Schizoaffective personality disorder
Schizoid personality disorder - Symptoms and causes
Overview
Schizoid personality disorder is an uncommon condition in which people avoid social activities and consistently shy away from interaction with others. They also have a limited range of emotional expression.
If you have schizoid personality disorder, you may be seen as a loner or dismissive of others, and you may lack the desire or skill to form close personal relationships. Because you don't tend to show emotion, you may appear as though you don't care about others or what's going on around you.
The cause of schizoid personality disorder is unknown. Talk therapy, and in some cases medications, can help.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Symptoms
If you have schizoid personality disorder, it's likely that you:
- Prefer being alone and choose to do activities alone
- Don't want or enjoy close relationships
- Feel little if any desire for sexual relationships
- Feel like you can't experience pleasure
- Have difficulty expressing emotions and reacting appropriately to situations
- May seem humorless, indifferent or emotionally cold to others
- May appear to lack motivation and goals
- Don't react to praise or critical remarks from others
Schizoid personality disorder usually begins by early adulthood, though some features may be noticeable during childhood. These features may cause you to have trouble functioning well in school, a job, socially or in other areas of life. However, you may do reasonably well in your job if you mostly work alone.
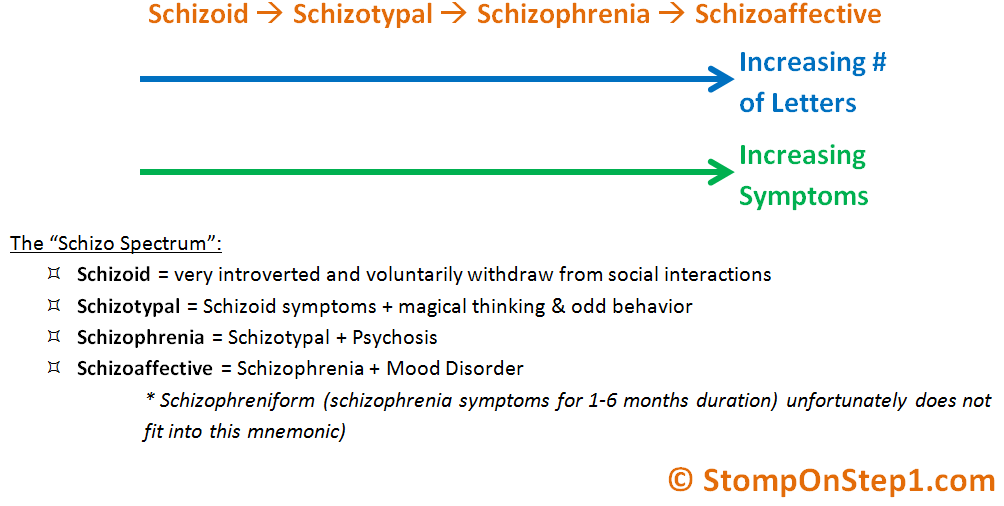
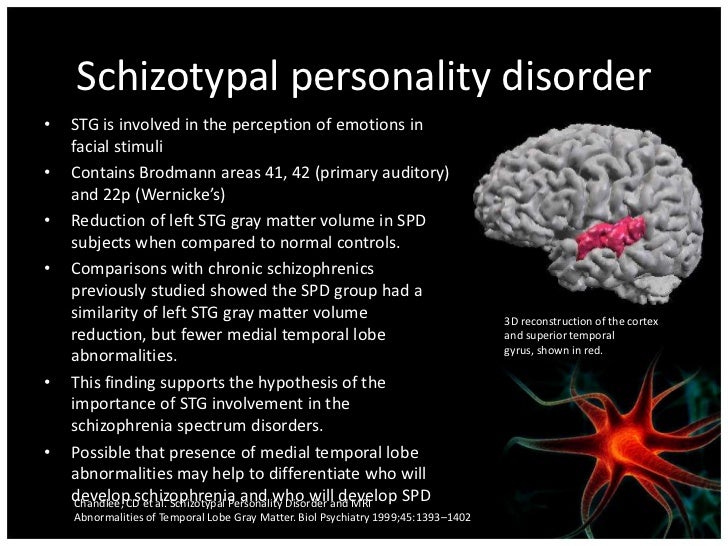
Schizotypal personality disorder and schizophrenia
Although a different disorder, schizoid personality disorder can have some similar symptoms to schizotypal personality disorder and schizophrenia, such as a severely limited ability to make social connections and a lack of emotional expression. People with these disorders may be viewed as odd or eccentric.
Even though the names may sound similar, unlike schizotypal personality disorder and schizophrenia, people with schizoid personality disorder:
- Are in touch with reality, so they're unlikely to experience paranoia or hallucinations
- Make sense when they speak (although the tone may not be lively), so they don't have conversational patterns that are strange and hard to follow
When to see a doctor
People with schizoid personality disorder usually only seek treatment for a related problem, such as depression.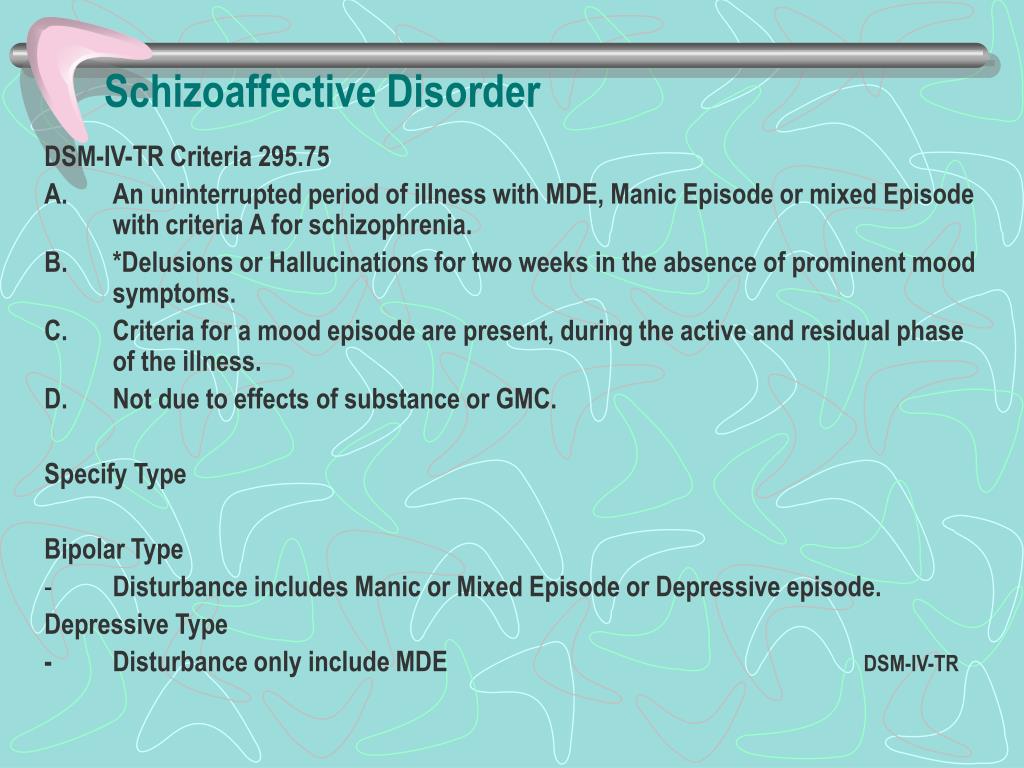
If someone close to you has urged you to seek help for symptoms common to schizoid personality disorder, make an appointment with a health care or mental health professional.
If you suspect a loved one may have schizoid personality disorder, gently suggest that the person seek medical attention. It might help to offer to go along to the first appointment.
Request an Appointment at Mayo Clinic
Causes
Personality is the combination of thoughts, emotions and behaviors that makes you unique. It's the way you view, understand and relate to the outside world, as well as how you see yourself. Personality forms during childhood, shaped through an interaction of inherited tendencies and environmental factors.
In normal development, children learn over time to accurately interpret social cues and respond appropriately. What causes the development of schizoid personality disorder is unknown, although a combination of genetic and environmental factors, particularly in early childhood, may play a role in developing the disorder.
Risk factors
Factors that increase your risk of developing schizoid personality disorder include:
- Having a parent or other relative who has schizoid personality disorder, schizotypal personality disorder or schizophrenia
- Having a parent who was cold, neglectful or unresponsive to emotional needs
Complications
People with schizoid personality disorder are at an increased risk of:
- Developing schizotypal personality disorder, schizophrenia or another delusional disorder
- Other personality disorders
- Major depression
- Anxiety disorders
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
Schizoaffective Disorder | NAMI: National Alliance on Mental Illness
- Overview
- Treatment
- Support
- Discuss
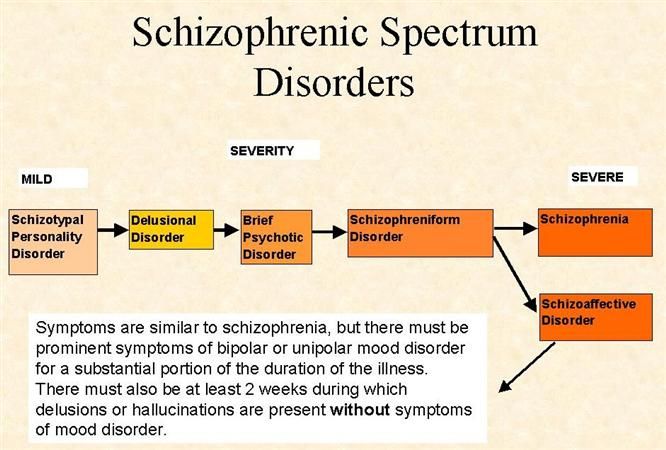
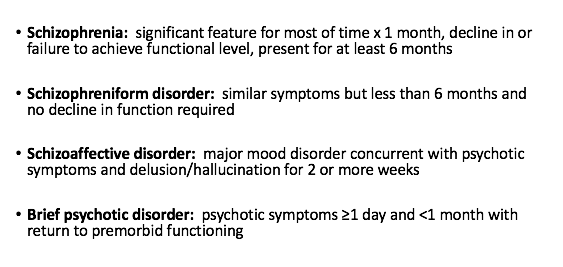
Schizoaffective disorder is a chronic mental health condition characterized primarily by symptoms of schizophrenia, such as hallucinations or delusions, and symptoms of a mood disorder, such as mania and depression.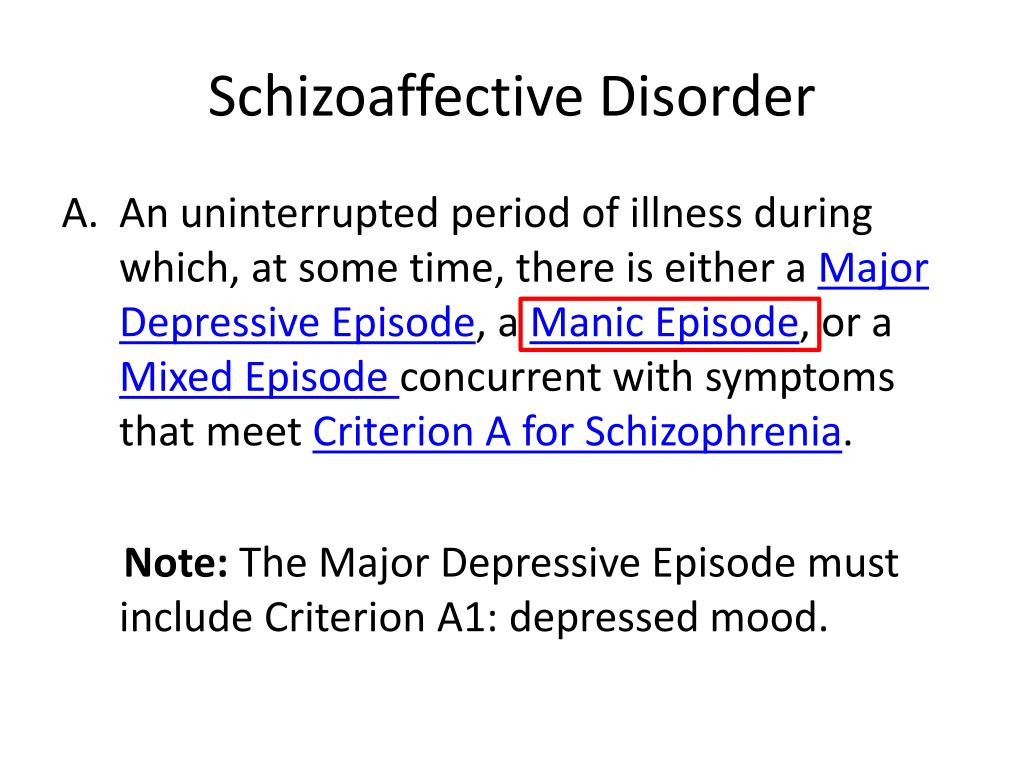
Many people with schizoaffective disorder are often incorrectly diagnosed at first with bipolar disorder or schizophrenia. Because schizoaffective disorder is less well-studied than the other two conditions, many interventions are borrowed from their treatment approaches.
Schizoaffective is relatively rare, with a lifetime prevalence of only 0.3%. Men and women experience schizoaffective disorder at the same rate, but men often develop the illness at an earlier age. Schizoaffective disorder can be managed effectively with medication and therapy. Co-occurring substance use disorders are a serious risk and require integrated treatment.
Symptoms
The symptoms of schizoaffective disorder can be severe and need to be monitored closely. Depending on the type of mood disorder diagnosed, depression or bipolar disorder, people will experience different symptoms:
- Hallucinations, which are seeing or hearing things that aren’t there.
- Delusions, which are false, fixed beliefs that are held regardless of contradictory evidence.
- Disorganized thinking. A person may switch very quickly from one topic to another or provide answers that are completely unrelated.
- Depressed mood. If a person has been diagnosed with schizoaffective disorder depressive type they will experience feelings of sadness, emptiness, feelings of worthlessness or other symptoms of depression.
- Manic behavior. If a person has been diagnosed with schizoaffective disorder: bipolar type they will experience feelings of euphoria, racing thoughts, increased risky behavior and other symptoms of mania.
Causes
The exact cause of schizoaffective disorder is unknown. A combination of causes may contribute to the development of schizoaffective disorder.
- Genetics. Schizoaffective disorder tends to run in families. This does not mean that if a relative has an illness, you will absolutely get it. But it does mean that there is a greater chance of you developing the illness.
- Brain chemistry and structure.
 Brain function and structure may be different in ways that science is only beginning to understand. Brain scans are helping to advance research in this area.
Brain function and structure may be different in ways that science is only beginning to understand. Brain scans are helping to advance research in this area. - Stress. Stressful events such as a death in the family, end of a marriage or loss of a job can trigger symptoms or an onset of the illness.
- Drug use. Psychoactive drugs such as LSD have been linked to the development of schizoaffective disorder.
Diagnosis
Schizoaffective disorder can be difficult to diagnose because it has symptoms of both schizophrenia and either depression or bipolar disorder. There are two major types of schizoaffective disorder: bipolar type and depressive type. To be diagnosed with schizoaffective disorder a person must have the following symptoms.
- A period during which there is a major mood disorder, either depression or mania, that occurs at the same time that symptoms of schizophrenia are present.
- Delusions or hallucinations for two or more weeks in the absence of a major mood episode.
- Symptoms that meet criteria for a major mood episode are present for the majority of the total duration of the illness.
- The abuse of drugs or a medication are not responsible for the symptoms.
Treatment
Schizoaffective disorder is treated and managed in several ways:
- Medications, including mood stabilizers, antipsychotic medications and antidepressants
- Psychotherapy, such as cognitive behavioral therapy or family-focused therapy
- Self-management strategies and education
Related Conditions
A person with schizoaffective disorder may have additional mental health conditions:
- Anxiety disorders
- Posttraumatic stress disorder (PTSD)
- Attention-deficit hyperactivity disorder (ADHD)
- Substance use disorders / Dual Diagnosis
Schizoaffective disorder - symptoms, causes, treatment
Schizoaffective disorder accounts for less than one percent of the disease statistics among the population, but still deserves special attention. It was already at the end of the 20th - beginning of the 21st centuries that this disease was distinguished into a separate type. Most often, schizoaffective disorder begins to manifest itself at the age of 16-30 years, in most cases in women.
It was already at the end of the 20th - beginning of the 21st centuries that this disease was distinguished into a separate type. Most often, schizoaffective disorder begins to manifest itself at the age of 16-30 years, in most cases in women.
Disease definition - schizoaffective disorder
Schizoaffective disorder is a mental illness characterized by episodic disorders with prominent manic and schizophrenic symptoms. In the International Classification of Diseases of the 10th revision (ICD-10), schizoaffective disorder is coded F25 in the group: schizophrenia, schizotypal states and delusional disorders (F20-F29).
The disease is otherwise called recurrent schizophrenia, intermittent schizophrenia, circular schizophrenia or schizoaffective psychosis. In any case, it is serious and requires the supervision of an experienced specialist. It manifests itself both as regular attacks with different duration (from several days to several years), and episodically, with long periods of remission.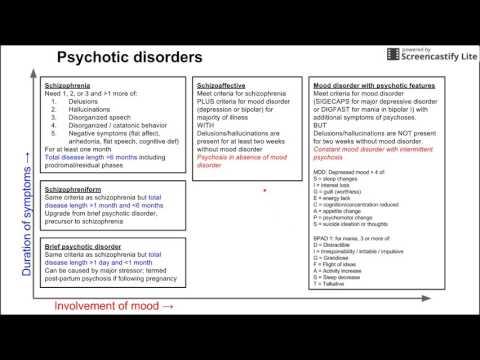 As statistics show, a third of patients suffered an attack of schizoaffective disorder only once in their entire lives. nine0003
As statistics show, a third of patients suffered an attack of schizoaffective disorder only once in their entire lives. nine0003
Schizoaffective personality disorder is a disease in which attacks appear periodically, differing in each individual case in duration and symptoms of manifestation.
Symptoms
Symptoms of schizoaffective personality disorder are manifested individually and with their own characteristics. In general, this is the presence in the patient's life of hallucinations, scattered thinking, mood swings, depressive states, obsessions and fantasies. nine0003
Since schizoaffective disorder is a borderline condition between schizophrenia, manic disorder and depression, the symptoms are distinguished by three signs.
Signs of schizoaffective disorder:
- Manic - exceeded: vital activity, talkativeness, sexual attention. The patient has accelerated speech, lack of sleep, impulsivity and aggressiveness.
- Depressive - changes in appetite and body weight (often with a big minus), lack of desire to do anything (the patient most often sleeps or wants to rest as soon as possible), haunting feelings of guilt and hopelessness, suicidal thoughts.
 nine0024
nine0024 - Mixed - hallucinations, delusions, atypical behavior, speech impairment and lethargy, lack of emotion and slowness of movement.
During periods of the peak of the disease, the patient does not see the difference between reality and fantasies, cannot distinguish them on his own.
Causes of disease
The causes of schizoaffective disorder have not been fully identified.
Depending on the individual manifestation and the specific case, general cases of the onset of schizoaffective disorder are distinguished: nine0003
- Genetic - a gene for the risk of schizophrenic diseases has been isolated. Every person has this gene, but it either does not appear until certain events, or does not make itself felt until the end of life.
- Prenatal - a pattern was revealed that most often patients born in early spring and late autumn suffer from schizoaffective disorder.
- Social - various stressful events can wake up the "sleeping" gene: life on the verge of begging, conditions of war and constant fear for one's life, loneliness.
 This also includes an asocial lifestyle and all kinds of addictions, especially alcohol and drugs. nine0024
This also includes an asocial lifestyle and all kinds of addictions, especially alcohol and drugs. nine0024
The pathogenesis of schizoaffective disorder is also not fully understood. The complexity of this disease lies in the fact that it is impossible to isolate specific changes in the body that indicate this disease. Each patient undergoes a thorough examination before such a diagnosis is made.
Not so long ago, scientists tried to find out the biochemical feature of diseases of the F25 group, but they still failed to give a clear answer, what exactly is missing in the body or is in excess. nine0003
Only correct observation of the patient gives the psychiatrist accurate grounds for talking about schizoaffective psychosis in the patient.
Stages and classification of the disease
Schizoaffective disorder goes through 2 stages. Each of them is characterized by its own characteristics, which make it possible to understand how to help a patient with a given manifestation of the disease.
Stages of schizoaffective psychosis:
- Stage 1 - the initial period. The patient has vegetosomatic disorders, affective fluctuations, sleep and dream disorders, episodic self-perception disorders. It can last from several weeks to several months. nine0024
- Stage 2 - active period. Accompanied by acute psychotic attacks.
Seizures also develop in stages and come in different types. The most frequent - the expanded type (an attack of oneiroid catatonia) - is characterized by stupor and arousal, in which the patient performs incomprehensible actions. Further, this state passes into an illusory-fantastic state.
The development of an attack may stop with the appearance of delirium. Such attacks are called affective-delusional. If the attack is limited to persecutory delusions with depression, then this is a depressive-paranoid attack. nine0003
You also need to remember that each case is individual. Patients may have both mixed types of seizures and dual states.
- Stage 3 - residual period. May not leave any residual disturbances and personality changes, however, there is a decrease in activity, concern for one's psychological health.
The classification of schizoaffective disorder is divided into types:
- Manic type (F 25.0) - a disorder in which schizophrenic and manic symptoms are pronounced. The most complex type of disease, has unfavorable prognosis in treatment. Often the behavior of the patient is a danger to him and others. nine0024
- Depressive type (F25.1) - a disorder in which both schizophrenic and depressive symptoms are pronounced. Accompanied by symptoms of moderate or severe depression.
- Mixed type (F25.2) - also called cyclic schizophrenia or mixed schizophrenic, and affective psychosis - symptoms of bipolar affective disorder are expressed.
An accurate diagnosis can only be made by an experienced psychiatrist in a specialized clinic.
Complications of the disease
The consequences of schizoaffective disorder can significantly worsen the patient's condition and reduce the quality of life.
- With the onset of remission, patients feel a sense of detachment from the world and life, a sense of shame.
- Serious manic problems such as excessive sexual behavior may appear.
- Drug addiction, drug addiction. Since the drugs are strong enough, the patient may experience euphoria, followed by apathy. nine0024
- One of the most serious complications of schizoaffective psychosis is suicidal behavior.
To avoid such complications, the patient's relatives need to contact a specialized clinic for help as soon as possible. It is important to learn how to respond correctly to the behavior of the patient, to know exactly when the attack begins and how to provide first aid.
Schizoaffective disorder is not a sentence, it is treated quite successfully, and relatives and friends are one of the important factors helping patients to return to normal faster. nine0003
Seeing a psychiatrist is the first step towards recognizing that there is a problem and that it needs to be treated. Unfortunately, in our society, psychiatric clinics and specialists are still perceived as a punitive method, and not a method of help.
The main thing is to understand that schizoaffective disorder has different manifestations and each patient has his own symptoms, and often the opposite: from fantasy illusions to silent inhibition. Therefore, if your loved one began to behave strangely - talking to fictional characters, getting lost in reality, saying things that do not correspond to reality, became aggressive, shows excessive sexual interest, try to convince him or go to the doctors yourself. Particular attention should be paid to such behavior if negative events have occurred in the life of the alleged patient. nine0003
nine0003
The most important thing is not to try to treat yourself and remember that schizoaffective disorder does not go away on its own. The patient needs specialized individual treatment under the supervision of a professional doctor.
Diagnosis
Diagnosis of schizoaffective disorder is carried out by a psychiatrist by monitoring the patient's condition. To make such a diagnosis, the doctor must state that the alleged patient has psychotic symptoms within 2 weeks, as well as the presence of an attack. nine0003
Criteria for the diagnosis of schizoaffective disorder:
- There are signs of affective disorders.
- At least 1 of the following is present:
- auditory hallucinations in the form of extraneous voices commenting or leading dialogues;
- delusions of control and influence;
- a feeling of telepathy, that is, the reception or transmission of thoughts at a distance, their openness or withdrawal;
- broken speech and neologisms; nine0024
- persistent delusions that are not characteristic of the patient's subculture;
- frequent and transient appearance of catatonic symptoms;
- Symptoms of schizophrenia and affective disorders are presented simultaneously with one exacerbation.
- The patient is not taking drugs or steroids at the time the condition is diagnosed.
- The patient does not have a seizure disorder.
Diagnosis - schizoaffective disorder, can only be a doctor of a specialized clinic. nine0003
Treatment
Treatment for schizoaffective disorder depends on the manifestation and symptoms of the illness.
In manic and depressive states, especially during attacks, schizoaffective psychosis requires inpatient treatment with the use of medications - antipsychotic drugs (atypical and traditional), antidepressants (monoamine oxidase inhibitors, tetracyclic and tricyclic), neuroleptics, anxiolytics and mood stabilizers. Electroconvulsive therapy (electric shock) may also be used. nine0003
In conjunction with drug treatment, psychotherapy is used, which enhances the effectiveness of drugs.
During the rehabilitation period, work is carried out not only with the patient, but also with relatives and relatives of the patient. Such activities help them interact with each other during remission.
Such activities help them interact with each other during remission.
Clinical guidelines for schizoaffective disorder include recommendations on daily routine, physical activity, mental stress, and taking special medications. Compliance with all prescriptions and constant monitoring by a psychiatrist makes it possible for a stable remission to occur, when the patient can return to normal habitual life and his professional activities. nine0003
+7 (495) 121-48-31
References:
- McWilliams N., reflections on schizoid dynamics
- T.A. Solokhina, prof. V.S. Yastrebov, L.S. Shevchenko - A model of organizing socio-psychological care for patients with schizophrenia.
- World Health Organization. International Classification of Diseases (10th Revision): Classification of Mental and Behavioral Disorders: Clinical Description and Diagnostic Guidelines. nine0024
- Weiner M., "Practical Psychotherapy"
- Roger McKinnon, Robert Michaels and Peter Buckley "Psychiatric interview in clinical practice" - effective treatment and keeping records and journals
- Kuzmenok G.
 F. Collection “Ways of Understanding. Collection of articles for the 15th anniversary of the Society for Psychoanalytic Psychotherapy” - about the combination of therapy and pharmacology.
F. Collection “Ways of Understanding. Collection of articles for the 15th anniversary of the Society for Psychoanalytic Psychotherapy” - about the combination of therapy and pharmacology. - Tiganov A.S. Guide to Psychiatry - M. Medicine
- Bukhanovsky A.O., Kutyavin Yu.A., Litvak M.E. General psychopathology
- A.V. Snezhnevsky - Clinical psychiatry.
FGBNU NTSPZ. ‹‹Endogenous mental illness››
Feedback form
Question about the work of the siteQuestion to a specialistQuestion to the administration of the clinic
email address
Name
Message text
nine0172 Schizoaffective psychosis — is a non-progredient endogenous mental illness with a relatively favorable prognosis, recurrent seizures, in the picture and dynamics of which circular affective disorders (depressive, manic, mixed) of an endogenous nature coexist or sequentially develop 2 and psychotic symptoms (delusional, hallucinatory) characteristic of schizophrenia that are not derived from affect.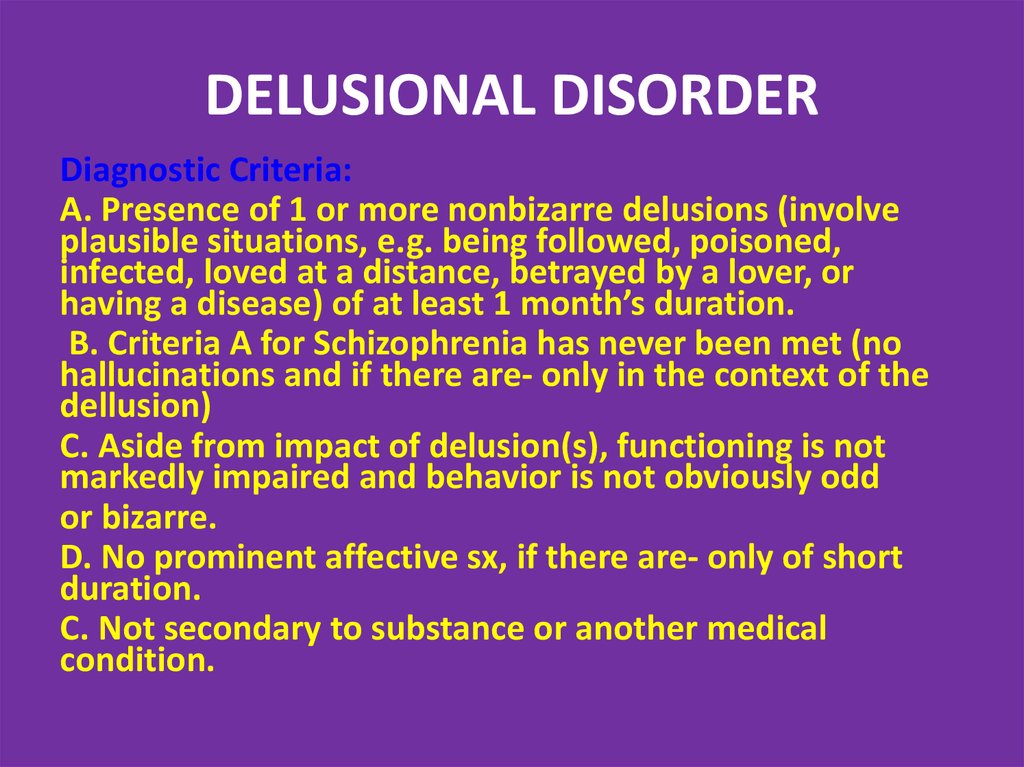 nine0212
nine0212
At the present level of psychiatric knowledge, the content of any definition of schizoaffective psychosis as an independent endogenous psychosis is conditional and debatable. To date, there are no generally accepted definitions that characterize the clinical essence of this disease. The reference to the fact that schizoaffective psychoses combine the signs of two diseases - schizophrenia and affective psychoses, is defined. regardless of external circumstances and psychotic experiences; in schizoaffective psychosis, the differentiation of circular and delusional affect is of great diagnostic importance, which allows only their assignment to the group of endogenous psychoses, but not their position in the systematics of endogenous mental illness. nine0003
The criteria on which the allocation of schizoaffective psychosis is based are most fully formulated in the ICD-10. According to the latter, schizoaffective psychosis is considered not as a "disease", but as "episodic (paroxysmal) disorders" (i.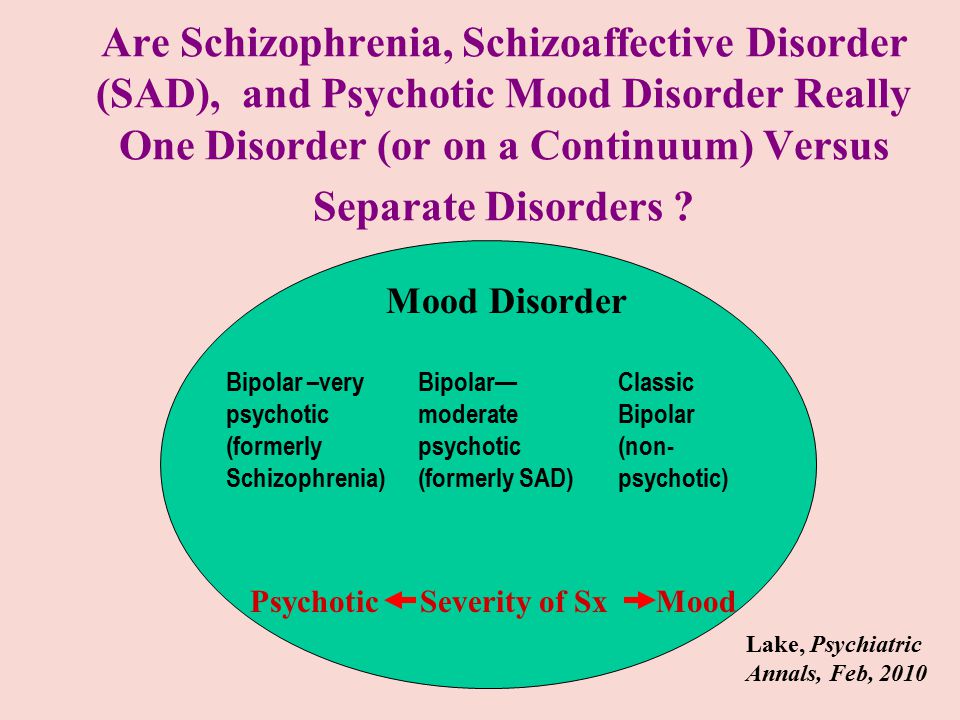 e., conditions) in which both affective and schizophrenic symptoms are present, listed in the diagnostic guidelines for F20 (schizophrenia), observed simultaneously or consecutively over several days, during the same attack, when the picture of the attack meets neither the criteria for schizophrenia nor the criteria for a manic-depressive episode. nine0003
e., conditions) in which both affective and schizophrenic symptoms are present, listed in the diagnostic guidelines for F20 (schizophrenia), observed simultaneously or consecutively over several days, during the same attack, when the picture of the attack meets neither the criteria for schizophrenia nor the criteria for a manic-depressive episode. nine0003
In one of the authoritative studies of the last decade, conducted by A. Marneros (1989), the concept of schizoaffective psychosis is also equated with the concept of schizoaffective disorders and is defined as a psychopathological syndrome, in the constellation of symptoms of which both schizophrenic and melancholic or manic signs are simultaneously or sequentially observed.
In DSM-IV, for the diagnosis of schizoaffective disorder, additional clarifying parameters have been introduced, allowing to attribute to schizoaffective psychosis only those manifestations in which: a) during a long period of the disease, distinct affective disorders (depressive, manic, mixed) and psychopathological symptoms, mandatory for the diagnosis of schizophrenia; b) delusions or hallucinations typical of schizophrenia in its pure form (i.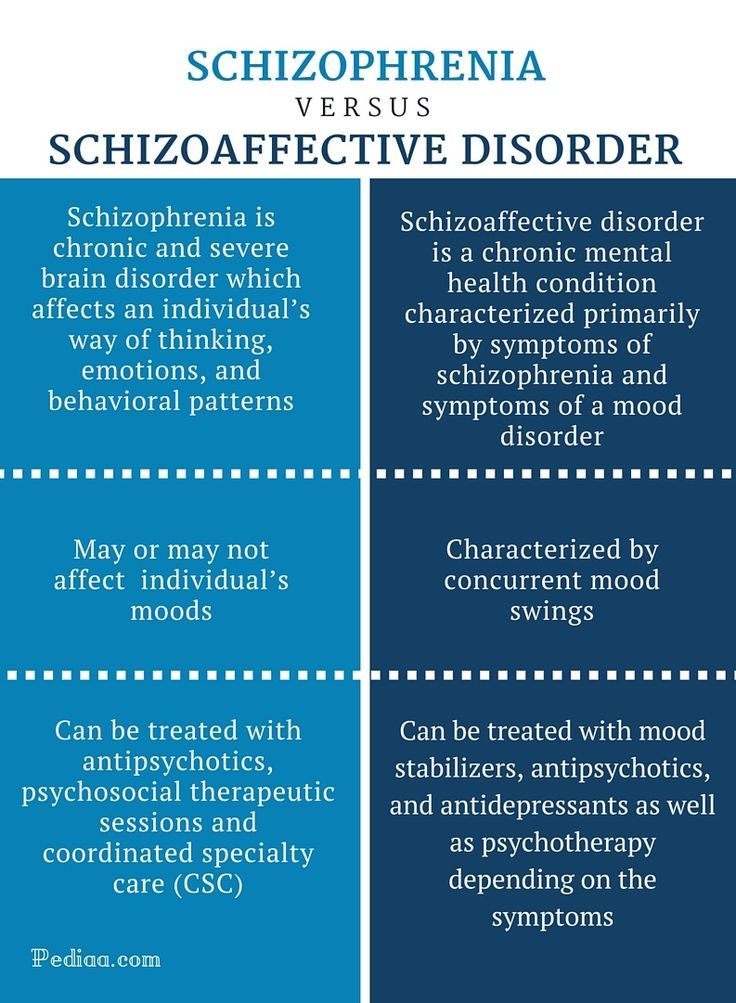 e., without the presence of pronounced affective disorders), lasting at least 2 weeks, should determine the patient's condition; c) the symptoms of affective disorders should take a significant period of time in the total duration of schizoaffective psychosis, in its active and residual stages; d) these psychopathological phenomena should not be the result of exposure to any toxic substances and drugs or somatoorganic diseases. nine0003
e., without the presence of pronounced affective disorders), lasting at least 2 weeks, should determine the patient's condition; c) the symptoms of affective disorders should take a significant period of time in the total duration of schizoaffective psychosis, in its active and residual stages; d) these psychopathological phenomena should not be the result of exposure to any toxic substances and drugs or somatoorganic diseases. nine0003
Despite such a relative specification of the criteria for diagnosing schizoaffective psychoses, their nosological allocation in the educational guidelines of many countries remains uncertain, and diagnostics are traditionally carried out within the framework of either affective or schizophrenic diseases. Nevertheless, today it is obvious that among endogenous psychoses there is a group of diseases, psychopathological manifestations, the course and outcomes of which differ in clinical originality and do not allow diagnosing them within the framework of the traditional dichotomous division of endogenous psychoses by E.