Obnoxious personality disorder
4 Ways to Deal with Obnoxious People
Source: Shutterstock
You're enjoying a social gathering when someone makes an unwanted comment that causes offense. Is it okay to call the person "obnoxious"?
Psychologists hesitate to use the term because it has no theoretical basis. Terms like that label a person, not a behavior. For our purposes here, however, we will consider any person or behavior "obnoxious" when it is deliberately offensive and makes others feel uncomfortable.
People engaging in this behavior do not self-regulate and so they may blurt out their inner feelings, regardless of the occasion. Here are some other typical examples:
- Someone continually plays pranks on friends, family, and co-workers, and it’s starting to get old. You no longer feel like laughing, nor does anyone else.
- A joker interrupts meetings, family gatherings, or casual conversations with friends to make a stream of witticisms, causing annoyance.
- A person frequently expresses racist, sexist, or ageist opinions in a public setting. Even if no one from the targeted category is present, the remarks offend others.
The University of Arizona’s Elizabeth Focella and colleagues (2015) examined methods to address and correct a biased individual who expresses opinions that offend both those present and the target of the prejudice. By applying some psychology to the situation, you can use the team's findings to foster more harmonious and fulfilling interactions.
Here, then, are 4 ways to respond to obnoxious people:
- Understand the source of your annoyance.
Consider whether your offense is realistic based on the gravity of the obnoxious behavior or a response to deep-seated insecurity that you have. Often, we experience "countertransference," used in psychodynamic psychotherapy, which distorts our perceptions of others due to our own insecurities. For example, you become enraged at a co-worker who pokes fun at the vacation photo you just put on your desk.
 The remark was not really that hostile, but it reminds you of your childhood feelings when your brother taunted you.
The remark was not really that hostile, but it reminds you of your childhood feelings when your brother taunted you. - Ignore the person or behavior.
People are more likely to act in ways that bring them some type of reinforcement. For people who behave in obnoxious ways, that reinforcement may be any form of attention. Is the person just wanting to elicit a reaction from others? Then make a pact with the other people in your group to refrain from laughing or paying any attention to the unwanted comments or actions. Without the desired response, the behavior may diminish on its own.
- Confront the person.
Focella and her team noted that direct confrontation can be effective in reducing someone else’s bias. However, for the confrontation to be effective in making the individual back off, we know that it should come from a person other than the target of that bias. For example, you’re a working woman at a group lunch where a man refuses to acknowledge that working women might be good mothers.
 As a working woman, if you point out the already compelling and still-mounting counter-evidence, you will engender that person’s dislike, extending and perhaps even exacerbating the "debate," and the unpleasantness for all, instead of quelling it. Strictly for the purpose of quieting the offending party, it would potentially be more effective for a non-working mother, or a man, to speak up.
As a working woman, if you point out the already compelling and still-mounting counter-evidence, you will engender that person’s dislike, extending and perhaps even exacerbating the "debate," and the unpleasantness for all, instead of quelling it. Strictly for the purpose of quieting the offending party, it would potentially be more effective for a non-working mother, or a man, to speak up. - Preserve the individual’s self-esteem.
According to Focella and her fellow researchers, people are more likely to change their prejudice if they first feel good about themselves. The Focella team recommends asking “self-affirming” questions of a person who you’re trying to "de-prejudice." For example, in the course of the conversation about working women, give the offending individual the opportunity to talk about what he perceives to be his greatest personal accomplishments. Bumping up an "obnoxious" individual's self-esteem may help him feel less threatened and he may alter his opinion, or at least drop the offending argument, so that everyone can move on.
Copyright Susan Krauss Whitbourne 2015
References
Focella, E. S., Bean, M. G., & Stone, J. (2015). Confrontation and beyond: Examining a stigmatized target's use of a prejudice reduction strategy. Social and Personality Psychology Compass, 9(2), 100-114. doi:10.1111/spc3.12153
7 Habits of Highly Obnoxious People
Obnoxious people rarely recognize themselves -- until they get tired, fired, or lonely. If you have one of these people in your workplace, stand clear until they get help. Otherwise, they create havoc and resentment for all concerned.
Let's face it: some people are off-putting. Unfortunately, they don't self-identify. They simply blunder through life either a) clashing with people, embroiled in conflict after conflict, or b) bouncing from relationship to relationship, lonely and confused about why they don't have close friends.
A few things can alter the picture so that obnoxious people have difficulty seeing themselves as others do: money, power, position and celebrity status. Often, those around obnoxious people will put up with nastiness or crass behavior because they like being seen with a celebrity, or they enjoy the benefits of the person's wealth or power.
Often, those around obnoxious people will put up with nastiness or crass behavior because they like being seen with a celebrity, or they enjoy the benefits of the person's wealth or power.
Advertisement
But obnoxious behavior grates on the nerves like fingernails on a whiteboard. Sooner or later, bystanders grit their teeth and wish them goodbye.
So how do these people irritate? Let me count the ways:
- Obnoxious people hog air time. Whether a face-to-face meeting, a teleconference, or a panel discussion, they monopolize. If someone reported their speaking time versus the total air time of all other participants, their obnoxious person's time would eclipse the air time of all the others involved.
 Typically, their "last word" goes something like this: "Well, mark my word." Or: "Just remember that I told you X." Or: "Don't say I didn't warn you!" "Have it your way, but don't blame me when you see the results."
Typically, their "last word" goes something like this: "Well, mark my word." Or: "Just remember that I told you X." Or: "Don't say I didn't warn you!" "Have it your way, but don't blame me when you see the results."Advertisement
 They simply give no thought to selecting a neutral word or phrase rather than the negative -- when the neutral would deliver the same clear message. They have no filter for what people in the cultural mainstream consider appropriate language for a civilized society. Rudeness is their rule-of-thumb. What they think or feel, they say. To them, nothing is sacred.
They simply give no thought to selecting a neutral word or phrase rather than the negative -- when the neutral would deliver the same clear message. They have no filter for what people in the cultural mainstream consider appropriate language for a civilized society. Rudeness is their rule-of-thumb. What they think or feel, they say. To them, nothing is sacred. As long as they hold the floor, no one else can be heard.
As long as they hold the floor, no one else can be heard.To repeat: Obnoxious people rarely recognize themselves -- until they get tired, fired, or lonely. If you have one of these people in your workplace, stand clear until they get help. Otherwise, they create havoc and resentment for all concerned.
CEO, BooherResearch.com Author of Communicate Like A Leader, Creating Personal Presence, What MORE Can I Say?
Popular in the Community
Trending
💊 Anancaste personality disorder: symptoms, diagnosis, 😷 treatment, prevention 🏥
Anancaste personality disorder (APD) is a mental disorder characterized by increased anxiety, anxiety, perfectionism, suspiciousness, hypertrophied fixation on details, stubbornness, excessive tendency to doubt, the desire for control, recurrent obsessive thoughts and actions (obsessions and compulsions).
Submit an application for diagnosis and treatment
I confirm that I accept the terms of consent to the processing of personal data.
Anancastic Personality Disorder (APD) is a mental disorder characterized by increased anxiety, anxiety, perfectionism, suspiciousness, hypertrophied fixation on details, stubbornness, excessive tendency to doubt, desire for control, recurrent obsessive thoughts and actions (obsessions and compulsions).
People suffering from anankastic personality disorder often suffer from anxiety-phobic disorders, experience difficulties with the emotional sphere of life, control over their own experiences and attitudes occupies an important place. Quite often, the cause of the development of this disorder is excessive demands on the child by parents to comply with high behavioral norms and standards, as well as certain "criteria of feeling and emotionality." Thus, anancaste disorder is a kind of protective mechanism that is formed in childhood, manifesting itself in personality traits. Anancaste personality disorder belongs to the group of obsessive-compulsive disorders (OCD), but has certain differences. This disorder refers to pathologies of character development with its inherent distinctive features of a personality disorder, and obsessive-compulsive disorder is a specific disease. Despite the similarity of symptoms, the dynamics and tactics of treatment of APD and OCD are fundamentally different.
Anancaste personality disorder belongs to the group of obsessive-compulsive disorders (OCD), but has certain differences. This disorder refers to pathologies of character development with its inherent distinctive features of a personality disorder, and obsessive-compulsive disorder is a specific disease. Despite the similarity of symptoms, the dynamics and tactics of treatment of APD and OCD are fundamentally different.
Causes of the anancaste disorder
Causes of anancaste disorder include:
- Genetic predisposition.
- Traumatic brain injuries at an early age and birth injuries of the head.
- Social factor. When parents from early childhood put increased pressure on the child, they force them to meet high standards, while prohibiting the manifestation of certain emotions, for example, weakness.
- Schizophrenia, autism, brain tumors and organic pathologies, epileptoid character accentuation, generalized anxiety disorder.
Symptoms of Anancaste Personality Disorder
Although Anancaste Personality Disorder is not a disease, the symptoms that appear are extremely difficult, and usually impossible, to be consciously controlled. Anancaste disorder in some of its manifestations has similar symptoms with schizophrenic disorders, autism, tumors and organic brain lesions, and may be a sign of these diseases. Symptoms of Anancastic Personality Disorder:
- Obsessive thoughts and actions (“did I close the door?”, “did I turn off the iron?”, wearing certain clothes on a certain day of the week, tics, twitches, etc.). He performs such rituals in order to avoid unpleasant consequences, most often far-fetched. They regularly reflect on the current situation, analyze their own actions. The patient considers these thoughts and actions tiresome, but cannot get rid of them.
- Excessive fixation on parts. Obsession with trifles interferes with anancasts in everyday life and at work, they come up with their own quality criteria, create special rules for housekeeping.
 It is almost impossible to convince them of the opposite, to make any changes to the existing procedure invented by them.
It is almost impossible to convince them of the opposite, to make any changes to the existing procedure invented by them. - Exaggerated sense of duty and responsibility, meticulousness, conscientiousness, utmost honesty, strict observance of rules and life priorities.
- Workaholism, perfectionism.
- Pathological craving for order, excessive accuracy and scrupulousness.
- Concerned about safety, striving for reliability in everything.
- Panic fear of losing control over oneself, fear of showing emotions and feelings. Disruptions in which a person is not able to "pull himself together" on his own.
- Stubbornness and rigidity of thinking (inflexibility).
- Tendency to keep old, unnecessary things for years.
- Almost no friends, leisure and entertainment.
- Too economical.
If symptoms of an anancaste disorder appear, it is necessary to seek qualified help from a psychiatrist.
Classification and stages of development of anankastic personality disorder
APD begins in childhood or adolescence. Throughout its course, it goes through a series of successive stages, which can be repeated and returned. Two main phases of personality disorders:
- compensation;
- decompensation.
In the compensation phase, APD features are smoothed out, bring minimal subjective discomfort, a person manages to get along with them. Often, for this, he adjusts his life accordingly: he forms around himself a safe environment of people who can support him and help him cope with anxieties and difficulties, he chooses a job with minimal responsibility (although people with APD can find a reason to worry everywhere), etc. In stabilizing the state and prolonging the compensation phase, psychotherapeutic work in a group or individually helps a lot. At the same time, the main method is the cognitive-behavioral (cognitive-behavioral) approach, which consists in working with the thoughts, feelings and behavior of a person. It helps people with APD:
It helps people with APD:
- to realize the degree of their anxiety, which brings them closer to reality, allows them to plan their lives more intelligently, avoid unnecessary stress;
- deal with anxious obsessions within one's consciousness;
- regain confidence in yourself, stabilize.
The decompensation phase is a period of exacerbation of non-adaptive personality traits, increased anxiety, doubts and indecision. This leads to severe subjective discomfort and prevents full adaptation in society. During these periods, people may experience depressive symptoms from incessant worries and anxieties, disrupt their relationships, and experience other social distress. The reason for the onset of the decompensation phase is usually "contact with death", i.e. an event that violates the psychological defenses of the individual (destroys the "illusion of immortality") and shows a person that death and suffering always walk next to him, and if you listen, you can "feel her cold, deathly breath in the back of my head. " In addition, social tests of identity, most often associated with puberty, can also decompensate such personalities.
" In addition, social tests of identity, most often associated with puberty, can also decompensate such personalities.
Diagnosis
Diagnosis is based on the person having the criteria for a personality disorder plus three or more of the following:
- Doubts. People with an anancaste personality disorder doubt everyone and everything, they are very cautious;
- Anancast perfectionism. Very often it serves as an obstacle to completing tasks. Such people are very conscientious, honest, petty and scrupulous. Preoccupied with production, no time for rest and interpersonal relationships;
- Detailing. Anancasters are preoccupied with the details, compiling a list of cases, studying the rules, keep order, are busy organizing their own and others' work, schedules. If the order of such a person is violated, he can be very upset, and even get sick;
- Pedantry. Anancasters are characterized by excessive pedantry in everything, and they are adherents of social conventions;
- People with anancaste personality disorder have a rigid and stubborn character;
- Anancast requires people to strictly follow all the rules.
 He seeks from others the strict implementation of all his recommendations and rules exactly as he does. It happens that the anancast is generally unacceptable for some work to be done by other people, nothing is alien to the human anancast, therefore suppressed thoughts and desires are constantly spinning in his head.
He seeks from others the strict implementation of all his recommendations and rules exactly as he does. It happens that the anancast is generally unacceptable for some work to be done by other people, nothing is alien to the human anancast, therefore suppressed thoughts and desires are constantly spinning in his head.
Treatment of an anancaste personality disorder
The basis of the treatment of an anancaste personality disorder is psychotherapy, which is aimed at softening and compensating for certain personality traits of the patient, and not at changing them. Among the methods of psychotherapeutic treatment of this disorder, the technique of introspection and behavioral therapy is used.
For breakdowns and severe forms of the disorder, drug therapy is prescribed. If this personality disorder is a consequence of a mental illness, then first of all the treatment is aimed at the causative disease. Quite often, anancasts suffer from depression, then a psychotherapist prescribes antidepressants. People with anancaste disorder on a conscious level willingly agree with all the recommendations of the attending physician, but on the unconscious level they show strong resistance. Close contact between the patient and the doctor is the key to effective treatment. The private psychiatric clinic IsraClinic employs the best specialists with many years of experience who have cured hundreds of patients. The doctors of the center are the authors of unique treatment methods, scientific works, professors of prestigious universities. An individual approach is carried out for each patient, taking into account all the characteristics of a person's personality. A significant advantage of IsraClinic is the absence of a language barrier, all the medical staff of the clinic is fluent in Russian.
Quite often, anancasts suffer from depression, then a psychotherapist prescribes antidepressants. People with anancaste disorder on a conscious level willingly agree with all the recommendations of the attending physician, but on the unconscious level they show strong resistance. Close contact between the patient and the doctor is the key to effective treatment. The private psychiatric clinic IsraClinic employs the best specialists with many years of experience who have cured hundreds of patients. The doctors of the center are the authors of unique treatment methods, scientific works, professors of prestigious universities. An individual approach is carried out for each patient, taking into account all the characteristics of a person's personality. A significant advantage of IsraClinic is the absence of a language barrier, all the medical staff of the clinic is fluent in Russian.
Possible complications and consequences
The main consequence of an anancaste personality disorder is a significant change and (or) deviation from the generally accepted behavioral norms and trends adopted in a particular social environment, accompanied by personal and social disintegration. Anancaste personality disorder often accompanies such mental illnesses as autism, manic-depressive psychosis, and schizophrenia. In this case, the formation of certain disorders in the actions, thinking and perception of others is noted, which leads to a deterioration in the quality of life of the patient and his immediate environment.
Anancaste personality disorder often accompanies such mental illnesses as autism, manic-depressive psychosis, and schizophrenia. In this case, the formation of certain disorders in the actions, thinking and perception of others is noted, which leads to a deterioration in the quality of life of the patient and his immediate environment.
Prognosis
Anancaste personality disorder has a positive prognosis and responds well to treatment, which allows people with this diagnosis to live a full life. In the absence of high-quality therapy, the patient will suffer from frequent breakdowns, during which the mechanisms that restrain emotions that have been hidden and suppressed for years are turned off. During such breakdowns, a person is unable to independently return to a normal state without the help of professionals.
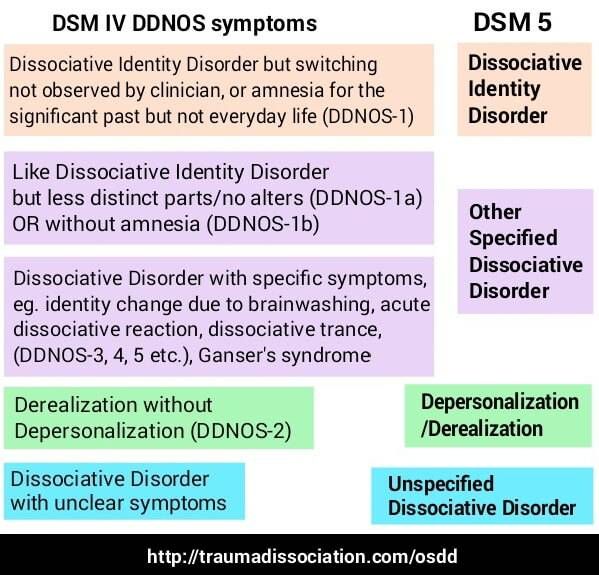
Dissociative identity disorder | Clinic Rehab Family
Dissociative identity disorder is a mental disorder in which a person self-identifies with multiple personalities. They seem to exist in him alone; each of them periodically dominates, determining his views, behavior and attitude towards himself as if other personalities were absent.
They seem to exist in him alone; each of them periodically dominates, determining his views, behavior and attitude towards himself as if other personalities were absent.
They may be of different genders, different ages and belong to different nationalities, each of them usually has its own name and biography. During the period of dominance of one of the personalities, the patient does not remember his original personality and is not aware of the existence of others. There is a tendency for a sudden transition from the dominance of one personality to another.
This disorder is also known as dissociative identity disorder, multiple personality disorder, split personality disorder, and multiple personality disorder. There are many names, but the essence is the same - a person with this disease may not even suspect that several characters live in his body at the same time.
In fact, this is a group of mental disorders, which are characterized by changes or disturbances in a number of mental functions - consciousness, memory, a sense of personal identity, awareness of the continuity of one's own identity. Dissociative disorder manifests itself involuntarily. The choice of this or that personality by the patient cannot be controlled.
Dissociative disorder manifests itself involuntarily. The choice of this or that personality by the patient cannot be controlled.
Symptoms of a dissociative disorder
The nature of the occurrence of this mental disorder most often comes down to a traumatic event in the past. It can be a terrorist act, an accident, military operations or violence. The splitting of the personality in this case becomes a manifestation of the body's defense mechanism.
Patients with a disorder feel as if they have become witnesses to the actions of others, observers from the outside. They perceive themselves and their bodies differently.
In general, there are two main features of a dissociative disorder:
- The presence of at least two personalities who would regularly take turns controlling the behavior of the individual.
- Memory loss that goes beyond normal forgetfulness and is described as a "switch".
Usually, memory loss in a disorder is not long-term and ends with a complete recovery. The disorder is more common in young women. Symptoms and signs of dissociative identity disorder should be a reason for a person to see a doctor.
The disorder is more common in young women. Symptoms and signs of dissociative identity disorder should be a reason for a person to see a doctor.
Causes of dissociative disorder
In most cases, the causes of this disorder are severe emotional trauma in early childhood, repeated physical, sexual or emotional abuse.
The human mind builds dissociations as a defense - this helps to separate traumatic memories and thoughts. No matter how hard a person tries to forget an unpleasant event, it pops up in the subconscious under the influence of triggers. Some things, people, events that bring back memories of psychological trauma can act in their role.
The causes of dissociative disorder can be:
- the influence of parents or other relatives who had a split personality;
- predisposition to multiple personality;
- abuse of others, lack of support;
- physical, emotional or sexual abuse.
It is important to note that children are not born with a holistic personality - it is formed into a single whole under the influence of biological and social factors. If the child grows up in an atmosphere of cruelty, then dissociative personality disorder may manifest itself at an older age.
If the child grows up in an atmosphere of cruelty, then dissociative personality disorder may manifest itself at an older age.
Other reasons include traumatic events at a conscious age (even if a person grew up in a healthy environment). For example, assault, car and plane crashes, natural disasters, war, participation in hostilities, rape.
Patients with an unstable psyche are also at risk - those who are diagnosed with incurable diseases, as well as people who abuse psychotropic substances. Dissociative mental disorders are not uncommon in people taking hallucinogens.
Classification of dissociative disorder
There are two main forms of mental disorder - possessed and unpossessed.
The first is characterized by a sudden change in behavior that is noticeable to the naked eye by those who know the person well. Each of the third-party personalities has a whole story - the patient may not introduce himself by his own name, behave in an unusual way. The clearest example is demonic possession. From the outside, it seems that someone has moved into the patient, he speaks in a different voice, performs non-standard actions. The possessed form very often has religious overtones.
Each of the third-party personalities has a whole story - the patient may not introduce himself by his own name, behave in an unusual way. The clearest example is demonic possession. From the outside, it seems that someone has moved into the patient, he speaks in a different voice, performs non-standard actions. The possessed form very often has religious overtones.
The second type of dissociative disorder is not as clearly distinguishable as the first. According to patients, they observe themselves as if from the outside, they cannot interfere with the behavior of an outsider and control their body as they want. At the same time, there is a clear feeling of a change in gender, age. Thoughts and feelings are also observed that were not previously characteristic of a person. There may be a temper tantrum in a temperamentally calm person or a sudden desire to change appearance. These are all the initial signs of a plurality of personality.
The more traditional form includes 7 states, each of which has its own characteristics.
- dissociative fugue. It is marked by complete depersonalization of the subject - a person can leave home, completely forget about who he is. There are two options for the development of events - either a state of confusion, a misunderstanding of what is happening, or a complete identification of oneself with a new personality. In the advanced form of fugue, patients can form a new family, get another job, or move to a new place of residence. When the true identity returns, the person suddenly finds himself in an unfamiliar place, next to strangers. Interestingly, during the period of personality change, the patient does not suspect that something has changed, he feels organic, and he turns to the doctor only when the memory of the original personality is restored.
- dissociative amnesia. It is more common than other forms of dissociative disorders. With it, the patient may partially or completely lose memory. At the same time, the person is quite clearly aware that he is in a state of amnesia.
 Usually it is caused by stressful or tragic situations. Patients are well oriented in their own personality, but cannot restore the events that have occurred.
Usually it is caused by stressful or tragic situations. Patients are well oriented in their own personality, but cannot restore the events that have occurred. - Trance and possession. This type of disorder is diagnosed in clergy, mediums. A person experiences confusion, as if he falls into a stupor, does not understand where he is and who he is. These are usually short episodes. They can occur with monotony and in situations that involve a loss of orientation in space. For example, aircraft pilots, drivers.
- Dissociative identity disorder. With this type of dissociative mental disorder, individuals of a different gender and age make themselves felt. For example, an adult has the behavior of a child. This form is connected with childhood - mistreatment, violence affects. In this case, many personalities come together to protect the original one. The transition to it occurs abruptly, and the patient cannot remember what happened during that period of time when side personalities predominated.
- Depersonalization disorder. Here a personality is manifested that cannot be defined as a specific person with a history. The patient may associate himself with a robot, extraterrestrial intelligence, or feel like a hero of a dream. This acute dissociative disorder destabilizes all spheres of life - a person cannot control his thoughts, body, feels like an outside observer.
- dissociative convulsions. These are similar to epileptic seizures, which are an imitation of a brain disease. The patient may twitch as if in convulsions, but unlike epilepsy, he will not bite his tongue and lose consciousness.
- Dissociative disorders of movement and sensation. The patient has a complete or partial loss of mobility, he does not respond to external stimuli, but consciousness is preserved.
Separately, it is worth highlighting organic dissociative disorder. With it, all the same symptoms are observed as with other forms of the disorder, but the reason for its occurrence is traumatic situations that are accompanied by damage to the brain. It can be provoked by traumatic brain injury, damage to brain neurons, and women during menopause are also susceptible to this type.
It can be provoked by traumatic brain injury, damage to brain neurons, and women during menopause are also susceptible to this type.
Complications of the disease
A patient with a disease may primarily harm himself during a change of personality. It is not known what qualities the new entity may have - perhaps it is suicidal.
Among the complications of dissociative disorder, it can be noted that the patient becomes potentially dangerous to society. It is not known what strategy of behavior the new personality will choose. She may be prone to overeating (this is fraught with disruption of the gastrointestinal tract), strive for extreme sports (this is traumatic, an unprepared person can easily get fractures and bruises), and convulsions with certain varieties can also cause injury - a person involuntarily twitches, falls to the floor .
Against the background of DID, depression can develop, which will lead to sleep disturbance, followed by malfunctions in the work of all systems and organs.
When to see a doctor
In the ICD, dissociative personality disorder occupies an entire section (F 44.8), which means that a specialist should deal with this violation. The slightest deviation from normal behavior (even according to close people) is a reason to visit a specialist.
If a person notices non-standard behavior, feels like an observer in his own body, or cannot remember some segments of his life, then it is likely that he is diagnosed with DID.
It is important to listen to loved ones who notice changes in the person's habitual state, and not try to cope with dissociative conversion disorders on their own.
Disease diagnosis
The initial task of a specialist in the diagnosis of DID is to exclude any organic brain damage. To do this, after clarifying the symptoms, the patient is sent for an MRI and CT scan of the brain. The same study helps the doctor rule out schizophrenia, epilepsy, dementia, and bipolar disorder.
It is also important to determine whether a person is faking or not. To do this, the survey must necessarily include an anamnesis and a survey that helps to establish the presence of traumatic situations and assess the patient's family relationships in childhood.
Also, for the diagnosis of dissociative disorder, constant monitoring of a person is necessary. At this point, it is also important to take into account the feedback of the patient's close people, because in a state of amnesia, a person himself is not able to remember whether personality splits occurred at some moments.
Diagnosis of the disease in children also includes a mandatory survey. If a child has fictitious friends, then this may be just a fantasy game. But observation at this age is also important.
Some doctors use hypnosis, during the dive they can discover other personalities in themselves, or the person himself recalls a situation in which he behaved outside the box. Amytal-caffeine disinhibition helps to achieve the same effect.
Treatment
Treatment for dissociative disorder does not have an established regimen. However, most specialists focus on psychotherapy, and the direction is chosen depending on the type of DID. It can be family, group, cognitive therapy or the already mentioned hypnosis.
During the sessions, the doctor aims to change the patient's thinking, work out stereotypes and eliminate them.
Medications help to alleviate the condition - tranquilizers and antidepressants, which are prescribed only in advanced cases. Medicines relieve depression, if necessary, restore sleep. They are selected for each patient individually.
Physiotherapy may be prescribed as maintenance therapy in the treatment of dissociative identity disorder.
Unfortunately, it is believed that DID is not completely cured, but some forms can still be corrected, and in patients with fugue and amnesia, recovery occurs quite quickly. The main thing is to ensure that the acute form does not turn into a chronic one.
+7 (495) 121-48-31
Prevention of disorder
To date, there are no measures that can prevent this mental disorder. Therefore, it is so important to track the disease in time at the initial stage.
Recommendations for dissociative disorder include regular visits to the doctor if there are predisposing factors for DID and, if possible, maintaining mental health.
References:
- Abolin L.M. Psychological mechanisms of human emotional stability. Kazan: Ed. Kazan University, 1987
- Gilligan S. Therapeutic trances. Guide to Ericksonian therapy. M.: Independent firm "Class", 1997
- Grof S. Beyond the Brain. M.: Ed. Transpersonal Institute, 1993
- Jones E. The Life and Works of Sigmund Freud. M.: Humanitarian, 1997
- Diekman H. Methods in analytical psychology. M.: OOO "TSGL" RON ", 2001
- Dmitrieva T.B. (ed.) Clinical Psychiatry. M.: GOETAR MEDICINE, 1998
- Enikolopov S.