Asperger self diagnosis
Do I Have Symptoms of ASD or Aspergers?
Do I Have ASD? Autism Test for Adults
Awareness of autism spectrum disorder (ASD) has grown dramatically in recent years, which reflects an increase in autism tests and diagnoses — and in the public’s understanding that, even late in life, an autism diagnosis can offer major benefits and relief. Still, symptoms of autism — particularly those previously associated with Aspergers — are still frequently misdiagnosed as attention deficit hyperactivity disorder (ADHD), mood disorders, obsessive compulsive disorder (OCD), and other related conditions — leading to poor treatment and lifelong challenges.
Adults with autism may have a history of delayed language language and/or movement skills, delayed cognitive or learning skills, unusual eating or sleeping habits, emotional dysregulation, anxiety, stress, and/or fear. If you recognize yourself or a loved one in the following descriptions of autism spectrum disorder, make an appointment with a health care professional to discuss an evaluation test for autism.
This free autism test was adapted from the Autism Spectrum Screening Questionnaire (ASSQ) designed to screen the possibility of ASD, and is for personal use only. This is not a diagnostic tool. An accurate diagnosis can only be made through clinical evaluation. This autism test is for personal use only.
Do you prefer to play individual games and sports like golf, where everyone works for themselves, instead of team sports and games where everyone works toward a common goal?
Very Often
Often
Sometimes
Rarely
Never
Did bullies target you in grade school?
Very Often
Often
Sometimes
Rarely
Never
Think about your daily routine. Would you say you follow the same schedule every day of the week, and don’t like unexpected events?
Very Often
Often
Sometimes
Rarely
Never
Are you always the first one to notice when a friend has gotten a haircut or made a small change to their appearance?
Very Often
Often
Sometimes
Rarely
Never
Is your memory like a steel trap, even for facts that you don’t fully understand?
Very Often
Often
Sometimes
Rarely
Never
Are you always bumping into things, or tripping over your own feet?
Very Often
Often
Sometimes
Rarely
Never
Do you have trouble understanding what people mean when they say they feel embarrassed for someone else?
Very Often
Often
Sometimes
Rarely
Never
Even when you’re in a quiet place, like the library, do you find yourself making involuntary noises, like clearing your throat over and over?
Very Often
Often
Sometimes
Rarely
Never
Are you really (really) good at a skill like math or music, but struggle to succeed in other areas?
Very Often
Often
Sometimes
Rarely
Never
When you’re having a conversation with someone, do you prefer to look at the wall, their shoes, or anywhere but directly into their eyes?
Very Often
Often
Sometimes
Rarely
Never
Do you talk to friends at a party the same way you would talk to co-workers in the office?
Very Often
Often
Sometimes
Rarely
Never
Do your family members lovingly refer to you as the “eccentric professor” of the family?
Very Often
Often
Sometimes
Rarely
Never
Do people say that you speak like a robot?
Very Often
Often
Sometimes
Rarely
Never
Have you always wanted a best friend, but never found one?
Very Often
Often
Sometimes
Rarely
Never
Do you prefer to read non-fiction over fiction books?
Very Often
Often
Sometimes
Rarely
Never
Do you enjoy inventing your own words and expressions that might seem quirky to others?
Very Often
Often
Sometimes
Rarely
Never
Are expressions like “Curiosity killed the cat” or “Don’t count your chickens before they hatch” odd to you?
Very Often
Often
Sometimes
Rarely
Never
(Optional) Would you like to receive your autism symptom test results — plus more helpful resources — via email from ADDitude?
Sign me up for your Adult ADHD newsletter.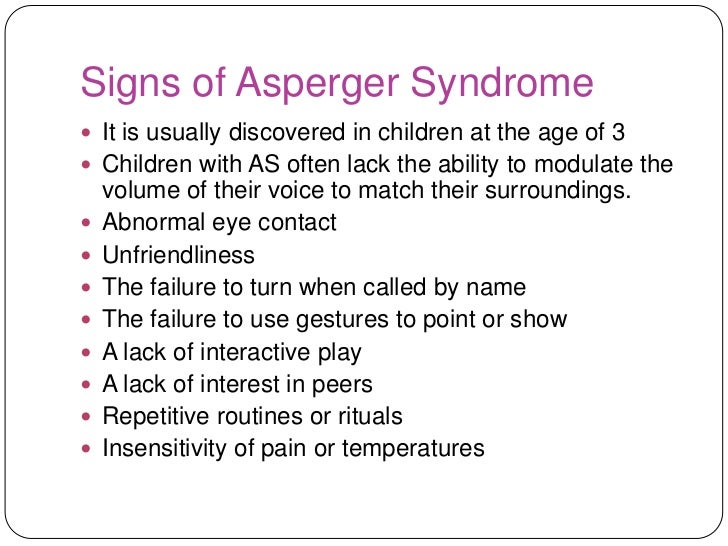
Can’t see the autism test questions above? Click here to open this test in a new window.
Autism Test Next Steps: Autism Spectrum Disorder In Adults
1. Take: The ADHD Test for Adults
2. Read: What Does Autism Look Like in Adults?
3. Find: Specialists or Clinics Near You
4. Read: How to Get Evaluated for Autism as an Adult
5. Take This Test: OCD in Adults
6. Get the eBook “The Truth About Autism in Adults”
7. Listen to the Webinar: “Could I Be on the Autism Spectrum?”
8. Take This Test The Autism Test from WebMD
9. Read: Say Goodbye to Aspergers Syndrome
10. Find: Specialists or Clinics Near You
Previous Article Next Article
Adult ASD: Self-diagnosis or Professional Diagnosis?
Diagnosis
musingsofanaspie 56 Comments
Part 5 in the I Think I Might Be Autistic Series
Whether you choose to seek a diagnosis or not is a personal decision. As an adult, there’s a good chance you don’t need a diagnosis. You’ve done your research, come to the conclusion that you’re on the spectrum and that’s good enough for you.
As an adult, there’s a good chance you don’t need a diagnosis. You’ve done your research, come to the conclusion that you’re on the spectrum and that’s good enough for you.
This is commonly known as self-diagnosis and when done correctly, it’s largely a well-respected approach in the ASD community. The primary reason? Getting an official diagnosis as an adult is difficult:
- Asperger’s Syndrome and autism present differently in adults than in children. Finding someone trained and experienced in adult diagnosis can be challenging.
- Many adults face numerous misdiagnoses before getting correctly diagnosed with Asperger’s or autism.
- Women in particular are often misdiagnosed because they present differently than male aspies on whom the traditional model is based.
- Diagnosis can be expensive and an adult evaluation isn’t covered by most health insurance.
- Diagnosis can lead to bias, stigma and/or create practical limitations, like not being able to join the military or having your parental rights questioned.
So how does self-diagnosis work? First, be prepared to do some work. Self-diagnosis isn’t as simple as taking the AQ and deciding you’re an aspie. Screening questionnaires can be a good place to start, but they’re just that: a first step.
(click on the graphic for a larger version)Here are some additional steps you can take to verify, challenge or test out your belief/suspicion that you’re on the spectrum:
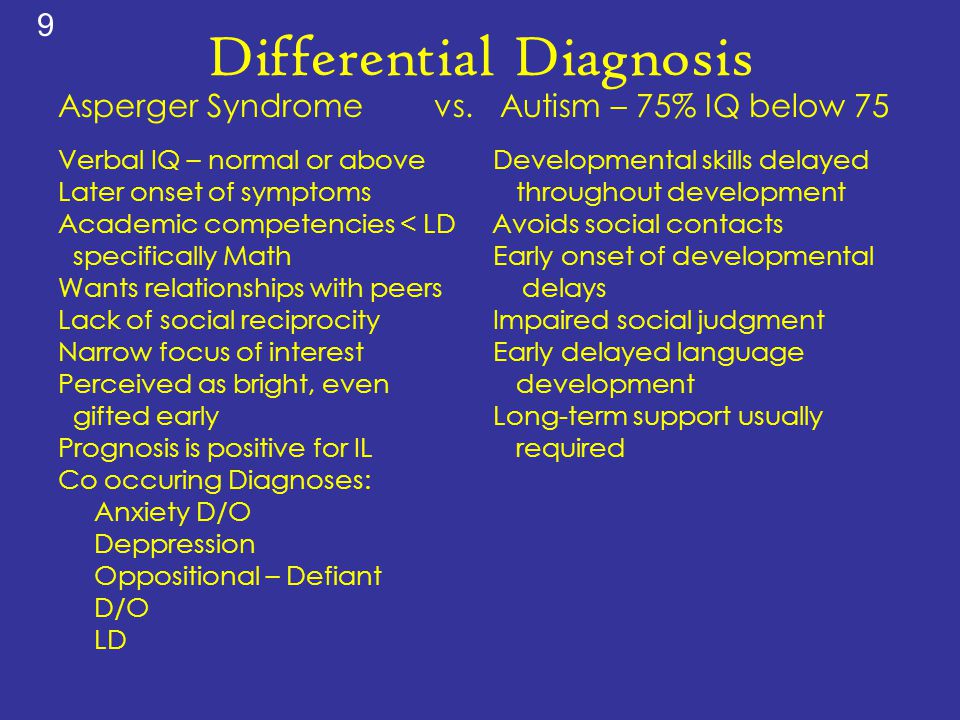
- Look at the DSM and/or ICD criteria for ASD (DSM-IV-TR criteria for Asperger’s and ASD, DSM-V criteria for ASD,ICD-10 criteria for Asperger’s and ASD).
- Be sure you understand what each of the criteria means. ASD criteria manifest differently in adults than in children, so look for examples of adult traits when considering whether the diagnostic criteria applies to you. It may also be helpful to think back to your childhood and try to determine whether you met the early signs of autism.
- Read books on the subject, both nonfiction (like The Complete Guide to Asperger’s Syndrome) and personal narratives (like Pretending to Be Normal or The Journal of Best Practices).
- Read about the experiences of Autistic adults (scroll to the bottom of the linked post for a list of Autistic bloggers). If possible, talk with one or more Autistic adults. Comparing experiences with diagnosed adults can be validating. Also, there are many Autistic adults online (Tumblr, Twitter, Facebook, bloggers) who are happy to answer questions about specific aspects of autism and being autistic. Just keep in mind that Autistic adults are people too and we have a broad range of opinions as well as differing comfort levels when it comes to sharing our personal experiences.
- Make a realistic assessment of your AS/autistic traits based on your reading.
- Talk with one or more trusted persons in your life about your self-assessment. Do they see the same traits that you’re perceiving? Share a list of ASD traits (female ASD traits) with them. Do they see traits that you haven’t considered?
- If you have access to childhood materials like report cards, school work, a baby book or old home movies/videos, review them in light of the childhood symptoms of AS/autism.
- If possible (and if you feel comfortable) ask your parents about your childhood. If you don’t want to frame your questions in terms of autistic symptoms, you could simply ask things like “Did my teachers say I [did X or behaved like Y]?” or “Do you remember me doing [X, Y or Z] when I was a toddler?”
As you do your research, keep in mind that not everyone has every symptom. Symptoms can change in severity and presentation over a lifetime, becoming either more or less noticeable with age. In fact, it’s not unusual to find that as you age, one trait (like sensory sensitivities) becomes more manageable while another (like executive dysfunction) increases in severity.
By the time you’ve completed your research, you should have a good idea of whether Asperger’s syndrome or autism is a good fit for you. Many adults are content with this and choose to self-identify as aspie or autistic based on their self-discovery process. Others feel the need (or have a specific reason) to seek out a professional diagnosis, which can be a long and difficult journey.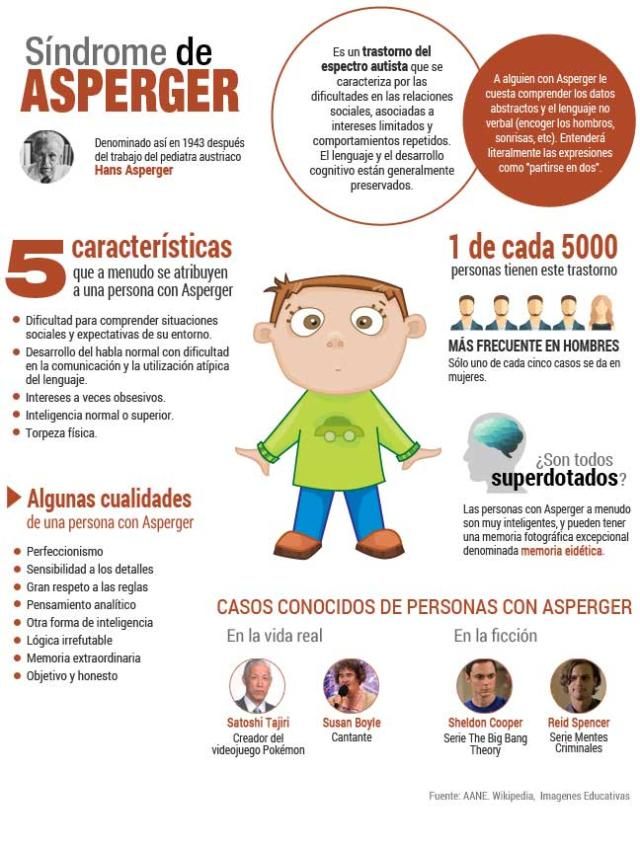
Even if you choose to pursue a professional diagnosis, you may want to work through the self-discovery process first. Often, getting diagnosed as an adult requires making a solid case for why you think an autism diagnosis fits you.
Weighing Self- vs. Professional Diagnosis
- Obtaining a diagnosis as an adult can be very difficult.
- Not everyone needs or wants a professional diagnosis.
- Self-diagnosis is widely accepted in the autism community when done with diligence.
- Self-discovery is a good first step toward professional diagnosis if you choose to pursue it.
Next in the series: Seeking a professional diagnosis
Like this:
Like Loading...
diagnosisorigin storyself-diagnosis
"Nerdy Shy and Socially Inappropriate"
Available from Amazon.com
"I Think I Might Be Autistic: A Guide to Autism Spectrum Disorder Diagnosis and Self-Discovery for Adults" e-book is available for Kindle (Amazon. com), Nook (BN.com) and iPad (iTunes store)
com), Nook (BN.com) and iPad (iTunes store)
Affordable stim toys, chewable jewelry and fidgets ~ Autistic owned and operated ~ 10% of sales go back to the autistic community ~ www.stimtastic.co
Taking The Aspie Quiz
That's What Love Is. Thoughts . . .
Aspie Tests
Taking the RAADS-R Test
Taking the SPD Checklist
-
Yesterday I ventured way way way outside my comfort zone to record an interview on Autism Spectrum Radio. The host, Rob Haupt, asked some great questions and was easy to talk to. You can listen to our conversation here. Rob does a short intro and then the rest of show (about 35 minutes) is our conversation.
musingsofanaspie 13 Comments
-
My friends Ibby Grace And Amy Sequenzia are editing an anthology titled “Typed Words, Loud Voices”, a collection of works by people who type to talk always or sometimes.
 They’re looking for essays, poems, stories or whatever form of expression you’d like to share your message in.
They’re looking for essays, poems, stories or whatever form of expression you’d like to share your message in.The full details about the book, including submission guidelines are at Typed Words, Loud Voices. Continue reading →
musingsofanaspie 5 Comments
-
As some of you noticed yesterday, I’ve updated the blog theme to add a little color. Maybe down the road I’ll experiment with some of the new features (like this one that allows short “aside” posts). It’ll take some getting used to, I know.
And yes the remodeling is an indication of just how bored I am with all the not writing I’m doing.
Triathlon training is chugging along nicely – 3 weeks to go and I feel great, if a bit worn out. The garden is producing lots of cucumbers and tomatoes, a few eggplants and peppers. And for some reason I’m the only person on earth who can’t grown squash? With the exception of one green squash a couple of weeks ago, all I’m getting are tiny little squash that turn yellow and wither.
Besides a renewed obsession with The Sims, that’s about all that’s new around these parts.
musingsofanaspie 53 Comments
Find me on Facebook:
- acceptance
- accomodations
- adolescence
- adult diagnosis
- aging
- alexithymia
- anxiety
- aphasia
- asperger's syndrome
- asperger's tests
- Asperger's traits
- asperger traits
- aspie and female
- aspie girlhood
- aspie strengths
- childhood
- cognitive function
- communication
- communication deficit
- coping strategies
- decision making
- diagnosis
- disability
- e-book
- echolalia
- emotional dysfunction
- emotions
- empathy
- executive function
- experiments
- flash blog
- gender
- gender differences
- giveaway
- identity
- interoception
- language
- marriage
- mental-health
- mindfulness
- Monday morning musings
- motherhood
- nonverbal communication
- origin story
- parenting
- perseveration
- reading facial expressions
- relationships
- self-awareness
- self-care
- self-employment
- sensory dysfunction
- sensory overload
- sensory processing
- sensory regulation
- sensory seeking
- sensory sensitivities
- social communication
- social communication issues
- social interaction
- social scripts
- social skills
- special interests
- speech
- stimming
- supports
- survey
- tactile defensiveness
- take a test Tuesday
- this is me
- unfiltered aspie
- verbal communication
- work
- writing
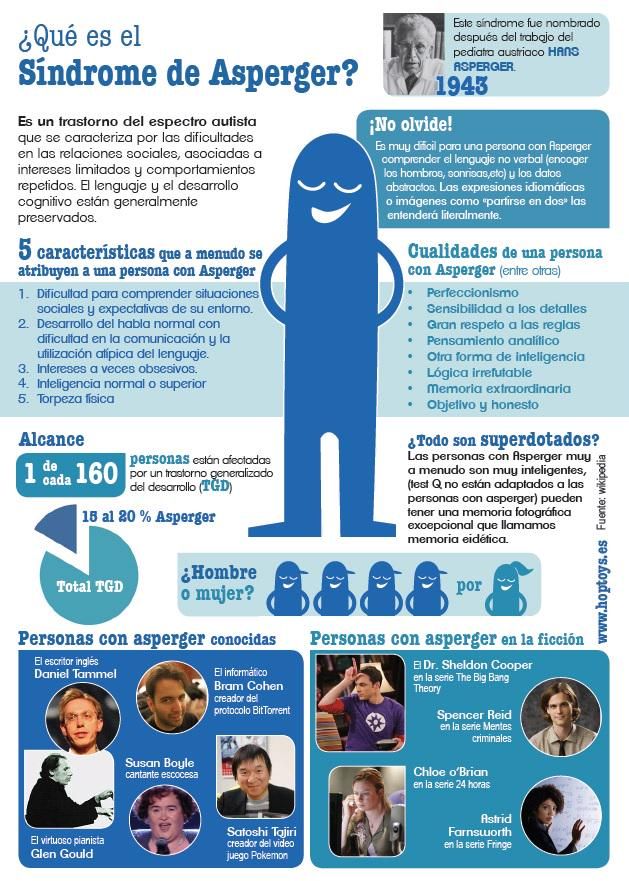
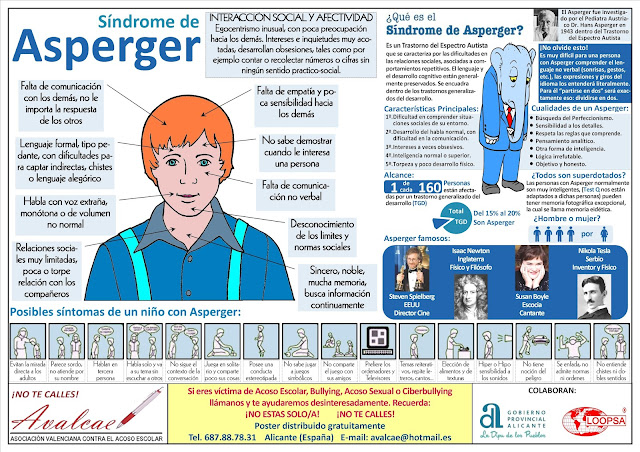
Self-diagnosis of Asperger's syndrome: before, during, after
Asperger's syndrome is a neurological condition that affects a person's development, his daily life and behavior.
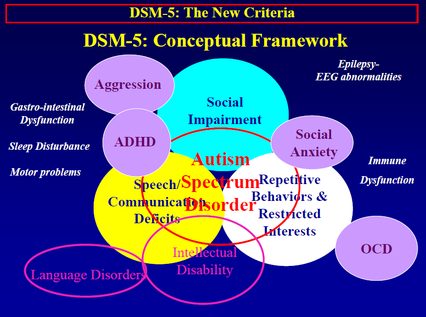
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), Asperger's syndrome is an autism spectrum disorder (associated with level 1). "International Classification of Diseases" (ICD-10) defines it as an independent diagnosis F84.5 of the class "General disorders of psychological development".
Historically, there is no diagnosis of Asperger's syndrome and autism in adults in Russia. Therefore, people are forced to resort to self-diagnosis in an attempt to understand their condition and shape their future life, taking into account their own characteristics.
1. Prerequisites for self-diagnosis of Asperger's Syndrome
1.1 Establishing and maintaining interaction in educational and work teams is accompanied by difficulties and sometimes failures.
1.2 Stress in case of changes or changes in the usual schedule, the need for predictability and stability.
1.3 Repeated references by others to atypical use of the non-verbal component of communication.
1.4 Regular remarks of others about inadequate response to events, situations.
1.5 Repeated remarks by others about the atypicality of sensorimotor processes.
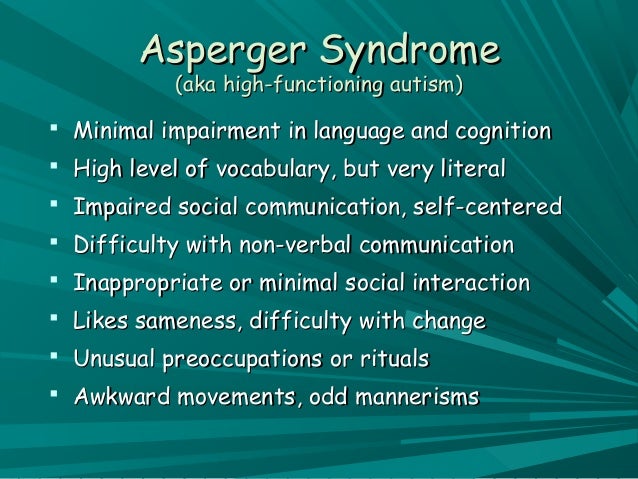
2. Recognizing the symptoms of Asperger's Syndrome
2.1 Atypical eye contact: tendency to avoid "eye-to-eye" gaze, directing gaze when communicating to the side or at the lips of the interlocutor, sometimes unnatural "staring" look.
2.2 Peculiar prosody: monotony, disturbed melody of speech, too loud or soft voice, poor intonation.
2.3 Body language is little used: atypical gesticulation or its absence, occasional use of nods or shrug as an accompaniment to speech, postures not aimed at expressing attitude to what is happening.
2.4 Motor skills are complicated: clumsiness, coordination difficulties, fine motor skills.
2.5 Expressing one's own emotions and understanding the emotions of others is often difficult, which in some cases is associated with alexithymia.
2.6 Selective dumbness (mutism): speech disappears under the influence of adverse external factors, due to stress, overload, anxiety.
2.7 Monologue in communications: tendency to present the topic without taking into account the reaction of others, ignoring remarks from outside, lack of pauses for feedback.
2.8 Sustained interest in a topic that is obsessive in nature: Fixation on a topic without considering its usefulness can last from several weeks to several years.
2.9 Behavioral rigidity: adherence to routine, schedule, routine, stress if necessary to change them.
2.10 Literal understanding: poor understanding of figurativeness and metaphors, allusions and jokes, rare use in one's own speech.
2.11 Focus on details: reasoning is deductive (from particular to general), induction is rarely used (from general to particular), understanding of the big picture is difficult, difficulty in distinguishing between the main and the secondary.
2.12 The executive function can be impaired: difficulties with setting priorities, organizing time.
2.13 "Model of the mental", empathy: the ability to "imagine yourself in the place of another person" is impaired, empathy is understood logically, non-verbal signals from interlocutors are perceived poorly and often erroneously.
2.14 Systematization, classification and logical approach to creating connections: rejection of illogical norms and traditions of society, conversations "about nothing", forms of greeting and farewell, stereotypes.
2.15 Processing of sensory information is disturbed: hypo- or hypersensitivity in all sense organs (sounds, light, textures and consistencies, temperature).
2.16 Stereotypical movements (stimming) as a reaction to overload and overfatigue: walking back and forth, rocking the body, shaking fingers, legs.
3. Sources of confirmation of the presence of Asperger's syndrome
3.1 Maintaining a list of symptoms, distinguishing from manifestations of OCD, ADHD, depression, anxiety disorder.
3.2 Self diagnostic tests: AQ, RAADS_R, EQ, TAS, ASSQ.
3.3 Diagnostic criteria for Asperger's syndrome and ASD according to DSM-IV, DSM-V, ICD-10.
3.4 Communities of people with Asperger's syndrome and ASD on the Internet: forums, groups, websites, personal blogs, self-diagnosis stories.
3.5 Meeting with people with Asperger's and ASD in a support group to compare appearances and discuss in person the possibility of having AS.
3.6 First person books in Russian:
- Stephen Shore "Behind the Wall"
- John Elder Robison "Look me in the eyes!"
- Temple Grandin "Opening the Doors of Hope"
- Rudy Simon "Aspie Girls"
- Mark Segar "Coping: A Survival Guide for People with Asperger's Syndrome"
- Robin Steward "Independence and Security: A Guide for Women with Autism Spectrum Disorders."
3.7 Private consultation with a psychologist, psychotherapist, psychiatrist (not recommended without prior feedback from other people with AS). It is desirable that specialists use the ADOS method (module 4 for adults with fluent speech and intact intelligence) for diagnosis.
4. Living with Asperger's Syndrome
4.1 Organize your life according to your strengths and weaknesses: keeping a schedule, looking for a job with minimal social activity, communicating in an appropriate way (letters instead of phone).
4.2 Specialist sessions if needed for cognitive behavioral therapy or treatment for depression, anxiety.
4.3 Visiting a support group for people with Asperger's to discuss problems and share experiences.
4.4 Familiarization of family, friends, colleagues (if possible) with the symptoms of Asperger's syndrome.
Asperger's syndrome: about self-diagnosis | Autistic City
Annotation
The article discusses the key issues related to the correct self-diagnosis of autism spectrum disorders, in particular Asperger's syndrome: the correct use of screening tests, the interpretation of existing diagnoses, the identification of key symptoms of autism spectrum disorder in adulthood, and the how not to confuse autistic disorders with other mental disorders. The material may be useful in the absence of official diagnostic facilities, as well as for reading before contacting a psychotherapist or going to a support group for people with Asperger's syndrome and autism spectrum disorders (ASD).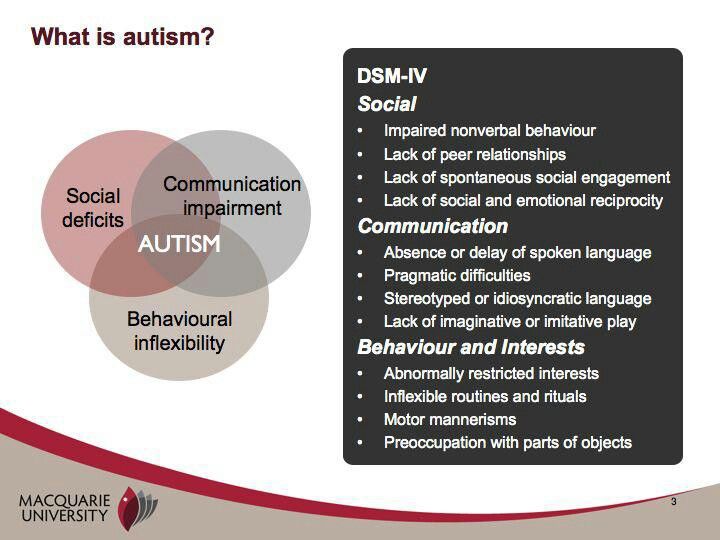
Contents
Introduction
Analysis of current diagnoses
Screening tests and their interpretation
What to look for?
What can be mistaken for Asperger's Syndrome and Autism Spectrum Disorders?
Conclusion
Introduction
The idea of writing an article about self-diagnosis of Asperger's syndrome (AS) came to us, the leaders of the Moscow support group for people with autism spectrum disorders (ASD), in the course of conversations with potential members of the group and new users of the aspergers forum. ru. It turned out that due to the inaccessibility of official diagnostics of AS in adults in Russia, combined with the ignorance of many people about the symptoms of ASD, we were faced with the need to answer a number of fairly similar and repetitive questions. At the same time, the FAQ format would not allow reflecting many important things, and therefore it was decided to write a full-fledged article devoted to tips for correct self-diagnosis of ASD in adults.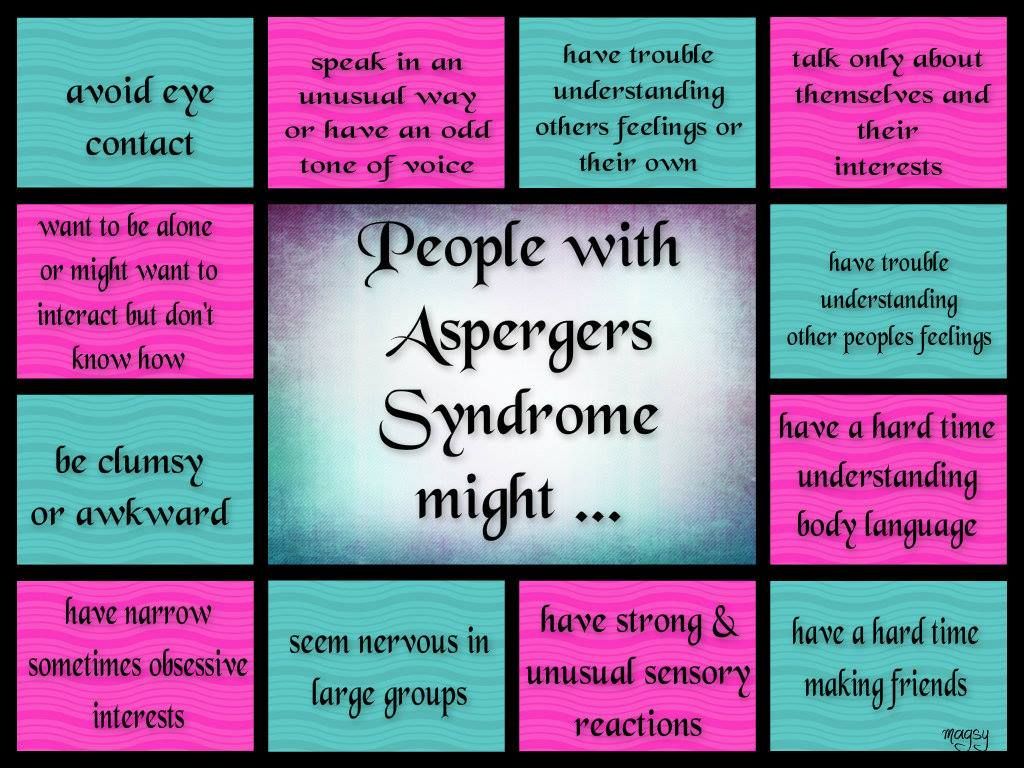
- greatly facilitate the search for a psychotherapist who specializes specifically in your problem
- promote a better understanding of oneself and accelerate the solution of a number of problems (communicative, sensory, etc.)
Attention! This article is not scientific, and the information in it cannot be considered medical advice and does not replace the advice of a specialist!
Analysis of existing diagnoses
Although the vast majority of people born in the USSR could not be diagnosed with Asperger's syndrome, it may make sense to find out if you were the object of attention of a psychiatrist, neuropathologist or speech therapist as a child.
If it turned out that yes, then pay attention to the following:
- Asperger's Syndrome is a type of autism.
- The diagnoses of autistic personality traits, autism traits, autistic-like behavior, autistic psychopathy, childhood schizoid disorder roughly correspond to Asperger's syndrome.

- Medical records for:
- violent reaction to loud, harsh, "metallic" sounds
- inadequate responses to physician questions, in particular, repeating the question instead of answering (i.e. echolalia)
- compulsive movements (sometimes they can be reflected as tics or increased motor excitability)
- obsessive interests
- increased nervous excitability, neurotic reactions, etc.
may indirectly indicate the presence of ASD.
Taking screening tests and interpreting them
Taking screening tests for autistic traits is an important part of self-diagnosis, as allows you to more objectively (compared to a simple self-comparison with the ICD-10 criteria) to assess their presence or absence. The experience of communicating in a face-to-face support group and aspergers.ru forums allows us to conditionally divide them into several groups:
1. Tests for autistic traits
This group includes tests
AQ, Aspie Quiz, RAADS-R; they are intended to provide a preliminary assessment of the presence of autistic traits and their severity.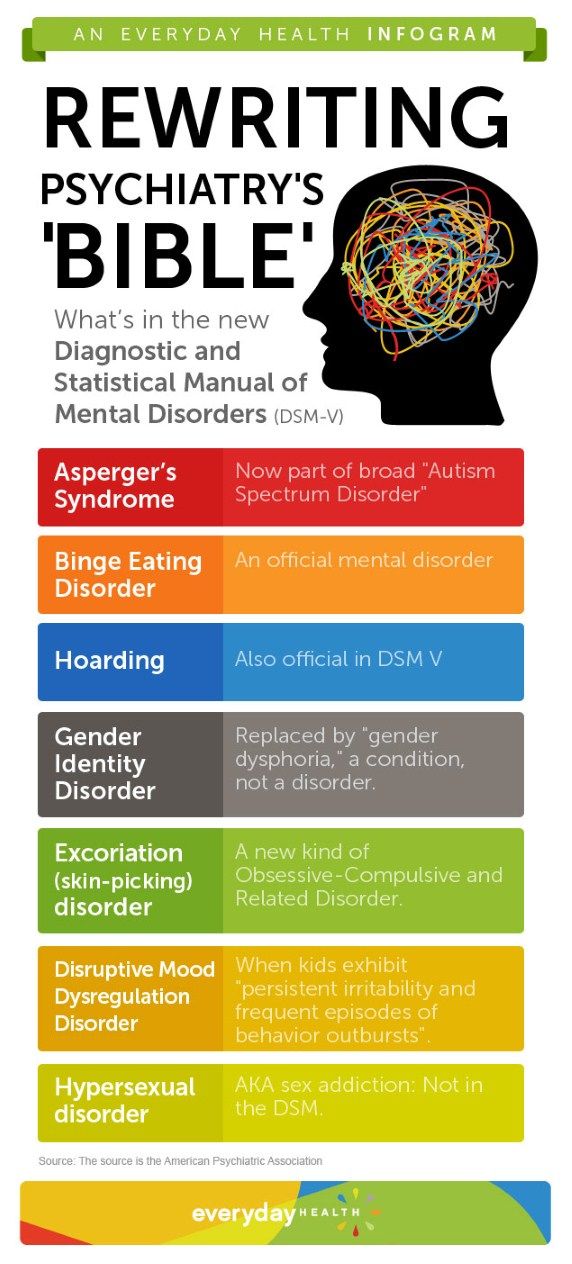 The practice of maintaining a support group has shown that the AQ test is the most preferable, because:
The practice of maintaining a support group has shown that the AQ test is the most preferable, because:
- the shortest and simplest of them all
- was originally designed for self-use as a screening test
- published in a peer-reviewed journal and statistically validated for sensitivity and selectivity
The Aspie Quiz is similar in many ways to the AQ, but contains three times as many questions and is comparable in sensitivity and selectivity (The AQ test vs Aspie Quiz).
The RAADS-R is intended for clinical use and may inflate results when used alone ( Ritvo R.A., Ritvo E.R., et al. // J. Autism Dev. Disorders. 2011 V.41. N.8. P.1076-1089).
Elevated (>=26) and especially high (>=32) AQ scores indicate the presence of pronounced autistic features, but do not speak about their nature (i.e. whether they are due to ASD), and in the case of ASD, as a rule, do not reflect the degree of its severity or lightness.
2.
 Tests for alexithymia
Tests for alexithymia This group of tests includes the Toronto Alexithymia Scale (TAS), which exists in two versions for 20 and 26 questions.
The newer and shorter TAS-20 of 20 questions should be used whenever possible.
Alexithymia (difficulty identifying and verbally describing one's emotions) occurs in 85% of people with autistic disorders (Berthoz S., Hill E.L. // European Psychiatry. 2005. V. 20, P. 291-298., Hill E., Berthoz S., Frith U. // J. Aut. Dev. Disorders. 2004. V.34(2), pp. 229-235.)
Asperger's syndrome is characterized by an elevated or high TAS score. If the result indicates the absence of alexithymia, then with a high probability you are not faced with ASD, but with something else.
3. SPQ test (for schizotypal traits) the symptoms of Asperger's syndrome and schizotypal disorder
(in the CIS - sluggish schizophrenia) may be outwardly similar, although these are different and mutually exclusive diagnoses that require a different approach and therapy.
 If the SPQ result is elevated, then the probability of schizotypal disorder is 55%. If you have an elevated SPQ but still think you have Asperger's Syndrome, consider the following:
If the SPQ result is elevated, then the probability of schizotypal disorder is 55%. If you have an elevated SPQ but still think you have Asperger's Syndrome, consider the following: - AS is not characterized by psychotic symptoms: hallucinations, delusions, "voices in the head", etc.
- for SA, high scores on the subscales "unusual perceptual experiences", "strange beliefs or magical thinking", "ideas of attitude", "suspiciousness" are not typical.
- SA is not characterized by a developed metaphorical thinking, a tendency to search for hidden meanings, "metaphysical intoxication", etc.
If you suspect that you have a schizotypal disorder, see a psychiatrist. its self-diagnosis and even more self-treatment are unacceptable.
4. Video Test Heider-Simmel Demonstration (HS1944)
This test is a video test.
Attention! If you have not watched it yet, then do not read further, but watch it and write down your impressions before reading the article further!
The HS1944 test is based on the fact that almost all neurotypical people, when watching a video, see characters playing a scene in geometric shapes (for example, a family scandal, a fight between guys over a girl, etc.). There are two extreme interpretations of the video:
- perception of the video as a purely mechanical movement of figures, the complete absence of their spontaneous "humanization". This interpretation indicates a high probability of having ASD.
- vision from the first seconds of the video of a complex social situation with a detailed description of the emotional states of
and the characters' personalities. This interpretation indicates a high probability of the absence of ASD (i.e., neurotypicality)
Many people (both neurotypical and autistic) can give answers that fall somewhere between the two extremes mentioned above. At the same time, autistic people will, as a rule, gravitate towards the first option, and neurotypical people - to the second.
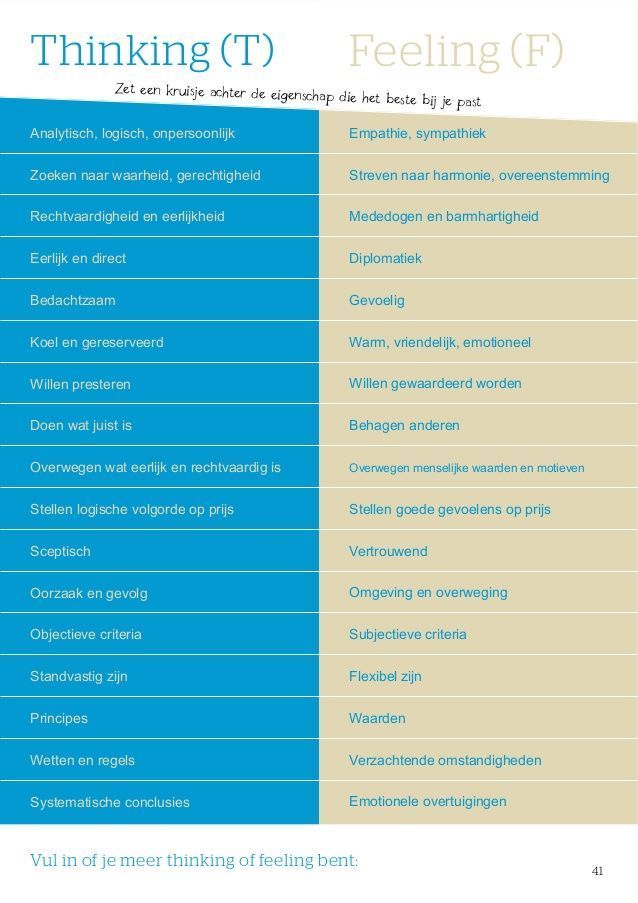
5. Cognitive Tests
Cognitive Tests include the EQ and SQ tests that measure empathy and systematization abilities, respectively. Asperger's syndrome is characterized by low total EQ scores (about 20 points, while for neurotypical people the average result is about 40 points) and a slightly increased SQ result. More information can be found on the pages with online versions of tests (see above). The most essential of these for self-diagnosis is the EQ test.
6. Childhood Behavior Tests
When self-diagnosing Asperger's syndrome, you need to pay attention to how you behaved in childhood: many of its symptoms are especially pronounced and specific in preschool and primary school age, which makes it possible to distinguish it from a number of others problems (primarily social phobia, personality traits and schizophrenia spectrum disorders).
The ASSQ and the Childhood Autism Rating Scale can be used to assess the severity of autistic traits in childhood. The advantages of the ASSQ are its simplicity and brevity, validation on real samples of children, and publication in a peer-reviewed journal. The strength of the Childhood Autism Rating Scale is its detailed description of the different levels of ASD symptoms in childhood, which can be useful in self-diagnosis.
The advantages of the ASSQ are its simplicity and brevity, validation on real samples of children, and publication in a peer-reviewed journal. The strength of the Childhood Autism Rating Scale is its detailed description of the different levels of ASD symptoms in childhood, which can be useful in self-diagnosis.
These tests should be filled out based on the memory of your behavior in primary school age (7-10 years). It is strongly recommended that one of your parents (or another person who remembers your childhood behavior well) fill them out and take the results into account in self-diagnosis.
It is highly recommended that you combine these tests with a conversation with a parent about your childhood behavior and its similarities to Asperger's. "Outside view" makes self-diagnosis more objective. If the parent does not know what Asperger's syndrome is, then you can give him (her) articles to read:
"What is Asperger's syndrome?",
"Diagnostic criteria for Asperger's syndrome",
"Children with Asperger's syndrome. What is Asperger's syndrome?",
What is Asperger's syndrome?",
"Answers to some frequently asked questions about ASD".
Summary
AQ, TAS, SPQ and HS1944 tests are required for good self-diagnosis. It is also desirable to pass the EQ test and one of the tests for behavioral characteristics in childhood ("childhood autism rating scale" or ASSQ test).
ASD characteristic results:
- AQ - high or high
- TAS-20 - high or high
- SPQ - normal
- HS1944 - reduced tendency to anthropomorphize
- EQ - low
- ASSQ test and Childhood Autism Rating Scale - High
What to look out for?
So, you have passed the screening tests and they came back positive. It is even possible that your parents filled out the Childhood Autism Rating Scale and the ASSQ test, and also recognized the similarity of your childhood behavior with the criteria for Asperger's syndrome, and some indirect evidence of the presence of ASD remained in the medical records. What should you pay attention to now When trying to understand the origin of your autistic traits?Next, we will look at several groups of symptoms that are characteristic of Asperger's syndrome in adulthood.0005
What should you pay attention to now When trying to understand the origin of your autistic traits?Next, we will look at several groups of symptoms that are characteristic of Asperger's syndrome in adulthood.0005
1. Congenitality of Asperger's Syndrome
In the case of ASD, symptoms appear at 2-3 years of age and are evident by 6-7 years of age.
They do not disappear with age, but their severity often gradually decreases.
2. Specific problems with communication from early childhood:
The main problems in communication with Asperger's syndrome are not shyness or isolation, but difficulties with an intuitive and quick understanding of other people's emotions, states, unwritten rules of behavior in social situations.
Typical examples of such difficulties in adulthood:
- intuitive understanding of the look and facial expressions of only basic and fairly pronounced emotions such as joy, fear or anger. Problems with "reading" weak and complex emotions: for example, it can be difficult to tell if a person is calm, tired, upset, annoyed, or resentful.

- using "eye contact" more as a habit to keep up with the rules of decency than to better understand the interlocutor; on the contrary, for an autistic person, the need to make eye contact can distract from the perception of speech and interfere with understanding the subject of conversation
- Orientation in social situations rather due to life experience and memorization of ready-made and detailed patterns of behavior. Anxiety in situations where already existing experience is unacceptable and intuition is needed.
- weak "infection" with other people's emotions and reduced spontaneous sensitivity to someone else's physical pain
- alexithymia and problems regulating one's own emotional state (for example, a tendency to increase anxiety and / or outbursts of poorly controlled rage (called "meltdowns").
- propensity for remarks "perceived by others as excessive straightforwardness, categoricalness, rudeness or rudeness, and not because of any conscious motives, but because of a lack of understanding of the intricacies of human relationships and informal hierarchy
3.
 Sensory Difficulties
Sensory Difficulties In Asperger's syndrome, it is very common to find hypersensitivity to any sensory stimuli: sounds, touch, light. Examples:
- sounds: sharp, high-pitched, "metallic", as well as noise of a complex nature in shopping centers, noisy companies, echoing audiences, etc. Often leads to the inability to make out someone else's speech even against the background of fairly quiet noises, in some cases - to disorientation, fragmentation of perception, derealization, lightheadedness and even fainting.
- visual stimuli: flickering of fluorescent lights, old monitors, a large number of objects in the field of view, especially moving and / or flickering.
- tactile stimuli: hypersensitivity to touch, very unpleasant sensations from certain fabrics (e.g. coarse wool), clothing tags, certain foods due to their texture
- increased or decreased sensitivity to pain. Unusual perception of certain types of pain
As part of the self-diagnosis, it is recommended to watch the following videos, which show extreme sensory overload (i.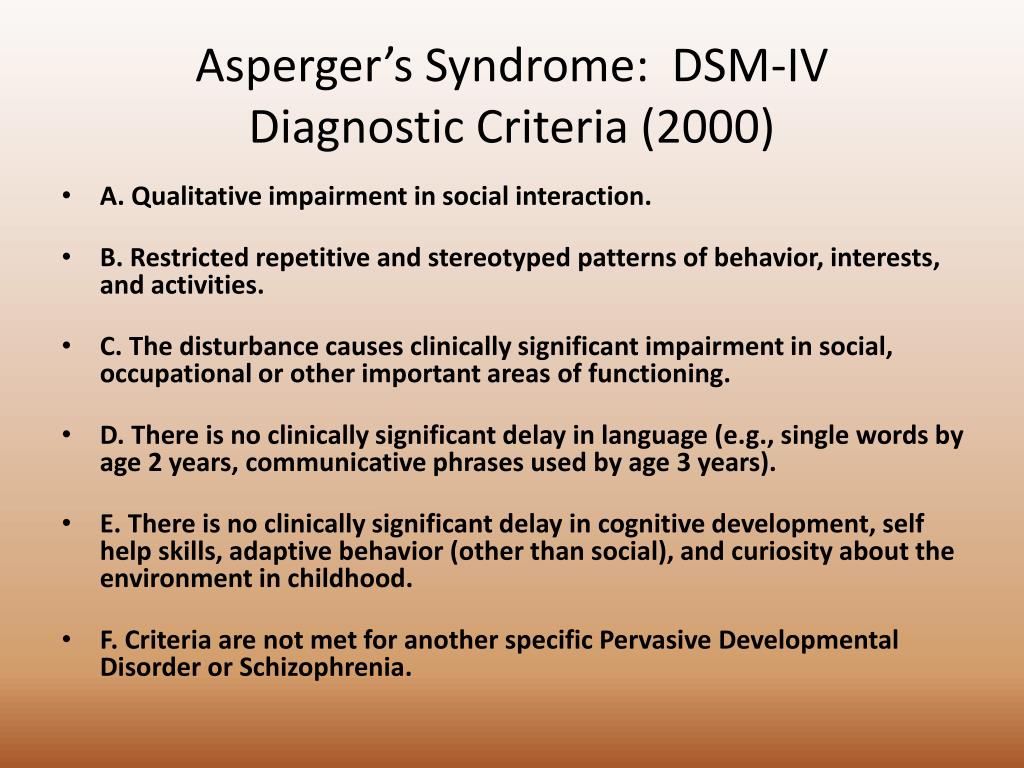 e. attempts to recreate the sensations of an autistic person).
e. attempts to recreate the sensations of an autistic person).
Remember that a person may not always be aware of the presence of sensory overload and "write off" their manifestations as lightheadedness, fatigue, anxiety, vegetative-vascular dystonia, etc. But at the same time, sensory overload should not be confused with panic attacks.
4. Special interests
Obsessive interests are a very common manifestation of ASD. They are distinguished from ordinary hobbies by obsession (somewhat reminiscent of falling in love), a natural tendency to reduce the conversation to them, often a narrow focus, unusualness, and lack of applied significance. Special interests are especially pronounced in childhood, as they grow older they can become more abstract and practical, and resemble a hobby and / or passion for a profession.
5. Stimming, i.e. motor stereotypes, compulsive movements
Stereotypes often persist into adulthood. Often they are repetitive movements of the hands, swinging, swinging the leg, etc. They are distinguished from similar movements of neurotypical people b o by a greater degree of obsession, often by their unconsciousness.
They are distinguished from similar movements of neurotypical people b o by a greater degree of obsession, often by their unconsciousness.
6. Clumsiness (problems with coordination of movements)
Motor clumsiness is a common but not mandatory manifestation of Asperger's syndrome.
Usually present in early childhood and may cause problems with learning to write, use cutlery, tie shoelaces, button up buttons, thread a needle, ride a bicycle, rollerblade, run, exercise, dance, etc.
7. Poor and/or peculiar facial expressions, as well as prosody (intonation) of speech, as well as "body language" in general
From the outside, non-verbal communication of an autistic person may give the impression of "eccentricity" and/or detachment.
Intonation may be perceived by others as "robot-like" or "chanting". The severity of this symptom varies greatly from person to person. Also, without experience of communicating with obviously autistic people, it can be difficult to assess what specific features of non-verbal communication are being discussed.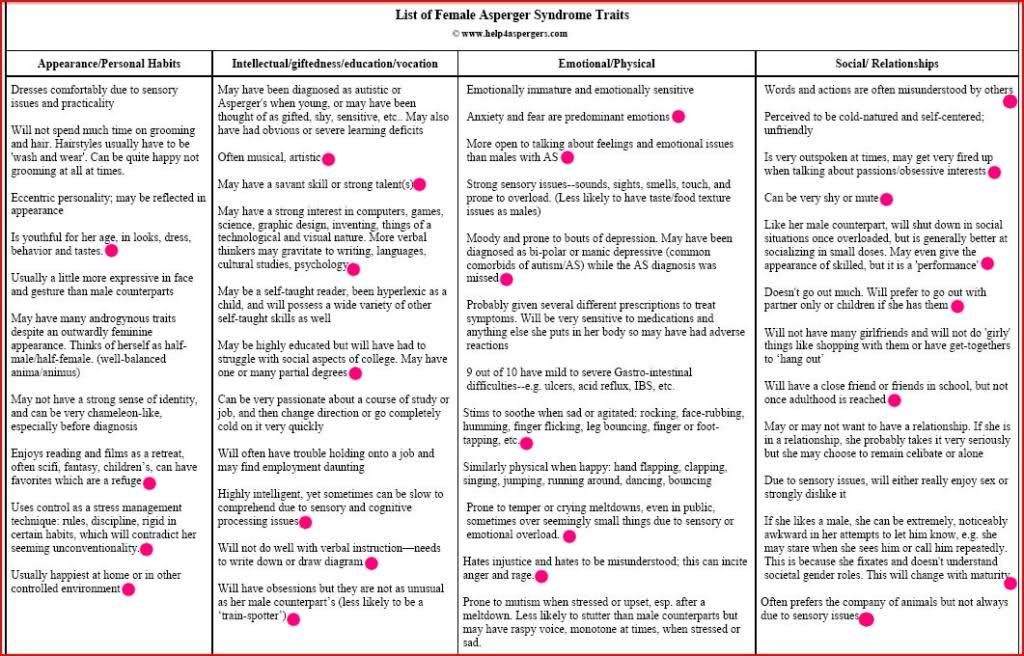
What can be mistaken for Asperger's syndrome and autism spectrum disorders?
When self-diagnosing autism spectrum disorders, their external similarity with other mental and neurological disorders and / or character traits presents some problem, especially for a person who has little studied their symptoms and has no experience of communicating with autistic people "in real life". Next, we will consider some of the features of the psyche that are most often mistaken for ASD.
1. Social phobia
Social phobia is a strong and poorly controlled fear of any specific social situations (public speaking, romantic acquaintances, talking with a sales assistant in a store, etc.) or a fear of communication in general. Often, its appearance is associated with some past negative communication experience and / or fear of making a negative impression on others. May lead (not always) to higher scores on the AQ test and sometimes - TAS.
Social phobia is often found among autistic people, but in itself is not autism, because.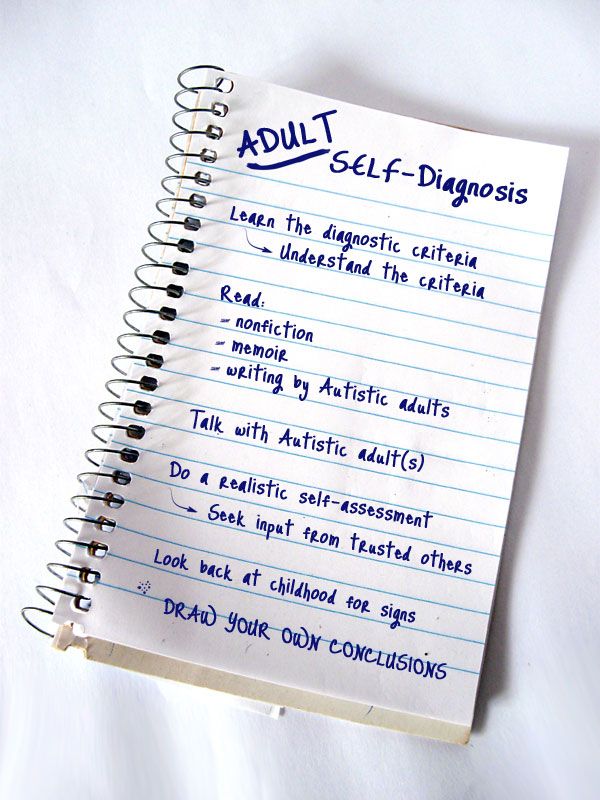 its symptoms do not include violations of empathy and social intelligence, sensory overload, special interests, a tendency to routine, features of facial expressions and prosody characteristic of ASD, etc.
its symptoms do not include violations of empathy and social intelligence, sensory overload, special interests, a tendency to routine, features of facial expressions and prosody characteristic of ASD, etc.
2. Introversion, schizoid character accentuation, schizoid personality disorder
Variants of normal character or personality disorders are often confused with ASD, which are manifested by isolation, desire to stay in one's inner world, selectivity in communication, heightened perception of violation of personal boundaries, etc. . At first glance, a deep introvert looks very similar to an autistic person (and even screening testing can give a false positive result), but in fact there are several important differences:
- ASD manifests itself from the age of 2-3 and is very noticeable by the time of entering school, while the character is formed rather in adolescence
- Social intelligence and empathy with ordinary introversion or schizoidness are usually normal, although communication skills may be poorly developed due to little communication experience
- introversion and schizoidness are not characterized by stimming (stereotypical movements), sensory overload, special interests
- introversion - a tendency to withdraw regardless of communication skills, Asperger's syndrome - serious problems with an intuitive understanding of other people, regardless of the desire to communicate (moreover, an autistic person can be an extrovert)
- Asperger's syndrome is not characterized by a tendency to strongly metaphorical thinking, complex allegories, "metaphysical intoxication", etc.

Although many autistic people are introverts, some of them are extroverts (the so-called Gillberg active group).
For more on the difference between autism and introversion/schizoidness, see note
by Daniela Tate: "Differential Diagnosis: Schizoid Personality Disorder vs. Autism").
3. Secondary autism
The causes of secondary autism are not autism spectrum disorder, but adverse conditions in childhood:
- lifestyle of the family, exclusively home-based education of the child),
- psychological traumas (domestic violence, upbringing in an orphanage, death of loved ones, bullying by peers, etc.).
Sometimes it can also appear due to transsexuality or homosexuality due to the need to hide one's true nature in a society that is not very tolerant of such mental characteristics.
Outwardly, secondary autism may look similar to Asperger's syndrome due to low communication skills, isolation, alexithymia, distrust.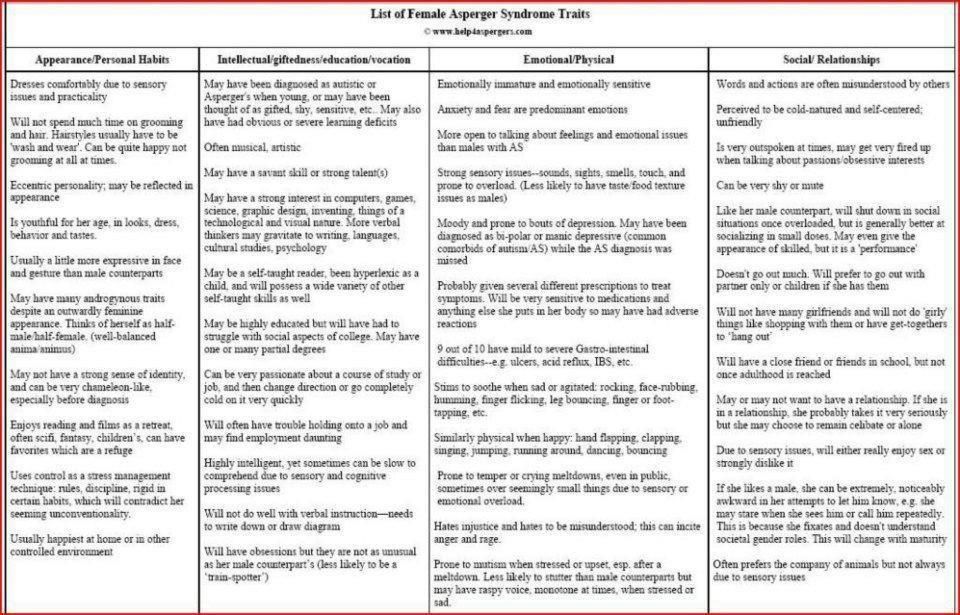 But, as with introversion, it will not have such obvious violations of empathy, "mental model", social intelligence, as in Asperger's syndrome, and a set of symptoms specific to autistic disorders such as sensory overload, stimming, special interests, adherence to routine and rituals.
But, as with introversion, it will not have such obvious violations of empathy, "mental model", social intelligence, as in Asperger's syndrome, and a set of symptoms specific to autistic disorders such as sensory overload, stimming, special interests, adherence to routine and rituals.
4. Schizotypal disorder and schizophrenia
Although this group of disorders is characterized by withdrawal, it has little in common with Asperger's syndrome. On screening testing, they may show high scores on AQ and TAS tests, as well as SPQ. Important differences:
- Asperger's syndrome always begins in early childhood, while schizophrenia usually begins in adolescence or early adulthood
- Asperger's syndrome is not characterized by psychotic symptoms (hallucinations, delusions, "voices"), as well as negative symptoms (disordered thinking, etc.)
- SA does not progress, but it is not treatable with psychotropic drugs and does not experience exacerbations and remissions
- about schizotypal disorder - see above for more details on the SPQ test.

Attention! If you suspect schizophrenia or schizotypal disorder, you need to contact a psychotherapist! Self-diagnosis and even more self-treatment are unacceptable: dangerous!
5. Other mental disorders
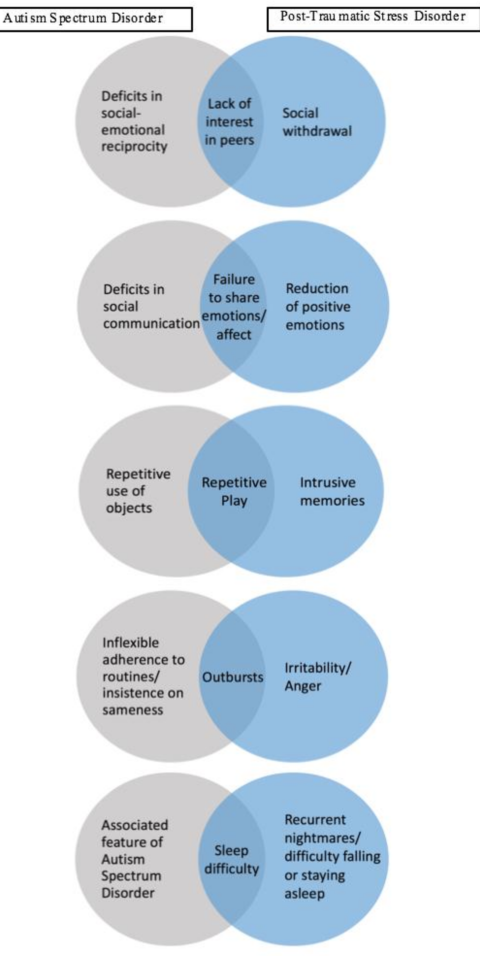
Generalized anxiety disorder, obsessive-compulsive disorder, post-traumatic stress disorder, bipolar affective disorder, depression, etc. are sometimes confused with ASD. It should be remembered that
- none of these disorders gives the whole set of symptoms of ASD, and their picture as a whole is significantly different
- as a rule, they do not begin in early childhood
- any of them can be in both a neurotypical and autistic person
6. Extended autism phenotype (XPA)
XPA is a variant of the normal psyche, qualitatively very similar to Asperger's syndrome, but in terms of the severity of the problems, it does not "reach" a psychiatric or neurological diagnosis. In adulthood, XRF can be difficult to distinguish from mild SA variants, even for specialists.