Reasons for high sex drive
Why Is My Sex Drive So High Lately? 20 Causes, Changes Over Time, More
Yes, that says FUN not “concerning.”
“It’s completely normal for your libido to fluctuate and for there to be points of time — days, weeks, months, years — where your sex drive is higher than usual,” says Dr. Jill McDevitt, resident sexologist at CalExotics.
Usually, a higher sex drive is absolutely nothing to be worried about.
As Dr. Jess O’Reilly, PhD, host of the @SexWithDrJess Podcast says, “Desiring sex more often does not suddenly make you a pervert.”
It makes you human.
There is no metric for measuring libido, says Searah Deysach, longtime sex educator and owner of Early to Bed. So there’s really no universal baseline for what counts as a normal, she says.
Now, can you have your own personal “normal”? Yes, says Deysach.
“But even that’s a range, because there are so many actors that can cause your personal libido norm to shift a little — or a lot — to the left or right. ”
These include:
- age
- relationship status or interactions
- sleep, diet, and exercise
- schedule
- mood and mental health
- hormones, medication, and physical health
You can’t — not really.
Do you feel friskier than you did this time last year? Have you been craving sex more than your personal normal? Is your sex drive higher than your partner’s? Then you might say your libido is high.
But there’s no diagnostic test or doctor-approved online quiz you can take to find out if your libido is high.
Feeling sexually insatiable? There are a few common culprits for the climb.
Your stress levels are lower
This is a big one. “If you’re going through a time of low-stress, your libido will likely increase,” says McDevitt.
She says that’s why “vacation sex” is such a Thing.
Your mental health is better than ever
According to clinical sex counselor Eric M. Garrison, author of “Mastering Multiple Position Sex,” being raised in a sexually-repressive household or religion can train folks to “turn off” — or at the very least disconnect from — their libido.
For these folks, going to a sex therapist or mental health professional to work through this shame can result in reconnecting with their sexual urges.
He says this can make folks feel like their sex drive is higher.
You’re having good sex
Thanks to your hormones, the more you have (good) sex, the more your body craves it.
So if you recently started sleeping with someone (or a new sex toy!) that rocks your world, it’s natural to want sex more often, says Dr. McDevitt.
You’ve been exercising more
“Some people find that they want sex more often when they exercise regularly,” says Dr. O’Reilly.
This could be credited to a number of things:
- boosted confidence
- reduced stress
- improved sleep
You swapped or stopped certain meds
Certain medications like antidepressants, SSRIs, birth control, and beta-blockers (to name a few) are known to squash libido.
Finally adjusting to these medications can also result in a higher libido, says Garrison.
And so can going off these medications. Friendly reminder: *don’t* go off any medication without talking to your healthcare provider first!
You’re at your “horny” spot in your menstrual cycle
Most menstruating humans have a “horny” part of their cycle — usually right before, during, or right after ovulation.
So if you or your partner is ravenous a few days a month, it’s the hormones talking!
“Your high libido is a problem if either you think it’s a problem, or if your high libido is leading you to act in a way that interferes with the rest of your life,” says Garrison.
If, for instance, you’re skipping work, cheating on your partner, blowing your savings on sex gadgets to meet your sexual impulses, or otherwise engaging in ~risky behavior~ as a result of your libido, that’s a problem.
In these instances, working with a mental healthcare professional is a M-U-S-T. They’ll help you come up with a game plan to regain control.
A few things!
Turn inward
Dr. McDevitt recommends doing some self-reflection: Is your libido actually interfering with your life? Are you actually bothered by this libido spike?
McDevitt recommends doing some self-reflection: Is your libido actually interfering with your life? Are you actually bothered by this libido spike?
Or is your partner or sex-negative upbringing making you feel gross, bad, or guilty about these urges?
Practice mindfulness
“If your high desire for sex is related to the fact that you find sex stress-relieving, finding other ways to relieve this stress such as breathing, visualization, and non-sexual touch exercises might help,” says Dr. O’Reilly.
Don’t pressure your partner… but talk to them
If your libido has increased and your partner’s hasn’t, it’s possible that either A) your partner feels guilty that they aren’t as interested in having sex or B) you’re feeling resentful that your partner doesn’t want to smash.
That’s why Garrison recommends talking to your partner about it. You might say:
- “I’ve been really in the mood to connect with you sexually recently. Would you be open to letting me massage your back and seeing where it goes?”
- “Recently, I’ve been so horny for you.
 Would you be open to scheduling a date night sometime soon?”
Would you be open to scheduling a date night sometime soon?” - “I know that I’ve been suggesting we have sex more than usual, lately. I’d love to talk about ways we connect physically and intimately that make us both feel good.”
Your sex drive isn’t strictly tied to a timeline. But there are some natural health and hormonal shifts that typically occur within each decade that can affect your libido.
Adolescence
“Generally speaking, the late teens is when most people’s libidos are the highest,” says Dr. McDevitt. Largely, due to hormones.
But (!), Garrison says, “That doesn’t mean that’s when people are having their most fulfilling, pleasurable sex lives.”
For cisgender women in particular, adolescence can be one of the least sexually gratifying times due to things like shame and lack of information.
20s
Hormonally speaking, this is a time when most folks want to get after it.
But Dr. O’Reilly says due to body image, communication, and relationship issues, for folks not in long-term, loving relationships, this decade may not be one of super-satisfying (or orgasmic!) romps.
30s
Stress is a libido killer. And for many, due to kids, work, household responsibilities, and aging parents, their 30s are a high-stress time.
Oh, and speaking of kids… the 30s are the prime decade for baby-making.
For those who get pregnant, the hormonal fluctuations during and after pregnancy can result in less interest in sex for the time being, says Dr. O’Reilly.
40s
For folks of all genders and sexualities, testosterone levels dip this decade, which can lead to less frisky business.
For vulva-owners this is due to perimenopause, and for penis-havers this is due to the natural aging process.
But, rest assured, Dr. O’Reilly says things that often accompany this decade can lead to a higher interest in sex and more fulfilling sex.
For example:
- kids leaving the house
- improved feelings about oneself and one’s body
- increased comfort with a partner
- reduced financial stress
50s
The average age penis-having folks go on Viagra is 53, which suggests many struggle to maintain an erection this decade.
And the average age vulva-owners hit menopause is 51, which can lead to less interest in sex and vaginal dryness.
But Dr. O’Reilly says things like vaginal moisturizers, lube, more creative understandings of sex (oral! anal! humping! kissing!) can make this an incredibly pleasurable and orgasm-rich decade.
60s and beyond
Sure, your libido may be a less high than it was 40 years ago.
But there’s no rule that says your sex life is worse in your 60s than it was in your 20s, says Dr. McDevitt.
“Some people get divorced in their 60s and get swept off their feet by an exciting new love and find that their sex drive rockets,” she says.
Others discover new ways of having sex with their long-term partner that are even more pleasurable.
A sex drive spike can be a great excuse to get down with yourself or your hunny and have some fun (read: orgasms)!
Can a high libido get to a point where it’s interfering with your life? Yes.
But so long as you’re not ditching work or other responsibilities to get off, go ahead and enjoy it — no matter your age.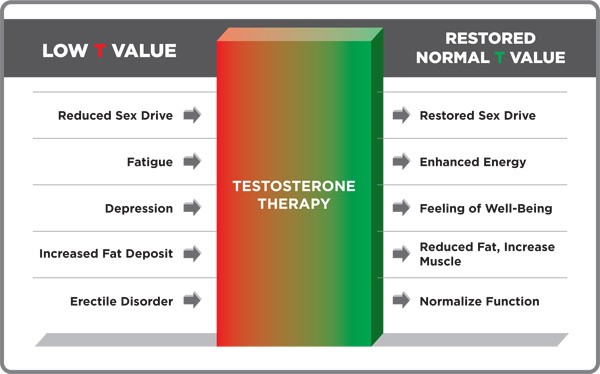
Gabrielle Kassel is a New York–based sex and wellness writer and CrossFit Level 1 Trainer. She’s become a morning person, tested over 200 vibrators, and eaten, drunk, and brushed with charcoal — all in the name of journalism. In her free time, she can be found reading self-help books and romance novels, bench-pressing, or pole dancing. Follow her on Instagram.
What It Means, Characteristics, Causes, and More
High Libido: What It Means, Characteristics, Causes, and MoreMedically reviewed by Janet Brito, Ph.D., LCSW, CST — By Scott Frothingham on February 28, 2020
Libido refers to sexual desire, or the emotion and mental energy related to sex. Another term for it is “sex drive.”
Your libido is influenced by:
- biological factors, such as testosterone and estrogen levels
- psychological factors, such as stress levels
- social factors, such as intimate relationships
High libido is difficult to define since the baseline for “normal” libido depends on the person. It’s different for everybody.
It’s different for everybody.
One person’s “normal” may be a desire for sex once a day, while someone else’s “normal” is having zero sex drive.
According to the Mayo Clinic, a high libido potentially becomes a problem when it results in sexual activity that feels out of control, such as sexual compulsion.
This is also known as hypersexuality or out of control sexual behavior (OCSB).
Signs of sexual compulsion often include:
- Your sexual behavior is having a negative impact on other areas of your life, such as your health, relationships, work, etc.
- You’ve repeatedly tried to limit or stop your sexual behavior but can’t.
- You’re secretive about your sexual behavior.
- You feel dependent on your sexual behavior.
- You don’t feel fulfilled when you substitute other activities for your sexual behavior.
- You use sexual behavior to escape from problems, such as anger, stress, depression, loneliness, or anxiety.
- You have difficulty establishing and maintaining stable, healthy relationships due to your sexual behavior.
The causes of compulsive sexual behavior haven’t been clearly established yet.
Potential causes include:
- Neurotransmitter imbalance. Compulsive sexual behavior may be related to high levels of chemicals in your brain known as neurotransmitters (think dopamine, serotonin, and norepinephrine) that help regulate your mood.
- Medication. Some dopamine agonist medications used to treat Parkinson’s disease may cause compulsive sexual behavior.
- Health conditions. Parts of the brain that affect sexual behavior may be damaged by conditions such as epilepsy and dementia.
If you feel that you’ve lost control of your sexual behavior, help is available.
Sexual behavior is deeply personal, making it difficult for some people to seek help if they’re having any sexual issues.
But remember:
- You’re not alone. There are many people also dealing with sexual problems.
- The right treatment can help improve the quality of your life.

- Your doctor will keep your information confidential.
Your libido isn’t quantifiable on a one-size-fits-all scale.
Everybody has their own standard libido. If your sex drive drops from that standard, you’re experiencing low libido. If your sex drive increases from that standard, you’re experiencing high libido.
If your sex drive starts interfering with your quality of life, speak to a doctor or other healthcare provider.
You can also speak to a mental health therapist who specializes in human sexuality. The American Association of Sexuality Educators, Counselors and Therapists (AASECT) has a nationwide directory of certified sex therapists.
Last medically reviewed on February 28, 2020
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Derbyshire K, et al. (2015). Compulsive sexual behavior: A review of the literature. DOI:
1556/2006.4.2015.003 - Mayo Clinic Staff. (2017). Compulsive sexual behavior.
mayoclinic.org/diseases-conditions/compulsive-sexual-behavior/symptoms-causes/syc-20360434 - Sexual dysfunction & disorders. (2015).
my.clevelandclinic.org/health/diseases/9121-sexual-dysfunction - Yes, you can have better sex in midlife and in the years beyond. (2017).
health.harvard.edu/womens-health/yes-you-can-have-better-sex-in-midlife-and-in-the-years-beyond
Share this article
Medically reviewed by Janet Brito, Ph.D., LCSW, CST — By Scott Frothingham on February 28, 2020
Read this next
Is It Actually Possible to Have Too Much Sex?
Medically reviewed by Janet Brito, Ph.D., LCSW, CST
Let’s start by putting your head to rest: You’re probably not having too much sex.
 Still, your frequency can interfere with you living a full, healthy…
Still, your frequency can interfere with you living a full, healthy…READ MORE
How Does Sex Affect Your Emotions? 12 Things to Know About Attraction and Arousal
Medically reviewed by Janet Brito, Ph.D., LCSW, CST
Sex can be the ultimate expression of romantic love. Or an emotional roller coaster. Or purely physical. It can be all of this and more. It means…
READ MORE
Managing Antidepressant Sexual Side Effects
Medically reviewed by Alan Carter, Pharm.D.
Sexual side effects, like erectile dysfunction, are common complaints of taking antidepressants. Most prescription antidepressants are part of a drug…
READ MORE
What Is Demisexuality?
Medically reviewed by Emelia Arquilla, DO
Demisexuality is a sexual orientation where people only experience sexual attraction to folks that they have close emotional connections with.

READ MORE
Sex Can Benefit Your Mental Health — Here’s How
Science has your back: The mental health benefits of a healthy sex life are abundant, whether you're getting it on solo or having fun with multiple…
READ MORE
2022 Nurx Review: Is It Right for You?
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
Nurx is a telemedicine company that offers birth control, emergency contraceptives, PrEP, and STI home test kits.
READ MORE
Let’s Talk Month: Planned Parenthood on Consent and Boundaries
Planned Parenthood shares the importance of consent and boundaries and how to talk about it with youth at any age.
READ MORE
How does the libido work?
The term libido is commonly used to describe sexual desire or desire for sexual activity.
 Modern medicine recognizes the importance of libido as one of the key indicators of overall health and quality of life. In the article we understand how the libido works, why it is for a person and why sometimes the libido changes.
Modern medicine recognizes the importance of libido as one of the key indicators of overall health and quality of life. In the article we understand how the libido works, why it is for a person and why sometimes the libido changes. Content
- Evolution and libido
- Which hormones regulate libido in women
- What governs male libido
- Neurotransmitters: libido in the head
- Why libido increases
- Why libido can decrease
- Note
Evolution and Libido
Although libido is influenced by many factors today, from psychological to cultural, its nature is evolutionary in origin.
Sex drive is a common trait in the reproduction of mammals and birds. The sexual activity of many species varies depending on the sexual cycle, that is, from periodically repeating changes in the body of females from one ovulation to another.
The fact is that the probability of conception is not uniform, but varies depending on the phase of the cycle. Man, for example, belongs to polyestrous animals, that is, species in which sexual cycles are repeated throughout the year. And although a person can conceive offspring on any day, the probability of fertilization is higher precisely on the days of ovulation. Libido these days is also, as a rule, increased.
Man, for example, belongs to polyestrous animals, that is, species in which sexual cycles are repeated throughout the year. And although a person can conceive offspring on any day, the probability of fertilization is higher precisely on the days of ovulation. Libido these days is also, as a rule, increased.
Fluctuating libido is a mechanism that allows you to increase the frequency of sexual intercourse on the most favorable days for conception. Libido is an important force of natural selection, which encourages us to reproduce with maximum efficiency and pass our genetic material to the next generations, that is, to win the evolutionary lottery.
What hormones regulate libido in women
The main hormones that regulate sexual desire are sex hormones: estrogen, progesterone and testosterone. All three hormones are present in both male and female bodies. However, women have significantly less testosterone than men. Conversely, estrogen and progesterone are mostly female sex hormones.
In the first (follicular) phase of the menstrual cycle, several follicles grow and mature in the ovaries at once, the level of estrogen in the blood also increases. About a week before ovulation, a single dominant follicle is determined and continues to grow. The remaining follicles stop in their development and undergo the opposite - atresia. At the same time, the concentration of estrogen in the blood grows further, due to the production of the hormone by the dominant follicle. In the middle of the cycle, the follicle bursts, ovulation occurs - the release of the egg into the uterus through the fallopian tubes. After ovulation, estrogen levels gradually decrease.
Experiments have shown that both men and women rate photographs of women's faces taken before ovulation as more attractive than photographs of the same women after ovulation.
Women's libido is also strongest around ovulation, when estrogen is at its peak.
In addition, estrogen plays an important role in women's health, energizes and enhances attractiveness.
After ovulation comes the second (luteal) phase of the menstrual cycle. In place of the bursting follicle, a corpus luteum is formed, which releases progesterone. If fertilization does not occur, then by the end of the menstrual cycle, the corpus luteum disintegrates, and progesterone levels fall.
Low estrogen levels and high progesterone levels at the end of the cycle lead to a decrease in libido. With the onset of menstruation, sexual desire increases again.
However, due to the fact that both progesterone and estrogen levels simultaneously decrease approximately one week before the end of the cycle, PMS symptoms may occur: swelling, bloating, lethargy, mood swings.
In women who take hormonal contraceptives, hormone fluctuations are less pronounced, so changes in libido are not so noticeable.
Some women who take oral contraceptives may not notice any change in sex drive, while others report decreased libido as an unwanted side effect.

What governs male libido
The main male sex hormone is testosterone. Its fluctuations can affect the level of sexual desire. Thus, a decrease in testosterone is associated with low libido.
But if in women hormonal fluctuations are extended for a long period (about a month), then in men changes occur more often: testosterone levels are usually elevated in the morning, and decrease in the evening. Therefore, sexual desire is also often higher in the morning and lower late in the evening. In addition to daily fluctuations, testosterone levels also change throughout life, reaching a maximum in adolescence with a gradual decrease after 30 years.
Testosterone is not the only fuel that fuels the male libido. Estradiol, the predominant form of estrogen, also affects sex drive.
In addition to testosterone, estradiol levels also affect libido. This is partly due to the fact that estradiol affects the areas of the brain that control sexual behavior, and partly due to the role of the hormone in the regulation of testosterone levels.
Sex hormones, their receptors and the aromatase enzyme are in a complex balance that regulates sexual behavior, erection, libido, as well as mood and mental state.
Neurotransmitters: libido in the head
The exact role of neurotransmitters, active brain chemicals, in sexual desire is not fully understood. But it can be noted that one of the “controlling” libido is a neurotransmitter and the hormone oxytocin. Oxytocin is called the hormone of love and affection because it is responsible for the positive emotions that a person experiences during the period of falling in love and at the peak of sexual desire. Oxytocin rises with arousal and orgasm.
Oxytocin is the hormone of love and affection. In women, nipple stimulation can cause a surge of oxytocin followed by arousal. In experiments on male rats, oxytocin has been shown to cause erection and ejaculation, and also increase sperm count.
One study showed that treating a patient with oxytocin nasal spray had a positive effect on libido, erection and orgasm. A little later, the successful experiment was repeated on 29 heterosexual couples. Participants reported that the introduction of the "love hormone" increased the intensity of orgasm and the satisfaction of partners after intercourse. In addition, participants were able to better share sexual desires and empathize with partners.
A little later, the successful experiment was repeated on 29 heterosexual couples. Participants reported that the introduction of the "love hormone" increased the intensity of orgasm and the satisfaction of partners after intercourse. In addition, participants were able to better share sexual desires and empathize with partners.
The effects were more pronounced in men. Men also noted higher levels of sexual satiety. However, the effect of treatment varied from small to moderate.
Another neurotransmitter that can influence libido is dopamine. Dopamine plays an important role in emotional behavior, attention, memory, reward and pleasure. Dopamine can affect testosterone levels, and testosterone can affect dopamine.
The neurotransmitter dopamine also affects libido. Sex hormones create conditions for increasing the synthesis of dopamine, and its release leads to an increase in sexual desire, by activating the right areas of the brain.
In men, one of the key areas of the brain responsible for sexual behavior is the medial preoptic area. Injections of substances that mimic the effects of dopamine into such an area in rats lead to an increase in sexual activity.
Injections of substances that mimic the effects of dopamine into such an area in rats lead to an increase in sexual activity.
An increase in libido can also occur after administration of the dopamine precursor, L-DOPA. Conversely, the introduction of molecules that block the work of dopamine leads to a decrease in libido.
Why libido increases
Hypersexuality due to various causes is diagnosed in approximately 2% of the population. An excessively high libido can be caused by:
- High levels of mood-regulating neurotransmitters such as dopamine and serotonin.
- A side effect of certain drugs (including those that affect dopamine levels).
- Damage to areas of the brain involved in sexual behavior (particularly in epilepsy).
Persistent sexual arousal that causes discomfort is a sign of hypersexual disorder.
There is a noticeable difference between high and too high libido. The cause for concern is the increase in sexual desire to a level that is out of control and interferes with daily life.
Why libido can decrease
A decrease in sexual desire is more common than an increase in it. Clinical criteria for diagnosing low libido have not been established, as there is a wide range of what is considered "low": normal sexual desire for one person may seem high or low for another. However, the following symptoms are commonly mentioned:
- Loss of desire for a partner.
- Disinterest in masturbation.
- Few or no sexual fantasies.
- Anxiety about lack of interest in sex.
Persistent reluctance to have sex may be a sign of hypoactive sexual desire disorder - anaphrodisia.
Hormonal disorders are a common cause of anaphrodisia. Libido may decrease in response to changes in estrogen, progesterone, and testosterone levels. Testosterone is the prime suspect.
In the absence of testosterone in men, libido is low, while treatment of testosterone deficiency leads to normalization of libido.
Women may also experience decreased sexual desire due to low testosterone, but decreased estrogen is more likely to be the cause. This is what happens during menopause. In a 2008 study, 27% of premenopausal women and 52% of menopausal women experienced low sex drive.
In addition to hormonal fluctuations, anaphrodisia can be caused by:
- Stress,
- Diabetes,
- High blood pressure,
- Certain medications, especially antidepressants,
- Alcohol abuse,
- Smoking,
- Underuse of drugs
In most cases, restoring libido can be achieved by making healthier lifestyle changes and reducing stress levels. Sometimes drug therapy is required to normalize hormonal balance.
Note
- Libido has an evolutionary origin. It helps mammals, including humans, maximize the chance of having offspring.
- The female libido is mainly dependent on progesterone and estrogen. In the first phase of the cycle before ovulation, there is a lot of estrogen, and little progesterone - libido is increased.
 In the second phase, estrogen becomes less and progesterone increases, so libido decreases.
In the second phase, estrogen becomes less and progesterone increases, so libido decreases. - Taking oral contraceptives may affect a woman's libido.
- Male libido is primarily controlled by testosterone. The highest level of the hormone is in adolescence, and after 30 years it gradually decreases. Following testosterone, libido may also decrease.
- In addition to hormones, sexual desire is influenced by neurotransmitters: dopamine and oxytocin.
- Increased or decreased libido are relative concepts. There are no single indicators for determining the "normality" of a libido: what is a "normal" sexual desire for one person may seem high or low for another.
- Decreased libido - anaphrodisia - may be associated with stress, hormonal imbalance, bad habits, taking certain medications.
- Increased libido may be a symptom of a hypersexual disorder or may occur after certain drugs, brain injury or damage, or neurotransmitter imbalance.
- If the change in libido causes discomfort, you should consult a doctor.

Quality of life, high libido, good mood are in many cases indicators of good health. The Atlas Genetic Test helps you take care of yourself, understand your predisposition to multifactorial diseases, and improve your health with personalized test results.
Atlas Blog Articles about attraction:
A conversation with an expert. How to enjoy sex?
Sleep, diet and giving up your smartphone: what habits will make you happier?
- Roslan et al. The Bio-Psycho-Social Dimension in Women's Sexual Desire: 'Argumentum ad novitatem'. 2019
- Motta-Mena, Puts. Endocrinology of human female sexuality, mating, and reproductive behavior. 2016
- Roberts et al. Female facial attractiveness increases during the fertile phase of the menstrual cycle. 2004
- Rastrelli et al.Testosterone and sexual function in men.2018
- Oti et al. Systemic effects of oxytocin on male sexual activity via the spinal ejaculation generator in rats.
 2021
2021 - MacDonald, Feifel. Dramatic improvement in sexual function induced by intranasal oxytocin. 2012
- Shoemaker. Male Libido, Testosterone, & Neurotransmitters. 2019
- Grazzotin. Libido: the biological scenario. 2000
- Montjero et al. Sexual side effects of antidepressant and antipsychotic drugs. 2015
- Shulster et al. The role of estradiol in male reproductive function. 2016
- Tuijl et. al. Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior? 2020
- West et. al. Prevalence of low sexual desire and hypoactive sexual desire disorder in a nationally representative sample of US women.2008
- Behnia et. al. Differential effects of intranasal oxytocin on sexual experiences and partner interactions in couples. 2014
- Dominguez, Hull. Dopamine, the medial preoptic area, and male sexual behavior.2005
Endocrine causes of sexual problems and infertility
Sexual relations are an innate need and an important function of the human body, like the functions of breathing, digestion and others..jpg) Success in these relationships is often a sign of overall social success. Therefore, the importance of sexual well-being and reproductive health cannot be overstated.
Success in these relationships is often a sign of overall social success. Therefore, the importance of sexual well-being and reproductive health cannot be overstated.
Traditionally society and even doctors themselves associate sexual disorders more often with men than with women. This is probably due to the fact that men pay more attention to this problem, and it is easier to identify these changes in men. In women, in most cases, sexual function is not assessed at all.
"Sexual and reproductive dysfunction" refers to long-term sexual problems:
- decreased libido;
- unstable potency;
- premature ejaculation;
- mild orgasm;
- menstrual disorders;
- infertility.
Sexual problems are much more common with age, but, unfortunately, young people are no exception. Violations can occur against the background of stress, psychological problems, alcohol intake, anabolic drugs, medications, or against the background of various diseases. With sexual problems, patients first of all turn to gynecologists or urologists, less often to andrologists. Often, on the basis of a minimal examination, a therapy is prescribed that has either a short-term effect or is not effective at all.
With sexual problems, patients first of all turn to gynecologists or urologists, less often to andrologists. Often, on the basis of a minimal examination, a therapy is prescribed that has either a short-term effect or is not effective at all.
The impact of endocrine diseases on sexual and reproductive health
Unfortunately, almost all endocrine diseases lead to sexual or reproductive dysfunction. At the very beginning, it is difficult to suspect endocrine disorders, since they can proceed under the guise of increased fatigue, depressed mood, reduced sexual desire, all of which is explained by chronic lack of sleep, stress, or workload. As the disease progresses, complaints become more pronounced, changes begin to appear in other organs and systems. Subsequently, an endocrine disease can cause infertility.
In men the hormone testosterone is responsible for sex drive. Produced in the testicles under the influence of luteinizing hormone (LH) - a hormone of the pituitary gland, the main gland of the brain. Decreased LH levels inevitably lead to a reduction in the production of testosterone by the testicles. The low level of testosterone in men is the cause of a decrease in sexual desire (libido), erectile dysfunction (impotence), a decrease in the quantity and quality of spermatozoa. These conditions include elevated prolactin levels, elevated cortisol levels, excess or deficiency of thyroid hormones (hyperthyroidism and hypothyroidism). And with an increase in blood glucose levels (diabetes mellitus), the cause of sexual dysfunction is not only a decrease in the amount of testosterone, but damage to small vessels and nerve endings.
Decreased LH levels inevitably lead to a reduction in the production of testosterone by the testicles. The low level of testosterone in men is the cause of a decrease in sexual desire (libido), erectile dysfunction (impotence), a decrease in the quantity and quality of spermatozoa. These conditions include elevated prolactin levels, elevated cortisol levels, excess or deficiency of thyroid hormones (hyperthyroidism and hypothyroidism). And with an increase in blood glucose levels (diabetes mellitus), the cause of sexual dysfunction is not only a decrease in the amount of testosterone, but damage to small vessels and nerve endings.
In women both female sex hormones (estrogen) and male sex hormones (testosterone) are responsible for sexual desire. In most cases, the peak of sexual desire in women occurs at ovulation, it is during this period that both estrogen and testosterone increase to the maximum. The production of testosterone and estrogen in a woman's body is affected by the level of the following hormones: prolactin, thyroid hormones, cortisol, male sex hormones (androgens). Therefore, diseases or conditions that are accompanied by a violation of the production of these hormones can be the cause of sexual dysfunction.
Therefore, diseases or conditions that are accompanied by a violation of the production of these hormones can be the cause of sexual dysfunction.
Now consider diseases and conditions that can result in sexual or reproductive problems.
Elevated prolactin levels (hyperprolactinemia)
The most common cause of an increase is a benign tumor - a pituitary adenoma that produces an excessive amount of prolactin (prolactinoma). Elevated levels of TSH (the hormone responsible for the production of thyroid hormones) can also cause hyperprolactinemia.
The most common complaints are decreased performance and headache.
In men, 6-20% develop gynecomastia - enlargement of the mammary glands or seals appear, sometimes painful to the touch. Sometimes there are discharges from the mammary glands. A feature of prolactinomas in men is that the disease is diagnosed at a fairly late stage, when the formation is already large. This is primarily due to the fact that in the early years of men, sexual dysfunction is associated with stress and many other reasons.
In women , the disease is diagnosed at an early stage, since even a slight increase in prolactin affects the menstrual cycle, which immediately attracts attention.
Low levels of thyroid hormones (hypothyroidism)
The most common cause of hypothyroidism is autoimmune thyroiditis, a disease in which the body's own immune cells "attack" the thyroid gland, mistaking it for a foreign organ. Under the influence of immune cells, a sluggish chronic inflammation develops in the thyroid gland, which is not associated with either viruses or bacteria. Subsequently, most patients develop reduced production of thyroid hormones against the background of inflammation.
In men even a slight decrease in the level of thyroid hormones can cause sexual dysfunction in the form of a decrease in libido, with a significant lack of hormones, infertility develops.
In women, hypothyroidism leads to menstrual irregularities and infertility. But the most important thing is the lack of thyroid hormones in a woman, even minor deviations, can lead to a missed pregnancy in the early stages.
But the most important thing is the lack of thyroid hormones in a woman, even minor deviations, can lead to a missed pregnancy in the early stages.
In addition, weakness, decreased performance, a feeling of chilliness, weight gain, swelling, memory impairment may be disturbing.
Increased amount of thyroid hormones (hyperthyroidism, thyrotoxicosis)
The most common cause of hyperthyroidism is excessive production of hormones by the thyroid gland itself due to a malfunction in the immune system.
In men with mild thyrotoxicosis, sexual dysfunction is quite rare. With the progression of thyrotoxicosis, complaints of erectile dysfunction appear due to a decrease in the amount of free (active) testosterone, due to the appearance of a large amount of inactive testosterone (total testosterone).
In women with thyrotoxicosis, as a rule, sexual dysfunction is observed quite rarely.
Increased stress hormone - cortisol (produced in the adrenal glands)
The cause of a slight increase in cortisol levels may be the appearance of a difficult or threatening situation - stress. Either formations in the pituitary gland (Cushing's disease) or formations in the adrenal glands (Cushing's syndrome) lead to a pronounced increase in the hormone.
Either formations in the pituitary gland (Cushing's disease) or formations in the adrenal glands (Cushing's syndrome) lead to a pronounced increase in the hormone.
Symptoms of elevated cortisol levels can be - the appearance of obesity mainly in the abdomen and face (becomes round), thinning of the upper and lower extremities, blush on the cheeks, the appearance of stretch marks on the skin of purple or purple-cyanotic color, increased blood pressure, depressed mood, up to the development of depression. With a long course of the disease during physical exertion, muscle weakness may appear.
In men excess cortisol leads to a decrease in libido, erectile dysfunction due to a decrease in testosterone levels; in men, the appearance of obesity leads to an excessive conversion of the male sex hormone (testosterone) into female sex hormones (estrogen).
In women excess cortisol leads to an increased content of male sex hormones (androgens). With an increased level of androgens, ovulation is disrupted, which can lead to impaired sexual and reproductive functions and even infertility.
Increased blood glucose levels (diabetes mellitus)
There are several types of diabetes mellitus, between which there is one fundamental difference - is there enough insulin in the body or not? Insulin is needed by the body for the absorption of glucose (the source of nutrition for cells). In type 1 diabetes, there is an absolute insufficiency of insulin, that is, without its additional administration, the patient simply dies. In type 2 diabetes, in most patients at the very beginning of the disease, on the contrary, an excess amount of insulin is observed, but the cells at the same time have low sensitivity to it (insulin resistance) and the so-called "relative deficiency" of insulin develops, when glucose is not absorbed by the cells. Over time, excess production of insulin leads to the depletion of reserves in the pancreas, it becomes necessary to administer it.
Men with diabetes may experience erectile dysfunction, retrograde ejaculation, infertility. The cause of sexual dysfunction is primarily damage to small vessels or nerve endings, observed with a prolonged increase in blood glucose levels. In addition, in obese men, there is a decrease in testosterone levels due to its excessive conversion in fat cells into estrogens (female sex hormones).
The cause of sexual dysfunction is primarily damage to small vessels or nerve endings, observed with a prolonged increase in blood glucose levels. In addition, in obese men, there is a decrease in testosterone levels due to its excessive conversion in fat cells into estrogens (female sex hormones).
In women with diabetes, sexual dysfunction develops due to damage to capillaries and nerve fibers, which leads to the development of atrophic changes, dryness in the genital tract. You may experience discomfort or pain during sexual intercourse.
An increase in the level of androgens - male sex hormones (hyperandrogenemia) in women
Two main diseases lead to an excess of androgens in women - polycystic ovary syndrome and congenital dysfunction of the adrenal cortex. More common is polycystic ovary syndrome, in which a woman's ovaries produce an excess amount of male sex hormones. The syndrome can be manifested by skin rashes (acne), excessive hair growth on the face and body, obesity, menstrual irregularities, and infertility. Subsequently, many women develop diabetes mellitus (due to reduced cell sensitivity to insulin), and the risk of developing endometrial cancer increases. Congenital dysfunction of the adrenal cortex is characterized by moderate hair growth, acne, menstrual irregularities, infertility, but the disease does not lead to the development of low cell sensitivity to insulin and diabetes mellitus.
Subsequently, many women develop diabetes mellitus (due to reduced cell sensitivity to insulin), and the risk of developing endometrial cancer increases. Congenital dysfunction of the adrenal cortex is characterized by moderate hair growth, acne, menstrual irregularities, infertility, but the disease does not lead to the development of low cell sensitivity to insulin and diabetes mellitus.
An excessive increase in the level of male sex hormones in women leads to a decrease in sexual desire, menstrual irregularities, and the development of infertility due to the lack of ovulation.
Exercise and anabolic steroids
Active exercise is associated with a healthy lifestyle. However, the desire for large muscle mass often leads to a "not ideal state" in sexual life. On the one hand, the body perceives prolonged exhausting physical activity as stress, producing an excess amount of cortisol. And cortisol affects the production of testosterone, which in the end can negatively affect sexual desire.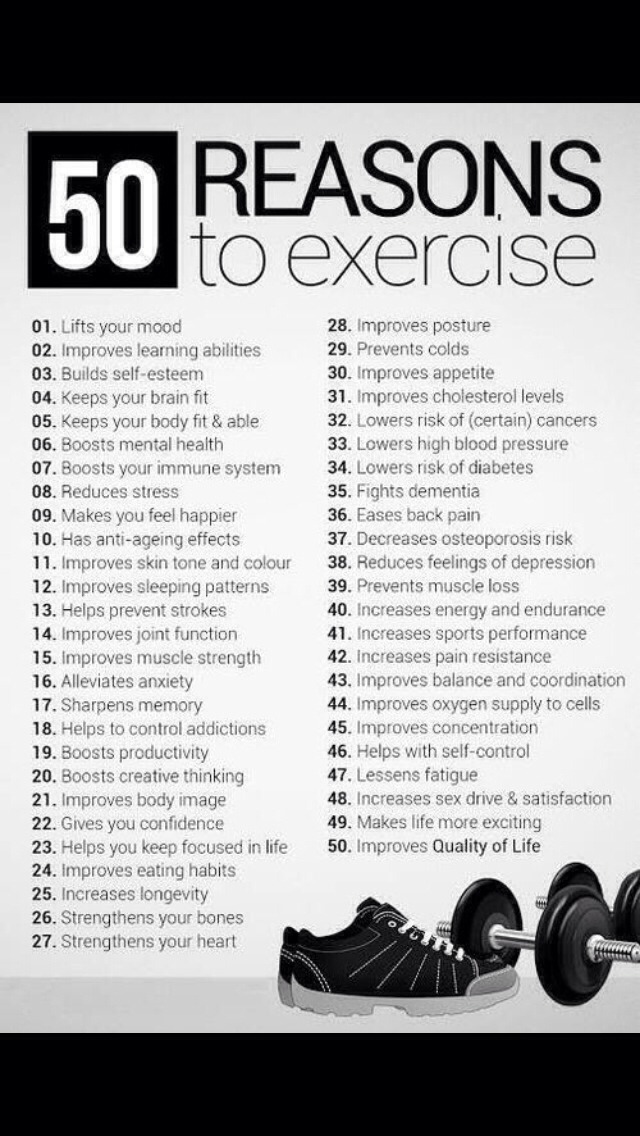 On the other hand, anabolic steroid drugs are often taken to accelerate muscle growth. Prolonged uncontrolled intake of such drugs leads to suppression of the production of one's own testosterone, which is fraught with the development of not only sexual dysfunction, but also infertility.
On the other hand, anabolic steroid drugs are often taken to accelerate muscle growth. Prolonged uncontrolled intake of such drugs leads to suppression of the production of one's own testosterone, which is fraught with the development of not only sexual dysfunction, but also infertility.
Summing up, I would like to emphasize that any form of sexual dysfunction can be a manifestation of endocrine diseases, and not just individual “coldness” or “fatigue”. If something bothers you in this delicate area, you should contact an endocrinologist, find the cause and improve the quality of your life. Particularly encouraging is the fact that if an endocrine disease is diagnosed in time and adequate treatment is received, then a complete restoration of sexual and reproductive functions is possible.
How to identify and eliminate endocrine disorders?
In cases where the main cause of problems in sexual life is endocrine diseases, timely and adequate therapy prescribed by an endocrinologist allows you to quickly and fully restore lost functions, avoid unnecessary complications and prevent possible recurrence of sexual disorders.