Psychological test samples
Frequently Performed Psychological Tests - Clinical Methods
Definition
A psychologic test is a set of stimuli administered to an individual or a group under standard conditions to obtain a sample of behavior for assessment. There are basically two kinds of tests, objective and projective. The objective test requires the respondent to make a particular response to a structured set of instructions (e.g., true/false, yes/no, or the correct answer). The projective test is given in an ambiguous context in order to afford the respondent an opportunity to impose his or her own interpretation in answering.
Technique
Psychologic tests are rarely given in isolation but as a part of a battery. This is because any one test cannot sufficiently answer the complex questions usually asked in the clinical situation. Most diagnostic questions require the assessment of personality, intelligence, and perhaps even the presence of organic involvement. A typical battery of tests includes projective tests to assess personality such as the Rorschach and the Thematic Apperception Test (TAT), an objective personality test such as the Minnesota Multiphasic Personality Inventory (MMPI), a semistructured test like the Rotter Incomplete Sentence Test, and an intelligence test, usually the Wechsler Adult Intelligence Scale Revised (WAIS-R).
The most important consideration for the physician is when to ask for psychologic assessment. As with medical diagnostic procedures, we are interested in finding answers to diagnostic questions that cannot be obtained through direct observation or interview. In our clinical experience, there are a myriad of circumstances requiring psychologic consultation either to assist in or rule out medical intervention. Some of the more typical situations include compliance, behavioral management, affirmation of clinical findings, the use of supportive drug therapies, and continuity of care issues.
Five case examples are offered to illustrate the above situations.
Mr. S. was a 35-year-old single salesman hospitalized for gastrointestinal problems associated with a previous operation. He had a history of noncompliance with both drugs and nutrition regimens. Severe debilitation would ensue following outpatient treatments, after which he would be hospitalized. This pattern repeated itself several times.
Psychologic assessment data were consistent with a pattern of addictive behavior and poor coping mechanisms under stressful conditions. Recommendations included a drug rehabilitation program and stress management techniques.
Dr. L., a 68-year-old retired dentist, had severe behavioral management problems with the nursing staff. He was verbally punitive and intrusive of other patients" privacy. Psychologic assessment revealed an organic brain syndrome indicating greater individual care and a lower expectation of his performance.
A 21-year-old single male, Mr. N., was admitted for hospitalization complaining of severe stomach pains and rectal bleeding. Psychologic testing was administered because the internist could find no evidence of physical pathology. Test battery results described a young man under an inordinate amount of stress due to a huge difference between his intellectual capabilities and the demands of his work place.
The recommendation was to find other employment and to work with a counselor to develop more realistic vocational goals.
Ms. C. was a middle-aged housewife complaining of panic attacks of unknown origin. She also said that she was in severe depression because of the death of her daughter 2 years previously. The clinical question was whether she should be given antidepressants or antianxiety agents as an adjunct to psychotherapeutic intervention. Test results were consistent with a state of anxiety as opposed to an affective disorder.
Ms. B. was a 23-year-old single female who was hospitalized following a drug overdose from a suicide attempt. Information was needed to determine how dangerous she was to herself, how restrictive an environment she needed for treatment, and what type of therapy was appropriate. Test results confirmed a compulsive personality with a dramatic flair. Ms. B. needed extensive individual psychotherapy but did not require lengthy hospitalization.
Nevertheless, it was essential to link her with outpatient care while she was still motivated to receive care.
Although the above examples are by no means exhaustive, they do point out the variety of commonly occurring circumstances in which psychologic assessment may be useful. It is important when ordering testing to formulate the diagnostic question in as specific a manner as possible. Such requests as "describe personality dynamics" or "rule out psychologic disturbance" are too general to answer in an effective and efficient manner. Do not hesitate to ask exactly what you want to know. The psychologist will inform you if he or she is unable to answer. Use the examples described above to formulate your question: Is this patient depressed? Is this patient psychotic? Why is this patient not conforming to the treatment regimen?
When presenting a patient to a psychologist for evaluation, it is helpful to have demographic data and a detailed history of the client. Also, the description presented of the problems should be in behavioral terms. Saying that a patient appears to be depressed is not as helpful as describing him or her as having a loss of appetite, early morning rising, or slowness of speech. If the patient is a management problem, give a concrete description of what this entails: won"t go to rehabilitation therapy, won"t let a technician draw blood.
Also, the description presented of the problems should be in behavioral terms. Saying that a patient appears to be depressed is not as helpful as describing him or her as having a loss of appetite, early morning rising, or slowness of speech. If the patient is a management problem, give a concrete description of what this entails: won"t go to rehabilitation therapy, won"t let a technician draw blood.
Finally, the referring physician may request either a specific test or an abbreviated battery. While some psychologists will go along with this practice, we do not encourage it. Psychologic tests, particularly personality ones, are only as good as the skills of the individual who administers and interprets them. The psychologist must feel confident and competent in the battery that he or she administers. Therefore, the number and choice of tests should be those of the psychologist, just as the medical procedures chosen for a patient are the responsibility of the physician in charge.
Basic Science
The most commonly used personality tests are the Rorschach, TAT, and MMPI. The assumptions underlying projective tests such as the Rorschach and TAT are that the standard set of stimuli are used as a screen to project material that cannot be obtained through a more structured approach. Ambiguous inkblots or pictures reinforce the use of individual expression and reduce resistance. A frequent criticism is the assumption that the individual simply responds to ambiguity with trivia or with what was most recently experienced, such as last night's television fare. The response to this criticism is the notion of psychic determinism. Behavior is a function of choice, not chance. Thus, how a person responds is a reflection of personal motives, fantasies, and needs.
The assumptions underlying projective tests such as the Rorschach and TAT are that the standard set of stimuli are used as a screen to project material that cannot be obtained through a more structured approach. Ambiguous inkblots or pictures reinforce the use of individual expression and reduce resistance. A frequent criticism is the assumption that the individual simply responds to ambiguity with trivia or with what was most recently experienced, such as last night's television fare. The response to this criticism is the notion of psychic determinism. Behavior is a function of choice, not chance. Thus, how a person responds is a reflection of personal motives, fantasies, and needs.
The best-known psychologic assessment tool is the Rorschach, the "inkblot test." It was first published by Hermann Rorschach in 1921 and was introduced to the United States in 1930 by Samuel Beck. The test consists of 10 symmetrical inkblots, half of which are acromatic. It is administered by giving the respondent one card at a time and asking him or her to describe what is seen. The respondent is told that he or she can see one or more things and that there are no right or wrong answers. The tester records the responses verbatim. There is then a second phase of testing called the inquiry. The respondent is again presented with each of the ten cards and asked to note the location of the response and what determines his or her answers.
The respondent is told that he or she can see one or more things and that there are no right or wrong answers. The tester records the responses verbatim. There is then a second phase of testing called the inquiry. The respondent is again presented with each of the ten cards and asked to note the location of the response and what determines his or her answers.
A large body of research takes to task the reliability and validity of projective techniques in general and the Rorschach in particular. The issue of reliability cannot be approached in a conventional sense with projective techniques. The Rorschach inkblots and the TAT pictures do not lend themselves to split-half reliability because the stimuli are not designed to be equivalent with each other. Test–retest reliability is difficult because many of the variables addressed by the test are affected by time. Interjudge reliability indices using Rorschach summary scores have been reported to be favorable, and Exner (1978), using his own scoring system, has reported test–retest reliability correlations ranging from . 50 to .90 on 17 different variables.
50 to .90 on 17 different variables.
Attempts at measuring the validity of the Rorschach also suffer from problems inherent in the nature of the test. The Rorschach is designed to assess highly complex, multidetermined behaviors for which prediction about specific acts is nearly impossible. It also assesses covert needs and fantasy life that may not currently or ever manifest themselves in overt behavior. Concurrent validity is contaminated by the unreliability of psychiatric diagnoses and the fact that individuals with similar diagnoses may indeed behave differently. In response to the criticisms on validity, Korner (1960) has answered that there is no good assessment technique capable of predicting behavior, so why criticize the Rorschach. He goes on to point out that projective techniques are not magic. They describe the personality at work, its adaptations and compromises, and the balance between fantasy and the demands of reality.
The TAT was developed by Henry Murray and Christiana Morgan in 1935. It consists of 30 achromatic picture cards, categorized into those appropriate for boys, girls, men, and women. It is customary to present approximately 10 cards to the respondent, who is then asked to tell a story about what is happening in the picture, what led up to it, and how will it turn out. The respondent is also asked to describe the characters" thoughts and feelings. As with the Rorschach, interjudge reliability is the most applicable test. Correlations have been about .80. The validity of the TAT can be measured when it is defined using specific procedures with a particular population and operationally defined criteria. Studies have examined both construct and concurrent validity. Stories have correlated significantly with behavioral measures of achievement and aggression. A correlation of .74 has been obtained between TAT expressed needs and those needs rated from autobiographies.
It consists of 30 achromatic picture cards, categorized into those appropriate for boys, girls, men, and women. It is customary to present approximately 10 cards to the respondent, who is then asked to tell a story about what is happening in the picture, what led up to it, and how will it turn out. The respondent is also asked to describe the characters" thoughts and feelings. As with the Rorschach, interjudge reliability is the most applicable test. Correlations have been about .80. The validity of the TAT can be measured when it is defined using specific procedures with a particular population and operationally defined criteria. Studies have examined both construct and concurrent validity. Stories have correlated significantly with behavioral measures of achievement and aggression. A correlation of .74 has been obtained between TAT expressed needs and those needs rated from autobiographies.
The most frequently used objective test for personality is the MMPI. It was published by Hathaway and McKinley in 1943 and revised in 1951. It is designed for ages 16 and over and contains 566 items to be answered yes or no. It may be administered to an individual or group, and the answer sheets can be hand- or machined-scored. The respondent is asked to read each question and decide what is true or false as applied to him or her and then to mark that response on the answer sheet. The test has four validity scales and eight clinical scales. The scales were developed empirically by administering an item pool to a large group of normal subjects, and contrasting their responses to those of selected homogeneous criteria groups of psychiatric patients. Those items that discriminate between the groups were used.
It is designed for ages 16 and over and contains 566 items to be answered yes or no. It may be administered to an individual or group, and the answer sheets can be hand- or machined-scored. The respondent is asked to read each question and decide what is true or false as applied to him or her and then to mark that response on the answer sheet. The test has four validity scales and eight clinical scales. The scales were developed empirically by administering an item pool to a large group of normal subjects, and contrasting their responses to those of selected homogeneous criteria groups of psychiatric patients. Those items that discriminate between the groups were used.
Results of the test are coded onto a profile sheet for interpretation. The mean t-score for each scale is 50 with a standard deviation (SD) of 10. The scale is significantly elevated beyond an SD of 2 or t-score of 70. Even though the MMPI is empirically derived, it shares a similar problem with the projective tests in terms of reliability and validity, that is, it is based on psychiatric diagnoses. How valid and reliable were the diagnoses of the patients in each of the criteria groups? The MMPI thoroughly addresses some other aspects of validity. The lie score (L) assesses social desirability. The F score is an internal consistency check, and the K score assesses test-taking attitude along a frankness–defensive continuum.
How valid and reliable were the diagnoses of the patients in each of the criteria groups? The MMPI thoroughly addresses some other aspects of validity. The lie score (L) assesses social desirability. The F score is an internal consistency check, and the K score assesses test-taking attitude along a frankness–defensive continuum.
An interesting hybrid between the projective and objective assessments is the semistructured incomplete-sentence test. While ostensibly a projective technique in which the respondent reflects his or her own wishes or conflicts to complete a sentence stem, it easily lends itself to objective scoring or screening for experimental use. The Rotter Incomplete Sentence Test is one of the more popular of this form of assessment. It contains 40 sentence stems each of which is to be completed by the respondent. The test takes approximately 20 minutes to complete and may be administered to an individual or to a group. It was originally used as a screening device to determine mental disturbance at an army convalescent hospital. Reliability and validity correlations are quite acceptable. The interjudge reliability is about .90, and split-half reliability is .83. As to validity, correlation coefficients with adjustment and maladjustment classifications for women was .64 and for men .77.
Reliability and validity correlations are quite acceptable. The interjudge reliability is about .90, and split-half reliability is .83. As to validity, correlation coefficients with adjustment and maladjustment classifications for women was .64 and for men .77.
The use of intelligence testing in a clinical setting may be puzzling to the reader. In many ways the intelligence test is the foundation for differential diagnosis to the psychologist. The intelligence test measures major mental abilities that may be affected by the presence of an organic disease or injury, thought disorder, or environmental stress. The patterning of the scores on the intelligence test gives the psychologist clues as to the presence, extent, and relative influence of each of the above factors. The most empirically sound intelligence test is the WAIS-R, which was revised in 1981. The WAIS-R contains 11 tests, 6 verbal and 5 nonverbal. It was standardized on a stratified sample of ages ranging from 16 to 74 years, 11 months. The basic score is the intelligence quotient (IQ), a comparison of the individual with the average score of his or her age group. Each of the 11 tests also has its own scale scores, which are conversions of raw scores dependent also on comparison to reference groups. The sum of scale scores are converted to three IQ scores: verbal, performance, and full-scale IQs. Mean IQ is 100 with an SD of 15; thus, two-thirds of all adults have an IQ between 85 and 115. Reliability coefficients are excellent in the mid-90's range. In terms of validity, there is a .50 correlation with school performance and a .85 correlation with the Stanford–Binet test of intelligence. The WAIS-R takes approximately 90 minutes to administer and requires a competent tester.
The basic score is the intelligence quotient (IQ), a comparison of the individual with the average score of his or her age group. Each of the 11 tests also has its own scale scores, which are conversions of raw scores dependent also on comparison to reference groups. The sum of scale scores are converted to three IQ scores: verbal, performance, and full-scale IQs. Mean IQ is 100 with an SD of 15; thus, two-thirds of all adults have an IQ between 85 and 115. Reliability coefficients are excellent in the mid-90's range. In terms of validity, there is a .50 correlation with school performance and a .85 correlation with the Stanford–Binet test of intelligence. The WAIS-R takes approximately 90 minutes to administer and requires a competent tester.
A physician who wants to rule out an organic brain syndrome may call upon neuropsychologic testing. This is particularly true when a CT scan is negative in the presence of suspicious symptomatology (early Alheizmer's disease), in assessing the relative importance of organic versus psychologic variables in the behavior of trauma victims, and in differentiating between dementia and depression in the elderly. For cases in which an intense work-up for neurologic deficits is required, the patient should be referred to a specialist for neuropsychologic assessment. Since this procedure can be costly and time-consuming, the physician may want to screen first for the presence of a brain dysfunction. Most psychologists are well trained for this task. We will briefly describe two neuropsychologic tests that are useful for screening purposes. We do not necessarily endorse them as the best available, but only those with which we have familiarity.
For cases in which an intense work-up for neurologic deficits is required, the patient should be referred to a specialist for neuropsychologic assessment. Since this procedure can be costly and time-consuming, the physician may want to screen first for the presence of a brain dysfunction. Most psychologists are well trained for this task. We will briefly describe two neuropsychologic tests that are useful for screening purposes. We do not necessarily endorse them as the best available, but only those with which we have familiarity.
The first test is the Aphasia Screening Test adapted by Reitan (1984) from the Halstead/Wepman Aphasia Screening Test. It assesses several areas of dysfunction including dysphonia, dyslexia, spelling and constructional dyspraxia, and dyscalculia. The test uses the sign approach, that is, positive findings have distinct and definite significance, but normal performance cannot rule out organicity. Anyone with a basic grade school education is capable of answering every item correctly. The test is simple to administer and consists of 32 items that do not usually require more than 20 minutes to complete. The second, called the Category Test, is the most powerful in the Halstead/Reitan test battery. It consists of 205 stimuli and is divided into seven subtests. The Category Test assesses central processing, abstraction, and reasoning. The cutoff score is 51 errors. While Reitan recommends the use of a slide presentation with his own design projector and feedback system, DeFillipis and McCampbell (1979) have designed a much simpler method of presentation. Their Booklet Category Test (BCT) is portable, requiring only two loose-leaf notebooks and an answer sheet. They report .91 correlation between the BCT and the Category Test. There are two major criticisms of the Category Test: there is no normative data, and reliability has not been adequately studied. One study did report a test–retest correlation of .93.
The test is simple to administer and consists of 32 items that do not usually require more than 20 minutes to complete. The second, called the Category Test, is the most powerful in the Halstead/Reitan test battery. It consists of 205 stimuli and is divided into seven subtests. The Category Test assesses central processing, abstraction, and reasoning. The cutoff score is 51 errors. While Reitan recommends the use of a slide presentation with his own design projector and feedback system, DeFillipis and McCampbell (1979) have designed a much simpler method of presentation. Their Booklet Category Test (BCT) is portable, requiring only two loose-leaf notebooks and an answer sheet. They report .91 correlation between the BCT and the Category Test. There are two major criticisms of the Category Test: there is no normative data, and reliability has not been adequately studied. One study did report a test–retest correlation of .93.
Clinical Significance
The Rorschach describes personality structure, offering a multidimensional picture of the individual's current functioning and potential. As Korner (1960) states, the Rorschach shows the personality at work. There are several scoring systems for the Rorschach, most being based on four major categories: location, determinants, content, and the use of populars and originals. The location, or area of the response, yields information about the respondent's ability toward perceptual organization, abstraction, and synthesis. Determinants of the response refer to those qualities that produce it, such as form, shape, and color. They are tied to such personality variables as emotionality, impulsivity versus control, and openness versus constrictiveness. The content of the block reveals the personal meanings, attitudes, and interests of the respondent. Originals and populars are related to the respondent's creativity, reality testing, and conventionality, among other variables.
As Korner (1960) states, the Rorschach shows the personality at work. There are several scoring systems for the Rorschach, most being based on four major categories: location, determinants, content, and the use of populars and originals. The location, or area of the response, yields information about the respondent's ability toward perceptual organization, abstraction, and synthesis. Determinants of the response refer to those qualities that produce it, such as form, shape, and color. They are tied to such personality variables as emotionality, impulsivity versus control, and openness versus constrictiveness. The content of the block reveals the personal meanings, attitudes, and interests of the respondent. Originals and populars are related to the respondent's creativity, reality testing, and conventionality, among other variables.
Whereas the Rorschach presents personality structure and organization, the TAT reflects the content of personality, including needs, pressures, conflicts, values, and interest. There are instances in which the content of a given TAT story is so revealing of the patient's difficulties that it would be reported verbatim in the psychologic report. Certain cards are said to "pull" specific types of themes: Card 1, attitudes toward authority; Card 4, attitudes toward heterosexual relationships; and Card 5, relationships with the mother figure. Also, diagnostic groups tend to have a certain orientation toward the stories. Obsessive–compulsives may be pedantic. Depressives may have short stories with monosyllabic words. Schizophrenics may have disjointed or delusional content.
There are instances in which the content of a given TAT story is so revealing of the patient's difficulties that it would be reported verbatim in the psychologic report. Certain cards are said to "pull" specific types of themes: Card 1, attitudes toward authority; Card 4, attitudes toward heterosexual relationships; and Card 5, relationships with the mother figure. Also, diagnostic groups tend to have a certain orientation toward the stories. Obsessive–compulsives may be pedantic. Depressives may have short stories with monosyllabic words. Schizophrenics may have disjointed or delusional content.
There are three approaches to interpretation of the MMPI: single scale, statistical, and clinical. Many physicians who order the MMPI are doing so because they are comfortable with the single scale approach. This involves looking at an elevated scale and making assumptions about the patient. As stated, there are eight clinical scales: HS (hypochondriasis), D (depression), HY (hysteria), PD (psychopathic deviant), PA (paranoia), PT (psychothemia), SC (schizophrenia), and MA (hypomania). Although space does not permit a description of all these scales, elevations of each are associated with a diagnostic grouping related to a cluster of symptoms; for example, elevated HS is associated with an immature person with lack of insight who tends to complain about his or her health. Interpretation of single scales must be taken with great caution. The scales were devised to fit with the Kraepelin System of diagnosis, which is outmoded. For instance, there is no longer a diagnostic grouping of psychopathic deviate. Each of the scales has a much different meaning in relation to more modern classifications.
Although space does not permit a description of all these scales, elevations of each are associated with a diagnostic grouping related to a cluster of symptoms; for example, elevated HS is associated with an immature person with lack of insight who tends to complain about his or her health. Interpretation of single scales must be taken with great caution. The scales were devised to fit with the Kraepelin System of diagnosis, which is outmoded. For instance, there is no longer a diagnostic grouping of psychopathic deviate. Each of the scales has a much different meaning in relation to more modern classifications.
The statistical approach for interpretation involves code types. A code type is a particular correlation of elevated clinical scales (e.g., 2 through 7). A large sample of patients are given the MMPI. They are grouped by similarity in code types. These groupings are then correlated with clinical and demographic data, the notion being that patients with similar MMPI profiles will manifest similar problems. The difficulty with this approach, often called the "cookbook" approach, is that the data do not tend to generalize to other settings.
The difficulty with this approach, often called the "cookbook" approach, is that the data do not tend to generalize to other settings.
The third approach to MMPI interpretation is the clinical approach. The expert clinician depends on his or her knowledge of personality dynamics, case history, and current environmental circumstances to formulate hypotheses as to psychologic difficulties of the respondent. The MMPI computer-generated report uses this type of approach. One has to be extremely cautious in relying too heavily on the report because its author has no firsthand knowledge of the respondent. The clinical psychologist administering the MMPI will use the clinical approach but seldom in isolation without other tests, or at least a clinical interview.
The Rotter Incomplete Sentence Blank is a screening device. We have found it useful as a way of obtaining content information similar to that of the TAT in patients who were too threatened or too depressed to take on the challenge of making up stories. Rotter has given several suggestions for interpretation in addition to a reliable scoring system. The adjusted person tends to produce stems that are more neutral and flippant. The statements tend to be short, concise, and humorous. The maladjusted individual tends to write longer sentences that are complicated and emotionally charged. A frequent theme is that nobody understands them.
Rotter has given several suggestions for interpretation in addition to a reliable scoring system. The adjusted person tends to produce stems that are more neutral and flippant. The statements tend to be short, concise, and humorous. The maladjusted individual tends to write longer sentences that are complicated and emotionally charged. A frequent theme is that nobody understands them.
It is not unusual for physicians to question the use of intelligence testing on their patients. The common assumption is that the test is not relevant to differential diagnosis. Contrary to this assumption, the intelligence test is an essential part of any test battery. First, the general level of intelligence will determine how much the patient is capable of understanding and therefore cooperating in his treatment. In other words, how concrete or simplified need the physician be in his or her instructions? Second, the intelligence test is a broad-based screening for organicity. The Verbal Scale IQ has been related to left hemisphere functioning and Performance Scale to right hemisphere. A significant difference of approximately 15 points between these two IQs requires more intense assessment. A dramatic difference between a given subscale mean and the mean for that scale may also be cause for concern. A third important use of the results of the intelligence test is its relationship to aspects of personality functioning. As an example, current state of anxiety can be related to subscale scores on digit span and picture completion. Loose association on the similarity or comprehension subtest may be associated with a psychotic process.
A significant difference of approximately 15 points between these two IQs requires more intense assessment. A dramatic difference between a given subscale mean and the mean for that scale may also be cause for concern. A third important use of the results of the intelligence test is its relationship to aspects of personality functioning. As an example, current state of anxiety can be related to subscale scores on digit span and picture completion. Loose association on the similarity or comprehension subtest may be associated with a psychotic process.
In the course of ordering psychologic consultation, if there is any question of the presence of brain dysfunction, the physician may want to order screening in the form of the Category Test and Aphasia Screening Test. The Category Test is the most powerful of the Halstead/Reitan battery. It is essentially a processing test assessing abstraction and reasoning. The Category Test measures level of performance and offers no information concerning localization. Further differentiation in terms of severity, location, or specificity requires more intense evaluation. A quick screening for localization would be the Aphasia Screening Test. It assesses both left and right hemisphere functioning with respect to language ability. If the respondent cannot copy correctly, we might suspect a right hemisphere lesion. On the other hand, if he or she cannot name an object, we might think about a left hemisphere lesion. In the use of this test there will be many false negatives but few false positives.
Further differentiation in terms of severity, location, or specificity requires more intense evaluation. A quick screening for localization would be the Aphasia Screening Test. It assesses both left and right hemisphere functioning with respect to language ability. If the respondent cannot copy correctly, we might suspect a right hemisphere lesion. On the other hand, if he or she cannot name an object, we might think about a left hemisphere lesion. In the use of this test there will be many false negatives but few false positives.
The physician usually receives the results of psychologic assessments in the form of a psychologic report. There are a variety of formats, so we will describe a typical one. The report will usually be about 2 to 3 typed pages, long enough to do the raw data justice but not so long as to impinge upon the valuable time of the physician. The first section will be a description of the presentation of the respondent and his or her test-taking behavior. The next section will describe the respondent's intellectual functioning, strengths and weaknesses, and the presence of organic symptoms. The third section is an overview of the respondent's current emotional and social functioning that may include samples of actual test responses as examples. In a final section, the psychologist summarizes the findings and offers recommendations. Interpretation of findings in psychologic test batteries largely depends on the clinical acumen of the psychologist. The organization and synthesis of test data require much skill and knowledge of personality dynamics. Each of the tests has a unique contribution to the overall clinical picture, but none can stand by itself. Thus, the psychologist must determine what is relevant, what is internally consistent, and what is central or irrelevant to diagnosis and intervention.
The third section is an overview of the respondent's current emotional and social functioning that may include samples of actual test responses as examples. In a final section, the psychologist summarizes the findings and offers recommendations. Interpretation of findings in psychologic test batteries largely depends on the clinical acumen of the psychologist. The organization and synthesis of test data require much skill and knowledge of personality dynamics. Each of the tests has a unique contribution to the overall clinical picture, but none can stand by itself. Thus, the psychologist must determine what is relevant, what is internally consistent, and what is central or irrelevant to diagnosis and intervention.
References
DeFilippis NA, McCampbell E. The manual for the Booklet Category Test. Odessa, FL: Psychological Assessment Resources, 1979.
Exner JE. The Rorschach: a comprehensive system. Vol. 2. New York: Wiley, 1978.
*Freeman FS.
 Theory and practice of psychological testing. New York: Holt, Rineholt & Winston, 1962.
Theory and practice of psychological testing. New York: Holt, Rineholt & Winston, 1962.Goldfried MR, Stricker G, Winer LB. Rorschach handbook of clinical and research applications. Englewood Cliffs, NJ: Prentice-Hall, 1971.
Harrison R. Thematic Apperception Test. In: Wolman B, ed. Handbook of clinical psychology. New York: McGraw-Hill, 1965;562–620.
*Hathaway SR, McKinley JC. Minnesota Multiphasic Personality Inventory: users guide for the Minnesota report. University of Minnesota, 1982.
*Jarvis PE, Barth JT. Halstead-Reitan Test Battery: an interpretative guide. Odessa, FL: Psychological Assessment Resources, 1984.
*Korner AF. Theoretical considerations concerning the scope and limitations of projective techniques. In: Murstin BI, ed. Handbook of projective techniques. New York: Basic Books, 1960;23–24.
MacInnes WE, Forch JR, Golden CJ. A cross-validation of a booklet form of the Category Test.
 Clin Neuropsychol. 1981;3:3–5.
Clin Neuropsychol. 1981;3:3–5.Mauger PA. Predicting response to treatment using the MMPI. In: Butcher J, Dahlstrom G, Gynther M, Schofield W, eds. Clinical notes on the MMPI. Nutley, NJ: Hoffman-LaRoche, 1980.
Reitan RM. Aphasia and sensory-perceptual deficits in adults. Tucson: Reitan Neuropsychology Laboratories, 1984.
Rotter JB, Fafferty JE, Schachtitz E. Validating the Rotter Incomplete Sentence Test for college screening. In: Murstein BI, ed. Handbook of projective techniques. New York: Basic Books, 1960;859–72.
*Schneidman ES. Projective techniques. In: Wolman BB, ed. Handbook of clinical psychology. New York: McGraw-Hill, 1965;498–521.
Wechsler D. The WAIS-R manual. New York: Harcourt Brace Jovanovich, 1981.
Frequently Performed Psychological Tests - Clinical Methods
Definition
A psychologic test is a set of stimuli administered to an individual or a group under standard conditions to obtain a sample of behavior for assessment. There are basically two kinds of tests, objective and projective. The objective test requires the respondent to make a particular response to a structured set of instructions (e.g., true/false, yes/no, or the correct answer). The projective test is given in an ambiguous context in order to afford the respondent an opportunity to impose his or her own interpretation in answering.
There are basically two kinds of tests, objective and projective. The objective test requires the respondent to make a particular response to a structured set of instructions (e.g., true/false, yes/no, or the correct answer). The projective test is given in an ambiguous context in order to afford the respondent an opportunity to impose his or her own interpretation in answering.
Technique
Psychologic tests are rarely given in isolation but as a part of a battery. This is because any one test cannot sufficiently answer the complex questions usually asked in the clinical situation. Most diagnostic questions require the assessment of personality, intelligence, and perhaps even the presence of organic involvement. A typical battery of tests includes projective tests to assess personality such as the Rorschach and the Thematic Apperception Test (TAT), an objective personality test such as the Minnesota Multiphasic Personality Inventory (MMPI), a semistructured test like the Rotter Incomplete Sentence Test, and an intelligence test, usually the Wechsler Adult Intelligence Scale Revised (WAIS-R).
The most important consideration for the physician is when to ask for psychologic assessment. As with medical diagnostic procedures, we are interested in finding answers to diagnostic questions that cannot be obtained through direct observation or interview. In our clinical experience, there are a myriad of circumstances requiring psychologic consultation either to assist in or rule out medical intervention. Some of the more typical situations include compliance, behavioral management, affirmation of clinical findings, the use of supportive drug therapies, and continuity of care issues.
Five case examples are offered to illustrate the above situations.
Mr. S. was a 35-year-old single salesman hospitalized for gastrointestinal problems associated with a previous operation. He had a history of noncompliance with both drugs and nutrition regimens. Severe debilitation would ensue following outpatient treatments, after which he would be hospitalized. This pattern repeated itself several times.
Psychologic assessment data were consistent with a pattern of addictive behavior and poor coping mechanisms under stressful conditions. Recommendations included a drug rehabilitation program and stress management techniques.
Dr. L., a 68-year-old retired dentist, had severe behavioral management problems with the nursing staff. He was verbally punitive and intrusive of other patients" privacy. Psychologic assessment revealed an organic brain syndrome indicating greater individual care and a lower expectation of his performance.
A 21-year-old single male, Mr. N., was admitted for hospitalization complaining of severe stomach pains and rectal bleeding. Psychologic testing was administered because the internist could find no evidence of physical pathology. Test battery results described a young man under an inordinate amount of stress due to a huge difference between his intellectual capabilities and the demands of his work place.
The recommendation was to find other employment and to work with a counselor to develop more realistic vocational goals.
Ms. C. was a middle-aged housewife complaining of panic attacks of unknown origin. She also said that she was in severe depression because of the death of her daughter 2 years previously. The clinical question was whether she should be given antidepressants or antianxiety agents as an adjunct to psychotherapeutic intervention. Test results were consistent with a state of anxiety as opposed to an affective disorder.
Ms. B. was a 23-year-old single female who was hospitalized following a drug overdose from a suicide attempt. Information was needed to determine how dangerous she was to herself, how restrictive an environment she needed for treatment, and what type of therapy was appropriate. Test results confirmed a compulsive personality with a dramatic flair. Ms. B. needed extensive individual psychotherapy but did not require lengthy hospitalization.
Nevertheless, it was essential to link her with outpatient care while she was still motivated to receive care.
Although the above examples are by no means exhaustive, they do point out the variety of commonly occurring circumstances in which psychologic assessment may be useful. It is important when ordering testing to formulate the diagnostic question in as specific a manner as possible. Such requests as "describe personality dynamics" or "rule out psychologic disturbance" are too general to answer in an effective and efficient manner. Do not hesitate to ask exactly what you want to know. The psychologist will inform you if he or she is unable to answer. Use the examples described above to formulate your question: Is this patient depressed? Is this patient psychotic? Why is this patient not conforming to the treatment regimen?
When presenting a patient to a psychologist for evaluation, it is helpful to have demographic data and a detailed history of the client. Also, the description presented of the problems should be in behavioral terms. Saying that a patient appears to be depressed is not as helpful as describing him or her as having a loss of appetite, early morning rising, or slowness of speech. If the patient is a management problem, give a concrete description of what this entails: won"t go to rehabilitation therapy, won"t let a technician draw blood.
Also, the description presented of the problems should be in behavioral terms. Saying that a patient appears to be depressed is not as helpful as describing him or her as having a loss of appetite, early morning rising, or slowness of speech. If the patient is a management problem, give a concrete description of what this entails: won"t go to rehabilitation therapy, won"t let a technician draw blood.
Finally, the referring physician may request either a specific test or an abbreviated battery. While some psychologists will go along with this practice, we do not encourage it. Psychologic tests, particularly personality ones, are only as good as the skills of the individual who administers and interprets them. The psychologist must feel confident and competent in the battery that he or she administers. Therefore, the number and choice of tests should be those of the psychologist, just as the medical procedures chosen for a patient are the responsibility of the physician in charge.
Basic Science
The most commonly used personality tests are the Rorschach, TAT, and MMPI. The assumptions underlying projective tests such as the Rorschach and TAT are that the standard set of stimuli are used as a screen to project material that cannot be obtained through a more structured approach. Ambiguous inkblots or pictures reinforce the use of individual expression and reduce resistance. A frequent criticism is the assumption that the individual simply responds to ambiguity with trivia or with what was most recently experienced, such as last night's television fare. The response to this criticism is the notion of psychic determinism. Behavior is a function of choice, not chance. Thus, how a person responds is a reflection of personal motives, fantasies, and needs.
The assumptions underlying projective tests such as the Rorschach and TAT are that the standard set of stimuli are used as a screen to project material that cannot be obtained through a more structured approach. Ambiguous inkblots or pictures reinforce the use of individual expression and reduce resistance. A frequent criticism is the assumption that the individual simply responds to ambiguity with trivia or with what was most recently experienced, such as last night's television fare. The response to this criticism is the notion of psychic determinism. Behavior is a function of choice, not chance. Thus, how a person responds is a reflection of personal motives, fantasies, and needs.
The best-known psychologic assessment tool is the Rorschach, the "inkblot test." It was first published by Hermann Rorschach in 1921 and was introduced to the United States in 1930 by Samuel Beck. The test consists of 10 symmetrical inkblots, half of which are acromatic. It is administered by giving the respondent one card at a time and asking him or her to describe what is seen. The respondent is told that he or she can see one or more things and that there are no right or wrong answers. The tester records the responses verbatim. There is then a second phase of testing called the inquiry. The respondent is again presented with each of the ten cards and asked to note the location of the response and what determines his or her answers.
The respondent is told that he or she can see one or more things and that there are no right or wrong answers. The tester records the responses verbatim. There is then a second phase of testing called the inquiry. The respondent is again presented with each of the ten cards and asked to note the location of the response and what determines his or her answers.
A large body of research takes to task the reliability and validity of projective techniques in general and the Rorschach in particular. The issue of reliability cannot be approached in a conventional sense with projective techniques. The Rorschach inkblots and the TAT pictures do not lend themselves to split-half reliability because the stimuli are not designed to be equivalent with each other. Test–retest reliability is difficult because many of the variables addressed by the test are affected by time. Interjudge reliability indices using Rorschach summary scores have been reported to be favorable, and Exner (1978), using his own scoring system, has reported test–retest reliability correlations ranging from . 50 to .90 on 17 different variables.
50 to .90 on 17 different variables.
Attempts at measuring the validity of the Rorschach also suffer from problems inherent in the nature of the test. The Rorschach is designed to assess highly complex, multidetermined behaviors for which prediction about specific acts is nearly impossible. It also assesses covert needs and fantasy life that may not currently or ever manifest themselves in overt behavior. Concurrent validity is contaminated by the unreliability of psychiatric diagnoses and the fact that individuals with similar diagnoses may indeed behave differently. In response to the criticisms on validity, Korner (1960) has answered that there is no good assessment technique capable of predicting behavior, so why criticize the Rorschach. He goes on to point out that projective techniques are not magic. They describe the personality at work, its adaptations and compromises, and the balance between fantasy and the demands of reality.
The TAT was developed by Henry Murray and Christiana Morgan in 1935. It consists of 30 achromatic picture cards, categorized into those appropriate for boys, girls, men, and women. It is customary to present approximately 10 cards to the respondent, who is then asked to tell a story about what is happening in the picture, what led up to it, and how will it turn out. The respondent is also asked to describe the characters" thoughts and feelings. As with the Rorschach, interjudge reliability is the most applicable test. Correlations have been about .80. The validity of the TAT can be measured when it is defined using specific procedures with a particular population and operationally defined criteria. Studies have examined both construct and concurrent validity. Stories have correlated significantly with behavioral measures of achievement and aggression. A correlation of .74 has been obtained between TAT expressed needs and those needs rated from autobiographies.
It consists of 30 achromatic picture cards, categorized into those appropriate for boys, girls, men, and women. It is customary to present approximately 10 cards to the respondent, who is then asked to tell a story about what is happening in the picture, what led up to it, and how will it turn out. The respondent is also asked to describe the characters" thoughts and feelings. As with the Rorschach, interjudge reliability is the most applicable test. Correlations have been about .80. The validity of the TAT can be measured when it is defined using specific procedures with a particular population and operationally defined criteria. Studies have examined both construct and concurrent validity. Stories have correlated significantly with behavioral measures of achievement and aggression. A correlation of .74 has been obtained between TAT expressed needs and those needs rated from autobiographies.
The most frequently used objective test for personality is the MMPI. It was published by Hathaway and McKinley in 1943 and revised in 1951. It is designed for ages 16 and over and contains 566 items to be answered yes or no. It may be administered to an individual or group, and the answer sheets can be hand- or machined-scored. The respondent is asked to read each question and decide what is true or false as applied to him or her and then to mark that response on the answer sheet. The test has four validity scales and eight clinical scales. The scales were developed empirically by administering an item pool to a large group of normal subjects, and contrasting their responses to those of selected homogeneous criteria groups of psychiatric patients. Those items that discriminate between the groups were used.
It is designed for ages 16 and over and contains 566 items to be answered yes or no. It may be administered to an individual or group, and the answer sheets can be hand- or machined-scored. The respondent is asked to read each question and decide what is true or false as applied to him or her and then to mark that response on the answer sheet. The test has four validity scales and eight clinical scales. The scales were developed empirically by administering an item pool to a large group of normal subjects, and contrasting their responses to those of selected homogeneous criteria groups of psychiatric patients. Those items that discriminate between the groups were used.
Results of the test are coded onto a profile sheet for interpretation. The mean t-score for each scale is 50 with a standard deviation (SD) of 10. The scale is significantly elevated beyond an SD of 2 or t-score of 70. Even though the MMPI is empirically derived, it shares a similar problem with the projective tests in terms of reliability and validity, that is, it is based on psychiatric diagnoses. How valid and reliable were the diagnoses of the patients in each of the criteria groups? The MMPI thoroughly addresses some other aspects of validity. The lie score (L) assesses social desirability. The F score is an internal consistency check, and the K score assesses test-taking attitude along a frankness–defensive continuum.
How valid and reliable were the diagnoses of the patients in each of the criteria groups? The MMPI thoroughly addresses some other aspects of validity. The lie score (L) assesses social desirability. The F score is an internal consistency check, and the K score assesses test-taking attitude along a frankness–defensive continuum.
An interesting hybrid between the projective and objective assessments is the semistructured incomplete-sentence test. While ostensibly a projective technique in which the respondent reflects his or her own wishes or conflicts to complete a sentence stem, it easily lends itself to objective scoring or screening for experimental use. The Rotter Incomplete Sentence Test is one of the more popular of this form of assessment. It contains 40 sentence stems each of which is to be completed by the respondent. The test takes approximately 20 minutes to complete and may be administered to an individual or to a group. It was originally used as a screening device to determine mental disturbance at an army convalescent hospital.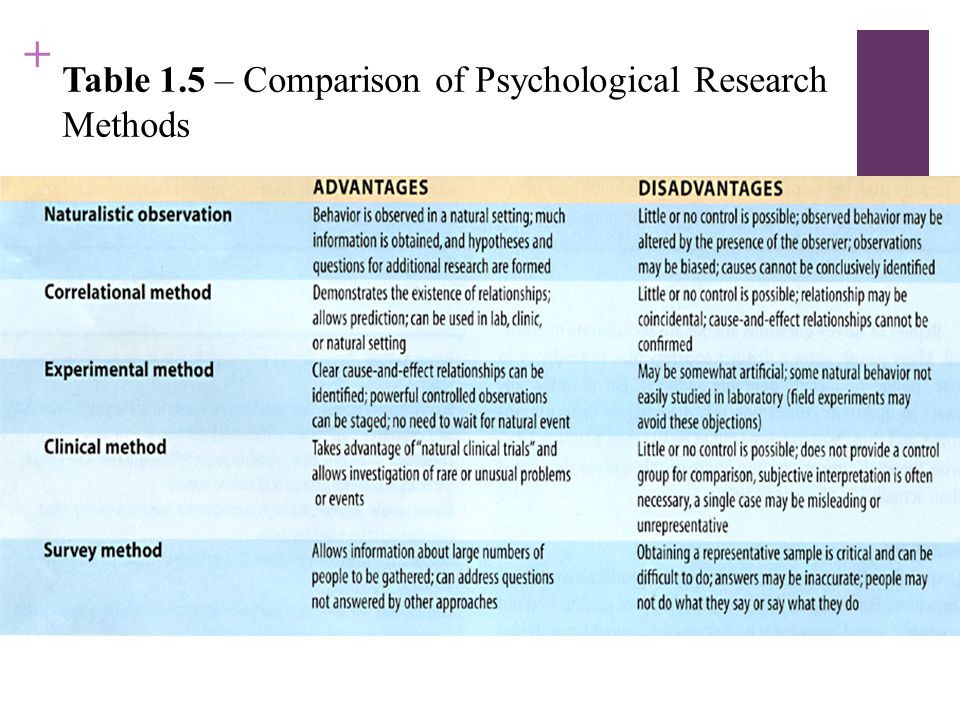 Reliability and validity correlations are quite acceptable. The interjudge reliability is about .90, and split-half reliability is .83. As to validity, correlation coefficients with adjustment and maladjustment classifications for women was .64 and for men .77.
Reliability and validity correlations are quite acceptable. The interjudge reliability is about .90, and split-half reliability is .83. As to validity, correlation coefficients with adjustment and maladjustment classifications for women was .64 and for men .77.
The use of intelligence testing in a clinical setting may be puzzling to the reader. In many ways the intelligence test is the foundation for differential diagnosis to the psychologist. The intelligence test measures major mental abilities that may be affected by the presence of an organic disease or injury, thought disorder, or environmental stress. The patterning of the scores on the intelligence test gives the psychologist clues as to the presence, extent, and relative influence of each of the above factors. The most empirically sound intelligence test is the WAIS-R, which was revised in 1981. The WAIS-R contains 11 tests, 6 verbal and 5 nonverbal. It was standardized on a stratified sample of ages ranging from 16 to 74 years, 11 months.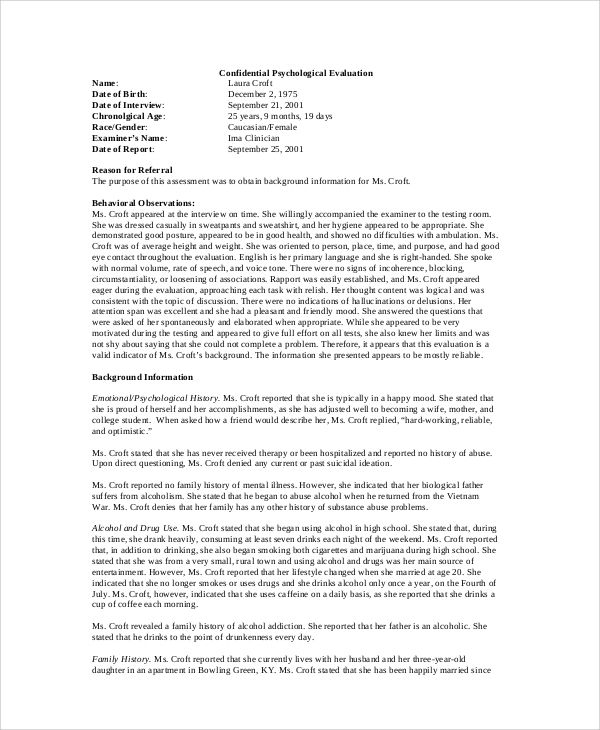 The basic score is the intelligence quotient (IQ), a comparison of the individual with the average score of his or her age group. Each of the 11 tests also has its own scale scores, which are conversions of raw scores dependent also on comparison to reference groups. The sum of scale scores are converted to three IQ scores: verbal, performance, and full-scale IQs. Mean IQ is 100 with an SD of 15; thus, two-thirds of all adults have an IQ between 85 and 115. Reliability coefficients are excellent in the mid-90's range. In terms of validity, there is a .50 correlation with school performance and a .85 correlation with the Stanford–Binet test of intelligence. The WAIS-R takes approximately 90 minutes to administer and requires a competent tester.
The basic score is the intelligence quotient (IQ), a comparison of the individual with the average score of his or her age group. Each of the 11 tests also has its own scale scores, which are conversions of raw scores dependent also on comparison to reference groups. The sum of scale scores are converted to three IQ scores: verbal, performance, and full-scale IQs. Mean IQ is 100 with an SD of 15; thus, two-thirds of all adults have an IQ between 85 and 115. Reliability coefficients are excellent in the mid-90's range. In terms of validity, there is a .50 correlation with school performance and a .85 correlation with the Stanford–Binet test of intelligence. The WAIS-R takes approximately 90 minutes to administer and requires a competent tester.
A physician who wants to rule out an organic brain syndrome may call upon neuropsychologic testing. This is particularly true when a CT scan is negative in the presence of suspicious symptomatology (early Alheizmer's disease), in assessing the relative importance of organic versus psychologic variables in the behavior of trauma victims, and in differentiating between dementia and depression in the elderly.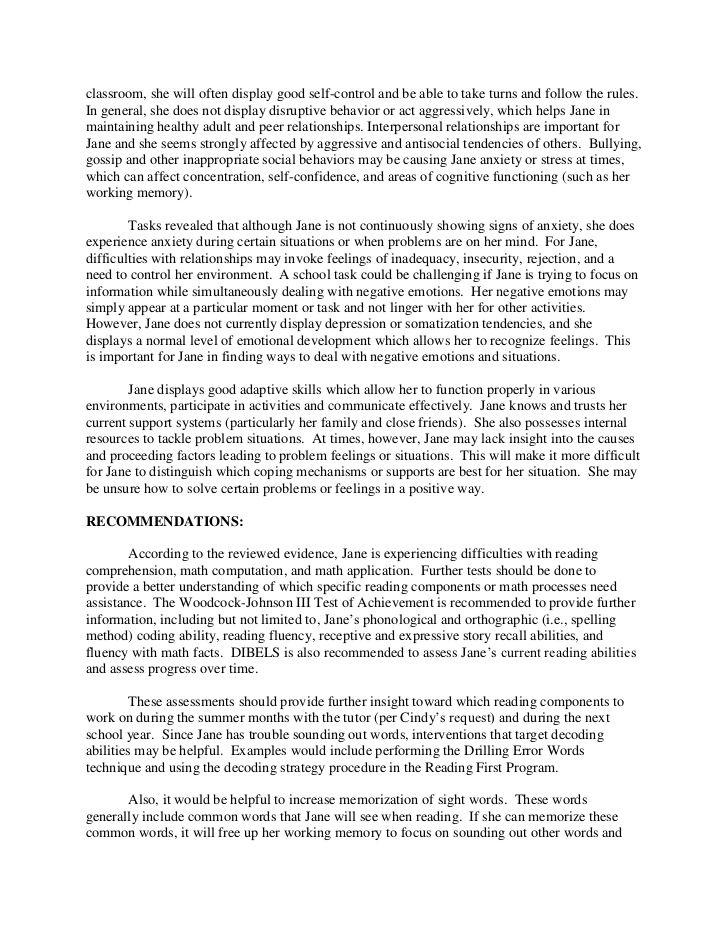 For cases in which an intense work-up for neurologic deficits is required, the patient should be referred to a specialist for neuropsychologic assessment. Since this procedure can be costly and time-consuming, the physician may want to screen first for the presence of a brain dysfunction. Most psychologists are well trained for this task. We will briefly describe two neuropsychologic tests that are useful for screening purposes. We do not necessarily endorse them as the best available, but only those with which we have familiarity.
For cases in which an intense work-up for neurologic deficits is required, the patient should be referred to a specialist for neuropsychologic assessment. Since this procedure can be costly and time-consuming, the physician may want to screen first for the presence of a brain dysfunction. Most psychologists are well trained for this task. We will briefly describe two neuropsychologic tests that are useful for screening purposes. We do not necessarily endorse them as the best available, but only those with which we have familiarity.
The first test is the Aphasia Screening Test adapted by Reitan (1984) from the Halstead/Wepman Aphasia Screening Test. It assesses several areas of dysfunction including dysphonia, dyslexia, spelling and constructional dyspraxia, and dyscalculia. The test uses the sign approach, that is, positive findings have distinct and definite significance, but normal performance cannot rule out organicity. Anyone with a basic grade school education is capable of answering every item correctly. The test is simple to administer and consists of 32 items that do not usually require more than 20 minutes to complete. The second, called the Category Test, is the most powerful in the Halstead/Reitan test battery. It consists of 205 stimuli and is divided into seven subtests. The Category Test assesses central processing, abstraction, and reasoning. The cutoff score is 51 errors. While Reitan recommends the use of a slide presentation with his own design projector and feedback system, DeFillipis and McCampbell (1979) have designed a much simpler method of presentation. Their Booklet Category Test (BCT) is portable, requiring only two loose-leaf notebooks and an answer sheet. They report .91 correlation between the BCT and the Category Test. There are two major criticisms of the Category Test: there is no normative data, and reliability has not been adequately studied. One study did report a test–retest correlation of .93.
The test is simple to administer and consists of 32 items that do not usually require more than 20 minutes to complete. The second, called the Category Test, is the most powerful in the Halstead/Reitan test battery. It consists of 205 stimuli and is divided into seven subtests. The Category Test assesses central processing, abstraction, and reasoning. The cutoff score is 51 errors. While Reitan recommends the use of a slide presentation with his own design projector and feedback system, DeFillipis and McCampbell (1979) have designed a much simpler method of presentation. Their Booklet Category Test (BCT) is portable, requiring only two loose-leaf notebooks and an answer sheet. They report .91 correlation between the BCT and the Category Test. There are two major criticisms of the Category Test: there is no normative data, and reliability has not been adequately studied. One study did report a test–retest correlation of .93.
Clinical Significance
The Rorschach describes personality structure, offering a multidimensional picture of the individual's current functioning and potential. As Korner (1960) states, the Rorschach shows the personality at work. There are several scoring systems for the Rorschach, most being based on four major categories: location, determinants, content, and the use of populars and originals. The location, or area of the response, yields information about the respondent's ability toward perceptual organization, abstraction, and synthesis. Determinants of the response refer to those qualities that produce it, such as form, shape, and color. They are tied to such personality variables as emotionality, impulsivity versus control, and openness versus constrictiveness. The content of the block reveals the personal meanings, attitudes, and interests of the respondent. Originals and populars are related to the respondent's creativity, reality testing, and conventionality, among other variables.
As Korner (1960) states, the Rorschach shows the personality at work. There are several scoring systems for the Rorschach, most being based on four major categories: location, determinants, content, and the use of populars and originals. The location, or area of the response, yields information about the respondent's ability toward perceptual organization, abstraction, and synthesis. Determinants of the response refer to those qualities that produce it, such as form, shape, and color. They are tied to such personality variables as emotionality, impulsivity versus control, and openness versus constrictiveness. The content of the block reveals the personal meanings, attitudes, and interests of the respondent. Originals and populars are related to the respondent's creativity, reality testing, and conventionality, among other variables.
Whereas the Rorschach presents personality structure and organization, the TAT reflects the content of personality, including needs, pressures, conflicts, values, and interest.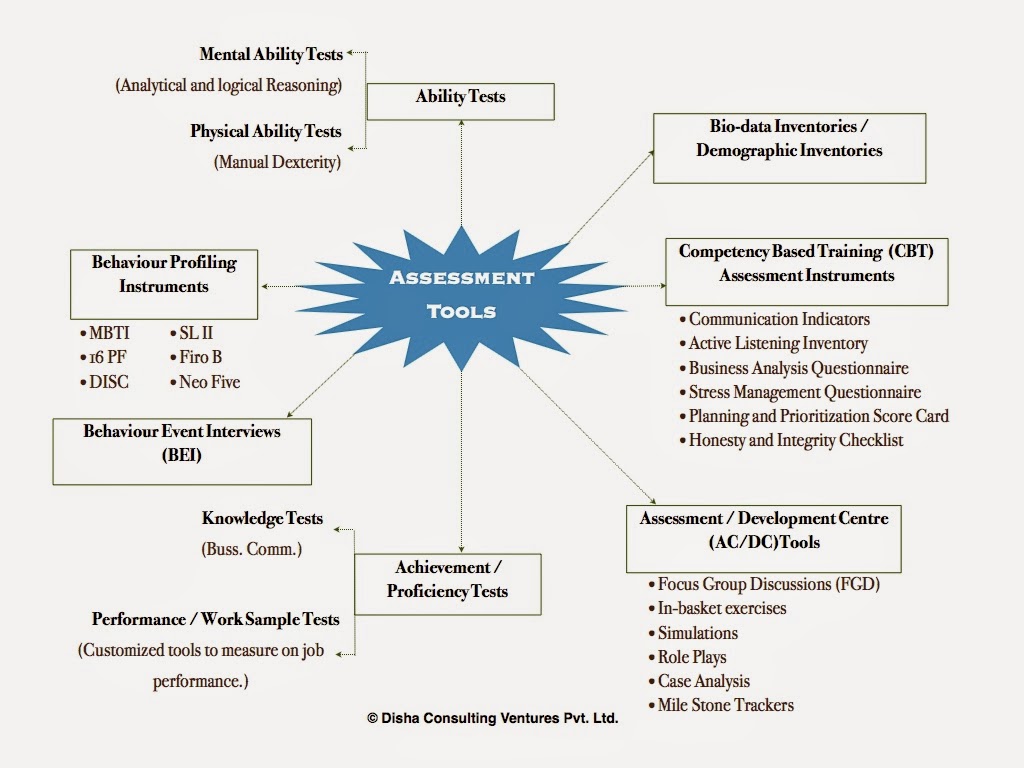 There are instances in which the content of a given TAT story is so revealing of the patient's difficulties that it would be reported verbatim in the psychologic report. Certain cards are said to "pull" specific types of themes: Card 1, attitudes toward authority; Card 4, attitudes toward heterosexual relationships; and Card 5, relationships with the mother figure. Also, diagnostic groups tend to have a certain orientation toward the stories. Obsessive–compulsives may be pedantic. Depressives may have short stories with monosyllabic words. Schizophrenics may have disjointed or delusional content.
There are instances in which the content of a given TAT story is so revealing of the patient's difficulties that it would be reported verbatim in the psychologic report. Certain cards are said to "pull" specific types of themes: Card 1, attitudes toward authority; Card 4, attitudes toward heterosexual relationships; and Card 5, relationships with the mother figure. Also, diagnostic groups tend to have a certain orientation toward the stories. Obsessive–compulsives may be pedantic. Depressives may have short stories with monosyllabic words. Schizophrenics may have disjointed or delusional content.
There are three approaches to interpretation of the MMPI: single scale, statistical, and clinical. Many physicians who order the MMPI are doing so because they are comfortable with the single scale approach. This involves looking at an elevated scale and making assumptions about the patient. As stated, there are eight clinical scales: HS (hypochondriasis), D (depression), HY (hysteria), PD (psychopathic deviant), PA (paranoia), PT (psychothemia), SC (schizophrenia), and MA (hypomania). Although space does not permit a description of all these scales, elevations of each are associated with a diagnostic grouping related to a cluster of symptoms; for example, elevated HS is associated with an immature person with lack of insight who tends to complain about his or her health. Interpretation of single scales must be taken with great caution. The scales were devised to fit with the Kraepelin System of diagnosis, which is outmoded. For instance, there is no longer a diagnostic grouping of psychopathic deviate. Each of the scales has a much different meaning in relation to more modern classifications.
Although space does not permit a description of all these scales, elevations of each are associated with a diagnostic grouping related to a cluster of symptoms; for example, elevated HS is associated with an immature person with lack of insight who tends to complain about his or her health. Interpretation of single scales must be taken with great caution. The scales were devised to fit with the Kraepelin System of diagnosis, which is outmoded. For instance, there is no longer a diagnostic grouping of psychopathic deviate. Each of the scales has a much different meaning in relation to more modern classifications.
The statistical approach for interpretation involves code types. A code type is a particular correlation of elevated clinical scales (e.g., 2 through 7). A large sample of patients are given the MMPI. They are grouped by similarity in code types. These groupings are then correlated with clinical and demographic data, the notion being that patients with similar MMPI profiles will manifest similar problems. The difficulty with this approach, often called the "cookbook" approach, is that the data do not tend to generalize to other settings.
The difficulty with this approach, often called the "cookbook" approach, is that the data do not tend to generalize to other settings.
The third approach to MMPI interpretation is the clinical approach. The expert clinician depends on his or her knowledge of personality dynamics, case history, and current environmental circumstances to formulate hypotheses as to psychologic difficulties of the respondent. The MMPI computer-generated report uses this type of approach. One has to be extremely cautious in relying too heavily on the report because its author has no firsthand knowledge of the respondent. The clinical psychologist administering the MMPI will use the clinical approach but seldom in isolation without other tests, or at least a clinical interview.
The Rotter Incomplete Sentence Blank is a screening device. We have found it useful as a way of obtaining content information similar to that of the TAT in patients who were too threatened or too depressed to take on the challenge of making up stories. Rotter has given several suggestions for interpretation in addition to a reliable scoring system. The adjusted person tends to produce stems that are more neutral and flippant. The statements tend to be short, concise, and humorous. The maladjusted individual tends to write longer sentences that are complicated and emotionally charged. A frequent theme is that nobody understands them.
Rotter has given several suggestions for interpretation in addition to a reliable scoring system. The adjusted person tends to produce stems that are more neutral and flippant. The statements tend to be short, concise, and humorous. The maladjusted individual tends to write longer sentences that are complicated and emotionally charged. A frequent theme is that nobody understands them.
It is not unusual for physicians to question the use of intelligence testing on their patients. The common assumption is that the test is not relevant to differential diagnosis. Contrary to this assumption, the intelligence test is an essential part of any test battery. First, the general level of intelligence will determine how much the patient is capable of understanding and therefore cooperating in his treatment. In other words, how concrete or simplified need the physician be in his or her instructions? Second, the intelligence test is a broad-based screening for organicity. The Verbal Scale IQ has been related to left hemisphere functioning and Performance Scale to right hemisphere.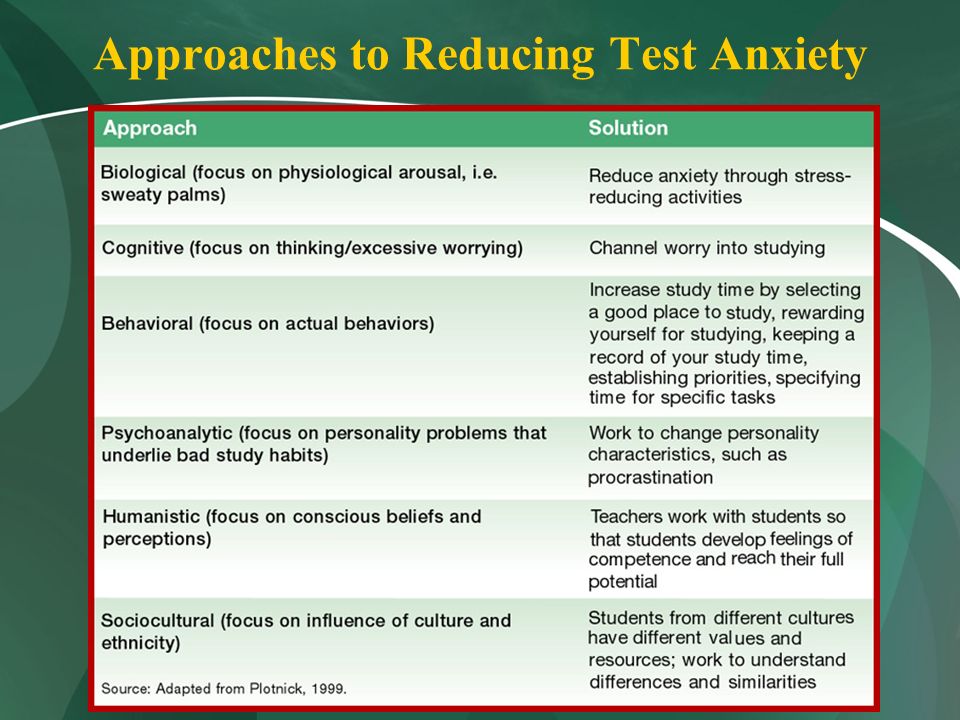 A significant difference of approximately 15 points between these two IQs requires more intense assessment. A dramatic difference between a given subscale mean and the mean for that scale may also be cause for concern. A third important use of the results of the intelligence test is its relationship to aspects of personality functioning. As an example, current state of anxiety can be related to subscale scores on digit span and picture completion. Loose association on the similarity or comprehension subtest may be associated with a psychotic process.
A significant difference of approximately 15 points between these two IQs requires more intense assessment. A dramatic difference between a given subscale mean and the mean for that scale may also be cause for concern. A third important use of the results of the intelligence test is its relationship to aspects of personality functioning. As an example, current state of anxiety can be related to subscale scores on digit span and picture completion. Loose association on the similarity or comprehension subtest may be associated with a psychotic process.
In the course of ordering psychologic consultation, if there is any question of the presence of brain dysfunction, the physician may want to order screening in the form of the Category Test and Aphasia Screening Test. The Category Test is the most powerful of the Halstead/Reitan battery. It is essentially a processing test assessing abstraction and reasoning. The Category Test measures level of performance and offers no information concerning localization. Further differentiation in terms of severity, location, or specificity requires more intense evaluation. A quick screening for localization would be the Aphasia Screening Test. It assesses both left and right hemisphere functioning with respect to language ability. If the respondent cannot copy correctly, we might suspect a right hemisphere lesion. On the other hand, if he or she cannot name an object, we might think about a left hemisphere lesion. In the use of this test there will be many false negatives but few false positives.
Further differentiation in terms of severity, location, or specificity requires more intense evaluation. A quick screening for localization would be the Aphasia Screening Test. It assesses both left and right hemisphere functioning with respect to language ability. If the respondent cannot copy correctly, we might suspect a right hemisphere lesion. On the other hand, if he or she cannot name an object, we might think about a left hemisphere lesion. In the use of this test there will be many false negatives but few false positives.
The physician usually receives the results of psychologic assessments in the form of a psychologic report. There are a variety of formats, so we will describe a typical one. The report will usually be about 2 to 3 typed pages, long enough to do the raw data justice but not so long as to impinge upon the valuable time of the physician. The first section will be a description of the presentation of the respondent and his or her test-taking behavior. The next section will describe the respondent's intellectual functioning, strengths and weaknesses, and the presence of organic symptoms. The third section is an overview of the respondent's current emotional and social functioning that may include samples of actual test responses as examples. In a final section, the psychologist summarizes the findings and offers recommendations. Interpretation of findings in psychologic test batteries largely depends on the clinical acumen of the psychologist. The organization and synthesis of test data require much skill and knowledge of personality dynamics. Each of the tests has a unique contribution to the overall clinical picture, but none can stand by itself. Thus, the psychologist must determine what is relevant, what is internally consistent, and what is central or irrelevant to diagnosis and intervention.
The third section is an overview of the respondent's current emotional and social functioning that may include samples of actual test responses as examples. In a final section, the psychologist summarizes the findings and offers recommendations. Interpretation of findings in psychologic test batteries largely depends on the clinical acumen of the psychologist. The organization and synthesis of test data require much skill and knowledge of personality dynamics. Each of the tests has a unique contribution to the overall clinical picture, but none can stand by itself. Thus, the psychologist must determine what is relevant, what is internally consistent, and what is central or irrelevant to diagnosis and intervention.
References
DeFilippis NA, McCampbell E. The manual for the Booklet Category Test. Odessa, FL: Psychological Assessment Resources, 1979.
Exner JE. The Rorschach: a comprehensive system. Vol. 2. New York: Wiley, 1978.
*Freeman FS.
 Theory and practice of psychological testing. New York: Holt, Rineholt & Winston, 1962.
Theory and practice of psychological testing. New York: Holt, Rineholt & Winston, 1962.Goldfried MR, Stricker G, Winer LB. Rorschach handbook of clinical and research applications. Englewood Cliffs, NJ: Prentice-Hall, 1971.
Harrison R. Thematic Apperception Test. In: Wolman B, ed. Handbook of clinical psychology. New York: McGraw-Hill, 1965;562–620.
*Hathaway SR, McKinley JC. Minnesota Multiphasic Personality Inventory: users guide for the Minnesota report. University of Minnesota, 1982.
*Jarvis PE, Barth JT. Halstead-Reitan Test Battery: an interpretative guide. Odessa, FL: Psychological Assessment Resources, 1984.
*Korner AF. Theoretical considerations concerning the scope and limitations of projective techniques. In: Murstin BI, ed. Handbook of projective techniques. New York: Basic Books, 1960;23–24.
MacInnes WE, Forch JR, Golden CJ. A cross-validation of a booklet form of the Category Test.
 Clin Neuropsychol. 1981;3:3–5.
Clin Neuropsychol. 1981;3:3–5.Mauger PA. Predicting response to treatment using the MMPI. In: Butcher J, Dahlstrom G, Gynther M, Schofield W, eds. Clinical notes on the MMPI. Nutley, NJ: Hoffman-LaRoche, 1980.
Reitan RM. Aphasia and sensory-perceptual deficits in adults. Tucson: Reitan Neuropsychology Laboratories, 1984.
Rotter JB, Fafferty JE, Schachtitz E. Validating the Rotter Incomplete Sentence Test for college screening. In: Murstein BI, ed. Handbook of projective techniques. New York: Basic Books, 1960;859–72.
*Schneidman ES. Projective techniques. In: Wolman BB, ed. Handbook of clinical psychology. New York: McGraw-Hill, 1965;498–521.
Wechsler D. The WAIS-R manual. New York: Harcourt Brace Jovanovich, 1981.
Psychological tests when applying for a job with answers online
Modern working conditions, productivity and quality of work performed, increasingly require from applicants appropriate performance, personal, psychological and business qualities.
For this, many serious organizations use testing when hiring, especially in such departments as the FSB, the Ministry of Internal Affairs, Russian Railways .., banks, including Sberbank .., as well as large corporations.
Who takes psychological tests online?
Soft Skills Test Flexible skills (assessment of competence)
Career guidance online
Employment tests are conducted for accountants, managers, police and firefighters, pilots and machinists, and for lawyers, and even for salesmen- consultants ...
On this page of the psychoanalytic site Psychoanalyst-Matveev.RF you can pass psychological tests used for hiring in various departments and organizations online and free of charge.
However, please note that these are examples of tests used when applying for a job, as each employer can use his testing, depending on the necessary personal, mental, emotional, moral and business qualities of the applicant for a particular position or profession, in a particular enterprise or institution.
(Large corporations use the SHL, Talent Q, Ontardent, Exect tests)
Important point: testing… set yourself up for success… (read more: how to pass an interview)
Examples of the main psychological tests used when applying for a job in various departments, organizations and enterprises, such as the FSB, the Ministry of Internal Affairs, the Ministry of Emergency Situations ..., Banks (Sberbank), trade ..., testing for the positions of a manager, chief accountant, policeman, firefighter, rescuer , a sales worker (sales assistant), a lawyer ... etc. (professional test)
Psychological tests
General psychological tests when applying for a job are not used as often as specialized ones for certain professions.
However, the results of tests for the speed of the course of nervous processes (temperament), character accentuation, memory, attention and attentiveness may be of interest to some employers.
Mandatory psychiatric examination of drivers upon employment (Labor Code of the Russian Federation art. 212, 213, Decree 695, 377, order of the Ministry of Health and Social Development of the Russian Federation 302n, order of the Federal Medical and Biological Agency of Russia (FMBA) 121)
212, 213, Decree 695, 377, order of the Ministry of Health and Social Development of the Russian Federation 302n, order of the Federal Medical and Biological Agency of Russia (FMBA) 121)
- Online profession test for teenagers and adults
- Personality test - (software version)
- Temperament test - (software version)
- Mindfulness test (attention switch)
- Test motivation for success (in profession, type of activity)
- Test for professional growth (career motivation)
- Psychological test from Sberbank when applying for a job
Verbal tests
A verbal test when applying for a job is the basis of an interview with an applicant for a position and profession, where the verbal (speech) abilities of the applicant are needed.
- Online verbal test
Math tests
Some corporations use math tests to determine an applicant's analytical skills when applying for a job.
- Math test (with answers)
- Analytical mindset
Numerical tests
For some positions, such as accounting, employers use numerical tests when applying for a job.
- Numerical Test
- SHL Test
Logic Tests
Logic Job Application Tests inform the employer about the applicant's ability to find the right solutions in unfamiliar situations.
Test for logical thinking
Test for logic
Emotional tests
Emotional stability, stress resistance - necessary indicators of certification - tests when hiring and subsequent re-certification - applicants and current employees in positions where you need to work with people in dangerous, emergency and stressful situations (for example, police, Ministry of Emergency Situations , trade…)
- Online stress test
- Burnout test
- Neuropsychic stability test
- Stress test
Personality tests
The main widely used personality test in hiring is the SMIL test (Standardized Multivariate Personality Research Method) - aka the Minnesota Multivariate Personality Inventory (MMPI) and its abbreviated version MMPI Mini-Mult
Intelligence tests
Level, coefficient intelligence (IQ) of the applicant is often the most important indicator of testing when applying for a job where the intellectual abilities of the future employee are necessary.
- Russian literacy test
- Online COT test (short indicative questionnaire for determining general mental abilities - sometimes used in the MIA CPD)
- Online IQ test
- Genius test (also known as the "Red Square" reaction test - sometimes used in the CPD of the Ministry of Internal Affairs)
- Intelligence test
- IQ test (aikyu)
Creative tests
Many modern organizations require creative, creative people who sometimes need to have organizational and even entrepreneurial abilities, so creative tests are also used when hiring.
- Creativity Test
- Creativity Test
- Organizational Ability Test
- Entrepreneurial Ability Test
- Test for creativity
- Test for general erudition
See all psychological tests of the site http://Psychoanalyst-Matveev. RF
RF
General list of psychological tests will be expanded upon admission bookmark the site and visit more often…
Psychoanalyst consultation before getting a job (for a fee)
Psychological training for each individual
Self-hypnosis to set yourself up for a device to work and pass testing.
Psycho-training to relieve stress before an interview and passing tests when applying for a job
10 psychological tests that will help you get to know yourself better
March 12, 2021Education
Questionnaires to test intelligence, anxiety level, conflict level and more.
Share
01. Raven IQ test
This test will help you determine how smart, quick-witted and logical you are. It consists of 60 tasks, the complexity of which gradually increases.
Each question is a picture with symbols or shapes linked together. Your task is to understand how they are located, and then insert the missing element into the image.
Pass the test →
2. SMIL test
This questionnaire will be useful to make your comprehensive psychological portrait. You will be able to find out the type of personality, dominant character traits, communication style, propensity to take risks, level of self-esteem ... And that's not all!
However, to get the coveted result, you have to work hard: the full version of the test consists of 567 statements. You will have to choose whether you agree with them or not. But there is also an abbreviated version for express diagnostics of 65 questions.
Take the full test →
Take the short test →
3. Thomas-Kilmann test
Find out how prone you are to conflict and how you behave when things get heated. Check which style of disagreement resolution suits you best: confrontation, compromise, or silence.
The questionnaire consists of 30 pairs of statements. In each question, you will need to choose the answer that most accurately characterizes your behavior.
Take the test →
4. Test "House, tree, person"
Drawings of a person can tell a lot about his inner world. Check it out for yourself: draw a house, a tree and a person on paper, and then find out what it all means.
After interpreting the results, you will receive information about what lies in your subconscious, how comfortable you feel in society, what worries you and other interesting data.
Take the test →
5. Interpersonal Relationship Questionnaire
This test will help you determine your level of socialization. Check how easy it is for you to get close to people, how much they influence you, and how great your need for communication and attention is in general.
Be as honest as possible when taking the test. Answer the way you really think, not the way others expect you to. Then the results will be more reliable.
Pass test →
6. Activity Styles Questionnaire
Activity style is the means and techniques by which a person achieves the set results. Answer questions about your temperament, character and interests, and then find out if you are an activist, thinker, theorist or pragmatist.
Answer questions about your temperament, character and interests, and then find out if you are an activist, thinker, theorist or pragmatist.
After passing the test, you will receive a detailed description of your type, and also find out what can reduce and increase your effectiveness in achieving your goals.
Pass test →
7. Taylor Anxiety Scale
Sometimes healthy anxiety can be helpful. It helps to be more attentive and more careful in unforeseen situations. But if anxiety arises for no reason and exceeds reasonable limits, it greatly complicates life. The test will help you find out if you are prone to this disorder.
Pass the test →
8. Boyko test for diagnosing burnout
Fatigue, irritability, poor sleep and inability to concentrate on the task at hand are true companions of emotional burnout. If you're experiencing any of these symptoms, take the test and see if it's time for you to take a vacation and get some rest.
Take the test →
9.