Bipolar or adhd quiz
Bipolar Disorder Test for Adults: Manic & Depressive Symptoms
Bipolar Symptoms Test for Adults
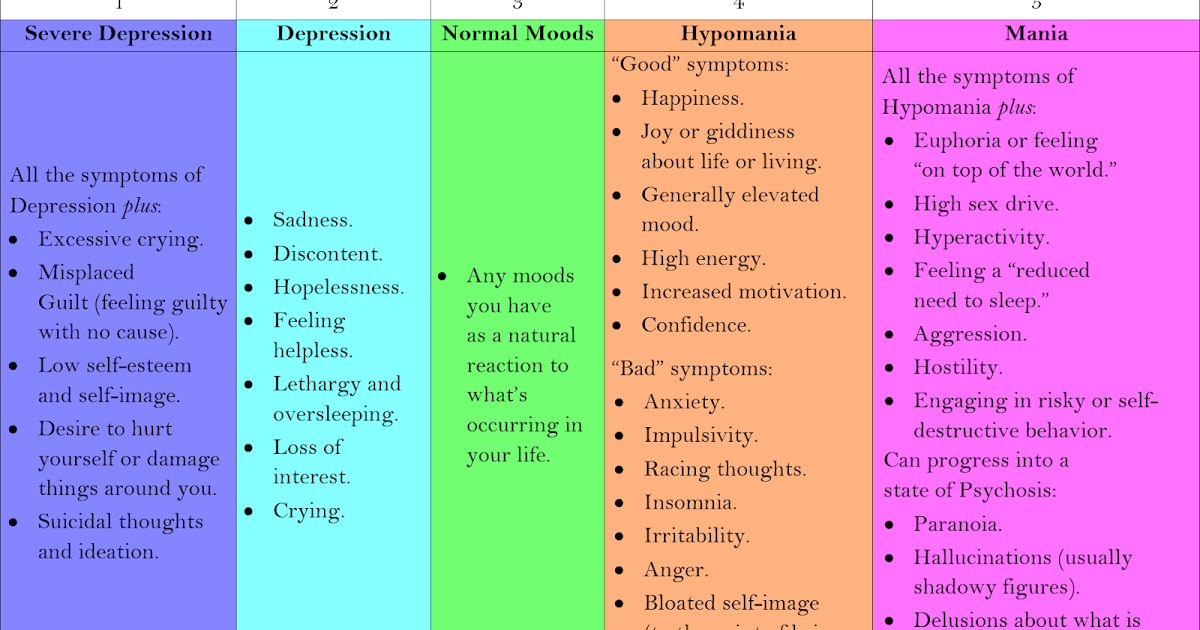
Bipolar disorder (once called manic depression) is a very serious condition that is marked by extreme — and sometimes violent — mood swings. Patients with bipolar disorder typically cycle back and forth between euphoric mania and debilitating depression, each lasting for weeks at a time. Bipolar has several subtypes, the most common of which are Bipolar I and Bipolar II, which is often misdiagnosed as depression. Around 70 percent of people with bipolar disorder also have ADHD.
Bipolar disorder is highly genetic, and usually comes on in the late teens or early adulthood. It affects approximately 2.6 percent of the U.S. population — or roughly 5.7 million Americans. It’s found across all genders, races, ethnic groups, and income levels, and it is sometimes mistaken for ADHD.
If you suffer from exaggerated psychological highs and lows, you may have bipolar disorder. Take this bipolar disorder test and then bring the results to a mental health professional for evaluation.
Adapted from the Goldberg Bipolar Spectrum Screening questionnaire (c. 1993) designed to screen for the possibility of bipolar spectrum disorders in individuals 18 or older who have already experienced at least one episode of depression. If you answer Yes to a significant number of these questions, consult a licensed mental health practitioner. An accurate diagnosis can only be made through clinical evaluation.
Do you vacillate between desires to be very social and to just be left alone?
Very Often
Often
Sometimes
Rarely
Never
Do you go through periods of great sadness, as well as periods of euphoria where you find almost anything funny?
Very Often
Often
Sometimes
Rarely
Never
Does your self-confidence seem to swing wildly from great self-doubt to great arrogance?
Very Often
Often
Sometimes
Rarely
Never
Do you experience some periods of mental slowness that alternate with periods of immensely creative thinking?
Very Often
Often
Sometimes
Rarely
Never
Do you occasionally feel extremely angry or hostile, for what seems like no reason?
Very Often
Often
Sometimes
Rarely
Never
Do you feel both high (overly happy) and low (depressed) at the same time?
Very Often
Often
Sometimes
Rarely
Never
Do you go through periods of great optimism and other periods of great pessimism?
Very Often
Often
Sometimes
Rarely
Never
Do you experience moods where you feel very revved up or agitated?
Very Often
Often
Sometimes
Rarely
Never
Do you occasionally become much more interested in sex than usual?
Very Often
Often
Sometimes
Rarely
Never
Do you become unusually talkative or overly gregarious, even in situations that may not warrant it?
Very Often
Often
Sometimes
Rarely
Never
Do you act uncharacteristically active and surprisingly outgoing?
Very Often
Often
Sometimes
Rarely
Never
Professionally, have you noticed a wide gap in the quantity or quality of your work — where you’re dramatically productive at times, but virtually useless at others?
Very Often
Often
Sometimes
Rarely
Never
(Optional) Would you like to receive your bipolar disorder symptom test results — plus more helpful resources — via email from ADDitude?
Sign me up for your Adult ADHD newsletter.
Can’t see the self-test questions above? Click here to open this test in a new window.
Bipolar Disorder in Adults: Next Steps
1. Take this Test: Full ADHD Symptom Test for Adults
2. Learn Where ADHD and Bipolar Disorder Overlap
3. Take This Test: Do You Have Rejection Sensitive Dysphoria?
4. Take This Test: Do You Have Emotional Hyperarousal?
5. Listen to the Webinar “How Bipolar Disorder Looks A Lot Like ADHD: Detection & Treatment of a Misunderstood Condition,” with Roberto Olivardia, Ph.D.
6. Download Is it Bipolar or ADHD? Solving the Puzzle
7. Find: Specialists or Clinics Near You
Previous Article Next Article
How to Tell the Difference
When a child is diagnosed with attention-deficit hyperactivity disorder (ADHD), they may be at risk for developing other mental health-related disorders in adulthood. These can include anxiety disorders, major depression, and bipolar disorder.¹
These can include anxiety disorders, major depression, and bipolar disorder.¹
While researchers have much to learn about the neurobiological interaction between the two disorders, a 2020 meta analysis of 71 studies (with nearly 650,000 participants from 18 countries) found that 1 in 13 adults with ADHD was also diagnosed with bipolar and nearly one in six adults with bipolar had ADHD.²
ADHD is a neurological condition; bipolar is a mood-based disorder. Many people with bipolar disorder may find that even when their mood is stabilized with the right medication and treatment, they still struggle to meet deadlines, keep their focus on a task, and stay organized.
Often, they mentally beat themselves up for not being motivated enough to change their behaviors. In these cases, ADHD may be the culprit, and by seeking treatment for both disorders, they can gain better control over their thoughts, emotions, and behaviors as well as improve their personal lives.
Adult ADHD Symptoms
ADHD symptoms may include the following:
Trouble focusing on a task
Feelings of restlessness
Organization problems
Feeling easily frustrated
Poor time management
Impulsive decision-making
Poor coping skills for stress
Adult Bipolar Symptoms
Bipolar symptoms can include manic, hypomanic, and/or depressive episodes. ³
³
Manic episode symptoms are as follows:
Decreased need for sleep
Talkativeness
Racing thoughts
Distractibility
Increase in goal-related activity (i.e. excessive spending)
Inflated sense of self
Risky behaviors (i.e. sexual, financial)
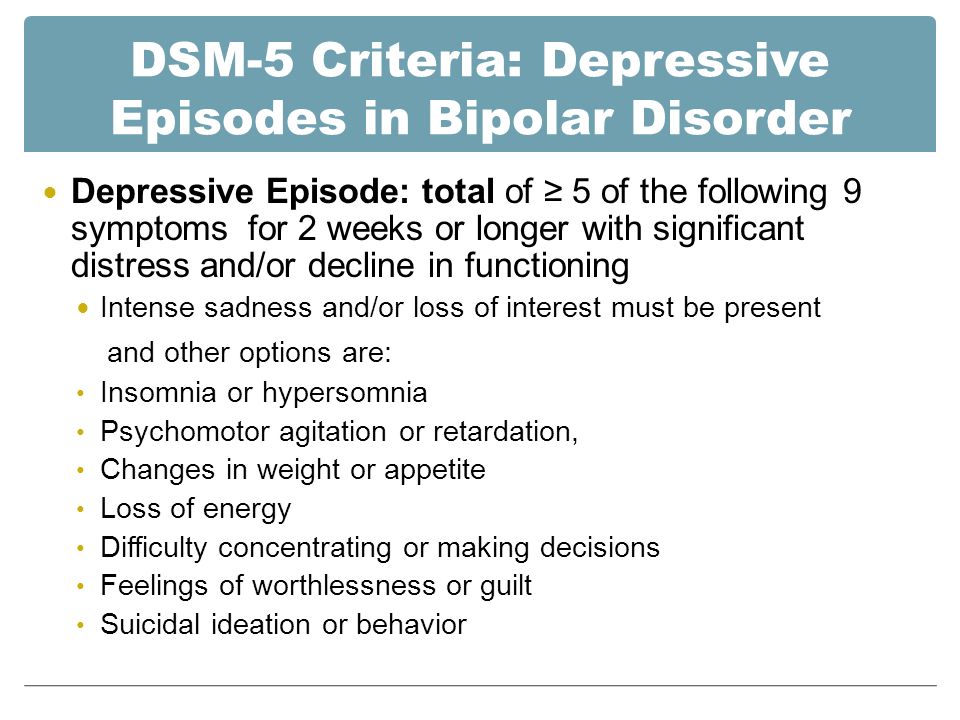
Depressive episode symptoms include:
Depressed mood
Lack of interest or pleasure in activities
Sleeping too little or too much
Changes in weight
Feelings of guilt or worthlessness
Trouble concentrating
Thoughts of suicide
How to Get the Right Diagnosis
Distinguishing between ADHD and bipolar disorder—or determining whether you might have both—can be challenging. Many of the symptoms of a manic bipolar episode and ADHD may be similar, such as distractibility, restlessness, or impulsivity. So ADHD may go undiagnosed in a person with bipolar disorder, if a doctor mistakes ADHD symptoms for a manic episode.
So ADHD may go undiagnosed in a person with bipolar disorder, if a doctor mistakes ADHD symptoms for a manic episode.
Doctors may use several criteria to determine the difference between ADHD and bipolar disorder or assess whether the disorders are co-occurring. Age of onset may be an indication that ADHD is present.Today, ADHD is considereda life-long condition—with symptoms often appearing at an early age—and while we know that children can have bipolar, it is unusual. According to NAMI, the National Alliance on Mental Illness, the average age of onset for bipolar disorder is about 25.⁴
If a person has been diagnosed with bipolar disorder, they may also have ADHD if the symptoms of ADHD continue in the absence of a depressive, manic, or hypomanic episode.⁵
But if symptoms like impulsivity, distractibility, and restlessness are cyclical, and there is an increase in goal-directed activity (behavior characterized by actions that illicit particular outcomes like travel or promiscuity), an inflated sense of self, and a decreased need for sleep, then a person may be experiencing a manic or hypomanic episode rather than (or in addition to) ADHD. ⁶
⁶
To assist in diagnosing ADHD in addition to bipolar disorder, here are some questions your doctor may ask:
Have you experienced symptoms of hyperactivity, impulsivity, or inattention since childhood?
Do you currently struggle with inattention or impulsivity when your mood is otherwise stable?
Are there other environmental stressors that might contribute to these symptoms?
Are there other medical or psychiatric conditions that might contribute to these symptoms?
Have symptoms interfered with your work, relationships, or other daily functioning?
In order to accurately diagnose ADHD and/or bipolar disorder, your doctor will need to rule out other potential diagnoses that may cause symptoms. These can include sleep disorders, head injury, other physical illness, anxiety disorders, major depression, personality disorders, the effects of medication, and the effects of substance use.⁷ They may also need to rule out environmental and situational stressors that can produce symptoms (i.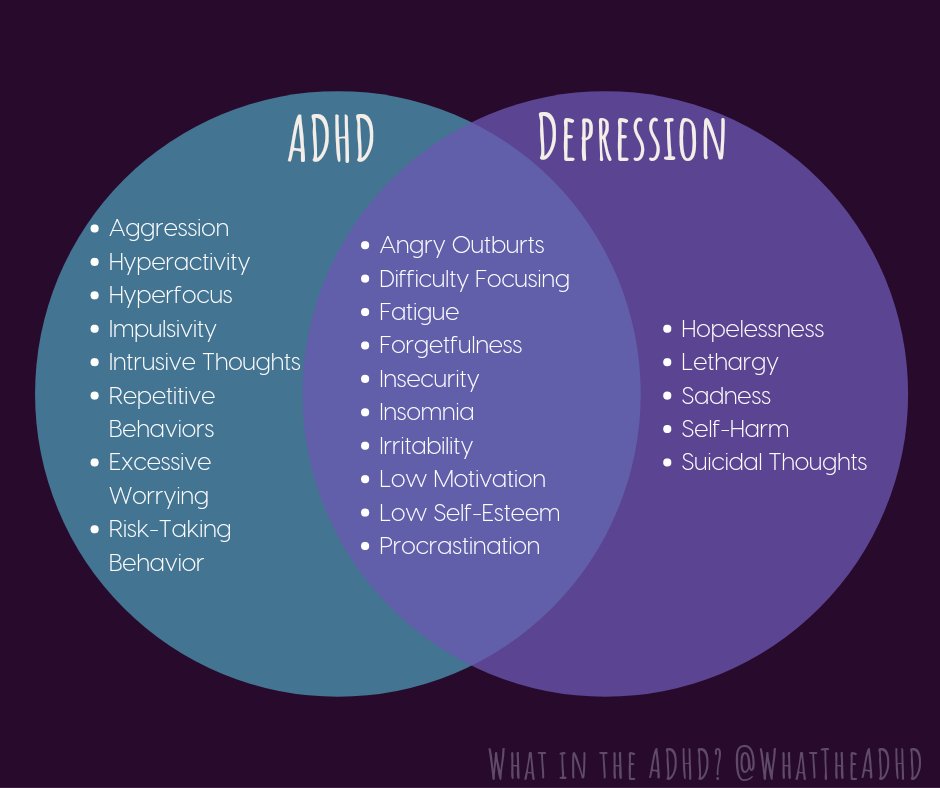 e. the impact of a life-changing circumstance such as a divorce, loss of a loved one, or financial stress.)
e. the impact of a life-changing circumstance such as a divorce, loss of a loved one, or financial stress.)
Comorbidity of ADHD and Adult Bipolar Disorder
As stated previously,² scientists do not completely understand why the illnesses often occur together, but some studies suggest that genetics may play a role, as well as the fact that both illnesses affect parts of the brain that control emotional regulation, executive functioning, and attention.⁷
Children with ADHD and Bipolar Disorder
Although symptoms of bipolar disorder typically don’t emerge until early adulthood, children can receive a diagnosis. A child with both ADHD and bipolar disorder will have behavioral outbursts, experience severe mood swings, and act impulsively.
If your child with ADHD exhibits an inflated sense of self, demonstrates risky sexual behavior, engages in self-harm, and has little need for sleep, then he or she also may be experiencing mania associated with bipolar disorder.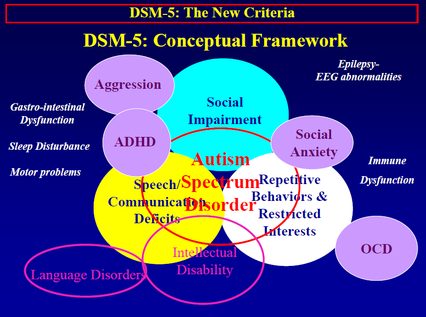 ² A child psychiatrist can help rule out other diagnoses and suggest treatment options.
² A child psychiatrist can help rule out other diagnoses and suggest treatment options.
Treatment Considerations
A co-occurring diagnosis of ADHD and bipolar disorder can put people at higher risk for substance use, relationship problems, suicidal behaviors, and legal problems.⁸ Therefore, early and comprehensive treatment is essential for healthy functioning. Because the effects of bipolar disorder are more severe if left untreated, treatment considerations typically involve stabilizing your mood before treating the symptoms of ADHD. This often involves a combination of medication, therapy, and education—especially about the dangers of substance use (people with ADHD and bipolar disorder are at much higher risk for a substance use disorder).
Because roughly 65% of people with ADHD and bipolar disorder will experience an anxiety disorder in their lifetime, a doctor or mental health professional may recommend treatment for anxiety as well.⁹ Researchers don’t completely understand the effects of stimulants on bipolar disorder, but some studies show that stimulants used to treat ADHD can increase anxiety or agitation and induce mania. ¹⁰
¹⁰
Medications that treat bipolar disorder, however, are unlikely to exacerbate the symptoms of ADHD.¹¹ Talk to your doctor about the risks and benefits and what signs and symptoms you should report immediately when taking medication.
Treatment Outlook for People With ADHD and Bipolar Disorder
Data on the treatment of people with ADHD and bipolar disorder is very limited. Receiving an accurate diagnosis is a key part of successful treatment, as ADHD in many adults goes undiagnosed. People with ADHD and bipolar disorder may also be at increased risk of suicide—one study found that adolescents with a comorbid diagnosis were twice as likely to commit suicide than adolescents with bipolar disorder alone.¹² This is why diagnosing and treating both disorders is so important.
Clinicians and researchers also still debate whether stimulant medications used to treat ADHD can trigger manic episodes in people with bipolar disorder and ADHD, or whether they can be an effective and safe part of treatment. ¹³ This is why working with a psychiatrist who has experiencing treating both disorders is essential.
¹³ This is why working with a psychiatrist who has experiencing treating both disorders is essential.
Because bipolar disorder operates in cycles, it may take months or longer to determine the most effective pharmacological response. But if a person is taking medication as subscribed, checking in with their doctor, avoiding illegal drugs or alcohol, getting the therapeutic support they need, and building a strong support network, they are giving themselves the opportunity to live a full life.
If you think you might have a diagnosis of ADHD in addition to bipolar disorder, make an appointment with your doctor to talk about your concerns. They may refer you to a mental health professional for a more thorough assessment. It’s important to remember that your symptoms are not a failure on your part, so don’t be afraid to speak up about your struggles.
The more accurately you can report signs and symptoms, the greater chance you have of treating them. Seeking treatment greatly increases your odds of thriving in the midst of life’s challenges, so consider what steps you can take today to get the right information and the best support.
- Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry. 2017;17(1):302. Published 2017 Aug 22. doi:10.1186/s12888-017-1463-3
- Schiweck C, Arteaga-Henriquez G, Aichholzer M, et al. Comorbidity of ADHD and adult bipolar disorder: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2021;124:100-123. doi:10.1016/j.neubiorev.2021.01.017
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: 2013.
- National Alliance on Mental Illness. Bipolar Disorder. Reviewed August 2017. Available at https://www.nami.org/About-Mental-Illness/Mental-Health-Conditions/Bipolar-Disorder#:~:text=The%20average%20age%2Dof%2Donset,of%20cases%20classified%20as%20severe. Accessed December 6, 2022.
- Med J Aust 2010; 193 (4): S18. || doi: 10.5694/j.1326-5377.2010.
 tb03892.x Published online: 16 August 2010.
tb03892.x Published online: 16 August 2010. - Duffy A. American Journal of Psychiatry. The Nature of the Association Between Childhood ADHD and the Development of Bipolar Disorder: A Review of Prospective High-Risk Studies. Published online December 2, 2012. Available at https://doi.org/10.1176/appi.ajp.2012.11111725 Accessed December 6, 2022.
- Trollor JN. Attention deficit hyperactivity disorder in adults: conceptual and clinical issues. Med J Aust. 1999;171(8):421-425. doi:10.5694/j.1326-5377.1999.tb123723.x
- American Academy of Pediatrics. ADHD and Bipolar. Available at https://www.healthychildren.org/English/health-issues/conditions/adhd/Pages/Mood-Disorders-ADHD.aspx Accessed December 6, 2022.
- Klassen LJ, Katzman MA, Chokka P. Adult ADHD and its comorbidities, with a focus on bipolar disorder. J Affect Disord. 2010;124(1-2):1-8. doi:10.1016/j.jad.2009.06.036 10.Kaustav Chakraborty and Sandeep Grover. Methylphenidate-induced mania-like symptoms.
 Indian J Pharmacol. 2011 Feb; 43(1): 80–81. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3062130/ 11.Gleason A, Castle D. Adult attention-deficit hyperactivity disorder and bipolar disorder. Advances in Psychiatric Treatment. 2012;18(3):198-204. doi:10.1192/apt.bp.110.008508
Indian J Pharmacol. 2011 Feb; 43(1): 80–81. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3062130/ 11.Gleason A, Castle D. Adult attention-deficit hyperactivity disorder and bipolar disorder. Advances in Psychiatric Treatment. 2012;18(3):198-204. doi:10.1192/apt.bp.110.008508 - Wen-Hsuan Lan, Ya-Mei Bai, Ju-Wei Hsu, Kai-Lin Huang, Tung-Ping Su, Cheng-Ta Li, Albert C. Yang, Wei-Chen Lin, Wen-Han Chang, Tzeng-Ji Chen, Shih-Jen Tsai, Mu-Hong Chen, Comorbidity of ADHD and suicide attempts among adolescents and young adults with bipolar disorder: A nationwide longitudinal study, Journal of Affective Disorders. Available at https://doi.org/10.1016/j.jad.2015.02.007.
- American Journal of Psychiatry. Available at https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2016.16040467 Accessed December 6, 2022.
Notes: This article was originally published October 17, 2017 and most recently updated December 6, 2022.
Attention-Deficit/Hyperactivity Disorder (ADHD), abbr.
 ADHD, is a neurological-behavioral developmental disorder that begins in childhood. Manifested by symptoms such as difficulty concentrating, hyperactivity and poorly controlled impulsivity.
ADHD, is a neurological-behavioral developmental disorder that begins in childhood. Manifested by symptoms such as difficulty concentrating, hyperactivity and poorly controlled impulsivity. ADHD was first described by Dr. Heinrich Hoffman in 1845. At 1902 Sir George F. Still published a series of lectures for the Royal College of Physicians in England describing a group of impulsive children with significant behavioral problems related to genetic dysfunction rather than poor parenting
ADHD more common in boys. The relative prevalence among boys and girls ranges from 3:1 to 9:1, depending on the criteria for diagnosis, study methods, and study groups (children who were referred to a doctor; schoolchildren; the general population). The estimates of the prevalence of ADHD also depend on these factors (from 1-2% to 25-30%). According to some data, the prevalence of the syndrome among younger schoolchildren is about 10-15%, in boys it occurred 2.8-3 times more often than in girls.
Clinic
The main symptoms of ADHD are attention deficit, hyperactivity and impulsivity. These signs appear at a very early age. Since many healthy children also have these symptoms, but to a lesser extent, or caused by another disorder, it is important for the child to have a thorough examination and an appropriate diagnosis made by a highly qualified specialist.
Symptoms of ADHD appear over many months, usually symptoms of impulsivity and hyperactivity precede symptoms of inattention, which may not appear for a year or more. Different symptoms appear under different social conditions, depending on the requirements for self-control of the child in a particular situation. A child who "can't sit still" or who ruins everything is visible at school, but an inattentive dreamer may not be noticed. An impulsive child who acts first and thinks later may be thought to have "discipline problems", while a passive or slow child may simply be considered not very motivated. However, both can have different types of ADHD. All children are sometimes restless, sometimes they do something without thinking, sometimes they float away somewhere in their dreams. When hyperactivity, distractibility, poor concentration, or impulsivity begin to affect school performance, relationships with other children, or behavior at home, ADHD may be suspected in a child. Since symptoms vary greatly depending on social conditions, it is very difficult to diagnose ADHD. This is especially true in cases where attention deficit is the primary symptom.
However, both can have different types of ADHD. All children are sometimes restless, sometimes they do something without thinking, sometimes they float away somewhere in their dreams. When hyperactivity, distractibility, poor concentration, or impulsivity begin to affect school performance, relationships with other children, or behavior at home, ADHD may be suspected in a child. Since symptoms vary greatly depending on social conditions, it is very difficult to diagnose ADHD. This is especially true in cases where attention deficit is the primary symptom.
Hyperactive children seem to be constantly on the move and on their feet. They destroy everything around them, grabbing and playing with everything that catches their eye or talking incessantly. It turns out to be a difficult task for them to sit quietly at the table during lunch and school lesson or to communicate calmly. They squirm and squirm in their chairs, or roam the room. Or they wiggle their feet, touch everything, tap loudly with a pencil. Hyperactive teenagers or adults feel inner anxiety. They often talk about how they need to be busy and may try to do several things at the same time.
Hyperactive teenagers or adults feel inner anxiety. They often talk about how they need to be busy and may try to do several things at the same time.
Impulsive children cannot control their immediate reaction or think before doing something. They often blurt out inappropriate comments, show their emotions uncontrollably, and act without considering the consequences of their behavior. Their impulsiveness prevents them from waiting for something they want or their turn in the game. They may take a toy from another child or hit if they are upset. Even teenagers or adults impulsively choose activities that bring even a small but immediate return, instead of doing something that requires a lot of effort, but also provides a much larger reward - but later.
Diagnostic criteria
The main diagnostic criteria include
- Inappropriate for age characteristics and indicating insufficient adaptation
- attention disorders
- hyperactivity and impulsivity
2. The first symptoms develop before the age of 7 years
The first symptoms develop before the age of 7 years
3. The symptoms persist continuously for 6 months in such a degree that indicates a poor adaptation of the child.
4. Insufficient adaptation manifests itself in various situations (at home, at school) despite the level of intellectual development corresponding to normal age indicators , increased motor activity, vegetative reactions, sleep disturbances, eating disorders, gastrointestinal disorders)
Stages of development in ADHD
Up to a year - increased neuro-reflex excitability syndrome (anxiety, unreasonable cry, increased motor activity, vegetative reactions, sleep disturbances, eating disorders, gastrointestinal disorders)
From a year to 3 years - increased excitability, motor restlessness, motor awkwardness, speech development disorders, sleep disorders, enuresis, encopresis
Preschool age - 3 to 7 years old. symptoms of hyperactivity and impulsivity are mainly manifested. Many lag behind their peers in the development of speech and motor skills.
School age - from 8 to 13 years, the formation of school maladjustment and difficulties in establishing relationships with peers. Often there are simple social phobias, irascibility, aggressive behavior. Weak psycho-emotional stability and low self-esteem. Hyperactivity subsides after age 9, but impulsivity and attention deficits remain.
Hyperactivity subsides after age 9, but impulsivity and attention deficits remain.
Adolescence - 14 to 18 school failure, difficulty completing long tasks, lack of autonomy, unable to work unaided, reckless, risk-taking behavior, poor peer relationships, difficulty following rules of conduct, subservience to social norms and laws
Adult age - from 19 years old - not organized, does not have sufficient planning skills, forgetful, absent-minded, often loses things. Difficulties with initiative and completion of work on various tasks, poor time planning for their activities, frequent job changes, difficulties in family life, difficulties with long-term maintenance of attention remain. Poorly tolerates negative emotions, disappointments.
Disorders sometimes associated with ADHD
Learning difficulties. Many children with ADHD, approximately 20-30 percent, also have specific learning difficulties. At preschool age, these problems consist of not understanding certain sounds or words, and/or they find it difficult to express their opinions in words. At school age, problems with reading, spelling, writing and arithmetic may appear. A common type of reading disorder is dyslexia. Almost 8% of primary school children have reading problems.
At school age, problems with reading, spelling, writing and arithmetic may appear. A common type of reading disorder is dyslexia. Almost 8% of primary school children have reading problems.
Gilles de la Tourette syndrome. A very small percentage of people with ADHD have a neurological disease called Gilles de la Tourette syndrome. People with this syndrome suffer from various nervous tics and repetitive actions, including blinking, facial tics, or grimacing. Others may repeatedly cough, snort, sniff, or yell swear words. This behavior can be controlled with medication. Although very few children suffer from Gilles de la Tourette syndrome, many children who do have it are associated with ADHD. In such cases, drugs are needed to treat both conditions.
Oppositional defiant disorder. One-third to one-half of all children with ADHD—mostly boys—have another disorder known as oppositional defiant disorder (ODD). Such children are usually impudent, stubborn, intractable, they are characterized by outbursts of anger or aggression. They argue with adults and refuse to obey.
They argue with adults and refuse to obey.
Conduct disorder. Approximately 20-40% of children with ADHD develop a conduct disorder, a more severe antisocial behavior, over time. These children often lie or steal, fight or bully others, and are more likely to have problems at school or with the police. They violate the fundamental rights of others, are aggressive towards other people or animals, destroy private property, break into people's homes, commit theft, carry or use weapons, or engage in vandalism. These children or teenagers are more likely to try drugs and then become addicted. They urgently need help.
Anxiety and depression. Some children with ADHD often have comorbid anxiety or depression. If anxiety or depression is diagnosed and treated, the child may be better able to control the problems associated with ADHD. Conversely, effective ADHD treatment may have a positive effect on anxiety, as the child is able to perform better in school.
Bipolar disorder. There are no accurate statistics on how many children with ADHD have bipolar disorder. In childhood, it is very difficult to distinguish between ADHD and bipolar disorder. In its classic form, bipolar disorder is characterized by alternating periods of good and bad mood. But it seems that children with bipolar disorder are more likely to have chronic mood dysregulation combined with euphoria, depression, and irritability. In addition, there are several symptoms that are common to both ADHD and bipolar disorder, such as increased activity and reduced need for sleep. The symptoms that differentiate ADHD from bipolar disorder are the elation and flatulence of a child with bipolar disorder.
There are no accurate statistics on how many children with ADHD have bipolar disorder. In childhood, it is very difficult to distinguish between ADHD and bipolar disorder. In its classic form, bipolar disorder is characterized by alternating periods of good and bad mood. But it seems that children with bipolar disorder are more likely to have chronic mood dysregulation combined with euphoria, depression, and irritability. In addition, there are several symptoms that are common to both ADHD and bipolar disorder, such as increased activity and reduced need for sleep. The symptoms that differentiate ADHD from bipolar disorder are the elation and flatulence of a child with bipolar disorder.
Treatment
Treatment and management of ADHD and available methods may differ from country to country. However, despite these differences, most experts consider the most effective integrated approach, which combines several methods, individually selected in each case. Methods are used: behavior modification, psychotherapy, pedagogical and neuropsychological correction.
Drug therapy is indicated on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug methods alone.
Neuropsychological method. When, with the help of various exercises, we return to the previous stages of ontogenesis and rebuild those functions that were formed archaically incorrectly and have already been fixed. To do this, they need, like any other ineffective pathological skill, to purposefully reveal, disinhibit, destroy and create a new skill that is more consistent with effective work. And this is carried out on all three floors of mental activity. This is a laborious, multi-month job. The child is born 9months. And neuropsychological correction is designed for this period. And then the brain begins to work more efficiently, with less energy costs. Old archaic connections, relations between the hemispheres are normalizing. Energy, management, active attention are built.
The syndromic method is that the child is given an interesting activity (voluntary).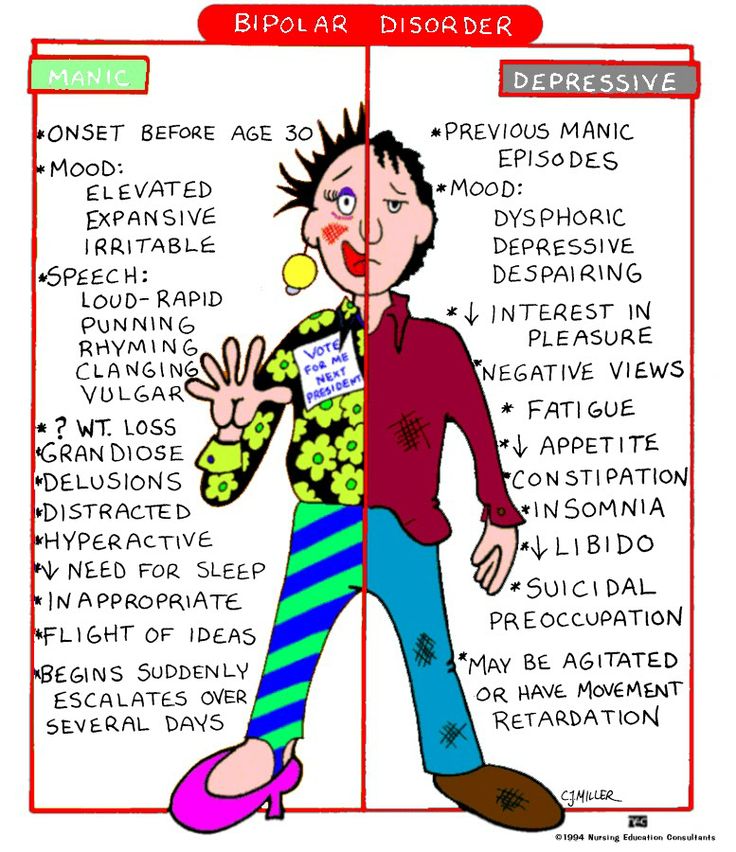 But in this activity there is post-voluntary attention (when we become interested in something and delved into it, we already strain without additional costs). Therefore, when they say that children with ADHD are able to sit at the computer for a very long time, then this is a completely different attention.
But in this activity there is post-voluntary attention (when we become interested in something and delved into it, we already strain without additional costs). Therefore, when they say that children with ADHD are able to sit at the computer for a very long time, then this is a completely different attention.
There are outdoor games that require only attention. The child moves according to the conditions of the game, he can be explosive, impulsive. This may help him win. But the game is about attention. This function is being trained. Then the restraint function is trained. However, he can be distracted. Each task is solved as it arrives. This improves each feature individually.
Behavioral or behavioral psychotherapy focuses on certain behavioral patterns, either shaping or extinguishing them through reward, punishment, coercion and inspiration.
Work on personality. Family psychotherapy, which forms the personality and which determines where to direct these qualities (disinhibition, aggressiveness, increased activity).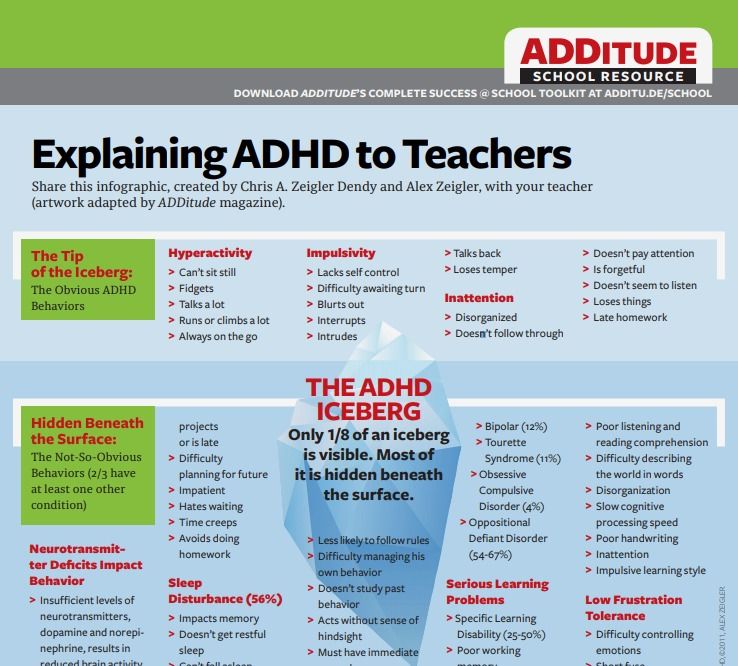
Formacological methods
In the treatment of ADHD, drugs are used as an auxiliary method. The best known of these are psychostimulants such as methylphenidate, dextroamphetamine with amphetamine, and dextroamphetamine. One of the disadvantages of these drugs is the need to take them several times a day (the duration of action is about 4 hours). Currently, methylphenidate and dextroamphetamine with long-acting amphetamines (up to 12 hours) have appeared. Other groups of drugs are also used, for example, atomoxetine.
The approach common in Russia and the CIS countries is nootropic drugs, substances that improve brain function, metabolism, energy, increase the tone of the cortex. Also prescribed drugs, consisting of amino acids, which improve the metabolism of the brain. However, there is currently no conclusive evidence for the effectiveness of such treatment.
VR game helped to identify ADHD in children
To do this, scientists observed eye movements while children coped with everyday tasks
Scientists invited children with ADHD to play a VR game to watch how their eyes move.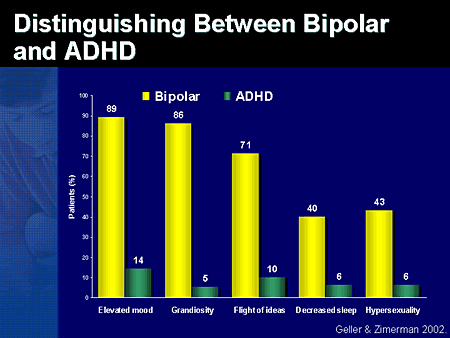 It turned out that there are differences in the eye movement of children with the syndrome and those with neurotypical development when they need to focus on everyday tasks or targets. The researchers hope that this technology will help diagnose ADHD more accurately than classical methods. The results of the study are published in Scientific Reports .
It turned out that there are differences in the eye movement of children with the syndrome and those with neurotypical development when they need to focus on everyday tasks or targets. The researchers hope that this technology will help diagnose ADHD more accurately than classical methods. The results of the study are published in Scientific Reports .
People with ADHD find it difficult to focus even on simple everyday tasks and are often distracted. Usually, in order to make this diagnosis, experts evaluate inattention, impulsivity and hyperactivity based on interviews, questionnaires or clinical observations - but all of these are often subject to subjective distortions. Therefore, doctors are still arguing about whether it is possible to find any quantitative markers to objectively diagnose ADHD.
For example, the eye movement of a person with ADHD can serve as such a marker. Previous research has confirmed that people with ADHD suffer from attention deficit disorder. They are worse at suppressing saccades (the rapid eye movements that allow us to scan the visual environment), so their eye movements are less accurate in relation to the target. It is also more difficult for such people to fixate on the target object: they more easily pay attention to strong stimuli. Therefore, one of the signs of ADHD in children can be the number and duration of fixation on bright objects that children are distracted by during tasks.
They are worse at suppressing saccades (the rapid eye movements that allow us to scan the visual environment), so their eye movements are less accurate in relation to the target. It is also more difficult for such people to fixate on the target object: they more easily pay attention to strong stimuli. Therefore, one of the signs of ADHD in children can be the number and duration of fixation on bright objects that children are distracted by during tasks.
Liya Merzon from Aalto University (Finland), together with colleagues from Finland, Great Britain and France, decided to study the eye movements of children who play the game in virtual reality. In a previous study, scientists have already noticed that children often perform irrelevant actions when solving problems and, as a result, complete fewer tasks. They hoped to confirm these results with data collected about eye movement.
The study involved 37 children with ADHD and a control group of 36 children with neurotypical development (9-13 years old).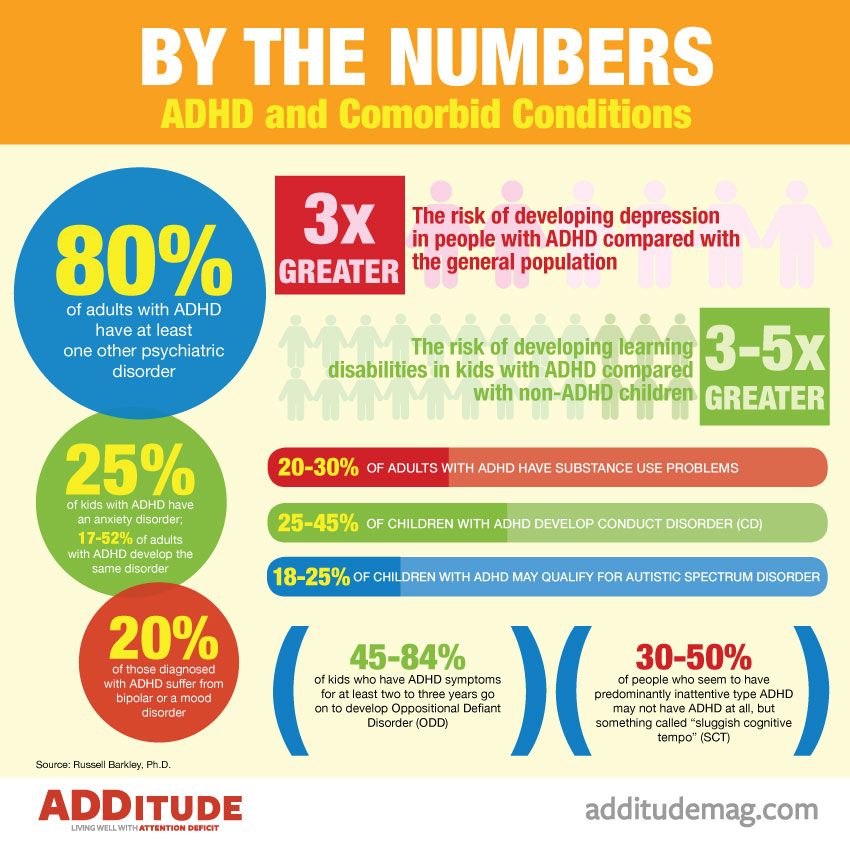 They had to go through two games and complete a number of tasks in them.
They had to go through two games and complete a number of tasks in them.
The first game, EPELI, simulated the real environment and real everyday tasks. It had 13 different scenarios to complete (for example, morning chores or returning from school), which consisted of four to six subtasks (for example, wash your hands, put your backpack back). Before each task, the dragon character gave the children instructions on all subtasks. The play environment simulated an apartment with a child's bedroom, a kitchen, a living room, a parent's bedroom, and a bathroom. Participants wore VR glasses and had to move around the virtual apartment and interact with objects using a controller. At the same time, there were 47 necessary items in the apartment and 243 more - irrelevant, distracting.
Based on the results of the game, scientists calculated various indicators, for example, the overall score based on the results of successfully completed tasks, the number of controller movements, and others. In all respects, the groups differed from each other: children with ADHD completed fewer subtasks, and their navigation was less efficient. On the other hand, they performed more controller movements (p = 0.0085) and actions in general (p = 0.0048) than the control group.
In all respects, the groups differed from each other: children with ADHD completed fewer subtasks, and their navigation was less efficient. On the other hand, they performed more controller movements (p = 0.0085) and actions in general (p = 0.0048) than the control group.
Participants with ADHD also had shorter saccades (average 57 ms versus 67 ms in the control group) with lower amplitude (average 5.44 degrees versus 6.29degrees at the control) in all tasks in the game. At the same time, the nature of eye movements differed between groups throughout the game and did not depend on specific scenarios or features of the stimulus.
An example of completing tasks in EPELI The researchers also found that children with different duration fix their eyes on relevant and irrelevant objects during tasks. But even taking into account the fact that children with ADHD kept their eyes on distracting objects longer compared to the control group, this effect did not reach a significant level (p = 0.060).
But even taking into account the fact that children with ADHD kept their eyes on distracting objects longer compared to the control group, this effect did not reach a significant level (p = 0.060).
In the second game, Shoot the Target, children had to find targets in virtual space and shoot them by looking at the object. Children with ADHD coped worse with these tasks than participants in the control group (p = 0.0018), but scientists did not record differences in movements and their speed between groups. Just like in the previous game, the scientists noticed longer fixation, shorter saccades, and lower amplitude in children with ADHD.
Thus, VR eye tracking has served as a reliable marker of attention deficit. The authors of the work believe that eye movement can be used to make a more accurate diagnosis. But they admit that it is still difficult to understand whether differences in eye movement are a cause or effect. Perhaps participants with ADHD perform worse on tasks because they have difficulty with visual attention.