Symptoms of effexor
Side effects of venlafaxine - NHS
Like all medicines, venlafaxine can cause side effects in some people, but many people have no side effects, or only minor ones.
Some of the common side effects of venlafaxine will gradually improve as your body gets used to it.
Common side effects
These common side effects of venlafaxine happen in more than 1 in 100 people. There are things you can do to help cope with them:
Feeling sick (nausea)Try taking venlafaxine with or after food. It may also help if you avoid rich or spicy food. If it carries on, tell your doctor.
Sweating and hot flushesTry wearing loose clothing and using or a fan, where possible. If there is no improvement after a week, speak to your doctor.
Make sure you rest, and drink plenty of fluids. It’s also best to avoid drinking too much alcohol. Ask your pharmacist to recommend a painkiller.
Headaches usually go away after the first week of taking venlafaxine. Talk to your doctor if they last longer than a week or are severe.
A dry mouthChew sugar-free gum or sugar-free sweets.
Feeling dizzyIf venlafaxine makes you feel dizzy when you stand up, try getting up very slowly or stay sitting down until you feel better. If you begin to feel dizzy, lie down so that you do not faint, then sit until you feel better.
Do not drive, ride a bike or use tools or machinery if you feel dizzy.
Feeling sleepyDo not drive, ride a bike or use tools or machinery if you're feeling sleepy. Cut down the amount of alcohol you drink as this will make you feel more tired. If this symptom does not go away after a week or two, ask your doctor for advice.
If this symptom does not go away after a week or two, ask your doctor for advice.
Take venlafaxine first thing in the morning.
ConstipationGet more fibre into your diet such as fresh fruit and vegetables and cereals, and drink plenty of water. Try to exercise, for example, by going for a daily walk or run. If this does not help, talk to your pharmacist or doctor.
If this advice does not help and any of these side effects bother you, talk to your doctor or pharmacist.
Serious side effects
It's not common, but some people (less than 1 in 100) may have serious side effects when taking venlafaxine.
Book an appointment with your doctor if:
- you gain weight or lose weight without trying
- you have changes in your periods such as heavy bleeding, spotting, or bleeding between periods
Call your doctor or contact 111 now if:
- you get constant headaches, long-lasting confusion, weakness, or frequent muscle cramps – these can all be signs of low sodium levels in your blood you have feelings of overwhelming happiness (euphoria), excessive enthusiasm or excitement, or a feeling of restlessness that means you cannot sit or stand still
- you have unexplained muscle pain or weakness
- the whites of your eyes or skin turn yellow, although this may be less obvious on black or brown skin – this can be a sign of liver problems
- you have any changes in your eyesight, like blurred vision or dilated pupils
- you cough up blood or have blood in your pee
- you have black or red poo, or blood in your vomit – these can be signs of bleeding in the stomach
- you are bleeding from the gums, or have bruises that appear without a reason or that get bigger
- you get shortness of breath, or a fast or irregular heart beat
- you have thoughts about harming yourself or ending your life
Go to 111. nhs.uk or call 111.
nhs.uk or call 111.
Immediate action required: Call 999 now if:
- you get chest pain or pressure in your chest, shortness of breath, or a fast or irregular heart beat
Serious allergic reaction
In rare cases, it's possible to have a serious allergic reaction (anaphylaxis) to venlafaxine.
Immediate action required: Call 999 or go to A&E now if:
- you get a skin rash that may include itchy, red, swollen, blistered or peeling skin
- you're wheezing
- you get tightness in the chest or throat
- you have trouble breathing or talking
- your mouth, face, lips, tongue or throat start swelling
You could be having a serious allergic reaction and may need immediate treatment in hospital.
Long-term side effects
For most people, venlafaxine is safe to take for a long time and there are no lasting effects.
A few people may get sexual side effects, such as problems getting an erection or a lower sex drive. In some cases these can continue even after stopping the medicine. Speak to your doctor if you are worried.
Other side effects
These are not all the side effects of venlafaxine. For a full list, see the leaflet inside your medicine packet.
Information:
You can report any suspected side effect using the Yellow Card safety scheme.
Visit Yellow Card for further information.
Page last reviewed: 10 February 2022
Next review due: 10 February 2025
Venlafaxine (Effexor) | NAMI: National Alliance on Mental Illness
Brand names:
- Effexor®
- Tablets (immediate release): 25 mg, 37.
 5 mg, 50 mg, 75 mg, 100 mg
5 mg, 50 mg, 75 mg, 100 mg
- Tablets (immediate release): 25 mg, 37.
- Effexor XR®
- Capsules (extended release): 37.5 mg, 75 mg, 150 mg
- Venlafaxine
- Tablets (extended release): 37.5, 75 mg, 150 mg, 225 mg
- Tablets (immediate release): 25 mg, 37.5 mg, 50 mg 75, mg 100 mg
Generic name: venlafaxine (ven la FAX een)
All FDA black box warnings are at the end of this fact sheet. Please review before taking this medication.
What Is Venlafaxine And What Does It Treat?
Venlafaxine is an antidepressant medication that works in the brain. It is approved for the treatment of major depressive disorder (MDD), generalized anxiety disorder (GAD), panic disorder, and social anxiety disorder (social phobia).
Symptoms of depression include:
- Depressed mood - feeling sad, empty, or tearful
- Feeling worthless, guilty, hopeless, and helpless
- Loss of interest or pleasure in your usual activities
- Sleep and eat more or less than usual (for most people it is less)
- Low energy, trouble concentrating, or thoughts of death (suicidal thinking)
- Psychomotor agitation (‘nervous energy’)
- Psychomotor retardation (feeling like you are moving and thinking in slow motion)
- Suicidal thoughts or behaviors
Generalized Anxiety Disorder (GAD) occurs when a person experiences excessive anxiety or worry for at least six months. Other symptoms include:
Other symptoms include:
- Restlessness
- Fatigue (low energy, feeling tired all the time)
- Difficulty concentrating
- Irritability
- Muscle tension
- Sleep disturbance (difficulty falling asleep or waking up in the middle of the night)
Panic Disorder occurs when a person experiences unexpected and repeated episodes of intense fear. These episodes have physical symptoms including chest pain, shortness of breath, heart palpitations, sweating, dizziness, and nausea. Fear of future episodes is also part of panic disorder.
Social phobia/social anxiety disorder is a fear of situations where one may feel as if they are being judged by others. Symptoms include:
- Blushing
- Difficulty talking
- Nausea
- Sweating
- Shaking
Venlafaxine may also be helpful when prescribed “off-label” for attention-deficit/hyperactivity disorder (ADHD) in adults and children/adolescents, diabetic neuropathy, migraine prevention, hot flashes, obsessive compulsive disorder (OCD), posttraumatic stress disorder (PTSD), and premenstrual dysphoric disorder (PMDD) . “Off-label” means that it hasn't been approved by the Food and Drug Administration for this condition. Your mental health provider should justify his or her thinking in recommending any “off-label” treatment. They should be clear about the limits of the research around that medication and if there are any other options.
“Off-label” means that it hasn't been approved by the Food and Drug Administration for this condition. Your mental health provider should justify his or her thinking in recommending any “off-label” treatment. They should be clear about the limits of the research around that medication and if there are any other options.
What Is The Most Important Information I Should Know About Venlafaxine?
Do not stop taking venlafaxine, even when you feel better. With input from you, your health care provider will assess how long you will need to take the medicine.
Missing doses of venlafaxine may increase your risk for relapse in your symptoms.
Stopping venlafaxine abruptly may result in one or more of the following withdrawal symptoms: irritability, nausea, feeling dizzy, vomiting, nightmares, headache, and/or paresthesias (prickling, tingling sensation on the skin).
Depression is also a part of bipolar illness. People with bipolar disorder who take antidepressants may be at risk for "switching" from depression into mania. Symptoms of mania include "high" or irritable mood, very high self-esteem, decreased need for sleep, pressure to keep talking, racing thoughts, being easily distracted, frequently involved in activities with a large risk for bad consequences (for example, excessive buying sprees).
Symptoms of mania include "high" or irritable mood, very high self-esteem, decreased need for sleep, pressure to keep talking, racing thoughts, being easily distracted, frequently involved in activities with a large risk for bad consequences (for example, excessive buying sprees).
Medical attention should be sought if serotonin syndrome is suspected. Please refer to serious side effects for signs/symptoms.
Are There Specific Concerns About Venlafaxine And Pregnancy?
If you are planning on becoming pregnant, notify your health care provider to best manage your medications. People living with MDD who wish to become pregnant face important decisions. Untreated MDD has risks to the fetus, as well as the mother. It is important to discuss the risks and benefits of treatment with your doctor and caregivers. For women who take antidepressant medications during weeks 13 through the end of their pregnancy (second and third trimesters), there is a risk that the baby can be born before it is fully developed (before 37 weeks).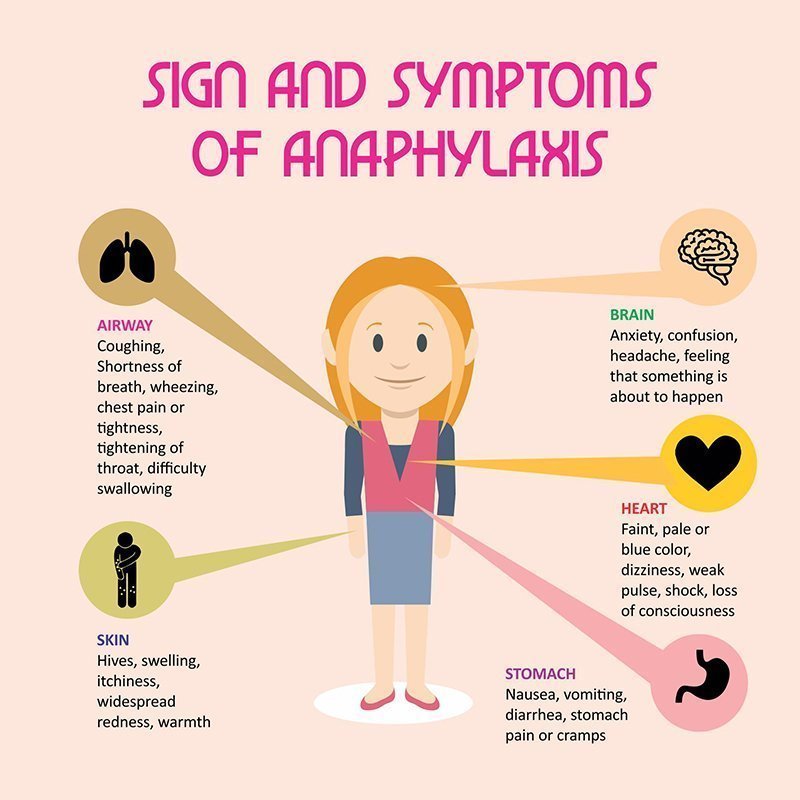
Caution is advised with breastfeeding since venlafaxine does pass into breast milk.
What Should I Discuss With My Health Care Provider Before Taking Venlafaxine?
- Symptoms of your condition that bother you the most
- If you have thoughts of suicide or harming yourself
- Medications you have taken in the past for your condition, whether they were effective or caused any adverse effects
- If you experience side effects from your medications, discuss them with your provider. Some side effects may pass with time, but others may require changes in the medication.
- Any other psychiatric or medical problems you have, including a history of bipolar disorder
- All other medications you are currently taking (including over the counter products, herbal and nutritional supplements) and any medication allergies you have
- Other non-medication treatment you are receiving, such as talk therapy or substance abuse treatment. Your provider can explain how these different treatments work with the medication.
- If you are pregnant, plan to become pregnant, or are breastfeeding
- If you drink alcohol or use drugs
How Should I Take Venlafaxine?
Venlafaxine immediate release tablets are usually taken two or three times per day with or without food. The extended release tablets and capsules are taken one time per day with or without food.
Typically patients begin at a low dose of medicine and the dose is increased slowly over several weeks.
The dose usually ranges from 37.5 mg to 300 mg. Only your health care provider can determine the correct dose for you.
Extended release tablets: swallow whole; do not chew, crush, or break
Extended release capsules: swallow whole or sprinkle onto food, such as applesauce or pudding and eat immediately.
Consider using a calendar, pillbox, alarm clock, or cell phone alert to help you remember to take your medication. You may also ask a family member or friend to remind you or check in with you to be sure you are taking your medication.
What Happens If I Miss A Dose Of Venlafaxine?
If you miss a dose of venlafaxine, take it as soon as you remember, unless it is closer to the time of your next dose. Discuss this with your health care provider. Do not double your next dose or take more than what is prescribed.
What Should I Avoid While Taking Venlafaxine?
Avoid drinking alcohol or using illegal drugs while you are taking antidepressant medications. They may decrease the benefits (e.g., worsen your condition) and increase adverse effects (e.g., sedation) of the medication.
What Happens If I Overdose With Venlafaxine?
If an overdose occurs, call your doctor or 911. You may need urgent medical care. You may also contact the poison control center at 1-800-222-1222.
A specific treatment to reverse the effects of venlafaxine does not exist.
What Are The Possible Side Effects Of Venlafaxine?
Common side effects
- Headache, nausea, diarrhea, dry mouth, increased sweating
- Feeling nervous, restless, fatigued, sleepy or having trouble sleeping (insomnia)
These will often improve over the first week or two as you continue to take the medication.
- Sexual side effects, such as problems with orgasm or ejaculatory delay
- Increased blood pressure
These often do not improve over time.
Rare/serious side effects
Increased heart rate, low blood pressure, increased salivation, irregular menstrual cycle, increased frequency of urination, changes in taste, low sodium (symptoms of low sodium levels may include headache, weakness, difficulty concentrating and remembering), teeth grinding, difficulty urinating, angle closure glaucoma (symptoms of angle closure glaucoma may include eye pain, changes in vision, swelling or redness in or around eye).
Serotonin syndrome (symptoms may include shivering, diarrhea, confusion, severe muscle tightness, fever, seizures, and death)
SNRI antidepressants including venlafaxine may increase the risk of bleeding events. Combined use of aspirin, nonsteroidal anti-inflammatory drugs (e.g., ibuprofen, naproxen), warfarin, and other anti-coagulants may increase this risk. This may include gums that bleed more easily, nose bleed, or gastrointestinal bleeding. Some cases have been life threatening.
This may include gums that bleed more easily, nose bleed, or gastrointestinal bleeding. Some cases have been life threatening.
Are There Any Risks For Taking Venlafaxine For Long Periods Of Time?
To date, there are no known problems associated with long term use of venlafaxine. It is a safe and effective medication when used as directed.
What Other Medications May Interact With Venlafaxine?
Venlafaxine should not be taken with or within 2 weeks of taking monoamine oxidase inhibitors (MAOIs). These include phenelzine (Nardil®), tranylcypromine (Parnate®), isocarboxazid (Marplan®), rasagiline (Azilect®), and selegiline (Emsam®).
Although rare, there is an increased risk of serotonin syndrome when venlafaxine is used with other medications that increase serotonin, such as other antidepressants, migraine medications called “triptans” (e.g., Imitrex®), some pain medications (e.g., tramadol (Ultram®), and the antibiotic linezolid (Zyvox®).
Venlafaxine may increase the effects of other medications that can cause bleeding (e. g., ibuprofen (Advil®, Motrin®), warfarin (Coumadin®) and aspirin).
g., ibuprofen (Advil®, Motrin®), warfarin (Coumadin®) and aspirin).
How Long Does It Take For Venlafaxine To Work?
Sleep, energy, or appetite may show some improvement within the first 1-2 weeks. Improvement in these physical symptoms can be an important early signal that the medication is working. Depressed mood and lack of interest in activities may need up to 6-8 weeks to fully improve.
Summary of FDA Black Box Warnings
Suicidal thoughts or actions in children and adults
Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications. This risk may persist until significant remission occurs.
In short-term studies, antidepressants increased the risk of suicidality in children, adolescents, and young adults when compared to placebo. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24. Adults age 65 and older taking antidepressants have a decreased risk of suicidality. Patients, their families, and caregivers should be alert to the emergence of anxiety, restlessness, irritability, aggressiveness and insomnia. If these symptoms emerge, they should be reported to the patient’s prescriber or health care professional. All patients being treated with antidepressants for any indication should watch for and notify their health care provider for worsening symptoms, suicidality and unusual changes in behavior, especially during the first few months of treatment.
Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24. Adults age 65 and older taking antidepressants have a decreased risk of suicidality. Patients, their families, and caregivers should be alert to the emergence of anxiety, restlessness, irritability, aggressiveness and insomnia. If these symptoms emerge, they should be reported to the patient’s prescriber or health care professional. All patients being treated with antidepressants for any indication should watch for and notify their health care provider for worsening symptoms, suicidality and unusual changes in behavior, especially during the first few months of treatment.
Provided by
(December 2020)
©2020 The College of Psychiatric and Neurologic Pharmacists (CPNP) and the National Alliance on Mental Illness (NAMI). CPNP and NAMI make this document available under the Creative Commons Attribution-No Derivatives 4. 0 International License. Last Updated: January 2016.
0 International License. Last Updated: January 2016.
This information is being provided as a community outreach effort of the College of Psychiatric and Neurologic Pharmacists. This information is for educational and informational purposes only and is not medical advice. This information contains a summary of important points and is not an exhaustive review of information about the medication. Always seek the advice of a physician or other qualified medical professional with any questions you may have regarding medications or medical conditions. Never delay seeking professional medical advice or disregard medical professional advice as a result of any information provided herein. The College of Psychiatric and Neurologic Pharmacists disclaims any and all liability alleged as a result of the information provided herein.
Depression
Russian Academy of Medical Sciences
SCIENTIFIC CENTER FOR MENTAL HEALTH
DEPRESSION (from hope to certainty).
(INFORMATION FOR PATIENTS AND THEIR FAMILIES)
nine0003
MOSCOW
2008
Oleichik I.V. - Candidate of Medical Sciences, Leading Researcher of the Department for the Study of Endogenous Mental Disorders and Affective States
© 2008, Oleichik I.V.
© 2008, NTsPZ RAMS
The vast experience accumulated by mankind and reflected in many literary works convincingly shows that sadness (sadness, spleen) has always gone side by side with people, being one of the natural human emotions. None of us is immune from failures, illness, breakups, loss of loved ones, financial collapse. Each person can face something inevitable and inevitable, when it seems that life loses its meaning, and despair becomes boundless. However, normally, sadness, sadness and melancholy, as natural reactions to traumatic events, weaken over time and the person's condition returns to normal without special treatment. The situation is different with depressions, which are mental disorders that differ from natural physiological reactions in greater intensity, special severity of experiences and persistence of manifestations. True depression rarely goes away on its own, requiring persistent, sometimes long-term treatment. nine0003 A depressive state (from the Latin word depressio - suppression, oppression) is a disease that concerns not only an individual specific sick person, but is also a significant burden of modern society, since it is spreading more and more widely in the world, causing enormous damage to the health of the population and the state. economy. And this applies to all countries, regardless of their level of social development. Every year, at least 200 million people in the world fall ill with depression. Perhaps these figures are even higher, since most victims of depression do not seek help because they are not aware of the painfulness of their condition. Scientists have calculated that almost one in five people who have reached adulthood will experience at least one episode of depression during their lifetime.
The situation is different with depressions, which are mental disorders that differ from natural physiological reactions in greater intensity, special severity of experiences and persistence of manifestations. True depression rarely goes away on its own, requiring persistent, sometimes long-term treatment. nine0003 A depressive state (from the Latin word depressio - suppression, oppression) is a disease that concerns not only an individual specific sick person, but is also a significant burden of modern society, since it is spreading more and more widely in the world, causing enormous damage to the health of the population and the state. economy. And this applies to all countries, regardless of their level of social development. Every year, at least 200 million people in the world fall ill with depression. Perhaps these figures are even higher, since most victims of depression do not seek help because they are not aware of the painfulness of their condition. Scientists have calculated that almost one in five people who have reached adulthood will experience at least one episode of depression during their lifetime. nine0003 In the most general sense, a depressive state is one of the possible forms of a person's response to the impact of stress factors. In some cases, depression can be triggered by external negative influences, for example, mental trauma, excessive educational or work overload, infection or other serious somatic disease, traumatic brain injury, changes in the hormonal background, which is especially important for the female body, regular certain medications, such as hormones, blood pressure medications, alcohol or other drug abuse. In other cases, depressive states develop as a manifestation of such mental illnesses, in which the main influence is heredity or characteristics of the nervous system (cyclothymia, dysthymia, manic-depressive psychosis, schizophrenia, etc.). If, based on the description of depressive symptoms set out later in our brochure, you realize that you have indeed developed a depressive state, do not fall into despair, do not “try to control yourself”, remember that depression is not a manifestation of weakness of will or character, on the contrary, weakening of volitional qualities is one of the main symptoms of depression.
nine0003 In the most general sense, a depressive state is one of the possible forms of a person's response to the impact of stress factors. In some cases, depression can be triggered by external negative influences, for example, mental trauma, excessive educational or work overload, infection or other serious somatic disease, traumatic brain injury, changes in the hormonal background, which is especially important for the female body, regular certain medications, such as hormones, blood pressure medications, alcohol or other drug abuse. In other cases, depressive states develop as a manifestation of such mental illnesses, in which the main influence is heredity or characteristics of the nervous system (cyclothymia, dysthymia, manic-depressive psychosis, schizophrenia, etc.). If, based on the description of depressive symptoms set out later in our brochure, you realize that you have indeed developed a depressive state, do not fall into despair, do not “try to control yourself”, remember that depression is not a manifestation of weakness of will or character, on the contrary, weakening of volitional qualities is one of the main symptoms of depression. Depression is a disease like rheumatism, arthritis or hypertension, it responds well to treatment, resulting in almost always a full recovery. You should not blame yourself for the occurrence of depression, it does not indicate either your fault, or your weakness, or the possible development of a more severe mental pathology. Below we will tell you about the symptoms of depression, which can be extremely diverse. nine0018
Depression is a disease like rheumatism, arthritis or hypertension, it responds well to treatment, resulting in almost always a full recovery. You should not blame yourself for the occurrence of depression, it does not indicate either your fault, or your weakness, or the possible development of a more severe mental pathology. Below we will tell you about the symptoms of depression, which can be extremely diverse. nine0018
Manifestations of depression
Manifestations of depression can be very different. Depressive states can be manifested by a violation of almost all aspects of mental life: mood, memory, will, activity, which is expressed in the appearance of sadness, sadness, mental and muscle retardation, lasting at least 2 weeks. Depressed mood during depression can manifest itself as mild sadness, sadness, and boundless despair. Often it is accompanied by a feeling of melancholy, unbearable heaviness in the soul, with excruciating pain behind the sternum, a feeling of hopelessness, deep depression, hopelessness, helplessness, despair and uncertainty. At the same time, the patient is completely immersed in his gloomy experiences, and external events, even the most joyful ones, do not affect him, do not affect his mood, and sometimes even worsen the latter. A constant "companion" of a depressive mood is also anxiety of varying severity: from mild anxiety or tension to violent excitement, riot. Anxiety and bad mood arise at the mere thought of the need to make some kind of decision or change your plans due to suddenly changed circumstances. Anxiety can also manifest itself on the physical (bodily) level in the form of belching, intestinal cramps, loose stools, frequent urination, shortness of breath, palpitations, headaches, increased sweating, etc.
At the same time, the patient is completely immersed in his gloomy experiences, and external events, even the most joyful ones, do not affect him, do not affect his mood, and sometimes even worsen the latter. A constant "companion" of a depressive mood is also anxiety of varying severity: from mild anxiety or tension to violent excitement, riot. Anxiety and bad mood arise at the mere thought of the need to make some kind of decision or change your plans due to suddenly changed circumstances. Anxiety can also manifest itself on the physical (bodily) level in the form of belching, intestinal cramps, loose stools, frequent urination, shortness of breath, palpitations, headaches, increased sweating, etc.
The picture of depression is complemented by the disappearance of desires, interests, a pessimistic assessment of everything around, ideas of one's own low value and self-blame. Deficiency of vital impulses is manifested in patients with a variety of symptoms - from lethargy, physical weakness to a state of weakness, loss of energy and complete impotence. Where an important decision is required, a choice between different options, human activity is sharply hampered. Depressed people are well aware of this: they complain that insignificant everyday tasks, small issues that used to be solved almost automatically, take on the significance of complex, painful, insoluble problems. At the same time, a person feels that he began to think, act and speak slowly, notes the suppression of instincts (including food and sexual instincts), the suppression or loss of the instinct of self-preservation and the lack of the ability to enjoy life up to complete indifference to what used to be liked evoked positive emotions. nine0003 People suffering from depression often feel "stupid", "mentally retarded", "feeble-minded". Thinking in depression becomes viscous, painful, requires special efforts, one mental image is hardly forced out by the next. The sick person is oppressed by the feeling of his own intellectual insolvency, professional collapse. Depressed patients can hardly describe their painful experiences to the doctor.
Where an important decision is required, a choice between different options, human activity is sharply hampered. Depressed people are well aware of this: they complain that insignificant everyday tasks, small issues that used to be solved almost automatically, take on the significance of complex, painful, insoluble problems. At the same time, a person feels that he began to think, act and speak slowly, notes the suppression of instincts (including food and sexual instincts), the suppression or loss of the instinct of self-preservation and the lack of the ability to enjoy life up to complete indifference to what used to be liked evoked positive emotions. nine0003 People suffering from depression often feel "stupid", "mentally retarded", "feeble-minded". Thinking in depression becomes viscous, painful, requires special efforts, one mental image is hardly forced out by the next. The sick person is oppressed by the feeling of his own intellectual insolvency, professional collapse. Depressed patients can hardly describe their painful experiences to the doctor. Only after getting out of depression, many of them say that the mood at that moment was lowered, thinking was slow, all undertakings (including treatment) seemed in vain, and the years lived were empty and useless. However, at the time of the first visit to the doctor, they could not explain this because of the almost complete absence of thoughts in their heads, “para-lich of thinking”. With depression, there are also often complaints of memory loss, which is why those suffering from it assume that they have "Alzheimer's disease", "schizophrenia", "senile dementia", which is not true. Especially often these complaints are found in depressions that develop in adolescence. nine0003 Typical story
Only after getting out of depression, many of them say that the mood at that moment was lowered, thinking was slow, all undertakings (including treatment) seemed in vain, and the years lived were empty and useless. However, at the time of the first visit to the doctor, they could not explain this because of the almost complete absence of thoughts in their heads, “para-lich of thinking”. With depression, there are also often complaints of memory loss, which is why those suffering from it assume that they have "Alzheimer's disease", "schizophrenia", "senile dementia", which is not true. Especially often these complaints are found in depressions that develop in adolescence. nine0003 Typical story
Aleksey, 18 years old, 1st year student of a technical university, describes his condition during depression as follows:
“From childhood, I was fond of technology and modeling, I could read special literature for hours, won school and regional olympiads in mathematics and physics. After graduating from school, my dream came true - I brilliantly passed the exams to a prestigious university. Then it seemed to me that the whole world was at my feet, I flew with happiness "as if on wings." In September, I happily began to study. At the beginning, everything worked out well, but after 2 months I began to notice that it was becoming increasingly difficult for me to absorb what I read, I did not remember the simplest text, I could not solve problems that I used to “click like nuts”. Trying to achieve success through many hours of brainstorming or drinking a few cups of coffee led to the fact that I completely stopped thinking about anything. It seemed to me that I was "finally and irreversibly stupid." At night I sobbed, wrapped in a blanket and thought about how best to commit suicide. Luckily, I met a senior in the library and shared my problems with him. My new acquaintance said that he experienced something similar and advised me to contact the psychiatrist of the student clinic. After the examination, I was diagnosed with juvenile depression and sent for treatment to a specialized medical center.
Then it seemed to me that the whole world was at my feet, I flew with happiness "as if on wings." In September, I happily began to study. At the beginning, everything worked out well, but after 2 months I began to notice that it was becoming increasingly difficult for me to absorb what I read, I did not remember the simplest text, I could not solve problems that I used to “click like nuts”. Trying to achieve success through many hours of brainstorming or drinking a few cups of coffee led to the fact that I completely stopped thinking about anything. It seemed to me that I was "finally and irreversibly stupid." At night I sobbed, wrapped in a blanket and thought about how best to commit suicide. Luckily, I met a senior in the library and shared my problems with him. My new acquaintance said that he experienced something similar and advised me to contact the psychiatrist of the student clinic. After the examination, I was diagnosed with juvenile depression and sent for treatment to a specialized medical center. After 2 months, I felt completely healthy, returned to my studies and caught up with my classmates. nine0018
After 2 months, I felt completely healthy, returned to my studies and caught up with my classmates. nine0018
Depression can also be accompanied by real setbacks: for example, a decrease in academic performance, the quality of work, family conflicts, sexual disorders and their consequences for personal relationships. As a rule, the significance of these failures is exaggerated and as a result there is a false sense of the irreparability of what happened, "the collapse of all hopes."
Another generally recognized danger of depression is the possibility of suicidal thoughts, which often lead to suicide attempts. The condition of a person suffering from depression can suddenly deteriorate sharply, which happens either without clear external causes, or under the influence of traumatic situations, unpleasant news. It is during these hours, and sometimes even minutes, that a fatal decision is made. Factors that increase the risk of suicide in depression are past suicide attempts, the severity and duration of the depressive state, the presence of anxiety in its structure, prolonged insomnia, loneliness or alienation in the family, alcohol and drug abuse, loss of work and a sharp change in lifestyle, as well as relatives commit suicide. nine0003 Typical story
nine0003 Typical story
Eugene E., 35 years old, leading manager of the company.
Almost all my life, my career went “on the ascending”, the goals set were clear, clear and achievable. The marriage was extremely harmonious, two beloved children grew up. He devoted almost all the time to the affairs of the company, occasionally, once every 1-2 months, he escaped with his family out of town, to the country. He often lacked sleep, stayed late at work, took home assignments, and was deeply worried about the affairs of the company. Gradually, irritability, fatigue, insomnia, difficulty concentrating appeared, more and more often he suffered a “fiasco” in intimate life. Thoughts appeared that life was lived in vain, that it is a "chain of tragic mistakes" that led to a dead end. He began to believe that the choice of work, friends, family was wrong, for which now "retribution has come." Analyzing the past years for a long time, he found more and more evidence and examples of his "duplicity, hypocrisy, insincerity, etc. " I realized that the only way to solve all problems is to voluntarily leave this life. At the same time, he believed that by this act he would free the family from the “burden”, “loser”, “loser”. I decided, having locked myself in the garage, to get poisoned by the exhaust gases of the car. However, by chance, in a semi-conscious state, he was discovered by an employee of a garage cooperative. He explained what happened as an "accident". The thought of leaving life did not leave the patient. I decided to shoot myself with a gas pistol, which I had long ago acquired for self-defense. After a shot in the mouth, in a serious condition, he was taken to the Research Institute. Sklifasovsky, from where he was discharged a week later. The alarmed wife, suspecting something was wrong, decided to consult her husband with a psychiatrist. He was admitted to the clinic. He agreed to this only out of respect for family relations, he himself believed that treatment by psychiatrists was completely useless, because.
" I realized that the only way to solve all problems is to voluntarily leave this life. At the same time, he believed that by this act he would free the family from the “burden”, “loser”, “loser”. I decided, having locked myself in the garage, to get poisoned by the exhaust gases of the car. However, by chance, in a semi-conscious state, he was discovered by an employee of a garage cooperative. He explained what happened as an "accident". The thought of leaving life did not leave the patient. I decided to shoot myself with a gas pistol, which I had long ago acquired for self-defense. After a shot in the mouth, in a serious condition, he was taken to the Research Institute. Sklifasovsky, from where he was discharged a week later. The alarmed wife, suspecting something was wrong, decided to consult her husband with a psychiatrist. He was admitted to the clinic. He agreed to this only out of respect for family relations, he himself believed that treatment by psychiatrists was completely useless, because. his situation is hopeless and no medicines will help here, but will only "stupefy" his psyche. However, after two weeks of taking a modern antidepressant, the patient's point of view changed. Everything began to look not so bleak and hopeless, interest in work and life in general returned, I began to feel more cheerful, more energetic, interest in intimate life appeared. He took work to the clinic, called up colleagues. After two months of treatment, he fully returned to his usual life. With bewilderment, he recalled his thoughts about insolvency, the collapse of life, suicide. He took the drug prophylactically for about six months, then, on the recommendation of a doctor, he gradually reduced the dose and stopped taking it. Over the next two years, the condition remained stable, career growth continued, another child was born. nine0018
his situation is hopeless and no medicines will help here, but will only "stupefy" his psyche. However, after two weeks of taking a modern antidepressant, the patient's point of view changed. Everything began to look not so bleak and hopeless, interest in work and life in general returned, I began to feel more cheerful, more energetic, interest in intimate life appeared. He took work to the clinic, called up colleagues. After two months of treatment, he fully returned to his usual life. With bewilderment, he recalled his thoughts about insolvency, the collapse of life, suicide. He took the drug prophylactically for about six months, then, on the recommendation of a doctor, he gradually reduced the dose and stopped taking it. Over the next two years, the condition remained stable, career growth continued, another child was born. nine0018
Depression is also characterized by sleep disturbances, occurring in approximately 80% of patients. As a rule, these are early awakenings with the inability to fall asleep, lack of a sense of sleep, difficulty falling asleep. These disorders, as well as restless sleep with unpleasant dreams, are often the very first symptoms of incipient depression.
These disorders, as well as restless sleep with unpleasant dreams, are often the very first symptoms of incipient depression.
If the depression is not deep, it is sometimes difficult to recognize it. This is due to the fact that people are ashamed to tell others about their problems, to admit to "weaknesses". Quite often, especially in Russia, depressive states are masked by alcohol abuse (“vodka heals”). In addition, often patients suffering from depression, in order to "shake themselves up", "throw into all serious", engage in casual sex, are fond of gambling or extreme sports, leave to serve on a contract in "hot spots", lead an idle lifestyle with constant attendance at entertainment events. Surrounding people, relatives who do not have psychiatric knowledge, often accuse them of debauchery, drunkenness, riotous lifestyle, parasitism. Meanwhile, this behavior is a kind of “cry for help”, an attempt to fill the spiritual emptiness brought by depression with new acquaintances and impressions. nine0003 Depressive conditions can occur in shallow forms that are easily treatable, but at least a third of depressions are more severe. Such depressions are characterized by:
nine0003 Depressive conditions can occur in shallow forms that are easily treatable, but at least a third of depressions are more severe. Such depressions are characterized by:
- ideas of guilt, sometimes reaching the degree of delirium, i.e. unshakable conviction in their sinfulness, low value (patients consider themselves great sinners, believe that because of them all relatives and Mankind will die, that they are “moral freaks” from birth, supposedly deprived of the foundations of morality and a sense of empathy for other people that they have no place on earth They find in their past numerous "confirmations" of what has been said above, they believe that the doctor and other patients are aware of these transgressions and express contempt and indignation with their facial expressions and gestures, but in the words “they hide, deny the obvious.” Both the patients themselves and their relatives must remember this in order to prevent the impending threat in time: remove all firearms, piercing and cutting objects, ropes, potent drugs and poisonous close household fluids, close windows or shutters, do not let the patient go anywhere alone. If these ideas become persistent and cannot be dissuaded, it is urgent to seek advice from a psychiatrist. neurological institution or call a psychiatrist at home. nine0003 - mood swings during the day: in typical cases, the patient, waking up, immediately feels longing. Sometimes, even before full awakening, through a dream he experiences a painful premonition of a heavy coming morning. In the evening, the state of health improves somewhat.
If these ideas become persistent and cannot be dissuaded, it is urgent to seek advice from a psychiatrist. neurological institution or call a psychiatrist at home. nine0003 - mood swings during the day: in typical cases, the patient, waking up, immediately feels longing. Sometimes, even before full awakening, through a dream he experiences a painful premonition of a heavy coming morning. In the evening, the state of health improves somewhat.
- the patient may experience a feeling of unmotivated hostility towards relatives, friends, constant internal discontent and irritation, which makes him unbearable for the family.
- in a number of people suffering from depression, constant doubts, fear for the health and well-being of loved ones, obsessive ones, come to the fore. arising against the will, ideas about the misfortunes and troubles of family members. nine0018
Typical story
Dmitry Petrovich, 58 years old, teacher.
“After minor troubles at work, I began to feel incomprehensible anxiety and agitation. Unpleasant thoughts came into my head that I did something wrong at work, because of which I double-checked everything many times and went home later than everyone else. But even at home, the anxiety did not let go: as soon as the daughter or wife lingered for at least half an hour, terrible pictures of traffic accidents or violence were drawn in the imagination. I fell asleep only in the morning, got up broken and felt sleepy all day. I took Valerian, Corvalol, but it practically did not help. At work, they hinted whether I should take a vacation. Friends advised me to consult a neuropathologist, but he did not find his pathology and sent me to a psychiatrist. I was diagnosed with anxiety depression. After a course of outpatient treatment, I completely recovered.” nine0018
Unpleasant thoughts came into my head that I did something wrong at work, because of which I double-checked everything many times and went home later than everyone else. But even at home, the anxiety did not let go: as soon as the daughter or wife lingered for at least half an hour, terrible pictures of traffic accidents or violence were drawn in the imagination. I fell asleep only in the morning, got up broken and felt sleepy all day. I took Valerian, Corvalol, but it practically did not help. At work, they hinted whether I should take a vacation. Friends advised me to consult a neuropathologist, but he did not find his pathology and sent me to a psychiatrist. I was diagnosed with anxiety depression. After a course of outpatient treatment, I completely recovered.” nine0018
- in many cases, depression is characterized by unpleasant sensations in the body, disturbances in the activity of internal organs in the absence of objective signs of true somatic, i.e. non-mental illness. At the same time, many patients constantly report pain, internal discomfort. Some complain of headaches, pains in the stomach, joints, lower back, others - of disorders in the intestines: constipation, indigestion, irritation of the colon, others pay attention to a decrease in sexual desire and potency. In women, menstruation often becomes painful and irregular. Approximately 50% of depressed people at the doctor's office complain of such physical ailments, without mentioning the depressed mood or state of mind underlying the depression. Experiencing chronic pain or other unpleasant sensations in the body, patients may not realize that they are suffering from depression, even with severe melancholy, considering the latter a reaction to painful bodily discomfort. nine0003 - some patients are convinced that they have some rare and difficult to diagnose disease and insist on numerous examinations in general medical institutions. Doctors call this condition masked (hidden) depression, in which a person may experience pain in the head, in the limbs, behind the sternum, in the abdomen and in any other parts of the body, he may be haunted by anxious fears, he may suffer from insomnia or, on the contrary, too much sleep.
Some complain of headaches, pains in the stomach, joints, lower back, others - of disorders in the intestines: constipation, indigestion, irritation of the colon, others pay attention to a decrease in sexual desire and potency. In women, menstruation often becomes painful and irregular. Approximately 50% of depressed people at the doctor's office complain of such physical ailments, without mentioning the depressed mood or state of mind underlying the depression. Experiencing chronic pain or other unpleasant sensations in the body, patients may not realize that they are suffering from depression, even with severe melancholy, considering the latter a reaction to painful bodily discomfort. nine0003 - some patients are convinced that they have some rare and difficult to diagnose disease and insist on numerous examinations in general medical institutions. Doctors call this condition masked (hidden) depression, in which a person may experience pain in the head, in the limbs, behind the sternum, in the abdomen and in any other parts of the body, he may be haunted by anxious fears, he may suffer from insomnia or, on the contrary, too much sleep. nine0003 - Patients may experience disturbances in the cardiovascular system, skin itching or lack of appetite. All of these are manifestations of depression.
nine0003 - Patients may experience disturbances in the cardiovascular system, skin itching or lack of appetite. All of these are manifestations of depression.
- the pathological sensations that patients experience during such depressions are quite real, painful, but they are the result of a special mental state, and not an internal disease. It must be remembered that the frequency of latent depressions exceeds the number of explicit ones many times over.
- with such depression, patients, as a rule, also have a changed attitude towards food: they can go without food for a long time and not feel hungry, and sitting down at the table, eat only 1-2 spoons - they have neither strength nor desire for more . nine0003 - a sign of depression can serve as a weight loss of more than 5 kg. within a month. In some people, especially women, the appetite for depression, on the contrary, increases, sometimes reaching the level of excruciating hunger, accompanied by severe weakness and pain in the epigastric region. In some cases, food is taken in excess due to an increased craving for sweets or attempts to distract oneself from painful thoughts by frequent eating.
In some cases, food is taken in excess due to an increased craving for sweets or attempts to distract oneself from painful thoughts by frequent eating.
Thus, we see that depression is a disease with many different manifestations that do not go away on their own, requiring special, sometimes long-term, medical intervention. Therefore, when the symptoms described above appear, it is necessary to seek help from a psychiatrist who will prescribe and monitor antidepressant treatment. nine0018
TREATMENT OF DEPRESSIVE DISORDERS
To date, it can be argued that the vast majority of cases of depression respond well to treatment. According to modern views, effective treatment of depression consists of a combination of pharmacotherapy, psychotherapy and, if necessary, other types of treatment. At the same time, the main role in therapy, of course, belongs to antidepressants - drugs specially designed for the treatment of various types of depression. nine0003 The creation of antidepressants is based on the discovery of scientists that depression develops as a result of a violation of the mechanism of biochemical transmission of nerve impulses in the brain regions responsible for mood, behavior, response to stress, sleep and wakefulness, appetite and some other functions. To ensure the coordination of the work of all these functional divisions, the brain sends special "commands" to them in the form of chemical impulses transmitted from the processes of one nerve cell (neuron) to the processes of another. This transmission is carried out with the help of chemical mediators (neurotransmitters), which, after transmitting a signal, partially return to the original neuron. This process is called neurotransmitter reuptake. Thanks to him, the number of mediators in the microscopic space between the processes of neurons (in the so-called synaptic cleft) decreases, which means that the necessary signals are transmitted worse. Numerous studies have shown that mediators of various structures, in particular, norepinephrine and serotonin, are involved in the transmission of signals that ensure the normal functioning of the nervous system.
nine0003 The creation of antidepressants is based on the discovery of scientists that depression develops as a result of a violation of the mechanism of biochemical transmission of nerve impulses in the brain regions responsible for mood, behavior, response to stress, sleep and wakefulness, appetite and some other functions. To ensure the coordination of the work of all these functional divisions, the brain sends special "commands" to them in the form of chemical impulses transmitted from the processes of one nerve cell (neuron) to the processes of another. This transmission is carried out with the help of chemical mediators (neurotransmitters), which, after transmitting a signal, partially return to the original neuron. This process is called neurotransmitter reuptake. Thanks to him, the number of mediators in the microscopic space between the processes of neurons (in the so-called synaptic cleft) decreases, which means that the necessary signals are transmitted worse. Numerous studies have shown that mediators of various structures, in particular, norepinephrine and serotonin, are involved in the transmission of signals that ensure the normal functioning of the nervous system. The first of them has a general activating effect, maintains the level of wakefulness of the body and takes part in the formation of adaptive reactions, and the second has the main antidepressant effect, controls impulsive actions, anxiety, aggressiveness, sexual behavior, falling asleep, feeling of pain, therefore serotonin is called sometimes a "good mood" regulator. A decrease in the number of mediators in the synaptic cleft causes symptoms of depression, while an increase, on the contrary, prevents their appearance. The ability of some drugs in one way or another to increase the concentration of mediators in the synaptic cleft allows them to be used as antidepressants. nine0003 Now antidepressants are used in Russia, which can be conditionally divided into 4 generations according to the time of creation.
The first of them has a general activating effect, maintains the level of wakefulness of the body and takes part in the formation of adaptive reactions, and the second has the main antidepressant effect, controls impulsive actions, anxiety, aggressiveness, sexual behavior, falling asleep, feeling of pain, therefore serotonin is called sometimes a "good mood" regulator. A decrease in the number of mediators in the synaptic cleft causes symptoms of depression, while an increase, on the contrary, prevents their appearance. The ability of some drugs in one way or another to increase the concentration of mediators in the synaptic cleft allows them to be used as antidepressants. nine0003 Now antidepressants are used in Russia, which can be conditionally divided into 4 generations according to the time of creation.
The first antidepressants to find wide clinical use were tricyclic drugs: amitriptyline and imipramine. They have a fairly powerful effect on most depressive states by blocking the reuptake of both norepinephrine and serotonin. However, the real clinical effect of these drugs is significantly offset by their undesirable side effects, which drastically reduce the quality of life of patients during treatment. Side effects of tricyclic antidepressants arise due to the nonspecificity of their effect on receptor structures. Acting in addition to the serotonin and norepinephrine system and other neurotransmitters (acetylcholine, histamine, dopamine), these antidepressants cause side effects such as urinary retention, dry mucous membranes, constipation, palpitations, fluctuations in blood pressure, confusion, tremor, sexual dysfunction. functions, weight gain. In such cases, it is necessary to prescribe other drugs to correct side effects or reduce the therapeutic dose of drugs, which naturally affects the effectiveness of the antidepressant action. It has been observed that up to 50% of patients refuse to take tricyclic antidepressants due to severe side effects. For the same reason, physicians are less likely to prescribe these drugs to patients on an outpatient basis.
However, the real clinical effect of these drugs is significantly offset by their undesirable side effects, which drastically reduce the quality of life of patients during treatment. Side effects of tricyclic antidepressants arise due to the nonspecificity of their effect on receptor structures. Acting in addition to the serotonin and norepinephrine system and other neurotransmitters (acetylcholine, histamine, dopamine), these antidepressants cause side effects such as urinary retention, dry mucous membranes, constipation, palpitations, fluctuations in blood pressure, confusion, tremor, sexual dysfunction. functions, weight gain. In such cases, it is necessary to prescribe other drugs to correct side effects or reduce the therapeutic dose of drugs, which naturally affects the effectiveness of the antidepressant action. It has been observed that up to 50% of patients refuse to take tricyclic antidepressants due to severe side effects. For the same reason, physicians are less likely to prescribe these drugs to patients on an outpatient basis. nine0003 The situation was somewhat improved by the introduction into practice of drugs of the second generation - tetracyclic antidepressants, which, along with the ability to block the reuptake of norepinephrine and serotonin, could also affect some other receptors. Being analogues of tricyclic compounds, these drugs have antidepressant activity comparable to them, but unlike their predecessors, they are safer, since they cause unwanted side effects much less frequently. In addition to the antidepressant, mianserin (lerivon) has a clear sedative, anti-anxiety and hypnotic effect. Maprotiline (Ludiamil) has a mild balanced antidepressant effect. In general, these drugs are able to cure mild to moderate depression, but are ineffective in patients with severe depression. nine0003 To date, antidepressants of the 3rd generation, such as fluoxetine (Prozac), fluvoxamine (Fevarin), paroxetine (Paxil), sertraline (Zoloft), citalopram (Cipralex) and some other drugs that selectively (selectively) affect the serotonin metabolism system, have received widespread recognition today.
nine0003 The situation was somewhat improved by the introduction into practice of drugs of the second generation - tetracyclic antidepressants, which, along with the ability to block the reuptake of norepinephrine and serotonin, could also affect some other receptors. Being analogues of tricyclic compounds, these drugs have antidepressant activity comparable to them, but unlike their predecessors, they are safer, since they cause unwanted side effects much less frequently. In addition to the antidepressant, mianserin (lerivon) has a clear sedative, anti-anxiety and hypnotic effect. Maprotiline (Ludiamil) has a mild balanced antidepressant effect. In general, these drugs are able to cure mild to moderate depression, but are ineffective in patients with severe depression. nine0003 To date, antidepressants of the 3rd generation, such as fluoxetine (Prozac), fluvoxamine (Fevarin), paroxetine (Paxil), sertraline (Zoloft), citalopram (Cipralex) and some other drugs that selectively (selectively) affect the serotonin metabolism system, have received widespread recognition today. , preventing its reuptake in the synaptic cleft. Based on the mechanism of action, these antidepressants are combined into a group of selective serotonin reuptake inhibitors. In addition to treating depression, they are used to correct eating disorders, level panic disorders, so-called social phobias, various obsessive-compulsive disorders and chronic pain symptoms. These drugs have gained popularity due to the possibility of a once-daily intake, concomitant anti-anxiety effect, the presence of a psychostimulant component and a small number of side effects. In addition, they have low toxicity and are well tolerated by elderly patients. However, some researchers note their lack of effectiveness in the treatment of severe forms of depressive states, probably associated with selective activity in relation to only one neurotransmitter - serotonin. It should be noted that in recent years, some American scientists have associated the use of these drugs with an increased risk of suicide, which, however, is not proven.
, preventing its reuptake in the synaptic cleft. Based on the mechanism of action, these antidepressants are combined into a group of selective serotonin reuptake inhibitors. In addition to treating depression, they are used to correct eating disorders, level panic disorders, so-called social phobias, various obsessive-compulsive disorders and chronic pain symptoms. These drugs have gained popularity due to the possibility of a once-daily intake, concomitant anti-anxiety effect, the presence of a psychostimulant component and a small number of side effects. In addition, they have low toxicity and are well tolerated by elderly patients. However, some researchers note their lack of effectiveness in the treatment of severe forms of depressive states, probably associated with selective activity in relation to only one neurotransmitter - serotonin. It should be noted that in recent years, some American scientists have associated the use of these drugs with an increased risk of suicide, which, however, is not proven. nine0003 Considering the high frequency of side effects in some of the above drugs and the insufficient antidepressant activity in others, psychopharmacologists have taken the path of developing more effective antidepressants - IV generation drugs that selectively block the reuptake of both serotonin and noradrenaline, without affecting other mediators. system and with minor side effects. Currently, 3 drugs meet these requirements: milnacipran (Ixel), duloxetine (Cymbalta) and venlafaxine (Effexor). Their antidepressant activity in the treatment of patients with severe and moderate depression has been confirmed in a number of specially conducted studies, which at the same time showed that these drugs are well tolerated. nine0003 It should be noted that antidepressants of plant origin (negrustin, gelarium hypericum, deprim, etc.) can be effective in mild depressive states, but there are no reliable data guaranteeing their effectiveness. The opinion of a number of doctors that all depression can be treated with herbs or, say, acupuncture, should be recognized as unfounded.
nine0003 Considering the high frequency of side effects in some of the above drugs and the insufficient antidepressant activity in others, psychopharmacologists have taken the path of developing more effective antidepressants - IV generation drugs that selectively block the reuptake of both serotonin and noradrenaline, without affecting other mediators. system and with minor side effects. Currently, 3 drugs meet these requirements: milnacipran (Ixel), duloxetine (Cymbalta) and venlafaxine (Effexor). Their antidepressant activity in the treatment of patients with severe and moderate depression has been confirmed in a number of specially conducted studies, which at the same time showed that these drugs are well tolerated. nine0003 It should be noted that antidepressants of plant origin (negrustin, gelarium hypericum, deprim, etc.) can be effective in mild depressive states, but there are no reliable data guaranteeing their effectiveness. The opinion of a number of doctors that all depression can be treated with herbs or, say, acupuncture, should be recognized as unfounded.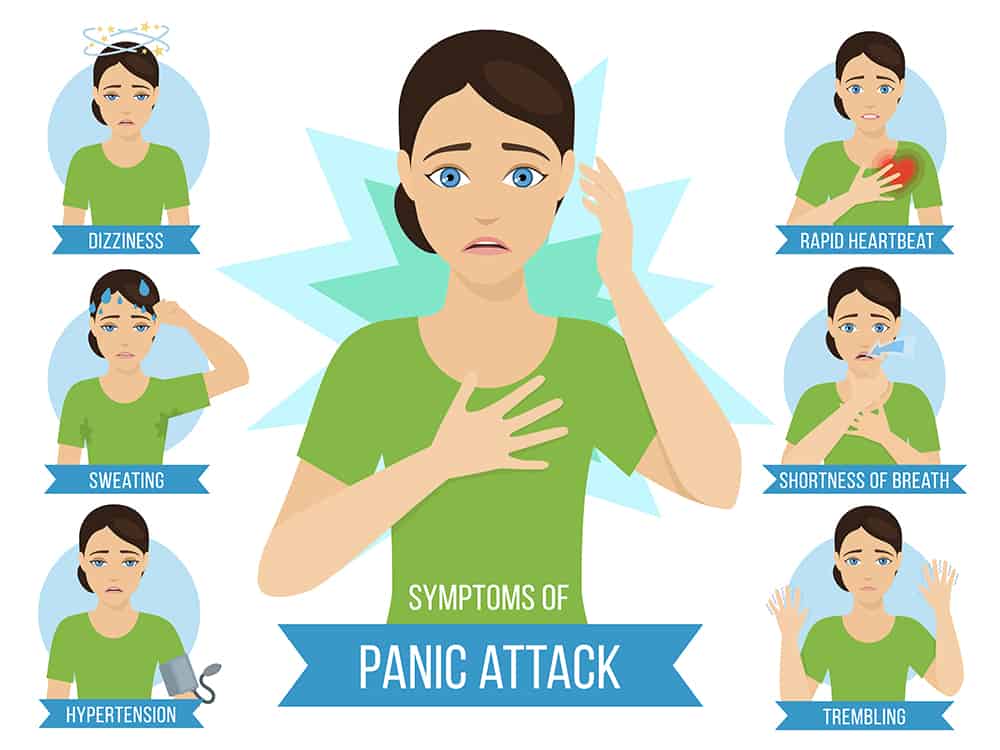
For extremely severe depressions that do not improve despite the use of the most powerful antidepressants, electroconvulsive therapy (ECT) can be effective, but this situation is extremely rare and requires careful justification by the commission of doctors and the consent of the patient. nine0003 An important additional role in antidepressant therapy, especially with concomitant anxiety, is played by tranquilizers - anti-anxiety drugs, such as Xanax, phenazepam, diazepam, nitrazepam, atarax, etc. Drugs that can, when taken systematically, prevent mood swings in various depressive disorders include so-called mood stabilizers or mood stabilizers - lithium preparations, carbamazepine, valproic acid salts, lamotrigine, topiramate. With their systematic intake in most patients, the clinical manifestations of depression either completely disappear or become rare and mild, requiring no hospitalization and not significantly affecting the ability to work. nine0003 Antipsychotics play a significant role in the treatment of certain forms of depression. These include both traditional drugs - fluanxol, triftazin, eglonil, teralen, neuleptil, sonapax, and atypical antipsychotics that are gaining more and more recognition among doctors: seroquel, solian, zeldox, rispolept, abilify, serdolect and others.
These include both traditional drugs - fluanxol, triftazin, eglonil, teralen, neuleptil, sonapax, and atypical antipsychotics that are gaining more and more recognition among doctors: seroquel, solian, zeldox, rispolept, abilify, serdolect and others.
In drug therapy of depressive conditions, an unconventional, strictly individual approach is used, with the obligatory provision of fruitful cooperation between the patient and the doctor. Otherwise, there may be a violation of medical recommendations regarding doses and regimens for taking medications. The patient's faith in the possibility of recovery, the absence of prejudice against the "harm" caused by psychotropic drugs, the systematic observance of the prescriptions prescribed by the doctor largely contribute to the achievement of therapeutic success. nine0003 Drug treatment of depression takes time. You should not expect a complete cure already in the first days of taking the drug. It must be remembered that all modern antidepressants begin to act on depressive symptoms no earlier than 1-2 weeks after the start of treatment. Cancellation of an antidepressant, as well as its appointment, should be carried out only by a doctor. Cancellation is usually made no earlier than 6 months from the normalization of the mental state. Even after the complete disappearance of all symptoms of depression, do not rush to stop taking the drug yourself, as there is a risk of an exacerbation of the disease. Therefore, doctors recommend continuing to take the antidepressant for a certain period of time. A common mistake is the premature withdrawal of drugs soon after a significant improvement in the condition or due to "forgetfulness". To avoid this, try to include the drug in the list of daily urgent matters - for example, store it in the bathroom and take it after hygiene procedures. When planning a trip, calculate exactly how many tablets you need for the entire period of absence from home. Breaking therapy is fraught with serious troubles. nine0003 Conducted along with drug treatment, psychotherapy of patients with depressive states implies various systems of influence, including individual conversations, family and group therapy, etc.
Cancellation of an antidepressant, as well as its appointment, should be carried out only by a doctor. Cancellation is usually made no earlier than 6 months from the normalization of the mental state. Even after the complete disappearance of all symptoms of depression, do not rush to stop taking the drug yourself, as there is a risk of an exacerbation of the disease. Therefore, doctors recommend continuing to take the antidepressant for a certain period of time. A common mistake is the premature withdrawal of drugs soon after a significant improvement in the condition or due to "forgetfulness". To avoid this, try to include the drug in the list of daily urgent matters - for example, store it in the bathroom and take it after hygiene procedures. When planning a trip, calculate exactly how many tablets you need for the entire period of absence from home. Breaking therapy is fraught with serious troubles. nine0003 Conducted along with drug treatment, psychotherapy of patients with depressive states implies various systems of influence, including individual conversations, family and group therapy, etc. An important element of social rehabilitation is participation in the work of mutual support groups for patients who have experienced depression. This allows other patients to feel help in understanding their problems, to realize that they are not alone in their misfortune, to see the possibilities of personal participation in rehabilitation activities and in social life. nine0018
An important element of social rehabilitation is participation in the work of mutual support groups for patients who have experienced depression. This allows other patients to feel help in understanding their problems, to realize that they are not alone in their misfortune, to see the possibilities of personal participation in rehabilitation activities and in social life. nine0018
Along with the changes in your body during menopause (a process that usually takes four to eight years), you may also notice some physical and emotional changes. The most common of these are:
- Irregular menstruation
- Tides
- Vaginal dryness
- Urinary tract infections
- Stress incontinence
- Night sweats nine0145 Insomnia
- Headaches
- Palpitations
- Carelessness
- Mood swings
- Restlessness and irritability
- Absentmindedness
There are many ways to relieve these symptoms if they make you uncomfortable. Discuss your situation with your doctor to determine which remedies are right for you.
Discuss your situation with your doctor to determine which remedies are right for you.
To help relieve the most common symptoms of menopause, the following actions are recommended:
Hot flashes during menopause . Although it is not known exactly what causes hot flashes, they are most likely the result of a narrowing of the temperature range that normally signals the brain to regulate core temperature. The pituitary gland raises the level of hormones associated with the ovaries - follitropin and luteinizing hormone. A decrease in estrogen levels and an increase in follitropin and luteinizing hormone cause deviations in core temperature. As a result, the vasomotor balance becomes unstable, which is why hot flashes occur. nine0018
Approximately 75 out of 100 women experience hot flashes at or after menopause, which usually lasts three to five years. Hot flashes may increase and become more frequent by the last menstruation, and then subside. As a rule, they completely disappear after a period of one to five years. For some women, hot flashes continue into their 70s.
For some women, hot flashes continue into their 70s.
During hot flashes there is a sudden sensation of heat in the face, neck and chest. There may be severe sweating and the pulse may increase. Some women experience dizziness and nausea. Hot flashes usually last two to four minutes, which can feel like an eternity. For some women, hot flashes are simply unbearable if they happen at the wrong time or at night, which interferes with sleep. nine0018
You can overcome the tides in different ways. For example, short-term hormone therapy (including estrogen alone or estrogen plus progesterone taken for about two to three years, but not more than five years). Herbal treatment is also used. A very easy and simple way can be a change in lifestyle. Try the following to get started:
- Wear layered clothing so you can take things off if you get hot.
- Sleep in a cool room. nine0146
- Drink plenty of water.
- Try not to consume anything that can cause hot flashes - do not eat hot foods such as soups; spicy foods, caffeine and alcohol.
- Try to avoid stress.
- Exercise regularly.
- If you feel the onset of the tide, breathe slowly and deeply - this can help "reduce" the heat of the tide or even prevent it.
- Use a fan.
Insomnia. Sleep problems often occur during menopause - hot flashes interfere with sleep (if they occur at night, they are called night sweats) - interrupt sleep or prevent sleep. To some extent, the increase and decrease in hormone levels are to blame. In addition, with age, the very pattern of sleep can change. Older adults sleep less, wake up earlier, and go to bed later or earlier than when they were younger.
In order to eliminate sleep problems, follow these recommendations:
- Sleep in a cool room to relieve hot flashes that interfere with sleep. In hot weather, you can lower the temperature in the bedroom, and use a fan to keep the air circulating.
- Exercise regularly.
- Do some routine activities for an hour before going to bed.

- Before going to bed, drink a glass of warm milk, but do not eat.
- Do not drink alcoholic beverages or smoke before bed. nine0146
- Do not watch TV in bed (some programs are far from relaxing!).
- Try relaxation techniques such as deep breathing.
- Review the medications you are taking - some of them may cause insomnia.
Sudden mood swings. For reasons that are not yet fully understood, the decline and fluctuations in estrogen levels during menopause can trigger emotional ups and downs and irritability. Irritability and depression can also be caused by lack of sleep due to night sweats. Even though your periods are coming to an end, you may still experience symptoms of premenstrual syndrome (PMS). In fact, for some women, emotional symptoms may worsen during menopause. You may also lose interest in sex. Reducing estrogen and changing the proportion of estrogen/testosterone can lower the sex drive in women during this period. nine0018
nine0018
Here are some tips to reduce mood swings and normalize your sex drive:
- Exercise - it will help improve your mood and make you feel better.
- Use relaxation techniques such as meditation and massage to help you calm down and reduce irritability.
- Discuss the symptoms and their possible causes with your partner; try to find new approaches to intimacy. nine0171
- Use non-hormonal vaginal creams or gels (with or without a doctor's prescription).
- If moisturizers and lubricants are not enough, use vaginal estrogen (prescription only) in cream, ring, or tablet form.
- Drink plenty of water to keep your body hydrated.
- Use long-acting vaginal moisturizers. nine0146
- Exercise to maintain muscle tone. Try Kegel exercises to strengthen the pelvic floor muscles that support the bladder and urethra. Kegel exercises help strengthen the vaginal canal, control urine flow, and increase orgasm. To make sure you know how to properly contract your pelvic floor muscles, try to stop urinating in the toilet. If you succeed, then you have found the right muscles. For Kegel exercises, you need to empty your bladder and then sit or lie down. Squeeze your pelvic floor muscles for three seconds, then relax for three seconds.
 Repeat the exercise 10 times. Once you've mastered the three-second contractions, try the same with four seconds. Over time, bring the exercise up to 10 seconds of contraction and 10 seconds of relaxation. It is advisable to perform 10 exercises in a row three times a day. nine0146
Repeat the exercise 10 times. Once you've mastered the three-second contractions, try the same with four seconds. Over time, bring the exercise up to 10 seconds of contraction and 10 seconds of relaxation. It is advisable to perform 10 exercises in a row three times a day. nine0146 - Talk to your doctor about any medications you take. Some may aggravate vaginal dryness. Also, if you have a urinary tract infection, you may need antibiotics.
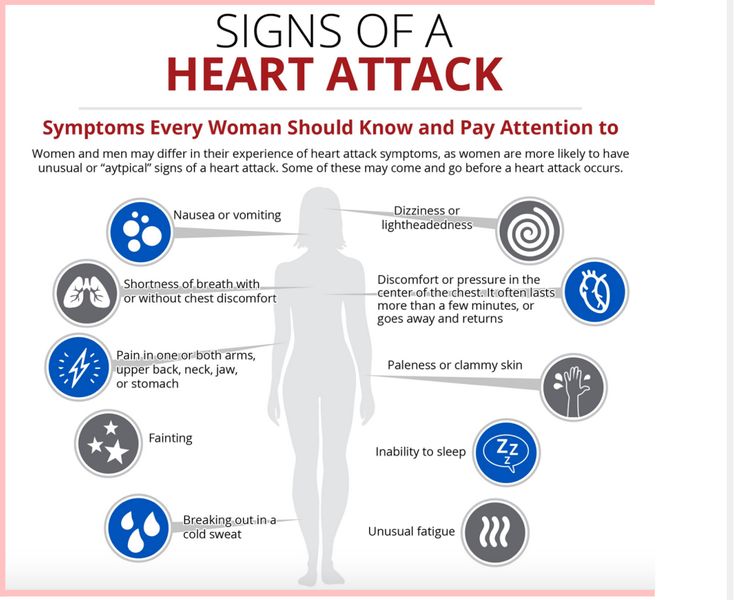
- shortness of breath;
- fast or irregular heartbeat;
- dizziness; nausea;
- pain in the neck, jaw, arm or chest, or shortness of breath.
- Make sure that these symptoms were caused by menopause and age, do not overthink it.
- During a period of forgetfulness, use memory techniques such as reminder sheets or messages.
- Use stress-reducing techniques such as breathing exercises, yoga and meditation, and try to be physically active at all times. nine0146
Vaginal dryness and frequent urinary tract infections. Estrogen, a natural hormone produced by the body, keeps the vagina moist and elastic. During menopause, estrogen levels decrease, the vagina becomes drier, and the vaginal walls become thinner. Sex can become quite painful. The wall of the urethra also becomes thinner as estrogen levels fall, thus increasing the risk of urinary tract infections. Urinary incontinence can become a problem as the muscles that support the bladder and urethra weaken. (This can also occur due to tissue stretching during childbirth. ) nine0018
) nine0018
To avoid vaginal dryness and frequent urinary tract infections, follow these guidelines:
Palpitation. Some women in their 50s are worried that their heart is beating hard for no apparent reason. This symptom, namely the feeling of palpitations, may be due to an irregular heartbeat or missing one or two beats. Although this symptom can be associated with several types of serious heart disease, it also appears around menopause and is usually not associated with heart disease. For example, a woman's heart rate may increase by 7 to 15 beats during a hot flush. nine0018
If you think you are experiencing palpitations:
Talk to your doctor right away if you have symptoms that could indicate serious heart disease. These symptoms include:
These symptoms include:
Ask your doctor to rule out conditions that can cause palpitations, such as thyroid conditions. Talk to your doctor about ways to manage your heartbeat problem, such as reducing your caffeine intake and taking certain medications. nine0018
Forgetfulness or distraction . During and after menopause, many women experience memory problems, mental retardation, and absent-mindedness.
Problems with memory and concentration can be caused by lack of sleep or sleep disorders. The stress associated with significant life changes, such as caring for aging parents or children moving away from home, can also cause sleep problems.
National Women's Health Association funded by the National Institute on Aging (USA), in May 2009published an essay in the journal Neurology. The article said that women in perimenopause are indeed undergoing cognitive changes, especially in the area of cognitive function.
The article said that women in perimenopause are indeed undergoing cognitive changes, especially in the area of cognitive function.
University of California, Los Angeles researchers selected 2,362 women aged 42 to 52 years and divided them into groups according to a specific period in menopause: premenopause, early perimenopause, late perimenopause, and postmenopause. They were then given tests on verbal memory, working memory, and processing speed. It has been found that cognitive function in women in early or late perimenopause deteriorates but recovers immediately upon the onset of postmenopause. nine0018
These studies also suggested a possible solution to the problem. The researchers concluded that women who take hormones before their last period have better cognitive performance. However, hormones have a negative impact later. Since women take hormones earlier, at the age of 40-50, and not at 60-70, they do not fall into the risk group described in the Women's Health Initiative, where the subjects were 65 and older. However, you should consult your doctor about all the risks and benefits of using hormones. nine0018
However, you should consult your doctor about all the risks and benefits of using hormones. nine0018
To correct problems with memory and absent-mindedness, you can use the following recommendations:
If you feel that these methods do not help, talk to your doctor about treatment.
Treatments to relieve various symptoms of menopause include:
Oral contraceptives (OC): Oral contraceptives can help relieve various symptoms associated with early menopause, such as irregular periods and mood swings. Usually, OCs are prescribed for women who are still menstruating. For women younger than 50, there is an additional benefit - OCs protect against unwanted pregnancies.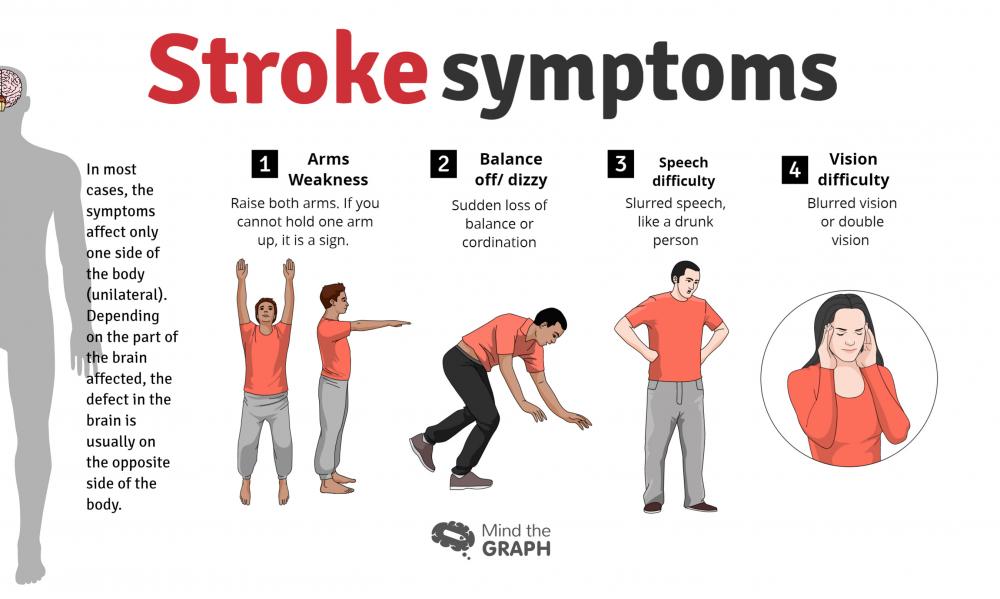 However, if OCs are taken when menopause is already in place, it becomes difficult to determine when menstruation ends. OK should not be taken by women who smoke, women with high blood pressure; migraines associated with atmospheric changes; history of diabetes, gallbladder disease, or blood clotting problems. Discuss your medical history with your doctor and ask about this treatment. nine0018
However, if OCs are taken when menopause is already in place, it becomes difficult to determine when menstruation ends. OK should not be taken by women who smoke, women with high blood pressure; migraines associated with atmospheric changes; history of diabetes, gallbladder disease, or blood clotting problems. Discuss your medical history with your doctor and ask about this treatment. nine0018
If you decide to take hormones rather than oral contraceptives to relieve your menopausal symptoms, be aware that there doses of estrogen and progesterone are usually sufficient for this purpose alone, but hormones are not good for contraception. Women of childbearing age should use higher hormonal contraceptives or use other means of contraception in addition to hormones.
Antidepressants . The antidepressants venlafaxine (Effexor), fluoxetine (Prozac), and paroxetine (Paxil) may alleviate hot flashes somewhat. However, the US Food and Drug Administration does not recommend taking antidepressants to treat hot flashes.