What are obsessive thoughts
When Unwanted Thoughts or Repetitive Behaviors Take Over
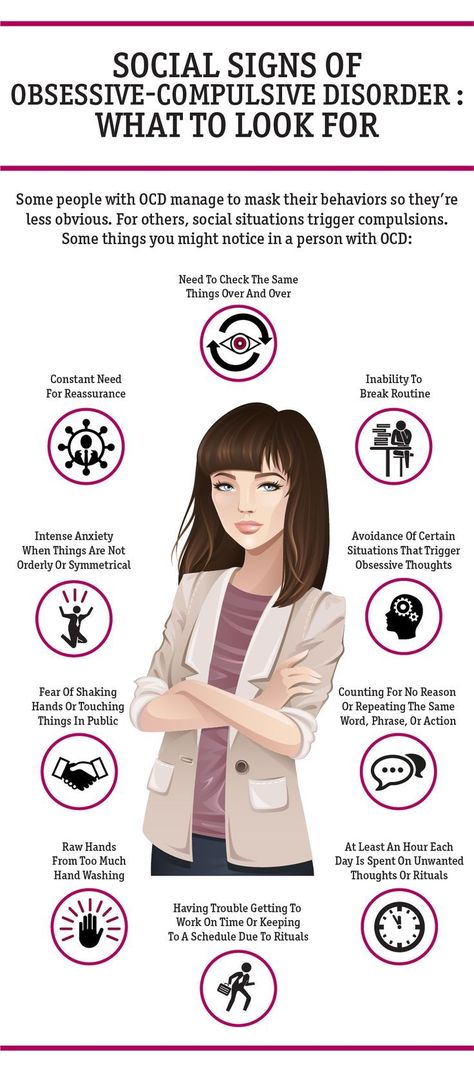
People who are distressed by recurring, unwanted, and uncontrollable thoughts or who feel driven to repeat specific behaviors may have obsessive-compulsive disorder (OCD). The thoughts and behaviors that characterize OCD can interfere with daily life, but treatment can help people manage their symptoms.
What is OCD?
OCD is a common, long-lasting disorder characterized by uncontrollable, recurring thoughts (obsessions) that can lead people to engage in repetitive behaviors (compulsions).
Although everyone worries or feels the need to double-check things on occasion, the symptoms associated with OCD are severe and persistent. These symptoms can cause distress and lead to behaviors that interfere with day-to-day activities. People with OCD may feel the urge to check things repeatedly or perform routines for more than an hour each day as a way of achieving temporary relief from anxiety.
If OCD symptoms are not treated, these behaviors can disrupt work, school, and personal relationships and can cause feelings of distress.
OCD symptoms tend to emerge in childhood, around age 10, or in young adulthood, around age 20 to 21, and they often appear earlier in boys than in girls. Most people are diagnosed with OCD by the time they reach young adulthood.
What are the signs and symptoms of OCD?
People with OCD may have obsessions, compulsions, or both.
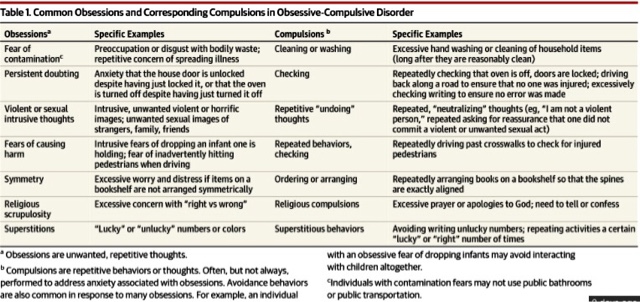
Obsessions are repeated thoughts, urges, or mental images that cause anxiety. Common obsessions include:
- Fear of germs or contamination
- Fear of forgetting, losing, or misplacing something
- Fear of losing control over one’s behavior
- Aggressive thoughts toward others or oneself
- Unwanted, forbidden, or taboo thoughts involving sex, religion, or harm
- Desire to have things symmetrical or in perfect order
Compulsions are repetitive behaviors that a person feels the urge to do in response to an obsessive thought. Common compulsions include:
Common compulsions include:
- Excessive cleaning or handwashing
- Ordering or arranging items in a particular, precise way
- Repeatedly checking things, such as that the door is locked or the oven is off
- Compulsive counting
How do I know if it’s OCD?
Not all rituals or habits are compulsions. Everyone double-checks things sometimes. In general, people with OCD:
- Can't control their obsessive thoughts or compulsive behaviors, even when they recognize those thoughts or behaviors as excessive
- Spend at least 1 hour a day on these obsessive thoughts or compulsive behaviors
- Don’t get pleasure when performing compulsive behaviors or rituals, but may feel brief relief from the anxiety brought on by obsessive thoughts
- Experience significant problems in daily life due to these thoughts or behaviors
Some individuals with OCD also have a tic disorder. Motor tics are sudden, brief, repetitive movements, such as eye blinking and other eye movements, facial grimacing, shoulder shrugging, and head or shoulder jerking. Common vocal tics include repetitive throat-clearing, sniffing, or grunting sounds. It is common for people with OCD also to have a diagnosed mood disorder or anxiety disorder.
Common vocal tics include repetitive throat-clearing, sniffing, or grunting sounds. It is common for people with OCD also to have a diagnosed mood disorder or anxiety disorder.
Symptoms of OCD may come and go, ease over time, or worsen. People with OCD may try to help themselves by avoiding situations that trigger their obsessions, or they may use alcohol or drugs to calm themselves. Although most adults with OCD recognize that their compulsive behaviors don’t make sense, some adults and most children may not realize that their behavior is out of the ordinary. Parents or teachers typically recognize OCD symptoms in children.
If you think you or your child may have OCD, talk to a health care provider about the possible symptoms. If left untreated, OCD can interfere in all aspects of life.
What causes OCD?
The exact causes of OCD aren’t known; however, a variety of factors are associated with an increased chance of developing the disorder.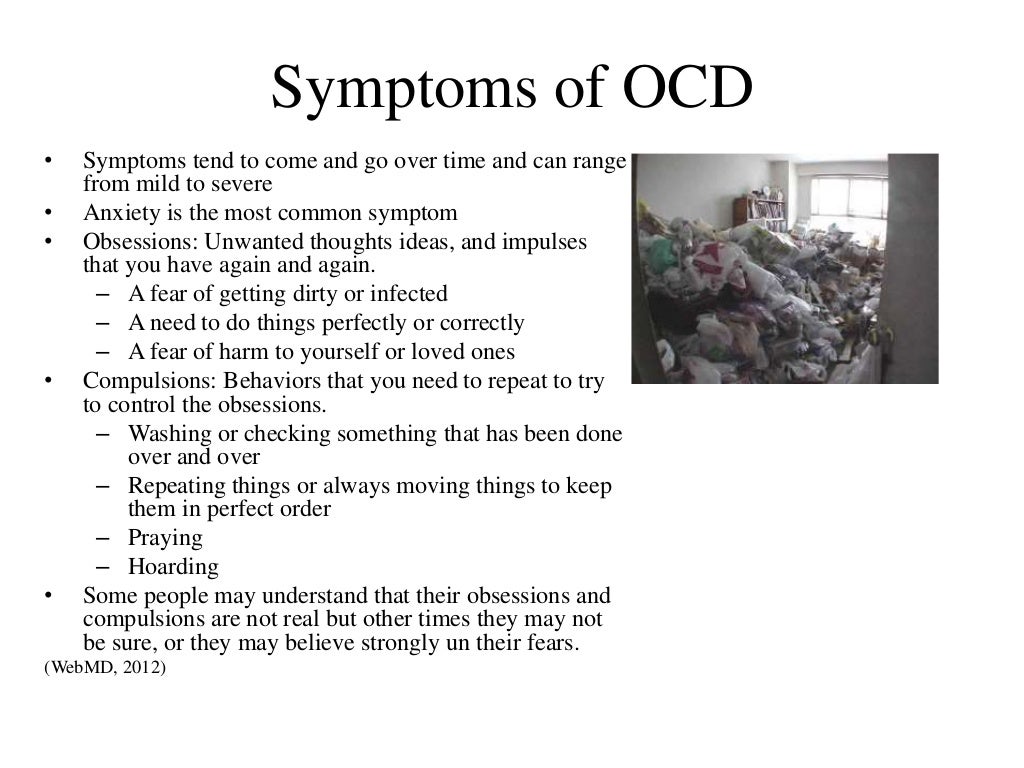
Genetics is one factor associated with OCD. Studies have shown that having a first-degree relative (parent, sibling, or child) with OCD is associated with an increased chance of developing the disorder. Scientists have not identified any one gene or set of genes that definitively lead to OCD, but studies exploring the connection between genetics and OCD are ongoing.
In addition to genetics, other biological factors may play a role. Brain imaging studies have shown that people with OCD often have differences in the frontal cortex and subcortical structures of the brain, areas of the brain that underlie the ability to control behavior and emotional responses. Researchers also have found that several brain areas, brain networks, and biological processes play a key role in obsessive thoughts, compulsive behavior, and associated fear and anxiety. Research is underway to better understand the connection between OCD symptoms and parts of the brain.
Some studies have reported an association between childhood trauma and obsessive-compulsive symptoms. More research is needed to understand this relationship.
More research is needed to understand this relationship.
Children who develop a sudden onset or worsening of OCD symptoms after a streptococcal infection may be diagnosed with a condition called Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS).
How is OCD treated?
The first step is to talk with your health care provider about your symptoms. Asking questions and providing information to your health care provider can improve your care.
Your health care provider will perform a physical exam and ask you about your health history to make sure that your symptoms are not caused by other illnesses or conditions. Your health care provider may refer you to a mental health professional, such as a psychiatrist, psychologist, social worker, or counselor, for further evaluation or treatment.
Treatment for OCD typically includes specific types of psychotherapy (such as cognitive behavioral therapy), medication, or a combination of the two. A mental health professional can talk about the benefits and risks associated with different treatment options and help identify the best treatment for you. Sometimes people with OCD also have other mental illnesses, such as anxiety, depression, and body dysmorphic disorder, a disorder in which someone mistakenly believes that a part of their body is abnormal. It is important to consider these other disorders when making decisions about treatment.
A mental health professional can talk about the benefits and risks associated with different treatment options and help identify the best treatment for you. Sometimes people with OCD also have other mental illnesses, such as anxiety, depression, and body dysmorphic disorder, a disorder in which someone mistakenly believes that a part of their body is abnormal. It is important to consider these other disorders when making decisions about treatment.
It is important to follow your treatment plan because both psychotherapy and medication can take some time to work. Although there is no cure for OCD, current treatments help many people with the disorder manage their symptoms, engage in day-to-day activities, and lead full, active lives.
For tips on how to talk to your health care provider about your mental health and get the most out of your visit, read the National Institute of Mental Health (NIMH) fact sheet, Taking Control of Your Mental Health: Tips for Talking With Your Health Care Provider.
Psychotherapy
Psychotherapy can be an effective treatment for adults and children with OCD. Research shows that certain types of psychotherapy, including cognitive behavioral therapy (CBT) and other related therapies (such as habit reversal training), can be as effective as medication for many people. For others, psychotherapy may be most effective when used in combination with medication.
Research shows that a specific type of CBT called Exposure and Response Prevention (ERP) is effective for reducing compulsive behaviors, even for people who did not respond well to medication. With ERP, people spend time in a situation that triggers their compulsion (such as touching dirty objects) and they are prevented from engaging in their typical compulsion (such as handwashing). Although this approach may cause feelings of anxiety at first, compulsions decrease for most people as they continue treatment.
Children with OCD may need additional help from family members and health care providers when it comes to recognizing and managing their OCD symptoms. Mental health professionals can work with young patients to identify strategies for managing stress and increasing support so that the children are able to manage their OCD symptoms at school and at home.
Mental health professionals can work with young patients to identify strategies for managing stress and increasing support so that the children are able to manage their OCD symptoms at school and at home.
Medication
Your health care provider may prescribe medication to help treat OCD. Serotonin reuptake inhibitors (SRIs) are the most common type of medication prescribed for the treatment of OCD.
SRIs, including selective serotonin reuptake inhibitors (SSRIs), are often used to treat depression, and they also are helpful for treating symptoms of OCD. With SRI treatment, it may take up to 8 to 12 weeks before symptoms begin to improve, and treatment for OCD may require higher SRI doses than are typically used in treating depression. For some people, these medications may cause side effects such as headaches, nausea, or difficulty sleeping.
People respond to medication in different ways, but most people with OCD find that medication, often in combination with psychotherapy, can help them manage their symptoms.
Your health care provider can adjust medication doses over time to minimize any side effects or withdrawal symptoms. Do not stop taking your medication without talking to your health care provider first. Your health care provider will work with you to monitor your health and can adjust the treatment plan in a safe and effective way.
The most up-to-date information on medications, side effects, and warnings is available on the U.S. Food and Drug Administration (FDA) website.
Other Treatments
In 2018, FDA approved the use of transcranial magnetic stimulation (TMS), most commonly used in treating depression, as an add-on treatment for adults with OCD. You can learn more about brain stimulation therapies, including TMS, on the NIMH website.
Beyond Treatment: Things You Can Do
There are several important things you can do to manage stress and anxiety associated with OCD.
- Create a consistent sleep schedule.
- Make regular exercise a part of your routine.

- Eat a healthy, balanced diet.
- Seek support from trusted family and friends.
Where can I go for help?
If you’re not sure where to get help, your health care provider is a good place to start. Your health care provider can refer you to a qualified mental health professional, such as a psychiatrist or psychologist, who has experience treating OCD and can evaluate your symptoms.
You can learn more about getting help and finding a health care provider on NIMH's Help for Mental Illnesses webpage. The Substance Abuse and Mental Health Services Administration (SAMHSA) has an online tool to help you find mental health services in your area.
I know someone who is in crisis. What do I do?
If you or someone you know is having thoughts about wanting to die or is thinking about hurting themselves or someone else, get help quickly.
- Do not leave a person who is in crisis alone.
- Call 911 or go to the nearest hospital emergency room.
- Call the toll-free National Suicide Prevention Lifeline at 1-800-273-TALK (8255). You also can text the Crisis Text Line (text HELLO to 741741) or use the Lifeline Chat on the National Suicide Prevention Lifeline website. These services are confidential, free, and available 24/7.
Participating in Clinical Research
Clinical trials are research studies that look at new ways to prevent, detect, or treat diseases and conditions. Although individuals may benefit from being part of a clinical trial, participants should be aware that the primary purpose of a clinical trial is to gain new scientific knowledge so that others may be better helped in the future.
Researchers at NIMH and around the country conduct many studies with patients and healthy volunteers. Talk to your health care provider about clinical trials, their benefits and risks, and whether one is right for you. For more information, visit NIMH’s clinical trials webpage.
Reprints
This publication is in the public domain and may be reproduced or copied without permission from NIMH. Citation of NIMH as a source is appreciated. To learn more about using NIMH publications, please contact the NIMH Information Resource Center at 1-866‑615‑6464, email [email protected], or refer to our reprint guidelines.
For More Information
MedlinePlus (National Library of Medicine) (En español)
ClinicalTrials.gov (En español)
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
National Institutes of Health
NIH Publication No. 20-MH-4676
Revised 2020
Obsessive-compulsive disorder (OCD) - Symptoms and causes
Overview
Obsessive-compulsive disorder (OCD) features a pattern of unwanted thoughts and fears (obsessions) that lead you to do repetitive behaviors (compulsions). These obsessions and compulsions interfere with daily activities and cause significant distress.
You may try to ignore or stop your obsessions, but that only increases your distress and anxiety. Ultimately, you feel driven to perform compulsive acts to try to ease your stress. Despite efforts to ignore or get rid of bothersome thoughts or urges, they keep coming back. This leads to more ritualistic behavior — the vicious cycle of OCD.
OCD often centers around certain themes — for example, an excessive fear of getting contaminated by germs. To ease your contamination fears, you may compulsively wash your hands until they're sore and chapped.
If you have OCD, you may be ashamed and embarrassed about the condition, but treatment can be effective.
Symptoms
Obsessive-compulsive disorder usually includes both obsessions and compulsions. But it's also possible to have only obsession symptoms or only compulsion symptoms. You may or may not realize that your obsessions and compulsions are excessive or unreasonable, but they take up a great deal of time and interfere with your daily routine and social, school or work functioning.
You may or may not realize that your obsessions and compulsions are excessive or unreasonable, but they take up a great deal of time and interfere with your daily routine and social, school or work functioning.
Obsession symptoms
OCD obsessions are repeated, persistent and unwanted thoughts, urges or images that are intrusive and cause distress or anxiety. You might try to ignore them or get rid of them by performing a compulsive behavior or ritual. These obsessions typically intrude when you're trying to think of or do other things.
Obsessions often have themes to them, such as:
- Fear of contamination or dirt
- Doubting and having difficulty tolerating uncertainty
- Needing things orderly and symmetrical
- Aggressive or horrific thoughts about losing control and harming yourself or others
- Unwanted thoughts, including aggression, or sexual or religious subjects
Examples of obsession signs and symptoms include:
- Fear of being contaminated by touching objects others have touched
- Doubts that you've locked the door or turned off the stove
- Intense stress when objects aren't orderly or facing a certain way
- Images of driving your car into a crowd of people
- Thoughts about shouting obscenities or acting inappropriately in public
- Unpleasant sexual images
- Avoidance of situations that can trigger obsessions, such as shaking hands
Compulsion symptoms
OCD compulsions are repetitive behaviors that you feel driven to perform. These repetitive behaviors or mental acts are meant to reduce anxiety related to your obsessions or prevent something bad from happening. However, engaging in the compulsions brings no pleasure and may offer only a temporary relief from anxiety.
These repetitive behaviors or mental acts are meant to reduce anxiety related to your obsessions or prevent something bad from happening. However, engaging in the compulsions brings no pleasure and may offer only a temporary relief from anxiety.
You may make up rules or rituals to follow that help control your anxiety when you're having obsessive thoughts. These compulsions are excessive and often are not realistically related to the problem they're intended to fix.
As with obsessions, compulsions typically have themes, such as:
- Washing and cleaning
- Checking
- Counting
- Orderliness
- Following a strict routine
- Demanding reassurance
Examples of compulsion signs and symptoms include:
- Hand-washing until your skin becomes raw
- Checking doors repeatedly to make sure they're locked
- Checking the stove repeatedly to make sure it's off
- Counting in certain patterns
- Silently repeating a prayer, word or phrase
- Arranging your canned goods to face the same way
Severity varies
OCD usually begins in the teen or young adult years, but it can start in childhood. Symptoms usually begin gradually and tend to vary in severity throughout life. The types of obsessions and compulsions you experience can also change over time. Symptoms generally worsen when you experience greater stress. OCD, usually considered a lifelong disorder, can have mild to moderate symptoms or be so severe and time-consuming that it becomes disabling.
Symptoms usually begin gradually and tend to vary in severity throughout life. The types of obsessions and compulsions you experience can also change over time. Symptoms generally worsen when you experience greater stress. OCD, usually considered a lifelong disorder, can have mild to moderate symptoms or be so severe and time-consuming that it becomes disabling.
When to see a doctor
There's a difference between being a perfectionist — someone who requires flawless results or performance, for example — and having OCD. OCD thoughts aren't simply excessive worries about real problems in your life or liking to have things clean or arranged in a specific way.
If your obsessions and compulsions are affecting your quality of life, see your doctor or mental health professional.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Causes
The cause of obsessive-compulsive disorder isn't fully understood. Main theories include:
- Biology.
 OCD may be a result of changes in your body's own natural chemistry or brain functions.
OCD may be a result of changes in your body's own natural chemistry or brain functions. - Genetics. OCD may have a genetic component, but specific genes have yet to be identified.
- Learning. Obsessive fears and compulsive behaviors can be learned from watching family members or gradually learned over time.
Risk factors
Factors that may increase the risk of developing or triggering obsessive-compulsive disorder include:
- Family history. Having parents or other family members with the disorder can increase your risk of developing OCD.
- Stressful life events. If you've experienced traumatic or stressful events, your risk may increase. This reaction may, for some reason, trigger the intrusive thoughts, rituals and emotional distress characteristic of OCD.
- Other mental health disorders. OCD may be related to other mental health disorders, such as anxiety disorders, depression, substance abuse or tic disorders.
Complications
Problems resulting from obsessive-compulsive disorder may include, among others:
- Excessive time spent engaging in ritualistic behaviors
- Health issues, such as contact dermatitis from frequent hand-washing
- Difficulty attending work, school or social activities
- Troubled relationships
- Overall poor quality of life
- Suicidal thoughts and behavior
Prevention
There's no sure way to prevent obsessive-compulsive disorder. However, getting treatment as soon as possible may help prevent OCD from worsening and disrupting activities and your daily routine.
By Mayo Clinic Staff
Related
Associated Procedures
treatment, causes, how to deal with obsessive thoughts
Obsessive thoughts (obsessions) are images or urges that uncontrollably, against the will of a person, invade consciousness. Attempts to get rid of these thoughts lead to outbreaks of anxiety and bring great discomfort. A person experiences constant fears and bad thoughts. If you do not seek help in time, obsessions lead to psychological exhaustion, social isolation and depression.
Attempts to get rid of these thoughts lead to outbreaks of anxiety and bring great discomfort. A person experiences constant fears and bad thoughts. If you do not seek help in time, obsessions lead to psychological exhaustion, social isolation and depression.
Obsessive thoughts are found in many diseases: neurosis, depression, obsessive-compulsive disorder (obsessive-compulsive disorder) and even schizophrenia.
Features that distinguish obsessive thoughts syndrome:
- a person cannot influence the appearance of such thoughts, thoughts arise against desire;
- obsessive thoughts are not connected with the usual thoughts of a person - they are separate, alien images;
- the syndrome of obsessive thoughts cannot be overcome by an effort of will;
- the disorder is associated with intense anxiety, irritability;
- clarity of consciousness and critical perception of one's condition are usually preserved.

The disorder is extremely difficult to bear. Usually a person realizes what obsessive thoughts mean, understands all the irrationality of the images that arise in the head, but cannot fight them. Attempts to stop the appearance of thoughts and the coercive actions associated with them are unsuccessful and lead to even greater experiences.
It is not difficult to convince people who suffer from this disorder that their obsessive thoughts have no basis. But it doesn't help to get rid of the problem. Situations repeat themselves over and over. A necessary step to get rid of painful conditions is to seek help from a specialist before complications arise.
What are obsessive thoughts
Obsessive thoughts torment a person, they are unpleasant and disturbing, you want to hide from them, run away. There are all kinds of obsessions.
Here are some examples of intrusive thoughts:
- concerns about pollution and disease;
- pathological need for order and symmetry;
- obsessive and uncontrolled account;
- obsessive thoughts about the bad: a person constantly thinks about accidents that can happen to him, to his relatives, to his property, or even to humanity as a whole;
- groundless and unreasonable avoidance of certain actions or objects;
- religious, sexual, aggressive or any other thoughts that are alien to the patient's thinking and arise against the will.
Constant intrusive thoughts cause unbearable discomfort. Of course, a person has a desire to succumb to these ideas and try to correct the situation. In this case, compulsions appear - actions that a person is forced to periodically perform, even if he does not want to, in order to control what is happening in his head. When obsessive thoughts (obsessions) and obsessive actions (compulsions) are present together, time-consuming, disruptive, and distressing, it indicates the presence of a disease such as obsessive-compulsive disorder (OCD).
A person begins to avoid cracks in the asphalt or touches every tree on the road because alien thoughts “tell” him that if he does not do this, something bad will happen.
Usually compulsions make you do something over and over again, like a ritual. By giving in to coercion, the person hopes that they can prevent or reduce the anxiety that accompanies obsessions. For example, he begins to avoid cracks in the asphalt or touches every tree on the road because alien thoughts "tell" him that if he does not do this, something bad will happen. Unfortunately, such actions do not bring relief and only get worse over time, taking the form of an endless ritual.
Unfortunately, such actions do not bring relief and only get worse over time, taking the form of an endless ritual.
In addition to OCD, there are other diseases in psychiatry that are characterized by different types of obsessive thoughts. Here is some of them:
- phobias,
- neurasthenia,
- schizophrenia.
A phobia is an anxiety disorder characterized by panic and an uncontrollable, irrational fear of certain situations or objects. Strong anxiety can arise even when thinking about a frightening situation, so the patient tries with all his might to avoid a terrible object. All terrible obsessive thoughts and anxieties are associated exclusively with this object.
There are different types of phobias. The most common:
- agoraphobia — fear of open spaces or crowded places;
- social phobia - fear of social interactions. There are other specific phobias that can relate to anything: airplanes, specific animals, the sight of blood.

A phobic disorder may include panic attacks - attacks of fear, which are accompanied by a feeling of impending death and physical sensations: retrosternal pain, interruptions in the heart, dizziness, feeling short of breath, numbness of the extremities, intestinal disorders. All this significantly limits the personal life and performance of a person.
Neurasthenia is a disorder that is associated with exhaustion of the nervous system. It happens after a long illness, physical overload, severe or prolonged stress. Characterized by persistent headache, symptoms of cardiovascular disorders, indigestion and sleep.
Intrusive delusional thoughts may be one of the manifestations of schizophrenia, but the diagnosis is made only in the presence of other signs of schizophrenia.
The disease has three forms-stages that develop one after another. In the hypersthenic form, emotional lability, irritability and intolerance are observed. In the second phase, which is called "irritable weakness", aggression and irritation are quickly replaced by emotional exhaustion and impotence. In the third, hyposthenic form, the patient arrives in a state of constant fatigue and bad mood. He focuses on his inner feelings, which depresses him even more. This phase is characterized by obsessive thoughts of a hypochondriacal nature.
In the second phase, which is called "irritable weakness", aggression and irritation are quickly replaced by emotional exhaustion and impotence. In the third, hyposthenic form, the patient arrives in a state of constant fatigue and bad mood. He focuses on his inner feelings, which depresses him even more. This phase is characterized by obsessive thoughts of a hypochondriacal nature.
Schizophrenia is a complex polymorphic mental illness characterized by a fundamental impairment of perception and the breakdown of thought processes. The clinical picture is varied and depends on the form of the disease: hallucinations, delusions, loss of natural mental functions, personality distortion, and much more.
A sick person who suffers from this disease needs full treatment from a psychiatrist. Intrusive delusional thoughts may be one of the manifestations of schizophrenia, but the diagnosis is made only in the presence of other signs that are specific, diagnostically significant criteria for this disorder.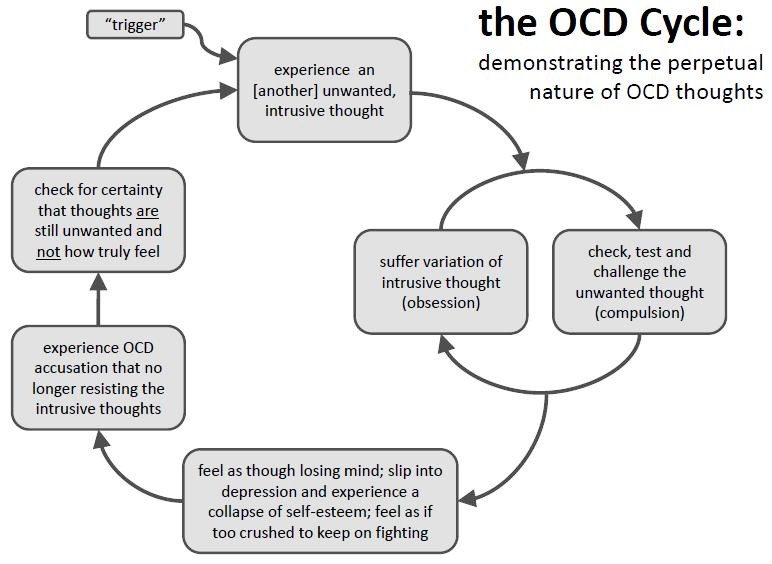
Causes of obsessive thoughts
The occurrence of obsessions is directly related to the underlying disease. For treatment to be effective, an accurate diagnosis is essential. It is not always possible to accurately answer the question of where obsessive thoughts come from. Factors that contribute to the occurrence of this disorder have been identified:
- genetic predisposition;
- brain dysfunction due to organic or biochemical causes, including imbalance of neurotransmitters;
- mental trauma and stress;
- personality traits: people with sensitive and labile temperament;
- the presence of somatic and infectious diseases, disability, pregnancy are predisposing causes of obsessive thoughts.
There are many disorders in which this syndrome occurs, so the diagnosis should be carried out by a highly qualified psychiatrist who can understand the intricacies of the clinical picture and understand why obsessive thoughts arise. When conducting diagnostics, the following methods are used:
When conducting diagnostics, the following methods are used:
- Psychiatric examination: a specialist will collect an anamnesis, understand the clinical manifestations and personal characteristics of each patient.
- Pathopsychological study: an effective and comfortable technique that, with the help of special experiments, surveys and observations, allows you to conduct a qualitative analysis of mental disorders and understand why obsessive thoughts come.
- Laboratory and instrumental examination: modern diagnostic tests, such as Neurotest and Neurophysiological test system, allow assessing the severity of pathological processes and making an accurate differential diagnosis. Functional methods will help to exclude organic pathology.
How to deal with obsessive thoughts
Mental illnesses that underlie the syndrome in question are a reason to immediately consult a psychiatrist. The symptoms vary greatly, and it is not always easy to notice the distinctive features. Therefore, it is necessary to address the question of what to do with obsessive thoughts to an experienced specialist.
Therefore, it is necessary to address the question of what to do with obsessive thoughts to an experienced specialist.
It happens that a person is afraid to seek help or tries to independently find a way to cope with obsessive thoughts that are so annoying. One of the most common decisions is the use of alcohol and drugs. If a person manages to be distracted, the illusion may be created for a short time that the problem has disappeared. In fact, the situation is only getting worse. You should not try to "kill" intrusive thoughts in this way, because it is likely that obsessions will only intensify when intoxicated.
Talk to someone you trust, such as your parents or friends. A great option is to go to group therapy, in a society of people with similar problems. This will allow you to share experiences and get support.
The consequences of drinking alcohol can be unpredictable. Even if there is a brief relief, thoughts will still arise again, and with even greater force. As a result, new health problems are added, dependence on alcohol or drugs develops, and the disorder worsens. With neurosis of obsessive thoughts, only a specialist will tell you how to get rid of or alleviate the condition.
As a result, new health problems are added, dependence on alcohol or drugs develops, and the disorder worsens. With neurosis of obsessive thoughts, only a specialist will tell you how to get rid of or alleviate the condition.
In addition to the stages of treatment that the doctor will select for you, you need to remember about self-control, rehabilitation and prevention. Here are a few tips beyond basic treatment to help you deal with intrusive thoughts:
- Learn more about your disorder. Learning about your condition will help you quickly accept the problem, calm down and motivate you to better adhere to the treatment plan.
- Talk to someone you trust, such as your parents or friends. A great option is to go to group therapy, in a society of people with similar problems. This will allow you to share experiences and get support.
- Normalization of lifestyle: proper sleep, diet, avoidance of alcohol and strong psychotropic substances, moderate physical activity.
- Do not give up your normal activities. Build a career, study, devote time to your favorite hobby. Spend time with family and friends. Don't let illness interfere with your life.
- Avoid Stress: The idea that a strong outburst of emotions will make the fight against obsessive thoughts more effective is false. It will be possible to be distracted only for a short time, but then the nervous system will become even more vulnerable.
Treatment of obsessive thoughts
With the help of modern medicine, it is possible to mitigate the intensity of manifestations, and often completely get rid of obsessions and compulsions.
For obsessive thoughts syndrome, treatment is most effective when combined with psychotherapy and medication. In some cases, one thing is enough. A competent specialist will select an individual program, which will depend on the clinical picture and the severity of the condition.
For obsessive thoughts, treatment may consist of psychotherapy and pharmacotherapy.
Psychotherapy allows you to fully analyze the situation and work out behavioral, psychological and social problems. Communication with a highly qualified psychotherapist teaches you how to manage symptoms, overcome fears and protect yourself from stress. The arsenal of a modern specialist includes cognitive behavioral therapy, hypno-suggestive techniques, auto-training and other effective approaches. Psychotherapy for obsessive thoughts is a key treatment that will help you understand the problem and deal with it.
Pharmacotherapy. Modern medicines help to correct neurotic symptoms, relieve fear and anxiety, and keep mood under control. Mild antidepressants, antipsychotics and tranquilizers are used.
Fortunately, modern psychiatry knows how to cure obsessive thoughts, reduce or completely eliminate symptoms. Thanks to effective treatment and rehabilitation provided by a competent specialist, patients return to an active life without fears and restrictions.
Obsessive thoughts - how it works and principles of self-help
Obsessive thoughts - how it works and principles of self-help
What supports obsessive thoughts/images?
- Traumatic experience experienced (accident, death/injury of a person, participation in hostilities, other events that caused strong emotional experiences, usually negative). Otherwise, such a phenomenon is called psychopathological re-experiencing, or flashback. A bit of a separate topic, because. can occur in any person not because of his personal qualities, inclinations, response characteristics that predispose him to the emergence of stable obsessive thoughts, but because of the severity of the experience. Such phenomena can often pass quickly enough with the use of certain psychotherapeutic techniques, for example, EMDH.
- Excessive control, the desire to control what is impossible to control. During a boring conversation, the mind of any person begins to wander.
 Just because you can think purposefully doesn't mean you can control your thinking. There are thoughts of insight, and there are uncontrollable thoughts of the opposite plan that are unpleasant to us, frighten us, cause horror, disgust, shame, etc. It's like trying to control dreams - just let them dream. And if such thoughts are comparable for you to nightmares from which you wake up in a sweat, then, of course, it is simply impossible not to do anything, however, fighting them with direct confrontation is the same as cutting off the heads of the Lernean Hydra (the mythical many-headed hydra, - if you cut her head, then two new heads immediately grew in its place). Because the more attention you give to such thoughts, the more meaningful they become. The more you try to control them and fight them, the more attention and importance you yourself give them.
Just because you can think purposefully doesn't mean you can control your thinking. There are thoughts of insight, and there are uncontrollable thoughts of the opposite plan that are unpleasant to us, frighten us, cause horror, disgust, shame, etc. It's like trying to control dreams - just let them dream. And if such thoughts are comparable for you to nightmares from which you wake up in a sweat, then, of course, it is simply impossible not to do anything, however, fighting them with direct confrontation is the same as cutting off the heads of the Lernean Hydra (the mythical many-headed hydra, - if you cut her head, then two new heads immediately grew in its place). Because the more attention you give to such thoughts, the more meaningful they become. The more you try to control them and fight them, the more attention and importance you yourself give them. - Giving excessive attention and importance to these thoughts which we have already touched upon in the previous paragraph.
 They seem to become overvalued if you constantly fight them. But what if they are like horror and a nightmare? We will talk about this further.
They seem to become overvalued if you constantly fight them. But what if they are like horror and a nightmare? We will talk about this further. - Fear that thoughts can become actions. The logic is this: if my thoughts do not obey me, then where is the guarantee that my actions will not become uncontrolled? In fact, it rather depends on the innate temperament - the type of reaction of the nervous system. There are people with predominant impulsiveness - they first react, act, and then cognitive processing takes place, then thoughts. And there are people who will think everything over, sometimes it’s too late to do it, but they thought everything through. And it's like two separate railway tracks, which are laid in such a way that one does not pass into the other. If you think obsessive thoughts while others act impulsively, then you can not disturb yourself in vain: it is as if you are walking on a different railway track, you have a different type of response of the nervous system.
 (In obsessive-compulsive disorder, both obsessive thoughts and compulsive actions occur, but actions are performed to prove that obsessive thoughts are erroneous, far-fetched, they are not actions confirming these thoughts and arise as an apotheosis of direct opposition to obsessive thoughts. For example, a person who has obsessive thoughts about a fire in the house because the iron is not turned off, can check several times before leaving and after leaving the house whether the iron is plugged in. He will not impulsively start a fire in the house, which obsessive thoughts scare him, but will do the opposite). You decide what actions to take, guided by your own will, mood, personal preferences, and also depending on your personality type. And if you have all this, then where will it disappear, and what kind of cow can lick all these characteristics of yours with its tongue so that they don’t remain, and you begin to be guided by behavior incomprehensibly by what? You just struggle with obsessive thoughts, and they fight back - they scare you, including impossible things.
(In obsessive-compulsive disorder, both obsessive thoughts and compulsive actions occur, but actions are performed to prove that obsessive thoughts are erroneous, far-fetched, they are not actions confirming these thoughts and arise as an apotheosis of direct opposition to obsessive thoughts. For example, a person who has obsessive thoughts about a fire in the house because the iron is not turned off, can check several times before leaving and after leaving the house whether the iron is plugged in. He will not impulsively start a fire in the house, which obsessive thoughts scare him, but will do the opposite). You decide what actions to take, guided by your own will, mood, personal preferences, and also depending on your personality type. And if you have all this, then where will it disappear, and what kind of cow can lick all these characteristics of yours with its tongue so that they don’t remain, and you begin to be guided by behavior incomprehensibly by what? You just struggle with obsessive thoughts, and they fight back - they scare you, including impossible things. Well, how impossible - very unlikely. This can happen in acute psychosis, when consciousness, perception, often memory become clouded, then the behavior behind them all becomes inadequate, but these are rare phenomena and are in no way associated with obsessive thoughts, they can rather be associated with a long history of alcohol, with schizophrenia , dementia, etc.
Well, how impossible - very unlikely. This can happen in acute psychosis, when consciousness, perception, often memory become clouded, then the behavior behind them all becomes inadequate, but these are rare phenomena and are in no way associated with obsessive thoughts, they can rather be associated with a long history of alcohol, with schizophrenia , dementia, etc. - Self-flagellation about the fact that "others would not have thought of it", a judgment that thoughts allegedly speak about a person's character or about his intentions. Character is shown in the way you lead your life. It is about what you decide to do or not do. Thoughts are just flashes in your mind. It is not you who decides whether thoughts arise or not. Your character is not shown in any way if there is no place for making a decision. A thought is not a fact or a statement about you as a person. Character is the decisions you make in life, not something that randomly pops into your mind.

- The belief that the more you think about something, the more likely it is to happen. The belief that thoughts are material. Here, certain features of perception play against a person. It is more true, I think, to say that the more you think about something, the more likely you are to notice and remember that it happened. And if the way we think does not happen, then our psyche tends to forget it as a failure, as a mismatch, as a failed connection (the synthesis of the two parts failed), as something unimportant. The brain analyzes and synthesizes, this is its job. What has not succumbed to synthesis does not deserve special attention. Therefore, we tend to remember those moments when our thoughts became reality, and many thoughts that cannot be connected with reality simply go unnoticed and unappreciated, and can emerge even after a long time if the brain finds for one of such old, abandoned thoughts communication in the real world. Therefore, people tend to remember those few forebodings that were justified (because they had personal significance), forgetting about the numerous cases when all doubts and fears were not justified in any way by subsequent events.
 Thoughts themselves are often based on guesses about the world around us and how it works, on our previous personal experience, etc. Thoughts rather influence whether we will try to do something, whether we will be afraid of what something to do, etc. They affect our attitude towards reality and our response rather than changes in reality per se.
Thoughts themselves are often based on guesses about the world around us and how it works, on our previous personal experience, etc. Thoughts rather influence whether we will try to do something, whether we will be afraid of what something to do, etc. They affect our attitude towards reality and our response rather than changes in reality per se. - The conviction that every thought is worthy of attention, and repetitive thoughts are of particular importance. Our consciousness and brain function in general can be compared to cable television. And sometimes our attention to our inner world can for a moment switch to one of the unnecessary, uninteresting, not characteristic of us or even alien to us channels - this moment can become an obsessive thought if we give it significance and start fighting it. Especially if you also believe that all thoughts are worth paying attention to, and that there are no and should not be useless channels in the mind. Then your attention may be absorbed by meaningless nonsense.
 If you begin to act impartially towards such useless thoughts, and not fight them just because they are, and if in the end you admit that they have no meaning, then in time they will simply disappear.
If you begin to act impartially towards such useless thoughts, and not fight them just because they are, and if in the end you admit that they have no meaning, then in time they will simply disappear.
Regarding the greater importance of repetitive thoughts - we have already discussed this feature of perception, that thoughts are repeated the more often, the more importance we attach to them - both in a positive context (we think about something with interest), and in a negative one (obsessive thoughts ). However, in a positive context, we do not make a problem out of it, and in a negative one, we can make a big problem over time if we try. It is as if a whole searchlight is directed at this thought - as soon as its significance increases - if this thought is tacitly declared a problem. However, if the issue is already declared, i.e. in fact, you feel that this is a problem for you, then just saying that this is not a problem can be tantamount to a waste of time. We need consistent actions, an analysis of our feelings and experiences.
- Strengthening the “importance of thought” on a sensory level. Here's how it works: when you're frightened or surprised or in danger, the area of the brain responsible for signaling alarms (amygdala/amygdala) sends signals of danger. In a stressful situation, the biological systems of the body are activated, supporting a clear strategy of behavior: “fight/flight/freeze”. Such a reaction occurs automatically, regardless of whether a false threat exists or a real one. The amygdala is not "specially smart". And it can't tell a real threat from a false signal. She just reacts to the trigger - real/imaginary - in the only way she can. She sends out an alarm. If you are frightened by a thought, and the amygdala automatically gives out a signal of danger, then the emotional reaction will be the same as in real danger. Feelings in the body appear such that the thought may seem dangerous or very important. But neurons in the cerebral cortex analyze and are able to distinguish a real threat from an apparent one.
 The cortex is responsible for rational thinking and judgment. The problem is that the impulses from the higher brain arrive about half a second later than the first automatic alarm. Therefore, the feeling of danger arises before the cerebral cortex has the opportunity to intervene. And we tend to consider the first impulse to be true and true, so we can no longer listen to the second, devalue it, wind ourselves up and worsen our life out of the blue.
The cortex is responsible for rational thinking and judgment. The problem is that the impulses from the higher brain arrive about half a second later than the first automatic alarm. Therefore, the feeling of danger arises before the cerebral cortex has the opportunity to intervene. And we tend to consider the first impulse to be true and true, so we can no longer listen to the second, devalue it, wind ourselves up and worsen our life out of the blue.
For lovers of a deeper understanding of the work of the brain - a paragraph about the peculiarities of the response of the amygdala, which in general we have already discussed in the previous paragraph. The amygdala (tonsil) can only be in two states - active or passive. Since the purpose is to warn you, the amygdala is activated at the slightest hint of a possible threat. Her job is to protect you, not to take care of your comfort, so she would rather give a thousand false signals and cause as many panic attacks when there is no problem than miss even one real danger. Initially, it was supposed to provide primitive survival. She reacts very quickly, trying to protect you from any possible threat. The amygdala learns to be afraid: loud noises and loss of support are two innate fear triggers. Children begin to use protective behavior near a hot stove, a socket, a sharp knife much later. The amygdala in people with obsessive thoughts has learned to "ring the alarm bell" because of certain thoughts. Now imagine if someone came up behind you and scared you with a loud sound, the startle reaction starts instantly. But then, turning around and realizing that this is such a stupid joke and nothing terrible happened, your fear passes. In this example, I will talk about two neural pathways to the amygdala. Loud sound comes from the ear through different structures, transforming into nerve impulses. Reaching the thalamus (the "control panel" in the brain), they are sent to the amygdala (one way) and to the cortex, where the signal that something may be wrong is analyzed, compared with additional factors, and the result is also sent to the amygdala (one more way).
Initially, it was supposed to provide primitive survival. She reacts very quickly, trying to protect you from any possible threat. The amygdala learns to be afraid: loud noises and loss of support are two innate fear triggers. Children begin to use protective behavior near a hot stove, a socket, a sharp knife much later. The amygdala in people with obsessive thoughts has learned to "ring the alarm bell" because of certain thoughts. Now imagine if someone came up behind you and scared you with a loud sound, the startle reaction starts instantly. But then, turning around and realizing that this is such a stupid joke and nothing terrible happened, your fear passes. In this example, I will talk about two neural pathways to the amygdala. Loud sound comes from the ear through different structures, transforming into nerve impulses. Reaching the thalamus (the "control panel" in the brain), they are sent to the amygdala (one way) and to the cortex, where the signal that something may be wrong is analyzed, compared with additional factors, and the result is also sent to the amygdala (one more way). This path is about half a second longer. This means that you get scared before you know the reason, and this is due to the neurophysiology of the brain. Your reaction in such a case is swift, automatic and unavoidable. The first fright passes quickly if the amygdala receives a message from the cerebral cortex that the trigger was not a threat. Assuming that the first fright attack is a reaction to the obsessive thought that you could jump off the balcony, then you might think: “Does this mean that I have suicidal tendencies that I did not know about?” or “How can you be sure it won’t happen?” etc. Thus, you would give a signal to the amygdala to continue to sound the alarm (to catch up with yourself a secondary fear, which can also increase the feeling of danger several times from the original).
This path is about half a second longer. This means that you get scared before you know the reason, and this is due to the neurophysiology of the brain. Your reaction in such a case is swift, automatic and unavoidable. The first fright passes quickly if the amygdala receives a message from the cerebral cortex that the trigger was not a threat. Assuming that the first fright attack is a reaction to the obsessive thought that you could jump off the balcony, then you might think: “Does this mean that I have suicidal tendencies that I did not know about?” or “How can you be sure it won’t happen?” etc. Thus, you would give a signal to the amygdala to continue to sound the alarm (to catch up with yourself a secondary fear, which can also increase the feeling of danger several times from the original).
- Fixing unnecessary associative connections in the brain. Our thinking creates many associations: "up-down", "north-south", "more-less", etc. So in general, nerves that react simultaneously - as if soldered together, are associated with each other (the concept of conditioning).
 Overcoming intrusive thoughts involves creating new associations that eliminate fear.
Overcoming intrusive thoughts involves creating new associations that eliminate fear.
Anxious thinking - a change in the state of consciousness when the amygdala is activated. Its characteristics:
- Merging thoughts and actions, imagination and experience of the situation. Questions like “What if…?” no longer look like conjectures, but are perceived as a reliable vision of the future. Thoughts seem to be predictions. "Fear has big eyes".
- All risks seem unreasonable. Anxious thinking requires absolute guarantees that the nightmares you may have thought will not happen. Everything else is cause for continued concern. Uncertainty is unbearable. Any uncertainty is perceived as a threat. And to complete this picture of the post-apocalypse, it should be noted that the brain during anxious thinking is in a functional mode of increased sensitivity to the threat.
- Thoughts tend to become intrusive.
 They seem to get stuck in the mind.
They seem to get stuck in the mind.
Some Exercises
Now imagine opening the following email: “Congratulations! Your lucky day has come. Your distant relative, who headed the diamond corporation in Chicago, died, leaving you a legacy of 14 billion dollars. To receive the inheritance, please follow the link below and provide us with your bank details for money transfer. Once again, let me congratulate you from the bottom of my heart."
Will you send this letter to spam or will you study and think about its content for a long time and in detail, about why it was sent to you, why now, etc.? If you just spam it, then why don't you do the same with intrusive thoughts?
An exercise explaining the mechanism of involvement.
- Please answer how strong emotional connotation do the words “cut” and “transfer” have for you (from 1 to 10)?
- Delete the letters from each word so that "beat" and "betray" remain.
 How powerful are these words?
How powerful are these words? - Now go back to the words "hack" and "transfer". Has their emotional perception changed?
If it has changed in the direction of strengthening, then you have become emotionally involved, because the words have emotional associations with other words that you cannot yet ignore. These words may already seem negative, speaking of danger, unpleasant. But words are just words. They don't have any color until you start to interpret them, and then it becomes very easy to get involved in the process.
Solving the problem
Alternative methods to what will be offered here may help someone, and they may even make someone worse. For example, prayer can reduce anxiety, but it can also increase involvement in those intrusive thoughts that a person wants to forget. Yoga and meditation can be used by a person who is intrinsically motivated to reduce the tendency to get "stuck in the mind" and get involved in thoughts, or maybe motivated to learn to control thoughts. In the latter case, the condition is likely to worsen.
In the latter case, the condition is likely to worsen.
This article suggests the following: acceptance of these thoughts. One should actively allow thoughts to emerge, not wanting them to disappear, because. it helps to realize that they are not important. Concentrate not on the result of a false alarm given by an overly cautious amygdala, but on how your thoughts are not an alarm signal to the amygdala.
You should also practice allowing reasonable uncertainty in your life. Certainty is a feeling, not a fact. If you continue to reassure yourself, then you can never get used to the fact that there is uncertainty in life, and constantly worry about this. Try to focus on the present as well. if you think about the future, you think about more uncertainty than if you think about the present. Yet too much uncertainty is hardly a good atmosphere for the absence of anxiety. Therefore, accept the uncertainty that cannot be reduced in a natural way, and if the uncertainty can be reduced without sacrificing anything, then do it. For example, focus on the present rather than the future. What do you hear, what do you feel, is it cold now or hot? These are simple questions for yourself in a more definite present that is and exists.
For example, focus on the present rather than the future. What do you hear, what do you feel, is it cold now or hot? These are simple questions for yourself in a more definite present that is and exists.
Feeling the need to do something urgently (panic) when obsessive thoughts arise - also arises from an attempt to deal with uncertainty. Panic sensations indicate discomfort, not danger, and discomfort should be tolerated if it proves to the brain that this discomfort is not dangerous. Actively and in a panic try to do something - like putting out a fire, fanning the flame. It happens that passivity is much more effective than effort. It's like peeling off a crust from a wound - supposedly it will pass faster, heal faster. Sometimes you just need to understand how to wait for the right time so as not to interfere with natural processes to fade away on their own.
False response of the brain makes one consider the thought dangerous and stay away from it, and in order to retrain the amygdala, one must evoke a reaction in it and then show that in this case there is no danger. So she will be retrained. And if you stay away from these thoughts, then they will be associated with danger, and with a decrease in cortical control (during stress, discomfort, in some situation reminiscent of these thoughts, etc.), they will be able to arise again and remind themselves through panic and a sense of danger that the amygdala will turn on. The amygdala learns not to be afraid only when the fear response is activated. To compromise and evoke in your mind not the most terrible thoughts of those that periodically torment you means forgetting that any thoughts are just thoughts. The best results come from regular practice in a variety of situations and conditions.
So she will be retrained. And if you stay away from these thoughts, then they will be associated with danger, and with a decrease in cortical control (during stress, discomfort, in some situation reminiscent of these thoughts, etc.), they will be able to arise again and remind themselves through panic and a sense of danger that the amygdala will turn on. The amygdala learns not to be afraid only when the fear response is activated. To compromise and evoke in your mind not the most terrible thoughts of those that periodically torment you means forgetting that any thoughts are just thoughts. The best results come from regular practice in a variety of situations and conditions.
Intrusive thoughts seem so frightening because the anxious type of thinking wins and the thought begins to look extremely plausible. You can compare the tormenting obsessive thoughts with a fairy-tale city, where the road of fear is the central one. If you use the method suggested here to dispel these intrusive thoughts, you can imagine that you are building a freeway next to the road of fear in this city.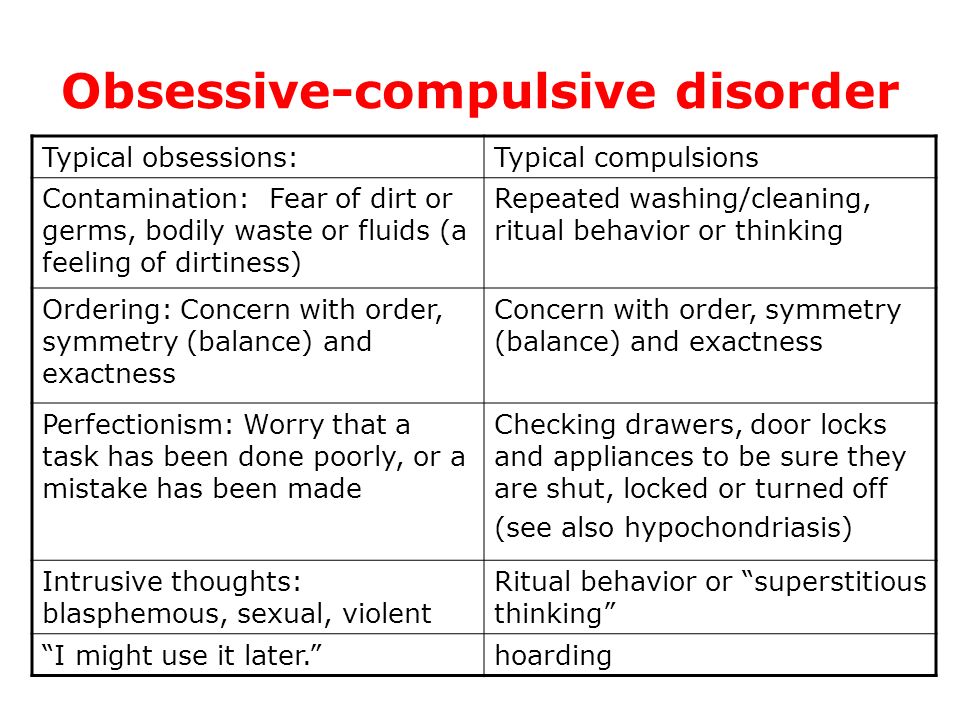 As a result, the built motorway will be used more and more often, because. this is energy-efficient (the brain exists according to the laws of conservation of energy, and if we offer a less energy-consuming option for solving a problem, in particular, dealing with obsessive thoughts, then this option is most likely to take root). But the path of fear has not disappeared either. Fear may arise even after many years, during times of stress or extreme fatigue, etc., but this does not mean that your achievements will be lost in an instant. The achievement is that the freeway is used much more often. This achievement is still with you, even if one or more cars drove along the old road. It is important to understand this in order not to destroy your own achievements, accepting for the truth that supposedly everything has returned to what it started. If you allow this fear into yourself, then this can indeed happen, but this can all become so only because you agreed with the amygdala's false signal of danger and also confirmed the almost emergency situation in the city with this thought that “everything comes back”, or “everything came back”, or “it didn’t work out for me again”, well, or “this method didn’t work either”.
As a result, the built motorway will be used more and more often, because. this is energy-efficient (the brain exists according to the laws of conservation of energy, and if we offer a less energy-consuming option for solving a problem, in particular, dealing with obsessive thoughts, then this option is most likely to take root). But the path of fear has not disappeared either. Fear may arise even after many years, during times of stress or extreme fatigue, etc., but this does not mean that your achievements will be lost in an instant. The achievement is that the freeway is used much more often. This achievement is still with you, even if one or more cars drove along the old road. It is important to understand this in order not to destroy your own achievements, accepting for the truth that supposedly everything has returned to what it started. If you allow this fear into yourself, then this can indeed happen, but this can all become so only because you agreed with the amygdala's false signal of danger and also confirmed the almost emergency situation in the city with this thought that “everything comes back”, or “everything came back”, or “it didn’t work out for me again”, well, or “this method didn’t work either”.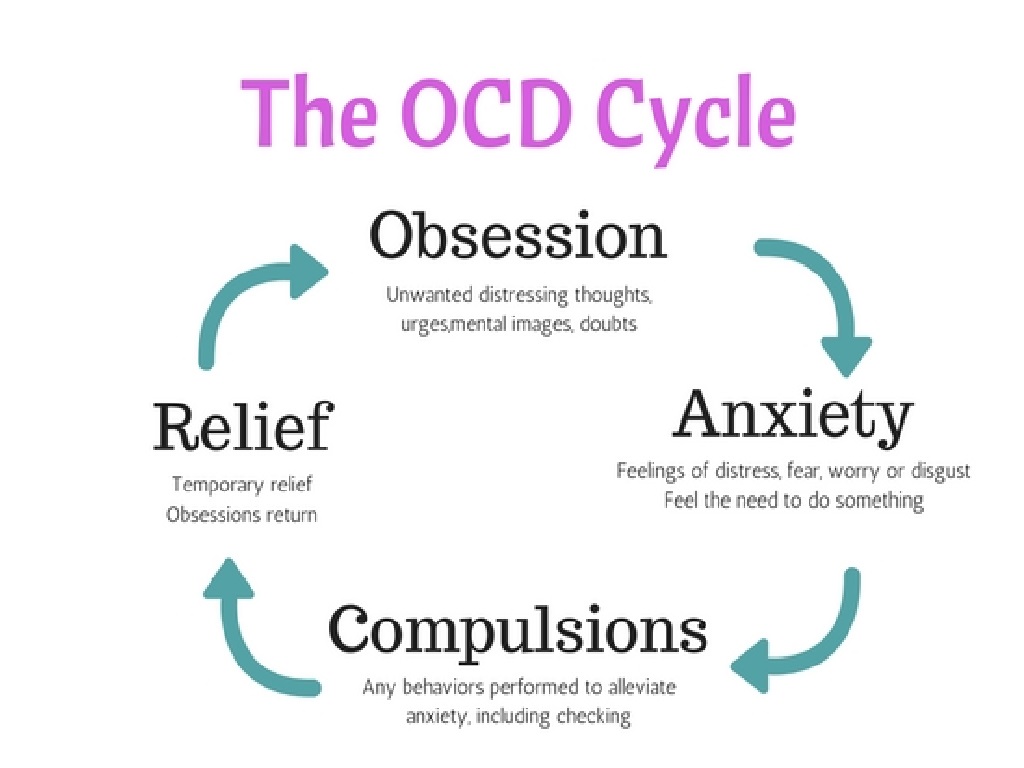 If you switch to the fact that nothing terrible has happened, these are just thoughts and you are able to endure these thoughts, then further on, based on its properties, the brain will continue to use and strengthen new mechanisms that are not associated with fear. This will become possible because you will remove the imaginary danger mode, and the brain will no longer need to solve the primary task - to survive.
If you switch to the fact that nothing terrible has happened, these are just thoughts and you are able to endure these thoughts, then further on, based on its properties, the brain will continue to use and strengthen new mechanisms that are not associated with fear. This will become possible because you will remove the imaginary danger mode, and the brain will no longer need to solve the primary task - to survive.
Here is an example of a possible internal dialogue: (after the dialogue, the division of the replicas into certain colors is deciphered, but I recommend that you just read first, then familiarize yourself with what the colors mean and read it again) *
- What if this does not work? What if I lose control of myself so much that I actually do what I fear?
- Don't be stupid, drop all these thoughts. This has happened so many times already, and not once did thoughts turn into actions.
- Please don't react to these thoughts. These are just thoughts.
- No, it will drive me crazy someday!
- You shouldn't even answer these thoughts.
- It really can happen, what will you do then?
- This is just an obsessive thought. Thought is just a thought.
- Oh, I might have a nervous breakdown right now from all this!
- However, I accept these thoughts and allow them to manifest. I have already tried other methods of struggle, you should not return to them.
- WHAT IF I CAN'T CONTROL MYSELF?
- I know that some other obsessive thought may follow.
- I don't think I can take it anymore!
- Let the time pass.
- I'm so worried about all this. What if I never settle down?
- I relax and observe.
- What if I actually do it?
- It's not even worth answering this question.
- Not sure if I can control myself.
- I allow thoughts to manifest.
- (softly) This has been going on for so long. What if it never stops?
- I accept thoughts
- (even more subtly) I'm not sure I can control myself.