Psychodynamic therapy depression
Psychodynamic Therapy for Depression: Techniques, Effectiveness, and More
Written by Joseph Saling
In this Article
- What Distinguishes Psychodynamic Therapy From Other Therapies for Depression?
- Is Psychodynamic Therapy an Effective Treatment for Depression?
- What Are the Main Features of Psychodynamic Therapy?
- What Can Someone Expect to Get From Psychodynamic Therapy?
Psychodynamic therapy is the kind of talk therapy many people imagine when they think of psychological treatment for depression. That's because the image of the psychiatrist and patient probing the past is a staple of our popular culture. It can be found on sitcoms or in jokes. And psychodynamic therapy has been a major element in movies like Good Will Hunting and Ordinary People and on the stage in plays like Equus.
Psychodynamic therapy is designed to help patients explore the full range of their emotions, including feelings they may not be aware of. By making the unconscious elements of their life a part of their present experience, psychodynamic therapy helps people understand how their behavior and mood are affected by unresolved issues and unconscious feelings.
What Distinguishes Psychodynamic Therapy From Other Therapies for Depression?
Psychodynamic therapy is one of three main types of therapy used to treat depression. The other two are cognitive behavioral therapy (CBT) and interpersonal therapy (IPT). What distinguishes them is the nature of their focus.
Both CBT and IPT are focused on understanding and modifying certain processes or behaviors. For CBT, the focus is on how a person thinks. Thoughts shape what a person does and how a person feels and reacts; CBT focuses on identifying and changing dysfunctional patterns of thought.
With IPT the emphasis is on identifying issues and problems in interpersonal relationships and learning ways to address and improve them. Both CBT and IPT are also time-limited, short-term therapies. The emphasis is on learning new patterns rather than analyzing why the dysfunctional patterns are there.
The emphasis is on learning new patterns rather than analyzing why the dysfunctional patterns are there.
Psychodynamic therapy, on the other hand, grew out of the theories and practices of Freudian psychoanalysis. Psychoanalysis is based on the idea that a person's behavior is affected by the unconscious mind and by past experiences. Psychoanalysis involves an intense, open-ended exploration of a patient's feelings, often with multiple sessions in a week. The sessions include an examination of the feelings the patient is aware of and those the patient is unaware of before therapy begins.
Psychodynamic therapy is less intense than formal psychoanalysis. Sessions usually occur once a week and are typically 50 minutes each. Patients usually sit up in a chair rather than lie on a couch with the therapist out of sight. But unlike IPT and CBT, both of which have sessions that adhere to a formal, outlined structure and that set specific learning agendas, psychodynamic therapy sessions are open-ended and based on a process of free association.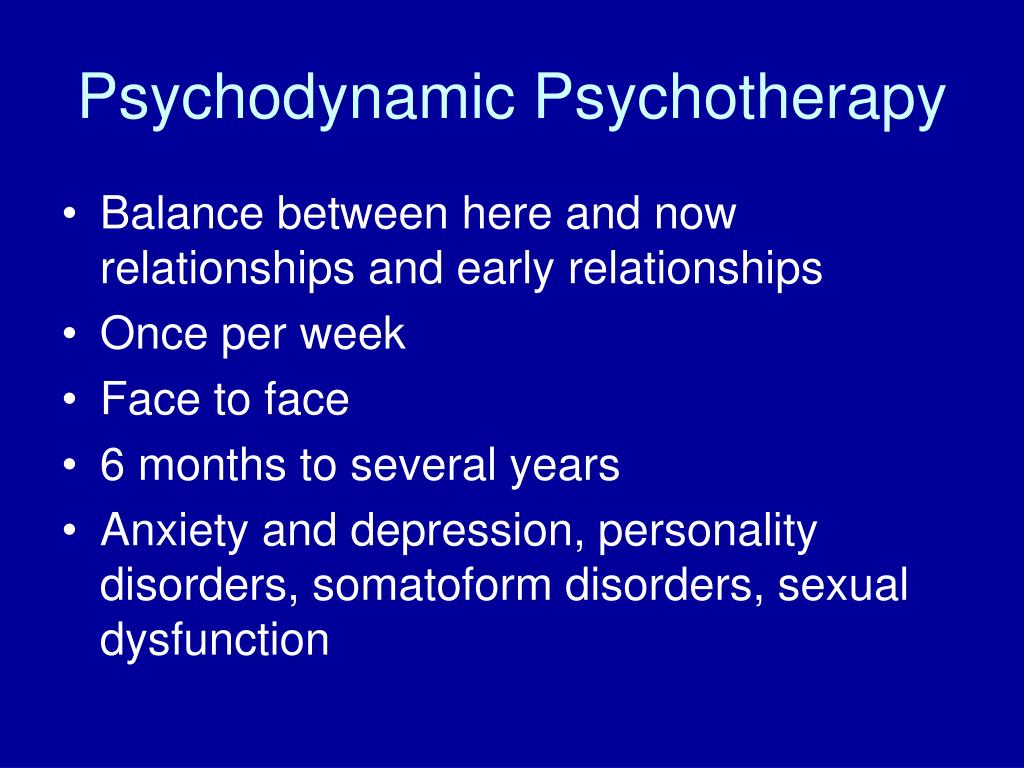
In psychodynamic therapy, the patient is encouraged to talk freely about whatever happens to be on their mind. As the patient does this, patterns of behavior and feelings that stem from past experiences and unrecognized feelings become apparent. The focus is then put on those patterns so the patient can become more aware of how past experience and the unconscious mind are affecting their present life.
Another distinction between the types of therapies is that psychodynamic therapy is not necessarily a short-term, time-limited treatment. While some courses of therapy may end after 16 to 20 weeks, other instances may go on for more than a year.
Is Psychodynamic Therapy an Effective Treatment for Depression?
Until recently, it was commonly thought there was little or no evidence to support the effectiveness of psychodynamic therapy as a treatment for depression. Part of the reason was that practitioners of psychodynamic therapy were not as focused on doing empirical research as practitioners of other therapies such as CBT and IPT.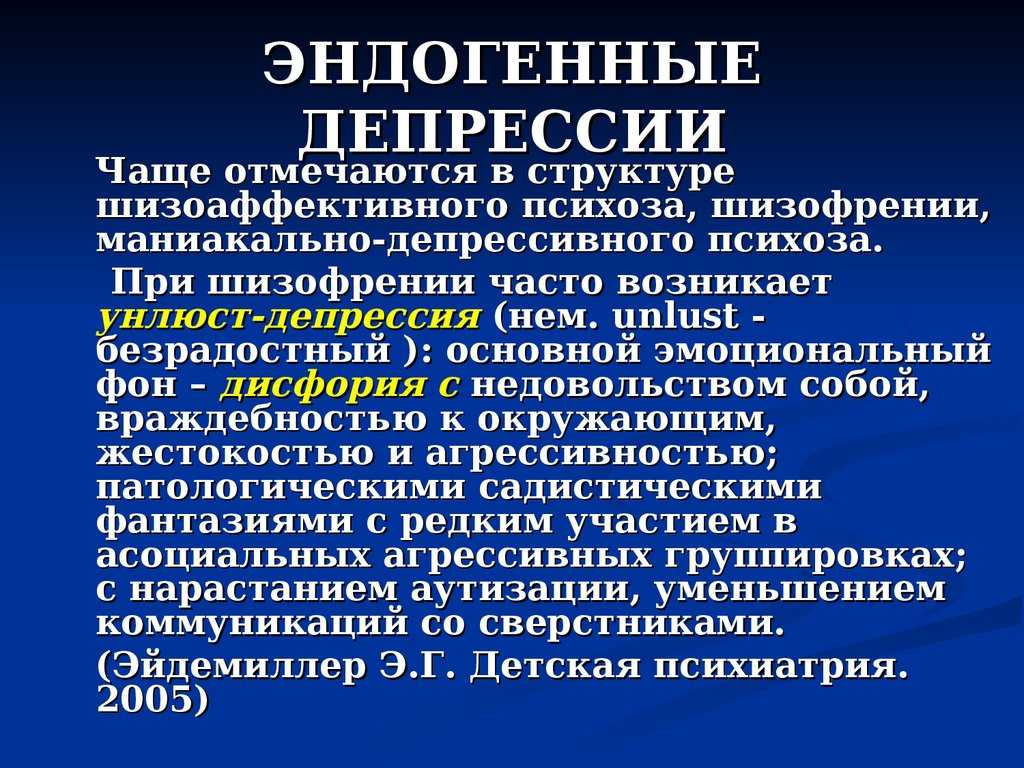 But over the past couple of decades, that has changed and more studies have appeared.
But over the past couple of decades, that has changed and more studies have appeared.
Early in 2010, a report published in the American Psychologist reviewed the data from existing studies of psychodynamic therapy and depression. The author concluded that not only did the data show that psychodynamic therapy was at least as effective as other evidence-based therapies, but also the benefits of psychodynamic therapy appeared to be longer lasting.
What Are the Main Features of Psychodynamic Therapy?
Psychodynamic therapy involves an exploration of the entire range of a patient's emotions. With the help of the therapist, the patient finds ways to talk about feelings that include contradictory feelings, feelings that are troubling or threatening, and feelings that the patient may not have recognized or acknowledged in the past. This exploration takes place in a context that recognizes the fact that being able to explain the reason for an emotional difficulty does not mean the person is capable of doing anything about it. The goal then is to foster the internal resources needed to deal with and effectively manage those difficulties.
The goal then is to foster the internal resources needed to deal with and effectively manage those difficulties.
In addition to a focus on emotions, psychodynamic therapy focuses on recognizing and addressing defense mechanisms -- reactions and behaviors a patient uses to avoid distressing thoughts and feelings. For instance, an individual may try to suppress memories of troublesome experiences or may habitually change the topic when certain topics come up. Other reactions might include being late or missing sessions when the topics have become too troublesome, or focusing on external details instead of the person's own role in something.
As the sessions continue, recurring patterns in the patient's thinking, feelings, and behavior will emerge. Often these patterns are subtle and unknown to the individual. The therapist helps the patient recognize these patterns and try to understand their significance and how they affect the patient's mood and reactions. Often, discussing the patterns will lead to an examination of past experiences that continue to influence the present.
There is also an emphasis in psychodynamic therapy on relationships, especially the relationship between the therapist and the patient. Seeing how the patient reacts inside that relationship gives the therapist an indication of how the patient reacts, feels, and interacts in other relationships. Often, psychological difficulties stem from problems in the way someone relates to others that interfere with the ability to have emotional needs met. An aim in psychodynamic therapy is to recognize those difficulties and to find ways to resolve them or cope with them better.
Psychodynamic therapy also involves the exploration of the patient's fantasy life, including the possible psychological meaning behind the imagery or emotional content of dreams. Because the patient is encouraged to speak freely, they are able to explore whatever is on their mind.
What Can Someone Expect to Get From Psychodynamic Therapy?
The primary goals of psychodynamic therapy are for an individual to achieve greater insight about their unconscious conflicts and self-awareness about their feelings and motivations. Insight is thought to be the mechanism that can lead to the relief of symptoms. In addition, psychodynamic therapy aims to help the patient develop internal psychological resources and greater capacity for dealing with psychological issues that have caused emotional suffering. The individual does this by confronting issues that have been unconsciously repressed but that still affect their life and by learning healthier ways to deal with them so they don't interfere with the effort to live a more fulfilling life.
Insight is thought to be the mechanism that can lead to the relief of symptoms. In addition, psychodynamic therapy aims to help the patient develop internal psychological resources and greater capacity for dealing with psychological issues that have caused emotional suffering. The individual does this by confronting issues that have been unconsciously repressed but that still affect their life and by learning healthier ways to deal with them so they don't interfere with the effort to live a more fulfilling life.
Depression Guide
- Overview & Causes
- Symptoms & Types
- Diagnosis & Treatment
- Recovering & Managing
- Finding Help
Depression and psychodynamic psychotherapy - PMC
Braz J Psychiatry. 2018; 40(1): 105–109.
Published online 2017 Jun 12. doi: 10.1590/1516-4446-2016-2107
,, and
Author information Article notes Copyright and License information Disclaimer
Depression is a complex condition, and its classical biological/psychosocial distinction is fading. Current guidelines are increasingly advocating psychotherapy as a treatment option. Psychodynamic psychotherapy models encompass a heterogeneous group of interventions derived from early psychoanalytic conceptualizations. Growing literature is raising awareness in the scientific community about the importance of these treatment options, as well as their favorable impact on post-treatment outcomes and relapse prevention. Considering the shifting paradigm regarding treatment of depressive disorder, the authors aim to provide a brief overview of the definition and theoretical basis of psychodynamic psychotherapy, as well as evaluate current evidence for its effectiveness.
Current guidelines are increasingly advocating psychotherapy as a treatment option. Psychodynamic psychotherapy models encompass a heterogeneous group of interventions derived from early psychoanalytic conceptualizations. Growing literature is raising awareness in the scientific community about the importance of these treatment options, as well as their favorable impact on post-treatment outcomes and relapse prevention. Considering the shifting paradigm regarding treatment of depressive disorder, the authors aim to provide a brief overview of the definition and theoretical basis of psychodynamic psychotherapy, as well as evaluate current evidence for its effectiveness.
Keywords: Depressive disorder, mood disorders, unipolar, psychotherapy, psychoanalysis and psychodynamic therapies
Depression is considered a frequent and complex condition. According to the World Health Organization, it is expected to be the third leading cause of disability worldwide by 2020. 1 The lifetime prevalence of major depressive disorder (MDD) is estimated at around 2-20%. The Global Burden of Disease Study 20102 revealed it as the second most prevalent cause of illness-induced disability, affecting people of all ages and social status, and a major impact factor in social, professional, and interpersonal functioning. Mathers et al.3 predicted MDD as the leading worldwide cause of disease burden in high-income countries by the year 2030. The decrement in health associated with depression is described as significantly greater than that associated with other chronic diseases.4 More than 60% of patients with MDD have a clinically significant impairment in their quality of life.5
1 The lifetime prevalence of major depressive disorder (MDD) is estimated at around 2-20%. The Global Burden of Disease Study 20102 revealed it as the second most prevalent cause of illness-induced disability, affecting people of all ages and social status, and a major impact factor in social, professional, and interpersonal functioning. Mathers et al.3 predicted MDD as the leading worldwide cause of disease burden in high-income countries by the year 2030. The decrement in health associated with depression is described as significantly greater than that associated with other chronic diseases.4 More than 60% of patients with MDD have a clinically significant impairment in their quality of life.5
Common features of all depressive disorders include the presence of sad or irritable mood, accompanied by somatic and cognitive changes that significantly affect the individual’s capacity to function.6 Overall, depression is characterized by a general feeling of sadness, anhedonia, avolition, worthlessness, and hopelessness. Cognitive and neurovegetative symptoms, such as difficulty in concentrating, memory alterations, anorexia, and sleep disturbances, are also present.
Cognitive and neurovegetative symptoms, such as difficulty in concentrating, memory alterations, anorexia, and sleep disturbances, are also present.
Various known risk factors for depression have been recorded in the literature: female gender, older age, poorer coping abilities, physical morbidity, impaired level of functioning, reduced cognition, and bereavement. Depression has been associated with an increased risk of mortality and poorer treatment outcomes in physical disorders.7
Although not fully understood, psychological, social and biological processes are thought to overdetermine the etiology of depression; comorbid psychiatric diagnoses (e.g., anxiety and various personality disorders) are common in depressed people.8
The classical biological/psychosocial distinction, which separates psychotherapy from pharmacotherapy as treatment options for depression, is fading out. Growing evidence from the neuroscientific literature supports similar (and different) changes in brain functioning with these approaches, concluding that both psychotherapy and pharmacotherapy are biological treatments, and that there is no legitimate ideological justification for the decline of the former. 9
9
Understandably, current treatment guidelines10,11 for depressive disorders are increasingly advocating psychotherapy as a treatment option, alone or in combination with antidepressant medications.
Considering this shifting paradigm regarding treatment of depressive disorder, the authors aim to evaluate current evidence for the effectiveness of psychodynamic psychotherapy (PDP) in depression. A brief clarification of the definition of PDP and its theoretical basis for understanding depression are also presented.
A narrative review was performed, including recent and current published papers on PDP and its role as a treatment modality in depressive disorders. Recent empirical studies were also included in order to integrate authors’ critical perspectives, supported by classical and contemporary literature.
Defining psychodynamic psychotherapy
PDP models are derived from early psychoanalytic conceptualizations, including ego psychology, object-relations theory, self-psychology, and attachment theory. Treatment goals or focus and setting changes have been reconsidered by contemporary authors. Gabbard12 described PDP’s basic principles as: much of mental life is unconscious; childhood experiences, in concert with genetic factors, shape the adult; the patient’s transference to the therapist is a primary source of understanding; the therapist’s countertransference provides valuable understanding about what the patient induces in others; the patient’s resistance to the therapeutic process is a major focus of therapy; symptoms and behaviors serve multiple functions, and are determined by complex and often unconscious forces; finally, the psychodynamic therapist assists the patient in achieving a sense of authenticity and uniqueness.
Treatment goals or focus and setting changes have been reconsidered by contemporary authors. Gabbard12 described PDP’s basic principles as: much of mental life is unconscious; childhood experiences, in concert with genetic factors, shape the adult; the patient’s transference to the therapist is a primary source of understanding; the therapist’s countertransference provides valuable understanding about what the patient induces in others; the patient’s resistance to the therapeutic process is a major focus of therapy; symptoms and behaviors serve multiple functions, and are determined by complex and often unconscious forces; finally, the psychodynamic therapist assists the patient in achieving a sense of authenticity and uniqueness.
PDP operates on an interpretive-supportive continuum. Interpretive interventions enhance the patient’s insight about repetitive conflicts sustaining his or her problems. The prototypic insight-enhancing intervention is an interpretation by which unconscious wishes, impulses, or defense mechanisms are made conscious.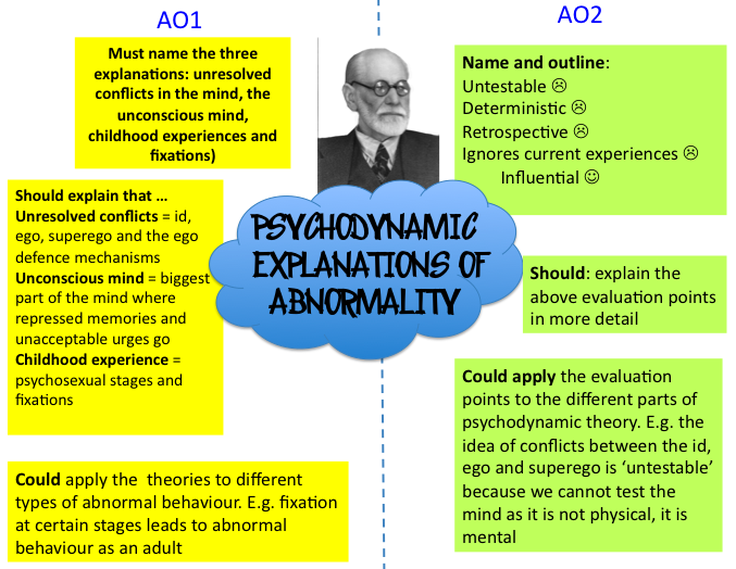 Supportive interventions aim to strengthen abilities (“ego functions”) that are temporarily not accessible to a patient due to acute stress or that have not been sufficiently developed. Thus, supportive interventions maintain or build ego functions. Supportive interventions include, for example, fostering a therapeutic alliance, setting goals, or strengthening ego functions such as reality testing or impulse control. The use of more supportive or more interpretive (insight-enhancing) interventions depends on the patient’s needs.13
Supportive interventions aim to strengthen abilities (“ego functions”) that are temporarily not accessible to a patient due to acute stress or that have not been sufficiently developed. Thus, supportive interventions maintain or build ego functions. Supportive interventions include, for example, fostering a therapeutic alliance, setting goals, or strengthening ego functions such as reality testing or impulse control. The use of more supportive or more interpretive (insight-enhancing) interventions depends on the patient’s needs.13
Common factors of psychotherapy and specific features of the psychodynamic approach
Common factors are currently understood as a set of common elements that collectively shape a theoretical model about the mechanisms of change during psychotherapy. A recent meta-analysis14 has shed light on strong evidence regarding factors such as therapeutic alliance, empathy, expectations, cultural adaptation, and therapist differences in terms of their importance for psychotherapeutic treatments in theory, research, and practice.
Overall, the influence of common factors in psychotherapies has been estimated at 30% when considering the variation in depression outcomes. Nonetheless, other factors, including specific techniques, expectancy, the placebo effect, and extratherapeutic effects, have also been studied.15
Zuroff & Blatt16 have concluded that the nature of the psychotherapeutic relationship, reflecting interconnected aspects of mind and brain operating together in an interpersonal context, predicts outcome more robustly than any specific treatment approach per se.
Regarding common factors in PDP, Luyten et al.15 mentioned the important differences between psychodynamic and other treatments. Comparatively to cognitive-behavioral therapists, psychodynamic therapists tend to place stronger emphasis on certain aspects, namely: affect and emotional expression; exploration of patients’ tendency to avoid topics; identification of recurring behavioral patterns, feelings, experiences, and relationships; the past and its influence on the present; interpersonal experiences; the therapeutic relationship; and exploration of wishes, dreams, and fantasies. Along with these features, specific characteristics of a psychodynamic-oriented treatment have been described: a focus on the patient’s internal world; a developmental perspective; and a person-centered approach.
Along with these features, specific characteristics of a psychodynamic-oriented treatment have been described: a focus on the patient’s internal world; a developmental perspective; and a person-centered approach.
Depression from the psychodynamic perspective
Psychodynamic understandings of depressive disorders were first described by Freud, Abraham, and Klein. Freud explored the individual’s reactions to an actual loss or disappointment associated to a loved person, or to a loss of an ideal. Plainly, he tried to explain why some people react with a mourning affect (surpassed after a period of time) and others succumb into melancholy (depression, as we now call it). Mourning is the reaction to the loss of a loved one or the loss of an abstraction, which has taken the place of something (a country, freedom, or an ideal, for example), and although it involves significant disruptions from one’s normal attitude towards life, it should not be regarded as pathological. Thus, mourning occurs following loss of an external object.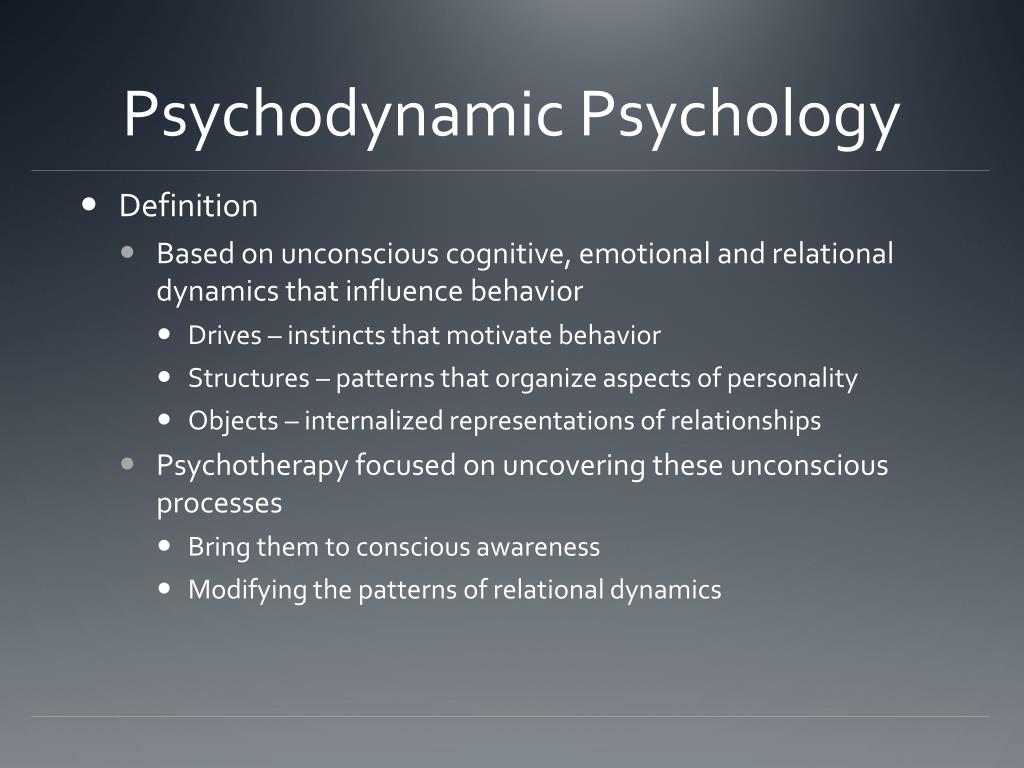 Melancholy, on the other hand, arises from the loss of the object’s love and is an unconscious process where a remarkable decrease in self-esteem is observed. Culpability is also a feature clearly present in melancholic processes, as the loss of the object comes with feelings of guilt, stressing the ambivalent feelings towards the lost object; not only because the individual knows that he or she attacked (in fantasy or in reality) the lost object, but mostly because he or she desired that very loss (due to the object’s unsatisfactory presence and love). Freud clearly outlined the symptoms of melancholy: “... a profoundly painful dejection, cessation of interest in the outside world, loss of capacity to love, inhibition of all activity, and lowering of the self-regarding feelings to a degree that finds utterance in self-reproaches and self-revilings and culminates in delusional expectations of punishment.”17 These features seem to resemble the current DSM definition of depression.
Melancholy, on the other hand, arises from the loss of the object’s love and is an unconscious process where a remarkable decrease in self-esteem is observed. Culpability is also a feature clearly present in melancholic processes, as the loss of the object comes with feelings of guilt, stressing the ambivalent feelings towards the lost object; not only because the individual knows that he or she attacked (in fantasy or in reality) the lost object, but mostly because he or she desired that very loss (due to the object’s unsatisfactory presence and love). Freud clearly outlined the symptoms of melancholy: “... a profoundly painful dejection, cessation of interest in the outside world, loss of capacity to love, inhibition of all activity, and lowering of the self-regarding feelings to a degree that finds utterance in self-reproaches and self-revilings and culminates in delusional expectations of punishment.”17 These features seem to resemble the current DSM definition of depression.
Abraham proposed a specific model for the melancholic process,18 consisting of a series of explanatory events: after an initial frustration (loss of an object), the subject reacts with externalization of the introjected object and its destruction, thus to an early anal-sadistic stage.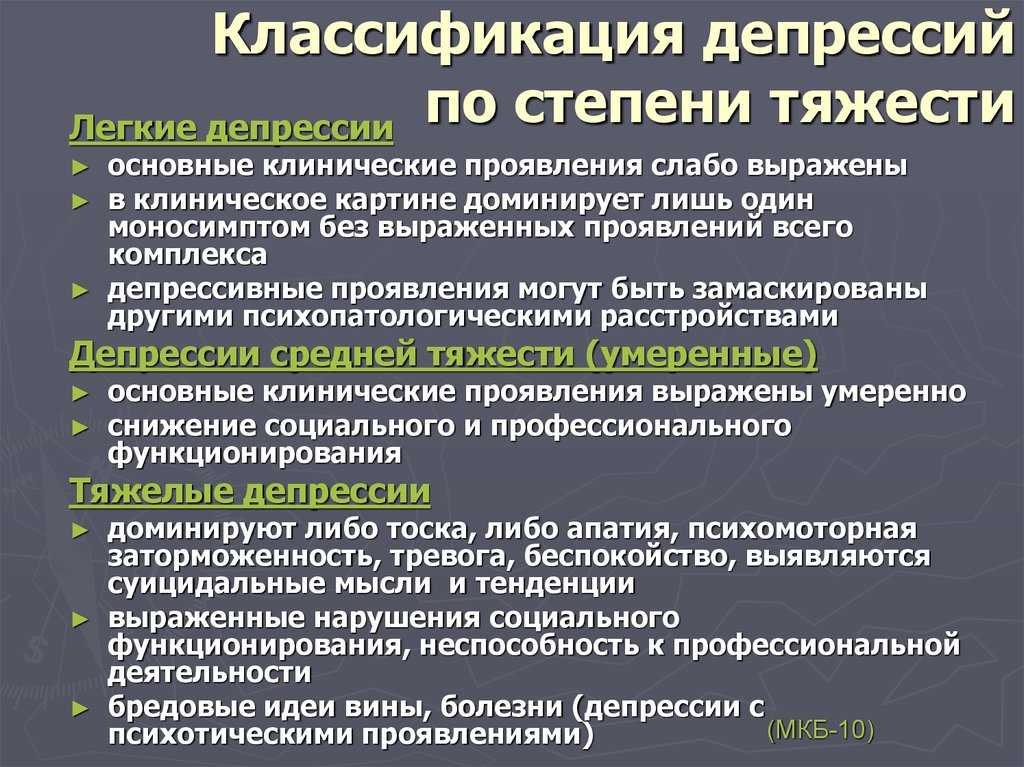 Identification with the object - (primary) narcissism - results in its introjection, thus explaining the sadistic vengeance against the object as part of the subject’s ego; one’s self-destruction often manifested as suicidal thoughts. Ambivalence plays a key role, as the subject struggles with his own survival and destruction.
Identification with the object - (primary) narcissism - results in its introjection, thus explaining the sadistic vengeance against the object as part of the subject’s ego; one’s self-destruction often manifested as suicidal thoughts. Ambivalence plays a key role, as the subject struggles with his own survival and destruction.
Klein later elucidated the importance of the establishment of an internal world in which the lost external object is “reinstated.” Thus, in melancholy, there is a regression to an earlier failure to integrate good and bad partial objects into whole objects in the inner world. The depressive individual believes himself omnipotently responsible for the loss, due to his inherent destructiveness, which has not been integrated with loving feelings. Klein argues that pining, mourning, guilt, reparation, possibly delusional thinking, omnipotence, denial, and idealization characterize depression.19
More recently, Luyten & Blatt15 commented on these works as “still clinically relevant” but “often over specified, lacking theoretical precision, and too broad to be empirically tested. ” However, these authors stated that unconscious motives and processes still play an important role in recent psychodynamic theories of depression.
” However, these authors stated that unconscious motives and processes still play an important role in recent psychodynamic theories of depression.
Evidence for psychotherapy as a treatment for depressive disorders
A meta-analysis of direct comparisons found psychotherapy about as effective as pharmacotherapies for depressive disorders.20 In another meta-analysis, Cuijpers et al.21 included 92 different randomized controlled trials (RCTs) and demonstrated the efficacy of psychotherapy in comparison with pharmacotherapy – equal in the short-term and superior in the long-term, regarding relapse prevention. Different forms of psychotherapy have been compared, with no clear differences observed or, when so, with certain methodological specificities pointed out.22 Nevertheless, the effectiveness of many well-recognized interventions has been regarded as possibly overestimated, considering that most evidence is based on symptom reduction.23 A comprehensive meta-analysis24 has highlighted the effectiveness of Interpersonal Psychotherapy (which has its structure and theoretical roots in PDP) in depression, as compared to other psychotherapies and vs.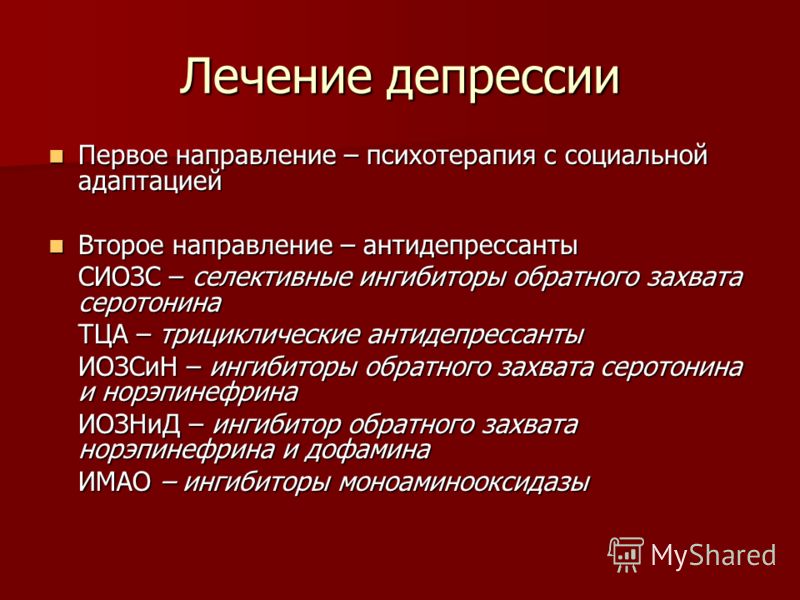 combined treatment, as well its role in preventing onset or relapse after successful treatment.
combined treatment, as well its role in preventing onset or relapse after successful treatment.
Extensive literature supports the efficacy of psychotherapy as an established treatment for MDD, stating its effectiveness and comparableness to that of antidepressant medications. The significance of these findings and possibility of publication bias have also been object of attention from the scientific community. A recent analysis stated an excess of significant findings relative to what would be expected for studies of psychotherapy’s effectiveness for MDD.25
On this subject, Driessen et al.26 found clear indications of study publication bias among U.S. National Institute of Health-funded clinical trials that examined the efficacy of psychological treatment for MDD, ascertained through direct empirical assessment. Through these data, the authors concluded that psychological treatment, like pharmacologic treatment, may not be as efficacious as the published literature would indicate.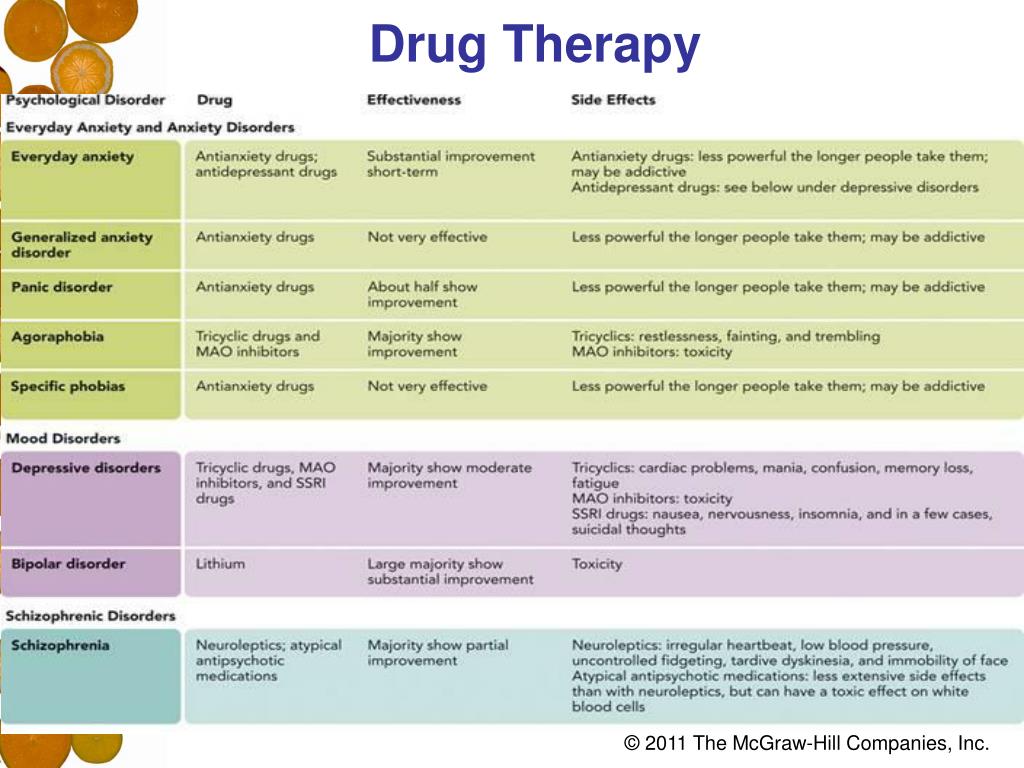
Cuijpers et al.27 published a meta-analysis on the effects of psychotherapies on remission, recovery, and improvement of MDD in adults. The response rate for the analyzed psychotherapies was 48% (vs. 19% in control conditions), and there was no significant difference between types of psychotherapy.
Evidence for psychodynamic psychotherapy as a treatment for depressive disorders
Shedler28 presented five independent meta-analyses showing that the benefits of PDP not only endure, but also increase with time (including after treatment end). Patients reported significant symptom reductions, which held up over time, and increased mental capacities, which allowed them to continue maturing over the years. Additionally, Shedler presented several studies demonstrating that it is the psychodynamic process that predicts successful outcome in cognitive therapy, rather than the pure cognitive aspects of treatment – i.e., non-psychodynamic psychotherapies may be effective because the more skilled practitioners utilize techniques that have long been central to psychodynamic theory and practice.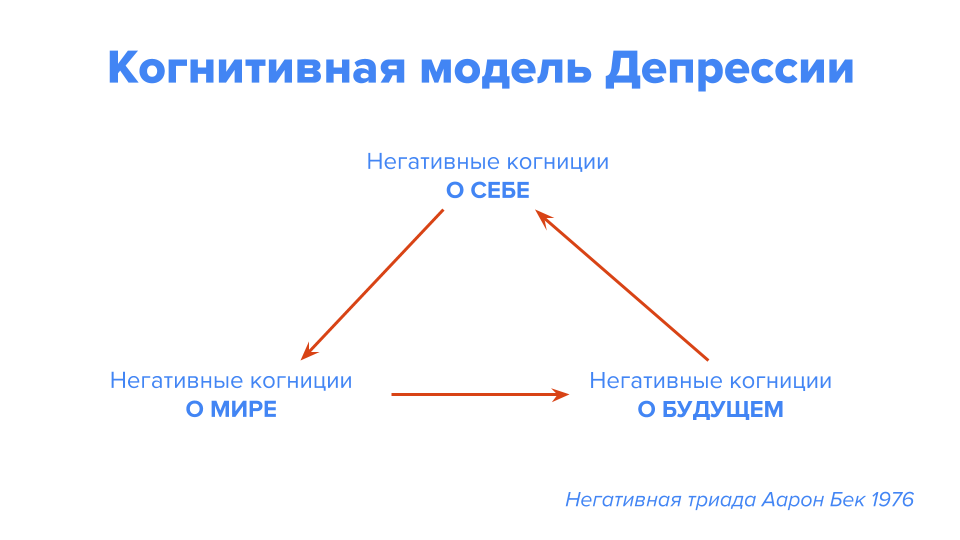
Leichsenring et al.22 conducted an empiric review of supported methods of PDP in depression and suggesting a unified protocol for the psychodynamic treatment of depressive disorders. The authors found a twofold risk for poor outcome in depression when patients were diagnosed with a comorbid personality disorder. However, several studies were found to have methodological limitations, such as taking a personality disorder diagnosis in account as a primary object of treatment, sample size differences, and divergent results, largely depending on the personality cluster identified. The findings of these authors contradict repeated claims that PDP is not empirically supported.
A subsequent systematic review by Leichsenring29 identified and included a total of 47 RCTs providing evidence for PDP in specific mental disorders; it stated the efficacy of PDP compared to cognitive-behavioral therapy (CBT) (but not to other forms of psychotherapy) in MDD, and concluded that several RCTs provide evidence for the efficacy of PDP in depressive disorders (including comparisons with control groups, waiting-list condition at the end of treatment, group therapy, pharmacotherapy, and brief supportive therapy).
Varying results have also been observed according to treatment duration – specifically, short-term (STPDP) vs. long-term psychodynamic psychotherapy (LTPDP) as applied in patients with depressive disorders. One recent meta-analysis30 evaluated the efficacy of a specific STPDP (experiential dynamic therapy) within multiple psychiatric disorders, and found the largest effect on depressive symptoms. A meta-analysis from the Cochrane Collaboration31 studied the effects of STPDP for common mental disorders across several studies, including 23 RCTs. It showed significantly greater improvement in the treatment groups as compared to controls, with most improvement maintained on medium- and long-term follow up.
Another meta-analysis by Leichsenring et al.32 examined the comparative efficacy of LTPDP in complex mental disorders in RCTs fulfilling specific inclusion criteria (therapy lasting for at least a year or 50 sessions; active comparison conditions; prospective design; reliable and valid outcome measures; treatments terminated).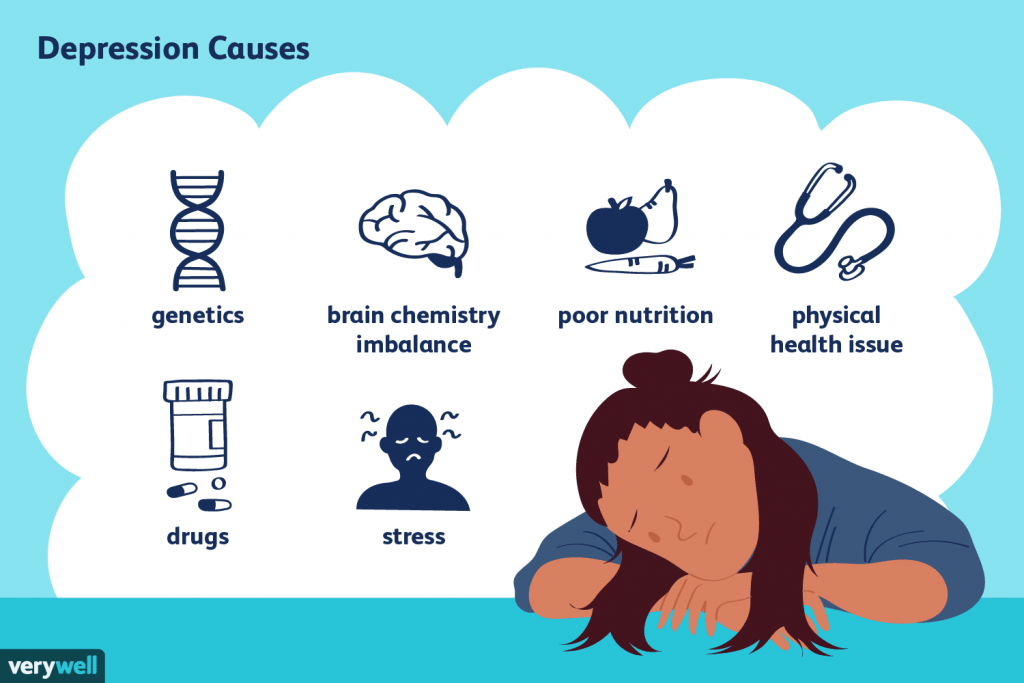 It concluded that LTPDP is superior to less intensive forms of psychotherapy in complex mental disorders.
It concluded that LTPDP is superior to less intensive forms of psychotherapy in complex mental disorders.
More recently, Driessen et al.33 published a meta-analysis of 54 studies highlighting STPDP outcomes in symptom reduction and function improvement during treatment. They found either maintained or further improved gains at follow-up, and stated that the efficacy of STPDP compared to control conditions and outcomes on depression did not differ from that of other psychotherapies.
A recent review34 provided evidence towards maintained effects with both modalities as a treatment option for depression, emphasizing their moderate (rather than large) effects. PDP is noted as a preferred alternative to pharmacotherapy in depressive disorders; nevertheless, the authors highlight the high frequency of studies involving psychotherapy in combination with medication – or adding to the effectiveness of medication. In comparison with CBT, PDP is described as neither largely nor reliably different. No single type of PDP was found particularly efficacious within its different forms. Regarding LTPDP, its cost-effectiveness and early stage are mentioned when describing its value, especially in more complex and chronic cases of depression.
No single type of PDP was found particularly efficacious within its different forms. Regarding LTPDP, its cost-effectiveness and early stage are mentioned when describing its value, especially in more complex and chronic cases of depression.
An extensive, growing body of literature confirms that the classical divergence in treatment approaches for depressive disorders is fading. Psychotherapy has been found as efficacious as pharmacotherapy, with different results regarding its superiority in short-term and long-term relapse prevention.20,23 Moreover, a systematic review has elucidated the potential benefits of a change in intervention design in depression, switching the paradigm from a symptom-oriented one to more rehabilitation- and functioning-oriented therapies.23 These results are in agreement with Westen et al,35 who presented evidence that treatments focusing on isolated symptoms or behaviors (rather than personality, emotional, and interpersonal patterns) are not effective in sustaining even narrowly defined changes.
The large number of publications in this topic has drawn the attention of the scientific community, prompting systematic analyses with increasing complexity and the creation of specific protocols for psychotherapeutic intervention, bearing in mind the importance of structured interventions by qualified clinical staff.
Although it would stray from the primary scope of this review, it is worth highlighting the growing number and relevance of published neuroscientific literature that reports neuroimaging and neurochemical changes exerted by psychotherapeutic interventions,9 specifically PDP.36
The effectiveness of PDP has been found difficult to isolate due to its limitations as a measurable intervention, which has led to the proposition of unified protocols both to facilitate training and to improve the status of evidence.22 The quality of PDP trials published from 1974 to 2010 was assessed in a review paper37 which concluded that the existing RCTs of PDP mostly show superiority of PDP to an inactive comparator. Studies concerning longer-term treatments are scarce but highly relevant, as they focus on important individual aspects like chronic mood problems, which often result from a combination of depression, anxiety, and significant personality and relational problems.15
Studies concerning longer-term treatments are scarce but highly relevant, as they focus on important individual aspects like chronic mood problems, which often result from a combination of depression, anxiety, and significant personality and relational problems.15
While these aspects are simple to clarify, few studies have taken them into account. Further RCTs could provide new evidence on the effectiveness of PDP, as well as facilitate its clear integration among the range of standard treatment options to consider for depressive disorders. One important related aspect refers to the training of future therapists in PDPs: institutes are mostly small and independent, and lack the necessary resources to conduct expensive or large-scale studies.
This narrative review presents certain limitations. Only recent published studies or systematic reviews were included. Due to practical reasons, only English-language publications were included, which may have left out important published findings. Publication bias may also be a factor, perhaps resulting in studies or systematic reviews that only showed positive or equal results for PDP treatments. However, we emphasize the importance of gathering and comparing recent findings and systematic reviews with classical published works in the field of PDP.
Publication bias may also be a factor, perhaps resulting in studies or systematic reviews that only showed positive or equal results for PDP treatments. However, we emphasize the importance of gathering and comparing recent findings and systematic reviews with classical published works in the field of PDP.
In conclusion, despite its controversial history, PDP’s influence in the psychiatric panorama is definitely increasing. The effectiveness of PDP has been demonstrated in various studies which have compared it with other treatment modalities. In recent years, the body of empirical evidence supporting said effectiveness has grown, and, more recently, meta-analyses have confirmed the role of PDP in the treatment of depressive disorders.
Many advances have been made in to enable high-quality scientific research in this complex, layered field. Nonetheless, contemporary authors continue to claim the importance of early conceptualizations of the psychodynamic perspective toward depression and depressive disorders.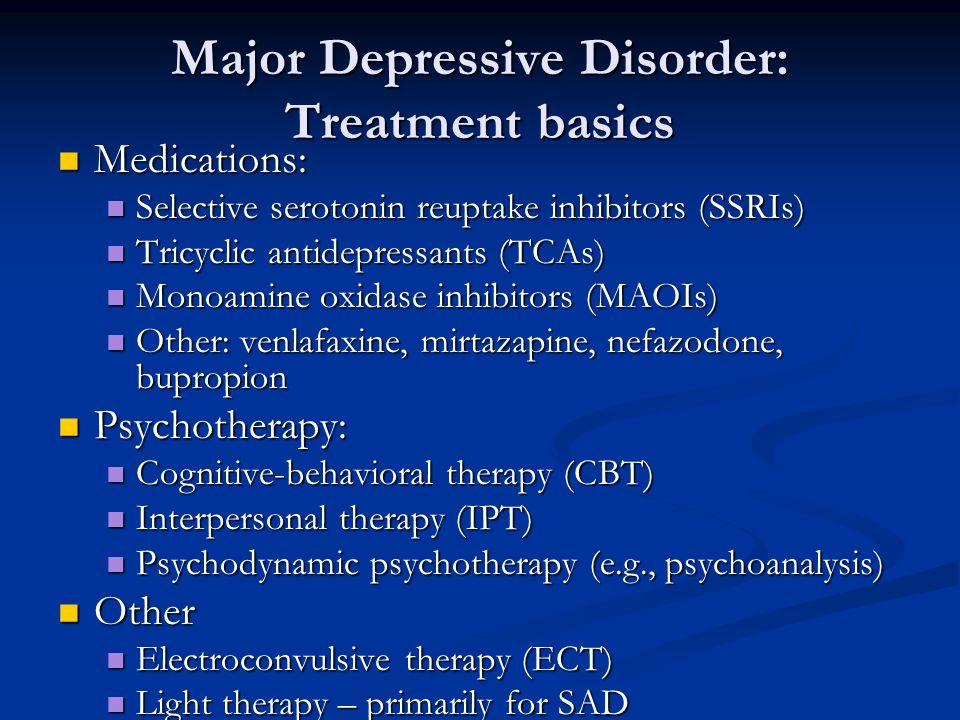
The authors report no conflicts of interest.
1. World Health Organization (WHO). The global burden of disease: 2004 update [Internet]. 2008 [cited 2017 Feb 21]. who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. [Google Scholar]
2. Ferrari AJ, Charlson FJ, Norman RE, Patten SB, Freedman G, Murray CJ, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013;10:e1001547. [PMC free article] [PubMed] [Google Scholar]
3. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PloS Med. 2006;3:e442. [PMC free article] [PubMed] [Google Scholar]
4. Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the world health surveys. Lancet. 2007;370:851–8. [PubMed] [Google Scholar]
5. Zilcha-Mano S, Dinger U, McCarthy KS, Barrett MS, Barber JP. Changes in well-being and quality of life in a randomized trial comparing dynamic psychotherapy and pharmacotherapy for major depressive disorder. J Affect Disord. 2014;152-154:538–42. [PMC free article] [PubMed] [Google Scholar]
Changes in well-being and quality of life in a randomized trial comparing dynamic psychotherapy and pharmacotherapy for major depressive disorder. J Affect Disord. 2014;152-154:538–42. [PMC free article] [PubMed] [Google Scholar]
6. American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington: American Psychiatric Publishing; 2013. [Google Scholar]
7. Sivertsen H, Bjørkløf GH, Engedal K, Selbæk G, Helvik AS. Depression and quality of life in older persons: a review. Dement Geriatr Cogn Disord. 2015;40:311–39. [PubMed] [Google Scholar]
8. Lemma A, Target M, Fonagy P. The development of a brief psychodynamic protocol for depression: dynamic interpersonal therapy (DIT) Psychoanal Psychother. 2010;24:329–46. [Google Scholar]
9. Prosser A, Bartosz H, Leucht S. Biological v. psychosocial treatments: a myth about pharmacotherapy v. psychotherapy. Br J Psychiatry. 2016;208:309–11. [PubMed] [Google Scholar]
10. American Psychiatric Association . Practice guideline for the treatment of major depressive disorder. 3rd ed. Washington: American Psychiatric Publishing; 2010. [Google Scholar]
American Psychiatric Association . Practice guideline for the treatment of major depressive disorder. 3rd ed. Washington: American Psychiatric Publishing; 2010. [Google Scholar]
11. National Collaborating Centre for Mental Health (UK), National Institute for Health and Care Excellence (NICE). Depression: the treatment and management of depression in adults (updated edition). Leicester: British Psychological Society; 2010. [Google Scholar]
12. Gabbard GO. Long-term psychodynamic psychotherapy: a basic text. 2nd ed. Washington: American Psychiatric Publishing; 2010. [Google Scholar]
13. Leichsenring F, Leweke F, Klein S, Steinert C. The empirical status of psychodynamic psychotherapy – an update: Bambi’s alive and kicking. Psychother Psychosom. 2015;84:129–48. [PubMed] [Google Scholar]
14. Wampold BE. How important are the common factors in psychotherapy? An update. World Psychiatry. 2015;14:270–7. [PMC free article] [PubMed] [Google Scholar]
15. Luyten P, Blatt SJ. Psychodynamic treatment of depression. Psychiatr Clin North Am. 2012;35:111–29. [PubMed] [Google Scholar]
Psychodynamic treatment of depression. Psychiatr Clin North Am. 2012;35:111–29. [PubMed] [Google Scholar]
16. Zuroff DC, Blatt SJ. The therapeutic relationship in the brief treatment of depression: contributions to clinical improvement and enhanced adaptive capacities. J Consult Clin Psychol. 2006;74:130–40. [PubMed] [Google Scholar]
17. Freud S. Mourning and melancholia, In. In: Dickson A, editor, editor. On metapsychology: the theory of psychoanalysis. London: Penguin Books; 1991. pp. 59–98. [Google Scholar]
18. Abraham K. A short study of the development of the libido, viewed in the light of mental disorders, In. In: Abraham K, editor. Selected papers on psychoanalysis. New York: Basic Books; 1954; 1924. pp. 418–501. [Google Scholar]
19. Klein M. Mourning and its relation to manic-depressive state’s, In. In: Klein M, editor. Love guilt and reparation. London: Vintage; 1998. pp. 344–70. [Google Scholar]
20. Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF.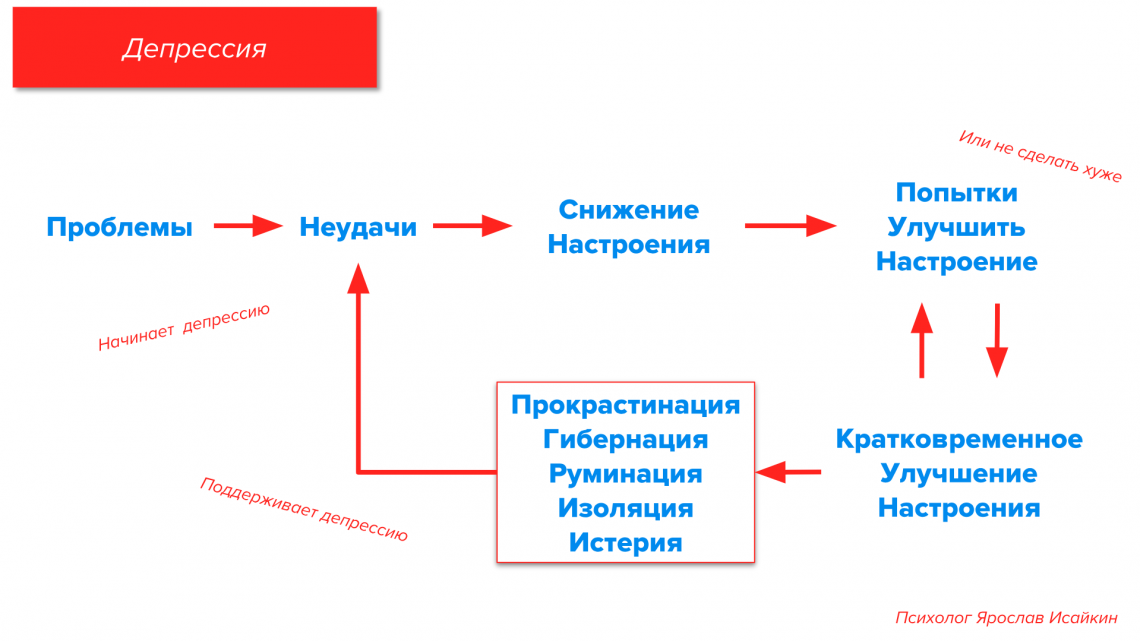 , 3rd The efficacy of psychotherapy and pharmacotherapy in treating depressive and anxiety disorders: a meta-analysis of direct comparisons. World Psychiatry. 2013;12:137–48. [PMC free article] [PubMed] [Google Scholar]
, 3rd The efficacy of psychotherapy and pharmacotherapy in treating depressive and anxiety disorders: a meta-analysis of direct comparisons. World Psychiatry. 2013;12:137–48. [PMC free article] [PubMed] [Google Scholar]
21. Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF., 3rd Adding psychotherapy to antidepressant medication in depression and anxiety disorders: a meta-analysis. World Psychiatry. 2014;13:56–67. [PMC free article] [PubMed] [Google Scholar]
22. Leichsenring F, Schauenburg H. Empirically supported methods of short-term psychodynamic therapy in depression – towards an evidence-based unified protocol. J Affect Disord. 2014;169:128–43. [PubMed] [Google Scholar]
23. Kamenov K, Cabello M, Coenen M, Ayuso-Mateos JL. How much do we know about the functional effectiveness of interventions for depression? A systematic review. J Affect Disord. 2015;188:89–96. [PubMed] [Google Scholar]
24. Cuijpers P, Donker T, Weissman MM, Ravitz P, Cristea IA. Interpersonal psychotherapy for mental health problems: a comprehensive meta-analysis. Am J Psychiatry. 2016;173:680–7. [PubMed] [Google Scholar]
Interpersonal psychotherapy for mental health problems: a comprehensive meta-analysis. Am J Psychiatry. 2016;173:680–7. [PubMed] [Google Scholar]
25. Flint J, Cuijpers P, Horder J, Koole SL, Munafò MR. Is there an excess of significant findings in published studies of psychotherapy for depression? Psychol Med. 2015;45:439–46. [PMC free article] [PubMed] [Google Scholar]
26. Driessen E, Hollon SD, Bockting CL, Cuijpers P, Turner EH. Does publication bias inflate the apparent efficacy of psychological treatment for major depressive disorder? a systematic review and meta-analysis of US national institutes of health-funded trials. PLoS One. 2015;10:e0137864. [PMC free article] [PubMed] [Google Scholar]
27. Cuijpers P, Karyotaki E, Weitz E, Andersson G, Hollon SD, van Straten A. The effects of psychotherapies for major depression in adults on remission, recovery and improvement: a meta-analysis. J Affect Disord. 2014;159:118–26. [PubMed] [Google Scholar]
28. Shedler J. The efficacy of psychodynamic psychotherapy. Am Psychol. 2010;65:98–109. [PubMed] [Google Scholar]
The efficacy of psychodynamic psychotherapy. Am Psychol. 2010;65:98–109. [PubMed] [Google Scholar]
29. Leichsenring F, Klein S. Evidence for psychodynamic psychotherapy in specific mental disorders: a systematic review. Psychoanal Psychother. 2014;28:4–32. [Google Scholar]
30. Lilliengren P, Johansson R, Lindqvist K, Mechler J, Andersson G. Efficacy of experiential dynamic therapy for psychiatric conditions: a meta-analysis of randomized controlled trials. Psychotherapy (Chic). 2016;53:90–104. [PubMed] [Google Scholar]
31. Abbass AA, Hancock JT, Henderson J, Kisely S. Short-term psychodynamic psychotherapies for common mental disorders. Cochrane Database Syst Rev. 2006;4:CD004687. [PubMed] [Google Scholar]
32. Leichsenring F, Rabung S. Long-term psychodynamic psychotherapy in complex mental disorders: update of a meta-analysis. Br J Psychiatry. 2011;199:15–22. [PubMed] [Google Scholar]
33. Driessen E, Hegelmaier LM, Abbass AA, Barber JP, Dekker JJ, Van HL, et al. The efficacy of short-term psychodynamic psychotherapy for depression: a meta-analysis update. Clin Psychol Rev. 2015;42:1–15. [PubMed] [Google Scholar]
The efficacy of short-term psychodynamic psychotherapy for depression: a meta-analysis update. Clin Psychol Rev. 2015;42:1–15. [PubMed] [Google Scholar]
34. Fonagy P. The effectiveness of psychodynamic psychotherapies: an update. World Psychiatry. 2015;14:137–50. [PMC free article] [PubMed] [Google Scholar]
35. Westen D, Novotny CM, Thompson-Brenner H. The empirical status of empirically supported psychotherapies: assumptions, findings, and reporting in controlled clinical trials. Psychol Bull. 2004;130:631–63. [PubMed] [Google Scholar]
36. Wiswede D, Taubner S, Buchheim A, Münte TF, Stasch M, Cierpka M, et al. Tracking functional brain changes in patients with depression under psychodynamic psychotherapy using individualized stimuli. PLoS One. 2014;9:e109037. [PMC free article] [PubMed] [Google Scholar]
37. Gerber AJ, Kocsis JH, Milrod BL, Roose SP, Barber JP, Thase ME, et al. A quality-based review of randomized controlled trials of psychodynamic psychotherapy.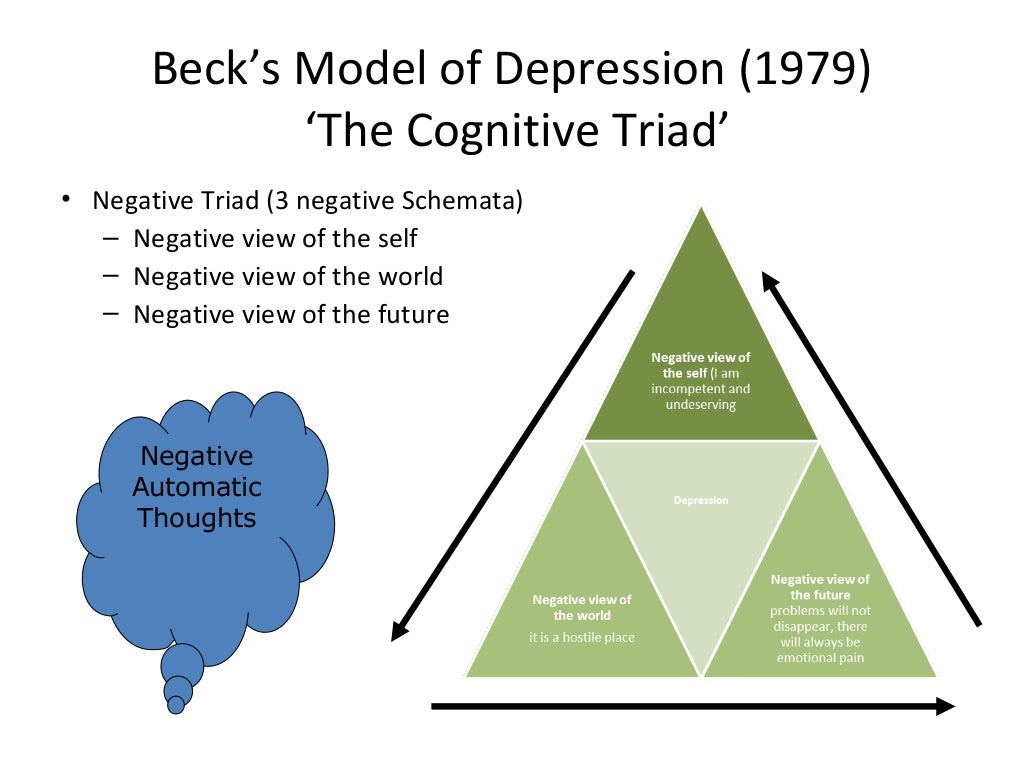 Am J Psychiatry. 2011;168:19–28. [PubMed] [Google Scholar]
Am J Psychiatry. 2011;168:19–28. [PubMed] [Google Scholar]
Psychological treatment - iFightDepression [EN]
Like drugs, psychological help is the other main treatment for depression.
Psychotherapy is the most common form of psychological treatment. Psychotherapy includes two main features: conversation and cooperation. There are several different types of proven psychotherapy, including cognitive behavioral therapy, psychodynamic psychotherapy, supportive counseling, and Mindfulness Practices.
Cognitive Behavioral Therapy
Cognitive Behavioral Therapy (CBT) is a type of behavioral therapy that has been shown to be effective in treating depression. It is based on the idea that negative feelings arise from useless thoughts and can lead to negative behavior such as a "vicious circle". CBT can start with exercises to learn how to structure your day and increase your daily activity. Later, CBT teaches how to identify useless thoughts to challenge them and replace them with ones that are more beneficial.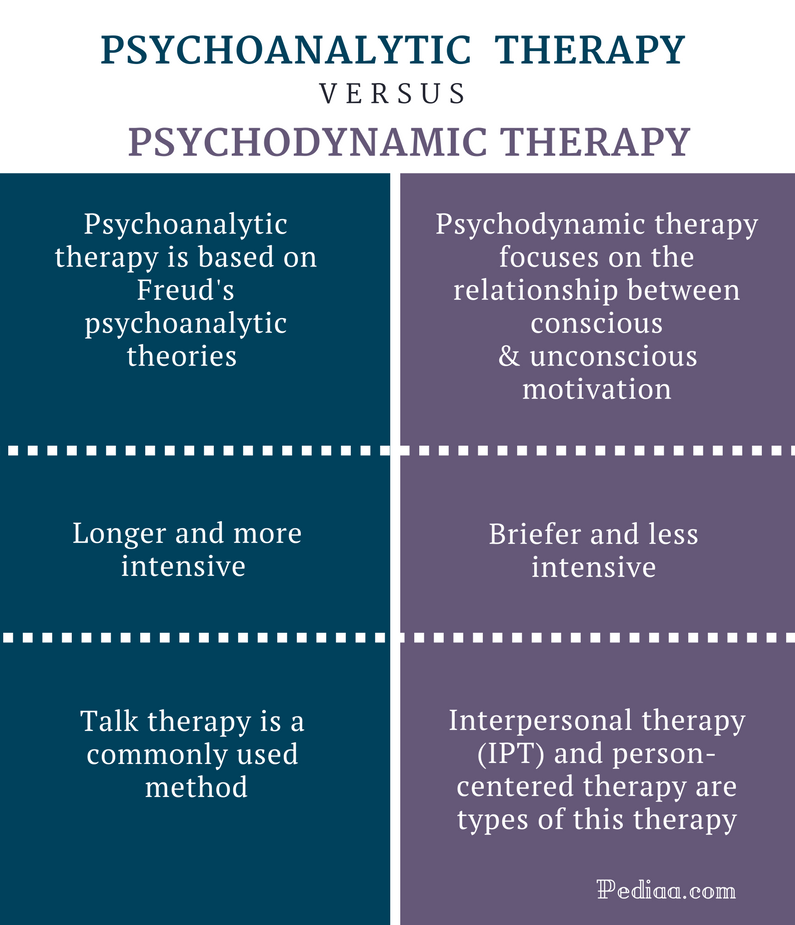
Another important part of therapy is education to learn more about the disorder (psychoeducation). Such changes have an indirect positive effect on mood and make it easier to manage external life events. In CBT, the client and therapist actively work together and learn from each other. As a rule, there are about 1-2 sessions per week. In general, the treatment takes 25 to 80 sessions maximum (approximately 3 months to a year).
Psychodynamic psychotherapy
Psychodynamic psychotherapy is based on knowledge from psychoanalysis. They are similar to similar assumptions about the causes of mental disorders, namely that they are the result of emotional problems in the subconscious. Unlike psychoanalysis, this type of psychotherapy preferably deals with ongoing internal conflicts and with the client's relationships with other people. In therapy, the client is in a seated position and both therapist and client have eye contact. The therapist's approach can range from being passive to participating and providing structuring. Usually there are one or two classes per week. In general, therapy can be either brief from 16-24 sessions or longer, taking 50-100 sessions, or even more.
Usually there are one or two classes per week. In general, therapy can be either brief from 16-24 sessions or longer, taking 50-100 sessions, or even more.
Supportive counseling .
Some psychotherapists use a supportive, non-directive counseling approach, either alone or in combination with other therapy approaches. Supportive counseling is also regularly used by other health professionals and volunteers. This type of counseling is used to help create a favorable environment for the client to solve their problems. This is achieved by the therapist listening in a caring and respectful manner to the person and encouraging them to talk about their situation in order to find possible solutions. This type of counseling can help calm and reassure the client, but its long-term effectiveness in treating depression has not yet been proven.
Mindfulness (Mindfulness) Practices
While CBT and psychodynamic therapy aim to change patterns associated with depression, Mindfulness (Mindfulness) Practices help a person develop greater powers of observation and take a non-reactive approach to their thoughts and feelings. Examples of such approaches include Mindfulness Practice-based Cognitive Psychotherapy and the Mindfulness Practice-based Stress Reduction Program. Like CBT, Mindfulness Practices teaches the automatic nature of negative thoughts and feelings in depression and the need to seek to interrupt them. Unlike CBT, the focus is on developing skills to endure bad thoughts and feelings that come and go without reacting to them. Cognitive psychotherapy based on Mindfulness Practices is especially good for people who suffer from recurrent depression.
Examples of such approaches include Mindfulness Practice-based Cognitive Psychotherapy and the Mindfulness Practice-based Stress Reduction Program. Like CBT, Mindfulness Practices teaches the automatic nature of negative thoughts and feelings in depression and the need to seek to interrupt them. Unlike CBT, the focus is on developing skills to endure bad thoughts and feelings that come and go without reacting to them. Cognitive psychotherapy based on Mindfulness Practices is especially good for people who suffer from recurrent depression.
Activating behavioral therapy for depression in adults
Review question
In this Cochrane review, we wanted to know how effective activating behavioral therapy is for depression in adults.
Why is this important?
Depression is a common mental health problem that can cause persistent feelings of sadness and loss of interest in people, activities and things that were once enjoyable. A person with depression may feel tearful, irritable, or tired most of the time, and may have trouble sleeping, concentrating, and remembering. These and other symptoms can make daily life difficult.
A person with depression may feel tearful, irritable, or tired most of the time, and may have trouble sleeping, concentrating, and remembering. These and other symptoms can make daily life difficult.
Treatment for depression includes medication (antidepressants) and psychotherapy (talking therapy). Behavioral activation is a type of psychological therapy that encourages a person to develop or return to activities that are meaningful to him. Psychotherapy included scheduling activities and behavior monitoring, as well as considering specific situations in which changing these behaviors and activities might be beneficial. The therapist may provide assistance in person, over the phone, or online, usually over several sessions.
It is important to know whether behavioral activation can be an effective and acceptable treatment for people with depression.
What We Did
In January 2020, we searched for studies on behavioral activating psychotherapy for depression in adults (over 18 years of age). We looked for randomized controlled trials in which treatments were assigned randomly to participants; these studies provide the most reliable evidence.
We looked for randomized controlled trials in which treatments were assigned randomly to participants; these studies provide the most reliable evidence.
We included 53 studies with 5495 participants. Studies have compared behavioral activation with no treatment, standard or usual care, sham treatment (placebo), medication, being on a waiting list for treatment, or other types of psychotherapy (cognitive behavioral therapy (CBT), third wave CBT, humanistic therapy, psychodynamic therapy). and integrative therapy).
Studies conducted in 14 countries; most of them are in the USA (27 studies). Most studies lasted between four and 16 weeks.
As a result, we focused on how well the treatment works and whether it is acceptable to the participants. How well a treatment worked (effectiveness) was measured by the number of people who responded well to treatment or no longer met criteria for depression at the end of treatment. Eligibility was measured by counting how many people dropped out of the study.
What did we find?
Behavioral activation may treat depression better than conventional care. We were not sure whether behavioral activation worked better than medication or being on a waiting list, and we found no evidence for this outcome when comparing behavioral activation to no treatment or placebo treatment.
We found no difference between behavioral activation and CBT in the treatment of depression. Although we did not find sufficient evidence to compare behavioral activation with other types of psychotherapy, it may work better than humanistic therapy, and we found no difference between behavioral activation and third wave CBT or psychodynamic therapy. There was no evidence available comparing behavioral activation with integrative therapy.
Behavioral activation is probably less acceptable to people than conventional help. We found no difference in acceptability of behavioral activation compared with being on a waiting list, no treatment, antidepressants, or placebo. We also found no difference in acceptability between behavioral activation and other psychotherapies studied (CBT, third wave CBT, humanistic therapy, integrative therapy). To compare behavioral activation with psychodynamic therapy, we did not find any evidence for the acceptability of the treatment.
We also found no difference in acceptability between behavioral activation and other psychotherapies studied (CBT, third wave CBT, humanistic therapy, integrative therapy). To compare behavioral activation with psychodynamic therapy, we did not find any evidence for the acceptability of the treatment.
Terminals
Behavioral activation may be an effective and acceptable treatment for depression in adults. Patients with depression who are prescribed this psychotherapy option will have more choice of treatment, and different formats and types of care can be explored to meet the demand for mental health support. Our confidence in these findings is limited due to concerns about the certainty of the evidence.
Most of the results were short term, which means that we cannot be sure that behavioral activation will be beneficial for people with depression in the long term.
Certainty of evidence
Our confidence in the evidence is generally low to moderate.