Antidepressant with the least amount of side effects
Overview - SSRI antidepressants - NHS
Selective serotonin reuptake inhibitors (SSRIs) are a widely used type of antidepressant.
They're mainly prescribed to treat depression, particularly persistent or severe cases, and are often used in combination with a talking therapy such as cognitive behavioural therapy (CBT).
SSRIs are usually the first choice medicine for depression because they generally have fewer side effects than most other types of antidepressant.
As well as depression, SSRIs can be used to treat a number of other mental health conditions, including:
- generalised anxiety disorder (GAD)
- obsessive compulsive disorder (OCD)
- panic disorder
- severe phobias, such as agoraphobia and social phobia
- bulimia
- post-traumatic stress disorder (PTSD)
SSRIs can sometimes be used to treat other conditions, such as premenstrual syndrome (PMS), fibromyalgia and irritable bowel syndrome (IBS). Occasionally, they may also be prescribed to treat pain.
How SSRIs work
It's thought that SSRIs work by increasing serotonin levels in the brain.
Serotonin is a neurotransmitter (a messenger chemical that carries signals between nerve cells in the brain). It's thought to have a good influence on mood, emotion and sleep.
After carrying a message, serotonin is usually reabsorbed by the nerve cells (known as "reuptake"). SSRIs work by blocking ("inhibiting") reuptake, meaning more serotonin is available to pass further messages between nearby nerve cells.
It would be too simplistic to say that depression and related mental health conditions are caused by low serotonin levels, but a rise in serotonin levels can improve symptoms and make people more responsive to other types of treatment, such as CBT.
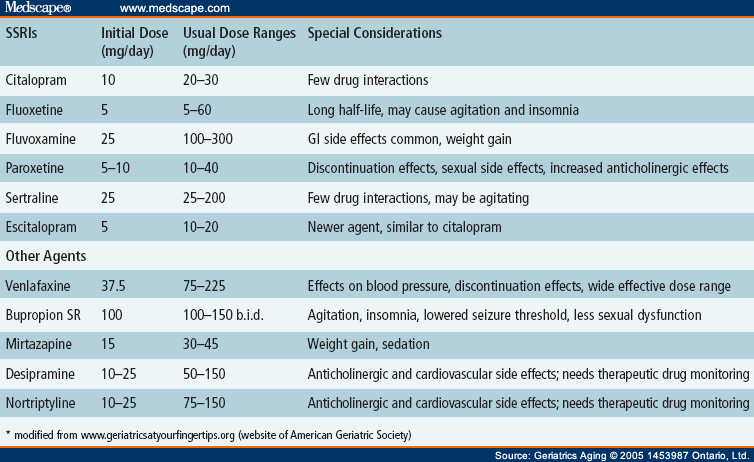
Doses and duration of treatment
SSRIs are usually taken in tablet form.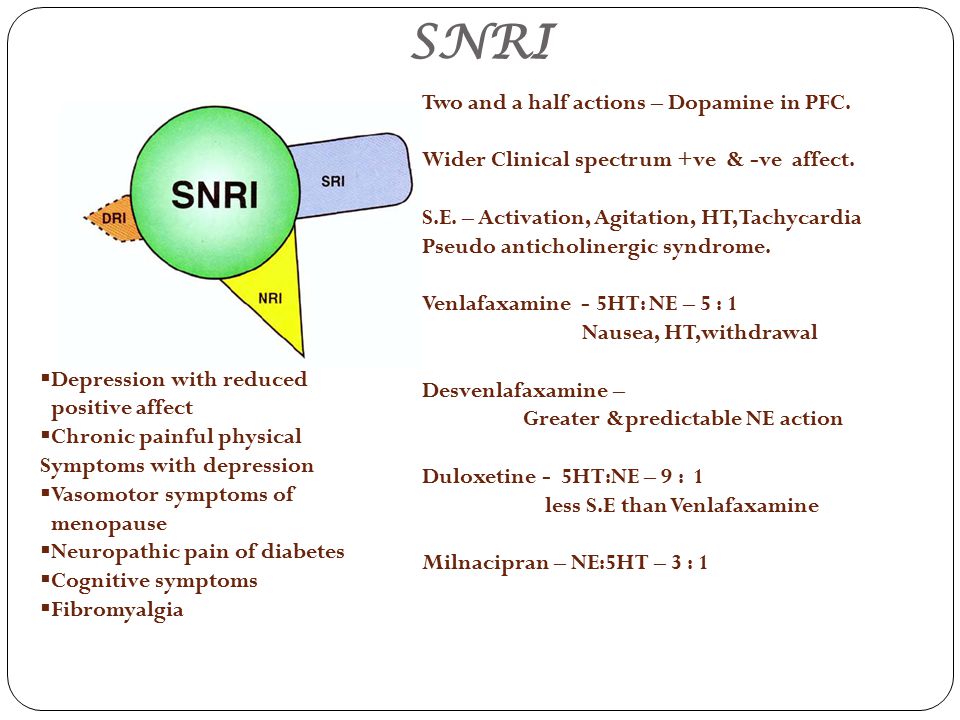 When they're prescribed, you'll start on the lowest possible dose thought necessary to improve your symptoms.
When they're prescribed, you'll start on the lowest possible dose thought necessary to improve your symptoms.
SSRIs usually need to be taken for 2 to 4 weeks before the benefit is felt. You may experience mild side effects early on, but it's important that you don't stop taking the medicine. These effects will usually wear off quickly.
If you take an SSRI for 4 to 6 weeks without feeling any benefit, speak to your GP or mental health specialist. They may recommend increasing your dose or trying an alternative antidepressant.
A course of treatment usually continues for at least 6 months after you feel better, although longer courses are sometimes recommended and some people with recurrent problems may be advised to take them indefinitely.
Things to consider
SSRIs aren't suitable for everyone. They're not usually recommended if you're pregnant, breastfeeding or under 18, because there's an increased risk of serious side effects. However, exceptions can be made if the benefits of treatment are thought to outweigh the risks.
However, exceptions can be made if the benefits of treatment are thought to outweigh the risks.
SSRIs also need to be used with caution if you have certain underlying health problems, including diabetes, epilepsy and kidney disease.
Some SSRIs can react unpredictably with other medicines, including some over-the-counter painkillers and herbal remedies, such as St John's wort. Always read the information leaflet that comes with your SSRI medicine to check if there are any medicines you need to avoid.
Side effects
Most people will only experience a few mild side effects when taking SSRIs. These can be troublesome at first, but they'll generally improve with time.
Common side effects of SSRIs can include:
- feeling agitated, shaky or anxious
- diarrhoea and feeling or being sick
- dizziness
- blurred vision
- loss of libido (reduced sex drive)
- difficulty achieving orgasm during sex or masturbation
- in men, difficulty obtaining or maintaining an erection (erectile dysfunction)
You'll usually need to see your doctor every few weeks when you first start taking SSRIs to discuss how well the medicine is working. You can also contact your doctor at any point if you experience any troublesome or persistent side effects.
You can also contact your doctor at any point if you experience any troublesome or persistent side effects.
Types of SSRIs
There are currently 8 SSRIs prescribed in the UK:
- citalopram (Cipramil)
- dapoxetine (Priligy)
- escitalopram (Cipralex)
- fluoxetine (Prozac or Oxactin)
- fluvoxamine (Faverin)
- paroxetine (Seroxat)
- sertraline (Lustral)
- vortioxetine (Brintellix)
Page last reviewed: 8 December 2021
Next review due: 8 December 2024
Types, Comparison Chart, and Suicide Risk
Antidepressant medications are a first-choice option for treating major depressive disorder (MDD), according to guidelines from the American Psychiatric Association. They can also help to treat anxiety conditions, including generalized anxiety disorder.
They can also help to treat anxiety conditions, including generalized anxiety disorder.
There are different types of antidepressants, based on how they work within the brain. Some are better for treating certain conditions and symptoms. But they all come with potential side effects.
Generally, each type causes somewhat different side effects, but there can still be some variance within a single type.
People can also respond differently to antidepressants. Some people may have no troubling side effects, while others may have one or more serious side effects. This is why you may need to try a few different medications before you find the right fit.
Here’s a look at the main types of antidepressants and some of the side effects commonly associated with them. If you take a certain type, you probably won’t experience all of the side effects associated with it. You might also experience other side effects, including some serious ones, that aren’t listed here.
SSRIs affect serotonin, which is a neurotransmitter that plays a role in many things, including your mood. Neurotransmitters act as chemical messengers within your body.
Neurotransmitters act as chemical messengers within your body.
When your brain releases serotonin, some of it is used to communicate with other cells, and some of it goes back into the cell that released it. SSRIs decrease the amount of serotonin that goes back into the cell that released it, leaving more available in your brain to communicate with other cells.
Experts aren’t completely sure about the role serotonin plays in depression. But many believe that low levels of serotonin are a contributing factor.
SSRI antidepressants include:
- citalopram (Celexa)
- escitalopram (Lexapro)
- paroxetine (Brisdelle, Paxil, Pexeva)
- fluoxetine (Prozac)
- fluvoxamine
- sertraline (Zoloft)
SSRIs are the most common choice for treating MDD, but they can also help with:
- generalized anxiety disorder
- panic disorder
- social anxiety disorder
- premenstrual dysphoric disorder
- post-traumatic stress disorder
- obsessive-compulsive personality disorder
- hot flashes
Common side effects
The more common side effects of SSRIs include:
- headaches
- nausea
- trouble sleeping
- dizziness
- diarrhea
- weakness and fatigue
- anxiety
- stomach upset
- dry mouth
- sexual problems such as low sex drive, erectile dysfunction, or ejaculation problems
SSRIs are more likely than some antidepressants to cause sexual side effects. They can also increase appetite, potentially leading to weight gain.
They can also increase appetite, potentially leading to weight gain.
Like SSRIs, SNRIs are often used to treat MDD. Similar to SSRIs, SNRIs prevent cells in your brain from reabsorbing certain neurotransmitters. This leaves more of them available to communicate with other cells.
In the case of SNRIs, the neurotransmitters affected are serotonin and norepinephrine.
SNRI antidepressants include:
- desvenlafaxine (Khedezla, Pristiq)
- duloxetine (Cymbalta)
- levomilnacipran (Fetzima)
- milnacipran (Savella)
- venlafaxine (Effexor XR)
SNRIs are often used to treat depression, but they can also help with:
- nerve damage caused by diabetes
- fibromyalgia
- generalized anxiety disorder
- hot flashes
Common side effects
The more common side effects of SNRIs include:
- headaches
- nausea
- insomnia
- drowsiness
- dry mouth
- dizziness
- loss of appetite
- constipation
- sexual problems such as low sex drive, erectile dysfunction, or ejaculation problems
- weakness and fatigue
- sweating
SNRIs can cause sexual side effects, but not as often as SSRIs. Some people who take SNRIs may also gain weight, but weight loss is more common.
Some people who take SNRIs may also gain weight, but weight loss is more common.
In some cases, people taking SNRIs may notice increased blood pressure.
TCAs are an older group of antidepressants. Like SNRIs, they help to increase levels of norepinephrine and serotonin your brain. But they also decrease the effects of another neurotransmitter called acetylcholine.
This impact on acetylcholine increases the risk of certain side effects. As a result, TCAs are typically only used if SSRIs and SNRIs don’t work well for you.
Some common TCAs include:
- amitriptyline (Elavil)
- clomipramine (Anafranil)
- desipramine (Norpramin)
- doxepin
- imipramine (Tofranil)
- nortriptyline (Pamelor)
In addition to treating depression, many TCAs are used for other conditions, including:
- nerve pain caused by shingles
- nerve damage caused by diabetes
- social anxiety disorder
- fibromyalgia
- migraine headache
- bedwetting in children
Common side effects
The more common side effects of TCAs include:
- headaches
- dry mouth
- blurred vision
- digestive issues, such as stomach upset, nausea, and constipation
- dizziness
- drowsiness
- trouble sleeping
- memory problems
- fatigue
- weight gain
- sexual problems such as low sex drive, erectile dysfunction, or ejaculation problems
- trouble urinating
- fast heart rate
- sweating
The side effects of TCAs are similar to those of SSRIs and SNRIs, but they tend to occur more frequently and can be more bothersome.
TCAs are also much more likely to cause certain side effects, including:
- dry mouth
- blurred vision
- constipation
- trouble urinating
- weight gain
- drowsiness
In rare cases, TCAs can also cause potentially dangerous heart-related side effects, such as:
- low blood pressure when standing up
- high blood pressure
- abnormal heart rate or arrhythmia
Like TCAs, MAOIs are an older group of medications. Today, they’re not commonly used for depression, but your healthcare provider might suggest them if others aren’t offering relief.
MAOIs work by preventing your body from breaking down certain neurotransmitters. This causes an increase in your levels of serotonin, norepinephrine, and dopamine.
Some common MAOIs include:
- isocarboxazid (Marplan)
- phenelzine (Nardil)
- tranylcypromine (Parnate)
- selegiline (Eldepryl, Emsam)
In addition to depression, some MAOIs are used for other conditions. Phenelzine and tranylcypromine are sometimes used for panic disorder and social anxiety. Selegiline is used for Parkinson’s disease.
Phenelzine and tranylcypromine are sometimes used for panic disorder and social anxiety. Selegiline is used for Parkinson’s disease.
Common side effects
The more common side effects of MAOIs include:
- low blood pressure
- nausea
- headaches
- drowsiness
- dizziness
- dry mouth
- weight gain
- stomach pain
- confusion
- diarrhea
- runny nose
- sexual problems such as low sex drive, erectile dysfunction, or ejaculation problems
MAOIs are more likely to cause low blood pressure than other antidepressants. These medications can also interact with foods containing tyramine and cause dangerously high blood pressure.
SARIs are also known as serotonin modulators or phenylpiperazine antidepressants. They’re sometimes considered atypical antidepressants because they work differently. SARIs can help treat:
- depression
- anxiety
- panic disorder
Like most other antidepressants, SARIs help to increase the amount of available serotonin — and sometimes other neurotransmitters — in your brain. But they do so in different ways from other antidepressants.
But they do so in different ways from other antidepressants.
Some SARIs include:
- nefazodone
- trazodone (Oleptro)
Common side effects
The more common side effects of SARIs include:
- drowsiness
- dry mouth
- headaches
- dizziness
- nausea
- fatigue
- vomiting
- blurred vision
- diarrhea
- constipation
- low blood pressure
- confusion
Many people taking SARIs experience drowsiness or sleepiness. This makes them a potentially good option for people with insomnia, especially if they also have depression.
Some antidepressants simply don’t fit into any of the main group, usually because of the way they work. These are known as atypical antidepressants.
Bupropion (Wellbutrin)
Unlike most other antidepressants, bupropion doesn’t increase serotonin. Instead, it works to increase norepinephrine and dopamine. It’s sometimes classified as a norepinephrine-dopamine reuptake inhibitor.
In addition to being used for depression, bupropion is also used to help people quit smoking.
The more common side effects of bupropion include:
- trouble sleeping
- headaches
- irritability or agitation
- dry mouth
- constipation
- loss of appetite
- weight loss
- nausea
- vomiting
- sweating
- dizziness
- anxiety
Compared with other antidepressants, bupropion is less likely to cause weight gain. In fact, weight loss is a common side effect.
Bupropion is also less likely to cause sexual problems. As a result, it’s sometimes prescribed alongside other antidepressants to reduce their sexual side effects.
But it’s more likely than some other antidepressants to cause insomnia and anxiety. In rare cases, bupropion can cause seizures, especially when used in high doses.
Mirtazapine (Remeron)
Mirtazapine increases the effects of norepinephrine, serotonin, and dopamine in your brain in a different way than other antidepressants. It’s sometimes classified as a noradrenergic antagonist-specific serotonin antagonist.
It’s sometimes classified as a noradrenergic antagonist-specific serotonin antagonist.
The more common side effects of mirtazapine include:
- drowsiness
- dry mouth
- increased appetite
- weight gain
- high cholesterol
- constipation
- weakness and fatigue
- dizziness
Like SARIs, mirtazapine may cause sleepiness or drowsiness. As a result, mirtazapine may be used for those who have depression and trouble sleeping.
Mirtazapine can also cause increased appetite, making it more likely to cause weight gain than other antidepressants.
Vilazodone (Viibryd)
Vilazodone increases serotonin’s effects in the brain in ways both similar to and different from SSRIs. It’s sometimes called a serotonin partial agonist reuptake inhibitor.
The more common side effects of vilazodone include:
- diarrhea
- nausea
- dizziness
- dry mouth
- trouble sleeping
- vomiting
Vilazodone is less likely to cause weight gain than many other antidepressants, such as SSRIs and TCAs. Some people who take vilazodone have sexual problems, such as low sex drive or erectile dysfunction, but this seems to be less common with vilazodone compared to SSRIs and SNRIs.
Some people who take vilazodone have sexual problems, such as low sex drive or erectile dysfunction, but this seems to be less common with vilazodone compared to SSRIs and SNRIs.
Vortioxetine (Trintellix)
Vortioxetine is sometimes called a multimodal antidepressant. It functions somewhat like an SSRI, but has additional effects on serotonin levels.
The more common side effects of vortioxetine include:
- sexual problems, such as orgasm or ejaculation problems
- nausea
- diarrhea
- dizziness
- dry mouth
- constipation
- vomiting
Vortioxetine is more likely to cause sexual side effects than many other antidepressants. But it’s less likely to cause weight gain.
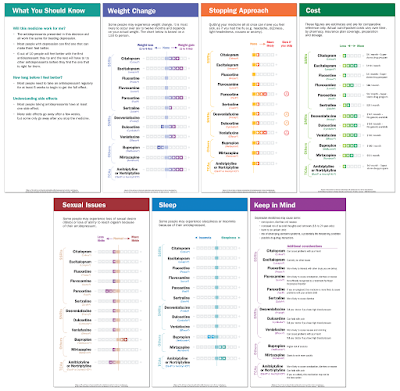
The chart below is a general comparison of the some of the more common side effects associated with different antidepressants.
When using this chart, keep a few things in mind:
- Everyone responds differently to antidepressants, so you may have additional side effects not listed here.
- You likely won’t experience every single side effect associated with a particular antidepressant.
- Some medications are more or less likely to cause certain side effects. Your healthcare provider can give you more information about common side effects linked to specific medications within each group.
- Some side effects may become milder or disappear completely over time as your body gets used to the medication.
- This chart only includes common side effects. Some antidepressants may have less common, more serious side effects, including increased suicidal thoughts.
| Side effect | SSRIs | SNRIs | TCAs | MAOIs | SARIs | bupropion | mirtazapine | vilazodone | vortioxetine |
| headache | X | X | X | X | X | X | |||
| diarrhea | X | X | X | X | X | X | |||
| dry mouth | X | X | X | X | X | X | X | X | X |
| fatigue | X | X | X | X | X | X | X | ||
| sweating | X | X | X | X | |||||
| dizziness | X | X | X | X | X | X | X | X | |
| blurred vision | X | X | X | ||||||
| sexual issues | X | X | X | X | X | X | |||
| drowsiness | X | X | X | X | X | X | X | ||
| insomnia | X | X | X | X | X | ||||
| weight gain | X | X | X | X | X | ||||
| weight loss | X | X | X |
Some antidepressants, including SSRIs, may cause an increase in suicidal thoughts or actions. This risk is higher in children, teenagers, and young adults. It’s also higher within the first few months of treatment or during dosage changes.
This risk is higher in children, teenagers, and young adults. It’s also higher within the first few months of treatment or during dosage changes.
You and your family members, caregivers, and healthcare provider should watch for any new or sudden changes in your mood, behaviors, thoughts, or feelings. Call your healthcare provider right away if you notice any changes.
Suicide prevention
If you think someone is at immediate risk of self-harm or hurting another person:
- Call 911 or your local emergency number.
- Stay with the person until help arrives.
- Remove any guns, knives, medications, or other things that may cause harm.
- Listen, but don’t judge, argue, threaten, or yell.
If you or someone you know is considering suicide, get help from a crisis or suicide prevention hotline. Try the National Suicide Prevention Lifeline at 800-273-8255.
There are many types of antidepressants. Each comes with its own list of potential side effects.![]() When choosing and trying an antidepressant, it’s important to work closely with your healthcare provider, especially as you get used to a medication’s side effects.
When choosing and trying an antidepressant, it’s important to work closely with your healthcare provider, especially as you get used to a medication’s side effects.
Before starting any new medication, let your healthcare provider know about any other medications you take, including over-the-counter drugs and herbal supplements, such as St. John’s wort. If you drink alcohol, make sure to also ask about any potential interactions it might have with your medication.
In addition to side effects, antidepressants can also cause allergic reactions in some people. Seek immediate medical treatment if you notice any symptoms of a severe allergic reaction, such as difficulty breathing or swelling in your face, tongue, or throat.
Selecting an antidepressant based on efficacy and tolerability
partners Keywords / keywords: Antidepressants, Velaxin, Venlafaxine, Categories of tolerability, Classification, Neuronal, Side effects, Neuropsychiatry, Toxic
Summary
The classification of side effects of antidepressants is presented. Side effects can be toxic or neuronal. Neuronal side effects are divided into "extra-therapeutic" (persistent or reversible), as well as "paratherapeutic". Seven categories of antidepressant tolerance have been identified. The lowest category VII included clomipramine, imipramine, maprotiline, agomelatine. Category VI includes amitriptyline, V - pipofezin, trazodone, mianserin and mirtazapine, IV - vortioxetine, III - venlafaxine and duloxetine, II - sertraline, paroxetine, citalopram, escitalopram, fluoxetine, fluvoxamine and milnacipran, and I - pirlindol and moclobemide. Among the most effective antidepressants (amitriptyline, imipramine, venlafaxine in high daily doses), venlafaxine turned out to be the best tolerability category. This drug is the most effective and well tolerated antidepressant. Other options for the practical use of classifications are discussed.
Side effects can be toxic or neuronal. Neuronal side effects are divided into "extra-therapeutic" (persistent or reversible), as well as "paratherapeutic". Seven categories of antidepressant tolerance have been identified. The lowest category VII included clomipramine, imipramine, maprotiline, agomelatine. Category VI includes amitriptyline, V - pipofezin, trazodone, mianserin and mirtazapine, IV - vortioxetine, III - venlafaxine and duloxetine, II - sertraline, paroxetine, citalopram, escitalopram, fluoxetine, fluvoxamine and milnacipran, and I - pirlindol and moclobemide. Among the most effective antidepressants (amitriptyline, imipramine, venlafaxine in high daily doses), venlafaxine turned out to be the best tolerability category. This drug is the most effective and well tolerated antidepressant. Other options for the practical use of classifications are discussed.
Summary
A classification of the side effects of antidepressants is presented. Side effects can be toxic or neuronal. Neuronal side effects are divided into "extratherapeutic" (persistent or reversible), as well as "paratherapeutic". Seven antidepressant tolerance categories have been identified. The lowest VII category included clomipramine, imipramine, maprotiline, agomelatine. Amitriptyline belongs to the VI category, pipofezin, trazodone, mianserin and mirtazapine to the V category, vortioxetine belongs to the IV category, venlafaxine and duloxetine to the III category, sertraline, paroxetine, citalopram, escitalopram, fluoxetine, fluvoxamine and milnacipran to the II category, and pirlindole and moclobemide to the I category. Among the most effective antidepressants (amitriptyline, imipramine, venlafaxine in high daily doses), venlafaxine was in the best category of tolerability. This drug is the most effective and tolerable antidepressant. Other options for the practical use of classifications are discussed.
Side effects can be toxic or neuronal. Neuronal side effects are divided into "extratherapeutic" (persistent or reversible), as well as "paratherapeutic". Seven antidepressant tolerance categories have been identified. The lowest VII category included clomipramine, imipramine, maprotiline, agomelatine. Amitriptyline belongs to the VI category, pipofezin, trazodone, mianserin and mirtazapine to the V category, vortioxetine belongs to the IV category, venlafaxine and duloxetine to the III category, sertraline, paroxetine, citalopram, escitalopram, fluoxetine, fluvoxamine and milnacipran to the II category, and pirlindole and moclobemide to the I category. Among the most effective antidepressants (amitriptyline, imipramine, venlafaxine in high daily doses), venlafaxine was in the best category of tolerability. This drug is the most effective and tolerable antidepressant. Other options for the practical use of classifications are discussed.
In the previous article, a description of the mechanism of action of various antidepressants (tricyclic - TcA, serotonin-modulating - CMA, four-cyclic - HcA, reversible monoamine oxidase type A inhibitors - RMAO-A, selective serotonin reuptake inhibitors - SSRIs, selective serotonin and norepinephrine reuptake inhibitors) was presented. - SNRIs, norepinephrine and selective serotonin - NaSSA, melatonergic - MeA, multimodal - MmA) (Table 1).
- SNRIs, norepinephrine and selective serotonin - NaSSA, melatonergic - MeA, multimodal - MmA) (Table 1).
Table 1. Known antidepressants in Russia, their effect on neurons and the "formula" of the mechanism of action (1-4).
* - white color - the drug does not affect neurons, dark gray - a pronounced increase in activity, light gray - a moderate increase in activity, ** - in high doses, IOD - neurotransmitter reuptake inhibitors, NERR - agents that affect regulatory receptors, RMAO-A - reversible inhibitors of monoamine oxidase type "A".
All these drugs, to varying degrees, contribute to the activation of serotonin (↑C or ↑s), noradrenaline (↑H or ↑n), dopamine (↑D or ↑d) or melatonin (↑M or ↑m) neurons, the “tone” of which decreases with depression. But the most pronounced effect on the vital activity of neurons is ↑SNd-antidepressants: amitriptyline and imipramine (TcA), as well as venlafaxine (SNRI) in high daily doses. It is no coincidence that many experts refer to their most effective drugs for the treatment of depression (5).
It is no coincidence that many experts refer to their most effective drugs for the treatment of depression (5).
Of course, the choice of any antidepressant should be associated not only with its medicinal properties (effectiveness), but also with side effects (tolerability). The vast majority of authors agree that tolerability is best with SSRIs and worse with TcA (6-9), with other drugs in between (1). This assessment of the tolerability of antidepressants is correct, but is generalized. To clarify it, one should refer to the data on the mechanisms of the formation of side effects.
A smaller part of them is due to the toxic effect of antidepressants on the organs and tissues of patients. These “toxic” side effects are very dangerous (10). For example, while taking some TcA (clomipramine, imipramine), as well as MeA (agomelaptin), drug-induced hepatitis is observed, which leads to the death of patients (10, 11). Serious toxic side effects are also found in maprotiline, which causes agranulocytosis and leukopenia (12). Fortunately, toxic side effects are very rare and can be detected in a timely manner by test results.
Fortunately, toxic side effects are very rare and can be detected in a timely manner by test results.
For example, when agomelatine was found to cause severe and drug-induced hepatitis, detailed precautionary instructions were added to its package leaflet (11). They include a biochemical blood test, which is prescribed to all patients (without exception) before prescribing the drug, as well as while taking it. A similar analysis is required for patients receiving clomipramine and imipramine (13,14). However, when prescribing these antidepressants, biochemical analysis is required only for patients with pre-existing liver disease. Finally, regular CBCs to detect agranulocytosis and leukopenia are also required during treatment with maprotiline (12).
Obviously, the need for additional tests can significantly complicate the use of antidepressants. Fortunately, this is only required when using the listed drugs. When prescribing other antidepressants, you do not need to resort to additional examinations.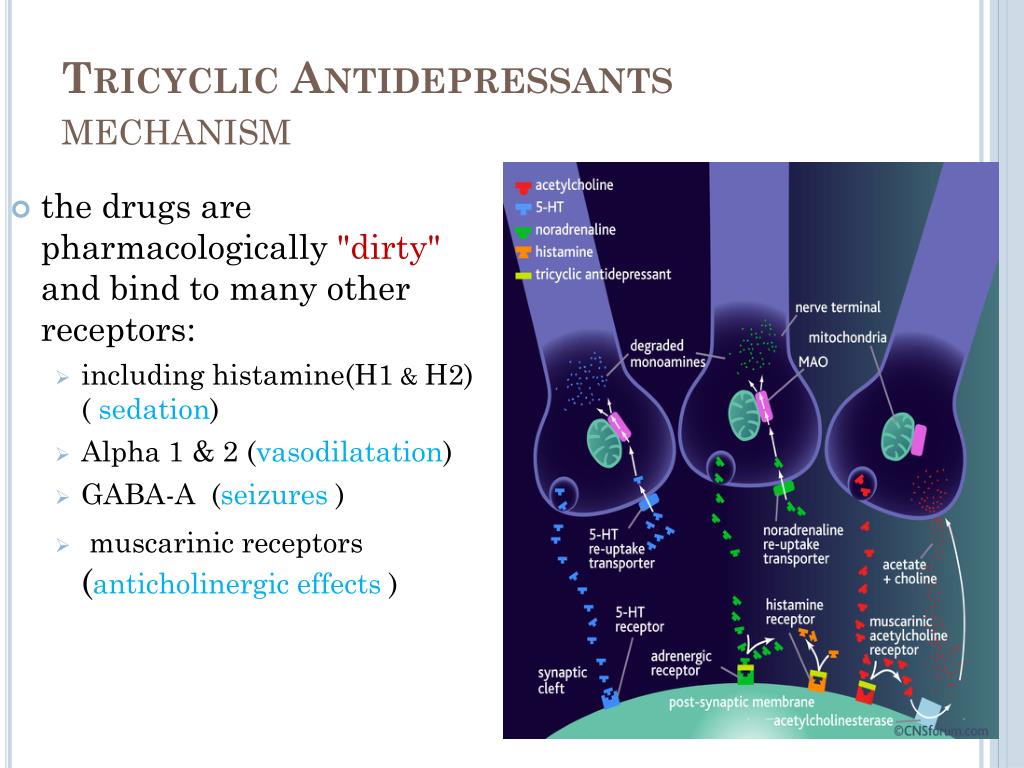 However, their tolerability may worsen due to the adverse effects of drugs on neurons. As a result, "neuronal" side effects are formed, which, however, do not directly threaten the lives of patients and are easily diagnosed by their complaints.
However, their tolerability may worsen due to the adverse effects of drugs on neurons. As a result, "neuronal" side effects are formed, which, however, do not directly threaten the lives of patients and are easily diagnosed by their complaints.
Some of the neuronal side effects are due to the effect of the antidepressant on histamine and acetylcholine neurons, which do not decrease their activity in the formation of mental disorders that are indications for antidepressant prescription (2,15). Accordingly, such pharmacological properties can be designated as "extra-therapeutic" (unnecessary, not related to the treatment process) side effects. They only increase the number of neuronal systems that suffer in the patient. Most often, "extra-curative" side effects are persistent. They may occur throughout the course of treatment, particularly when the antidepressant blocks excitatory receptors on histamine and acetylcholine neurons (15).
This mechanism of action, which is more characteristic of antipsychotics than antidepressants, leads to a sharp drop in the activity (inhibition) of these nerve cells (↓G and ↓A) (1,2). Moreover, normal histamine and acetylcholine neurons cannot restore their functions, since there are no effective compensatory mechanisms for this. Accordingly, patients develop persistent mental and somatic symptoms that seriously complicate treatment (Table 2).
Moreover, normal histamine and acetylcholine neurons cannot restore their functions, since there are no effective compensatory mechanisms for this. Accordingly, patients develop persistent mental and somatic symptoms that seriously complicate treatment (Table 2).
Table 2. The main "extra-therapeutic" side effects of antidepressants associated with the blockade of excitatory receptors on histamine and acetylcholine neurons (1,2)
Drowsiness, fatigue, deterioration of memory and attention are characteristic. There are complaints of dry mouth, disturbances of accommodation and urination, constipation, pain in the eyes due to an increase in intraocular pressure, heart rhythm disturbances, increased appetite and weight gain.
There is, however, an antidepressant that does not have permanent "off-the-shelf" side effects. This drug is vortioxetine. It does not inhibit histamine and acetylcholine neurons (due to the blockade of excitatory receptors), but increases their "tone" by influencing regulatory receptors (16). On the one hand, this provides vortioxetine with a unique nature of “non-therapeutic” side effects. In particular, when taking this antidepressant, excitement, anger, "unusual" dreams, and insomnia can be observed (Table 3).
On the one hand, this provides vortioxetine with a unique nature of “non-therapeutic” side effects. In particular, when taking this antidepressant, excitement, anger, "unusual" dreams, and insomnia can be observed (Table 3).
Table 3. "Extra-curative" side effects of vortioxetine (16,17).
Characterized by ketoacidosis, somatic complaints of dizziness, itching (including generalized), sweating, hot flashes, nausea, diarrhea, vomiting. On the other hand, these side effects are fundamentally reversible, since neurons have special mechanisms that are aimed at combating excessive activation. To do this, they can, for example, desensitize their regulatory receptors (a mechanism known as self-regulation). Therefore, the “non-therapeutic” side effects of vortioxetine often resolve spontaneously within the first two weeks of treatment (16).
Turning now to the rest of the antidepressants, we point out that the vast majority of them do not have "extra-curative" side effects at all, which increase the number of affected neuronal systems (2). Many drugs do not affect histamine and acetylcholine neurons. Moreover, they increase the activity of only those neurons (serotonin, norepinephrine and dopamine), whose "tone" is reduced in mental disorders, which are indications for the appointment of antidepressants. However, even this feature cannot save antidepressants from "neuronal" side effects. The latter will arise due to the fact that within any affected system of neurons, the activity of only part of the nerve cells decreases, while the functions of the other part are not disturbed. Antidepressants both activate the "affected" neurons and create therapeutic effects, and increase the "tone" of normally functioning nerve cells and cause side effects.
Many drugs do not affect histamine and acetylcholine neurons. Moreover, they increase the activity of only those neurons (serotonin, norepinephrine and dopamine), whose "tone" is reduced in mental disorders, which are indications for the appointment of antidepressants. However, even this feature cannot save antidepressants from "neuronal" side effects. The latter will arise due to the fact that within any affected system of neurons, the activity of only part of the nerve cells decreases, while the functions of the other part are not disturbed. Antidepressants both activate the "affected" neurons and create therapeutic effects, and increase the "tone" of normally functioning nerve cells and cause side effects.
At the same time, the tolerability of antidepressants paradoxically turns out to be a “hostage” of their therapeutic properties. The more effectively the drug activates the affected neurons, the more it affects similar nerve cells that are still functioning at the proper level. Therefore, it is advisable to designate the side effects under consideration as “paratherapeutic”. They are manifested by anxiety, restlessness, insomnia and anxiety (Table 4).
Therefore, it is advisable to designate the side effects under consideration as “paratherapeutic”. They are manifested by anxiety, restlessness, insomnia and anxiety (Table 4).
Table 4. Main "paratherapeutic" side effects of antidepressants (15)
Somatic complaints are represented by sexual dysfunction, disruption of the digestive organs and heart rhythm, fluctuations in blood pressure. As a rule, "paratherapeutic" side effects are reversible. They may resolve on their own in the second or third week of treatment (18). This is due to the above-mentioned ability of "normal" neurons to quickly adapt to excessive activation, reducing their sensitivity to neurotransmitters (2) 2 .
The presented data on toxic and neuronal side effects can be used to classify antidepressants into seven tolerability categories, where the last, seventh, is the worst, and the first is the best (Table 5).
Table 5. Antidepressant tolerance categories based on toxic and neuronal side effects.
Antidepressant tolerance categories based on toxic and neuronal side effects.
Thus, antidepressants from the lowest category VII (clomipramine, imipramine, maprotiline, agomelatine) have toxic side effects that directly threaten the lives of patients. Moreover, their appointment requires additional examination of patients. Problems with tolerability of other antidepressants are already due to neuronal side effects. All of them are not fatal, and additional examination is usually not required to identify them.
Neuronal side effects are divided into "extra-therapeutic" and "para-therapeutic". The first, as already mentioned above, are associated with an "additional" dysfunction of histamine and acetylcholine neurons, which do not reduce their activity in mental disorders, which are indications for prescribing antidepressants. Accordingly, "non-therapeutic" side effects, expanding the range of affected neuronal systems, determine the belonging of drugs to lower tolerance categories (VI, V and IV). In particular, amitriptyline contributes to a persistent decrease in the activity of histamine and acetylcholine neurons and is therefore classified as tolerability category VI. “Extra-curative” side effects for Category V antidepressants are more limited. After all, pipofezin, trazodone, mianserin and mirtazapine contribute to a persistent decrease in the activity of only histamine neurons. Vortioxetine is assigned to the next higher tolerance category IV. This antidepressant has the ability to increase the activity of histamine and acetylcholine neurons. However, the associated side effects are often reversible.
In particular, amitriptyline contributes to a persistent decrease in the activity of histamine and acetylcholine neurons and is therefore classified as tolerability category VI. “Extra-curative” side effects for Category V antidepressants are more limited. After all, pipofezin, trazodone, mianserin and mirtazapine contribute to a persistent decrease in the activity of only histamine neurons. Vortioxetine is assigned to the next higher tolerance category IV. This antidepressant has the ability to increase the activity of histamine and acetylcholine neurons. However, the associated side effects are often reversible.
The highest tolerance categories I-III include antidepressants that affect only serotonin, norepinephrine and dopamine neurons, which suffer from mental disorders that are indications for prescribing drugs. These drugs are characterized by "paratherapeutic" side effects that do not increase the number of affected neuronal systems (Table 5). They arise due to the activation of a part of serotonin, norepinephrine and dopamine neurons, which still retain their normal "tone" (2). At the same time, the severity of "paratherapeutic" side effects depends, first of all, on the ability of the antidepressant to act on serotonin and norepinephrine nerve cells, since they all have little effect on dopamine (Table 1).
At the same time, the severity of "paratherapeutic" side effects depends, first of all, on the ability of the antidepressant to act on serotonin and norepinephrine nerve cells, since they all have little effect on dopamine (Table 1).
Accordingly, antidepressants, which simultaneously effectively activate serotonin and norepinephrine neurons, are assigned to category III of tolerance. These drugs are venlafaxine and duloxetine (Tables 1 and 5). The first of them, depending on the dose, is ↑CH- or ↑CHd-antidepressant. As for duloxetine, it has the properties of a ↑CH drug. Category II includes antidepressants that contribute to a pronounced activation of only serotonin or only norepinephrine neurons (Tables 1 and 5). These include all ↑C-antidepressants (sertraline, paroxetine, citalopram, escitalopram, fluoxetine, fluvoxamine), as well as ↑cHd antidepressant - milnacipran. Finally, drugs that are not capable of strong activation of serotonin and norepinephrine neurons have the highest tolerance category I (Tables 1 and 5). These are two ↑snd antidepressants - pirlindol and moclobemide.
These are two ↑snd antidepressants - pirlindol and moclobemide.
In conclusion, it should be noted that the presented classification of antidepressants according to tolerability does not claim to be comprehensive. However, it provides clear criteria for assessing the main side effects, which allow you to compare different drugs with each other. It seems that this is especially important in a situation where there are no clear recommendations for taking into account side effects when prescribing antidepressants. For example, a generalized formula is currently used in various publications and instructions. An antidepressant is suggested to be used "only after careful assessment of the expected benefit/risk ratio in patients" (11). But the results of such a "thorough assessment" tend to be in favor of prescribing the drug.
In particular, they write about agomelatine that if all the requirements of the instructions for prescribing an antidepressant are met, then the risk of developing drug-induced hepatitis becomes minimal (19).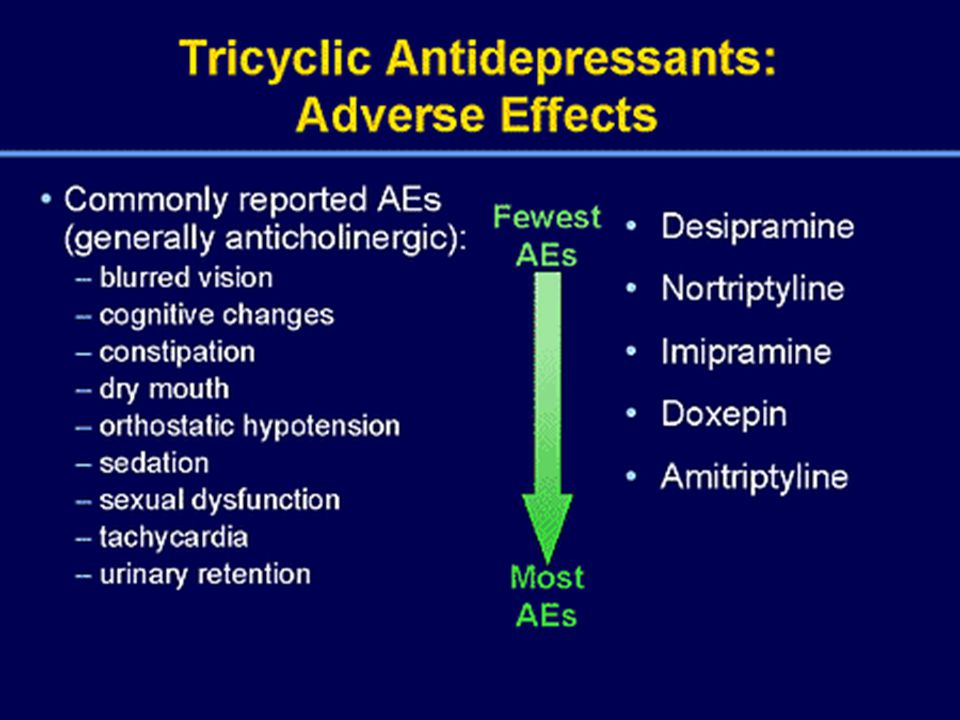 However, the unique mechanism of action attributed to agomelatine suggests that the benefits of prescribing an antidepressant are far greater than the disadvantages associated with its hepatotoxicity (19). Meanwhile, all the uniqueness of the mechanism of action of agomelatine is reduced to the possibility of influencing the neurons of the suprachiasmatic nucleus, the neurotransmitter of which is melatonin. And this effect is not required at all for the treatment of depression, since any antidepressant that activates serotonin and norepinephrine neurons can compensate for the deficiency of melatonin activity (20).
However, the unique mechanism of action attributed to agomelatine suggests that the benefits of prescribing an antidepressant are far greater than the disadvantages associated with its hepatotoxicity (19). Meanwhile, all the uniqueness of the mechanism of action of agomelatine is reduced to the possibility of influencing the neurons of the suprachiasmatic nucleus, the neurotransmitter of which is melatonin. And this effect is not required at all for the treatment of depression, since any antidepressant that activates serotonin and norepinephrine neurons can compensate for the deficiency of melatonin activity (20).
The recommendations for "thorough evaluation" presented here are not the only examples of flippant judgments about the tolerability of antidepressants. Some authors believe that side effects are weakly related to the mechanism of action of drugs. Side effects are said to be non-specific, probabilistic and therefore almost unpredictable (18). Other authors are at least looking for the reasons for the formation of side effects in order to take them into account when prescribing antidepressants. Unfortunately, they find these reasons not in the mechanisms of action of drugs, but in the characteristics of depression, public opinion or the psychology of the patient.
Unfortunately, they find these reasons not in the mechanisms of action of drugs, but in the characteristics of depression, public opinion or the psychology of the patient.
Thus, it is reported that even with the use of any of the “most easily tolerated drugs in 80% of patients with mild to moderate depression” (21), heterogeneous adverse events are noted. They are most common in dysthymia, first depressive states, with anxiety and somatic symptoms (21, 22), in persons over 45 years of age, with a high body weight deficit (22), and a history of negative placebo reactions in anamnesis (23). Poor tolerability of antidepressants has been reported to be associated with patients' high demands for quality of life (24) and their anxiety about social exclusion (25). The initially negative attitude towards psychiatry on the part of public opinion, the patient's low awareness of his own illness and the therapy recommended by the doctor, the unsatisfactory experience of previous treatment, etc. , also contribute to the problem. (22, 26).
, also contribute to the problem. (22, 26).
The speculation of such constructions is obvious. To refute them, it suffices to say that the side effects of drugs, as defined by the WHO, are caused by their pharmacological properties (37). It is hard to imagine that the inhibition of histamine and acetylcholine neurons arose due to the patient's high demands on the quality of life, the excessive activation of serotonin, norepinephrine and dopamine neurons due to the negative attitude towards psychiatry on the part of public opinion, and drug-induced hepatitis due to anxiety about social maladaptation.
Thus, the presented classification of antidepressants according to tolerability categories allows us to return the study of side effects to the mainstream of biological psychiatry. In addition, this classification is easy to use in practical medicine. In particular, the lower the tolerability category of an antidepressant, the greater the need for a special justification for prescribing it (effectiveness, positive experience of treatment in the past, the patient's desire, etc. ). In turn, the appearance of such a detailed justification in the history of the disease will help to avoid many problems (psychological, social and others) that arise in the process of treatment between the doctor and his patient.
). In turn, the appearance of such a detailed justification in the history of the disease will help to avoid many problems (psychological, social and others) that arise in the process of treatment between the doctor and his patient.
With the help of the presented classification, it is easy to decide on the choice of the most effective and tolerable antidepressant. To do this, it is only necessary to compare the tolerability categories of the most effective drugs: amitriptyline (TcA), imipramine (TcA) and venlafaxine (SNRI) (5). The first of them (amitriptyline) belongs to the VI category of tolerance (Table 5). The side effects of the second antidepressant (imipramine) are even worse. This drug belongs to the VII category of tolerance. As for venlafaxine, the side effects of this antidepressant are much weaker, and this drug belongs to category III tolerance. Thus, venlafaxine, when used at high doses, is the most effective and tolerated drug in the treatment of depression.
Venlafaksin is well-known in our country under the trade name Velaksin (Egis). This drug has been studied in leading scientific organizations that carry out cutting-edge research in the field of psychiatry. Among them are the Federal State Budgetary Institutions “State Scientific Center for Social and Forensic Psychiatry named after V.P. Serbsky" and "Moscow Research Institute of Psychiatry" of the Ministry of Health of Russia, St. Petersburg Research Institute. V.M. Bekhterev (28.29). Prolonged-release capsules (Velaxin retard) (30) are also well-known, with the use of which there is a significant reduction in the frequency of such a side effect of the drug as nausea (31). In addition, the study of Velaksin was successfully carried out not only in psychiatry, but also in neurology (32).
This drug has been studied in leading scientific organizations that carry out cutting-edge research in the field of psychiatry. Among them are the Federal State Budgetary Institutions “State Scientific Center for Social and Forensic Psychiatry named after V.P. Serbsky" and "Moscow Research Institute of Psychiatry" of the Ministry of Health of Russia, St. Petersburg Research Institute. V.M. Bekhterev (28.29). Prolonged-release capsules (Velaxin retard) (30) are also well-known, with the use of which there is a significant reduction in the frequency of such a side effect of the drug as nausea (31). In addition, the study of Velaksin was successfully carried out not only in psychiatry, but also in neurology (32).
M.Yu Drobizhev's video on the same topic can be viewed at the link: https://www.youtube.com/watch?v=SwtO_bC_838&t=11s
References
- Antidepressant therapy and other treatments for depressive disorders.
 Report of the CINP Working Group based on a review of the evidence. Ed. V.N. Krasnov. M., 2008. - 215 S.
Report of the CINP Working Group based on a review of the evidence. Ed. V.N. Krasnov. M., 2008. - 215 S. - Stahl S.M. Stahl's essential psychopharmacology: neuroscientific basis and practical application. — 3nd ed. Cambridge University Press, 2008. - 1117P.
- Drobizhev M. Yu., Fedotova A. V., Kikta S. V., Antokhin E. Yu. Between depression and fibromyalgia: the fate of an antidepressant. Journal of Neurology and Psychiatry. S.S. Korsakov. 2016;116(4): 114-120. DOI:10.17116/jnevro201611641114-120.,
- Shagiakhmetov F.Sh., Anokhin P.K., Shamakina I.Yu. Vortioxetine: mechanisms of multimodality and clinical efficacy. Social and Clinical Psychiatry 2016;26(4): 84-96
- Bauer M., Pfennig A., Severus E., Weibrau P.S., J. Angst, Müller H.-J. Clinical guidelines of the World Federation of Societies of Biological Psychiatry for the biological therapy of unipolar depressive disorders. Part 1: Acute and ongoing treatment of unipolar depressive disorders as of 2013.
 Modern therapy of mental disorders 2015;4:33-39.).
Modern therapy of mental disorders 2015;4:33-39.). - Anderson IM. SSRIS versus tricyclic antidepressants in depressed inpatients: a meta-analysis of efficacy and tolerability. depression. Anxiety. 1998;7(Suppl 1):11-17.
- Anderson IM, Nutt DJ, Deakin JF. Evidence based guidelines for treating depressive disorders with antidepressants: a revision of the 1993 British Association for Psychopharmacology guidelines. J Psychopharmacol. 2000;14:3-20.
- Peretti S, Judge R, Hindmarch I. Safety and tolerability considerations: tricyclic antidepressants vs. selective serotonin reuptake inhibitors. Acta Psychiatr. Scand. 2000; Suppl. 403:17-25.
- Wilson K, Mottram P, Sivanranthan A, Nightingale A. Antidepressant versus placebo for depressed elderly. 2001 Cochrane. database. Syst. Rev. CD000561.) and worse for TcA
- Liver Tox. https://livertox.nlm.nih.gov
- Valdoxan - instructions for the medical use of the drug.
 https://medi.ru/instrukciya/valdoksan_5084/
https://medi.ru/instrukciya/valdoksan_5084/ - Lyudiomil - official instructions for use. https://medi.ru/instrukciya/lyudiomil_9448/
- Anafranil tablets - instructions (information for specialists) on the use of the drug. https://medi.ru/instrukciya/anafranil-tabletki_8616/
- Melipramine tablets - official instructions for use. https://medi.ru/instrukciya/melipramin-tabletki_4780/
- Drobizhev M.Yu., Ovchinnikov A.A., Kikta S.V. Why do antidepressants have side effects? Pharmateka. 2015. No. 20 (313). pp. 72-77.
- Brintellix (Brintellix). https://www.rlsnet.ru/tn_index_id_87791.htm
- Subeesh V, Singh H, Maheswari E, Beulah E. Novel adverse events of vortioxetine: A disproportionality analysis in USFDA adverse event reporting system database. Asian J Psychiatr. 2017 Dec;30:152-156. doi: 10.1016/j.ajp.2017.09.005.
- Borodin V.I. Tolerability of treatment in patients with depressive disorders (complex analysis).
 Abstract for the competition … doc. honey. Sciences. Moscow. 2009.
Abstract for the competition … doc. honey. Sciences. Moscow. 2009. - Freiesleben SD, Furczyk K.J A systematic review of agomelatine-induced liver injury. Mol Psychiatry. 2015 Apr 21;3(1):4. doi: 10.1186/s40303-015-0011-7. eCollection 2015.
- Drobizhev M.Yu. Timing of meta-analyses and efficacy of antidepressants in depression. Social and clinical psychiatry. 2017;4:81-88.
- Aldushin A.A. Antidepressant therapy tolerance and withdrawal forecast based on the analysis of nocebo effects. Russian psychiatric journal. 2009; 3:55-61.
- Avedisova A.S., Borodin V.I., Aldushin A.A. Comparison of the efficacy and tolerability of antidepressants of different groups in mild and moderate depression. Journal of Neurology and Psychiatry. S.S. Korsakov. 2006;11:15-19.
- Lapin I.P. Personality and medicine. Introduction to the psychology of pharmacotherapy. - St. Petersburg: Dean, 2001.-416C.
- Roberis H. Neurotic patients who terminate their own treatment.
 Br. J. Psychiatry. 1985; 146(4):443-445.
Br. J. Psychiatry. 1985; 146(4):443-445. - Mosolov S.N., red. Reference guide to psychopharmacology. Psychopharmacological and antiepileptic drugs approved for use in Russia: 2nd ed. BINOM, Moscow, 2004. - 304C.
- Avedisova A.S., Borodin V.I. Non-compliance or refusal of psychopharmacotherapy? Russian psychiatric journal. 2006; 1:61-65.
- http://vmede.org/sait/?id=Farmakologija_klin_farm_y4ebnik_kykes_2009&menu=Farmakologija_klin_farm_y4ebnik_kykes_2009&page=7
- Krasnov V.N., Kryukov V.V. Velaxin® (venlafaxine) in modern therapy of depression: results of the first Russian multicenter efficacy and safety study. Psychiatry and psychopharmacotherapy. 2007;9 (4), http://www.consilium-medicum.com/magazines/special/psychiatry/article/15426
- Mosolov S.N., Kostyukova E.G., Gorodnichev A.V., Timofeev I.V., Ladyzhensky M.Ya., Serditov O.V. Clinical efficacy and tolerability of venlafaxine (Velaxin) in the treatment of moderate and severe depression.
 Modern therapy of mental disorders. 2007;3:58-63.
Modern therapy of mental disorders. 2007;3:58-63. - Avedisova A.S., Zakharova K.V., Kanaeva L.S., Vazagaeva T.I., Aldushin A.A. Psychiatry and psychopharmacotherapy. 2009;11(1):36-40.
- Avedisova A.S. Venlafaxine (velaxin): results of international trials of a third-generation antidepressant. Psychiatrist. and a psychopharmacologist. 2006; 11(2):2-7.
- Mosolov S.N. Clinical use of modern antidepressants. SPb., 1995.-565C.).
M.Yu. Drobizhev , Doctor of Medical Sciences, Head of the Educational Department of the Training Center of the Association of Medical and Pharmaceutical Universities of Russia. Contact information – [email protected]
E.Yu. Antokhin , Candidate of Medical Sciences, Associate Professor, Head of the Department of Clinical Psychology and Psychotherapy, Orenburg State Medical University, Ministry of Health of Russia.
R. I. Palaeva – Assistant of the Department of Clinical Psychology and Psychotherapy of FSBEI HE “Orenburg State Medical University” of the Ministry of Health of Russia.
I. Palaeva – Assistant of the Department of Clinical Psychology and Psychotherapy of FSBEI HE “Orenburg State Medical University” of the Ministry of Health of Russia.
S. V. Kikta , candidate of medical sciences, head. Department of the Federal State Budgetary Institution "Polyclinic No. 3" of the Administration of the President of the Russian Federation, Moscow
1 There are probably side effects due to excessive activation of melatonin nerve cells. However, they are not yet described even in the instructions for agomelatine, a melatonergic drug that has a direct effect on them (11).
2 Theoretically, “paratherapeutic” side effects can be observed even against the background of “extra-therapeutic” ones. After all, any antidepressants to varying degrees activate serotonin, norepinephrine or dopamine neurons. However, drugs are dominated by "extra-curative" side effects, if only because they are most often persistent. At the same time, "paratherapeutic" side effects are always reversible. In addition, not all antidepressants that have “non-therapeutic” side effects are capable of seriously activating serotonin, norepinephrine and dopamine neurons.
At the same time, "paratherapeutic" side effects are always reversible. In addition, not all antidepressants that have “non-therapeutic” side effects are capable of seriously activating serotonin, norepinephrine and dopamine neurons.
whether they help, treat or relieve symptoms, cause addiction, make them gain weight
Daniil Davydov
medical journalist
Author profile
million people.
At the same time, the cures for this disease are surrounded by many myths. Antidepressants are accused of ineffectiveness and severe side effects, but often the problem is not with the drugs themselves, but with their misuse.
We collected 8 myths about antidepressants and found out how close they are to the truth.
Go see a doctor
Our articles are written with love for evidence-based medicine. We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
Myth 1
Antidepressants almost never helpMost likely, this myth arose due to the fact that antidepressants do not work in all patients - so even some doctors and scientists doubt their effectiveness. However, antidepressants cannot be called ineffective, there are just important nuances in the use of these drugs.
Antidepressants are a class of drugs that normalize the level of neurotransmitters, that is, chemicals that help nerve cells in the brain exchange information.
What are Antidepressants - International Drug Database RxLis
What Medications Help Clinical Depression in Adults - International Primer for Physicians UpToDate
How Antidepressants Help Pain - Mayo Clinic Bulletin
All Antidepressants Used to Treat Depression in Adults , work - The Lancet
Who Antidepressants Help and Who Don't - Clinical Guidelines for British PhysiciansPDF, 141 KB
These medicines help people whose problems are due to a deficiency or excess of neurotransmitters. Antidepressants reduce symptoms of depression, obsessive-compulsive disorder, generalized anxiety disorder, post-traumatic stress disorder, and bipolar affective disorder.
Antidepressants reduce symptoms of depression, obsessive-compulsive disorder, generalized anxiety disorder, post-traumatic stress disorder, and bipolar affective disorder.
There is evidence that antidepressants are effective for chronic pain. Antidepressants increase the amount of neurotransmitters in the spinal cord, which reduces pain signals.
Most specialists have no doubts that antidepressants work. For example, according to the British Royal College of Psychiatry, 50-65% of people with depression who take antidepressants feel better - compared with 25-30% of those who take a placebo.
However, there are situations where the benefit of antidepressants is questionable. For example, antidepressants are good for treating moderate to severe depression, but do not work well for people with mild depression - psychotherapy is more suitable for them.
And there are situations when these medicines were prescribed by mistake. Then antidepressants really won't help.
When antidepressants don't help
Sergey Divisenko
psychotherapist
There are three cases when antidepressants most often cause problems.
The antidepressant didn't work because the doctor prescribed the wrong dose. Minimum doses of these drugs do not help in half of the cases. Then competent doctors increase the doses to those recommended in clinical guidelines, while illiterate ones refuse them.
Sometimes, in order for antidepressants to work, they need to be augmented—i.e., enhanced—with other classes of drugs. For example, second-generation antipsychotics, or normothymics, that is, drugs that stabilize mood. If this is not done, the person taking antidepressants will not feel relief.
The antidepressant didn't work because the doctor misdiagnosed and was trying to treat a condition for which these drugs don't work. To help a person, one had to either use other drugs or use non-drug methods of treatment: for example, psychotherapy, transcranial stimulation, or electroconvulsive therapy.
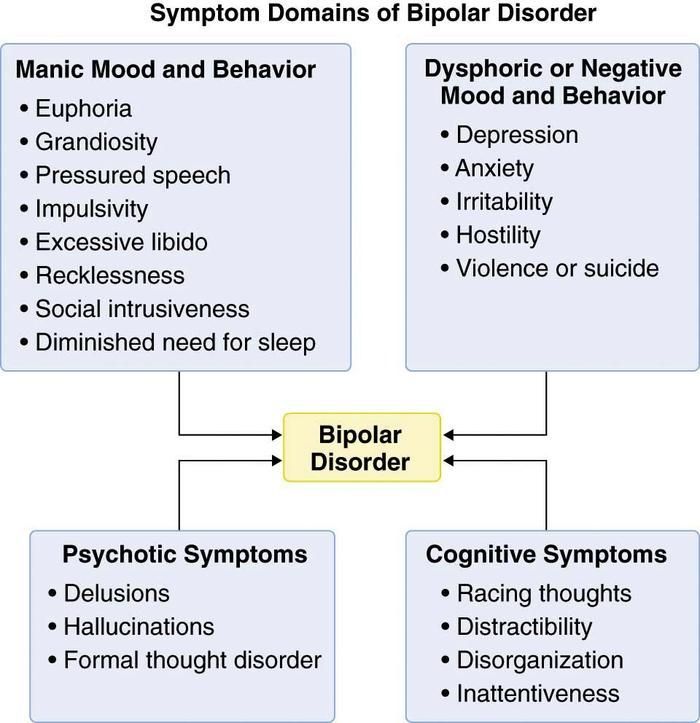
For example, in bipolar disorder, symptoms can be very similar to depression or anxiety. But with bipolar disorder, antidepressants help only if they are used together with other drugs - mood stabilizers. By themselves, they will either work for a short time, or they will not work, or they can cause a phase inversion - that is, a person will switch from a depressive phase to a manic one.
The patient was not helped by a particular antidepressant, but another might. Antidepressants differ in the principle of action - on this basis they are divided into classes. It happens that one antidepressant does not work, but another from the same or another class helps. If the treatment does not work, you should not stop drug therapy, but continue to look for a drug that will help this particular patient.
Myth 2
Antidepressants only relieve symptoms, but do not eliminate the cause of the disorder In most cases, this is not a myth. However, in some situations, antidepressants act on the cause of the disorder.
Depression is a heterogeneous disease. Experts identify a different number of subtypes of depression - from 4 to 12. But for our purposes, depression can be divided into two large subtypes.
American Criteria for Depressive Disorders - A Handbook for Psychiatrists DSM-5PDF, 32 MB
What Depression Is - An International Primer for Physicians UpToDate
associated with depression. Disorders that can be attributed to this group are more common.
If these causes affect a person long enough and he does not understand how to deal with them, depression may develop. In this situation, antidepressants act as drugs that alleviate the symptoms of the disease. To influence the cause of the problem, psychotherapy is needed.
Depression provoked by internal causes. Approximately 7% of people with depression have the correct way of thinking, there are no internal conflicts and injuries, and there are no serious illnesses. In this situation, the cause of depression is the lack of neurotransmitters: serotonin, norepinephrine and dopamine in the synapses of brain nerve cells.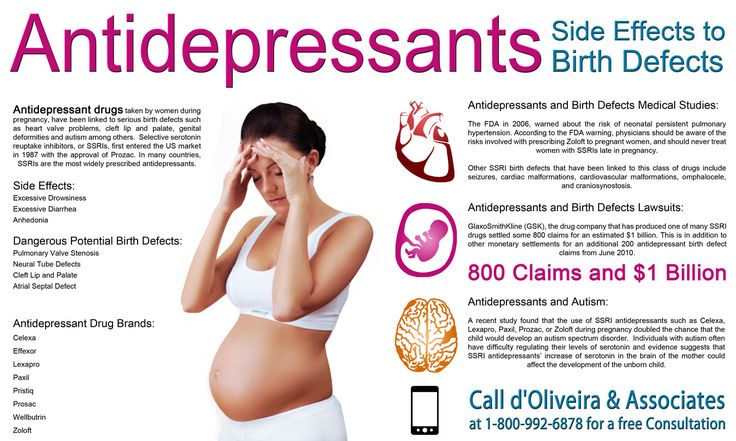 In such people, the antidepressant acts precisely on the cause of the disease, that is, it corrects the production of serotonin in neuronal synapses.
In such people, the antidepressant acts precisely on the cause of the disease, that is, it corrects the production of serotonin in neuronal synapses.
Myth 3
As soon as it gets better, you can stop taking the antidepressantThis is also not entirely a myth - it would be more correct to call it a belief that is true only for some, but not for all patients with depression.
It is generally advised to continue taking antidepressants for at least six months after remission. If the duration of the disease is short, that is, the person was ill for about two weeks, then for the onset of remission, one or two months usually need to take medication. If the duration of the disease is long, from several months or years, then more time is required for the onset of remission. It’s impossible to say exactly how much: different people with depression have different recovery times.
Some people have recurrent depression. In this case, the period during which you need to take the medicine depends on how many bouts of depression have already been during your life.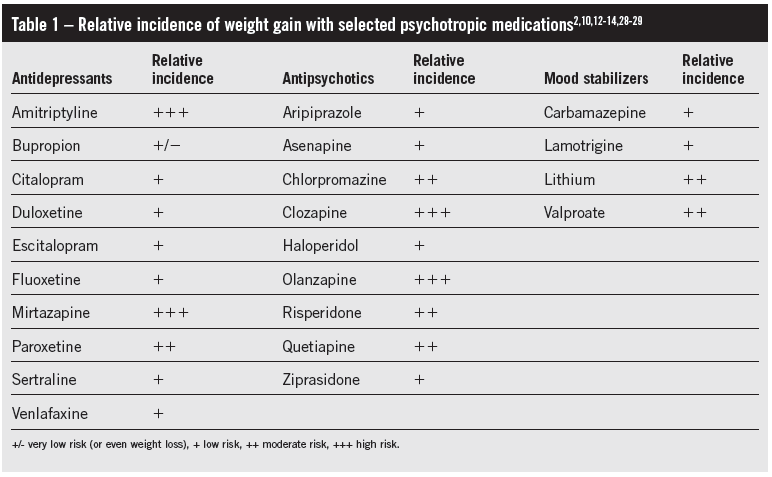 If more than three, it is recommended to take antidepressants for several years or for life.
If more than three, it is recommended to take antidepressants for several years or for life.
Myth 4
Antidepressants cause addictionPerhaps the roots of this myth are that some people need to take depression medication for life. And at the beginning of treatment, some patients have to increase the dose. But in fact, antidepressants do not cause either true physical or drug dependence.
True physical dependence on a drug is a situation where a person becomes so addicted to the drug that when it is withdrawn, the symptoms of the disease sharply increase. People who are dependent on the drug have to increase the dosage, otherwise the drug stops helping.
What is True Drug Addiction - Bulletin of the National Institute for the Study of Drug AbusePDF, 7 MB
What is Drug Addiction - Bulletin of the American Psychiatric Association
Drug dependence may include physical dependence on a drug. But this addiction has a unique feature. Dependence can also develop in a healthy person who used the drug not to recover, but to enjoy it. But when he tries to quit the drug, he still experiences physical suffering, which is called the withdrawal syndrome. As a result, a person is forced to look for a new dose of a drug.
Dependence can also develop in a healthy person who used the drug not to recover, but to enjoy it. But when he tries to quit the drug, he still experiences physical suffering, which is called the withdrawal syndrome. As a result, a person is forced to look for a new dose of a drug.
Although a person who takes antidepressants to treat depression gets better, the drugs themselves are neither pleasurable nor addictive. Taking them as drugs is useless.
Of all the drugs that are used in psychiatry, true physical dependence can only be caused by psychostimulants that activate mental activity and anti-anxiety, that is, benzodiazepine tranquilizers. Antidepressants are not included in this list, because there is no need to increase the dosage of correctly selected drugs from this group.
However, some people who stop taking antidepressants early sometimes experience withdrawal symptoms such as nausea, hand tremors, and some feel “shocks” in the head, similar to the sensations of an electric shock. Depressive symptoms return to patients who need to take the medicine for a very long time.
Depressive symptoms return to patients who need to take the medicine for a very long time.
Antidepressants are sometimes abused, but they cannot cause addiction - Journal of Modern Psychiatry
To avoid unpleasant consequences, stop taking antidepressants only if the attending physician says that they are no longer needed. But even in this situation, it is necessary to cancel antidepressants slowly, that is, gradually reducing the dose. This will help avoid unpleasant side effects.
Myth 5
A person on antidepressants becomes lethargic and loses interest in lifeThis popular myth is based on real but outdated data.
These mental changes are seen in patients taking first-generation tricyclic antidepressants such as amitriptyline. It has a sedative, that is, a sedative effect. A person who takes high doses of amitriptyline can indeed become sleepy and indifferent to the outside world.
Amitriptyline - Sedative - Drugs.com International Drug Database
SSRIs do not sedate - Drugs. com International Drug Database
com International Drug Database
Current second-generation antidepressants that are recommended to start treatment with, such as selective serotonin reuptake inhibitors, or SSRIs almost never cause drowsiness and apathy.
On the contrary, in most people with depression they return interest in life.
Sometimes SSRIs do cause drowsiness, but this has not yet been proven
Sergey Divisenko
psychotherapist
It is believed that in rare cases, modern antidepressants can provoke SSRI-induced apathy. But this condition is extremely rare.
And even then psychiatrists still doubt that the cause is precisely in the drugs, and not in the patient's condition. After all, some people during the time of taking antidepressants may develop other adverse mental states in which apathy occurs: for example, schizotypal disorder, which was not noticed before.
Myth 6
Antidepressants have many side effects This is partly true: both SSRIs and antidepressants from other groups have side effects. But it is quite possible to deal with them.
But it is quite possible to deal with them.
At the start of treatment, when people first start taking antidepressants, many complain of increased anxiety, dry mouth, nausea, and trouble sleeping. But after a few days or weeks after the start of the course of treatment, these symptoms usually disappear. If the side effects do not stop, it makes sense to consult a doctor - he will replace the antidepressant.
Dealing with antidepressant side effects - advice from the Mayo Clinic staff
Here's what to do before the side effects go away:
- Take your antidepressant with meals, unless the instructions say otherwise, so the antidepressant will be less annoying stomach;
- put a bottle of clean water on the work table - if your mouth is dry, you can take a sip. Unsweetened lollipops and chewing gum also help with dry mouth;
- take a walk for at least half an hour before going to bed to make it easier to fall asleep. If you can’t sleep at all, you can ask your doctor to pick up sleeping pills.

The second most common side effect is increased anxiety at the beginning of antidepressant use. To avoid this problem, psychiatrists resort to two effective methods:
- titrate the dose - that is, start with the minimum dose of the antidepressant and then gradually increase it;
- at the beginning of the reception, sedatives - tranquilizers are prescribed together with the antidepressant.
The third common side effect of SSRIs, especially sertraline, known as Zoloft, and escitalopram, better known as Cipralex, is decreased libido. Approximately 20-30% of people taking antidepressants from this group experience a decrease in sexual desire to one degree or another. At the same time, it is difficult to say how much the drugs are to blame, because approximately 35-50% of people with depression have already experienced sexual dysfunction.
Many people with depression experience sexual dysfunction before starting antidepressants - Harvard Medical School Bulletin
Switching to another antidepressant usually helps, but many people prefer to wait until the medication can be stopped. In some cases, psychiatrists prescribe antidepressants from other groups in addition to the libido-lowering antidepressant. Sometimes it helps to regain interest in sex.
In some cases, psychiatrists prescribe antidepressants from other groups in addition to the libido-lowering antidepressant. Sometimes it helps to regain interest in sex.
Myth 7
Weight gain due to antidepressantsThis is not a myth, but a half-truth. There are both antidepressants that contribute to weight gain, and those that do not have a similar effect.
The most common complaint about weight gain during treatment is people taking the tetracyclic antidepressant mirtazapine, which actually increases appetite. Another weight gaining antidepressant is paroxetine, better known by the trade name Paxil. But "Zoloft" and "Cipralex" do not contribute to weight gain.
If a patient feels that an antidepressant is causing them to overeat, it is wise to consult a doctor and discuss a change of medication.
Myth 8
Antidepressants are expensive True, but not for all patients. Most people can cure depression and not go broke.
Antidepressants from different groups vary greatly in price. There are both very expensive drugs and relatively low-cost drugs among them. At the same time, both of them work equally well. However, there are situations when a cheap antidepressant cannot be dispensed with.
On the left - inexpensive "Zoloft" for 327 R, a drug based on sertraline, on the right - the most expensive antidepressant "Ixel" based on milnacipran for 2453 R For example, there is a good antidepressant venlafaxine. The maximum dose of venlafaxine can reach up to 375 mg per day. If these are inexpensive tablets of a domestic manufacturer, then a course of treatment for a month costs about 2000 R. But sometimes inexpensive tablets are not very well tolerated: they cause headache, nausea, sweating, tachycardia, that is, rapid heartbeat. In such cases, you need to switch to a prolonged form of venlafaxine - "Venlafaxine Retard", or "Velaxin XR". But this drug is more expensive: a course of treatment will cost about 5000 R per month.