Best antidepressant for panic disorder
Panic attacks and panic disorder - Diagnosis and treatment
Diagnosis
Your primary care provider will determine if you have panic attacks, panic disorder or another condition, such as heart or thyroid problems, with symptoms that resemble panic attacks.
To help pinpoint a diagnosis, you may have:
- A complete physical exam
- Blood tests to check your thyroid and other possible conditions and tests on your heart, such as an electrocardiogram (ECG or EKG)
- A psychological evaluation to talk about your symptoms, fears or concerns, stressful situations, relationship problems, situations you may be avoiding, and family history
You may fill out a psychological self-assessment or questionnaire. You also may be asked about alcohol or other substance use.
Criteria for diagnosis of panic disorder
Not everyone who has panic attacks has panic disorder. For a diagnosis of panic disorder, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association, lists these points:
- You have frequent, unexpected panic attacks.
- At least one of your attacks has been followed by one month or more of ongoing worry about having another attack; continued fear of the consequences of an attack, such as losing control, having a heart attack or "going crazy"; or significant changes in your behavior, such as avoiding situations that you think may trigger a panic attack.
- Your panic attacks aren't caused by drugs or other substance use, a medical condition, or another mental health condition, such as social phobia or obsessive-compulsive disorder.
If you have panic attacks but not a diagnosed panic disorder, you can still benefit from treatment. If panic attacks aren't treated, they can get worse and develop into panic disorder or phobias.
More Information
- Electrocardiogram (ECG or EKG)
Treatment
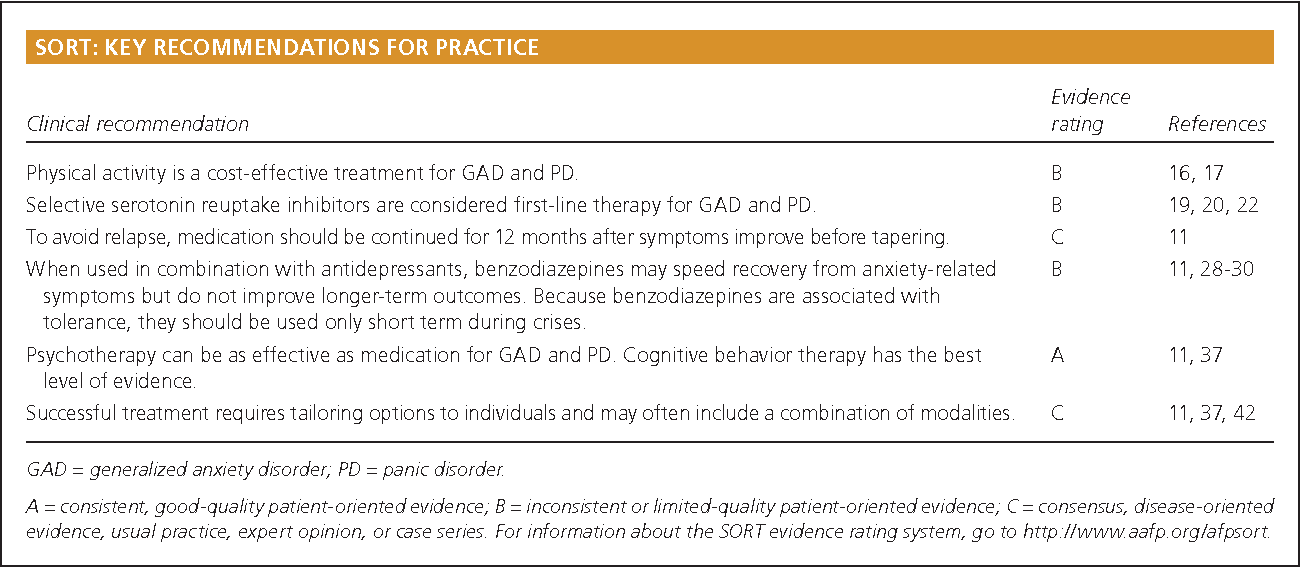
Treatment can help reduce the intensity and frequency of your panic attacks and improve your function in daily life. The main treatment options are psychotherapy and medications. One or both types of treatment may be recommended, depending on your preference, your history, the severity of your panic disorder and whether you have access to therapists who have special training in treating panic disorders.
One or both types of treatment may be recommended, depending on your preference, your history, the severity of your panic disorder and whether you have access to therapists who have special training in treating panic disorders.
Psychotherapy
Psychotherapy, also called talk therapy, is considered an effective first choice treatment for panic attacks and panic disorder. Psychotherapy can help you understand panic attacks and panic disorder and learn how to cope with them.
A form of psychotherapy called cognitive behavioral therapy can help you learn, through your own experience, that panic symptoms are not dangerous. Your therapist will help you gradually re-create the symptoms of a panic attack in a safe, repetitive manner. Once the physical sensations of panic no longer feel threatening, the attacks begin to resolve. Successful treatment can also help you overcome fears of situations that you've avoided because of panic attacks.
Seeing results from treatment can take time and effort. You may start to see panic attack symptoms reduce within several weeks, and often symptoms decrease significantly or go away within several months. You may schedule occasional maintenance visits to help ensure that your panic attacks remain under control or to treat recurrences.
You may start to see panic attack symptoms reduce within several weeks, and often symptoms decrease significantly or go away within several months. You may schedule occasional maintenance visits to help ensure that your panic attacks remain under control or to treat recurrences.
Medications
Medications can help reduce symptoms associated with panic attacks as well as depression if that's an issue for you. Several types of medication have been shown to be effective in managing symptoms of panic attacks, including:
- Selective serotonin reuptake inhibitors (SSRIs). Generally safe with a low risk of serious side effects, SSRI antidepressants are typically recommended as the first choice of medications to treat panic attacks. SSRIs approved by the Food and Drug Administration (FDA) for the treatment of panic disorder include fluoxetine (Prozac), paroxetine (Paxil, Pexeva) and sertraline (Zoloft).
- Serotonin and norepinephrine reuptake inhibitors (SNRIs).
 These medications are another class of antidepressants. The SNRI venlafaxine (Effexor XR) is FDA approved for the treatment of panic disorder.
These medications are another class of antidepressants. The SNRI venlafaxine (Effexor XR) is FDA approved for the treatment of panic disorder. - Benzodiazepines. These sedatives are central nervous system depressants. Benzodiazepines approved by the FDA for the treatment of panic disorder include alprazolam (Xanax) and clonazepam (Klonopin). Benzodiazepines are generally used only on a short-term basis because they can be habit-forming, causing mental or physical dependence. These medications are not a good choice if you've had problems with alcohol or drug use. They can also interact with other drugs, causing dangerous side effects.
If one medication doesn't work well for you, your doctor may recommend switching to another or combining certain medications to boost effectiveness. Keep in mind that it can take several weeks after first starting a medication to notice an improvement in symptoms.
All medications have a risk of side effects, and some may not be recommended in certain situations, such as pregnancy. Talk with your doctor about possible side effects and risks.
Talk with your doctor about possible side effects and risks.
More Information
- Cognitive behavioral therapy
- Psychotherapy
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which
information is beneficial, we may combine your email and website usage information with
other information we have about you. If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
Lifestyle and home remedies
While panic attacks and panic disorder benefit from professional treatment, these self-care steps can help you manage symptoms:
- Stick to your treatment plan. Facing your fears can be difficult, but treatment can help you feel like you're not a hostage in your own home.
- Join a support group. Joining a group for people with panic attacks or anxiety disorders can connect you with others facing the same problems.
- Avoid caffeine, alcohol, smoking and recreational drugs. All of these can trigger or worsen panic attacks.
- Practice stress management and relaxation techniques. For example, yoga, deep breathing and progressive muscle relaxation — tensing one muscle at a time, and then completely releasing the tension until every muscle in the body is relaxed — also may be helpful.

- Get physically active. Aerobic activity may have a calming effect on your mood.
- Get sufficient sleep. Get enough sleep so that you don't feel drowsy during the day.
Alternative medicine
Some dietary supplements have been studied as a treatment for panic disorder, but more research is needed to understand the risks and benefits. Herbal products and dietary supplements aren't monitored by the Food and Drug Administration (FDA) the same way medications are. You can't always be certain of what you're getting and whether it's safe.
Before trying herbal remedies or dietary supplements, talk to your doctor. Some of these products can interfere with prescription medications or cause dangerous interactions.
Preparing for your appointment
If you've had signs or symptoms of a panic attack, make an appointment with your primary care provider. After an initial evaluation, he or she may refer you to a mental health professional for treatment.
What you can do
Before your appointment, make a list of:
- Your symptoms, including when they first occurred and how often you've had them
- Key personal information, including traumatic events in your past and any stressful major events that occurred before your first panic attack
- Medical information, including other physical or mental health conditions that you have
- Medications, vitamins, herbal products and other supplements, and the dosages
- Questions to ask your doctor
Ask a trusted family member or friend to go with you to your appointment, if possible, to lend support and help you remember information.
Questions to ask your primary care provider at your first appointment
- What do you believe is causing my symptoms?
- Is it possible that an underlying medical problem is causing my symptoms?
- Do I need any diagnostic tests?
- Should I see a mental health professional?
- Is there anything I can do now to help manage my symptoms?
Questions to ask if you're referred to a mental health professional
- Do I have panic attacks or panic disorder?
- What treatment approach do you recommend?
- If you're recommending therapy, how often will I need it and for how long?
- Would group therapy be helpful in my case?
- If you're recommending medications, are there any possible side effects?
- For how long will I need to take medication?
- How will you monitor whether my treatment is working?
- What can I do now to reduce the risk of my panic attacks recurring?
- Are there any self-care steps I can take to help manage my condition?
- Are there any brochures or other printed material that I can have?
- What websites do you recommend?
Don't hesitate to ask any other questions.
What to expect from your doctor
Your primary care provider or mental health professional may ask:
- What are your symptoms, and when did they first occur?
- How often do your attacks occur, and how long do they last?
- Does anything in particular seem to trigger an attack?
- How often do you experience fear of another attack?
- Do you avoid locations or experiences that seem to trigger an attack?
- How do your symptoms affect your life, such as school, work and personal relationships?
- Did you experience major stress or a traumatic event shortly before your first panic attack?
- Have you ever experienced major trauma, such as physical or sexual abuse or military battle?
- How would you describe your childhood, including your relationship with your parents?
- Have you or any of your close relatives been diagnosed with a mental health problem, including panic attacks or panic disorder?
- Have you been diagnosed with any medical conditions?
- Do you use caffeine, alcohol or recreational drugs? How often?
- Do you exercise or do other types of regular physical activity?
Your primary care provider or mental health professional will ask additional questions based on your responses, symptoms and needs. Preparing and anticipating questions will help you make the most of your appointment time.
Preparing and anticipating questions will help you make the most of your appointment time.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
Which Anxiety Medication is Best for Me?
Sign in
Welcome!Log into your account
your username
your password
Forgot your password?
Privacy Policy
Password recovery
Recover your password
your email
Search
Every day, millions of people search the internet for answers about treating their anxiety. Which anxiety medication is best? Which antidepressant actually works? What should I take for panic attacks? The search results can be conflicting because there is no “one-size-fits-all” answer for the best medication to treat anxiety. Since every individual is different, a medication that helps your friend’s anxiety may not work for you.
Since every individual is different, a medication that helps your friend’s anxiety may not work for you.
In the United States, starting on anxiety medication requires communicating with a healthcare professional to have a prescription issued for you. If you do not already have a family doctor, we can help you find a healthcare provider.
Family doctors or primary care providers tend to have their own shortlist of anxiety medications that they consistently prescribe from, based on their professional experience. After discussing your anxiety symptoms and reviewing your medical history, he or she may prescribe an SSRI or SNRI from their go-to list.
Most people would prefer to play an active role in their healthcare. With evidence-based guidelines and a few considerations, you can go into the discussion as an informed consumer. You can familiarize yourself with the best available options and prepare your own suggestions.
The majority of people who experience various anxiety disorders can find relief with the help of an SSRI or SNRI medication. Selective serotonin reuptake inhibitors (SSRIs) are medications that increase brain serotonin levels by preventing the reabsorption of serotonin. Low serotonin levels are linked to anxiety and depression. Serotonin-norepinephrine reuptake inhibitors (SNRIs) are medications that work by blocking the reabsorption of both serotonin and norepinephrine in the brain. Norepinephrine has many essential functions and helps the body respond to stressful situations.
Selective serotonin reuptake inhibitors (SSRIs) are medications that increase brain serotonin levels by preventing the reabsorption of serotonin. Low serotonin levels are linked to anxiety and depression. Serotonin-norepinephrine reuptake inhibitors (SNRIs) are medications that work by blocking the reabsorption of both serotonin and norepinephrine in the brain. Norepinephrine has many essential functions and helps the body respond to stressful situations.
Let’s Get Specific: Which SSRI/SNRI Medications are Best for Which Anxiety Conditions?
What does it mean to be “FDA approved”? Before they can be marketed, prescription medicines must go through an extensive approval process to prove that they work and that their benefits outweigh their risks. It takes an average of 12 years for a new drug to hit the pharmacy shelves, and hundreds of millions of dollars are spent on research, development, and clinical trials. Note that the FDA does not actually perform testing; it only reviews the testing process.
The FDA’s decision to approve a medication is supported by reliable scientific data. A long, detailed document accompanies every FDA-approved prescription drug, referred to as the “package insert” or “label.” The approved label provides key information about the medication that includes the specific conditions that the drug is approved to treat as well as dosage and safety info.
Healthcare providers may choose to prescribe a medication for an “off-label” or unapproved use when they judge that it is medically appropriate for their patients. Off-label prescribing is very common for the treatment of various types of anxiety disorders but typically not before trying first-line options.
Generalized Anxiety Disorder (GAD)Selective serotonin reuptake inhibitors (SSRIs) are the standard first-line therapies for generalized anxiety disorder (GAD). Many SSRIs and serotonin-norepinephrine reuptake inhibitors (SNRIs) have effectively treated GAD in clinical trials, but only four medications are FDA-approved for this indication:
- escitalopram (Lexapro) (SSRI)
- paroxetine (Paxil) (SSRI)
- duloxetine (Cymbalta) (SNRI)
- venlafaxine (Effexor XR) (SNRI)
Escitalopram (Lexapro) is generally well tolerated and has fewer reported side effects compared to paroxetine (Paxil), duloxetine (Cymbalta), and venlafaxine (Effexor XR).
Paroxetine (Paxil) may cause more weight gain and should be avoided in people who struggle to maintain a healthy weight. Paroxetine is not a good choice for older adults, for people with a history of heart problems, or people taking multiple medicines due to its risk of drug interactions.
Duloxetine (Cymbalta), an SNRI, may be a better choice than escitalopram (Lexapro) for people that also have fibromyalgia or chronic musculoskeletal pain because it can provide “double duty” relief of pain along with easing the symptoms of GAD.
Medical researchers have performed head-to-head comparison studies of escitalopram (Lexapro) and venlafaxine (Effexor XR) for the treatment of GAD. The study results concluded that overall, escitalopram and venlafaxine are equally effective treatments for GAD. However, more of the study participants reported that they quit taking venlafaxine due to side effects compared to escitalopram, which was better tolerated with fewer side effects.
Social Anxiety Disorder (SAD)Social Anxiety Disorder (SAD) is also known as social phobia. Although many medications have been used off-label to treat SAD effectively, only three SSRIs are FDA-approved for this indication:
Although many medications have been used off-label to treat SAD effectively, only three SSRIs are FDA-approved for this indication:
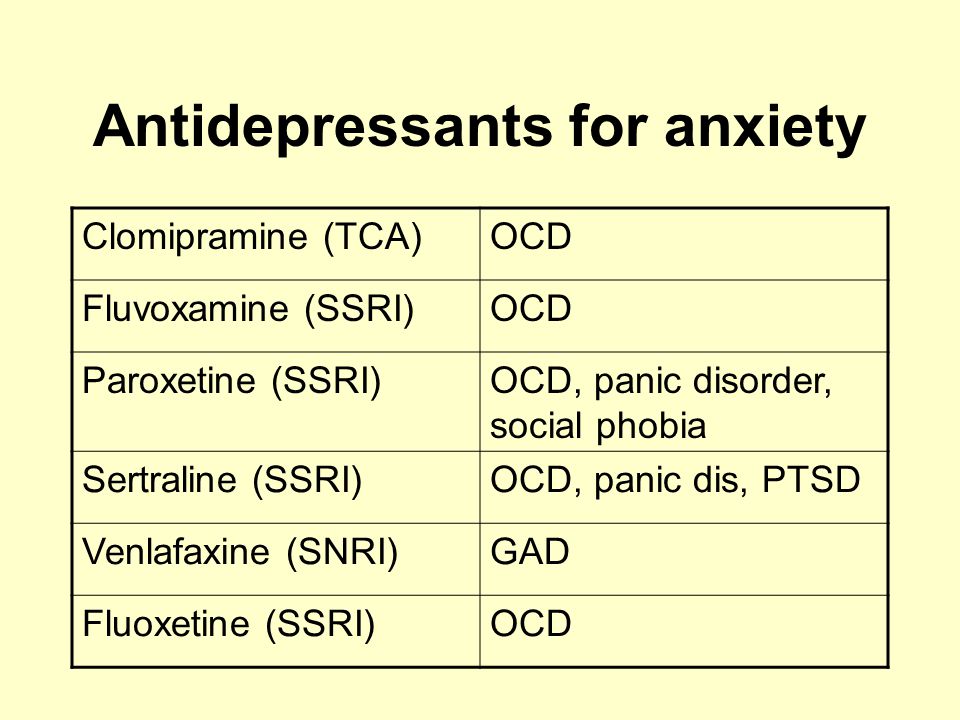
- Fluvoxamine (Luvox)
- Paroxetine (Paxil)
- Sertraline (Zoloft)
Paroxetine (Paxil) was the first medication to receive FDA approval for the indication of social anxiety disorder and is frequently still chosen as first-line treatment by healthcare providers for that reason. As mentioned under GAD, the side effects and safety concerns of paroxetine limit its use.
Sertraline (Zoloft) has a more favorable safety profile compared to paroxetine. Sertraline is the safest SSRI for people with a history of heart problems. Sertraline is also considered safe in pregnancy, breastfeeding, and is approved for use in teens as well as adults.
Fluvoxamine (Luvox) has more potential to interact with other medications, and its effects can be decreased by smoking cigarettes. However, these interactions can be managed with dose adjustments, and fluvoxamine may be the right choice, especially for people who have both social anxiety and obsessive-compulsive disorder (OCD).
The FDA has approved five medications for the treatment of obsessive-compulsive disorder (OCD), which include the following four SSRIs, which are considered first-line treatment options:
- Fluoxetine (Prozac)
- Fluvoxamine (Luvox)
- Paroxetine (Paxil)
- Sertraline (Zoloft)
Before SSRIs came onto the market in the 1980s, the first-line treatment for OCD was a tricyclic antidepressant known as clomipramine (Anafranil). Clomipramine is still an available treatment for OCD in adults and children (10 years and older), but due to its unfavorable side effects, SSRIs are now preferred as first-line.
Fluvoxamine was the first SSRI to be approved by the FDA for OCD, but it has not been proven to be any more or less effective than fluoxetine, paroxetine, or sertraline. Sertraline and fluoxetine are both well-tolerated compared to paroxetine (Paxil). Paroxetine (Paxil) is the SSRI most likely to cause weight gain and should be avoided as the first-line option.
OCD is most commonly treated with SSRIs, but at much higher doses than used to treat anxiety or depression. For reasons not clear, it takes longer for OCD to respond to SSRI treatment than other depressive and anxiety disorders. It may take a trial of 10 to 12 weeks to see improvement.
For people with OCD who only gain limited improvement on a first-line SSRI like sertraline or fluoxetine, one option is to switch to another SSRI. It is estimated that 50% of people with OCD who do not respond to one SSRI will do better with another SSRI. The downside of switching is that this may take another 10 to 12 weeks of waiting to see improvement of the OCD symptoms. Instead of switching SSRIs, another option is to add on another medicine, such as clomipramine (Anafranil), which can produce results within four weeks.
OCD is usually a lifelong illness, though its severity can vary over time. Even with medications and psychotherapy, the symptoms of OCD may never completely go away. However, people with OCD can learn how to manage their symptoms, find support in groups like PACS, and still have enjoyable, fulfilling lives.
However, people with OCD can learn how to manage their symptoms, find support in groups like PACS, and still have enjoyable, fulfilling lives.
Panic disorder and panic attacks are two of the most common mental health problems in the United States. Medications can reduce the intensity and number of panic attacks as well as anxiety related to anticipating a panic attack. The first-line treatments for panic disorder are SSRIs and SNRIs.
FDA-approved SSRIs for the treatment of panic disorder:
- Fluoxetine (Prozac)
- Paroxetine (Paxil)
- Sertraline (Zoloft)
FDA-approved SNRI for the treatment of panic disorder:
- Venlafaxine (Effexor, Effexor XR)
The FDA-approved package inserts for fluoxetine, sertraline, paroxetine, and venlafaxine include the wording “indicated for the treatment of panic disorder, with or without agoraphobia.” Agoraphobia is a type of anxiety disorder in which you fear and avoid places or situations that might cause you to panic.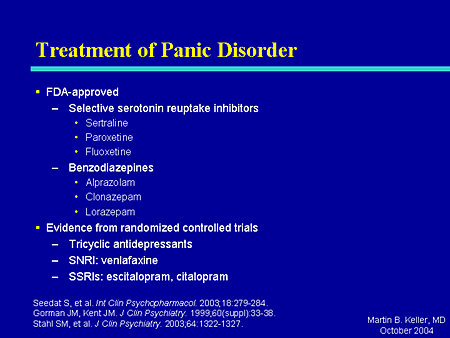
The most popular first-choice medications for panic disorder are sertraline (Zoloft), fluoxetine (Prozac), and venlafaxine (Effexor). Of these options, fluoxetine (Prozac) is relatively activating and not the best choice for people who struggle with insomnia in addition to panic disorder. Paroxetine (Paxil) causes more weight gain compared to other SSRIs and is not an ideal selection for people with diabetes or heart problems.
Sertraline (Zoloft) and venlafaxine (Effexor) are equally useful for treating panic disorder with or without agoraphobia. They are also overall the most well-tolerated medications for the treatment of panic disorder. Of the two, sertraline would be a safer choice for people with a history of heart problems.
Note that medications like sertraline (Zoloft) and venlafaxine (Effexor) must be taken for one to three weeks before beginning to improve the symptoms of panic. SSRIs and SNRIs will not help when taken in the middle of a panic attack, but they can prevent future panic attacks.
Benzodiazepines (alprazolam, lorazepam) may be prescribed for panic attacks, especially during the initial phase of starting an SSRI or SNRI, which may take a few weeks to start working. Benzodiazepines are fast-acting and bring relief within 30 to 60 minutes. They promote relaxation and reduce muscular tension and other panic symptoms. Long-term use of benzodiazepines is usually not recommended due to problems related to building up a tolerance and becoming dependent.
Choosing a MedicationAnxiety disorders may run in your family. When choosing a medication with your doctor, be sure to mention if you know if a particular drug worked well for your parent’s or sibling’s anxiety. Due to shared genetics, the same medication could be beneficial for you too.
It is essential to understand that taking an SSRI or SNRI is a commitment to improving your health. Your dose must be taken every day, around the same time each day. If you miss doses, you may not feel very well due to withdrawal-like symptoms (headache, nausea, irritability). You could also experience a sudden return of your anxiety symptoms.
If you miss doses, you may not feel very well due to withdrawal-like symptoms (headache, nausea, irritability). You could also experience a sudden return of your anxiety symptoms.
It may take time for you to find a doctor, therapist, support network, and medication that helps you manage your symptoms. It is very common to try more than one remedy before finding one that works well for your anxiety disorder and does not cause bothersome side effects. Work actively with your healthcare provider to craft your personalized treatment plan. Have patience and take one step at a time towards a healthier you.
Related Articles
About Us
© 2022 Panic and Anxiety Community Support | All rights reserved
Contact Us
Fighting depression: 10 modern drugs
{{if type === 'partner-stocks'}}
{{/if}}
{{/if}} {{each list}}${this} {{if isGorzdrav}} nine0003
Delete
{{/if}}
{{/each}} {{/if}} Search by drug, disease, substance: DERMAKOSMETIKA, SOLGAR, R. O.C.S., Bifiform,
O.C.S., Bifiform, Home
Articles nine0003
Fighting depression: 10 modern drugs
Depression is an urgent problem, the number of visits to doctors is growing every year. It can be solved by contacting a psychotherapist and taking antidepressants . These are drugs that regulate the production of hormones and biochemical processes in the body. It is strictly forbidden to prescribe them to oneself , as these are complex drugs with certain restrictions, side effects effects . The doctor must authorize their appointment and control the intake. We will tell you which of them are the most effective and common in medicine, how many they have pluses and minuses.
What is meant by
depressionDoctors have known it since ancient Greece and Egypt. Hippocrates described it as melancholy - a condition that is accompanied by anxiety, despondency, insomnia, refusal of food, irritability. Most often, the cause is childhood trauma or severe, frequent stress in adulthood. There are many provoking factors: the death of a loved one, deterioration of living conditions, alcoholism, brain diseases. Such cases are referred to as psychogenic depression. nine0003
The second type is endogenous. The problem appears not from large external shocks, but because of internal causes. A person is constantly dissatisfied with himself, subjecting himself to criticism. Many patients have panic attacks , haunted by a feeling of fear, anxiety.
How long the period of depression lasts
Many people mistake ordinary periods of low mood for depression. If they do not last long and are quickly replaced by periods of recovery, then we are not talking about a depressive state. The problem is obvious when the symptoms persist for months and dramatically change a person's life. Then you need to see a doctor. nine0003
The problem is obvious when the symptoms persist for months and dramatically change a person's life. Then you need to see a doctor. nine0003
What happens to the body
The most common theory is that there is a malfunction of neurotransmitters located in the brain. These substances transmit signals from neuron to neuron and are responsible for a person's mood. Dysfunction leads to a slowdown in the rate of this transmission and a decrease in the number of neurotransmitters themselves. Serotonin, which is called the "hormone of happiness", suffers the most. For clarity, this biochemical process can be compared, for example, with a drop in blood sugar levels in diabetes mellitus. nine0003
How is
treated depression Depression has been treated in different ways. In the ancient world - emetics and laxatives. In the Renaissance - wine and sunbathing. In the Age of Enlightenment - external stimuli, for example, insects. The 19th century brought new recipes - in particular, a solution of camphor in tartaric acid. The treatment also included the use of drugs, which are now no longer allowed for sale, and some are recognized as narcotic.
The treatment also included the use of drugs, which are now no longer allowed for sale, and some are recognized as narcotic.
Obviously, all these drugs had no effect on increasing the amount of serotonin. And the treatment is precisely to normalize its production. This was done after creating modern antidepressants , which have a minimum of side effects, are safe for the body and are not addictive. These are medicines, whose action is aimed specifically at balancing the disturbed balance of neurotransmitters: serotonin, norepinephrine, dopamine.
Prescription
If a healthy person takes antidepressants , there will be no effect . For a depressed patient, taking them will help:
- improve psychological state;
- get rid of irritability;
- panic fear;
- increase mental and physical activity;
- overcome the dreary mood.
Psychiatrists prescribe antidepressants for chronic back pain, headaches. And also with irritable bowel syndrome, incontinence and other cases when the body stops producing its own painkillers. Medication helps restore pain suppression mechanisms. nine0003
These drugs can only be taken with a doctor's prescription, as many of them are strong stimulants. Self-administration may cost dearly - the condition may worsen. Only a doctor will correctly calculate how many medicines to take per day. In parallel with the treatment by a psychiatrist, a neurologist, a consultation of a psychotherapist is required.
Precautions
- Prescribed drug start drinking from a small dose - the first couple of days they take a quarter of a tablet. Gradually increase the dose to normal.
 So the body adapts better. Finish the course by reducing the dose.
So the body adapts better. Finish the course by reducing the dose. - The first effect of appears only 2 weeks after the start of administration. Sustained action - after six months. All this time, you need to take remedy, without making passes, breaks.
-
Products are not combined with melatonin, St. John's wort, products and dietary supplements based on sibutramine, 5-HTP. Their combination can raise serotonin to dangerous levels. Also, you can not combine them with monoamine oxidase inhibitors, for example, Cipralex. When writing a prescription, the doctor takes these points into account. nine0003
- Drinking antidepressants is better in parallel with visits to a psychotherapist. If the drugs normalize the biochemical processes in the body, then this doctor will help normalize the psychological state after depression.
The best antidepressants
In medicine, they have long argued that some drugs give only a placebo effect. The purpose of the study was to find out which of them are the most effective and valid . The project involved 116 thousand patients, and its results were published by the authoritative edition of the Lancet. We offer a list of the best.
The purpose of the study was to find out which of them are the most effective and valid . The project involved 116 thousand patients, and its results were published by the authoritative edition of the Lancet. We offer a list of the best.
1. Agomelatine
New generation drug. Agomelatine is used for severe depressive disorders, high levels of anxiety. Enhances the release of dopamine and norepinephrine, stimulates melatonin receptors. The standard therapeutic dose is 25-50 mg 1 time / day. Helps to restore the normal structure of sleep, get rid of anxiety and panic attacks attacks
Pros
+ Does not adversely affect attention and memory.
+ No lethargy during the day.
+ No sexual deviations.
+ No relation to blood pressure.
+ Do not reduce dosage upon discontinuation.
Cons
— In 1-10% of cases, increased sweating, diarrhea, constipation.
- Possible increased fatigue, drowsiness.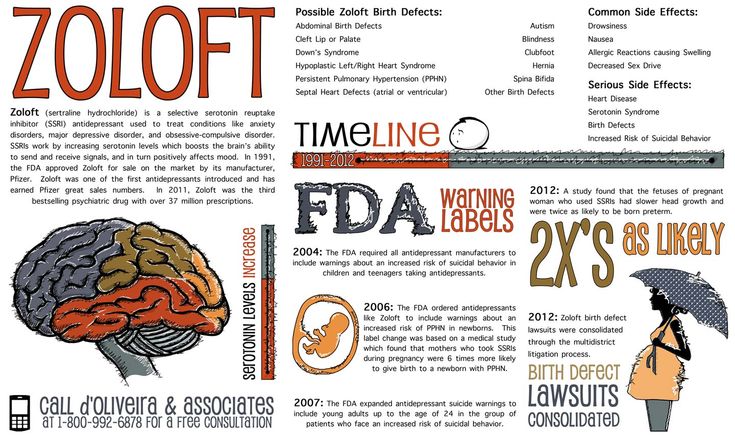
- There are no evidence-based safety studies in people with renal or hepatic insufficiency, therefore, such patients are advised to refrain from taking drugs with active ingredient agomelatine.
2. Amitriptyline
Tricyclic antidepressant. Moreover, the World Health Organization considers Amitriptyline the most reliable in this group. The standard dose is 200-250 mg / day. The action is to block the reuptake of neurotransmitters. A good remedy for moderate to severe disorders of the endogenous type. Additionally, it has a sedative and hypnotic effect. Effective in the treatment of neuropathic pain, for the prevention of migraine. nine0003
Pluses
+ Preparations with active ingredient amitriptyline are inexpensive.
+ High reliability, minimum side effects.
+ Relatively safe during breastfeeding.
Cons
- Possible side effect in the form of blurred vision, dry mouth.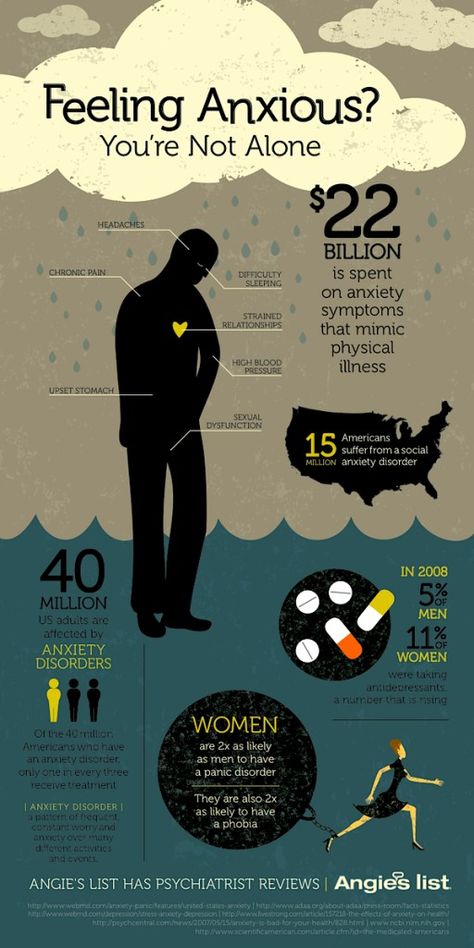
- Lowering blood pressure.
- Some patients experience constipation.
- Drowsiness. nine0003
3. Escitalopram
It belongs to the group of modern serotonin reuptake inhibitors (SSRIs). Most often, it is recommended to take for anxiety, panic attacks. It is taken once, the standard dose is 10 mg per day. Escitalopram has a milder effect and is prescribed to patients for whom tricyclic drugs are contraindicated.
Pluses
+ Lasting effect comes after 3 months. nine0003
+ Indicated for patients with disorders of the cardiovascular system.
+ Soft action.
Cons
- In some patients, the functions of the gastrointestinal tract are disturbed, which is most often expressed in diarrhea.
- Anxiety may increase during the first 2 weeks, therefore it is recommended to start treatment with low doses and gradually increase them.
- Contraindicated in pregnancy and lactation.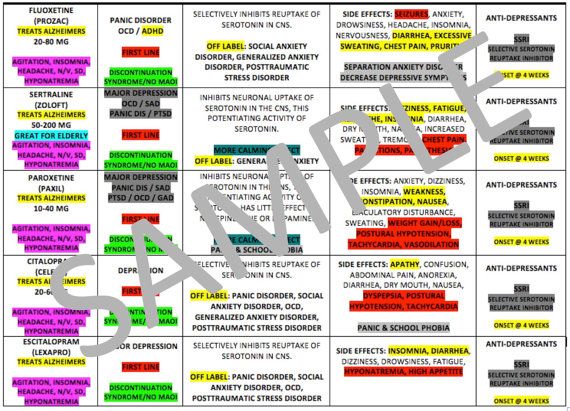
4. Mirtazapine
A drug of the tetracyclic group. Mirtazapine - good stimulant for anxious depressions, has a moderate sedative effect. The average amount is 30 mg / day, it must be consumed once. Usually it is prescribed to patients who lose interest in life, cease to experience joy, pleasure. Effective in the correction of sleep, in particular, early awakenings.
Pros
+ Earlier onset of action than SSRIs (1 week).
+ Works well with most general medicines. nine0003
+ Full effect in 4 weeks.
+ Does not affect sexual function.
Cons
- The active substance mirtazapine is contraindicated in diabetes mellitus, arterial hypotension, increased intraocular pressure.
— During the appointment, you must drive carefully and engage in potentially hazardous types of work.
- 18% of patients experience drowsiness, 15% dry mouth, 5% weight loss. Other side effects occur in 1-3% of cases.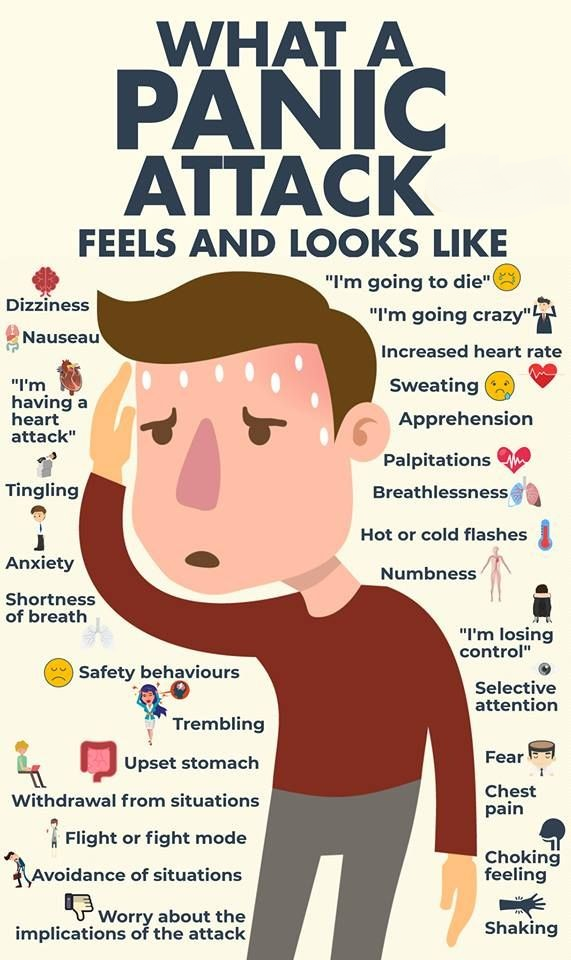 nine0003
nine0003
5. Paroxetine
Belongs to the SSRI group, is used most often for severe anxiety, panic, social phobia, nightmares, stress after trauma. Paroxetine can resolve the problems of anxious depression, anxiety-phobic disorders. Take once a day at a dose of 20 mg.
Pros
+ The most powerful stimulant among SSRIs.
+ Anxiety and insomnia pass quickly.
+ Minimal side effects in the form of vomiting, diarrhea. nine0003
+ Suitable for patients with cardiovascular problems.
Cons
— Not suitable for patients with severe motor, mental inhibition.
- Reduces libido.
- Harmful to the fetus when taken during pregnancy.
6. Fluoxetine
One of the most commonly used antidepressants in the SSRI group. Known as Prozac. Fluoxetine is also known as a good mood stimulant. Patients have a feeling of fear, tension, anxiety, gloomy dislike for others. Pluses + There is practically no effect on the work of the heart. + Does not cause sedation. + Effective for patients with motor retardation and excessive daytime sleepiness. Cons - May cause weight loss. — Hypoglycemia is possible in diabetes mellitus. - Contraindicated in severe renal impairment. Another SSRI drug. Fluvoxamine is similar to Prozac Fluoxetine but is fast acting and may cost cheaper. The effect is in a more active slowing down of the reuptake of serotonin by neurons. It is indicated for depression of various origins, as well as obsessive-compulsive disorders. The average daily dose is 100 mg. Pros + Lower price than traditional Prozac. + Faster action than him. + Relatively minor side effects (diarrhea, dry mouth, drowsiness). Cons - Contraindicated in diabetes. - Pregnant women - with caution, lactation - prohibited. - Causes nausea in some patients. One of the widely used and universal drugs of the SSRI group. They treat almost any depressive condition, panic disorder, social phobia. However, in severe clinical cases, sertraline may not be effective enough. The standard dose is 50 mg/day. Pros + No cardiotoxicity. nine0003 + The patient's psychomotor activity does not change. + Does not increase body weight. + Combines well with other groups of antidepressants. Cons — In the first 2 weeks there may be problems with sleep, diarrhea. - Side effects of a sexual nature. - Contraindicated in pregnant women. The drug is classified as an SSRI. Its difference is in its effectiveness in depression, which is accompanied by involuntary movements (tic, tremor, chewing, smacking). Pluses + Effective in tardive dyskinesia. + One of the most powerful SSRIs. + More pronounced thymoleptic effect (improvement of mood) compared to many antidepressants of the same group. Cons - In some patients, anxiety increases within 2 weeks after starting treatment. — Gastrointestinal disorders, insomnia, agitation are possible. — Use during pregnancy only in extreme cases, incompatible with feeding. nine0003 Belongs to the SNRI group. In addition to blocking the reuptake of serotonin, venlafaxine has a similar effect on another neurotransmitter, norepinephrine. The medicine is prescribed for depressive conditions of various origins, social phobias, anxiety, panic. Usually take 150 mg per day. Pros + Better tolerated by patients than most tricyclics. + More pronounced effect than classic SSRIs. nine0003 + Fewer contraindications. Cons - Traditional side effects of most antidepressants: nausea, drowsiness, dry mouth, diarrhea or constipation. - May increase eye pressure. - The most severe withdrawal syndrome among antidepressant drugs. This list is not to be used as a recommendation. In any case, consult your doctor before purchasing. Be healthy! Why is this review important? Panic disorder is common in the general population. It is characterized by panic attacks, periods of fear or anxiety of rapid onset, accompanied by other symptoms (physical sensations and obsessive fear). Treatment for panic disorder includes psychological and pharmacological interventions, often combined. According to the recommendations, antidepressants of various classes are the standard option for pharmacological intervention. Who might be interested in this review? Panic disorder sufferers and general practitioners. What questions does this review seek to answer? How effective are antidepressants in treating panic disorder compared to a sham treatment (known as a placebo)? What is the acceptability of antidepressants in the treatment of panic disorder compared to placebo? How many unwanted and adverse effects occur when using antidepressants in the treatment of panic disorder compared with placebo? nine0003 What studies were included in this review? We searched all relevant studies in electronic databases. The included medical studies compared antidepressant treatment with placebo in adults diagnosed with panic disorder. The studies were to be randomized controlled trials (RCTs), i.e. allocation of participants to receive intervention or placebo was to be random. What does the evidence from this review say? We found evidence that antidepressants are better than placebo in terms of efficacy and early dropout rates. However, our results also indicated that antidepressants were less well tolerated than placebo and resulted in more withdrawals due to adverse effects. The results have the following limitations: some studies were funded by pharmaceutical companies and only assessed short-term outcomes. We found almost no data on other clinically relevant outcomes such as function and quality of life. The quality of the available evidence ranged from very low to high. nine0003 What should happen next? Studies should be conducted that evaluate outcomes over a long-term follow-up period to determine whether the effect is transient or permanent. Any harm experienced by trial participants should be more fully reported. In addition, a future network meta-analysis will cover all pharmacological interventions used in panic disorder and is likely to shed light on this complex issue by providing more data on the comparative effectiveness of different interventions. Depending on the indications, the average daily dose is 20-60 mg. nine0003
Depending on the indications, the average daily dose is 20-60 mg. nine0003 7. Fluvoxamine
 nine0003
nine0003 8. Sertraline
9. Escitalopram
 Escitalopram is prescribed to patients with panic, anxiety, phobias, obsessive thoughts or actions. The daily dose is 20 mg. nine0003
Escitalopram is prescribed to patients with panic, anxiety, phobias, obsessive thoughts or actions. The daily dose is 20 mg. nine0003 10. Venlafaxine
 Evidence for their effectiveness and acceptability is unclear. nine0003
Evidence for their effectiveness and acceptability is unclear. nine0003  We included in this review 41 RCTs involving 9377 people.
We included in this review 41 RCTs involving 9377 people.