What is an sd relationship
What Is SD/SB Relationship?
In This Article
The world is full of all different kinds of relationships. Many people choose a committed partnership, in which they settle down, get married, and share household bills and responsibilities. While this may be the norm, some people choose a different route: the SD/SB relationship.
The SD/SB arrangement, while perhaps not conventional, is a legitimate relationship, and those who participate in such a partnership find it to be beneficial. Learn the ins and outs of SB/SD dating here.
What is SD/SB relationship
Put simply, the SD/SB relationship is a sugar daddy, sugar baby partnership. One member of the relationship takes the role of the wealthy “sugar daddy,” while the other is his companion, or “sugar baby.”
What SD means in the relationship
Well, in the SD/SB relationship, SD stands for “sugar daddy.” The sugar daddy is typically a well-off man who wants the company of an attractive younger woman. In exchange for her time and attention, the sugar daddy or SD assists the sugar baby in some way, typically financially.
While a sugar daddy may quite literally assist the sugar baby by giving her money, he may also provide connections that help her to grow her career or get ahead in life, or he may shower her with gifts and take her on expensive vacations.
What SB means in the relationship
On the other hand, the SB in the SD/SB partnership is the sugar baby. This is an attractive younger woman who seeks the help of a sugar daddy.
The sugar baby may need financial support for school, or may be seeking financial assistance to help with bills like housing or a car payment. In exchange for her companionship and affection, however, this may look, the sugar baby receives assistance from the sugar daddy.
Types of SB/SD arrangements
The SD/SB type of relationship does not have just one look. In fact, there are multiple types of sugar relationships, depending upon what the couple agrees to as the terms of their partnership.
People may think that all sugar relationships involve a sugar baby giving sex in exchange for money, but there is more to sugar relationships than this. There are multiple types of sugar babies, and just as many types of sugar daddies to go along with them.
Consider the following types of sugar relationships:
- Mentorships
Sometimes, an SD/SB relationship can be as simple as the sugar daddy mentoring a younger woman and helping her to advance her career. He may link her to job opportunities or assist her with networking to grow her business.
The sugar daddy may also educate the sugar baby and share his skills and knowledge to help her better herself. In exchange for his mentoring, the sugar baby provides companionship to the sugar daddy.
Related Reading: Are You Gaining Something From Your Relationship?
- Friendships
As previously mentioned, SD/SB dating doesn’t always involve sex. Sometimes, both parties are simply interested in friendship. The sugar daddy may have a busy work schedule and a stressful life, and he may just need a friend to support him and listen to him.
Sometimes, both parties are simply interested in friendship. The sugar daddy may have a busy work schedule and a stressful life, and he may just need a friend to support him and listen to him.
The sugar baby may benefit from this arrangement if she is just seeking a connection and financial support without the challenges that come with romantic relationships.
A wealthy sugar daddy who has to travel for business may invite a sugar baby along on his trips to keep him company.
He benefits from the companionship so he doesn’t have to be so lonely while traveling for work, while the sugar baby gets to explore the world and enjoy exotic vacations at his expense.
- Sexual SD/SB dating
In some cases, there is sex involved in the SD/SB relationship. What makes this different from prostitution, however, is that there is an emotional connection between the partners.
The sugar baby provides not only companionship but also sex, and in turn, the sugar daddy supports her financially in some way.
Sexual SD/SB dating is also different from prositution, because the partnership involves repeated sex between the two parties, whereas prositution typically involves a man having sex with a prostitute once, and never seeing her again. SD/SB relationships, on the other hand, are an ongoing commitment.
Also Try: Are You Good at Sex Quiz
Some types of sugar daddies may prefer to meet only online, with no in-person or physical connection. This may involve chatting, emailing, or exchanging photos. Sometimes, the sugar daddy may request sexual photos. So, it is important to use caution if engaging in this type of SD/SB relationship.
Some sugar babies may find that this arrangement works perfectly for them, because they get the financial support of a sugar daddy without having to meet up with him and can conduct the entire relationship virtually.
Keep in mind that some sugar daddies may be married, and simply have sugar babies on the side for additional companionship.![]() They may help the sugar baby to advance her career, or give her some sort of financial support in exchange for dates or friendship.
They may help the sugar baby to advance her career, or give her some sort of financial support in exchange for dates or friendship.
Some sugar babies may also be in committed relationships, in which their significant others allow them to maintain contact with the sugar daddy for financial benefit.
Also Try: Should I Date Him Quiz
What are the terms of an SD/SB relationshipThe reality is that each SD/SB relationship works a little differently, because the couple has to decide the terms that guide the relationship.
Ultimately, they are a form of negotiation. The sugar daddy gives pampering in exchange for some type of companionship from the sugar baby, whether it be in the form of friendship, sex, or dates.
What these relationships all have in common is that one person offers companionship, in exchange for some sort of compensation. The compensation may be in the form of an allowance, gifts, vacations, or tuition payments.
Some SD/SB relationships may even be entirely monogamous relationships between a man and a woman while others could be non-monogamous. What makes them an SD/SB relationship is that the woman is benefitting in the form of pampering and compensation that she wouldn’t otherwise receive.
The terms of SD/SB relationships also involve an ongoing commitment. They are not a one-time meet up or one-time hookup in which a sugar daddy gives money to compensate for sex. This is what is seen with prostitution or escort services, which is an entirely different concept.
How to have a successful SD/SB relationshipIf you want a successful SD/SB relationship, there are some tips to follow to make this type of relationship work. The following strategies can help you to have a successful SD/SB arrangement:
Even if you are getting something out of the relationship, you have a right to stand up for your needs and interests. Be clear with your partner about what it is you expect from the relationship.
Being clear about your needs from the start prevents you from ending up in a situation that wasn’t what you wanted.
It’s also important that if you have a committed relationship with a spouse or significant other and are seeking a sugar daddy outside of your primary relationship, you have the consent of your partner to participate in the SD/SB relationship.
Related Reading: 5 Emotional Needs Every Couple Needs to Know
If you’re not willing to have sex with a sugar daddy and simply want more of a companionship type relationship, you shouldn’t feel obligated to have sex.
If a sexual relationship isn’t your intent, make it known and stick to it. Or, perhaps you aren’t comfortable having sex right away. Don’t feel the need to put out immediately in order to satisfy the sugar daddy.
Some sugar daddies may be more likely to agree to give an allowance or a tuition payment if you discuss the specific need for the funds.
For example, if you’re going back to school or attempting to start a business, they may see their payments to you as an investment. Or, perhaps you have specific bills you need assistance with. Either way, knowing where their money is going can be reassuring for some sugar daddies.
Or, perhaps you have specific bills you need assistance with. Either way, knowing where their money is going can be reassuring for some sugar daddies.
Related Reading: How Does Money Affect Relationships? 3 Tips for Money Conflicts
- Keep yourself safe
Maybe you’re meeting up with your sugar daddy in person for the first time, or you’re traveling across the country to visit with him. If this is the case, make sure you are taking steps to stay safe.
Tell a trusted friend that you’re going to see him, and make sure you share your location with them so they can keep tabs on you or send help in case something goes wrong.
Related Reading: Creating A Safe Haven For Communication
- Use a website
If you are an SB looking for SD, you might consider looking for a partner on SB/SD sites. These websites can link you to people who are looking for similar arrangements. Just be sure to use caution, as mentioned above.
Just be sure to use caution, as mentioned above.
Related Reading: 15 Best Websites for Online Relationship Advice
Check out this video explaining how you can be a successful sugar baby:
An SD/SB relationship isn’t for everyone, but some people find that this arrangement meets their needs perfectly.
You can think of the SD/SB arrangement as a sort of agreement in which one person receives a form of companionship in exchange for pampering, in the form of gifts, trips, or financial compensation.
For those who participate in SD/SB dating, the arrangement can be just as loving as any other relationship, although the terms may be different.
What Does SD/SB Mean? A Simple Guide To The Slang Internet Term Everyone's Using
There are many different types of relationships.
There are open relationships and codependent relationships. There are “convenient” relationships and long-distance relationships. There are friends with benefits (FWB) relationships and there are long-term monogamous relationships.
What does SD/SB mean and what type of relationship is involved in this dynamic?
SD/SB is an acronym that stands for Sugar Daddy (SD) and Sugar Baby (SB), but for many, these relationships are so much more than a title.
There is more to Sugar Daddies and Babies than a name.
In fact, according to Bustle, “sugaring... is a type of relationship/lifestyle in which a Sugar Baby (SB) ‘provides companionship in exchange for being pampered,’ while a Sugar Daddy (SD) ‘pampers Sugar Babies in return for companionship.’”
via GIPHY
RELATED: How To Get Your Very Own Sugar Daddy (As Written By A First Class Sugar Baby)
Of course, pampering and companionship are broad terms, and for good reason.
Pampering “can include [anything from] explicitly negotiated financial compensation — like an allowance, tuition payments, or an investment into a Sugar Baby's business venture — [to] gifts, trips, and other treats,” while companionship can be anything from sex “to casual dating, to a monogamous relationship.”
But while the terms of the relationship can change, the general concept remains the same: SDs and SBs offer each other something in exchange for something else.
RELATED: 7 Super-Sweet Perks Of Being A Sugar Baby (To A Sugar Daddy)
That said, the SD/SB relationship is confusing to some.
Many question the ethical implications of such courtships and wonder how Sugar Babies differ from prostitutes (and Daddies from their clients.)
But according to Seeking (formerly known as SeekingArrangement, there is one major distinction.
“Prostitute[s] and client[s] have a transactional relationship," the site states. "They meet, exchange funds, and participate in some sort of physical act and [then] part ways. Typically, this is a one time occurrence. A job. [But] Sugar Babies and Sugar Daddies have ongoing relationships, not transactions. [And] more often than not, a Sugar relationship will resemble that of a girlfriend-boyfriend relationship. There are real connections and real possibilities at romance, something that is not in the realm of possibility with an escort or prostitute.”
Typically, this is a one time occurrence. A job. [But] Sugar Babies and Sugar Daddies have ongoing relationships, not transactions. [And] more often than not, a Sugar relationship will resemble that of a girlfriend-boyfriend relationship. There are real connections and real possibilities at romance, something that is not in the realm of possibility with an escort or prostitute.”
via GIPHY
Still not sure what that means?
Consider the relationships of infamous playboys Hugh Hefner, John F. Kennedy, and Charlie Sheen.
Of course, this type of relationship is not for everyone — and that's okay.
Related Stories From YourTango:
The Type Of Cheating People Don't Talk About (But Can End Your Marriage)
4 Ways To Create The Type Of Chemistry That Drives Men Completely Wild
The Love Horoscope For Each Zodiac Sign On Friday, January 13, 2023
The beauty of relationships is that they can be varied and unique. But SD/SB relationships are (and can be) just as good, strong, and loving as any relationship.
But SD/SB relationships are (and can be) just as good, strong, and loving as any relationship.
Because love is love.
RELATED: How I Kept A Sugar Daddy Without Trading Any Kinky Favors
More for You:
Nicole Lane is a wife, mother, writer, and regular contributor for YourTango. She is a staunch defender of women's rights, she believes firmly in equality and parity, and she is an advocate for women's health, mental health, and sexuality.
Sign up for YourTango's free newsletter!
Attitude towards the disease of patients with diabetes mellitus type 1 and 2 | Motovilin
The influence of the patient's psychological characteristics on the course of diabetes mellitus (DM) is currently beyond doubt, and their study is becoming increasingly important [1–5]. The endocrinologist interacts not only with the body, but also with the personality of the patient, or rather, with their huge variety. Of course, the nature of the doctor's work does not allow delving into the subtleties of the patient's psychology, but finding out the most general patterns is not only of scientific, but also of obvious practical interest. The clinician's focus on the patient's psychology and the resulting ability to help the patient more productively modify diabetes-related behavior may improve disease outcomes. nine0003
The clinician's focus on the patient's psychology and the resulting ability to help the patient more productively modify diabetes-related behavior may improve disease outcomes. nine0003
One of the most important characteristics of a patient in terms of their influence on the course of a chronic disease is the internal picture of the disease (IDP), the highest level of which represents the attitude towards one's disease [6, 7]. As shown in a number of studies, the attitude towards the disease is associated with the psychological well-being of the patient, and even with the clinical characteristics of the disease [1, 2, 5]. Two categories of patients: with type 1 DM (DM1) and type 2 DM (DM2), despite the commonality of some characteristics of the disease, have significant differences in age, a number of clinical features (body weight, comorbidities), as well as in therapeutic approaches. It can be assumed that the ICP will be different in these two categories of patients. nine0003
To confirm this assumption, we conducted a comparative study of the attitude towards the disease of patients with DM1 and DM2. Since, along with age, the most obvious difference between these categories is the type of treatment, to minimize the influence of this factor on the results of the study, a group of patients with type 1 diabetes was compared with a group of patients with type 2 diabetes receiving insulin.
Since, along with age, the most obvious difference between these categories is the type of treatment, to minimize the influence of this factor on the results of the study, a group of patients with type 1 diabetes was compared with a group of patients with type 2 diabetes receiving insulin.
Research materials and methods
The sample of subjects consisted of 210 people, including 140 patients with DM1 and 70 patients with DM2 on insulin therapy for at least 3 months. The groups did not differ significantly in the ratio of men and women, the level of HbA1c and the duration of the disease (Table 1). nine0003
To study the attitude to the disease, the methods "Type of attitude to the disease" (TOBOL) NIPNI them. V.M. Bekhterev and "Color test of relations" (CTO) E.M. Etkind. The first is a questionnaire and allows you to identify the leading type of attitude towards the disease (harmonious, anxious, etc.). However, the greatest interest for the study is not so much this leading type, but the degree of representation of various components in a holistic attitude towards the disease (for example, in two patients with a leading harmonious attitude, the anxiety component can be expressed to different degrees). All attitude options are divided into adaptive (contributing to psychological adaptation to life in conditions of illness) and maladaptive (preventing adaptation). nine0003
All attitude options are divided into adaptive (contributing to psychological adaptation to life in conditions of illness) and maladaptive (preventing adaptation). nine0003
The TOBOL technique is aimed at studying well-recognized components of the attitude towards the disease, due to which it can be subject to distortions under the influence of social desirability (ie, attempts to guess the “correct” answer). To reduce this effect, a fundamentally different technique was used - CTO. It is built on the principle of a color-associative experiment and is designed to reveal the deeper, hidden aspects of the relationship to something, in this case, to the disease. In this method, the subject must associate with the stimulus word offered to him one of the 8 colors that were previously ranked by him according to the degree of preference (1st place is the most preferred, 8 is the least preferred color). The following concepts related to diabetes were used as stimulus words: health, illness, pain, diabetes, life with diabetes, hyperglycemia, hypoglycemia, injections, diet, sugar measurement, diabetes management, medical examination, complications, doctors, hospital. The concepts were formulated in the spoken language of the patient. nine0003
The concepts were formulated in the spoken language of the patient. nine0003
The association of the color that is in the first place with a certain word indicates a positive attitude towards the content of this concept. And vice versa, if the respondent selects the color that occupies the last place for the concept, this indicates emotional rejection, rejection of the content of the concept. Those. the higher the rank, the worse the attitude. CTO is one of the most widely used projective tests, allowing to neutralize the influence of various protective mechanisms that distort the results of the study of the mental sphere of the subject. nine0003
The Medical Outcomes Study 36-Item Short Form Health Survey (SF-36), Spielberger-Khanin Situational and Personal Anxiety (SPILBERGER-KHANIN SITUATIONAL AND PERSONAL ANXIETY) ( CLT), the Center for Epidemiological Research Depression Scale (CES-D), as well as the Dembo-Rubinstein self-assessment method, which is a visual analogue scale on which the patient needs to mark their health level from 1 to 10 points. nine0003
nine0003
All patients signed informed consent.
Student's t and U Mann-Whitney tests, cluster and correlation analysis were used for statistical processing. Processing was performed using the statistical package SPSS 15.
Results
The use of the TOBOL method revealed some differences between the DM1 and DM2 groups (Table 2).
Thus, on the one hand, patients with type 1 diabetes have slightly higher scores on the melancholic attitude scale, which reflects disbelief in the success of treatment. However, the melancholic component, in comparison with the other 11 scales, occupies the second place from the bottom in the DM1 group, i.e. it only to a small extent affects the general attitude towards the disease. nine0003
At the same time, patients with DM2 have higher scores on the scale of sensitive attitude, which indicates their increased vulnerability due to the disease, fear of adverse reactions from others. Among all 9 maladaptive scales (scales 4–11 in Table 2), the sensitive attitude has the highest rates in both groups. From this we can conclude that patients with DM are quite strongly concerned about how their disease is perceived by others, and such feelings are more pronounced in the group of patients with DM2. nine0003
From this we can conclude that patients with DM are quite strongly concerned about how their disease is perceived by others, and such feelings are more pronounced in the group of patients with DM2. nine0003
However, the nature of these concerns is somewhat different. Thus, in the DM1 group, indicators on the scale of sensitive attitude negatively correlate with self-esteem indicators on the health scale of the Dembo-Rubinshtein method (r=-0.301, p=0.003). That is, if the patient evaluates his health low, then he has an increased fear of the negative attitude of others, emotional rejection on their part.
In patients with DM2, this correlation is absent, but an unexpected positive correlation with the ergopathic attitude scale is found (r=0.361, p=0.009), which belongs to the category of adaptive and reflects the desire to overcome the disease by immersing in vigorous activity, primarily labor. In other words, the more a person is focused on work activity in conditions of illness, the more he experiences in connection with how others perceive him. This connection can be understood in such a way that a middle-aged patient with DM2 (average age in the sample is 60 years) is afraid not so much of rejection from others, but of the threat of becoming a burden for loved ones, or becoming dependent on them. These fears can cause a desire to be more active in the workplace. nine0003
This connection can be understood in such a way that a middle-aged patient with DM2 (average age in the sample is 60 years) is afraid not so much of rejection from others, but of the threat of becoming a burden for loved ones, or becoming dependent on them. These fears can cause a desire to be more active in the workplace. nine0003
So, the results of the TOBOL method allow us to speak about a certain discrepancy between the DM1 and DM2 groups, but not too pronounced.
When analyzing the results of the CTO methodology, which concerns a deep, emotionally direct relationship to the disease, more significant differences between groups are found. First of all, it was revealed that patients with DM2 demonstrate a greater emotional rejection of the very concept of "diabetes" (average place 4.6 and 5.4 in the DM1 and DM2 groups, respectively, p = 0.04). nine0003
The results of the DTT methodology were subjected to hierarchical cluster analysis (All used concepts are presented as variables from 1 to 8, where 1 reflects the most positive attitude to the content of the concept (emotional acceptance), and 8 - the most negative (emotional rejection). two variables is the correlation coefficient applied to the matrices of variables.As a result of the analysis, a cluster structure is formed in which variables are combined at different levels.The lower the level at which the variables were combined into a single cluster, the closer the relationship between them.). It made it possible to determine the degree of closeness of patients' attitudes to various concepts associated with DM (see above). nine0003
two variables is the correlation coefficient applied to the matrices of variables.As a result of the analysis, a cluster structure is formed in which variables are combined at different levels.The lower the level at which the variables were combined into a single cluster, the closer the relationship between them.). It made it possible to determine the degree of closeness of patients' attitudes to various concepts associated with DM (see above). nine0003
The dendrograms (Figs. 1 and 2) show a hierarchy of clusters that reflects the structure of attitudes towards the analyzed concepts, which is typical for patients with DM2 and DM1. The level of association of two variables (or clusters) can be assessed by the scale of intercluster distance above the dendrogram: a low distance coefficient indicates a very high degree of similarity of attitude towards two concepts (or clusters of concepts). For example, in fig. 1, the concepts of “disease” and “pain” (distance coefficient - 1.3), “hyperglycemia” and “hypoglycemia” (distance coefficient - 2), “sugar measurement” and “medical examination” (distance coefficient - 3 ,five).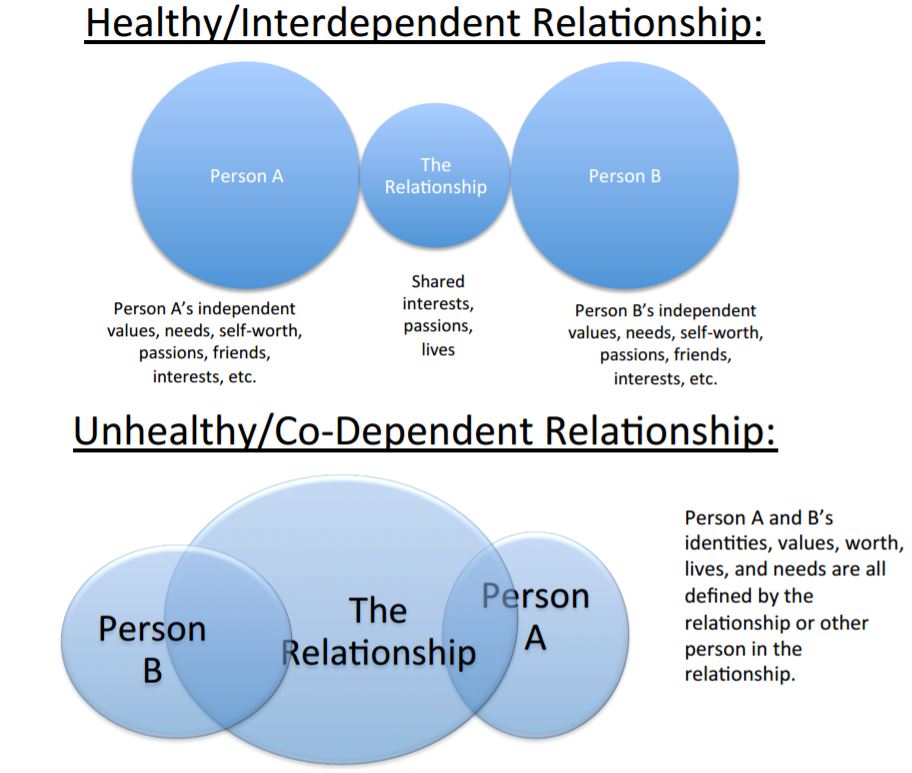 nine0003
nine0003
In the CD2 group, the concepts were grouped in a quite predictable way. As seen in fig. 1, all the concepts used were combined into two large clusters, in which the words are related in meaning. The first cluster includes concepts that reflect pathological phenomena: illness, pain, my condition with hyper- and hypoglycemia, complications. The word "diabetes" is also in this group. Therefore, for patients in the DM2 group, diabetes is associated with its adverse symptoms and consequences. nine0003
The second cluster includes concepts related to the treatment of diabetes, with the life that the patient must lead to maintain health: "diet, self-measurement of sugar, injections, etc." It is quite predictable that the word "health" is associated precisely with this group of concepts.
Cluster analysis of the results of testing patients with DM1 reveals somewhat similar trends (Fig. 2). All concepts are also combined into two groups of similar content: cluster 1 - pathological phenomena and 2 - necessary measures to maintain health. However, it is surprising that the word "diabetes" does not fall into the "pathological" cluster, as in patients with type 2 diabetes, but into the "health maintenance" cluster. This phenomenon demonstrates a fundamental difference in the attitude of patients of two groups towards their disease: patients with type 2 diabetes more often perceive diabetes as a disease associated with severe symptoms (pain, hyper- or hypoglycemia), complications, while for young patients with type 1 diabetes, the concept of "diabetes" means something close to lifestyle (the words "diabetes" and "life with diabetes" are closest to each other). nine0003
However, it is surprising that the word "diabetes" does not fall into the "pathological" cluster, as in patients with type 2 diabetes, but into the "health maintenance" cluster. This phenomenon demonstrates a fundamental difference in the attitude of patients of two groups towards their disease: patients with type 2 diabetes more often perceive diabetes as a disease associated with severe symptoms (pain, hyper- or hypoglycemia), complications, while for young patients with type 1 diabetes, the concept of "diabetes" means something close to lifestyle (the words "diabetes" and "life with diabetes" are closest to each other). nine0003
Continuing the discussion of the results of the cluster analysis of the survey data of the two groups presented in fig. 1 and 2, a number of differences that are important for understanding the behavioral characteristics of patients with different types of DM should be highlighted.
In the DM2 group, such concepts as "measurement of sugar" and "self-management of diabetes" are also far removed from "health" (distance coefficient - 17), and in the DM1 group, on the contrary, they are quite close to it (distance coefficient - 7, 7). Those. young patients with type 1 diabetes are more likely (at a deep, emotional level) to measure glycemia and, in general, to their own activity in managing diabetes as an important condition for maintaining health. Older patients with T2DM are likely to find it harder to comply with the requirements for measuring glycemia due to their lack of an appropriate attitude towards self-control in the broad sense of the word. They are not inclined to show their own activity in the treatment of DM - and probably rely more on external assistance, on visiting medical institutions, as evidenced by the rather close location of the concepts of "health" and "hospital" in their dendrogram. nine0003
Those. young patients with type 1 diabetes are more likely (at a deep, emotional level) to measure glycemia and, in general, to their own activity in managing diabetes as an important condition for maintaining health. Older patients with T2DM are likely to find it harder to comply with the requirements for measuring glycemia due to their lack of an appropriate attitude towards self-control in the broad sense of the word. They are not inclined to show their own activity in the treatment of DM - and probably rely more on external assistance, on visiting medical institutions, as evidenced by the rather close location of the concepts of "health" and "hospital" in their dendrogram. nine0003
So, the analysis of the results of TOBOL and CTO methods shows that between patients with type 1 and type 2 diabetes there are not only quantitative, but also qualitative differences in relation to their disease, and this manifests itself not so much at the level of cognitive representations, knowledge about the disease (TOBOL) , how much at a deeper level of emotional experience of reality (CTO).
The next task of the study was to identify the relationship between attitudes towards the disease and the psychological well-being of patients. To solve it, a comparative analysis of the psychological well-being of patients with different attitudes towards the disease was carried out. nine0003
Quality of life (Fig. 3) and emotional state (Fig. 4) in the examined samples were used as the main indicators of psychological well-being. The results of the implementation of the relevant methods (SF-36, SLT, CES-D) showed a better psychological state of patients with DM1.
Patients from the DM1 group have significantly higher scores on all scales (p<0.05), except for mental health. The differences are most pronounced on the scales associated with the physical state (the first three scales), which can be explained by the influence of age, as well as on the scale of role functioning associated with the emotional state, which may be due not so much to age as to differences in attitude to one's disease. nine0003
nine0003
An analysis of the results of methods designed to diagnose anxiety and depression confirms this assumption.
The emotional state of patients in the DM1 group is more favorable. Thus, they have significantly lower levels of both situational and personal anxiety, as well as depression (p<0.05). It can be assumed that the differences between the DM1 and DM2 groups are also due to the peculiarities of the attitude of patients to their disease. As shown above, patients with DM1 subjectively perceive diabetes not so much as a disease, but as their individual feature, as part of their lifestyle, which reduces the degree of threat posed by it. Patients with DM2 are less prone to such psychological processing of diabetes, they evaluate themselves as sick, as evidenced by their lower self-esteem on the health scale in the Dembo-Rubinstein method (DM1 - 5.45, DM2 - 4.71, p = 0.032) and lower scores on the General Health scale in the SF-36 method (p=0.007). This prevents the normalization of their emotional state, improvement of psychological well-being. nine0003
nine0003
Thus, it can be assumed that the revealed differences in the psychological well-being of respondents in the DM1 and DM2 groups are associated not only with the discrepancy in age, but also with the attitude towards their disease. However, this assumption needs to be verified.
To confirm this assumption, we compared two groups with different attitudes to DM, balanced by age and by the representation of patients with different types of DM. To this end, we applied k-means cluster analysis (All used concepts are presented as variables from 1 to 8, where 1 reflects the most positive attitude towards the content of the concept (emotional acceptance), and 8 - the most negative (emotional rejection). between two variables is the correlation coefficient applied to the matrices of variables.As a result of the analysis, a cluster structure is formed in which variables are combined at different levels.The lower the level at which the variables were combined into a single cluster, the closer the relationship between them.
The hierarchical clustering procedure was described above using the same data. The difference between the two variants of cluster analysis lies in the fact that in the first case (hierarchical cluster analysis), concepts associated with diabetes were classified according to the similarity of patients' attitudes towards them. This classification can be conditionally called vertical. In the second case, the purpose of using cluster analysis using the k-means method was to classify not concepts, but the subjects themselves based on the similarity of their attitudes towards SD. It is rather a horizontal classification, because all subjects are divided into two groups without establishing complex hierarchical relationships between them.), which allows you to divide all the subjects into a certain number of groups. nine0003
For analysis, we used the degree of "negativity" of patients' attitudes towards DM (ie, its emotional rejection). As variables for clustering, the results of the CTO methodology were used, namely: the ranks of the color associated with diabetes and other related concepts. The ranks reflect the level of negative/positive attitude of the respondent to the concept: the higher the rank, the worse the attitude.
The ranks reflect the level of negative/positive attitude of the respondent to the concept: the higher the rank, the worse the attitude.
The results of comparison of the groups selected by means of cluster analysis are presented in fig. 5. The first group consisted of patients in whom "diabetes" and related concepts have higher ranks, which indicates a pronounced negative attitude towards diabetes, its emotional rejection (hereinafter referred to as group 1). The second group was formed by those whose attitude towards DM is less negative (hereinafter referred to as group 2). nine0003
Patients with DM1 and DM2 are unevenly represented in groups 1 and 2 (Table 3).
This inconsistency corresponds to previously identified tendencies of a more favorable attitude of young patients with type 1 diabetes to the disease, but it does not reach the level of statistical significance. Age differences between groups are also insignificant.
Given this fact, the differences in quality of life (Fig. 6) and emotional state (Fig. 7) described below can be explained by the variant of the attitude towards the disease, and not by the type of DM and the age associated with it. nine0003
6) and emotional state (Fig. 7) described below can be explained by the variant of the attitude towards the disease, and not by the type of DM and the age associated with it. nine0003
Comparison of the two groups clearly demonstrates the impact of attitudes towards illness on psychological well-being. Group 1 patients have a significantly higher quality of life on all scales of the SF-36 questionnaire (p=0.035 and below), except for pain intensity. The greatest differences are on the scale of role functioning due to the emotional state, which allows us to say that with a pronounced negative attitude towards DM, the patient develops such unfavorable emotional states that prevent a full life and may interfere with the performance of daily duties and work activities. nine0003
Role functioning worsens for another reason: patients who have a negative attitude towards DM also feel worse physically, as evidenced by a significant difference between groups on scales of general health and role functioning due to physical condition. In the Dembo-Rubinshtein self-esteem study methodology, patients from group 1 also assess their health significantly lower than group 2 (4.3 and 6.02, respectively, p=0).
In the Dembo-Rubinshtein self-esteem study methodology, patients from group 1 also assess their health significantly lower than group 2 (4.3 and 6.02, respectively, p=0).
As shown in fig. 7, the condition of patients from group 1 is characterized by a greater severity of symptoms of both anxiety and depression (all differences are significant, p=0.002 and below). Based on this, it can be argued that a negative attitude towards DM, its subjective rejection provokes a significant deterioration in the patient's emotional state. This is consistent with the above results of the SF-36 methodology, according to which, with a negative attitude towards DM, a person's daily life suffers to the greatest extent due to emotional distress. nine0003
It should be noted that the level of HbA1c in the two groups did not differ (9.2%), which indicates the absence of a linear relationship between the metabolic compensation of DM and the patient's attitude to his disease, but does not exclude the possibility of another, non-linear relationship between these parameters.
Discussion of the results
The conducted study revealed differences in the attitude of patients with DM1 and DM2 towards the disease.
A young person with type 1 diabetes, facing a serious lifelong illness, finds himself in a psychologically difficult situation. He has not yet taken place as a person, and only makes life plans, while the disease becomes a serious threat to his future. DM is also subjectively dangerous for self-esteem, since the presence of a pronounced negative difference between oneself and others (peers) often leads to the development of a feeling of inferiority [4, 7, 8]. Therefore, in order to preserve the psychological well-being of a young patient with DM, it is necessary to make significant efforts to develop such an attitude towards the disease that would subjectively minimize the threat from its side. This attitude is the perception of DM as a way of life, and not as a disease, found in the studied sample of patients with DM1. nine0003
T2DM, which occurs at a much later age, leads to the formation of a different life situation. By this time, many people may already have other chronic diseases (cardiovascular, etc.), so diabetes is not the only and most serious difficulty that needs to be overcome. Rather, it becomes one of those difficulties, and therefore cannot generate the same coping options that are activated at a young age. It should also be taken into account that an elderly person has fewer resources for psychologically overcoming an illness. Together, these factors prevent the formation of such an attitude towards the disease, which is typical for young patients with type 1 diabetes. Patients with type 2 diabetes on insulin therapy, as shown in this study, relate to their disease differently. For them, diabetes does not become a “way of life”, but is perceived precisely as a disease. Their attitudes towards DM itself, its symptoms and treatment are generally more negative than those of young patients with DM1. nine0003
By this time, many people may already have other chronic diseases (cardiovascular, etc.), so diabetes is not the only and most serious difficulty that needs to be overcome. Rather, it becomes one of those difficulties, and therefore cannot generate the same coping options that are activated at a young age. It should also be taken into account that an elderly person has fewer resources for psychologically overcoming an illness. Together, these factors prevent the formation of such an attitude towards the disease, which is typical for young patients with type 1 diabetes. Patients with type 2 diabetes on insulin therapy, as shown in this study, relate to their disease differently. For them, diabetes does not become a “way of life”, but is perceived precisely as a disease. Their attitudes towards DM itself, its symptoms and treatment are generally more negative than those of young patients with DM1. nine0003
Regardless of the type of DM, the attitude towards the disease becomes one of the most important factors determining both the quality of life and the emotional state of patients. A pronounced negative attitude towards diabetes, its emotional rejection indicate the patient's inability to psychologically adequately process the situation that has developed under the conditions of the disease. For a long time, the patient continues to perceive DM as a threat, and such a threat that cannot be eliminated due to the lifelong nature of the disease and which will necessarily lead to serious consequences. Such a perception of the life situation inevitably provokes a deterioration in the emotional state (an increase in anxiety and depression). Moreover, a negative attitude towards the disease exacerbates the perception of oneself as a sick person, worsens even his physical well-being, despite the fact that the objective state does not always correspond to such a sense of self. nine0003
A pronounced negative attitude towards diabetes, its emotional rejection indicate the patient's inability to psychologically adequately process the situation that has developed under the conditions of the disease. For a long time, the patient continues to perceive DM as a threat, and such a threat that cannot be eliminated due to the lifelong nature of the disease and which will necessarily lead to serious consequences. Such a perception of the life situation inevitably provokes a deterioration in the emotional state (an increase in anxiety and depression). Moreover, a negative attitude towards the disease exacerbates the perception of oneself as a sick person, worsens even his physical well-being, despite the fact that the objective state does not always correspond to such a sense of self. nine0003
In conclusion, the following should be noted. It is obvious that important tasks when working with a patient with diabetes are diagnosing attitudes towards the disease and, if necessary, changing it from expressed rejection to emotional acceptance. This is possible, in particular, in the process of learning, properly constructed interaction with the doctor, sometimes only as a result of psychotherapy. Such a change will improve the quality of life, the psychological well-being of the patient, and, possibly, will also indirectly contribute to the compensation of DM by changing the patient's behavior to a more compliant one. However, it is necessary to refrain from a simplistic understanding of the relationships between different aspects of the disease. nine0003
This is possible, in particular, in the process of learning, properly constructed interaction with the doctor, sometimes only as a result of psychotherapy. Such a change will improve the quality of life, the psychological well-being of the patient, and, possibly, will also indirectly contribute to the compensation of DM by changing the patient's behavior to a more compliant one. However, it is necessary to refrain from a simplistic understanding of the relationships between different aspects of the disease. nine0003
In this study, there was no direct relationship between the emotional attitude to the disease and the level of HbA1c. This phenomenon is in some way consistent with the results of our earlier study, which showed that the relationship between HbA1c and another level of attitude to the disease - intellectually mediated - is non-linear [2].
Therefore, one should not expect an "automatic" improvement in the quality of life and psychological well-being after the improvement of metabolic parameters, as well as the inevitable achievement of target glycemia by the patient due to the normalization of the emotional state. The complex nature of the relationship between the two sides of the disease - objective and subjective - should definitely be the subject of further research, but today it should be taken into account by endocrinologists, psychologists and psychotherapists in the treatment of patients with diabetes. nine0003
The complex nature of the relationship between the two sides of the disease - objective and subjective - should definitely be the subject of further research, but today it should be taken into account by endocrinologists, psychologists and psychotherapists in the treatment of patients with diabetes. nine0003
The authors declare no duality (conflict) of interest related to the manuscript.
Clinic Zdorovye - Diabetes mellitus is not a death sentence, but a reason to pay more attention to your health!
Today I would like to draw your attention to such a chronic disease as diabetes mellitus. Fear, bewilderment, resentment, a sense of helplessness - this is not a complete list of feelings experienced by a person who is faced with this problem. How to live on? Who can help me? What is diabetes anyway? Questions I will try to answer. nine0003
There are different types of diabetes. The most common types of this disease are type 1 diabetes and type 2 diabetes. The first type of diabetes is associated with the fact that patients do not produce insulin and in order to live they must take daily injections. Type 2 diabetes mellitus develops more often in middle and old age. These patients have their own insulin, it just doesn't work that way.
The first type of diabetes is associated with the fact that patients do not produce insulin and in order to live they must take daily injections. Type 2 diabetes mellitus develops more often in middle and old age. These patients have their own insulin, it just doesn't work that way.
It's important to note that type 2 diabetes often doesn't have bright symptoms that reflect high blood sugar, meaning you may not experience a sudden deterioration in well-being, extreme thirst or dry mouth. It often happens that the symptoms of high blood sugar bother patients at the initial stage of the disease, and then the body "gets used" to living on high sugars and the symptoms of hyperglycemia disappear. Many patients do not feel unwell even at a blood sugar level of 16-18 mmol / l. The appearance or intensification of weakness, fatigue, skin itching should make you additionally control  According to statistics, about 7 years pass from the moment of development of type 2 diabetes mellitus and the moment of its diagnosis. That is, a person can have an elevated blood glucose level for a long time and does not even know about it. In fact, you may have already forgotten what it means to feel good, not to feel weak, tired.
According to statistics, about 7 years pass from the moment of development of type 2 diabetes mellitus and the moment of its diagnosis. That is, a person can have an elevated blood glucose level for a long time and does not even know about it. In fact, you may have already forgotten what it means to feel good, not to feel weak, tired.
It must be taken into account that today there is a significant “rejuvenation of type 2 diabetes”. There used to be a saying "40 years - wait for diabetes." Today we have to state that type 2 diabetes is also found in children. Of course, this is directly related to body weight. According to modern data, obesity is recognized by the World Health Organization (WHO) as a global non-communicable epidemic. After all, excess weight is not just an aesthetic problem, but the presence of many diseases that a person probably also knows about, but this does not mean that they do not exist. Identification of these conditions at an early stage is the key to health and the absence of problems in the future. Proper examination and correction of metabolic disorders will avoid many health problems. And when people see a doctor at a later stage, they usually already have a large number of complications, including a high risk of cardiovascular pathology
Proper examination and correction of metabolic disorders will avoid many health problems. And when people see a doctor at a later stage, they usually already have a large number of complications, including a high risk of cardiovascular pathology
The danger of high blood sugar is that at a high level in the blood, it does not enter the peripheral organs and tissues, thus, the cells are not provided with the energy they need. As a result, the usual mechanism of energy supply to the cells is disrupted in the body. Here you can draw an analogy with a car, where gasoline is in the gas tank, but does not enter the engine. As a result, the car will not go anywhere. So it is in the body, since glucose is the main source of nutrition for organs and tissues. In such a situation, cells all the time do not receive the necessary “fuel” and starve, while excess sugar in the blood constantly destroys the walls of blood vessels and nerve fibers. Many processes depend on the level of blood sugar, including the development of late complications of diabetes, which can ultimately lead to a heart attack, stroke, loss of vision, amputation of the legs. But even the detection of late complications of diabetes mellitus is not a reason for pessimism, but a reason for active struggle against these disorders, which in most cases are reversible or it is possible to stabilize them at the initial level. And here you can come to the aid of modern medicine with effective drugs and a competent approach to their appointment. Today, according to statistics, patients with diabetes live longer than the average for the population, due to the fact that they monitor their health more closely and strictly follow medical recommendations.
So it is in the body, since glucose is the main source of nutrition for organs and tissues. In such a situation, cells all the time do not receive the necessary “fuel” and starve, while excess sugar in the blood constantly destroys the walls of blood vessels and nerve fibers. Many processes depend on the level of blood sugar, including the development of late complications of diabetes, which can ultimately lead to a heart attack, stroke, loss of vision, amputation of the legs. But even the detection of late complications of diabetes mellitus is not a reason for pessimism, but a reason for active struggle against these disorders, which in most cases are reversible or it is possible to stabilize them at the initial level. And here you can come to the aid of modern medicine with effective drugs and a competent approach to their appointment. Today, according to statistics, patients with diabetes live longer than the average for the population, due to the fact that they monitor their health more closely and strictly follow medical recommendations.