formed. First - with beta-blockers treatment, second one - with travoprost 0.004%. The rate of intensity of the depression symptoms was evaluated with the help of Bek's scale (1961). Rate from 0 to 9 scores was considered as “absence of the depression”, 10–15 – “light depression”, 16–19- "moderate depression", 20 and more - "severe depression".
Results: 98 patients (age 56–75 years old) were examined. In the first group (beta-blockers) depression was in 15 (30.6%) patients, in the second one (travoprost) - in 5 patients (10.2%). Average score was 16.4±0.05 and 8.4±0.02 accordingly.
Conclusion: Depression could be masked with other somatic complaints. This should be taken into consideration regarding all patients treated with beta-blockers, irrespective of the route of administration.
Key words: beta-blockers, depression, travoprost.
Relevance. According to WHO, depression is one of the most common diseases with a steady upward trend. Depression is a side effect of many drugs, so there is always a concern that the use of beta-blockers (BAB) can affect the psyche of patients. This issue is controversial today, especially when it comes to the use of BAB in the form of eye drops. Obviously, changes in the mental state can adversely affect the quality of life of patients with glaucoma, cause great damage to their families and society [1,2,7–9].
Depression is a side effect of many drugs, so there is always a concern that the use of beta-blockers (BAB) can affect the psyche of patients. This issue is controversial today, especially when it comes to the use of BAB in the form of eye drops. Obviously, changes in the mental state can adversely affect the quality of life of patients with glaucoma, cause great damage to their families and society [1,2,7–9].
Objective: to establish the presence and characteristics of depressive disorders in two groups of patients with glaucoma: those who use BAB to reduce intraocular pressure (IOP) and those who use Travatan 0.004%.
Materials and methods. The study involved 98 people aged 56 to 75 years (mean age 64 + 4.56 years). The selection criterion for the survey was the absence of taking BAB tablets. The patients were divided into two groups of equal size: the 1st group used BAB to reduce IOP, the 2nd group used travatan 0.004%.
The presence of depression in the subjects was established according to the ICD-10, when the patients for more than 2 weeks. there were two main symptoms: depressed mood and anhedonia (loss of interest and/or pleasure). Also, the subjects had to report the presence of at least 3 additional signs: pessimism, constant feelings of anxiety or fear, low self-esteem, inability to concentrate and make decisions, thoughts about death, unstable appetite, disturbed sleep [3,6].
there were two main symptoms: depressed mood and anhedonia (loss of interest and/or pleasure). Also, the subjects had to report the presence of at least 3 additional signs: pessimism, constant feelings of anxiety or fear, low self-esteem, inability to concentrate and make decisions, thoughts about death, unstable appetite, disturbed sleep [3,6].
The severity of depressive symptoms was assessed using the A.T. Beck (1961). Having carefully read the groups of statements, the patients chose those that most corresponded to their condition. The sum from 0 to 9 points was regarded as the absence of depression, 10-15 - mild depression, 16-19 - moderate, 20 or more - severe [4,5].
Results. The survey to detect depression took a little time. In each case, the interview with the patient and the processing of the questionnaire took no more than 5–10 minutes.
In the 1st group, depression was detected in 15 (30.6%) patients, in the 2nd group - only 5 (10.2%) people. The average score of depression on the Beck scale was 16. 4±0.05 in the 1st group, 8.4±0.02 in the 2nd group. The severity of depressive symptoms are presented in Table 1.
4±0.05 in the 1st group, 8.4±0.02 in the 2nd group. The severity of depressive symptoms are presented in Table 1.
During the study, we did not notice the dependence of the presence and severity of a depressive state on the duration of the use of BAB. Almost half of the patients with depression - 22 (44.9%) people used these drugs for only 1 to 6 months.
The literature describes cases when patients with depression try to hide mental changes with the help of somatic complaints. They are sure that keeping emotions under control is their own business, they are afraid to be referred to a psychiatrist for treatment and turn mainly to general practitioners [2].
We observed the same picture in patients with glaucoma. They tried to remain silent about their depressive symptoms and complained of a constant feeling of anxiety associated with deteriorating vision, memory loss, asthenia, fatigue, pain in the heart or stomach, poor sleep, changes in appetite, and constipation. All men with signs of a depressive state reported sexual disorders.
Conclusions. Depression in patients with glaucoma may be associated with traumatic events and concomitant somatic diseases, but in patients who use BAB to reduce IOP, they occur 3 times more often than with instillations of travatan 0.004%. Such patients try to disguise the change in the psycho-emotional state with the help of somatic complaints. Therefore, special attention should be paid to patients taking BAB in all dosage forms, regardless of the duration of their use.
An ophthalmologist, as well as a general practitioner, can identify depression with the help of short questionnaires and conversation. Patients with significant psychometric changes need more clinical evaluation and treatment, with the involvement of consultants if necessary. In such cases, it is possible to recommend replacing the BAB with travatan 0.004%, since against its background, depressive changes in the psycho-emotional state are much less common.
Literature
1. Egorov E. A. Ophthalmopharmacology. M.: GEOTAR-Med, 2004. S. 24–26.
A. Ophthalmopharmacology. M.: GEOTAR-Med, 2004. S. 24–26.
2. Erichev V.P. The main directions of antihypertensive treatment of patients with primary glaucoma // Rus. ophthalmol. magazine 2000. V. 1. No. 1. C. 18–21.
3. Zotov P.B., Umansky M.S. Depression in general medical practice (clinic, diagnosis, drug therapy). Methodical manual for doctors. M., 2006. 35 p.
4. Ilyin E.P. Emotions and feelings. SPb., 2001. S. 505–507.
5. Prokhorov A.O. Workshop on the psychology of states: Textbook. St. Petersburg: Rech, 2004. 480 p.
6. Churkin A.A., Martyushov A.N. A practical guide to the use of the ICD-10 in psychiatry and narcology. M.: Publishing house of the SSC S and SP im. V.P. Serbian, 2004. 140 p.
7. Detry–Morel D. Side effects of glaucoma medications // Bull. soc. BelgeOphtalmol. 2006. No. 299. P. 27–40.
8. Schweitzer I., Maguire K., Tuckwell V. Antiglaucoma medication and clinical depression. // Austr & New Zealand J. of Psych. 2001. No. 35.