Anger panic attack
Relationship of Anxiety and Anger
Anxiety is tightly linked to worry and fear that is out of the ordinary for everyday triggers. Many individuals with an anxiety disorder will often be quick to anger; however, the link between anger and anxiety is often missed or overlooked. Anxiety is often connected with overstimulation from a stressful environment or threat, combined with the perceived inability to deal with that threat. In contrast, anger is often tied to frustration. Often when anxiety is left unacknowledged and unexpressed, it can turn into frustration, which can lead to anger. When anxiety turns to anger, it is because an individual who expresses anger will have an underlying fear about something in their life. When individuals are scared or worried about something, they often choose anger, unconsciously, as a way to feel as though they are in control of their anxiety.
Unprocessed Anger
Anxiety not only presents as a pounding heart, shortness of breath, clammy skin, and racing thoughts, but anxiety can also present in more subtle ways such as anger or frustration. Individuals with undiagnosed anxiety may find themselves lashing out and becoming frustrated over everyday occurrences that usually do not warrant an emotional reaction.
Road rage is a perfect example of this. Traffic and crowds are often triggers of anxiety, which can result in becoming angry with people on the road. Maybe they are going to be late for work, are in a bad mood, or have a stressful deadline looming ahead. Sitting in traffic is only adding fuel to their fire. As a result, these people lash out at other cars when, in reality, they are anxious about the stressful environment and personal issues they have going on in their life.
Giving in to anger can ruin relationships and have adverse effects on every aspect of an individual’s life. It can lead to lashing out, making rash decisions, and engaging in risky behaviors.
When individuals feel threatened, their fight or flight response kicks in, and individuals go into defense mode, which sometimes means fighting.
Not all anger is linked to anxiety, but often if individuals take a step back and uncover what is triggering their anger, they may discover that they are showing signs of fear and panic, which may be the root of an anxiety disorder.
How Symptoms of Anxiety Can Trigger Anger
Individuals with anxiety usually have difficulty falling asleep or staying asleep and, as a result, may be sleep deprived. Over time, lack of sleep can trigger individuals to become more sensitive to small problems and, as a result, are quick to anger. Yelling at the dog for barking, becoming angry in traffic, getting upset because of a long line at the grocery store, or lashing out over an honest mistake are all small triggers that turn into monumental challenges for an individual who is struggling with anxiety and is sleep-deprived. Anger does not have to be intentional, and with individuals who have an anxiety disorder, this anger is often an automatic reaction to an anxious trigger or the effects of long-standing anxiety.
Individuals who have an anxiety disorder are often rigid in their daily routines since the fear of the unknown is often a trigger for their anxiety. When something disrupts their daily routine, it is not uncommon for the individual to not know how to cope with the change and, as a result, lash out in anger.
Seeking Help For Anger and Anxiety
Anxiety and anger can be a toxic combination. Seeking treatment for the anxiety disorder can help an individual uncover the reasons for their anger. Being mindful about anger outbursts by keeping a journal and taking time to reflect on why this anger occurred can often help individuals realize their anxiety triggers, and then seek therapy to find healthy ways to cope with them. If you or a loved one are in search of treatment for anxiety, please contact Discovery Mood & Anxiety Programs or fill out our mental health evaluation.
Kristen Fuller, M.D., is a clinical content writer and enjoys writing about evidence-based topics in the cutting-edge world of mental health and addiction medicine. She is a family medicine physician and author, who also teaches and contributes to medicine board education. Her passion lies within educating the public on preventable diseases including mental health disorders and the stigma associated with them. She is also an outdoor activist and spends most of her free time empowering other women to get outside into the backcountry.
She is a family medicine physician and author, who also teaches and contributes to medicine board education. Her passion lies within educating the public on preventable diseases including mental health disorders and the stigma associated with them. She is also an outdoor activist and spends most of her free time empowering other women to get outside into the backcountry.
Rage Attacks | Cedars-Sinai
ABOUT DIAGNOSIS TREATMENT
Overview
Rage attacks are sudden, out-of-control bursts of anger. These explosive outbursts can start without warning. They may also seem to be out of proportion to what triggered the episode.
Rage attacks are different than tantrums. Tantrums are goal-oriented with the intent of getting an observer to do what the person wants. Rage attacks are more about the release of pent up tension than about achieving a specific goal.
In the past, rage attacks were thought to be related to epilepsy or Tourette syndrome. This is now understood to be false.
This is now understood to be false.
Symptoms
Rage attacks may seem to begin without warning. However, little signs may be seen, including:
- Increased stressed
- Increased agitation
- Anxiety
When a rage attack happens, symptoms may include:
- Yelling or shouting
- Intense anger
- Physical aggression
Causes and Risk Factors
Rage attacks are sometimes incorrectly linked with epilepsy or Tourette syndrome. In very rare cases, limbic seizures can be linked to out-of-control behavior. However, this is uncommon.
The cause of rage attacks is unknown.
Some children or teenagers may have rage attacks only at home and not at school. Others may have the attacks at school.
Rage attacks can be triggered by stressors such as:
- Social pressure
- School work
Diagnosis
If the patient has symptoms similar to a seizure, the doctor will often test the patient for epilepsy. The most useful test in confirming epilepsy is an electroencephalogram (EEG). This test records electrical activity in the brain. It can show abnormal spikes or waves in electrical activity patterns. Different types of epilepsy can be identified with these patterns.
The most useful test in confirming epilepsy is an electroencephalogram (EEG). This test records electrical activity in the brain. It can show abnormal spikes or waves in electrical activity patterns. Different types of epilepsy can be identified with these patterns.
A patient with rage attacks that are unrelated to epilepsy will not show unusual electrical activity in the brain on the EEG.
Magnetic resonance imaging (MRI) and computed tomography (CT) scans may be used to look for epilepsy as well. However, these tests are not very helpful for rage attacks.
If the doctor suspects rage attacks, the patient will be referred to a psychologist for further diagnosis and treatment.
Treatment
Psychotherapy is the most common treatment for rage attacks. This may include cognitive behavioral therapy (CBT). CBT examines thoughts and their links to feelings and behaviors. CBT and other psychotherapies take several months to work. It is important that the patient continue their treatment plan during this time.
Rage attacks do not respond to anti-seizure medications. However, medications for depression or anxiety may be used as part of the treatment plan.
© 2000-2022 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare professional's instructions.
90,000 Anger and panic attacks. PsyMagThe topic of panic attacks, neurosis and VVD (vegetative-vascular dystonia) occupies a fairly large proportion of my professional and personal interests. I am trying to understand these processes from the perspective of neurophysiology, personality psychology, trauma therapy and cognitive behavioral therapy (CBT). This article was inspired by a colleague's statement that a panic attack is covert, unexpressed aggression. And as soon as the customers start punching the bag, everything returns to normal ...
I thought. Is there really such a direct connection?
The first point that confuses me in this statement is that aggression must be expressed. This opinion was formed thanks to Feshbach's "catharsis hypothesis" (the assumption that the tendency to aggression can be reduced by watching movies or programs with scenes of violence). The scientist tried to prove (and he seemed to succeed) that by experiencing anger when viewing such content, a person is freed from it and will be less aggressive in the future. This hypothesis, subsequently, was subjected to serious criticism and was refuted. But it cemented the folk wisdom or metaphor of the “boiling kettle”: “if you are angry - let off steam”, “pour out your anger to make it easier”, which has firmly entered the tools of fellow psychologists working with aggression. And the belief that punching a pear helps to remove aggression has become firmly established in everyday life. nine0003
This opinion was formed thanks to Feshbach's "catharsis hypothesis" (the assumption that the tendency to aggression can be reduced by watching movies or programs with scenes of violence). The scientist tried to prove (and he seemed to succeed) that by experiencing anger when viewing such content, a person is freed from it and will be less aggressive in the future. This hypothesis, subsequently, was subjected to serious criticism and was refuted. But it cemented the folk wisdom or metaphor of the “boiling kettle”: “if you are angry - let off steam”, “pour out your anger to make it easier”, which has firmly entered the tools of fellow psychologists working with aggression. And the belief that punching a pear helps to remove aggression has become firmly established in everyday life. nine0003
But it wasn't there!
The experiments of such scientists as C. Turner, D. Goldsmith, R. Green, R. Walters, M. Brown, B. Bushman, R. Baumeister and others since the 50s of the last century prove the opposite. If you express, splash out aggression, it does not decrease, but on the contrary, it increases.
If you express, splash out aggression, it does not decrease, but on the contrary, it increases.
This fact, perhaps, is worth fixing: if aggression is thrown out, it intensifies.
In principle, if we follow the statement that panic attacks are hidden, unexpressed aggression, then we get the following logical chain: if a person expresses hidden aggression, then it will grow, which means there will be more panic attacks. It turns out that either my colleague is mistaken, or everything is much more interesting. nine0003
Let's look at panic attacks from the standpoint of cognitive theory. If you try to rewind back to the moment when a person had the first panic attack, then often it will be associated with overwork, prolonged stress, a conflict situation, the use of stimulants (coffee, energy drinks, alcohol, etc.), excessive physical exertion. In the first episode of a panic attack, a person may experience a strong heartbeat, shortness of breath, sweating, and possibly numbness of the limbs. And then he will begin to analyze what is happening to him? In a situation of information deficiency, the brain will begin to throw up different versions and memories. And a person who is in a neurosis or with a neurotic personality will draw rather gloomy conclusions and catastrophize the situation, thereby increasing anxiety. Basically, the cause of a panic attack is a misinterpretation of the symptoms. And thanks to "mental chewing gum" and Google, you can find a lot of evidence for this interpretation and even make up a new, even more terrible one. Further, according to cognitivists, a person falls into a "vicious circle of anxiety" and panic attacks are already repeated, developing from a single case into a panic disorder. nine0003
And then he will begin to analyze what is happening to him? In a situation of information deficiency, the brain will begin to throw up different versions and memories. And a person who is in a neurosis or with a neurotic personality will draw rather gloomy conclusions and catastrophize the situation, thereby increasing anxiety. Basically, the cause of a panic attack is a misinterpretation of the symptoms. And thanks to "mental chewing gum" and Google, you can find a lot of evidence for this interpretation and even make up a new, even more terrible one. Further, according to cognitivists, a person falls into a "vicious circle of anxiety" and panic attacks are already repeated, developing from a single case into a panic disorder. nine0003
Therefore, a panic attack, in my opinion, is not about anger, but about fear. But fear is secondary. When a person is afraid and avoids places where a panic attack has occurred, he is afraid of loneliness, the death of loved ones or a serious illness.
Fear of fear itself.
Let's look at panic attacks from the position of neurophysiology and psychotherapy of trauma.
By nature, we have three main reactions to a life-threatening situation - “hit-run-freeze”. And these reactions are included in response to a strong fright. Adrenaline is released into the blood, the sympathetic nervous system is turned on, blood pressure rises, hyperventilation begins, blood rushes to the muscles - the body is ready to run or fight. nine0003
And the first trap into which the brain drives us is that we "freeze". There is no real threat. And since a panic attack is, in fact, a distorted interpretation of the symptoms, the threat is inside the person. And you can't run from yourself. So it turns out that the whole cocktail of hormones that stood out for fight or flight does not go anywhere. It accumulates. And this is an important point. In nature, if an animal froze in order to survive, it knows how to defuse the "cocktail of hormones" that has been released. It starts to tremble. Thus, the body relieves stress and "burns" hormones. When the process is completed, you can be glad that you are still alive. Hooray! nine0003
It starts to tremble. Thus, the body relieves stress and "burns" hormones. When the process is completed, you can be glad that you are still alive. Hooray! nine0003
But this is in animals...
What does a person do when he starts to tremble? That's right, trying to calm down, stop trembling. This only reinforces the belief that “something is wrong with him!”. Hormones and stress remain in the body. And the more often a person experiences panic attacks, the greater the concentration of stress hormones will be.
There is another puzzle in this picture. Vegetative-vascular dystonia. A disease that collects all the symptoms that cannot be explained. Therefore, it is increasingly viewed with skepticism. They say, “no matter how much you treat, you won’t cure”, “VSD - such a disease does not exist”, “VDS is put when they cannot determine the real diagnosis”, etc.
Let's understand a little. Of course, I'm not a doctor. But during my training, a lot of time was devoted to knowledge of the anatomy of the central nervous system and the physiology of higher nervous activity.
So, the basics.
Our nervous system is divided into central and peripheral. Within the framework of the topic, we are interested in the peripheral part. It is also divided into two "departments": the somatic nervous system and the autonomic. The somatic nervous system regulates what is under conscious control: coordination, movement, receiving external information. And vegetative - regulates those processes that a person does not consciously control. These are all processes that occur in the body on an ongoing basis (respiration, circulation, digestion, secretion of glands, etc.). nine0003
When the autonomic nervous system works smoothly, our body functions like a clock, all processes in it occur clearly and in a timely manner. But imbalance can lead to discomfort. To begin with, this system is also divided into two sections: the sympathetic and parasympathetic nervous system. The sympathetic system regulates processes in a state of activity, including stress and danger. It is she who causes all those changes in the state of the body that occur during a panic attack and which we have already described above. And the parasympathetic nervous system regulates processes at rest, when we rest, recover, digest and assimilate food. When it is active, we are in a blissful and relaxed state. We are safe. nine0003
It is she who causes all those changes in the state of the body that occur during a panic attack and which we have already described above. And the parasympathetic nervous system regulates processes at rest, when we rest, recover, digest and assimilate food. When it is active, we are in a blissful and relaxed state. We are safe. nine0003
And here's what's important: when one department is activated, the second one automatically reduces its activity.
Why all this? Moreover, with overwork and exhaustion of the nervous system, these departments are unbalanced. I will not now describe the deeper mechanisms at the cellular level, but it turns out that a person with an unbalanced autonomic nervous system, being in constant stress, lives in a state of constant readiness for war. This means that the “hit-run-freeze” reactions are always ready and can work at the most inopportune moment. nine0003
And here we will record the following important point: during a panic attack, a false start is triggered for the sympathetic nervous system, the body activates resources to implement the “fight or flight” reaction to the danger, but reacts by freezing.

The next puzzle in this picture is my understanding of the meaning and interaction of different emotions. In my mind, fear is more about freezing, and anger is more about action. The "freeze" response is pure fear. “I see the enemy. He is stronger and faster. Freeze to survive." But add a little anger to the fear and we get the “run” response. “I see the enemy. He's stronger, but I'm faster. Run to survive! And anger in its purest form is the “hit” response. And when anger is turned on, then there is no place for fear. It turns out that we can cope with fear with the help of anger. nine0003
Let's fix this: anger is a weapon against fear.
And here are my long-awaited conclusions for those who survived this long read.
Why can punching a punching bag work in dealing with panic attacks?
In my opinion, the mechanism is as follows. With these actions, we turn on the active position. We turn on anger and intensify it. It helps us overcome fear. Thus, we break the “vicious circle of anxiety”. And vigorous activity helps to burn a cocktail of stress hormones. Punching a pear, we turn on the “hit” reaction. But we do not necessarily need a pear, we can run away. I mean, go for a quick walk or jog. Maybe not during the panic attack itself, but right after. Well, ideally, make sports or feasible physical activity a permanent part of your lifestyle. nine0003
We turn on anger and intensify it. It helps us overcome fear. Thus, we break the “vicious circle of anxiety”. And vigorous activity helps to burn a cocktail of stress hormones. Punching a pear, we turn on the “hit” reaction. But we do not necessarily need a pear, we can run away. I mean, go for a quick walk or jog. Maybe not during the panic attack itself, but right after. Well, ideally, make sports or feasible physical activity a permanent part of your lifestyle. nine0003
Well, colleagues? How do you like the idea? Can we simulate an experiment to test this hypothesis?
Why panic attacks do not lead to insanity. — Berkana Center
The most common fears experienced during panic attacks are the fear of death, the fear of losing self-control and the fear of going crazy. Patients are often sure that some kind of catastrophe is happening in their body or psyche: myocardial infarction, stroke, schizophrenia. In reality, the content of thoughts during a panic attack is strictly subjective and obeys the laws of emotional logic, i. e. tendency to catastrophize. By the way, this explains the fact that between panic attacks the patient is completely rational, understands that no one died from panic attacks or went crazy, that a panic attack is a kind of training for the body, but during an anxiety attack all these protective statements go far then they disappear. nine0003
e. tendency to catastrophize. By the way, this explains the fact that between panic attacks the patient is completely rational, understands that no one died from panic attacks or went crazy, that a panic attack is a kind of training for the body, but during an anxiety attack all these protective statements go far then they disappear. nine0003
So why don't panic attacks go crazy? In order to understand this, you first need to explain what panic attacks are. Clinically, a panic attack (PA) is manifested by the following symptoms (at least 4):
1. Tachycardia.
2. Sweating.
3. Trembling or shaking of the body.
4. Feeling short of breath.
5. Choking.
6. Pain or discomfort in the chest. nine0082
7. Nausea or stomach discomfort.
8. Dizziness, unsteadiness or weakness.
9.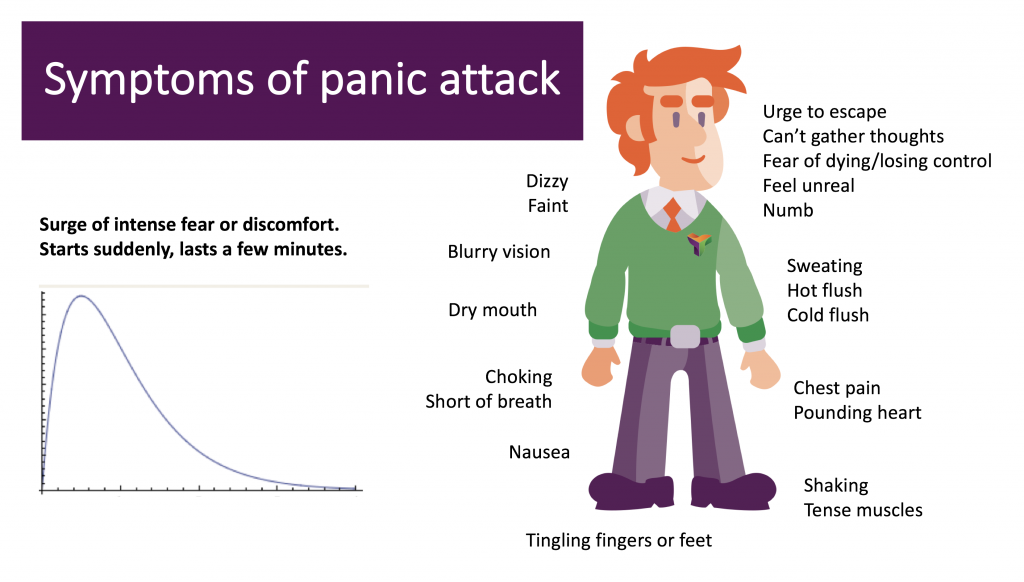 Derealization (feeling of the unreality of the surrounding world and what is happening) or depersonalization (feeling of alienation of one's own body or dissimilarity of one's own sensations).
Derealization (feeling of the unreality of the surrounding world and what is happening) or depersonalization (feeling of alienation of one's own body or dissimilarity of one's own sensations).
10. Fever or chills.
11. Paresthesia (tingling, numbness, or crawling).
12. Fear of dying.
13. Fear of losing control or going crazy.
Seizures can be repetitive, unpredictable and not limited to any particular situation (as opposed to, for example: social phobia - seizures in social situations, or agoraphobia - seizures in situations in which it is difficult to get help or get out of them). A panic attack rarely lasts more than 30 minutes. The average duration is 5-10 minutes. Avoidance of any situation in which the panic attack arose for the first time is formed secondarily, for example: being alone, crowded places, repetition of panic attacks - the so-called attack anticipation anxiety. nine0003
nine0003
It is important to mention that panic disorder occurs under circumstances not associated with an objective threat, i.e. PA is caused by an intrapsychic (intrasubjective) unconscious conflict. What are the elements of this conflict?
Panic attack is a classic manifestation of anxiety neurosis. The personality of a person predisposed to panic disorder is characterized by an integrated, but rigid (ossified, inflexible attitudes and rules) Super-Ego, whose instrument is a generalized sense of guilt. As a result, in response to unacceptable needs for dependence and love, as well as emerging anger and hostility towards others, unconscious anxiety turns on, transforming into a somato-vegetative symptom - a panic attack. nine0003
Thus, PA is not a signal of impending death or insanity, but the result of self-punishment for an unacceptable (immoral - from the point of view of children's morality self-punishing Super-Ego controller) impulse. The figure shows the mechanism of PA formation:
Otto Kernberg (1975) singled out 3 structural personality organizations: neurotic, borderline and psychotic. Panic attacks are a prerogative of a neurotic nature, in which the development of psychosis, for example: schizophrenia or paranoia, is not possible. nine0003
Panic attacks are a prerogative of a neurotic nature, in which the development of psychosis, for example: schizophrenia or paranoia, is not possible. nine0003
How does a neurotic personality differ from a psychotic one?
The neurotic organization of the personality is characterized by a "welded" Self - a clear boundary between the Self and ideas about others (between one's thoughts and feelings and fantasies about others). A holistic identity, in which conflicting images of the Self and others are integrated into a coherent picture. That does not allow the loss of connection with reality, even with significant stress. In addition, a strong Ego with productive, more mature psychological defenses is guarding the boundaries of Self: rationalization, repression, reactive formation, isolation, destruction, intellectualization. The ability to test reality - the ability to distinguish between Self and non-Self, intrapsychic and environmental factors is preserved. nine0003
So why is the psychotic person vulnerable to developing schizophrenia?
1. For the psychotic organization of the personality (in which the development of psychosis is possible and subject to the concept of stress diathesis, i.e. increased "vulnerability" to stresses), an ambiguous, but still hereditary predisposition is characteristic.
For the psychotic organization of the personality (in which the development of psychosis is possible and subject to the concept of stress diathesis, i.e. increased "vulnerability" to stresses), an ambiguous, but still hereditary predisposition is characteristic.
2. The psychotic personality is characterized by a weakness of the ego, which cannot cope with anxiety, does not control impulses and has only primitive psychological defenses, is not capable of sublimation. nine0003
3. Reality testing suffers in the psychotic organization of personality. It can be defined as the ability to distinguish between Self and non-Self, to distinguish the intrapsychic from the external source of perception and stimulation, and also as the ability to evaluate one's affects, behavior and thoughts in terms of the social norms of an ordinary person. In a clinical study, the following signs tell us about the ability to test reality: (1) the absence of hallucinations and delusions; (2) the absence of manifestly inappropriate or bizarre forms of affect, thought, and behavior; (3) if others notice the inadequacy or strangeness of the patient's affects, thinking and behavior in terms of the social norms of an ordinary person, the patient is able to empathize with the experiences of others and participate in their clarification. Reality testing must be distinguished from distortions of the subjective perception of reality, which can appear in any patient during psychological difficulties, as well as from a distortion of attitude towards reality, which always occurs both in character disorders and in more regressive psychotic states. nine0003
Reality testing must be distinguished from distortions of the subjective perception of reality, which can appear in any patient during psychological difficulties, as well as from a distortion of attitude towards reality, which always occurs both in character disorders and in more regressive psychotic states. nine0003
4. In addition, the psychotic organization of personality is characterized by "diffuse identity" (self-perception and self-understanding). Clinically, "diffuse identity" is represented by poor integration between self and significant others. A constant feeling of emptiness, contradictions in the perception of oneself, inconsistency in behavior that cannot be integrated in an emotionally meaningful way, and a pale, flat, poor perception of others are all manifestations of a diffuse identity. Psychotic structural organization implies a regressive rejection of the boundary between self and others, or the fuzziness of this boundary. In the mental organization of the borderline personality, there is a fairly clear barrier between the Self and the other. nine0003
nine0003
In the psychotic organization of the personality, there may be attacks of annihilation (vital) anxiety, but unlike panic attacks, they are characterized by originality and staging:
1st stage of psychosis - delusional mood. When a person is confused and anxious.
2nd stage - delusional perception, when the awareness and perception of the environment changes, everything that happens is realized as having something to do with the patient.
3rd stage - of special importance. Everything is perceived by the patient in accordance with some special meaning and significance of objects and phenomena. nine0003
The symptoms observed in borderline patients are similar to those of ordinary neuroses or character pathology, but the combination of certain features is characteristic of borderline cases. The following symptoms are especially important:
1. Anxiety. Borderline patients have chronic, permeating, "free-floating" anxiety.
2. Polysymptomatic neurosis. Many patients have one or another set of neurotic symptoms, but here we mean only those cases where the patient has a combination of at least two of the following:
Polysymptomatic neurosis. Many patients have one or another set of neurotic symptoms, but here we mean only those cases where the patient has a combination of at least two of the following:
a. Multiple phobias, especially those that significantly limit the patient's activities in daily life.
b. Symptoms of obsession, which for the second time became Ego-synthonic (acceptable for the Self) and acquired the quality of “overvalued” thoughts and actions.
in. Multiple complex or bizarre conversion symptoms, especially chronic ones.
Dissociation reactions, especially hysterical twilight states and fugues, as well as amnesia accompanied by disturbances of consciousness. nine0003
e. Hypochondria.
e. Paranoid and hypochondriacal tendencies in association with any other symptomatic neuroses (a typical combination suggestive of a diagnosis of borderline personality organization).
3. Polymorphic perverse sexual tendencies. This refers to patients with severe sexual deviations, in which several different perverse tendencies coexist. The more chaotic and multiple the patient's perverse fantasies and actions, and the more unstable the object relations that develop around such sexuality, the more reason to suspect a borderline personality organization. nine0003
The more chaotic and multiple the patient's perverse fantasies and actions, and the more unstable the object relations that develop around such sexuality, the more reason to suspect a borderline personality organization. nine0003
4. “Classic” prepsychotic personality structure, including the following features:
a. Paranoid personality (paranoid features are manifested to such an extent that they come to the fore in a descriptive diagnosis).
b. schizoid personality.
in. Hypomanic personality and cyclothymic personality organization with marked hypomanic tendencies.
5. Impulsive neurosis and addictions. This refers to such forms of severe character pathology that are manifested in behavior by a “breakthrough of the impulse” to satisfy instinctive needs, and such impulsive episodes are ego-dystonic (alien to the ego) when recalling them, but ego-syntonic (acceptable to the ego) and bring great pleasure at the very moment of their performance.