Stress response syndrome
Mental Health: Adjustment Disorder
Written by WebMD Editorial Contributors
In this Article
- What Is Adjustment Disorder (Stress Response Syndrome)?
- Adjustment Disorder vs. Major Depression
- Adjustment Disorder vs. Posttraumatic Stress Disorder (PTSD)
- Symptoms of Adjustment Disorder/Stress Response Syndrome (AD/SRS)
- AD/SRS Causes and Risk Factors
- Diagnosing AD/SRS
- AD/SRS Treatment and Home Care
- AD/SRS Prevention
What Is Adjustment Disorder (Stress Response Syndrome)?
Adjustment disorder (stress response syndrome) is a short-term condition that happens when you have great difficulty managing with, or adjusting to, a particular source of stress, such as a major life change, loss, or event. In 2013, the mental health diagnostic system technically changed the name of "adjustment disorder" to "stress response syndrome."
Because people with stress response syndrome often have some of the symptoms of clinical depression, such as tearfulness, feelings of hopelessness, and loss of interest in work or activities, adjustment disorder is sometimes informally called "situational depression. "
Adjustment Disorder vs. Major Depression
Adjustment syndrome/stress response syndrome has some symptoms that overlap with those of major depression. Unlike major depression, an adjustment disorder doesn't involve as many of the physical and emotional symptoms of clinical depression (such as changes in sleep, appetite, and energy) or high levels of severity (such as suicidal thinking or behavior).
Adjustment Disorder vs. Posttraumatic Stress Disorder (PTSD)
An adjustment disorder/stress response syndrome is not the same as posttraumatic stress disorder (PTSD). PTSD is a reaction to a life-threatening event that happens at least 1 month after the event, and its symptoms tend to last longer than in adjustment disorders/stress response syndromes. By comparison, adjustment disorders/stress response syndromes rarely last longer than 6 months.
Symptoms of Adjustment Disorder/Stress Response Syndrome (AD/SRS)
Adjustment disorder/stress response syndrome changes the way you feel and think about the world and your place in it.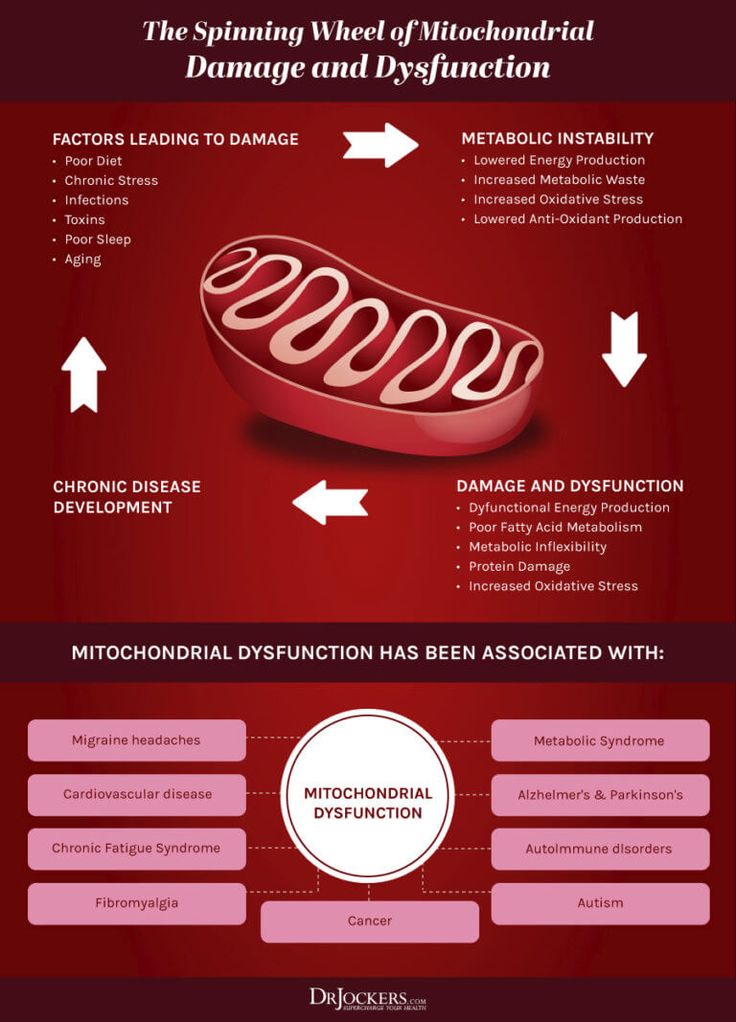 A person with AD/SRS has emotional and/or behavioral symptoms as a reaction to a stressful event. These symptoms generally begin within 3 months of the event and rarely last for longer than 6 months after the event or situation has ended.
A person with AD/SRS has emotional and/or behavioral symptoms as a reaction to a stressful event. These symptoms generally begin within 3 months of the event and rarely last for longer than 6 months after the event or situation has ended.
In adjustment disorder/stress response syndrome, the reaction to the stressor is greater than what is typical or expected for the situation or event. The symptoms may cause problems with a person's ability to function; for example, the person may have trouble with sleep, work, or studying. It can have a wide variety of symptoms that are changes from someone's usual self, which may include:
- Feeling of hopelessness
- Sadness
- Frequent crying
- Anxiety (nervousness)
- Worry
- Headaches or stomachaches
- Palpitations (an unpleasant sensation of irregular or forceful beating of the heart)
- Withdrawal or isolation from people and social activities
- A new pattern of absence from work or school
- New and out-of-the-ordinary dangerous or destructive behavior, such as fighting, reckless driving, and vandalism
- Changes in appetite; either loss of appetite or overeating
- Problems sleeping
- Feeling tired or without energy
- Using alcohol or other drugs more
Symptoms in children and teens tend to be more behavioral in nature, such as skipping school, fighting, or acting out.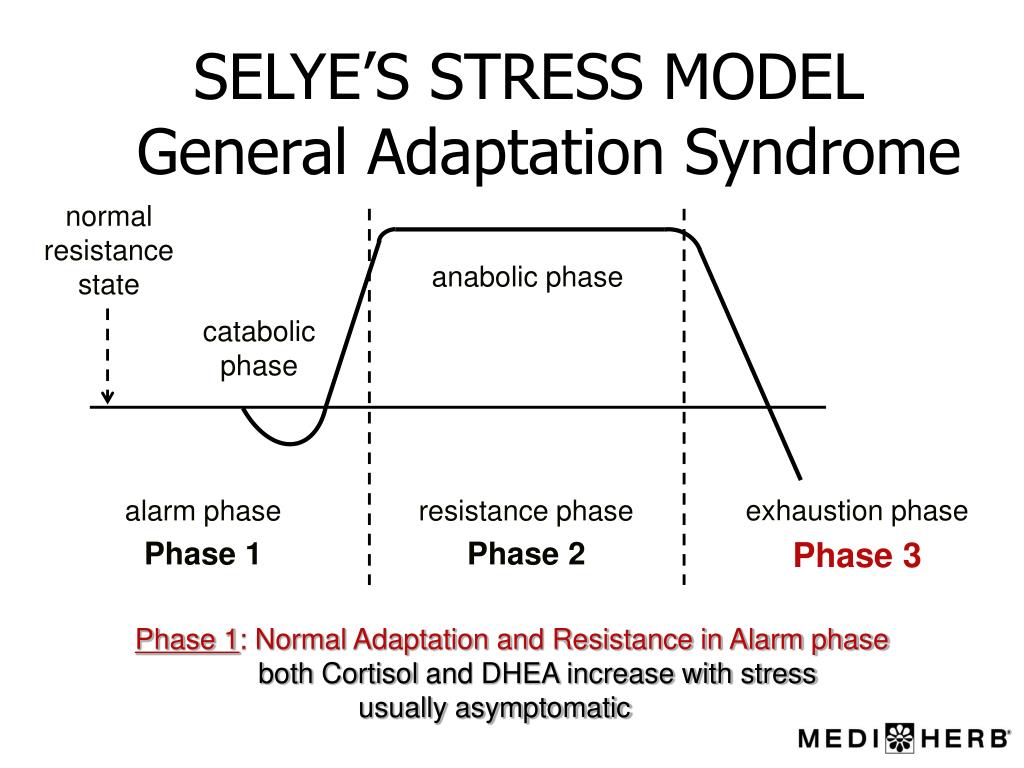 Adults, on the other hand, tend to have more emotional symptoms, such as sadness and anxiety.
Adults, on the other hand, tend to have more emotional symptoms, such as sadness and anxiety.
AD/SRS Causes and Risk Factors
AD/SRS is very common and can affect anyone, regardless of gender, age, race, or lifestyle. Although an adjustment disorder can occur at any age, it is more common at times of major transitions, such as adolescence, midlife, and late life.
The type of stress that can trigger an adjustment disorder/stress response syndrome varies depending on the person, but can include:
- Ending of a relationship or marriage
- Losing or changing a job
- Death of a loved one
- A serious illness (yourself or a loved one)
- Being a victim of a crime
- Having an accident
- Having a major life change (such as getting married, having a baby, or retiring from a job)
- Living through a disaster, such as a fire, flood, or hurricane
Diagnosing AD/SRS
If you suspect you may have an AD/SRS, see your doctor. If you have symptoms, your doctor may do a physical exam and ask questions about your medical and mental health histories. Although there are no imaging or lab tests to specifically diagnose the syndrome, the doctor may sometimes use laboratory tests -- such as blood or imaging tests like CT or MRI scans -- to rule out physical illness or other medical causes of changes in mood or behavior (such as head trauma) as the cause of your symptoms.
If you have symptoms, your doctor may do a physical exam and ask questions about your medical and mental health histories. Although there are no imaging or lab tests to specifically diagnose the syndrome, the doctor may sometimes use laboratory tests -- such as blood or imaging tests like CT or MRI scans -- to rule out physical illness or other medical causes of changes in mood or behavior (such as head trauma) as the cause of your symptoms.
If AD/SRS is suspected, your doctor will likely refer you to a psychiatrist, psychologist, or other mental health professional who is trained to help people when they have trouble coping with and managing stressful life events. They’ll look for other mental illnesses, such as posttraumatic stress disorder, major depression, or an anxiety disorder.
Your doctor will diagnose you with AD/SRS based on the criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM–5):
- A change in emotional or behavioral symptoms that happens within 3 months of a stressful event in your life
- Showing a level of distress that’s more intense than would normally be expected in response to what happened
- Having significant problems in your personal life and/or at work or school
- Symptoms that aren’t related to another illness or mental health disorder
AD/SRS Treatment and Home Care
If you have symptoms of AD/SRS, it is important that you seek medical care. Adjustment disorder can sometimes turn into major depressive episodes in people who are at risk for getting mood disorders. If you turn to alcohol or drugs to manage your stress and anxiety, you may develop a substance abuse problem.
Adjustment disorder can sometimes turn into major depressive episodes in people who are at risk for getting mood disorders. If you turn to alcohol or drugs to manage your stress and anxiety, you may develop a substance abuse problem.
Treatment for AD/SRS may include:
- Psychotherapy or talk therapy
- Medications, including antidepressants or anti-anxiety drugs
- Support groups
You can also take steps to build your resilience and feel better. Try these tips:
- Connect with friends and family.
- Find activities that give you purpose.
- Eat right and exercise.
- Sleep well.
- Work on your coping skills.
- Have a positive attitude.
- Recognize and build your strengths.
- Face your fears.
- Work to problem-solve.
Most people with adjustment disorder/stress response syndrome recover completely. In fact, a person who is treated for adjustment disorder/stress response syndrome may learn new skills that actually allow them to function better than before the symptoms began.
AD/SRS Prevention
There is no known way to prevent adjustment disorder/stress response syndrome. But strong family and social support can help a person work through a particularly stressful situation or event. The best prevention is early treatment, which can teach new coping skills, make symptoms less severe, and cut how long your symptoms last.
Adjustment disorders - Symptoms and causes
Overview
Adjustment disorders are stress-related conditions. You experience more stress than would normally be expected in response to a stressful or unexpected event, and the stress causes significant problems in your relationships, at work or at school.
Work problems, going away to school, an illness, death of a close family member or any number of life changes can cause stress. Most of the time, people adjust to such changes within a few months. But if you have an adjustment disorder, you continue to have emotional or behavioral reactions that can contribute to feeling anxious or depressed.
You don't have to tough it out on your own, though. Treatment can be brief and it's likely to help you regain your emotional footing.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Symptoms
Signs and symptoms depend on the type of adjustment disorder and can vary from person to person. You experience more stress than would normally be expected in response to a stressful event, and the stress causes significant problems in your life.
Adjustment disorders affect how you feel and think about yourself and the world and may also affect your actions or behavior. Some examples include:
- Feeling sad, hopeless or not enjoying things you used to enjoy
- Frequent crying
- Worrying or feeling anxious, nervous, jittery or stressed out
- Trouble sleeping
- Lack of appetite
- Difficulty concentrating
- Feeling overwhelmed
- Difficulty functioning in daily activities
- Withdrawing from social supports
- Avoiding important things such as going to work or paying bills
- Suicidal thoughts or behavior
Symptoms of an adjustment disorder start within three months of a stressful event and last no longer than 6 months after the end of the stressful event.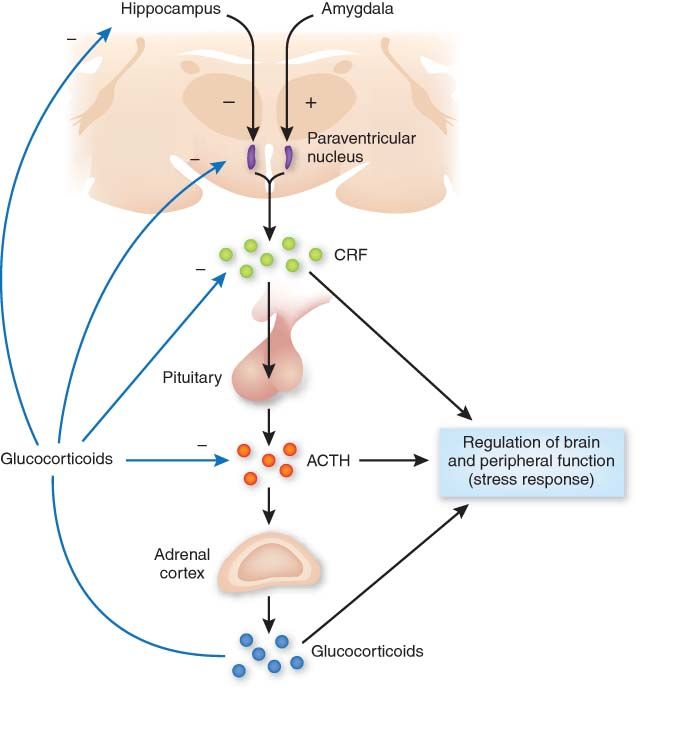 However, persistent or chronic adjustment disorders can continue for more than 6 months, especially if the stressor is ongoing, such as unemployment.
However, persistent or chronic adjustment disorders can continue for more than 6 months, especially if the stressor is ongoing, such as unemployment.
When to see a doctor
Usually stressors are temporary, and we learn to cope with them over time. Symptoms of adjustment disorder get better because the stress has eased. But sometimes the stressful event remains a part of your life. Or a new stressful situation comes up, and you face the same emotional struggles all over again.
Talk to your doctor if you continue to struggle or if you're having trouble getting through each day. You can get treatment to help you cope better with stressful events and feel better about life again.
If you have concerns about your child's adjustment or behavior, talk with your child's pediatrician.
Suicidal thoughts or behavior
If you have thoughts of hurting yourself or someone else, call 911 or your local emergency number immediately, go to an emergency room, or confide in a trusted relative or friend. Or call a suicide hotline number — in the United States, call the National Suicide Prevention Lifeline at 1-800-273-TALK (1-800-273-8255) to reach a trained counselor.
Or call a suicide hotline number — in the United States, call the National Suicide Prevention Lifeline at 1-800-273-TALK (1-800-273-8255) to reach a trained counselor.
Request an Appointment at Mayo Clinic
Causes
Adjustment disorders are caused by significant changes or stressors in your life. Genetics, your life experiences, and your temperament may increase your likelihood of developing an adjustment disorder.
Risk factors
Some things may make you more likely to have an adjustment disorder.
Stressful events
Stressful life events — both positive and negative — may put you at risk of developing an adjustment disorder. For example:
- Divorce or marital problems
- Relationship or interpersonal problems
- Changes in situation, such as retirement, having a baby or going away to school
- Adverse situations, such as losing a job, loss of a loved one or having financial issues
- Problems in school or at work
- Life-threatening experiences, such as physical assault, combat or natural disaster
- Ongoing stressors, such as having a medical illness or living in a crime-ridden neighborhood
Your life experiences
Life experiences can impact how you cope with stress. For example, your risk of developing an adjustment disorder may be increased if you:
For example, your risk of developing an adjustment disorder may be increased if you:
- Experienced significant stress in childhood
- Have other mental health problems
- Have a number of difficult life circumstances happening at the same time
Complications
If adjustment disorders do not resolve, they can eventually lead to more serious mental health problems such as anxiety disorders, depression or substance abuse.
Prevention
There are no guaranteed ways to prevent adjustment disorders. But developing healthy coping skills and learning to be resilient may help you during times of high stress.
If you know that a stressful situation is coming up — such as a move or retirement — call on your inner strength, increase your healthy habits and rally your social supports in advance. Remind yourself that this is usually time-limited and that you can get through it. Also consider checking in with your doctor or mental health professional to review healthy ways to manage your stress.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
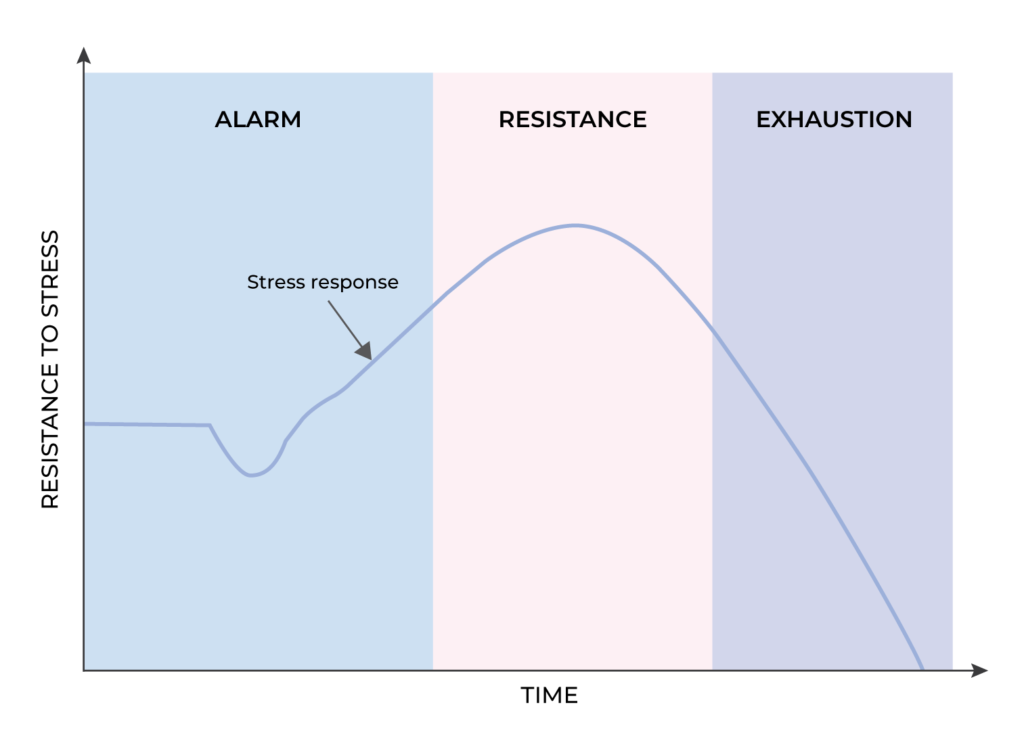
Selye's three stages of stress: anxiety, resistance, exhaustion
Hits: 232588 Published: / Updated:
- Stress
General information
Stress is one of the normal conditions of the body, as it is associated with an increase in adaptive mechanisms. Stress is an essential part of life. Stress reactions phylogenetically helped a person to cope with difficulties, therefore, in this aspect, stress reactions are useful. However, when stress has a vivid expression and a long manifestation, in this case it causes harm to human health.
Types of stress
According to the type of impact, stress is systemic and mental. Systemic stress reflects the body's response to injury, inflammation, infection, and so on.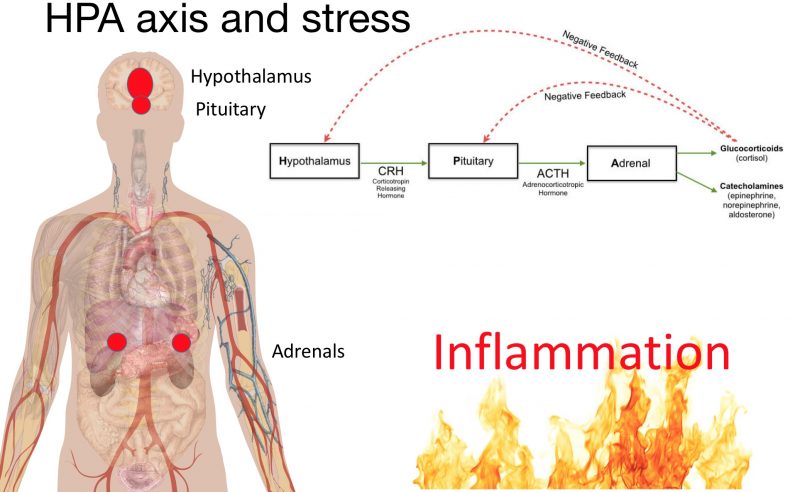 Mental stress first causes changes in the psycho-emotional sphere, and then manifests itself at the biological level.
Mental stress first causes changes in the psycho-emotional sphere, and then manifests itself at the biological level.
Selye's observations
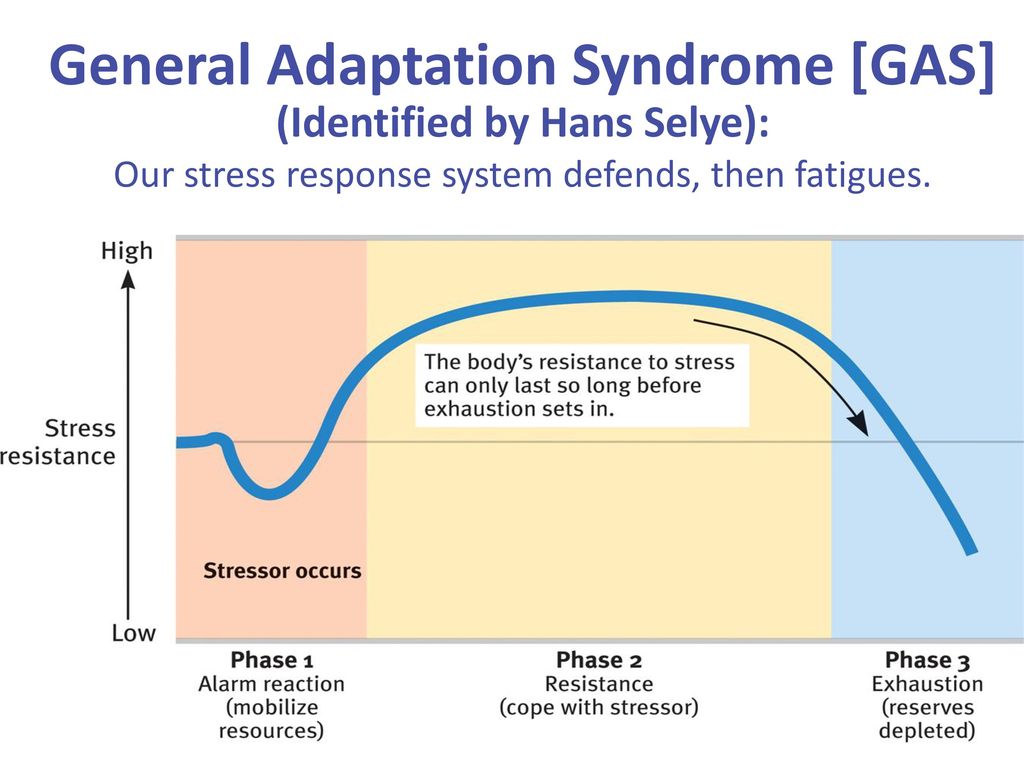
Hans Selye is considered the founder of the theory of biological stress. Hans Selye's model of the general adaptation syndrome provides a clear biological explanation for how the body reacts and adapts to stress.
In his research, Selye noticed that the body adapts to external stressors in terms of a biological model that tries to restore and maintain internal balance. In its attempt to maintain homeostasis, the body uses a hormonal response that directly combats the stressor. The body's struggle against stress is the main theme of the general adaptation syndrome.
Another observation that Selye made was that stress responses have their limits. The body's limited supply of energy to adapt to a stressful environment is depleted when the body is constantly exposed to a stressor.
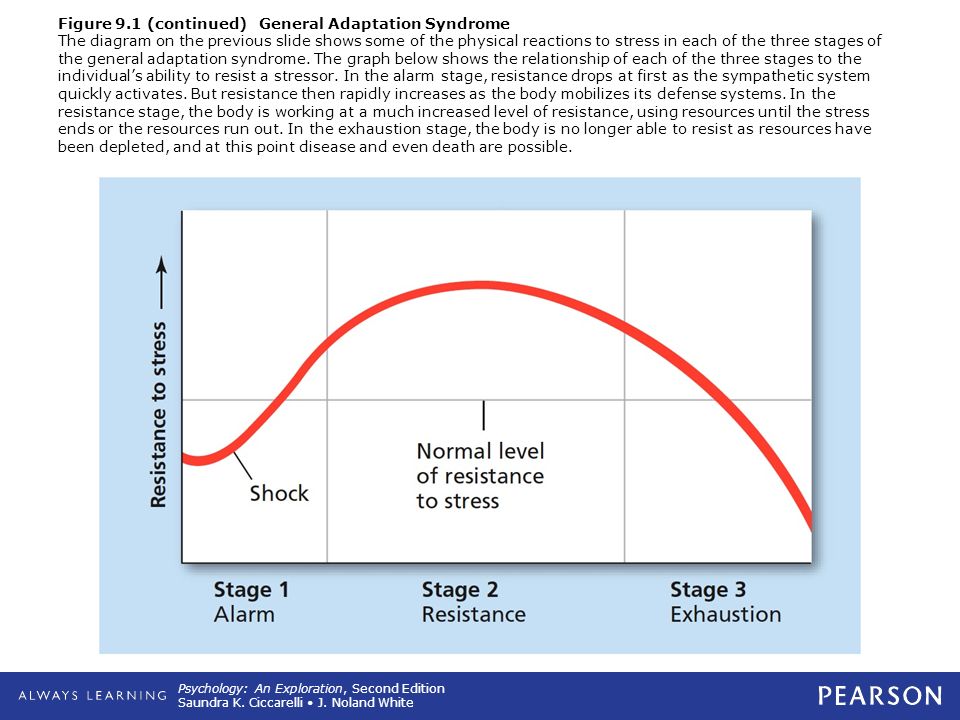
Three phases of the stress response
General Adaptation Syndrome is a model that consists of three elements or phases that describe the body's response to stress:
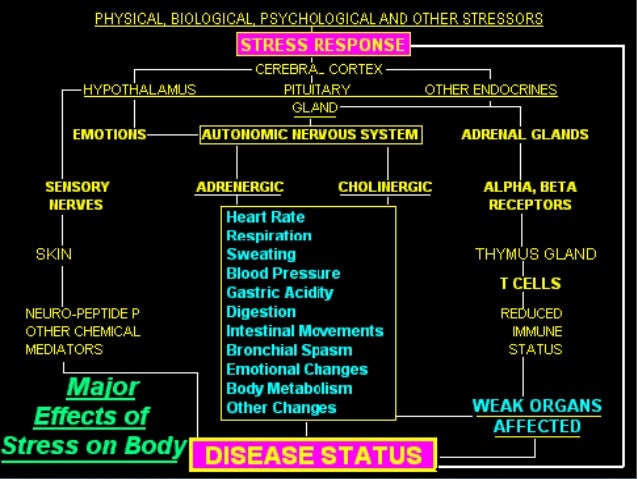
called the hypothalamus. The hypothalamus ensures the release of hormones called glucocorticoids.
Glucocorticoids trigger the release of adrenaline and cortisol. Adrenaline gives a person a boost of energy: the heart rate increases, blood pressure rises, blood sugar also rises. These physiological changes are regulated by a part of the human autonomic nervous system called the sympathetic branch.
The adrenal glands begin to actively produce an increased amount of cortisol and are in a state of hyperfunction. This condition can be confirmed by using a pattern of changes in the hormonal profile of saliva, which will be the following indicators: elevated cortisol levels / normal DHEA levels.
2. Resistance stage
During the resistance stage, the body attempts to counteract the physiological changes that occurred during the alarm reaction stage.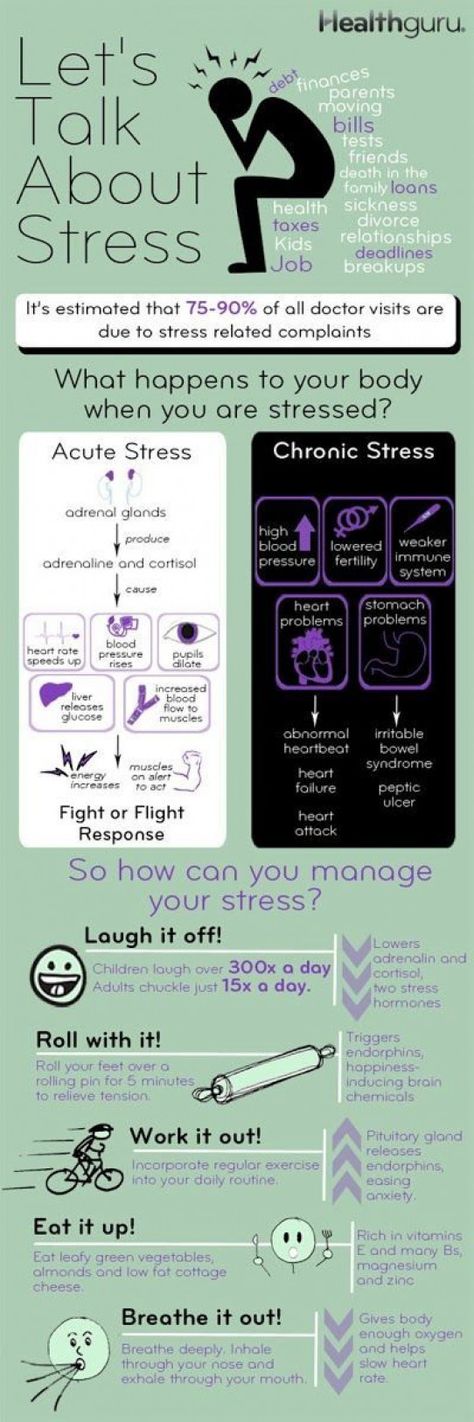 The resistance stage is regulated by a part of the autonomic nervous system called the parasympathetic.
The resistance stage is regulated by a part of the autonomic nervous system called the parasympathetic.
The parasympathetic nervous system is trying to bring the body back to normal: the amount of cortisol produced decreases, heart rate and blood pressure begin to return to normal. The level of body resistance is much higher than usual. At this stage, a balanced expenditure of adaptation resources is carried out.
If the stressful situation ends, the resistance phase returns the body to its normal state. However, if the stressor remains, the body remains on guard to fight its manifestations.
The adrenals adapt to this stage already using a mechanism called "pregnenolone hijack". Pregnenolone is a cholesterol metabolite and is the precursor chemical for the production of both cortisol and sex hormones, including testosterone. When the metabolism of pregnenolone changes, the level of testosterone produced in the body decreases. At this stage, the pattern of the hormonal profile in saliva will be represented by the following indicators: elevated cortisol/low DHEA.
3. Exhaustion stage
In this stage, stress persists for a long period. The body begins to lose the ability to deal with the stressor and reduce its harmful effects, as all adaptive capacity is depleted. The exhaustion stage can lead to stress overload and health problems if not addressed immediately.
At this stage, the adrenal glands are no longer able to adapt to stress and have exhausted their functionality. Initially, salivary hormonal profiles will show normal cortisol/low DHEA levels (or cortisol levels indicative of hyperfunction and reduced function will be combined with normal DHEA levels). When the adrenal glands have exhausted their capacity, will be determined: low cortisol / low DHEA.
If stress continues, the cofactors needed to produce cortisol are depleted, causing the body to break the pregnenolone bypass mechanism and switch back to producing DHEA. This pattern would be low cortisol/normal DHEA.
PTSD
") end if %>
Variant of Acrobat Samana Gaze | Acrobat Reader Samana Download
PTSD is a normal response
for severe traumatic events.
This booklet deals with signs,
symptoms and treatments for PTSD.
New York State
Department of Mental Health
Have you experienced a terrible and dangerous event? Note please, those cases in which you recognize yourself.
- Sometimes, out of the blue, everything that happened to me is happening again. I never know when to expect it again.
- I have nightmares and memories of the terrible incident which I have experienced.
- I avoid places that remind me of that incident.
- I jump on the spot and feel uneasy at any sudden movement or surprise. I feel alert all the time.
- It's hard for me to trust someone and get close to someone.
- Sometimes I just feel emotionally drained and deaf.
- I get angry very easily.
- I am tormented by guilt that others died, but I survived.
- I sleep poorly and experience muscle tension.
PTSD is a very serious condition that needs to be treated.
Many people who have experienced terrible events suffer from this disease.
It is not your fault that you fell ill, and you should not suffer from it.
Read this booklet to find out how you can be helped.
You can get well and enjoy life again!
What is post-traumatic stress disorder (PTSD/PTSD)?
PTSD is a very serious condition. PTSD symptoms may occur in a person who has experienced a terrible traumatic event. This disease is susceptible medical and therapeutic treatment.
PTSD can occur after you:
- Have been a victim of sexual abuse
- Have been a victim of physical or emotional domestic violence
- Victim of a violent crime
- Been in a car accident or plane crash
- Survived a hurricane, tornado or fire
- Were at war
- Survived a life-threatening event
- Witnessed any of the above events
If you have post-traumatic stress disorder, you often have nightmares or memories associated with the event. you try to hold on away from anything that might remind you of the experience.
you try to hold on away from anything that might remind you of the experience.
You are angry and unable to trust or care for others. You are always on your guard and see a hidden threat in everything. You become not by itself, when something happens suddenly and without warning.
When does PTSD start and how long does it last?
In most cases, post-traumatic stress manifests itself approximately three months after the traumatic event. In some cases, signs Post-traumatic stress symptoms only show up years later. Post-traumatic Stress affects people of all ages. Even children are not immune from it.
Some get better after six months, others may suffer from it illness for much longer.
Am I the only one with this disease?
No, you are not alone. Every year, 5.2 million Americans suffer from PTSD.
Women suffer from this disease two and a half times more often than men. The most common traumatic events that cause PTSD in men are: rape, participation in hostilities, abandonment and abuse in childhood.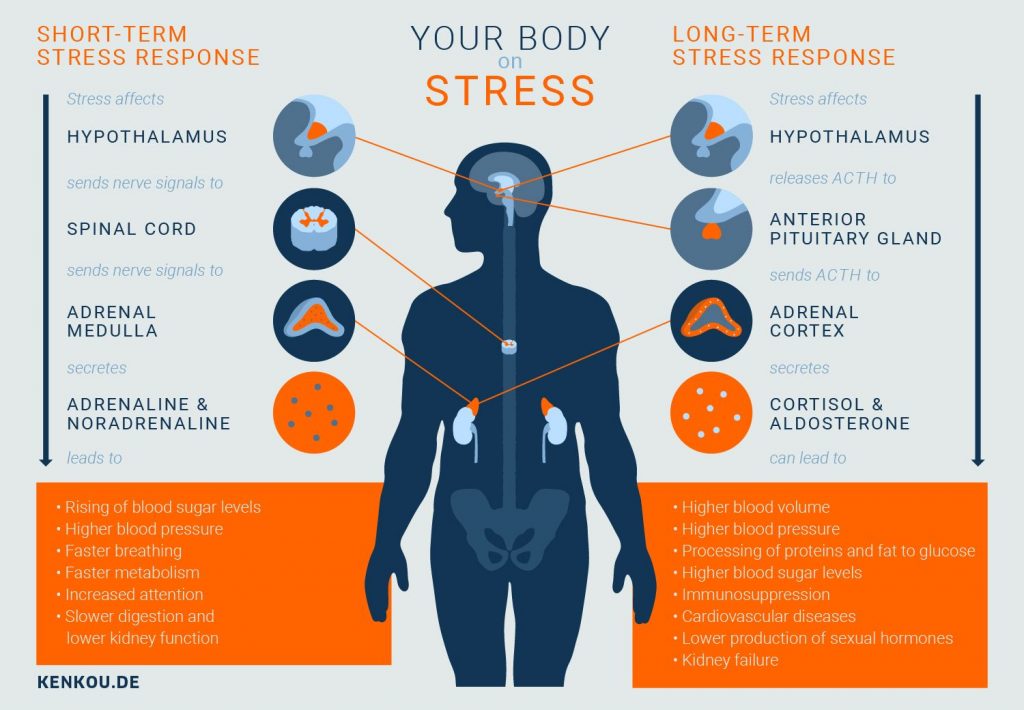 The most traumatic events in women are rape, sexual molestation, physical assault, threat weapons and childhood abuse.
The most traumatic events in women are rape, sexual molestation, physical assault, threat weapons and childhood abuse.
What other conditions can accompany PTSD?
Comorbid depression, alcohol and drug addiction, or other common anxiety disorders. The likelihood of successful treatment increases if these comorbidities to identify and treat in time.
Frequent headaches, gastroenterological problems, problems with the immune system, dizziness, chest pain or discomfort in other parts of the body. It often happens that a doctor treats physical symptoms, unaware that their cause lies in PTSD.
The National Institute of Mental Health (NIMH) recommends therapists to learn from patients about experiences of violence, recent losses and traumatic events, especially when symptoms persist are returning. After diagnosing PTSD, it is recommended to refer patient to a mental health specialist who has experience in the treatment of patients with PTSD.
What can I do to help myself in this situation?
Talk to your doctor and tell him about your experience, and how you feel. If you are visited by terrible memories, overcomes depression and sadness if you have trouble sleeping and constantly embittered - you should tell your doctor about all this. Tell him Are any of these conditions preventing you from doing your daily activities? lead a normal life. You may want to show this booklet to your doctor. This may help explain to him how you feel. Ask your doctor examine you to make sure there are no physical illnesses.
Ask your doctor if he has previously had patients suffering from post-traumatic stress. If your doctor does not have a special preparation, ask him for directions to doctor with relevant experience.
How can a doctor or psychotherapist help me?
Your doctor may prescribe medication to help reduce your fear or tension.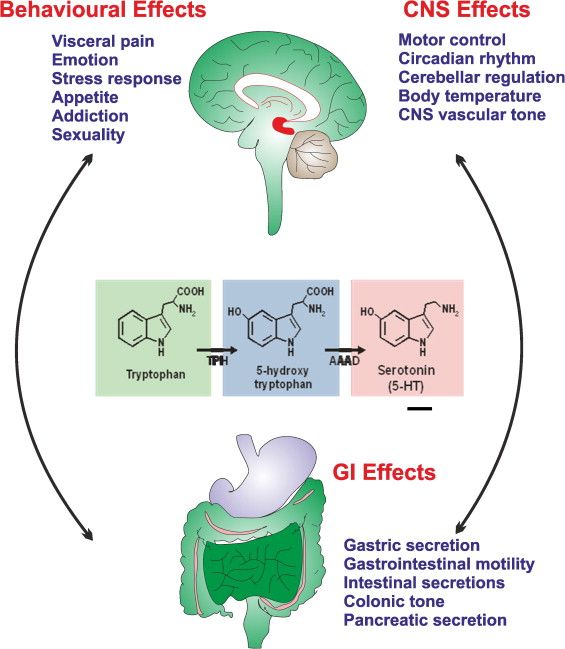 However, it should be borne in mind that usually several weeks before the medicine starts to work.
However, it should be borne in mind that usually several weeks before the medicine starts to work.
Many PTSD sufferers benefit from talking with a professional or other people who have experienced traumatic events. This is called "therapy". Therapy will help you get over your nightmare.
One man's story:
"After I was attacked, I He constantly felt fear and depression, became irritable. I couldn't sleep well and lost my appetite. Even when I tried not think about what happened, I was still tormented nightmares and terrible memories.
“I was completely at a loss and didn't know what to do. one buddy advised to see a doctor. My doctor helped me find a specialist in post-traumatic stress."
“I needed a lot of strength, but after medication and a course of therapy, I gradually come to my senses. It’s good that I called my doctor then.”
PTSD and the military
If you are in the military, you have probably been in combat.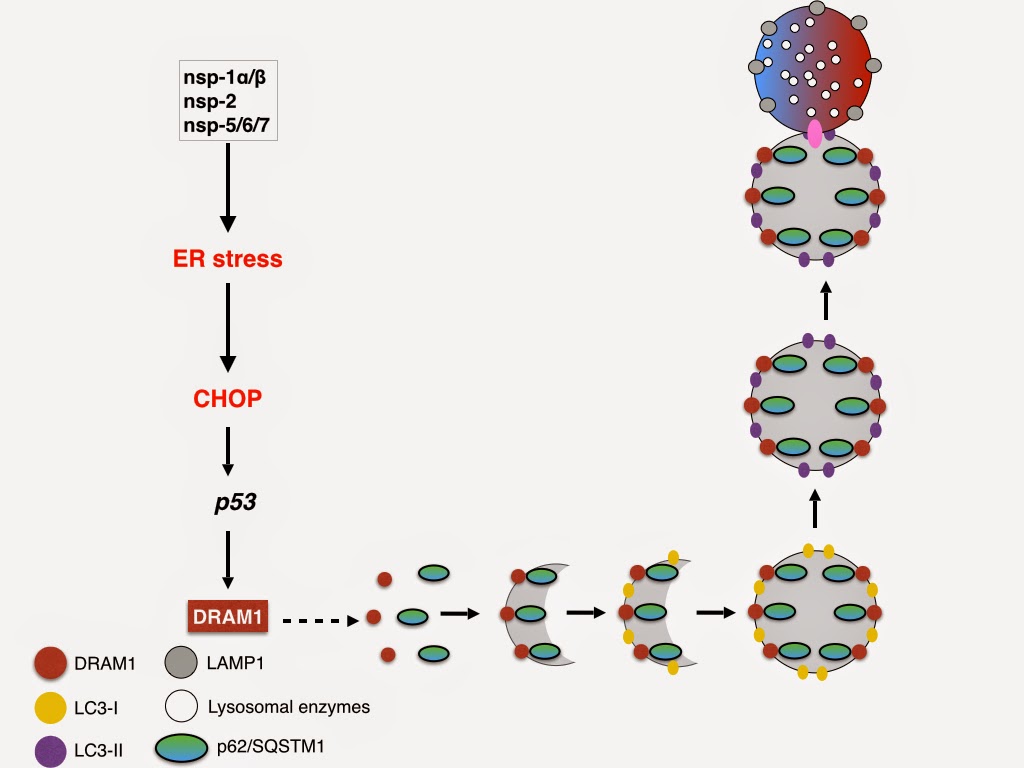 You, probably got into terrible and life-threatening situations. They shot at you you have seen your friend shot, you have seen death. experienced you events can cause PTSD.
You, probably got into terrible and life-threatening situations. They shot at you you have seen your friend shot, you have seen death. experienced you events can cause PTSD.
Experts say PTSD occurs:
- Nearly 30% of Vietnam War veterans
- Nearly 10% of Gulf War veterans (Operation Desert Storm)
- Almost 25% of veterans of the war in Afghanistan (operations "Introducing freedom") and veterans of the war in Iraq (operations "Iraqi Freedom")
Other factors of the military situation can serve as an additional stress to and so stressful situation and can contribute to the development of PTSD and other mental problems. Among these factors are the following: your military specialty, the political aspects of the war, where the battle takes place and who your enemy is.
Another reason that contributes to PTSD in military personnel can be Military Sexual Assault (MST) – any form of sexual harassment or sexual abuse while serving in the military. MST can happen with men and women, and can occur in peacetime, during war training or during the war.
MST can happen with men and women, and can occur in peacetime, during war training or during the war.
Veterans Affairs (VA) health care approximately:
- 23 out of 100 women (23%) report sexual violence during military service
- 55 out of 100 women (55%) and 38 out of 100 men (38%) were exposed to sexual harassment while serving in the army
Although the trauma of sexual assault is more common in the military among women, more than half of veterans who have experienced sexual trauma violence in the army - it's men.
Remember, you can get the help you need right now:
Tell your doctor about your experience and how you feel. If your doctor does not have special training in the treatment of PTSD, ask him for a referral to a doctor who has relevant experience.
PTSD research
To help those suffering from PTSD, the National Institute of Conservation Mental Health (NIMH) supports research into the study of PTSD, as well as other thematically related to PTSD research on problems anxiety and fear.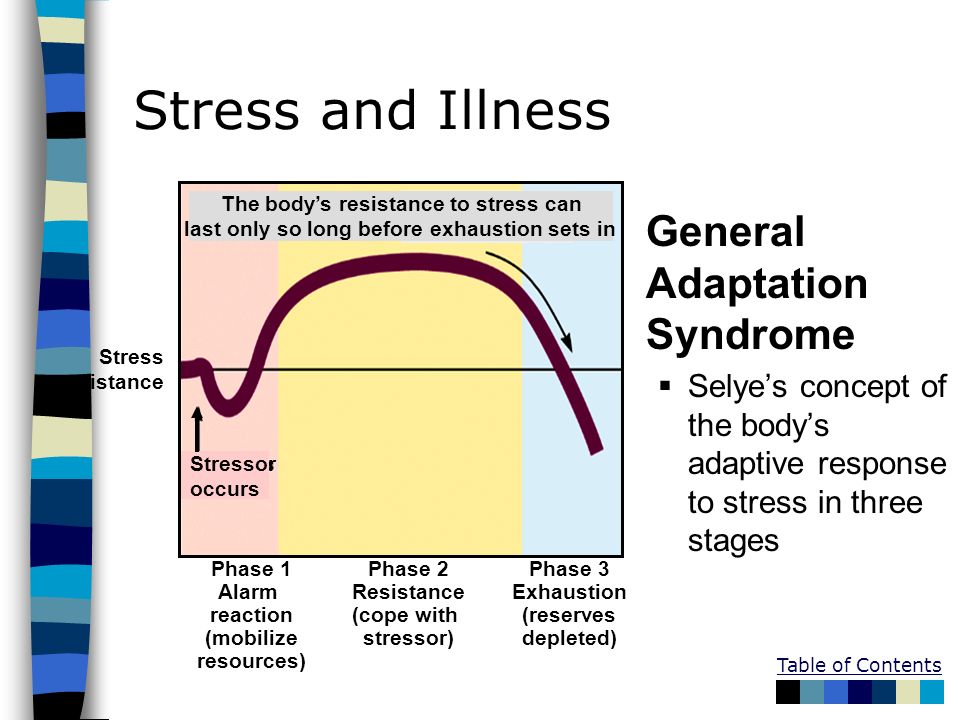 The challenge for research is to find new ways to help people cope with trauma, as well as find new treatment options and, The main thing is to prevent disease.
The challenge for research is to find new ways to help people cope with trauma, as well as find new treatment options and, The main thing is to prevent disease.
Research on possible risk factors for PTSD
Today, the attention of many scientists is focused on the genes that play a role in having terrible memories. Understanding the mechanism of "creation" of scary memories can help improve or find new ways to alleviate symptoms of PTSD. For example, PTSD researchers have identified genes that are responsible for:
Statmin - a protein involved in the formation terrible memories. During one experiment, mice were placed in environment designed to instill fear in them. In this situation mice lacking the statmin gene, in contrast to normal mice were less likely to "freeze" - i.e. exercise natural defensive response to danger. Also in the environment designed to evoke innate fear in them, they demonstrated it to a lesser extent than normal mice, more willingly mastering the open "dangerous" space.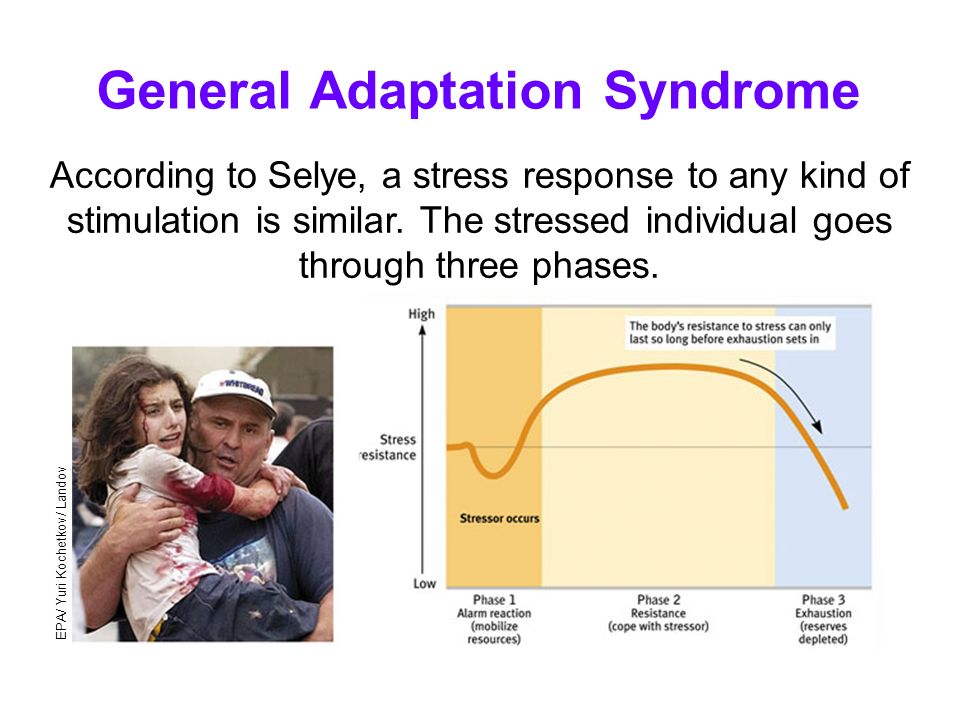 1
1
GRP (gastrin-releasing peptide/ GRP) - signal substance brain released during emotional events. At in mice, GWP helps control the fear response, and lack of GWP can lead to a longer memory of fear. 2
Scientists have also discovered a variant of the 5-HTTLPR gene that controls the level of serotonin (a brain substance associated with mood), which, as it turns out, feeds the fear response. 3 It seems that, like in the case of other mental disorders, in the development of PTSD different genes are involved, each of which contributes to the formation of the disease.
Understanding the causes of PTSD can also be helped by studying different areas brain responsible for fear and stress. One of these areas is cerebellar amygdala, responsible for emotions, learning and memory. It turned out that she plays an active role in the emergence of fear (or other words, "teaches" to be afraid of something, for example, to touch a hot stove), as well as in the early phases of fear repayment (or in other words, "teaches" Do not be scared).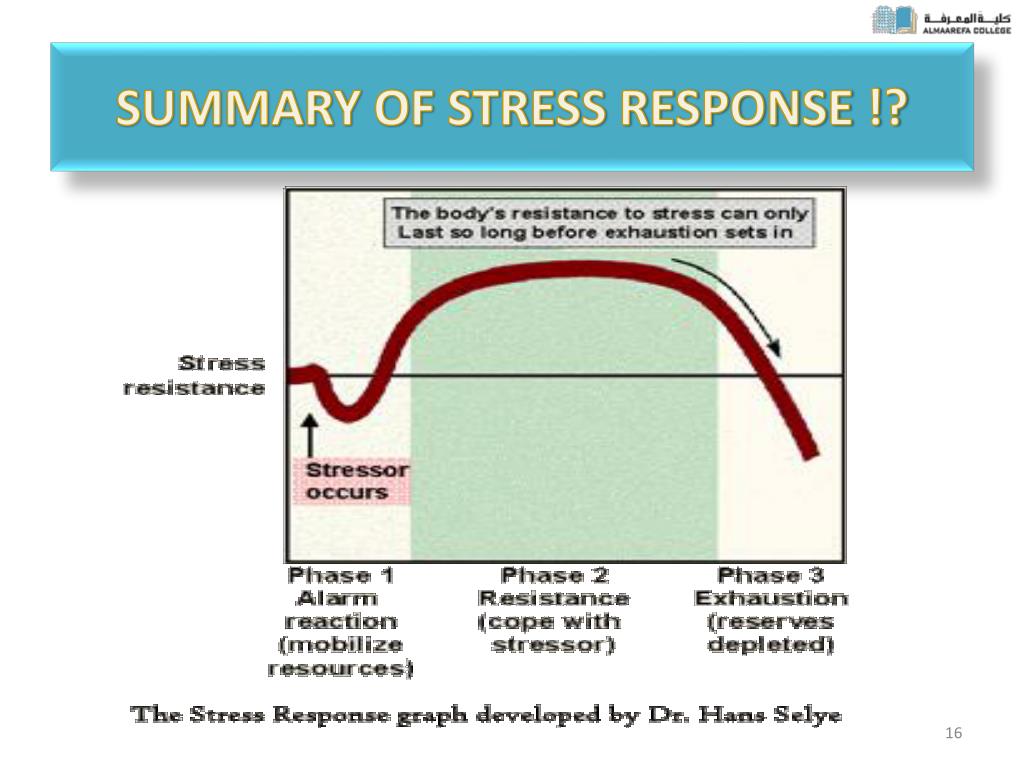 4
4
The storage of faded memories and the weakening of the initial fear reaction are associated with the prefrontal cortex (PFC / PFC) of the brain, 4 responsible for decision making, problem solving and situation assessment. Each zone PFC has its own role. For example, when the PFC believes that a stressor is amenable to control, the medial prefrontal zone of the PFC suppresses the anxiety center deeply in the brainstem and controls the response to stress. 5 Ventromedial PFC helps maintain long-term fading of fearful memories, and her ability to perform this feature can be affected by its size. 6
Individual differences in genes or characteristics of regions of the brain brain can only set the stage for PTSD, but by themselves do not cause no symptoms. environmental factors such as childhood trauma, head trauma or mental illness in family, favor the development of the disease and increase the risk of disease, affecting the brain in the early stages of its growth.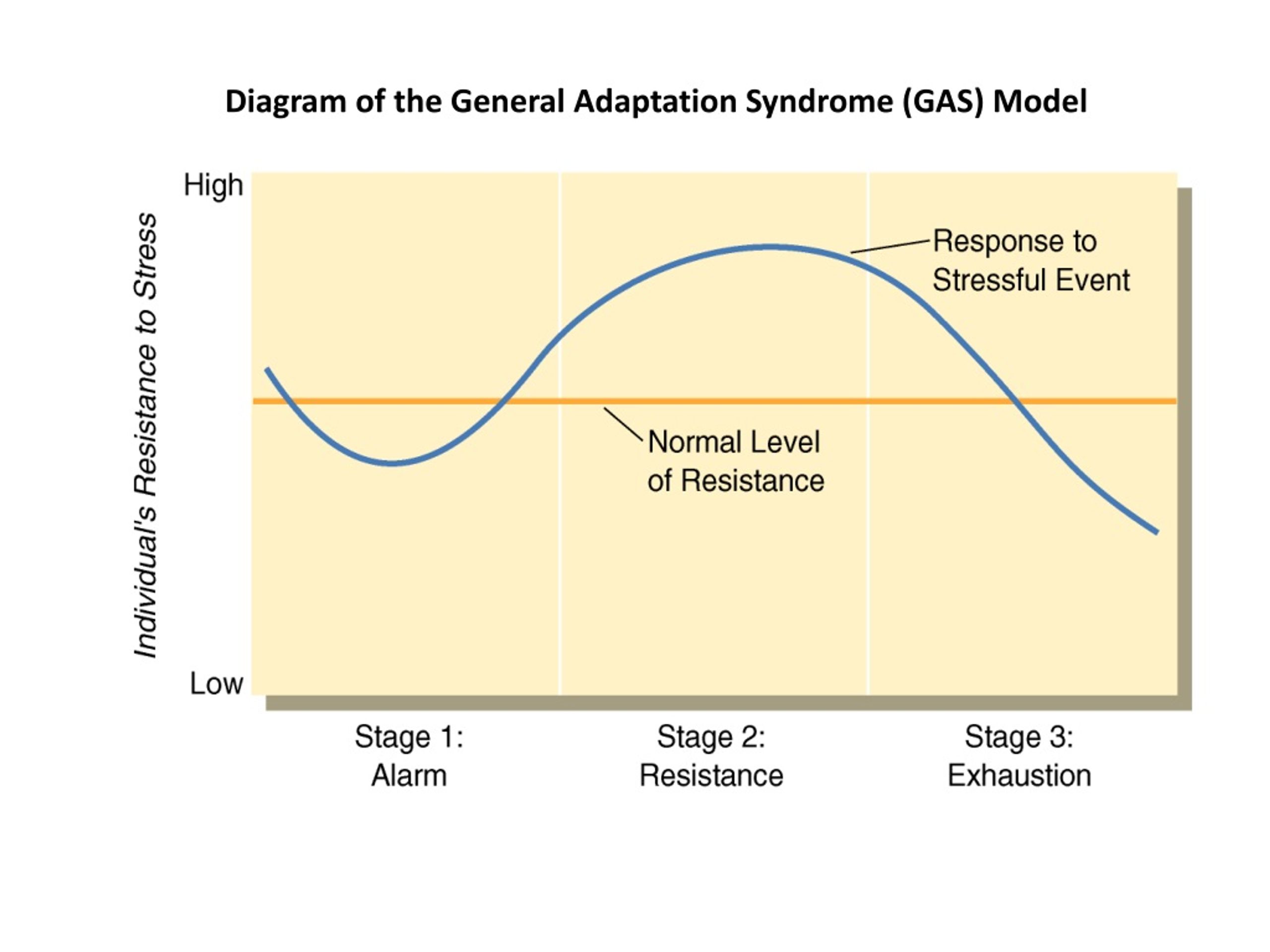 7 Except In addition, how people adapt to trauma is likely to be influenced by and characteristics of character and behavior, such as optimism and a tendency to consider problems in a positive or negative way, as well as social factors such as availability and use of social support. 8 Further research may show what combination of these factors or what other factors will allow ever predict who has a traumatic event cause PTSD, and who doesn't.
7 Except In addition, how people adapt to trauma is likely to be influenced by and characteristics of character and behavior, such as optimism and a tendency to consider problems in a positive or negative way, as well as social factors such as availability and use of social support. 8 Further research may show what combination of these factors or what other factors will allow ever predict who has a traumatic event cause PTSD, and who doesn't.
PTSD research
Currently, psychotherapy is used in the treatment of PTSD ("talk" therapy), drugs or drug-therapeutic combination.
Psychotherapy
Cognitive behavioral therapy (CBT) helps you learn differently think and react to frightening events that are the impetus for development PTSD, and can help bring the symptoms of the disease under control. There are several types cognitive behavioral therapy, including:
"Push" method - uses mental images, writing or visiting a place experienced trauma to help those affected face the overwhelming their fear and take control of it.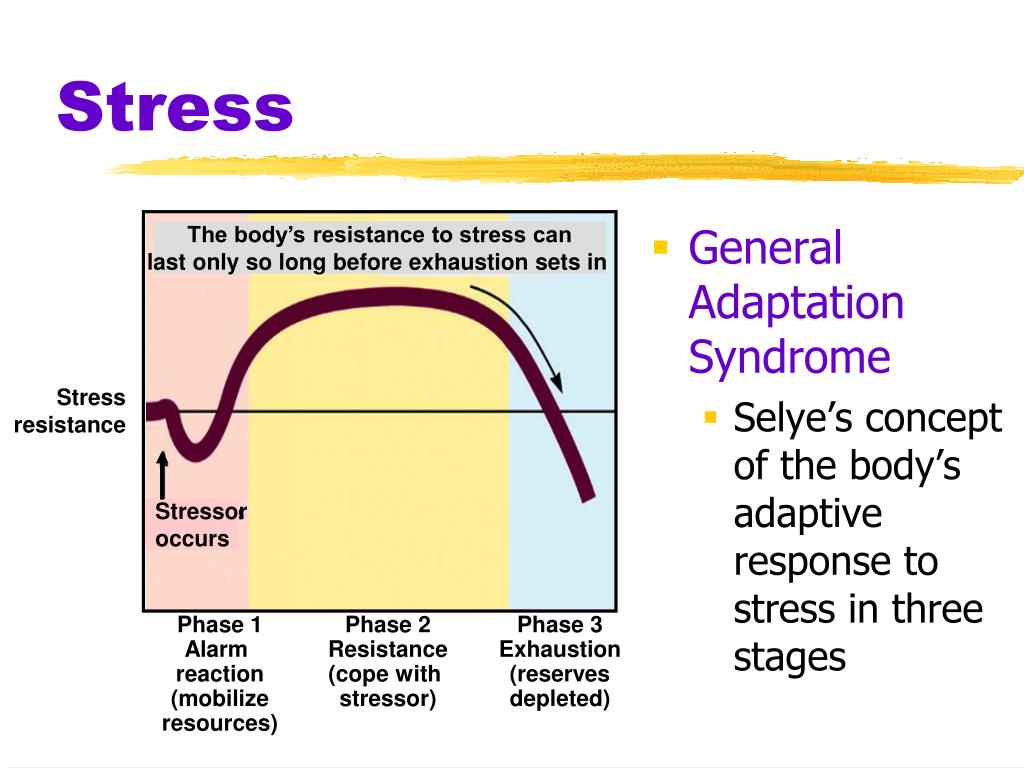
Behavior restructuring (cognitive restructuring) - encourages survivors of a traumatic event express depressing (often erroneous) thoughts about experienced trauma, challenge these thoughts and replace them with more balanced and appropriate.
Implementation in a stressful situation - teaches ways to reduce anxiety and the ability to cope with it, helping to reduce the symptoms of PTSD, and helps to correct the erroneous train of thought associated with the trauma experienced. NIMH is currently conducting research to study the reaction brain response to cognitive behavioral therapy versus response sertraline (Zoloft) - one of two drugs recommended and approved US Food and Drug Administration funds (FDA) for the treatment of post-traumatic stress. This research may help find out why some people respond better to medications, and others for psychotherapy
Medicines
Recently, in a small study, NIMH scientists found that if patients who are already taking a dose of prazosin (Minipress) at bedtime, add a daily dose, then this weakens the general symptoms of PTSD and stress reaction to reminders of the trauma experienced.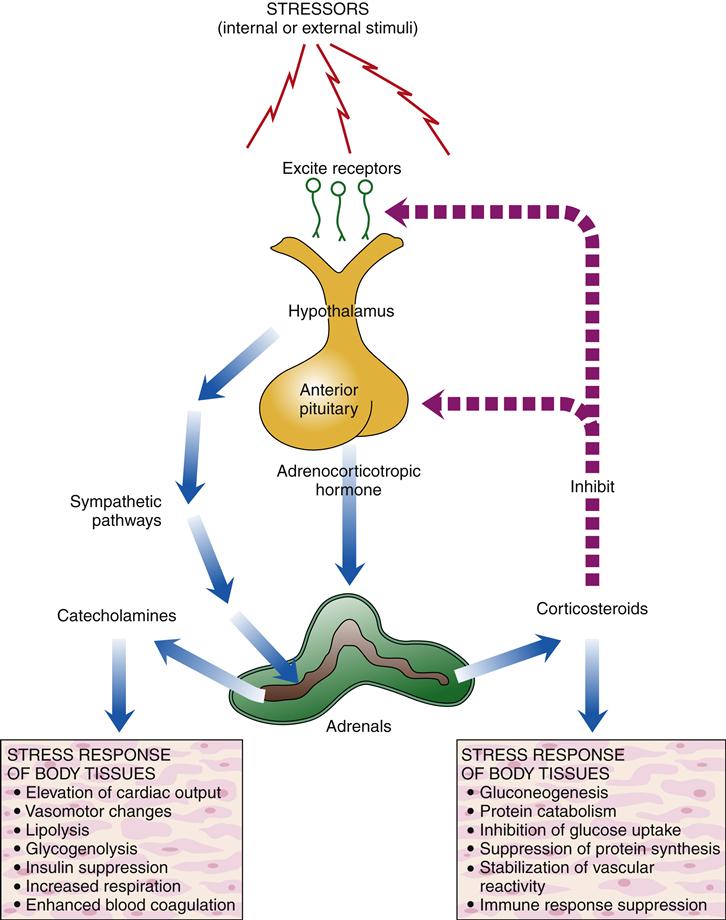 9
9
Another drug of interest is D-cycloserine (Seromycin), which increases the activity of a brain substance called N-methyl-D-aspartate, needed to pay off fear. During the study, which was attended by 28 people suffering from a fear of heights, scientists found that patients who received "push" therapy before a session D-cycloserine, showed lower levels of fear during the session compared to those who did not receive the drug. 10 Currently scientists study the effectiveness of the combined use of D-cycloserine and therapy for the treatment of post-traumatic stress.
Propranolol (Inderal), a beta-blocker drug, also under study whether it can be used to reduce post-traumatic stress and break the chain of scary memories. First experiments gave consoling results: it was possible to successfully weaken and, it seems, prevent PTSD in a small number of victims of traumatic events. 11
For example, in one preliminary study, researchers created a website self-help, based on the use of a psychotherapeutic method implementation in a stressful situation.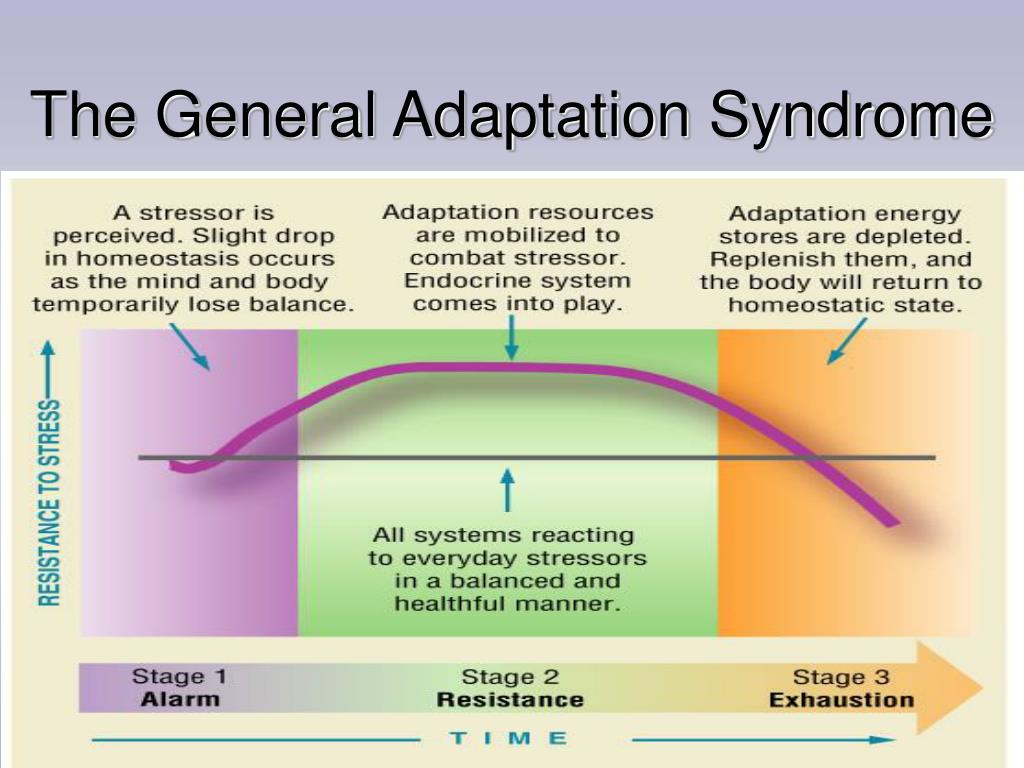 First, patients with PTSD meet in person with doctor. After this meeting, participants can go to the site to find more information about PTSD and how to deal with the problem; their doctors may also visit the site to give advice or briefing. In general, scientists believe that therapy in this form - promising treatment for a large number of people suffering from PTSD. 12
First, patients with PTSD meet in person with doctor. After this meeting, participants can go to the site to find more information about PTSD and how to deal with the problem; their doctors may also visit the site to give advice or briefing. In general, scientists believe that therapy in this form - promising treatment for a large number of people suffering from PTSD. 12
Scientists are also working to improve methods for testing early treatment and monitoring of survivors of massive trauma, on developing ways to teach them self-assessment skills and introspection and referral mechanism to psychiatrists (if necessary).
Prospects for PTSD research
In the last decade, rapid progress in the study of mental and biological PTSD has led scientists to conclude that there is a need to focus on prevention, as the most realistic and important goal.
For example, in order to find ways to prevent PTSD, with funding NIMH conducts research to develop new and orphan drugs, aimed at combating the underlying causes of the disease.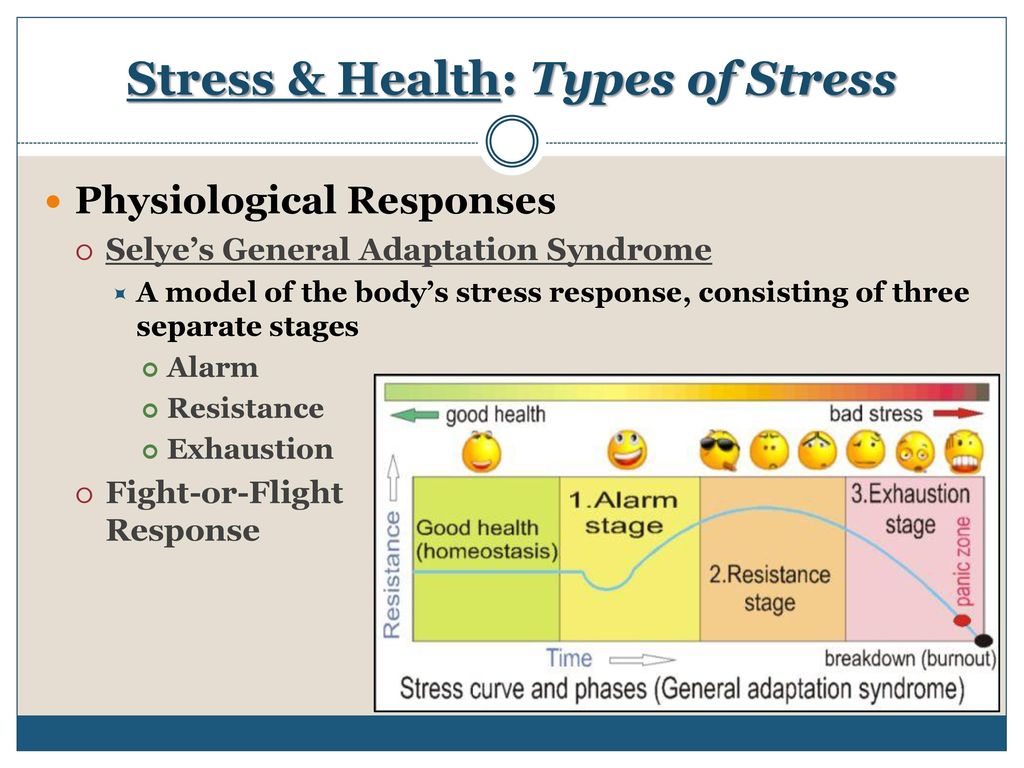 During another research scientists are looking for ways to enhance behavioral, personality and social protective factors and minimizing risk factors for prevent the development of PTSD after trauma. Another study is studying the question of what factors influence the difference in response to one or another method of treatment, which will help in the development of more individual, effective and productive methods of treatment.
During another research scientists are looking for ways to enhance behavioral, personality and social protective factors and minimizing risk factors for prevent the development of PTSD after trauma. Another study is studying the question of what factors influence the difference in response to one or another method of treatment, which will help in the development of more individual, effective and productive methods of treatment.
Where can I find more information?
MedlinePlus - resource from the American National Library of Medicine (U.S. National Library of Medicine and the National Institutes of Health) - offers the latest information on many health issues. Information about You can find PTSD at: www.nlm.nih.gov/medlineplus/posttraumaticstressdisorder.html.
National Institute of Mental Health
Office of Science Policy, Planning, and Communications
[National Institute of Mental Health
Science Policy Division research, planning and communications]
6001 Executive Boulevard
Room 8184, MSC 9663
Bethesda, MD 20892-9663
Phone: 301-443-4513; Fax: 301-443-4279
fax answering system Free answering machine: 1-866-615-NIMH (6464)
Text phone: 1-866-415-8051 toll-free
Email: nimhinfo@nih.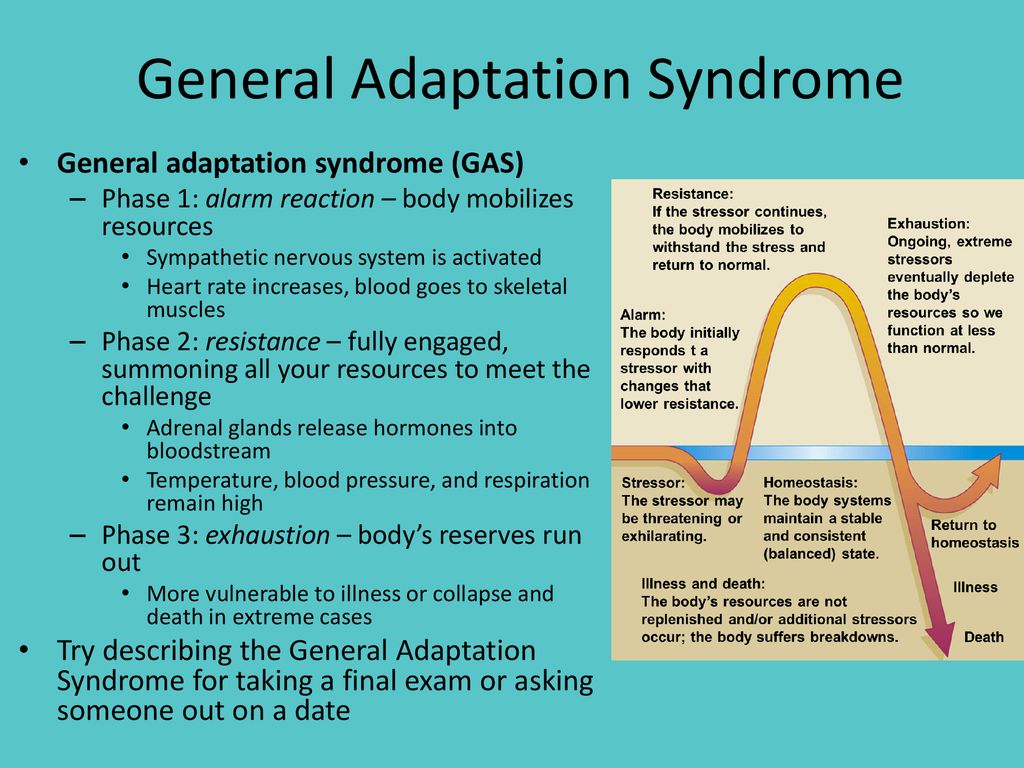 gov
gov
National Center for Post-traumatic Stress Disorder
[National PTSD Center]
VA Medical Center (116D)
215 North Main Street
White River Junction, VT 05009
802-296-6300
www.ncptsd.va.gov
NOTES
- Shumyatsky GP, Malleret G, Shin RM, et al. Stathmin, a Gene Enriched in the Amygdala, Controls Both Learned and Innate Fear. cell. Nov 18 2005;123(4):697-709.
- Shumyatsky GP, Tsvetkov E, Malleret G, et al. Identification of a signal network in lateral nucleus of amygdala important for inhibiting memory specifically related to learned fear. cell. Dec 13 2002;111(6):905-918.
- Hariri AR, Mattay VS, Tessitore A, et al. Serotonin transporter genetic variation and the response of the human amygdala.Science. Jul 192002;297(5580):400-403.
- Milad MR, Quirk GJ. Neurons in medial prefrontal cortex signal memory for fear extinction.
 Nature. Nov 7 2002;420(6911):70-74.
Nature. Nov 7 2002;420(6911):70-74. - 5 Amat J, Baratta MV, Paul E, Bland ST, Watkins LR, Maier SF. Medial prefrontal cortex determines how stressor controllability affects behavior and dorsal raphe nucleus. Nat Neurosci. Mar 2005;8(3):365-371.
- Milad MR, Quinn BT, Pitman RK, Orr SP, Fischl B, Rauch SL. Thickness of ventromedial prefrontal cortex in humans is correlated with extinction memory. Proc Natl Acad Sci USA. Jul 26 2005;102(30):10706-10711.
- Gurvits TV, Gilbertson MW, Lasko NB, et al. Neurological soft signs in chronic posttraumatic stress disorder.Arch Gen Psychiatry. Feb 2000;57(2):181-186.
- Brewin CR. Risk factor effect sizes in PTSD: what this means for intervention. J Trauma Dissociation. 2005;6(2):123-130.
- Taylor FB, Lowe K, Thompson C, et al. Daytime Prazosin Reduces Psychological Distress toTrauma Specific Cues in Civilian Trauma Posttraumatic stress disorder.
 Biol Psychiatry. Feb 3 2006.
Biol Psychiatry. Feb 3 2006. - Ressler KJ, Rothbaum BO, Tannenbaum L, et al. Cognitive enhancers as adjuncts to psychotherapy: use of D-cycloserine in phobic individuals to facilitate extinction of fear. Arch Gen Psychiatry. Nov 2004;61(11):1136-1144.
- Pitman RK, Sanders KM, Zusman RM, et al. Pilot study of secondary prevention of posttraumatic stress disorder with propranolol.Biol Psychiatry. Jan 15 2002;51(2):189-192.
- Litz BTWL, Wang J, Bryant R, Engel CC.A therapist-assisted Internet self-help program for traumatic stress. Prof Psychol Res Pr. December 2004;35(6):628-634.
New York State Department of Mental Health expresses thanks to the National Institute of Mental Health for the information, used in this booklet.
Published by the State Division of Mental Health New York, June 2008.
New York State
Andrew M. Cuomo, Governor
Mental Health Division
Head of Department Michael F.