Psychiatry cheat sheet
Mental Health ICD-10 Cheat Sheet – My Clients Plus
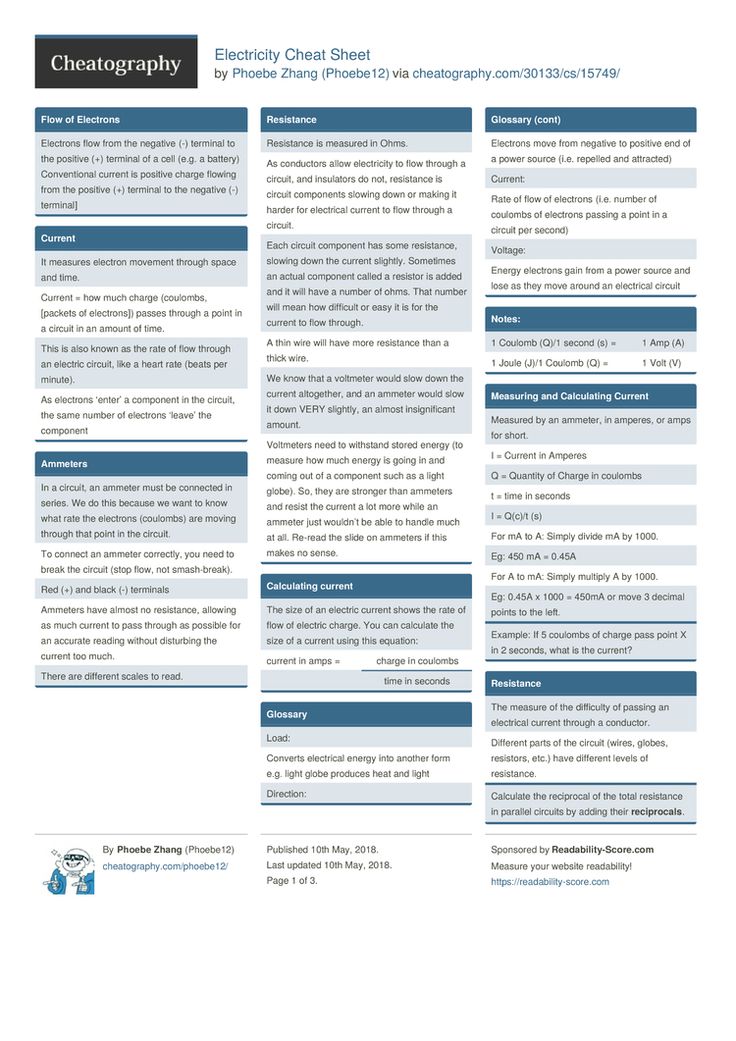
As a therapist, you may find the billing and claims submission process cumbersome. And for good reason: billing is complex due to the requirements of insurance companies that want detailed justification for the services you’re providing. In addition to the CPT services codes that you’ll bill for, you must also include ICD-10 diagnoses codes in your claims. In this post, we explore a bit of background on the ICD-10 and offer a cheat sheet for mental health ICD-10 codes that you can use as a reference.
What is the ICD-10 Exactly?
Before we dive into the specifics of how the ICD-10 is laid out and share the codes applicable to mental health, here’s what you should know about the code set to give you a broader understanding.
“ICD” stands for International Classification of Disease and is the title of the classification tool for medical diagnoses compiled by the World Health Organization (WHO). It was originally designed to help medical professionals worldwide communicate with one another about various diseases in an effort to cooperate in their efforts, particularly in cases of epidemics and pandemics. Now it’s used for a variety of purposes, including insurance billing.
The WHO updates the ICD periodically and the current version is the ICD-10. This is a worldwide reference, so the U.S. has developed its own clinical modification (ICD-10-CM) for use in this country. While the ICD-10-CM is based on the WHO’s ICD-10 set, there are a few unique differences. (Typically, when people in the U.S. refer to the ICD-10, they’re talking about the ICD-10-CM.) The U.S. version has over 70,000 different codes that describe diseases, signs and symptoms, abnormal findings, complaints, and external causes of injury or diseases. These codes are used in the healthcare claims submission process for purposes of reporting and reimbursement — they help provide justification for providing a client with the services you did.
How the ICD-10 Mental Health Codes Are Organized: G, Z, and F Codes
The mental health ICD-10 codes are organized into three primary categories: G, Z, and F.
The G codes comprise diseases of the nervous system. The Z codes describe situations where the client doesn’t have a specific disorder but services are required anyway, such as if a client has a personal history of psychological trauma or if an authority body has requested a general psychiatric examination for someone. The F codes make up the majority of the mental health ICD-10 codes.
The Z codes describe situations where the client doesn’t have a specific disorder but services are required anyway, such as if a client has a personal history of psychological trauma or if an authority body has requested a general psychiatric examination for someone. The F codes make up the majority of the mental health ICD-10 codes.
ICD-10 Codes for Mental Health Cheat Sheet
While there are many codes that may conceivably be used in healthcare situations, you won’t encounter all of them in your therapy practice. You’re unlikely to encounter the G codes since these are typically dealt with in a medical setting, but we’ve included the ones in this cheat sheet that you may come across. The list also includes the Z codes you’re likely to encounter. Since the F category is the most robust, we’ve included the most common F codes in this list, although you may encounter others that are less common. You can find a complete list of the major F subcategories here.
Common G Codes
- G20 (Parkinson’s disease)
- G30 (Alzheimer’s disease)
- G90 (disorders of autonomic nervous system)
Common Z Codes
- Z00.
 4 (general psychiatric examination, not elsewhere classified)
4 (general psychiatric examination, not elsewhere classified) - Z03.2 (observation for suspected mental and behavioral disorders)
- Z04.6 (general psychiatric examination, requested by authority)
- Z09.3 (follow-up examination after psychotherapy)
- Z13.3 (special screening examination for mental and behavioral disorders)
- Z13.4 (special screening examination for certain developmental disorders in childhood)
- Z50.4 (psychotherapy, not elsewhere classified)
- Z54.3 (convalescence following psychotherapy)
- Z63.0 (problems in relationship with spouse or partner)
- Z71.1 (person with feared complaint in whom no diagnosis is made)
- Z71.9 (counseling, unspecified)
- Z81.8 (family history of other mental and behavioral disorders)
- Z91.4 (personal history of psychological trauma, not elsewhere classified)
Common F Codes
- F41.1 (generalized anxiety disorder)
- F43.23 (adjustment disorder with mixed anxiety and depressed mood)
- F43.
 22 (adjustment disorder with anxiety)
22 (adjustment disorder with anxiety) - F33.1 (major depressive disorder, recurrent, moderate)
- F43.20 (adjustment disorder, unspecified)
- F41.9 (anxiety disorder, unspecified)
- F43.21 (adjustment disorder with depressed mood)
- F43.12 (post-traumatic stress disorder, chronic)
- F34.1 (dysthymic disorder)
- F43.10 (post-traumatic stress disorder, unspecified)
- F32.1 (major depressive disorder, single episode, moderate)
- F33.0 (major depressive disorder, recurrent, mild)
- F32.9 (major depressive disorder, single episode, unspecified)
- F90.2 (attention-deficit hyperactivity disorder, combined type)
- F60.9 (personality disorder, unspecified)
- F40.228 (other natural environment type phobia)
- F43.25 (adjustment disorder w mixed disturb of emotions and conduct)
- F06.1 (catatonic disorder due to known physiological condition)
- F33.2 (major depressive disorder, recurrent severe without psychotic features)
- F41.
 0 (panic disorder without agoraphobia)
0 (panic disorder without agoraphobia) - F90.0 (attention-deficit hyperactivity disorder, predominantly inattentive type)
- F32.0 (major depressive disorder, single episode, mild)
- F42.2 (mixed obsessional thoughts and acts)
- F84.0 (childhood autism)
Use as a Reference, But Understand the Nuances of the Codes
It’s important to note that you shouldn’t rely on the short descriptions of the codes only. Payers can be very particular when it comes to the codes they’re looking for to accompany specific services, and you’ll want to make sure you’re using the right ones. This is especially important as occasionally a therapist will use a code or set of codes that have a higher pay rate than the one they should be using (this practice is called upcoding or unbundling), and payers see this as abuse or fraud. However, with an understanding of the details of each diagnosis, this cheat sheet will serve as a reminder to jog your memory.
Mental Status Exam Cheat Sheet
A mental status exam is an assessment of a patient's cognitive and behavioral functioning. It’s based on the clinician’s observations and the client's subjective descriptions. You might think of a mental status exam as a psychiatrist’s version of a physical exam. Behavioral health professionals use mental status exams to create a picture of how a person looks in the present moment — not all of the time.
It’s based on the clinician’s observations and the client's subjective descriptions. You might think of a mental status exam as a psychiatrist’s version of a physical exam. Behavioral health professionals use mental status exams to create a picture of how a person looks in the present moment — not all of the time.
- What Are the Components of a Mental Status Exam?
- Why Are Mental Status Exams Important?
- When Are Mental Status Exams Performed?
- Who Uses Mental Status Exams?
- How Do I Write a Mental Status Exam?
- Mental Status Exam Checklist
- Mental Status Exam Example
- Claim Your Free Trial of ICANotes
What Are the Components of a Mental Status Exam?
In general, the components of a mental status exam include descriptions of the following:
- Appearance
- General behavior
- Speech and language
- Emotions
- Thought and perception
- Cognition
The exam may also include cognitive testing, depending on a client’s needs.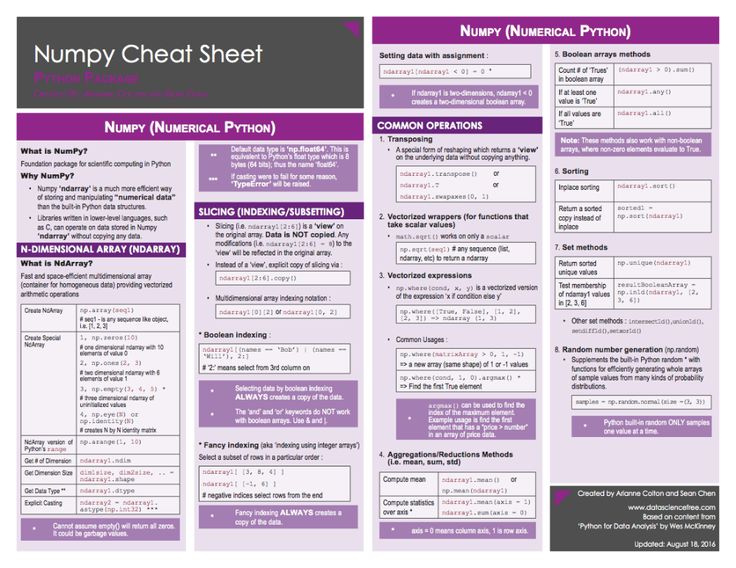
Why Are Mental Status Exams Important?
In combination with family and personal histories, the mental status exam forms the foundation for a psychiatric diagnosis.Clinicians can also use mental status exams for the following reasons:
- To determine if certain issues are improving or getting worse
- To identify areas that need attention from a specialist
- To offer a snapshot of a client at a specific point in time and provide that information to another provider
When Are Mental Status Exams Performed?
Mental status exams are often performed during the first one or two sessions with a client as part of the initial assessment and when reassessing their symptoms. It should be performed in person and not over the phone due to its visual elements. Mental status exams are especially useful in helping clinicians differentiate between various psychiatric and neurological disorders.
Typically, these exams are used for patients who have chronic, severe, or acute symptoms. A mental status exam aims to capture dysfunction, though you can still use them to confirm ordinary function for clients.
A mental status exam aims to capture dysfunction, though you can still use them to confirm ordinary function for clients.
As a behavioral health professional, you may choose to complete regular mental status exams to identify progress or on an as-needed basis throughout the treatment process. Completing a mental status exam at the end of treatment can highlight the differences in a client's presentation and illustrate their growth.
Who Uses Mental Status Exams?
Although mental status exams have been an assessment tool mainly used in clinical psychology, psychiatry, and social work to examine patients with an altered mental status or evolving impairment of cognition, counselors and therapists can also use this type of exam as an informal way to gain information about a client’s cognitive and behavioral functioning. The counselor's findings can help them diagnose and treat a mental health disorder. Mental status exams also provide an excellent source of documentation to support a diagnosis.
How Do I Write a Mental Status Exam?
In private practice, you have the flexibility to create the sections you want to include in your mental status exam. When you are writing your mental status exam, review the typical sections, and identify which ones you believe will be useful to document during your intake assessments with clients. Keep in mind that some sections may be more or less relevant for specific clients.
To determine which portions to include in your mental status exam, consider your current clients. Would this apply to at least half of them? If so, it will likely be useful for you. If not, maybe you don't need to include it every time, and you can add it whenever necessary. You may also want to have an "other" section for topics that may come up during a mental status exam but do not fit in already established sections.
Mental Status Exam Checklist
To help you use a mental status exam as an assessment tool, we've created a cheat sheet. The following checklist is meant to be easy to read, so you can use it as a quick reference. Although you can customize a mental status exam to suit each client, you’ll generally want to focus on the categories in this checklist:
The following checklist is meant to be easy to read, so you can use it as a quick reference. Although you can customize a mental status exam to suit each client, you’ll generally want to focus on the categories in this checklist:
1. Appearance
Appearance includes your observations of how a client looks initially and throughout the assessment. A client's appearance gives you an idea of their functioning level, their history, and symptoms they're experiencing. Always look for signs of self-neglect and note anything unusual.
Hygiene and Grooming
Would you describe your client's hygiene and grooming as:
- Clean
- Neat
- Shaven
- Body odor
- Disheveled
Dress
Is your client's clothing:
- Casual
- Immaculate
- Neat
- Business
- Fashionable
- Bizarre
- Inappropriate
- Dirty
- Stained
- Ragged
Makeup
Is your client's makeup:
- Appropriate
- Garish
- Bizarre
- No makeup
Distinguishing Features
Does your client have any distinguishing features, such as:
- Tattoos
- Piercings
- Scars
Apparent Age
Does your client appear:
- Older than their stated age
- Younger than their stated age
Habitus
Is your client's habitus:
- Normal
- Underweight
- Overweight
- Obese
Facial Expressions
Does your client appear:
- Calm
- Sad
- Anxious
- Disgusted
- Angry
- Perplexed
2.
 General Behavior
General BehaviorDescribe how your client moves and behaves physically during the assessment. Always note if they are being hostile, uncooperative or have inappropriate impulses.
Eye Contact
Isyour client's eye contact:
- Appropriate
- Decreased
- Heightened
- Avoidant
Motor Activity
Does your client display:
- Normal activity
- Decreased activity
- Restlessness
- Tension
- Agitation
Gait
Does your client:
- Seem unsteady
- Limp
- Shuffle
- Use a cane, crutches or another device
Orofacial Dyskinesia
Does your client display unusual movements in the jaw, face or tongue, such as:
- Grimacing
- Tongue writhing
- Lip smacking
- Lip pursing
- Chewing
Cooperativeness and Attitude
Doesyour client exhibit an appropriate level of cooperation, or are they:
- Evasive
- Guarded
- Playful
- Ingratiating
- Passive
- Sullen
- Withdrawn
- Manipulative
- Demanding
- Hostile
- Overly friendly
- Relaxed
- Open
- Shy
- Candid
- Suspicious
Movements
Does your client display any unusual or repetitive movements, such as:
- Tics
- Twitches
- Tremor
- Mannerisms
- Stereotypies
- Posturing
3.
 Speech and Language
Speech and LanguageConsider how your client speaks and uses language. The amount a client speaks and how they talk can indicate a mental health issue such as depression or anxiety or a neurocognitive disorder.
General
Does your client speak clearly or have an:
- Accent
- Stutter
- Lisp
Rate
Is your client's rate of speech:
- Normal
- Slow
- Fast
- Delayed onset
Rhythm
Is your client's speech:
- Articulate
- Slurred
- Monotone
- Dysarthric
Volume
Is your client's speech:
- Soft
- Loud
- Mute
Content
Is your client:
- Loquacious
- Fluent
- Impoverished
4. Emotions
Try to determine your client's emotional state by asking them how they feel and observing their facial expressions and body language.
Mood
Does your client say they feel:
- Depressed
- Sad
- Angry
- Irritable
- Good
- Fantastic
Affect
Does your client seem to be:
- Euthymic
- Depressed
- Irritable
- Angry
- Elated
- Euphoric
- Anxious
Range
Is your client's affect range:
- Broad: The client shows a normal range of emotions.
- Restricted: Theclient seems limited in expressing emotions.
- Flat: The client does not show any change in mood.
- Labile: The client's mood changes rapidly.
- Anhedonic: The client seems incapable of a pleasurable response.
Congruency
Is your client's affect:
- Congruent to their mood
- Incongruent to their mood
5. Thought and Perception
Consider how your client's thoughts flow and connect and whether your client has a normal, linear thought process or if they go off-topic or make disorganized associations. Also, listen to what your client focuses on and find out if they're experiencing hallucinations. Always note hallucinations or the presence of delusions, and take appropriate action if a client expresses plans to carry out suicidal or homicidal ideation.
Thought Process
Would you describe your client's thought process as:
- Goal-directed: The client answers your questions and does not move onto other related topics.
- Impoverished: The client displays slow thinking and does not share many ideas.
- Rapid: The client expresses racing thoughts and rapid thinking.
- Illogical: The client does not make sense when they speak.
- Incoherent: The client's speech is disorganized, and there is no meaning to what they're saying.
- Distractible: The client cannot stay focused.
- Blocking: The client's thoughts are interrupted.
- Circumstantial: The client provides unnecessary detail but gets to the point eventually.
- Perseverative: The client shows a repetition of words, ideas or phrases.
- Tangential: The client moves from one related thought to the next but never reaches the point.
- Loose: The client shifts illogically between unrelated topics.
- Flight of ideas: The client quickly jumps from one idea to the next.
- Word salad: The client speaks words randomly.
Thought Content
Do your client's thoughts consist of:
- Suicidal ideation
- Homicidal ideation
- Grandiose, somatic, paranoid or other delusions
- Distortions
- Obsessions
- Worries
- Compulsions
- Phobias
- Ruminations
Perception
Is your client experiencing:
- No hallucinations
- Auditory hallucinations
- Visual hallucinations
- Tactile hallucinations
- Olfactory hallucinations
- Illusions
- Derealization, or feeling detached from the surroundings
- Depersonalization, or feeling separated from him- or herself
6. Cognition
When evaluating a client's cognition, clinicians commonly assess the person's alertness or level of consciousness, orientation, attention, concentration and memory. If your client shows symptoms of a neurocognitive disorder, consider using additional tools such as the Mini-Mental State Examination or the Montreal Cognitive Assessment.
Alertness
Is your client:
- Alert
- Lethargic
- Obtunded
- In a stupor
- Comatose
Orientation
Does your client know:
- Their name
- Their current location
- The date
- The time
Memory
To test your client's memory, you might ask them to do the following:
- Repeat three words immediately and again in five minutes.
- Sign their name while answering unrelated questions.
- Tell you their birthday, where they were born and their parents' names.
Does your client display:
- No impairment
- Short-term impairment
- Long-term impairment
Attention
Does your client's attention seem:
- Normal
- Distracted
Insight
Describe your client's insight or their awareness of their situation or condition. Start by answering the following questions:
- How well does your client understand the reasons for their behavior?
- How well does your client appreciate how they contribute to a problem?
- Does your client recognize or acknowledge the severity of an issue?
- What do they perceive is the best way to address a problem?
Is your client's insight:
- Good
- Fair
- Poor
Judgment
Consider if your client anticipates the consequences of their behavior and makes decisions to safeguard their well-being and that of others. Is their judgment:
Is their judgment:
- Good
- Fair
- Poor
Impulse Control
Does your client show:
- Normal impulse control
- Impaired impulse control
Motivation
Would you describe your client's motivation level as:
- Good
- Fair
- Poor
Reliability
Consider your client's reliability and accuracy as they share details about their situation. Do you consider your client to be:
- Reliable
- Unreliable
7. Environment
If part of your mental status exam includes assessing the client's living environment, you may want to describe their surroundings. Ask yourself the following:
- Have they made odd decisions, such as blocking doors or windows with furniture?
- Are there unusual decorations or wires that lead nowhere?
- Are they using any household objects inappropriately?
- Is their home extremely cluttered or dirty?
- Do they collect junk or garbage?
Mental Status Exam Example
The following is a brief example of a mental status exam:
- Appearance: The client is slouched and disheveled.
- General behavior:The client is uncooperative and has poor eye contact.
- Speech:The client speaks fast and soft.
- Emotions:The client states he feels "depressed and anxious."
- Thinking process: The client is incoherent and disorganized.
- Cognition: The client is focused and alert, and he performed well on working memory tests.
- Insight: The client displays poor insight.
- Judgment: The client shows fair judgment.
- Reliability: The client is unreliable because he gave false impressions of himself.
Claim Your Free Trial of ICANotes
At ICANotes, we offer behavioral health electronic health record (EHR) software to reduce documentation time and improve compliance. Our EHR is the most clinically robust software for behavioral health professionals and comes with preconfigured templates for every setting and discipline. With our EHR, you can create:
With our EHR, you can create:
- Discharge summaries
- Group therapy notes
- Initial assessments
- Progress notes
- Treatment plans
ICANotes is ready right out of the box and can make behavioral health documentation comprehensive, quick and sophisticated enough to meet even the most stringent standards. You can effectively use ICANotes with little training. It's highly intuitive with a clinically logical workflow because its designers were clinicians with a thorough understanding of behavioral health.
ICANotes is the EHR software that thinks like a clinician. If you are a behavioral health clinician working in a residential setting or private practice, claim your free trial of ICANotes to aid with documentation.
Watch a Live Demo
Start a Free Trial
Related Posts:
CPT Code Basics: What You Should Know
What Intake Forms Do You Need for Your Behavioral Health Practice?
How to Make Your Practice Virtual
Billing Pitfalls for Mental Health Clinicians
How to Make Your Therapy Note-Writing Process More Efficient
Cheat sheets on psychiatry and narcology
Psychiatry is a medical discipline that studies the diagnosis and treatment, etiology, pathogenesis and distribution. ..
..
more »
The nosological direction in modern psychiatry (from the Greek nosos - "disease") is widespread as...
more »
Psychoneurological dispensaries operating on a territorial basis were established in 1923 ...
more »
The law “On Psychiatric Care and the Guarantee of the Rights of Citizens in the Provision of It” is based on the Decree...
more »
The syndrome as a stage of the disease can be the same in various mental disorders, which leads to...
details »
more »
Hallucinations are a disorder of perception in the form of images and ideas that arise without real information...
more »
True hallucinations - the patient perceives hallucinatory images as part of the real world, containing. ..
..
details »
Hallucinosis is a psychopathological syndrome, the leading disorder of which are hallucinations. Gal...
details »
Mental automatism - alienation of the patient's own mental processes and motor acts ...
more »
Accelerated pace (tachyphrenia) – thinking is superficial, thoughts flow quickly, easily shift...
details »
more »
Brad staging. The patients are convinced that those around them are putting on a performance especially for them....
details »
Memory is a cognitive (gnostic) function that allows to accumulate perceived information. ..
..
details »
Hypomnesia (dysmnesia) - memory loss. As a rule, all three functions are reduced. Process is broken...
more »
Intellect is a set of human cognitive abilities, the desire to acquire new knowledge....
details »
Dementia is an acquired form of dementia. Dementia, unlike oligophrenia, is always progradient, although...
more »
Tachyphasia - accelerated speech, can be manifested by verbosity or interspersed with proverbs, kalambu ...
more »
Emotions are called sensual reactions (affect) of a person to objects and phenomena of the surrounding world, they...
details »
Depression is a condition accompanied by an affect of melancholy (hypothymia), mental retardation and decreased...
details »
Somatized (masked, larvated) depression. The leader is the somato-vegetative kom...
The leader is the somato-vegetative kom...
more »
Will is a purposeful human activity, the ability to set goals. Big sign...
more »
Movement disorders (psychomotor disorders) include hypokinesias, dyskinesias and gi...
details »
Hyperkinesias include various violent automatic movements due to involuntary...
more »
Attraction is a need that arises as an unconscious desire for something. Disorders of inclinations ...
more »
Hypoeroticism (hyposexuality) - weakening, lowering sexual desire. Observed in asthenia,...
more »
Consciousness is a set of knowledge and ideas of a person about the world around him and about himself. Violations...
more »
Delirium is a pronounced disorder of subject orientation with the preservation of personal orientation. The prod...
more »
Oneiroid (schizophrenic delirium) is a change in consciousness with an influx of fantastic notions, which...
details »
It is observed in neurasthenia, somatic diseases, mild variants of exogenous organic races...
more »
The clinic of hysterical syndrome is characterized by a variety and variability of symptoms. Always in that...
more »
Depressive syndrome is manifested by a triad of obligate symptoms: worsening of mood, mental...
details »
Paroxysms (seizures) - suddenly developing, short-term (up to several seconds, less often up to several ...
more »
Absences (absence - "absence") - a short-term loss of consciousness, sometimes accompanied by a fall . ..
..
more » Memory disorders affect all three of its functions (fixation, retention, and reproduction) to some extent...
more details »
Negative syndromes are persistent or reversible personality changes in the form of a decrease, defect, or...
more »
The hyperthymic personality type is distinguished, as a rule, by an elevated mood, high vitality...
details »
more »
Schizoid psychopathy is distinguished by the following personality traits: inability to experience pleasure...
details »
Mood - prevailing for a certain period and influencing all mental activity ...
more » Schizophrenia is a progredient mental illness that appears on the basis of a genetic predisposition.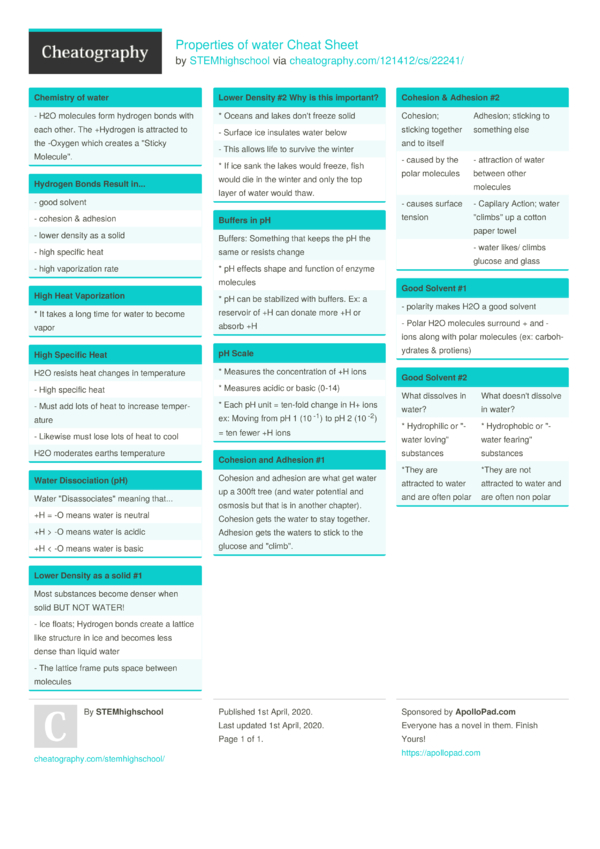 ..
..
more »
For patients with schizophrenia, pathology of volitional functions is typical. They are especially often detected in varying degrees...
more »
Closeness, selective sociability, formal contact are more common. In extreme cases, more...
more »
The states of clouded consciousness in schizophrenia are relatively rare. The vast majority...
more »
Almost all hallucinatory-paranoid syndromes are quite typical for schizophrenia: paranoiac, syn...
more »
more »
Attack-like progredient (fur-like) schizophrenia. Coat-like schizophrenia is the most common medium...
Coat-like schizophrenia is the most common medium...
more »
biological therapy. The leading place in the biological treatment of schizophrenia belongs to the psychopharmacoter...
more »
Treatment and rehabilitation. In the treatment of patients with schizophrenia, almost all methods of biological...
details »
more details »
The first stage (the stage of mental dependence). The main among the initial signs is pathology...
details »
False binges appear at stage II of alcoholism and arise as a result of socio-psychological...
details »
A drug is a narcotic drug included in the official state list due to social . ..
..
details »
At the first stage, addiction develops quite quickly: it is enough to repeat injections 5 times...
more »
Most often they smoke hashish, marijuana, "plan" - a dried and compressed substance that appears on the surface ...
more »
Ephedron is manufactured in illicit laboratories from medicines containing ephedrine. Derivative primary ...
more »
Psychiatry ticket answers
Crib
- doc format
- size 36.65 KB
- added January 25, 2012
Answers to 16 page
- Academic and specialized literature
- Medical disciplines
- Medical periodicals
- Bulletin of Psychiatry and Psychology of Chuvashia
- Academic and specialized literature
- Medical disciplines
- Medical periodicals
- Journal of Psychiatry and Medical Psychology
- Academic and specialized literature
- Medical disciplines
- Medical periodicals
- Independent Psychiatric Journal
- Academic and specialized literature
- Medical disciplines
- Medical periodicals
- Mental health
- Academic and specialized literature
- Medical disciplines
- Medical periodicals
- Russian Psychiatric Journal
- Academic and specialized literature
- Medical disciplines
- Forensic medicine
- Forensic psychiatry
- Academic and specialized literature
- Medical disciplines
- Pharmacology
- General and private pharmacology
- Psychopharmacology
- Academic and specialized literature
- Psychological disciplines
- Academic and specialized literature
- Psychological disciplines
- Periodicals in psychology
- Child and adolescent mental health issues
- Academic and specialized literature
- Legal disciplines
- Forensic examination
See also
- djvu format
- size 10.
 28 MB
28 MB - added February 10, 2011
Authors: Michael Gelder Professor of Psychiatry, University of Oxford Dennis Gath Professor of Clinical Psychiatry, Oxford. Univer. Richard Mayo Prof. clinical psychiatry oxf. Univer. This book was written primarily as an introductory guide for psychiatric interns and as an advanced textbook for medical students to provide them with in-depth professional training. We hope that this guide will...
- djvu format
- size 4.46 MB
- added November 17, 2009
M.: Medicine, 2002. -544 p. A new textbook on psychiatry for medical schools was created in accordance with the latest international classification of ICD-10. The most important sections of psychiatry are covered in detail: general psychopathology, major mental illnesses, methods of therapy and rehabilitation, social and legal issues of psychiatry. What is new is the selection of chapters that describe the somatic symptoms of mental illness, the characteristics of mental disorders ...
What is new is the selection of chapters that describe the somatic symptoms of mental illness, the characteristics of mental disorders ...
- format rar, doc
- size 359.04 KB
- added February 05, 2010
Yu. V. Kannabikh, the most prominent Russian psychiatrist of the early 20th century, outlines the main stages in the development of classical psychiatry from ancient times, and also shows the evolution of its basic concepts and principles. The course of development of psychiatric thought and applied psychiatry is given in connection with general medicine, sociology, philosophy and other sciences. It is intended for students and teachers of medical universities, but it can be useful to everyone who is interested...
- pdf format
- size 1.58 MB
- added November 28, 2009
Thesis for the degree of candidate of philosophical sciences. - M .: Moscow State University. M. V. Lomonosov, 2002. The history of psychiatry and the change of its paradigms in the 19–20 centuries. The relationship of scientific consciousness with the "spirit" of the cultural era. Alternative model of psychiatry (existential-phenomenological psychiatry), its values and goals in therapy. Analysis of Laing's theory of schizophrenia from the point of view of various scientific approaches. The question of the criteria for the norm and illness in psychiatry ....
- M .: Moscow State University. M. V. Lomonosov, 2002. The history of psychiatry and the change of its paradigms in the 19–20 centuries. The relationship of scientific consciousness with the "spirit" of the cultural era. Alternative model of psychiatry (existential-phenomenological psychiatry), its values and goals in therapy. Analysis of Laing's theory of schizophrenia from the point of view of various scientific approaches. The question of the criteria for the norm and illness in psychiatry ....
- djvu format
- size 14.99 MB
- added December 28, 2009
Ed. Academician G.V. Morozov. - M .: Medicine, 1988. This guide to psychiatry was compiled with the participation of leading experts from the socialist countries. The general problems of psychiatry are considered, the concepts of the subject and tasks of psychiatry are analyzed, the history of the doctrine of mental illness is given with the characteristics of the main psychiatric schools, the issues of the structural-functional and socio-biological foundations of mental illness are highlighted, about . ..
..
- pdf format
- size 2.16 MB
- added June 30, 2011
Nizhny Novgorod: Publishing House of NGMA, 1998 - 426 p. The manual is a fundamental work entirely devoted to propaedeutics in psychiatry. Semiotics, symptoms and syndromes of mental illness, issues of clinical research of the mentally ill, diagnostics and deontology in psychiatry are considered in detail. A separate chapter is devoted to psychosomatic medicine. The erudition and breadth of views of the authors allows them to refer both to Russians and to ...
abstract
- docx format
- size 35.83 KB
- added October 26, 2010
Contents Introduction History of foreign psychiatry. Its directions Clinical direction of psychiatry Biological direction of psychiatry Psychoanalytic direction of psychiatry Social psychiatry Development of Russian and modern psychiatry Conclusion List of sources used
Its directions Clinical direction of psychiatry Biological direction of psychiatry Psychoanalytic direction of psychiatry Social psychiatry Development of Russian and modern psychiatry Conclusion List of sources used
abstract
- rtf format
- size 223.59 KB
- added February 01, 2011
Siberian State Medical University Abstract on psychiatry on the topic: "Deontology in psychiatry" Tomsk. 2002. Page- 24 Introduction Development of Ethical Norms in the History of Psychiatry Treatment of mental patients and human rights Specificity of ethical problems in psychiatry Moral principles in psychiatry Models of mental illness Moral conflicts in psychiatry Ethics of a psychiatric nurse Psychotherapeutic role of a nurse Sp...
- doc format
- size 21.42 MB
- added May 31, 2010
This reference manual is a summary (in the form of diagrams, tables and figures) of clinical psychiatry. It deals with issues of general and private psychiatry, differential diagnosis of mental disorders, as well as selected issues of extreme psychiatry. A comparative analysis of domestic and international (ICD-10) classification approaches has been carried out. A concise dictionary of psychiatric and psychoanalytic ...
- doc format
- size 239 KB
- added July 24, 2011
Psychiatry examination for clinical psychologists. Consists of two parts. Part 1. Contains the following questions and answers: Epilepsy, Mental disorders in vascular diseases of the brain, Neurosis, Bipolar affective disorder, Schizophrenia.