Ocd confessing past mistakes
Real Event OCD: What Is It? Symptoms and Treatment
What Is Real Event OCD?
Real events obsessive-compulsive disorder (OCD) is a subtype of OCD characterized by ongoing intrusive thoughts and compulsive behaviors around someone’s past actions. While most types of OCD cause a person to fixate on feared future-oriented events, someone with real events OCD experiences intense anxiety over what they did or potentially could have done in the past. Someone with this OCD subtype will spend extensive energy attempting to gain certainty about a past event and whether they’ve done something potentially immoral or wrong.
Real Event OCD symptoms
Practically everyone experiences regret or doubt about the past. However, people with real events OCD often experience all-or-nothing thinking about these events. This is one of the main symptoms of this subtype. A person without OCD may think, “I probably shouldn’t have made fun of that boy in middle school,” reflect on their feelings, and move on.
For someone with real events OCD, guilt over this reflection can feel overwhelming, equivalent to committing a murder. Their OCD will take hold of past events and warp them until they are a villain who can never be excused. Even if the person dismisses these thoughts in their mind with rational explanations of their innocence (e.g. everyone makes mistakes when they are growing up), the OCD will morph to find even more reasons they are guilty.
Real event OCD will latch onto even the slightest doubt and cause fear that is not proportional to the action one is worried about. It often focuses on your teenage years, when there was more ambiguity and higher potential for regret. People with real events OCD will generally spend at least one hour per day and often greater on these obsessions and compulsions.
These obsessions often pop into the person’s mind seemingly out of nowhere and can occur with or without any apparent connection to the present. For example, during a workday, you might suddenly experience obsessive thoughts about cheating on an exam in middle school. The thoughts will take over your mind, and you won’t be able to concentrate on anything else. The fear of potentially harmful past actions drives people with this OCD subtype to engage in various compulsions aimed at gaining certainty about what exactly they’ve done and what this means about who they are as a person (e.g., searching for the person they bullied in middle school).
The thoughts will take over your mind, and you won’t be able to concentrate on anything else. The fear of potentially harmful past actions drives people with this OCD subtype to engage in various compulsions aimed at gaining certainty about what exactly they’ve done and what this means about who they are as a person (e.g., searching for the person they bullied in middle school).
Real events OCD can be incredibly time-consuming, drain someone of energy, and send them on a downward spiral of guilt as their OCD warps minor regrets into inexcusable crimes. These thoughts will go on and on, often for hours or days, and won’t leave until the person has engaged in a compulsion or found reassurance either internally or externally to dismiss these concerns. Often the person will replay the event in their mind and experience doubting thoughts about whether they remember the event correctly (e.g., “What if I didn’t accidentally cause my sister to trip when we were 5? What if I did it on purpose?”)
Examples of Real Event OCD obsessions
- I told my friend 10 years ago that I supported her choice of partner, and I didn’t tell her that I noticed a few potential red flags.
 Now they are getting a divorce. What if it’s my fault because I didn’t tell her what I really think?
Now they are getting a divorce. What if it’s my fault because I didn’t tell her what I really think? - Last year, I gave a restaurant a bad review, and I just found out they’ve shut down. It was all my fault their business tanked.
- When I was 12 I laughed at my classmate. What if they are still suffering because of what I did to them?
- A month ago, I told my friend she should get the haircut she wanted even though I didn’t think it would look good. Now she is miserable and hasn’t left the house in weeks. I could have prevented this.
- As a teenager, I drove after drinking a glass of wine. Nothing happened, thankfully, but what if something had? I can’t believe I risked that.
- When I was a teenager, I stole chips from a deli. I haven’t done anything like this since, but what if this act is still somehow a part of me? What if part of me is still a thief, and I unknowingly transfer this characteristic to my kids? What if they become thieves and it’s my fault?
Examples of Real Events OCD compulsions
- Mental reviewing: This is the most common compulsion for people with real events OCD.
 They will replay the event they are concerned about in their mind over and over until they feel like they’ve gained clarity and experience relief. Because it’s impossible to know exactly what happened in the past, it’s usually only a matter of time before these obsessive thoughts return and the cycle begins again.
They will replay the event they are concerned about in their mind over and over until they feel like they’ve gained clarity and experience relief. Because it’s impossible to know exactly what happened in the past, it’s usually only a matter of time before these obsessive thoughts return and the cycle begins again. - Reassurance seeking: Someone who is concerned that stealing potato chips as a teenager makes them a bad person may ask the people in their life questions like, “Have you ever stolen anything when you were younger?” and, “Do you think stealing one time makes someone a bad person?” These questions are aimed at giving this person relief from their fear of being guilty. They may also confess to a friend, “Hey, when I was 12, I stole chips from a deli. Does this make me a bad person?” They may also engage in compulsive research online, searching things like, “How to know if you’re a bad person?” “Why do people steal?” or “How to make sure your children won’t steal?”
- Confession: The guilt people with real events OCD experience can be very intense.
 This can drive people to confess to figures of authority. A person with this subtype may consider this the only way they can experience relief from their guilt.
This can drive people to confess to figures of authority. A person with this subtype may consider this the only way they can experience relief from their guilt.
Real event OCD ERP therapy
The best course of treatment for real events OCD, like all types of OCD, is exposure and response prevention (ERP) therapy. The idea behind ERP is that repeated exposure to obsessive thoughts, without engaging in compulsions, is the most effective way to treat OCD. When you continually reach out for the compulsions, it only strengthens your need to engage them. On the other hand, when you prevent yourself from engaging in your compulsions, you teach yourself a new way to respond and will very likely experience a noticeable reduction in your anxiety.
ERP is considered the gold standard for OCD treatment and has been found to be 80% effective. The majority of patients experience results within 12-20 sessions. As part of ERP therapy, you will track your obsessions and compulsions, and make a list of how distressing each thought is.
You’ll work with your therapist to slowly put yourself into situations that bring on your obsessions. This has to be carefully planned to ensure it’s effective, and so that you’re gradually building toward your goal rather than moving too quickly and getting completely overwhelmed.
Examples of Real Events OCD exposures
Using an imaginal exposure script is a common form of ERP therapy for real events OCD. This is where you take one of the fears driving your obsessive thoughts and play it out to the worst possible end. For example, you might play out the fear that you stole something as a teenager and are still somehow a thief. What if that’s true? What will happen if your children do turn out to be thieves and it’s because of something you unknowingly taught them? Then what? Will they get caught? What happens next?
As you can imagine, using imaginal exposure scripts can be uncomfortable because it requires unfolding hypothetical scenarios your mind has labeled the worst possible thing that can happen. However, the idea behind ERP is to habituate yourself to these fearful thoughts so that they will loosen their grip on you. Eventually you’ll get to a point where you are relatively comfortable with the uncertainty of these past actions, and the obsessive thoughts will reside.
However, the idea behind ERP is to habituate yourself to these fearful thoughts so that they will loosen their grip on you. Eventually you’ll get to a point where you are relatively comfortable with the uncertainty of these past actions, and the obsessive thoughts will reside.
How to get help
Real events OCD can be a tricky diagnosis to spot because it’s an unconventional type of OCD. Instead of being driven by fears of things that may happen in the future, this subtype is driven by what’s already happened. A mental health professional who specializes in OCD will be able to make an accurate diagnosis. If you’re interested in learning about real events OCD and how it’s treated with ERP, you can schedule a free call with the NOCD clinical team to find out how this type of treatment can help you. All of our therapists specialize in OCD and receive ERP-specific training and ongoing guidance from our clinical leadership team. Many of them have dealt with OCD themselves and understand how crucial ERP therapy is. NOCD offers live face-to-face video therapy sessions with OCD therapists, in addition to ongoing support on the NOCD telehealth app, so that you’re fully supported during the course of your treatment. You can also join our Real Event OCD community and get 24/7 access to personalized self-management tools built by people who have been through OCD and successfully recovered.
NOCD offers live face-to-face video therapy sessions with OCD therapists, in addition to ongoing support on the NOCD telehealth app, so that you’re fully supported during the course of your treatment. You can also join our Real Event OCD community and get 24/7 access to personalized self-management tools built by people who have been through OCD and successfully recovered.
Learn More About Real Event OCD
- What is Real Events OCD? Overview, Examples and Treatment
- A Quick Guide to Some Common OCD Subtypes
- What is a Compulsion?
- Here’s What a Typical Journey Through OCD ERP Therapy Looks Like
Real Event OCD and 10 Steps to Getting Better
Turning Point Psychological Services
OCD & Co.
Turning Point Psychological Services
OCD & Co.
Photo by: Anita Jankovic / unsplash.com
Contact
My OCD is DifferentIt happened years ago. You even forgot about it for a while, until you remembered and all of a sudden, it hit you and now you can’t stop thinking about what you’ve done. You spent hours researching how to get rid of the shame and guilt about something you did in the past. Your friends and family told you to get over it, that it wasn’t a big deal. You’ve spent years convincing yourself you didn’t do anything wrong. You’ve replayed it in your head countless times. And yet, none of it seems to relieve your intense guilt
While obsessively Googling (again) and asking questions in online forums, you may have stumbled upon information related to OCD and its symptoms.
It seemed that what you are experiencing is very consistent with having obsessions and compulsions. But then – how can that be OCD? After all, you have read that people with OCD are constantly worried about something bad happening in the future. And that they are unlikely to do what they are afraid of doing. Your case, however, is very different as you actually DID do what seems like an immoral or horrible act.
And that they are unlikely to do what they are afraid of doing. Your case, however, is very different as you actually DID do what seems like an immoral or horrible act.
So it can’t be OCD, right? But if not, then what is it? And how do you step out of this never-ending struggle of trying to find reassurance and get rid of the horrible guilt feelings? How do you move on with your life?
And how to know whether it’s OCD or not?
Doubting that you may have OCD is a common OCD symptom. This is one of the lies that OCD tells you, and in no other type of OCD is this lie as effective at hooking you as in real event OCD.
OCD is a doubting disorder. It will make you doubt your memory, your recollection of things, your morals, your intentions, your identity and – that’s right –whether you even have OCD! As it would have you believe, maybe you are just a horrible person who uses OCD as an excuse to avoid paying the moral price for your past misdeeds.
Some Examples of Past Events That People with Real Event OCD Tend to Ruminate about:- I stole someone’s work idea and presented it as my own
- I bullied a kid when I was in school
- I was really mean to a friend
- I cheated on my partner
- I engaged in a sexual play with my brother when we were kids
- I broke up with my girlfriend in the worst possible way
- I cheated on an exam/assignment
- I had sex with a girl who didn’t seem 100% sure about having sex with me
- I abused my sibling
- I made a racist remark at a co-worker
- I drank and drove
- I made a fraudulent claim when submitting taxes
- I was involved in a mean prank on friends
- I made a horrible mistake and my life will never be the same because of it
Common Real Event OCD Obsessions- Intrusive thoughts, images, memories, and flashbacks about what happened
- Intrusive thoughts and worries about being immoral, bad, mean, sick, racist, deceitful, cruel, hypocritical, despicable, unauthentic
- Thoughts about needing punishment for your actions
- Overwhelming feelings of guilt or shame
Common Real Event OCD Compulsions- Mental review
- Trying hard to figure out what exactly happened, why it happened, and what it says about you as a person
- Trying to recall all the little details of the event (while constantly questioning the accuracy of your recollection)
- Replaying the event in your mind again and again
Of course, like with every other OCD type, the more you seek certainty, the less certain you become.And while the compulsions may sometimes bring you temporary relief, in the long run, they just lead to stickier obsessions.
- Confessing
- Seeking reassurance
- Self-reassurance
- Ruminating
- Trying to rationalize
- Googling topics that are related to the event
- Googling how other people overcame a similar event
- If you harmed another person, following that person on social media and trying to get information about them in an attempt to find out if what you did continues to negatively affect their life
- Trying to achieve 100% certainty in remembering what happened
- Reading about ways to forgive yourself
- Trying to block or neutralize the thought
- Asking others if you are a good person
- Reading about what it means to be a good person
- Trying to prevent doing something bad in the future
- Trying to distract yourself
- Excessive self-reflection
- Avoiding anything that can remind you about the event
- Avoiding the place where the event happened (or, on the opposite, going back to that place trying to recreate the event in your mind or to check how you are feeling
- Debating whether to search for the person you harmed and apologize or to stay away
- Asking others for their opinions
- Asking others if something like that ever happened to them
- Coming up with scenarios of a similar event happening in the future and trying to figure out with absolute certainty that you will behave differently then
- Trying to “neutralize” the disturbing thoughts by reassuring yourself that you are a good, moral person
- Punishing yourself
- Cultivating self-hate in an attempt to relieve the guilt
- Trying to repent by doing “good deeds”
Of course, like with every single other OCD type, the more you seek certainty, the less certain you become. And while the compulsions may sometimes bring you temporary relief, in the long run, they just lead to stickier obsessions.
And while the compulsions may sometimes bring you temporary relief, in the long run, they just lead to stickier obsessions.
Contact
How Do I Know if It’s Really OCD?These events aren’t something that anybody would be proud of, but most people find a way to continue living their life in spite of their regrets and remorse. In your case, however, you feel stuck and are unable to get over what happened. You question your identity and feel you don’t deserve to move on until you find a way to figure everything out and make amends.
Real event OCD, as well as false memory OCD described below, is very commonly present in combination with all kinds of moral, scrupulosity, and harm OCD, and, specifically, with pedophilic OCD (POCD) and sexual orientation OCD (HOCD).
As with every OCD type (and there are many more commonalities between all the OCD types than differences between them), it’s not the nature of the event that determines if it’s OCD or not. It’s the process of your engagement with your thoughts that indicates that it may be OCD.
It’s the process of your engagement with your thoughts that indicates that it may be OCD.
Here are some signs that you may have OCD:
- You are overwhelmed by uncertainty about what really happened, how it may have affected you or others, and what kind of person you are. This uncertainty feels unbearable and leads you to seek ways to get rid of it and figure out once and for all, with the 100% certainty what happened
- You feel that you can’t move on without figuring it all out
- Your thoughts are very sticky, and you are preoccupied with them
- You have a sense of urgency to do something about the event right away
- A great deal of your day is dominated by your thoughts and feelings, as well as by your attempts to “deal” with them
- Your daily functioning (work, studies, relationships, hobbies, self-care, motivation, etc.) is negatively affected
- You find yourself in a never-ending quest to find relief, but the relief is always short-lived and additional doubts and questions seem to be constantly generated by your mind
- The more you try to figure out your past, your future, and what kind of person you are, the more doubts you have
Now, to go back to the beginning of this article – you are probably skimming through this page with an urgent question in mind: HOW DO I KNOW FOR SURE IF IT’S OCD?
Please brace yourself for an answer: Your question by itself is an OCD symptom – a desperate need to have certainty. You think that if only you knew for sure that it’s really OCD, then you could forgive yourself and move on. But the thing is – like with every single one of OCD’s questions – you will never know for sure. It’s this quest for certainty that keeps your OCD going. And the only way to recovery is by accepting the uncertainty. None of us know anything for sure. And you are not special in that way. You may never know for sure either.
You think that if only you knew for sure that it’s really OCD, then you could forgive yourself and move on. But the thing is – like with every single one of OCD’s questions – you will never know for sure. It’s this quest for certainty that keeps your OCD going. And the only way to recovery is by accepting the uncertainty. None of us know anything for sure. And you are not special in that way. You may never know for sure either.
It’s the quest for certainty that keeps your OCD going. And the only way to recovery is by accepting the uncertainty.
So, the answer to your question is: You may never know for sure and making peace with this not-knowing is your first step to regaining your life.
Here are a couple of other similar and not well-known OCD types related to past events:
False Memory OCDA person with this OCD type may be unsure if they did or said something bad or immoral. It is usually related to a specific, neutral time or event after which the person starts doubting if maybe, during that time, they somehow did something bad, said something insensitive or insulting, left an offensive or racist comment on a social media post, or messaged or emailed something inappropriate.
Another possible manifestation of this OCD type may be a person doubting if they were the ones who committed a high-profile crime that happened in their area. On the one hand, the person knows that he or she didn’t do it, but on another level, there is a doubt - what if they somehow did it and just blocked it from their memory.
In this case, the person is not sure if anything actually happened or not, but the possibility that something COULD have happened drives the compulsions.
Of course, exactly like in the case of Real Event OCD, no amount of mental review (or physical checking), rumination, or reassurance is enough to relieve the uncertainty. And the more the person thinks about it, the more real and detailed the false memory feels. In time, it actually does become a memory of its own - shaped and embellished by numerous retrievals. The more the person ruminates about it, the more OCD will "fill in the blanks" of what supposedly happened.
The false memory (the obsession) and the attempts to figure out whether the event happened (the compulsions) create a vicious cycle where the more the person ruminates, the more real the memory seems. And the more real the memory seems, the more compelled to ruminate/review/figure out the person feels, which, in turn, leads to the memory seeming even more real.
And the more real the memory seems, the more compelled to ruminate/review/figure out the person feels, which, in turn, leads to the memory seeming even more real.
This is the need to record and document everything that is happening in a person’s life. It’s a kind of mental hoarding where the person feels compelled to “collect” their memories in case they will need to retrieve them with 100% accuracy someday. They feel that if they don’t “save” the memories very accurately, the memories may get fully or partially lost, distorted, or misconstrued. A person may try to memorize an event, an inter-personal interaction, or the details of their environment.
Of course, with these other two OCD subtypes, exactly like with real event OCD, the attempt to get absolute certainty about the past leads to more and more doubt.
There is a huge overlap between the compulsions among all these OCD types and, in general, among all OCD types. Real event OCD and false memory OCD are especially related to moral scrupulosity (and, thus, to ROCD, sexual-themed OCD, and harm OCD).
Real event OCD and false memory OCD are especially related to moral scrupulosity (and, thus, to ROCD, sexual-themed OCD, and harm OCD).
As with all OCD types, it is not the obsessions that drive your OCD. The obsessions are just the thoughts that are generated by your mind. When you engage in compulsions, you are sending your mind the message that these intrusive thoughts are important and the mind then, in turn, generates even more of them.
Here are some strategies for you to start breaking free from being pushed around by your obsessions:
1. OCD is known for attacking what matters the most to us, so this is your chance to use your obsessions as a guide to understanding yourself.
Which values lie underneath your regret? What is your pain trying to tell you? What matters most to you in your life? What kind of person would you like to be? How would you like to treat yourself, others, and the world around you?
As opposed to to being consumed by your intrusive thoughts, memories, and emotions, use them to uncover your core values and start taking active steps toward them in the present instead of being consumed by the past.
2. Start making a list of what gets neglected while you continue being entangled in the battle with your mind. Is being consumed by the past preventing you from having a present? Do you find that being hooked by your thoughts prevents you from taking effective action toward your goals? Are you spending so much time in your head that you don’t feel present or engaged in the moment with people you care about and in doing what you love? What would you be doing differently if you could put your memories aside and reengage with what matters to you in your life?
Make a list, put it somewhere visible, and use it for motivation in the moments where your OCD tries to hijack your attention by making you compulse.
3. Every time you have an urge to check, ruminate, neutralize, reassure, or do any other compulsion – ask yourself, “If I let these thoughts and emotions determine what I do in the next few minutes or an hour, will it get me closer to the person I want to be or will it move me even further away?”
You have to make a choice here: do you move toward your values, or toward your compulsions? It can be one or the other – never both. Practice making choices that serve you and not your OCD.
Practice making choices that serve you and not your OCD.
4. Put a visible reminder somewhere that it’s OCD that is your enemy now, not your past event.
5. Do not try to get rid of your thoughts and emotions. They will come and go at their own time. Let them be and redirect your attention toward taking a step toward something that is important to you (not to your OCD). Don’t wait for the difficult emotions to subside. You can have them and still live your life the way you choose to in the present.
6. Ban rumination. This is a very insidious compulsion that masquerades as problem-solving. Even trying to figure out whether it is really OCD is an example of rumination.
As just stated, there is no point in trying to get rid of your initial thoughts. The more you try to get rid of them the more attention you are giving to them. But engaging with the thoughts (as in ruminating) is a whole different issue. It may seem automatic and involuntary to you now. But the good news is that with practice, you can learn to redirect your attention elsewhere.
It may seem automatic and involuntary to you now. But the good news is that with practice, you can learn to redirect your attention elsewhere.
Think about your intrusive thoughts as spam emails. There may not be much to do to stop them. But you don’t have to open them, read them, respond to them, or spend time thinking about them.
Your intrusive thoughts thrive on your attention. Whether you try to debate them, prove them wrong, examine them, get rid of them, discuss them, confess them, get deeper to their meaning, worry that you’ll never be able to stop them, or whatever else you may be doing, — all of it just makes them stronger. Instead, start noticing them and redirect your attention elsewhere. It doesn’t matter where. You don’t even have to redirect your attention to anything specific, you can let your attention wander — as long as you do not direct it to the obsessive thought.
In the beginning, it will be difficult. But you will soon learn that you have much more control over your attention than you realized. And while you will still be aware of your intrusive thought (we are not trying to get rid of it, remember?), it will remain somewhere at the background while you go about your life without engaging with it.
And while you will still be aware of your intrusive thought (we are not trying to get rid of it, remember?), it will remain somewhere at the background while you go about your life without engaging with it.
7. Practice self-compassion. This is not the same as forgiveness (which, in your case, most likely will just constitute another compulsion).
Self-compassion is acknowledging that you are suffering. You can remind yourself that suffering is a common human experience and is a part of life. Give yourself a moment of kindness without reassuring yourself. Put a hand on your heart and say to yourself, “This is very hard. This causes me a lot of pain. I have such a strong urge to do a compulsion. I am allowed to be kind to myself.”
(Yes, yes, I know: your OCD will probably tell you that you don’t deserve kindness. Or that kindness is another way to trick yourself into thinking you didn’t do anything wrong. Please treat this thought just like every other obsession – let it be and continue practicing self-compassion)
8. This is a tough one. The only way to recover from OCD is to be willing to live with the fact that your scary thoughts may (or may not) be right. It doesn’t mean that you accept that they ARE right. It just means that you accept the not knowing.
This is a tough one. The only way to recover from OCD is to be willing to live with the fact that your scary thoughts may (or may not) be right. It doesn’t mean that you accept that they ARE right. It just means that you accept the not knowing.
As long as you continue living with the hope that you will have certainty about the past, the future, and the kind of person you are, OCD will continue to have a grip on you. Yes, the thoughts about what you did and what kind of an immoral human being you may be are horrific. But these are thoughts. Not facts. Hold them lightly. All our thoughts may or may not be true. As long as we don’t take them too seriously, we have the freedom to live our life. Allow the uncertainty to be there and continue with your day.
9. Seek treatment. Your OCD will, of course, tell you that treatment will not help, that you will be judged, that going to therapy is just an excuse to avoid repenting, that nobody can possibly understand what you are going through, that the shame will be unbearable, that your OCD is very different from other OCDs and that, of course, it may not even be a real OCD. Just like with the other thoughts, hold these thoughts lightly and don’t allow them to sway you from getting your life back.
Just like with the other thoughts, hold these thoughts lightly and don’t allow them to sway you from getting your life back.
10. Make sure that your therapist specializes in OCD and practices ERP (Exposure and Response Prevention) and ACT (Acceptance and Commitment Therapy). This is crucial. Seeing somebody whose method of treatment is CBT but who doesn’t mention ERP as their treatment approach on their website or in your phone conversation is not enough. Not all CBT is applicable for OCD and the therapist needs to know a very special way of using CBT for the treatment of OCD.
If your therapist is not an OCD expert, he or she may just unwittingly co-compulse with you by providing reassurance, engaging in figuring things out, examining your thoughts, teaching you strategies to get rid of the thoughts or arguing with the thoughts, etc. If you read this article up to this point, you know that all of those are compulsions and that the relief from them is very short-lived.
OCD is a treatable disorder. There is so much that you can do to get your life back. Don’t delay living your life and don’t lose hope.
Think you may have a real event OCD? Share your story in the comments below!
If you enjoyed this article, follow us on Facebook for more great tips and resources!
Contact
Anna Prudovski is a Psychologist and the Clinical Director of Turning Point Psychological Services. She has a special interest in treating anxiety disorders and OCD, as well as working with parents.
Anna lives with her husband and children in Vaughan, Ontario. When she is not treating patients, supervising clinicians, teaching CBT, and attending professional workshops, Anna enjoys practicing yoga, going on hikes with her family, traveling, studying Ayurveda, and spending time with friends. Her favorite pastime is reading.
Her favorite pastime is reading.
Related Posts
Tagged: OCD
- Anxiety
- Depression
- Emotions
- Mindfulness
- OCD & Co.
- Panic Disorder
- Parenting
- Social Anxiety
- Therapy
- 𝛙 My Thoughts
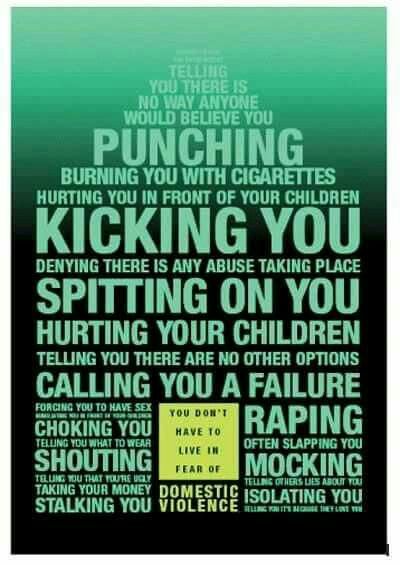
Obsessive-compulsive disorder
A prominent role among mental illnesses is played by syndromes (complexes of symptoms), united in the group of obsessive-compulsive disorder (OCD), which received its name from the Latin terms obsessio and compulsio.
Obsession (lat. obsessio - taxation, siege, blockade).
Compulsions (lat. compello - I force). 1. Obsessive drives, a kind of obsessive phenomena (obsessions). Characterized by irresistible attraction that arises contrary to the mind, will, feelings. Often they are unacceptable to the patient, contrary to his moral and ethical properties. Unlike impulsive drives, compulsions are not realized. These drives are recognized by the patient as wrong and painfully experienced by them, especially since their very appearance, due to its incomprehensibility, often gives rise to a feeling of fear in the patient 2. The term compulsions is also used in a broader sense to refer to any obsessions in the motor sphere, including obsessive rituals. nine0003
In domestic psychiatry, obsessive states were understood as psychopathological phenomena, characterized by the fact that phenomena of a certain content repeatedly appear in the mind of the patient, accompanied by a painful feeling of coercion [Zinoviev PM, 193I]. For N.s. characteristic involuntary, even against the will, the emergence of obsessions with clear consciousness. Although the obsessions are alien, extraneous in relation to the patient's psyche, the patient is not able to get rid of them. They are closely related to the emotional sphere, accompanied by depressive reactions, anxiety. Being symptomatic, according to S.L. Sukhanov [1912], "parasitic", they do not affect the course of intellectual activity in general, remain alien to thinking, do not lead to a decrease in its level, although they worsen the efficiency and productivity of the patient's mental activity. Throughout the course of the disease, a critical attitude is maintained towards obsessions. N.s. conditionally divided into obsessions in the intellectual-affective (phobia) and motor (compulsions) spheres, but most often several of their types are combined in the structure of the disease of obsessions. The isolation of obsessions that are abstract, affectively indifferent, indifferent in their content, for example, arrhythmomania, is rarely justified; An analysis of the psychogenesis of a neurosis often makes it possible to see a pronounced affective (depressive) background at the basis of the obsessive account.
Although the obsessions are alien, extraneous in relation to the patient's psyche, the patient is not able to get rid of them. They are closely related to the emotional sphere, accompanied by depressive reactions, anxiety. Being symptomatic, according to S.L. Sukhanov [1912], "parasitic", they do not affect the course of intellectual activity in general, remain alien to thinking, do not lead to a decrease in its level, although they worsen the efficiency and productivity of the patient's mental activity. Throughout the course of the disease, a critical attitude is maintained towards obsessions. N.s. conditionally divided into obsessions in the intellectual-affective (phobia) and motor (compulsions) spheres, but most often several of their types are combined in the structure of the disease of obsessions. The isolation of obsessions that are abstract, affectively indifferent, indifferent in their content, for example, arrhythmomania, is rarely justified; An analysis of the psychogenesis of a neurosis often makes it possible to see a pronounced affective (depressive) background at the basis of the obsessive account. Along with elementary obsessions, the connection of which with psychogeny is obvious, there are “cryptogenic” ones, when the cause of painful experiences is hidden [Svyadoshch L.M., 1959]. N.s. are observed mainly in individuals with a psychasthenic character. This is where apprehensions are especially characteristic. In addition, N.S. occur within the framework of neurosis-like states with sluggish schizophrenia, endogenous depressions, epilepsy, the consequences of a traumatic brain injury, somatic diseases, mainly hypochondria-phobic or nosophobic syndrome. Some researchers distinguish the so-called. "Neurosis of obsessive states", which is characterized by the predominance of obsessive states in the clinical picture - memories that reproduce a psychogenic traumatic situation, thoughts, fears, actions. In genesis play a role: mental trauma; conditioned reflex stimuli that have become pathogenic due to their coincidence with others that previously caused a feeling of fear; situations that have become psychogenic due to the confrontation of opposing tendencies [Svyadoshch A.
Along with elementary obsessions, the connection of which with psychogeny is obvious, there are “cryptogenic” ones, when the cause of painful experiences is hidden [Svyadoshch L.M., 1959]. N.s. are observed mainly in individuals with a psychasthenic character. This is where apprehensions are especially characteristic. In addition, N.S. occur within the framework of neurosis-like states with sluggish schizophrenia, endogenous depressions, epilepsy, the consequences of a traumatic brain injury, somatic diseases, mainly hypochondria-phobic or nosophobic syndrome. Some researchers distinguish the so-called. "Neurosis of obsessive states", which is characterized by the predominance of obsessive states in the clinical picture - memories that reproduce a psychogenic traumatic situation, thoughts, fears, actions. In genesis play a role: mental trauma; conditioned reflex stimuli that have become pathogenic due to their coincidence with others that previously caused a feeling of fear; situations that have become psychogenic due to the confrontation of opposing tendencies [Svyadoshch A. M., 1982]. It should be noted that these same authors emphasize that N.s.c. occurs with various character traits, but most often in psychasthenic personalities.
M., 1982]. It should be noted that these same authors emphasize that N.s.c. occurs with various character traits, but most often in psychasthenic personalities.
Currently, almost all obsessive-compulsive disorders are united in the International Classification of Diseases under the concept of "obsessive-compulsive disorder".
OKR concepts have undergone a fundamental reassessment over the past 15 years. During this time, the clinical and epidemiological significance of OCD has been completely revised. If it was previously thought that this is a rare condition observed in a small number of people, now it is known that OCD is common and causes a high percentage of morbidity, which requires the urgent attention of psychiatrists around the world. Parallel to this, our understanding of the etiology of OCD has broadened: the vaguely formulated psychoanalytic definition of the past two decades has been replaced by a neurochemical paradigm that explores the neurotransmitter disorders that underlie OCD. And most importantly, pharmacological interventions specifically targeting serotonergic neurotransmission have revolutionized the prospects for recovery for millions of OCD patients worldwide. nine0003
And most importantly, pharmacological interventions specifically targeting serotonergic neurotransmission have revolutionized the prospects for recovery for millions of OCD patients worldwide. nine0003
The discovery that intense serotonin reuptake inhibition (SSRI) was the key to effective treatment for OCD was the first step in a revolution and spurred clinical research that showed the efficacy of such selective inhibitors.
As described in ICD-10, the main features of OCD are repetitive intrusive (obsessive) thoughts and compulsive actions (rituals).
In a broad sense, the core of OCD is the syndrome of obsession, which is a condition with a predominance in the clinical picture of feelings, thoughts, fears, memories that arise in addition to the desire of patients, but with awareness of their pain and a critical attitude towards them. Despite the understanding of the unnaturalness, illogicality of obsessions and states, patients are powerless in their attempts to overcome them. Obsessional impulses or ideas are recognized as alien to the personality, but as if coming from within. Obsessions can be the performance of rituals designed to alleviate anxiety, such as washing hands to combat "pollution" and to prevent "infection". Attempts to drive away unwelcome thoughts or urges can lead to severe internal struggle, accompanied by intense anxiety. nine0003
Obsessional impulses or ideas are recognized as alien to the personality, but as if coming from within. Obsessions can be the performance of rituals designed to alleviate anxiety, such as washing hands to combat "pollution" and to prevent "infection". Attempts to drive away unwelcome thoughts or urges can lead to severe internal struggle, accompanied by intense anxiety. nine0003
Obsessions in the ICD-10 are included in the group of neurotic disorders.
The prevalence of OCD in the population is quite high. According to some data, it is determined by an indicator of 1.5% (meaning "fresh" cases of diseases) or 2-3%, if episodes of exacerbations observed throughout life are taken into account. Those suffering from obsessive-compulsive disorder make up 1% of all patients receiving treatment in psychiatric institutions. It is believed that men and women are affected approximately equally. nine0003
CLINICAL PICTURE
The problem of obsessive-compulsive disorders attracted the attention of clinicians already at the beginning of the 17th century. They were first described by Platter in 1617. In 1621 E. Barton described an obsessive fear of death. Mentions of obsessions are found in the writings of F. Pinel (1829). I. Balinsky proposed the term "obsessive ideas", which took root in Russian psychiatric literature. In 1871, Westphal coined the term "agoraphobia" to refer to the fear of being in public places. M. Legrand de Sol [1875], analyzing the features of the dynamics of OCD in the form of "insanity of doubt with delusions of touch, points to a gradually becoming more complicated clinical picture - obsessive doubts are replaced by ridiculous fears of" touch "to surrounding objects, motor rituals join, the fulfillment of which is subject to the whole life sick. However, only at the turn of the XIX-XX centuries. researchers were able to more or less clearly describe the clinical picture and give syndromic characteristics of obsessive-compulsive disorders. The onset of the disease usually occurs in adolescence and adolescence. The maximum of clinically defined manifestations of obsessive-compulsive disorder is observed in the age range of 10-25 years.
They were first described by Platter in 1617. In 1621 E. Barton described an obsessive fear of death. Mentions of obsessions are found in the writings of F. Pinel (1829). I. Balinsky proposed the term "obsessive ideas", which took root in Russian psychiatric literature. In 1871, Westphal coined the term "agoraphobia" to refer to the fear of being in public places. M. Legrand de Sol [1875], analyzing the features of the dynamics of OCD in the form of "insanity of doubt with delusions of touch, points to a gradually becoming more complicated clinical picture - obsessive doubts are replaced by ridiculous fears of" touch "to surrounding objects, motor rituals join, the fulfillment of which is subject to the whole life sick. However, only at the turn of the XIX-XX centuries. researchers were able to more or less clearly describe the clinical picture and give syndromic characteristics of obsessive-compulsive disorders. The onset of the disease usually occurs in adolescence and adolescence. The maximum of clinically defined manifestations of obsessive-compulsive disorder is observed in the age range of 10-25 years. nine0003
nine0003
Main clinical manifestations of OCD:
Obsessional thoughts - painful, arising against the will, but recognized by the patient as their own, ideas, beliefs, images, which in a stereotyped form forcibly invade the patient's consciousness and which he tries to resist in some way. It is this combination of an inner sense of compulsive urge and efforts to resist it that characterizes obsessional symptoms, but of the two, the degree of effort exerted is the more variable. Obsessional thoughts may take the form of single words, phrases, or lines of poetry; they are usually unpleasant to the patient and may be obscene, blasphemous, or even shocking. nine0003
Obsessional imagery is vivid scenes, often violent or disgusting, including, for example, sexual perversion.
Obsessional impulses are urges to do things that are usually destructive, dangerous or shameful; for example, jumping into the road in front of a moving car, injuring a child, or shouting obscene words while in society.
Obsessional rituals include both mental activities (eg, counting repeatedly in a particular way, or repeating certain words) and repetitive but meaningless acts (eg, washing hands twenty or more times a day). Some of them have an understandable connection with the obsessive thoughts that preceded them, for example, repeated washing of hands - with thoughts of infection. Other rituals (for example, regularly laying out clothes in some complex system before putting them on) do not have such a connection. Some patients feel an irresistible urge to repeat such actions a certain number of times; if that fails, they are forced to start all over again. Patients are invariably aware that their rituals are illogical and usually try to hide them. Some fear that such symptoms are a sign of the onset of insanity. Both obsessive thoughts and rituals inevitably lead to problems in daily activities. nine0003
Obsessive rumination (“mental chewing gum”) is an internal debate in which the arguments for and against even the simplest everyday actions are endlessly revised. Some obsessive doubts relate to actions that may have been incorrectly performed or not completed, such as turning off the gas stove faucet or locking the door; others concern actions that could harm other people (for example, the possibility of driving past a cyclist in a car, knocking him down). Sometimes doubts are associated with a possible violation of religious prescriptions and rituals - “remorse of conscience”. nine0003
Some obsessive doubts relate to actions that may have been incorrectly performed or not completed, such as turning off the gas stove faucet or locking the door; others concern actions that could harm other people (for example, the possibility of driving past a cyclist in a car, knocking him down). Sometimes doubts are associated with a possible violation of religious prescriptions and rituals - “remorse of conscience”. nine0003
Compulsive actions - repetitive stereotypical actions, sometimes acquiring the character of protective rituals. The latter are aimed at preventing any objectively unlikely events that are dangerous for the patient or his relatives.
In addition to the above, in a number of obsessive-compulsive disorders, a number of well-defined symptom complexes stand out, and among them are obsessive doubts, contrasting obsessions, obsessive fears - phobias (from the Greek. phobos).
nine0002 Obsessive thoughts and compulsive rituals may intensify in certain situations; for example, obsessive thoughts about harming other people often become more persistent in the kitchen or some other place where knives are kept. Since patients often avoid such situations, there may be a superficial resemblance to the characteristic avoidance pattern found in phobic anxiety disorder. Anxiety is an important component of obsessive-compulsive disorders. Some rituals reduce anxiety, while after others it increases. Obsessions often develop as part of depression. In some patients, this appears to be a psychologically understandable reaction to obsessive-compulsive symptoms, but in other patients, recurrent episodes of depressive mood occur independently. nine0003
Since patients often avoid such situations, there may be a superficial resemblance to the characteristic avoidance pattern found in phobic anxiety disorder. Anxiety is an important component of obsessive-compulsive disorders. Some rituals reduce anxiety, while after others it increases. Obsessions often develop as part of depression. In some patients, this appears to be a psychologically understandable reaction to obsessive-compulsive symptoms, but in other patients, recurrent episodes of depressive mood occur independently. nine0003 Obsessions (obsessions) are divided into figurative or sensual, accompanied by the development of affect (often painful) and obsessions of affectively neutral content.
Sensual obsessions include obsessive doubts, memories, ideas, drives, actions, fears, an obsessive feeling of antipathy, an obsessive fear of habitual actions.
Obsessive doubts - intrusively arising contrary to logic and reason, uncertainty about the correctness of committed and committed actions. The content of doubts is different: obsessive everyday fears (whether the door is locked, whether windows or water taps are closed tightly enough, whether gas and electricity are turned off), doubts related to official activities (whether this or that document is written correctly, whether the addresses on business papers are mixed up , whether inaccurate figures are indicated, whether orders are correctly formulated or executed), etc. Despite repeated verification of the committed action, doubts, as a rule, do not disappear, causing psychological discomfort in a person suffering from this kind of obsession. nine0003
The content of doubts is different: obsessive everyday fears (whether the door is locked, whether windows or water taps are closed tightly enough, whether gas and electricity are turned off), doubts related to official activities (whether this or that document is written correctly, whether the addresses on business papers are mixed up , whether inaccurate figures are indicated, whether orders are correctly formulated or executed), etc. Despite repeated verification of the committed action, doubts, as a rule, do not disappear, causing psychological discomfort in a person suffering from this kind of obsession. nine0003
Obsessive memories include persistent, irresistible painful memories of any sad, unpleasant or shameful events for the patient, accompanied by a sense of shame, remorse. They dominate the mind of the patient, despite the efforts and efforts not to think about them.
Obsessive impulses - urges to commit one or another tough or extremely dangerous action, accompanied by a feeling of horror, fear, confusion with the inability to get rid of it. The patient is seized, for example, by the desire to throw himself under a passing train or push a loved one under it, to kill his wife or child in an extremely cruel way. At the same time, patients are painfully afraid that this or that action will be implemented. nine0003
The patient is seized, for example, by the desire to throw himself under a passing train or push a loved one under it, to kill his wife or child in an extremely cruel way. At the same time, patients are painfully afraid that this or that action will be implemented. nine0003
Manifestations of obsessive ideas can be different. In some cases, this is a vivid "vision" of the results of obsessive drives, when patients imagine the result of a cruel act committed. In other cases, obsessive ideas, often referred to as mastering, appear in the form of implausible, sometimes absurd situations that patients take for real. An example of obsessive ideas is the patient's conviction that the buried relative was alive, and the patient painfully imagines and experiences the suffering of the deceased in the grave. At the height of obsessive ideas, the consciousness of their absurdity, implausibility disappears and, on the contrary, confidence in their reality appears. As a result, obsessions acquire the character of overvalued formations (dominant ideas that do not correspond to their true meaning), and sometimes delusions. nine0003
nine0003
An obsessive feeling of antipathy (as well as obsessive blasphemous and blasphemous thoughts) - unjustified, driven away by the patient from himself antipathy towards a certain, often close person, cynical, unworthy thoughts and ideas in relation to respected people, in religious persons - in relation to saints or ministers churches.
Obsessive acts are acts done against the wishes of the sick, despite efforts made to restrain them. Some of the obsessive actions burden the patients until they are realized, others are not noticed by the patients themselves. Obsessive actions are painful for patients, especially in those cases when they become the object of attention of others. nine0003
Obsessive fears, or phobias, include an obsessive and senseless fear of heights, large streets, open or confined spaces, large crowds of people, the fear of sudden death, the fear of falling ill with one or another incurable disease. Some patients may develop a wide variety of phobias, sometimes acquiring the character of fear of everything (panphobia). And finally, an obsessive fear of the emergence of fears (phobophobia) is possible.
Hypochondriacal phobias (nosophobia) - an obsessive fear of some serious illness. Most often, cardio-, stroke-, syphilo- and AIDS phobias are observed, as well as the fear of the development of malignant tumors. At the peak of anxiety, patients sometimes lose their critical attitude to their condition - they turn to doctors of the appropriate profile, require examination and treatment. The implementation of hypochondriacal phobias occurs both in connection with psycho- and somatogenic (general non-mental illnesses) provocations, and spontaneously. As a rule, hypochondriacal neurosis develops as a result, accompanied by frequent visits to doctors and unreasonable medication. nine0003
Specific (isolated) phobias - obsessive fears limited to a strictly defined situation - fear of heights, nausea, thunderstorms, pets, treatment at the dentist, etc. Since contact with situations that cause fear is accompanied by intense anxiety, the patients tend to avoid them.
Obsessive fears are often accompanied by the development of rituals - actions that have the meaning of "magic" spells that are performed, despite the critical attitude of the patient to obsession, in order to protect against one or another imaginary misfortune: before starting any important business, the patient must perform some that specific action to eliminate the possibility of failure. Rituals can, for example, be expressed in snapping fingers, playing a melody to the patient or repeating certain phrases, etc. In these cases, even relatives are not aware of the existence of such disorders. Rituals, combined with obsessions, are a fairly stable system that usually exists for many years and even decades. nine0003
Obsessions of affectively neutral content - obsessive sophistication, obsessive counting, recalling neutral events, terms, formulations, etc. Despite their neutral content, they burden the patient, interfere with his intellectual activity.
Contrasting obsessions ("aggressive obsessions") - blasphemous, blasphemous thoughts, fear of harming oneself and others. Psychopathological formations of this group refer mainly to figurative obsessions with pronounced affective saturation and ideas that take possession of the consciousness of patients. They are distinguished by a sense of alienation, the absolute lack of motivation of the content, as well as a close combination with obsessive drives and actions. Patients with contrasting obsessions and complain of an irresistible desire to add endings to the replicas they have just heard, giving an unpleasant or threatening meaning to what has been said, to repeat after those around them, but with a touch of irony or malice, phrases of religious content, to shout out cynical words that contradict their own attitudes and generally accepted morality. , they may experience fear of losing control of themselves and possibly committing dangerous or ridiculous actions, injuring themselves or their loved ones. In the latter cases, obsessions are often combined with object phobias (fear of sharp objects - knives, forks, axes, etc.
). The contrasting group also partially includes obsessions of sexual content (obsessions of the type of forbidden ideas about perverted sexual acts, the objects of which are children, representatives of the same sex, animals). nine0003
Obsessions of pollution (mysophobia). This group of obsessions includes both the fear of pollution (earth, dust, urine, feces and other impurities), as well as the fear of penetration into the body of harmful and toxic substances (cement, fertilizers, toxic waste), small objects (glass fragments, needles, specific types of dust), microorganisms. In some cases, the fear of contamination can be limited, remain at the preclinical level for many years, manifesting itself only in some features of personal hygiene (frequent change of linen, repeated washing of hands) or in housekeeping (thorough handling of food, daily washing of floors). , "taboo" on pets). This kind of monophobia does not significantly affect the quality of life and is evaluated by others as habits (exaggerated cleanliness, excessive disgust). Clinically manifested variants of mysophobia belong to the group of severe obsessions. In these cases, gradually becoming more complex protective rituals come to the fore: avoiding sources of pollution and touching "unclean" objects, processing things that could get dirty, a certain sequence in the use of detergents and towels, which allows you to maintain "sterility" in the bathroom. Stay outside the apartment is also furnished with a series of protective measures: going out into the street in special clothing that covers the body as much as possible, special processing of wearable items upon returning home. In the later stages of the disease, patients, avoiding pollution, not only do not go out, but do not even leave their own room. In order to avoid contacts and contacts that are dangerous in terms of contamination, patients do not allow even their closest relatives to come near them. Mysophobia is also related to the fear of contracting a disease, which does not belong to the categories of hypochondriacal phobias, since it is not determined by fears that a person suffering from OCD has a particular disease.
In the foreground is the fear of a threat from the outside: the fear of pathogenic bacteria entering the body. Hence the development of appropriate protective actions. nine0003
A special place in the series of obsessions is occupied by obsessive actions in the form of isolated, monosymptomatic movement disorders. Among them, especially in childhood, tics predominate, which, unlike organically conditioned involuntary movements, are much more complex motor acts that have lost their original meaning. Tics sometimes give the impression of exaggerated physiological movements. This is a kind of caricature of certain motor acts, natural gestures. Patients suffering from tics can shake their heads (as if checking whether the hat fits well), make hand movements (as if discarding interfering hair), blink their eyes (as if getting rid of a mote). Along with obsessive tics, pathological habitual actions (lip biting, gnashing of teeth, spitting, etc.) are often observed, which differ from obsessive actions proper in the absence of a subjectively painful sense of persistence and experience them as alien, painful. Neurotic states characterized only by obsessive tics usually have a favorable prognosis. Appearing most often in preschool and primary school age, tics usually subside by the end of puberty. However, such disorders can also be more persistent, persist for many years and only partially change in manifestations. nine0003
The course of obsessive-compulsive disorder.
Unfortunately, chronization must be indicated as the most characteristic trend in the OCD dynamics. Cases of episodic manifestations of the disease and complete recovery are relatively rare. However, in many patients, especially with the development and preservation of one type of manifestation (agoraphobia, obsessive counting, ritual handwashing, etc.), a long-term stabilization of the condition is possible. In these cases, there is a gradual (usually in the second half of life) mitigation of psychopathological symptoms and social readaptation. For example, patients who experienced fear of traveling on certain types of transport, or public speaking, cease to feel flawed and work along with healthy people. In mild forms of OCD, the disease usually proceeds favorably (on an outpatient basis). The reverse development of symptoms occurs after 1 year - 5 years from the moment of manifestation. nine0003
More severe and complex OCDs such as phobias of infection, pollution, sharp objects, contrasting performances, multiple rituals, on the other hand, may become persistent, resistant to treatment, or show a tendency to recur with disorders that persist despite active therapy. Further negative dynamics of these conditions indicates a gradual complication of the clinical picture of the disease as a whole.
DIFFERENTIAL DIAGNOSIS
It is important to distinguish OCD from other disorders that involve compulsions and rituals. In some cases, obsessive-compulsive disorder must be differentiated from schizophrenia, especially when the obsessive thoughts are unusual in content (eg, mixed sexual and blasphemous themes) or the rituals are exceptionally eccentric. The development of a sluggish schizophrenic process cannot be ruled out with the growth of ritual formations, their persistence, the emergence of antagonistic tendencies in mental activity (inconsistency of thinking and actions), and the uniformity of emotional manifestations. Prolonged obsessional states of a complex structure must be distinguished from the manifestations of paroxysmal schizophrenia. Unlike neurotic obsessive states, they are usually accompanied by a sharply increasing anxiety, a significant expansion and systematization of the circle of obsessive associations, which acquire the character of obsessions of "special significance": previously indifferent objects, events, random remarks of others remind patients of the content of phobias, offensive thoughts and thereby acquire in their view a special, menacing significance. In such cases, it is necessary to consult a psychiatrist in order to exclude schizophrenia. It can also be difficult to differentiate between OCD and conditions with a predominance of generalized disorders, known as Gilles de la Tourette's syndrome. Tics in such cases are localized in the face, neck, upper and lower extremities and are accompanied by grimaces, opening the mouth, sticking out the tongue, and intense gesticulation.
In these cases, this syndrome can be excluded by the coarseness of movement disorders characteristic of it and more complex in structure and more severe mental disorders. nine0003
Genetic factors
Speaking about hereditary predisposition to OCD, it should be noted that obsessive-compulsive disorders are found in approximately 5-7% of parents of patients with such disorders. Although this figure is low, it is higher than in the general population. While the evidence for a hereditary predisposition to OCD is still uncertain, psychasthenic personality traits can be largely explained by genetic factors.
FORECAST
Approximately two-thirds of OCD patients improve within a year, more often by the end of this period. If the disease lasts more than a year, fluctuations are observed during its course - periods of exacerbations are interspersed with periods of improvement in health, lasting from several months to several years. The prognosis is worse if we are talking about a psychasthenic personality with severe symptoms of the disease, or if there are continuous stressful events in the patient's life. Severe cases can be extremely persistent; for example, a study of hospitalized patients with OCD found that three-quarters of them remained symptom-free 13 to 20 years later. nine0003
TREATMENT: BASIC METHODS AND APPROACHES
Despite the fact that OCD is a complex group of symptom complexes, the principles of treatment for them are the same. The most reliable and effective method of treating OCD is considered to be drug therapy, during which a strictly individual approach to each patient should be manifested, taking into account the characteristics of the manifestation of OCD, age, gender, and the presence of other diseases. In this regard, we must warn patients and their relatives against self-treatment. If any disorders similar to mental ones appear, it is necessary, first of all, to contact the specialists of the psycho-neurological dispensary at the place of residence or other psychiatric medical institutions to establish the correct diagnosis and prescribe competent adequate treatment. At the same time, it should be remembered that at present a visit to a psychiatrist does not threaten with any negative consequences - the infamous "accounting" was canceled more than 10 years ago and replaced by the concepts of consultative and medical care and dispensary observation. nine0003
When treating, it must be borne in mind that obsessive-compulsive disorders often have a fluctuating course with long periods of remission (improvement). The apparent suffering of the patient often seems to call for vigorous effective treatment, but the natural course of the condition must be kept in mind in order to avoid the typical error of over-intensive therapy. It is also important to consider that OCD is often accompanied by depression, the effective treatment of which often leads to an alleviation of obsessional symptoms. nine0003
The treatment of OCD begins with an explanation to the patient of the symptoms and, if necessary, with the reassurance that they are the initial manifestation of insanity (a common cause for concern for patients with obsessions). Those suffering from certain obsessions often involve other family members in their rituals, so relatives need to treat the patient firmly, but sympathetically, mitigating the symptoms as much as possible, and not aggravating it by excessive indulgence in the morbid fantasies of the patients. nine0003
Drug therapy
The following therapeutic approaches exist for the currently identified types of OCD. Of the pharmacological drugs for OCD, serotonergic antidepressants, anxiolytics (mainly benzodiazepine), beta-blockers (to stop autonomic manifestations), MAO inhibitors (reversible) and triazole benzodiazepines (alprazolam) are most often used. Anxiolytic drugs provide some short-term relief of symptoms, but should not be given for more than a few weeks at a time. If anxiolytic treatment is required for more than one to two months, small doses of tricyclic antidepressants or small antipsychotics sometimes help. The main link in the treatment regimen for OCD, overlapping with negative symptoms or ritualized obsessions, are atypical antipsychotics - risperidone, olanzapine, quetiapine, in combination with either SSRI antidepressants or other antidepressants - moclobemide, tianeptine, or with high-potency benzodiazepine derivatives ( alprazolam, clonazepam, bromazepam). nine0003
Any comorbid depressive disorder is treated with antidepressants at an adequate dose. There is evidence that one of the tricyclic antidepressants, clomipramine, has a specific effect on obsessive symptoms, but the results of a controlled clinical trial showed that the effect of this drug is insignificant and occurs only in patients with distinct depressive symptoms.
In cases where obsessive-phobic symptoms are observed within the framework of schizophrenia, intensive psychopharmacotherapy with proportional use of high doses of serotonergic antidepressants (fluoxetine, fluvoxamine, sertraline, paroxetine, citalopram) has the greatest effect. In some cases, it is advisable to connect traditional antipsychotics (small doses of haloperidol, trifluoperazine, fluanxol) and parenteral administration of benzodiazepine derivatives. nine0003
Psychotherapy
Behavioral psychotherapy
One of the main tasks of the specialist in the treatment of OCD is to establish fruitful cooperation with the patient. It is necessary to instill in the patient faith in the possibility of recovery, to overcome his prejudice against the "harm" caused by psychotropic drugs, to convey his conviction in the effectiveness of treatment, subject to the systematic observance of the prescribed prescriptions. The patient's faith in the possibility of healing must be supported in every possible way by the relatives of the OCD sufferer. If the patient has rituals, it must be remembered that improvement usually occurs when using a combination of the method of preventing a reaction with placing the patient in conditions that aggravate these rituals. Significant but not complete improvement can be expected in about two-thirds of patients with moderately heavy rituals. If, as a result of such treatment, the severity of rituals decreases, then, as a rule, the accompanying obsessive thoughts also recede. In panphobia, predominantly behavioral techniques are used to reduce sensitivity to phobic stimuli, supplemented by elements of emotionally supportive psychotherapy.
In cases where ritualized phobias predominate, along with desensitization, behavioral training is actively used to help overcome avoidant behavior. Behavioral therapy is significantly less effective for obsessive thoughts that are not accompanied by rituals. Thought-stopping has been used by some experts for many years, but its specific effect has not been convincingly proven. nine0003
Social rehabilitation
We have already noted that obsessive-compulsive disorder has a fluctuating (fluctuating) course and over time the patient's condition may improve regardless of which particular methods of treatment were used. Until recovery, patients can benefit from supportive conversations that provide continued hope for recovery. Psychotherapy in the complex of treatment and rehabilitation measures for patients with OCD is aimed at both correcting avoidant behavior and reducing sensitivity to phobic situations (behavioral therapy), as well as family psychotherapy to correct behavioral disorders and improve family relationships. If marital problems exacerbate symptoms, joint interviews with the spouse are indicated. Patients with panphobia (at the stage of the active course of the disease), due to the intensity and pathological persistence of symptoms, need both medical and social and labor rehabilitation. In this regard, it is important to determine adequate terms of treatment - long-term (at least 2 months) therapy in a hospital with subsequent continuation of the course on an outpatient basis, as well as taking measures to restore social ties, professional skills, family relationships. Social rehabilitation is a set of programs for teaching OCD patients how to behave rationally both at home and in a hospital setting. Rehabilitation is aimed at teaching social skills to properly interact with other people, vocational training, as well as skills necessary in everyday life. Psychotherapy helps patients, especially those who experience a sense of their own inferiority, treat themselves better and correctly, master ways to solve everyday problems, and gain confidence in their strength.
nine0003
All of these methods, when used judiciously, can increase the effectiveness of drug therapy, but are not capable of completely replacing drugs. It should be noted that explanatory psychotherapy does not always help, and some patients with OCD even worsen because such procedures encourage them to think painfully and unproductively about the subjects discussed in the course of treatment. Unfortunately, science still does not know how to cure mental illness once and for all. OCD often has a tendency to recur, which requires long-term prophylactic medication. nine0003
Obsessive-compulsive disorder | The CALDA Clinic
Treatment Options: Obsessive-Compulsive Disorder
Approximately 2-3 percent of all people have an obsessive-compulsive disorder at some time in their lives. Among them are many celebrities: “When I am under stress, the same thought constantly revolves in my head, because I am afraid that otherwise something bad will happen,” singer Camila Cabello admits to Cosmopolitan magazine. The star of the musical Mamma Mia, Amanda Seyfried, also openly admits her obsessive-compulsive disorder and explains that she treated him with antidepressants for more than eleven years. nine0003
What is obsessive-compulsive disorder?
Obsessive-compulsive disorder, formerly also called obsessive-compulsive disorder, is a serious mental illness. Patients perform repetitive unwanted actions and "rituals" accompanied by corresponding negative or dangerous thoughts. The disease usually begins around the age of 20. The first symptoms may also appear during puberty or during childhood. Even healthy people can experience temporary compulsions. For example, many people are familiar with anxious thoughts that arise after leaving the house, such as “Did I turn off the coffee maker, turn off the light, lock the door, etc.?”. Despite the fact that a person knows for sure that everything has been done, he has a short desire to double-check again. Most people manage to calm down in such a situation, and only a few really "bother". nine0003
More than just a fad
However, people with obsessive-compulsive disorder are usually quite aware that their obsessive thoughts are far from reality and exaggerated and that obsessive actions are useless or even harmful. However, unlike healthy people, they do not manage to reset this obsession. Patients who try to stop unwanted "rituals" experience a very strong tension that they cannot endure for a long time. Therefore, in order to reduce the internal pressure, they soon return to harmful thoughts and actions. Despite the fact that they are illogical and often quite unpleasant, the patient still returns to obsessive thoughts and compulsive actions again and again in a stereotypical manner for several days a week or even several times a day, often for hours. This creates a vicious circle that is extremely painful for the patient and greatly impairs the quality of his daily life, well-being and performance. nine0003
How does OCD manifest itself?
Obsessive-compulsive disorder can manifest itself in obsessive thoughts and/or obsessive actions (compulsions). In most cases, obsessive thoughts and compulsions occur at the same time. Depending on the primary symptoms, obsessive-compulsive disorder is divided into three types:
Obsessive-compulsive disorder. Important features:
- mostly intrusive thoughts or ruminations;
- mostly compulsive actions;
- mixed obsessive thoughts and actions.
. Intrusive thoughts are usually negative, distressing, and very disturbing to the person. They are often in the form of "mental spirals". In this sense, one can speak of obsessive thoughts. Intrusive thoughts are usually perceived by people as belonging to themselves. At the same time, a person in most cases recognizes the meaninglessness and uselessness of these thoughts. But he can't get rid of them. This can lead to the impossibility of making even simple everyday decisions, since it is necessary to first weigh all possible, including completely irrational, alternatives. Obsessive-compulsive thoughts are characterized by anxiety, threat, often contradiction and inconsistency with the situation in which the person is actually located. In particular, mental urges to act are often perceived as extremely frightening and are usually not put into practice. Typical examples of obsessive thoughts or compulsive impulses Obsessive Compulsive Disorder can also be characterized by repetitive rituals and activities that the patient cannot avoid. Typical examples: Fearing possible infections, patients wash their hands with soap and water many times a day, take a shower several times, rub their skin with hard brushes, constantly wash and change clothes, endlessly clean the apartment, disinfect doorknobs, work surfaces, objects, etc. nine0003 Items must be arranged, placed or assembled in a very specific order or manner. They must match a certain size, color, quantity, theme, symmetry, etc. This correspondence is regularly rechecked and infinitely corrected. The patient constantly checks to see if the door is locked, if the windows are closed, if electrical appliances are turned off, if the faucet is leaking, etc. nine0003 Because of the fear of throwing away something important, the patient accumulates everything, even unnecessary items and rubbish. If something is thrown away, there is often a strong urge to search the trash cans to make sure nothing important has been thrown away. In order to prevent imaginary dangers, catastrophes, etc., the patient is forced to repeat certain actions in a certain amount and in a certain order over and over again. This should help prevent the impending "danger". For example, the patient may forbid himself from touching certain tiles, stones, patterns, and so on. In more than 90%, that is, in the vast majority of cases, obsessive thoughts and obsessive actions occur simultaneously. This means that the majority of all patients suffer from obsessive-compulsive disorder, in which there are both painful obsessive-compulsive thoughts and stereotypical compulsive actions. Obsessive-compulsive disorder is not a quirk of some people who may appear slightly superstitious, overly clean, or especially tidy. This is a serious disease in which people cease to control their thoughts and actions, even if they really want to, and because of which they suffer painfully. It is not uncommon for sufferers to waste several hours a day performing compulsive acts and tormenting themselves with intrusive thoughts. The exact causes of OCD are not yet clearly understood. However, certain factors have been identified that are known to be particularly conducive to the development or maintenance of OCD. As a rule, the development of OKR requires the combination of several factors. The importance of individual factors for each individual patient is individual. The most important risk factors for developing obsessive-compulsive disorder are: Research shows that heredity does play a role in the development of OCD. Imaging has also shown that metabolism and brain activity in certain areas of the brain in people with obsessive-compulsive disorder is markedly increased. In particular, it was possible to detect anomalies in the basal ganglia, which, among other things, are responsible for motor processes. In addition, the balance of serotonin is disturbed. The environment in which a person grows up has a significant impact on the development of personality. A parenting style with high academic demands, strict assessment models, and perfectionist demands, as well as "fearful" parenting methods in which the child is overprotective and constantly protected from all sorts of adversity, can all contribute to the development of obsessive-compulsive disorders. Also important risk factors for the development of obsessive-compulsive disorders are experienced trauma or mental overload. Excessively stressful events such as violence, abuse, rape, death of a loved one, etc. can unsettle a person and often cause a strong sense of insecurity and insecurity. Understandably, there is also a growing desire for control and security. The performance of "protective", "neutralizing", or "cleansing" compulsions and rituals gives the sufferer a sense of control over a situation in which they would otherwise feel helpless. nine0003 Last but not least, individual personality structure also determines to some extent whether a person develops obsessive-compulsive disorder. People who are inherently fearful, vulnerable, unstable, or overly sensitive have a higher risk of developing obsessive-compulsive disorder than confident and calm individuals. Obsessive-compulsive disorders are often diagnosed together with other mental and dermatological diseases. The most common comorbidities associated with obsessive-compulsive disorder include: — Depressive moods and depressions — Eating disorders — Anxiety disorders — Social phobias Post-traumatic stress disorders0002 -Dermatillomania and trichotillomania impulse control disorders in which the patient repeatedly scratches, pinches and injures the skin or pulls out hair, eyebrows or eyelashes. - Dysmorphophobic disorder distorted perception of one's own body, in which a slight "anomaly" is regarded as a completely disfiguring feature, and there is an excessive concern for an imagined flaw. - Atopic dermatitis and other skin diseases eczema occurs mainly in compulsive washing syndrome due to persistent over-irritation of the skin. People with OCD know that their thoughts, actions, and rituals are irrational, but are unable to deal with them on their own. As a rule, they are very ashamed of this and try their best to hide their suffering from others. Therefore, obsessive-compulsive disorders are often diagnosed very late. On average, it takes 10 years for patients to seek professional help, but periods of 20 to 30 years are also not uncommon. Often patients are forced to see a doctor not even by the obsessive-compulsive disorder itself, but by a concomitant disease, such as severe dermatitis. At this stage, the disease has usually already taken root, and the symptoms have greatly increased both in number and severity. nine0003 As with most diseases, it is best to start treatment as early as possible if you have OCD. However, even at an extended stage, very good therapeutic results can still be achieved. Modern treatments for obsessive-compulsive disorder have so far mainly involved the use of psychotherapy and psychotropic drugs. Everything is different with us! The CALDA concept: Let us help you! As a client of the CALDA clinic, you are assigned a 1:1 individual therapy based on the CALDA concept, which is tailored specifically to your needs. It is a personalized, highly effective, holistically oriented, ultra-precise therapy: scientifically based methods of classical medicine are combined with specially approved therapies of complementary, traditional Chinese (TCM) and orthomolecular medicine. nine0003
Symptoms. Examples of obsessive thoughts
Obsessive Compulsive Disorder
or requires himself to take ten steps back fifty times, say a "special" saying seven times, and so on. nine0003
Obsessive-compulsive disorder with obsessive thoughts and actions
Obsessive-compulsive disorder: impact on daily life
This not only burdens daily life and reduces the patient's ability to work, but also has a huge impact on his social environment, i.e. parents, partners, children, etc. Normal life becomes impossible for long periods of time, causing close family members to leave at some point and marriages to fall apart. In addition to serious psychological and social consequences, there are usually complaints about the physical condition. Serious skin diseases can occur, especially when the disease is accompanied by an obsessive desire to wash and clean. nine0003
Causes of OCD
Although the disease is not directly transmitted, the risk of a child getting OCD has been shown to increase if one or both parents have OCD. This is also supported by the results of twin studies.
nine0003
Common comorbidities of obsessive-compulsive disorder
What are the treatments for OCD?
Complex causes require complex treatment at multiple levels
The multimodal approach, combining a variety of proven therapeutic options, has proven to be particularly effective. It allows you to accurately recognize many different individual causes of the disease and provide optimal treatment for the patient at every stage and at different levels. In addition, this technique allows you to recognize and effectively eliminate any individually caused physical problems and imbalances and professionally treat all associated diseases. nine0003