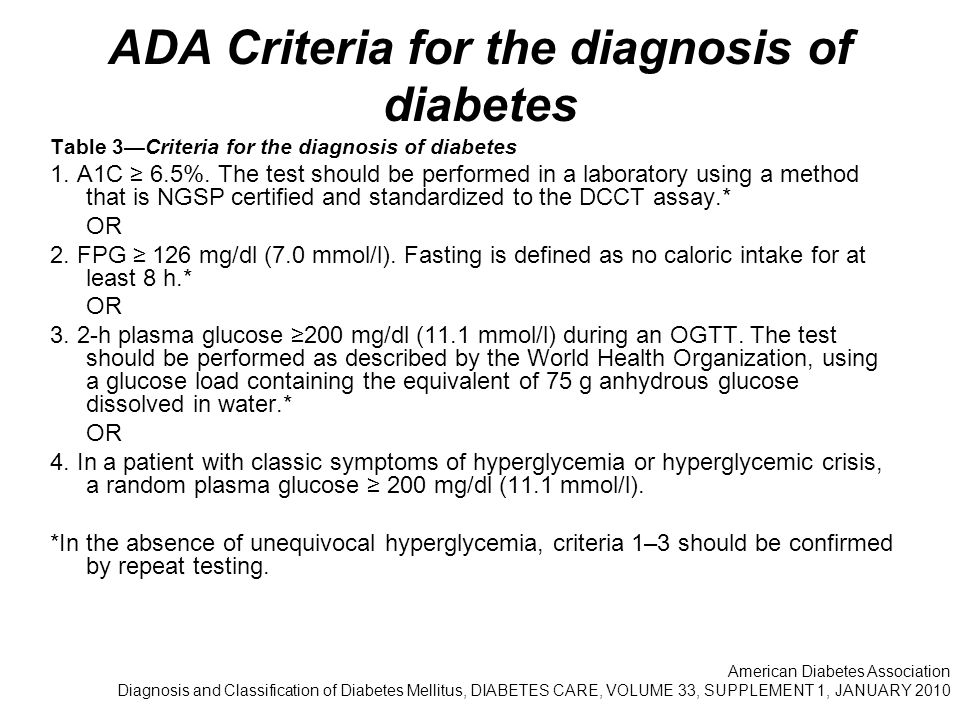
Narcolepsy criteria for diagnosis
Narcolepsy: Practice Essentials, Background, Pathophysiology
Vendrame M, Havaligi N, Matadeen-Ali C, Adams R, Kothare SV. Narcolepsy in children: a single-center clinical experience. Pediatr Neurol. 2008 May. 38(5):314-20. [QxMD MEDLINE Link].
Plazzi G, Serra L, Ferri R. Nocturnal aspects of narcolepsy with cataplexy. Sleep Med Rev. 2008 Apr. 12(2):109-28. [QxMD MEDLINE Link].
Palaia V, Poli F, Pizza F, Antelmi E, Franceschini C, Moghadam KK, et al. Narcolepsy with cataplexy associated with nocturnal compulsive behaviors: a case-control study. Sleep. 2011 Oct 1. 34(10):1365-71. [QxMD MEDLINE Link]. [Full Text].
Plazzi G, Pizza F, Palaia V, Franceschini C, Poli F, Moghadam KK, et al. Complex movement disorders at disease onset in childhood narcolepsy with cataplexy.
Brain. 2011 Dec. 134:3480-92. [QxMD MEDLINE Link]. [Full Text].
Rogers AE, Aldrich MS, Lin X. A comparison of three different sleep schedules for reducing daytime sleepiness in narcolepsy. Sleep. 2001 Jun 15. 24(4):385-91. [QxMD MEDLINE Link].
Benbadis SR. Effective treatment of narcolepsy with codeine in a patient receiving hemodialysis. Pharmacotherapy. 1996 May-Jun. 16(3):463-5. [QxMD MEDLINE Link].
Szakacs Z, Dauvilliers Y, Mikhaylov V, Poverennova I, Krylov S, Jankovic S, et al. Safety and efficacy of pitolisant on cataplexy in patients with narcolepsy: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2017 Mar. 16 (3):200-207. [QxMD MEDLINE Link].
Wakix (pitolisant) [package insert]. Plymouth Meeting, PA: Harmony Biosciences, LLC.
 August, 2019. Available at [Full Text].
August, 2019. Available at [Full Text].American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013. 372-78.
American Academy of Sleep Medicine. The International Classification of Sleep Disorders-Revised: Diagnostic and Coding Manual. 3rd ed. Rochester, MN: American Academy of Sleep Medicine; 2014.
Ruoff C, Rye D. The ICSD-3 and DSM-5 guidelines for diagnosing narcolepsy: clinical relevance and practicality. Curr Med Res Opin. 2016 Jul 20. 1-12. [QxMD MEDLINE Link].
American Academy of Sleep Medicine. International Classification of Sleep Disorders,. 2nd ed. Darien, IL: American Academy of Sleep Medicine.; 2005.
webmd.com">Naumann A, Daum I. Narcolepsy: Pathophysiology and neuropsychological changes. Behav Neurol. 2003. 14(3,4):89-98. [QxMD MEDLINE Link].
Burgess CR, Scammell TE. Narcolepsy: neural mechanisms of sleepiness and cataplexy. J Neurosci. 2012 Sep 5. 32(36):12305-11. [QxMD MEDLINE Link]. [Full Text].
Lin L, Faraco J, Li R, et al. The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell. 1999 Aug 6. 98(3):365-76. [QxMD MEDLINE Link].
Chemelli RM, Willie JT, Sinton CM, Elmquist JK, Scammell T, Lee C, et al. Narcolepsy in orexin knockout mice: molecular genetics of sleep regulation. Cell. 1999 Aug 20. 98(4):437-51. [QxMD MEDLINE Link].
Diniz Behn CG, Klerman EB, Mochizuki T, Lin SC, Scammell TE.
 Abnormal sleep/wake dynamics in orexin knockout mice. Sleep. 2010 Mar. 33(3):297-306. [QxMD MEDLINE Link]. [Full Text].
Abnormal sleep/wake dynamics in orexin knockout mice. Sleep. 2010 Mar. 33(3):297-306. [QxMD MEDLINE Link]. [Full Text].Mignot E, Lammers GJ, Ripley B, Okun M, Nevsimalova S, Overeem S, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002 Oct. 59(10):1553-62. [QxMD MEDLINE Link].
Partinen M, Saarenpää-Heikkilä O, Ilveskoski I, Hublin C, Linna M, Olsén P, et al. Increased incidence and clinical picture of childhood narcolepsy following the 2009 h2N1 pandemic vaccination campaign in Finland. PLoS One. 2012. 7(3):e33723. [QxMD MEDLINE Link]. [Full Text].
Nohynek H, Jokinen J, Partinen M, Vaarala O, Kirjavainen T, Sundman J, et al. AS03 adjuvanted Ah2N1 vaccine associated with an abrupt increase in the incidence of childhood narcolepsy in Finland.
 PLoS One. 2012. 7(3):e33536. [QxMD MEDLINE Link]. [Full Text].
PLoS One. 2012. 7(3):e33536. [QxMD MEDLINE Link]. [Full Text].Abad VC, Guilleminault C. Review of rapid eye movement behavior sleep disorders. Curr Neurol Neurosci Rep. 2004 Mar. 4(2):157-63. [QxMD MEDLINE Link].
Mignot E, Lammers GJ, Ripley B, Okun M, Nevsimalova S, Overeem S, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002 Oct. 59(10):1553-62. [QxMD MEDLINE Link].
Thannickal TC, Moore RY, Nienhuis R, Ramanathan L, Gulyani S, Aldrich M, et al. Reduced number of hypocretin neurons in human narcolepsy. Neuron. 2000 Sep. 27(3):469-74. [QxMD MEDLINE Link].
Thannickal TC, Nienhuis R, Siegel JM. Localized loss of hypocretin (orexin) cells in narcolepsy without cataplexy.
 Sleep. 2009 Aug 1. 32(8):993-8. [QxMD MEDLINE Link]. [Full Text].
Sleep. 2009 Aug 1. 32(8):993-8. [QxMD MEDLINE Link]. [Full Text].Blouin AM, Thannickal TC, Worley PF, Baraban JM, Reti IM, Siegel JM. Narp immunostaining of human hypocretin (orexin) neurons: loss in narcolepsy. Neurology. 2005 Oct 25. 65(8):1189-92. [QxMD MEDLINE Link].
Nishino S, Sakurai E, Nevsimalova S, Yoshida Y, Watanabe T, Yanai K. Decreased CSF histamine in narcolepsy with and without low CSF hypocretin-1 in comparison to healthy controls. Sleep. 2009 Feb 1. 32(2):175-80. [QxMD MEDLINE Link]. [Full Text].
Kanbayashi T, Kodama T, Kondo H, Satoh S, Inoue Y, Chiba S. CSF histamine contents in narcolepsy, idiopathic hypersomnia and obstructive sleep apnea syndrome. Sleep. 2009 Feb 1. 32(2):181-7. [QxMD MEDLINE Link]. [Full Text].
Overeem S, Black JL 3rd, Lammers GJ. Narcolepsy: immunological aspects. Sleep Med Rev. 2008 Apr. 12(2):95-107. [QxMD MEDLINE Link].
Cvetkovic-Lopes V, Bayer L, Dorsaz S, Maret S, Pradervand S, Dauvilliers Y, et al. Elevated Tribbles homolog 2-specific antibody levels in narcolepsy patients. J Clin Invest. 2010 Mar. 120(3):713-9. [QxMD MEDLINE Link]. [Full Text].
Dauvilliers Y, Abril B, Mas E, Michel F, Tafti M. Normalization of hypocretin-1 in narcolepsy after intravenous immunoglobulin treatment. Neurology. 2009 Oct 20. 73(16):1333-4. [QxMD MEDLINE Link].
Knudsen S, Mikkelsen JD, Bang B, Gammeltoft S, Jennum PJ. Intravenous immunoglobulin treatment and screening for hypocretin neuron-specific autoantibodies in recent onset childhood narcolepsy with cataplexy. Neuropediatrics.
 2010 Oct. 41(5):217-22. [QxMD MEDLINE Link].
2010 Oct. 41(5):217-22. [QxMD MEDLINE Link]. Sehgal A, Mignot E. Genetics of sleep and sleep disorders. Cell. 2011 Jul 22. 146(2):194-207. [QxMD MEDLINE Link]. [Full Text].
Mignot E. Sleep, sleep disorders and hypocretin (orexin). Sleep Med. 2004 Jun. 5 Suppl 1:S2-8. [QxMD MEDLINE Link].
Weiner Lachmi K, Lin L, Kornum BR, Rico T, Lo B, Aran A, et al. DQB1*06:02 allele-specific expression varies by allelic dosage, not narcolepsy status. Hum Immunol. 2012 Apr. 73(4):405-10. [QxMD MEDLINE Link]. [Full Text].
Hor H, Kutalik Z, Dauvilliers Y, Valsesia A, Lammers GJ, Donjacour CE, et al. Genome-wide association study identifies new HLA class II haplotypes strongly protective against narcolepsy. Nat Genet. 2010 Sep. 42(9):786-9.
 [QxMD MEDLINE Link].
[QxMD MEDLINE Link]. Hallmayer J, Faraco J, Lin L, Hesselson S, Winkelmann J, Kawashima M, et al. Narcolepsy is strongly associated with the T-cell receptor alpha locus. Nat Genet. 2009 Jun. 41(6):708-11. [QxMD MEDLINE Link]. [Full Text].
Kornum BR, Kawashima M, Faraco J, Lin L, Rico TJ, Hesselson S, et al. Common variants in P2RY11 are associated with narcolepsy. Nat Genet. 2011 Jan. 43(1):66-71. [QxMD MEDLINE Link]. [Full Text].
Shimada M, Miyagawa T, Kawashima M, Tanaka S, Honda Y, Honda M, et al. An approach based on a genome-wide association study reveals candidate loci for narcolepsy. Hum Genet. 2010 Oct. 128(4):433-41. [QxMD MEDLINE Link].
Longstreth WT Jr, Koepsell TD, Ton TG, Hendrickson AF, van Belle G. The epidemiology of narcolepsy.
 Sleep. 2007 Jan 1. 30(1):13-26. [QxMD MEDLINE Link].
Sleep. 2007 Jan 1. 30(1):13-26. [QxMD MEDLINE Link]. Silber MH, Krahn LE, Olson EJ, Pankratz VS. The epidemiology of narcolepsy in Olmsted County, Minnesota: a population-based study. Sleep. 2002 Mar 15. 25(2):197-202. [QxMD MEDLINE Link].
Dauvilliers Y, Arnulf I, Mignot E. Narcolepsy with cataplexy. Lancet. 2007 Feb 10. 369(9560):499-511. [QxMD MEDLINE Link].
Doherty L, Crowe C, Sweeney B. National narcolepsy survey. Ir Med J. 2010 Apr. 103(4):110, 112-3. [QxMD MEDLINE Link].
Douglas NJ. The psychosocial aspects of narcolepsy. Neurology. 1998 Feb. 50(2 Suppl 1):S27-30. [QxMD MEDLINE Link].
Pakola SJ, Dinges DF, Pack AI. Review of regulations and guidelines for commercial and noncommercial drivers with sleep apnea and narcolepsy.
 Sleep. 1995 Nov. 18(9):787-96. [QxMD MEDLINE Link].
Sleep. 1995 Nov. 18(9):787-96. [QxMD MEDLINE Link]. Prasad M, Setty G, Ponnusamy A, Hussain N, Desurkar A. Cataplectic facies: clinical marker in the diagnosis of childhood narcolepsy-report of two cases. Pediatr Neurol. 2014 May. 50 (5):515-7. [QxMD MEDLINE Link].
Guilleminault C, Pelayo R. Narcolepsy in prepubertal children. Ann Neurol. 1998 Jan. 43(1):135-42. [QxMD MEDLINE Link].
Bassetti C, Aldrich MS, Quint DJ. MRI findings in narcolepsy. Sleep. 1997 Aug. 20(8):630-1. [QxMD MEDLINE Link].
Melberg A, Hetta J, Dahl N, et al. Autosomal dominant cerebellar ataxia deafness and narcolepsy. J Neurol Sci. 1995 Dec. 134(1-2):119-29. [QxMD MEDLINE Link].
Dauvilliers Y, Baumann CR, Carlander B, Bischof M, Blatter T, Lecendreux M, et al.
 CSF hypocretin-1 levels in narcolepsy, Kleine-Levin syndrome, and other hypersomnias and neurological conditions. J Neurol Neurosurg Psychiatry. 2003 Dec. 74(12):1667-73. [QxMD MEDLINE Link].
CSF hypocretin-1 levels in narcolepsy, Kleine-Levin syndrome, and other hypersomnias and neurological conditions. J Neurol Neurosurg Psychiatry. 2003 Dec. 74(12):1667-73. [QxMD MEDLINE Link]. Vossler DG, Wyler AR, Wilkus RJ, et al. Cataplexy and monoamine oxidase deficiency in Norrie disease. Neurology. 1996 May. 46(5):1258-61. [QxMD MEDLINE Link].
Maeda M, Tamaoka A, Hayashi A, et al. [A case of HLA-DR2, DQw1 negative post-traumatic narcolepsy]. Rinsho Shinkeigaku. 1995 Jul. 35(7):811-3. [QxMD MEDLINE Link].
Fry JM. Treatment modalities for narcolepsy. Neurology. 1998 Feb. 50(2 Suppl 1):S43-8. [QxMD MEDLINE Link].
US Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy.
 Neurology. 2000 Mar 14. 54(5):1166-75. [QxMD MEDLINE Link].
Neurology. 2000 Mar 14. 54(5):1166-75. [QxMD MEDLINE Link]. Golicki D, Bala MM, Niewada M, Wierzbicka A. Modafinil for narcolepsy: systematic review and meta-analysis. Med Sci Monit. 2010 Aug. 16(8):RA177-86. [QxMD MEDLINE Link].
The Nuvigil website. Available at http://www.nuvigil.com/. Accessed: 12/8/2009.
Thorpy MJ, Shapiro C, Mayer G, Corser BC, Emsellem H, Plazzi G, et al. A randomized study of solriamfetol for excessive sleepiness in narcolepsy. Ann Neurol. 2019 Mar. 85 (3):359-370. [QxMD MEDLINE Link].
Xyrem Web site. Available at https://www.xyrem.com/.
Lockrane B, Bhatia P, Gore R. Successful treatment of narcolepsy and cataplexy: A review. Can Respir J.
 2005 May-Jun. 12(4):225-7. [QxMD MEDLINE Link].
2005 May-Jun. 12(4):225-7. [QxMD MEDLINE Link]. Black J, Pardi D, Hornfeldt CS, Inhaber N. The nightly use of sodium oxybate is associated with a reduction in nocturnal sleep disruption: a double-blind, placebo-controlled study in patients with narcolepsy. J Clin Sleep Med. 2010 Dec 15. 6(6):596-602. [QxMD MEDLINE Link]. [Full Text].
Xywav [package insert]. Palo Alto, CA: Jazz Pharmaceuticals, Inc. July 2020. Available at [Full Text].
Vignatelli L, D'Alessandro R, Candelise L. Antidepressant drugs for narcolepsy. Cochrane Database Syst Rev. 2005 Jul 20. CD003724. [QxMD MEDLINE Link].
[Guideline] Morgenthaler TI, Kapur VK, Brown T, Swick TJ, Alessi C, Aurora RN, et al. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin.
 Sleep. 2007 Dec. 30(12):1705-11. [QxMD MEDLINE Link]. [Full Text].
Sleep. 2007 Dec. 30(12):1705-11. [QxMD MEDLINE Link]. [Full Text].Spencer TJ, Madras BK, Bonab AA, Dougherty DD, Clarke A, Mirto T, et al. A positron emission tomography study examining the dopaminergic activity of armodafinil in adults using [¹¹C]altropane and [¹¹C]raclopride. Biol Psychiatry. 2010 Nov 15. 68(10):964-70. [QxMD MEDLINE Link].
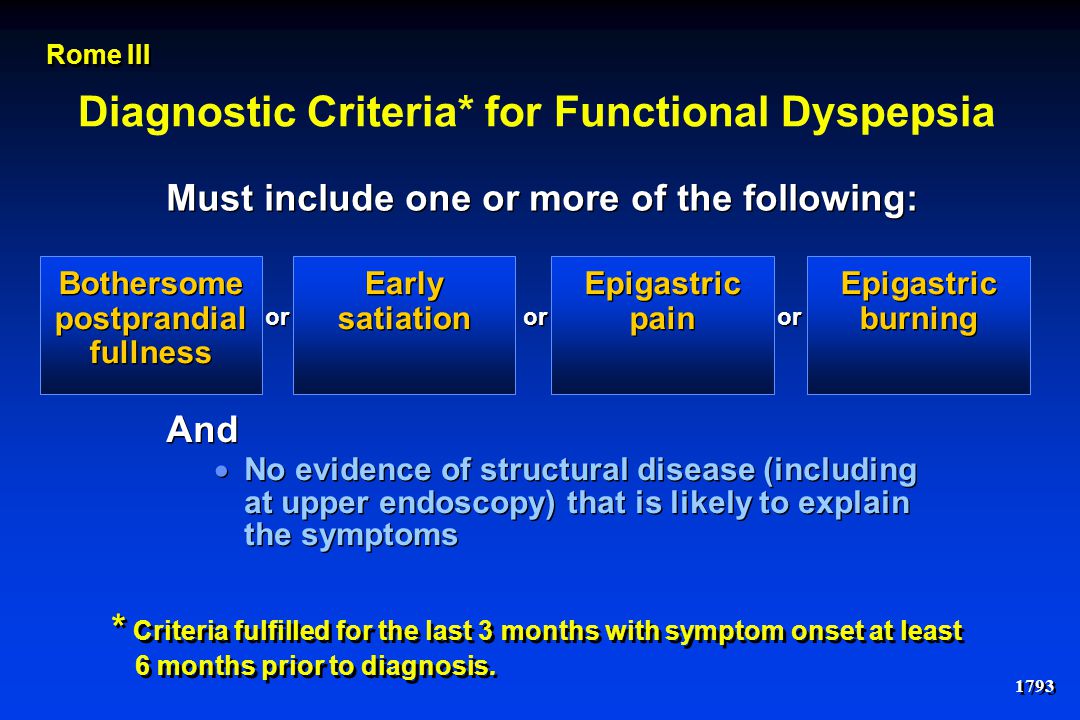
ICSD-3 Narcolepsy Type 2 Diagnostic Criteria
INDICATIONS AND USAGE
XYREM® (sodium oxybate) oral solution, 0.5 g/mL is indicated for the treatment of cataplexy or excessive daytime sleepiness (EDS) in patients 7 years of age and older with narcolepsy.
Important Safety Information
CONTRAINDICATIONS
XYREM is contraindicated for use in:
- combination with sedative hypnotics or alcohol
- patients with succinic semialdehyde dehydrogenase deficiency.
WARNINGS AND PRECAUTIONS
Central Nervous System Depression
The concurrent use of XYREM with other CNS depressants, including but not limited to opioid analgesics, benzodiazepines, sedating antidepressants or antipsychotics, sedating anti-epileptic drugs, general anesthetics, muscle relaxants, and/or illicit CNS depressants, may increase the risk of respiratory depression, hypotension, profound sedation, syncope, and death. If use of these CNS depressants in combination with XYREM is required, dose reduction or discontinuation of one or more CNS depressants (including XYREM) should be considered. In addition, if short-term use of an opioid (eg, post- or perioperative) is required, interruption of treatment with XYREM should be considered.
After first initiating treatment and until certain that XYREM does not affect them adversely (eg, impair judgment, thinking, or motor skills), caution patients against hazardous activities requiring complete mental alertness or motor coordination such as operating hazardous machinery, including automobiles or airplanes. Also caution patients against these hazardous activities for at least 6 hours after taking XYREM. Patients should be queried about CNS depression-related events upon initiation of XYREM therapy and periodically thereafter.
Also caution patients against these hazardous activities for at least 6 hours after taking XYREM. Patients should be queried about CNS depression-related events upon initiation of XYREM therapy and periodically thereafter.
Abuse and Misuse
XYREM is a Schedule III controlled substance. The active ingredient of XYREM, sodium oxybate or gamma hydroxybutyrate (GHB), is a Schedule I controlled substance. Abuse of illicit GHB, either alone or in combination with other CNS depressants, is associated with CNS adverse reactions, including seizure, respiratory depression, decreases in the level of consciousness, coma, and death. The rapid onset of sedation, coupled with the amnestic features of XYREM, particularly when combined with alcohol, has proven to be dangerous for the voluntary and involuntary user (eg, assault victim). Physicians should carefully evaluate patients for a history of drug abuse and follow such patients closely.
XYWAV and XYREM REMS
Because of the risks of central nervous system depression and abuse/misuse, XYREM is available only through a restricted distribution program called the XYWAV and XYREM REMS.
Notable requirements of the XYWAV and XYREM REMS include the following:
- Healthcare Providers who prescribe XYREM are specially certified
- XYREM will be dispensed only by the central pharmacy that is specially certified
- XYREM will be dispensed and shipped only to patients who are enrolled in the XYWAV and XYREM REMS with documentation of safe use
Further information is available at www.XYWAVXYREMREMS.com or 1-866-997-3688.
Respiratory Depression and Sleep-Disordered Breathing
XYREM may impair respiratory drive, especially in patients with compromised respiratory function. In overdoses, life-threatening respiratory depression has been reported. Prescribers should be aware that increased central apneas and clinically relevant desaturation events have been observed with XYREM administration in adult and pediatric patients. Prescribers should be aware that sleep-related breathing disorders tend to be more prevalent in obese patients, in men, in postmenopausal women not on hormone replacement therapy and among patients with narcolepsy.
Depression and Suicidality
In adult clinical trials in patients with narcolepsy (n=781), there were two suicides and two attempted suicides in XYREM-treated patients, including three patients with a previous history of depressive psychiatric disorder. Of the two suicides, one patient used XYREM in conjunction with other drugs. XYREM was not involved in the second suicide. Adverse reactions of depression were reported by 7% of 781 XYREM-treated patients, with four patients (
Other Behavioral or Psychiatric Adverse Reactions
During adult clinical trials in narcolepsy, 3% of 781 patients treated with XYREM experienced confusion, with incidence generally increasing with dose. In a controlled trial in adults where patients were randomized to fixed total daily doses of 3 g, 6 g, or 9 g per night or placebo, a dose-response relationship for confusion was demonstrated, with 17% of patients at 9 g per night experiencing confusion. In all cases in that controlled trial, the confusion resolved soon after termination of treatment. In Trial 3 where sodium oxybate was titrated from an initial 4.5 g per night dose, there was a single event of confusion in one patient at the 9 g per night dose. In the majority of cases in all adult clinical trials in patients with narcolepsy, confusion resolved either soon after termination of dosing or with continued treatment.
In Trial 3 where sodium oxybate was titrated from an initial 4.5 g per night dose, there was a single event of confusion in one patient at the 9 g per night dose. In the majority of cases in all adult clinical trials in patients with narcolepsy, confusion resolved either soon after termination of dosing or with continued treatment.
Anxiety occurred in 5.8% of the 874 patients receiving XYREM in adult clinical trials in another population. Other neuropsychiatric reactions reported in adult XYREM clinical trials in patients with narcolepsy and the post-marketing setting included hallucinations, paranoia, psychosis, aggression, and agitation. In the pediatric clinical trial in patients with narcolepsy, neuropsychiatric reactions, including acute psychosis, confusion, and anxiety, were reported while taking XYREM. The emergence or increase of behavioral or psychiatric events in adult and pediatric patients taking XYREM should be carefully monitored.
Parasomnias
Instances of significant injury or potential injury were associated with sleepwalking during a clinical trial of XYREM in adult patients with narcolepsy. Parasomnias, including sleepwalking, also have been reported in the pediatric clinical trial and in postmarketing experience with XYREM. Episodes of sleepwalking should be fully evaluated and appropriate interventions considered.
Parasomnias, including sleepwalking, also have been reported in the pediatric clinical trial and in postmarketing experience with XYREM. Episodes of sleepwalking should be fully evaluated and appropriate interventions considered.
Use in Patients Sensitive to High Sodium Intake
XYREM has a high salt content. In patients sensitive to salt intake (eg, those with heart failure, hypertension, or renal impairment), consider the amount of daily sodium intake in each dose of XYREM.
MOST COMMON ADVERSE REACTIONS
In three controlled adult clinical trials in patients with narcolepsy, the most common adverse reactions (incidence ≥5% and twice the rate seen with placebo) in XYREM-treated patients were nausea, dizziness, vomiting, somnolence, enuresis, and tremor.
In the pediatric clinical trial in pediatric patients 7 years of age and older with narcolepsy, the most common adverse reactions (≥5%) were nausea (20%), enuresis (19%), vomiting (18%), headache (17%), weight decreased (13%), decreased appetite (9%), dizziness (8%) and sleepwalking (6%). The overall adverse reaction profile of XYREM in the pediatric clinical trial was similar to that seen in the adult clinical trial program.
The overall adverse reaction profile of XYREM in the pediatric clinical trial was similar to that seen in the adult clinical trial program.
ADDITIONAL ADVERSE REACTIONS
Additional adverse reactions that occurred in ≥2% of patients in any treatment group for three controlled adult trials and were more frequent in any XYREM treatment group than with placebo were diarrhea, upper abdominal pain, dry mouth, pain, feeling drunk, peripheral edema, cataplexy, muscle spasms, extremity pain, attention disturbance, paresthesia, sleep paralysis, disorientation, irritability, sleepwalking, anxiety, and hyperhidrosis.
Discontinuation: Of the 398 XYREM-treated adult patients with narcolepsy, 10.3% of patients discontinued because of adverse reactions compared with 2.8% of patients receiving placebo. The most common adverse reaction leading to discontinuation was nausea (2.8%). The majority of adverse reactions leading to discontinuation began during the first few weeks of treatment. In the pediatric clinical trial, 7 of 104 patients reported adverse reactions that led to withdrawal from the study (hallucination, tactile; suicidal ideation; weight decreased; sleep apnea syndrome; affect lability; anger, anxiety, depression; and headache).
In the pediatric clinical trial, 7 of 104 patients reported adverse reactions that led to withdrawal from the study (hallucination, tactile; suicidal ideation; weight decreased; sleep apnea syndrome; affect lability; anger, anxiety, depression; and headache).
Dose-Response Information: In clinical trials in adult patients with narcolepsy, a dose-response relationship was observed for nausea, vomiting, paresthesia, disorientation, irritability, disturbance in attention, feeling drunk, sleepwalking, and enuresis. The incidence of all these reactions was notably higher at 9 g per night. In controlled trials in adults with narcolepsy, discontinuations of treatment due to adverse reactions were greater at higher doses of XYREM.
DRUG INTERACTIONS
XYREM is contraindicated for use in combination with alcohol or sedative hypnotics. Use of other CNS depressants may potentiate the CNS-depressant effects of XYREM.
Concomitant use of XYREM with divalproex sodium resulted in a 25% mean increase in systemic exposure to XYREM (AUC ratio range of 0. 8 to 1.7) and in a greater impairment on some tests of attention and working memory. An initial dose reduction of XYREM at least 20% is recommended if divalproex sodium is prescribed to patients already taking XYREM. Prescribers are advised to monitor patient response closely and adjust dose accordingly if concomitant use of XYREM and divalproex sodium is warranted.
8 to 1.7) and in a greater impairment on some tests of attention and working memory. An initial dose reduction of XYREM at least 20% is recommended if divalproex sodium is prescribed to patients already taking XYREM. Prescribers are advised to monitor patient response closely and adjust dose accordingly if concomitant use of XYREM and divalproex sodium is warranted.
PREGNANCY AND LACTATION
There are no adequate data on the developmental risk associated with the use of sodium oxybate in pregnant women. XYREM should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. GHB is excreted in human milk after oral administration of sodium oxybate. There is insufficient information on the risk to a breastfed infant, and there is insufficient information on milk production in nursing mothers. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for XYREM and any potential adverse effects on the breastfed infant from XYREM or from the underlying maternal condition.
PEDIATRIC USE
Safety and effectiveness of XYREM in pediatric patients below the age of 7 years have not been established.
GERIATRIC USE
Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
HEPATIC IMPAIRMENT
The starting dose of XYREM should be reduced in patients with liver impairment.
Dosage Modification in Patients with Hepatic Impairment: The recommended starting dosage in patients with hepatic impairment is one-half of the original dosage per night, administered orally divided into two doses.
DEPENDENCE AND TOLERANCE
There have been case reports of withdrawal, ranging from mild to severe, following discontinuation of illicit use of GHB at frequent repeated doses (18 g to 250 g per day) in excess of the recommended dosage range. Signs and symptoms of GHB withdrawal following abrupt discontinuation included insomnia, restlessness, anxiety, psychosis, lethargy, nausea, tremor, sweating, muscle cramps, tachycardia, headache, dizziness, rebound fatigue and sleepiness, confusion, and, particularly in the case of severe withdrawal, visual hallucinations, agitation, and delirium. These symptoms generally abated in 3 to 14 days. In cases of severe withdrawal, hospitalization may be required. The discontinuation effects of XYREM have not been systematically evaluated in controlled clinical trials.
Signs and symptoms of GHB withdrawal following abrupt discontinuation included insomnia, restlessness, anxiety, psychosis, lethargy, nausea, tremor, sweating, muscle cramps, tachycardia, headache, dizziness, rebound fatigue and sleepiness, confusion, and, particularly in the case of severe withdrawal, visual hallucinations, agitation, and delirium. These symptoms generally abated in 3 to 14 days. In cases of severe withdrawal, hospitalization may be required. The discontinuation effects of XYREM have not been systematically evaluated in controlled clinical trials.
In the clinical trial experience with XYREM in narcolepsy/cataplexy patients at recommended doses, two patients reported anxiety and one reported insomnia following abrupt discontinuation at the termination of the clinical trial; in the two patients with anxiety, the frequency of cataplexy had increased markedly at the same time.
Tolerance to XYREM has not been systematically studied in controlled clinical trials. There have been some case reports of symptoms of tolerance developing after illicit use at dosages far in excess of the recommended XYREM dosage regimen.
There have been some case reports of symptoms of tolerance developing after illicit use at dosages far in excess of the recommended XYREM dosage regimen.
Please see full Prescribing Information, including BOXED Warning.
Psychogenically induced narcolepsy
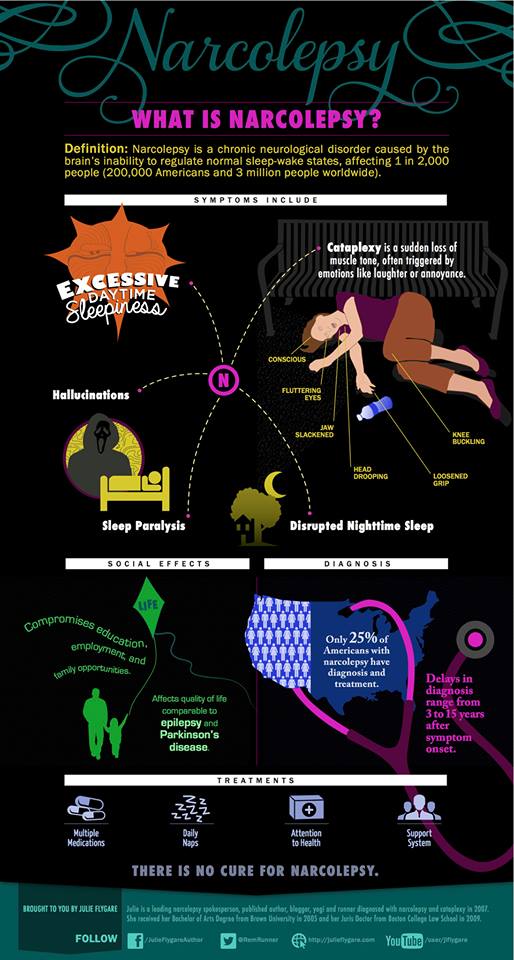
According to modern concepts, narcolepsy refers to hypersomnia, i.e. to conditions whose main symptom is excessive daytime sleepiness. This disease was described in detail in 1880 by the French neurologist J. Gelino (J. Gelineau).
In accordance with the International Classification of Sleep Disorders (3rd edition, 2014), type 1 narcolepsy (synonyms: hypocretin deficiency syndrome, narcolepsy with cataplexy) and type 2 narcolepsy (narcolepsy without cataplexy) are distinguished. nine0003
The prevalence of type 1 narcolepsy is 25 to 50 cases per 100,000 people, and type 2 narcolepsy is 42 to 73 cases per 100,000 people [1]. The disease usually manifests at 10–25 years of age, but the first symptoms may appear both at an earlier and later age (from 4 to 70 years) [2]. Men and women are affected with equal frequency.
Men and women are affected with equal frequency.
The etiology and pathogenesis of this disease have not been studied enough, but it has been established that the development of narcolepsy is associated with a decrease in the content of hypocretin (orexin) in hypothalamic neurons. Hypocretin is a neuropeptide responsible for maintaining the state of wakefulness. As a result, there is a dysregulation of the work of neurotransmitters (histamine, norepinephrine, dopamine, serotonin, acetylcholine), which leads to a deterioration in the regulation of the sleep phase with rapid eye movement and disruption of the sleep-wake cycle. There are works [3-5], the results of which indicate the possible genetic nature of the disease and the involvement of autoimmune mechanisms of destruction of hypocretin/orexin neurons and the role of infection as a trigger factor. The noted changes relate to type 1 narcolepsy, which is characterized by a loss of up to 90% of neurons secreting hypocretin [6]. The cause of type 2 narcolepsy remains unclear; the heterogeneity of this group of conditions and a partial decrease in the level of hypocretin are allowed [6, 7]. The clinical picture of type 1 narcolepsy is characterized by attacks of catalepsy, which do not occur in type 2 narcolepsy.
The cause of type 2 narcolepsy remains unclear; the heterogeneity of this group of conditions and a partial decrease in the level of hypocretin are allowed [6, 7]. The clinical picture of type 1 narcolepsy is characterized by attacks of catalepsy, which do not occur in type 2 narcolepsy.
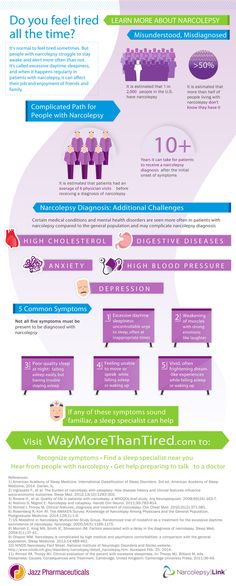
Attacks of daytime sleepiness in narcolepsy often occur when performing monotonous work (while riding in transport, in class, while reading, etc.). They can last from several minutes to several hours. The frequency of attacks can be up to several dozen during the day. After an attack, for some time, patients feel quite cheerful and can continue their work. Cataplexy attacks develop in 60-70% of cases [1]. We are talking about a local or generalized decrease in muscle tone, more often against the background of emotional stress. In addition, hypnagogic (when falling asleep) or hypnopompic (when waking up) hallucinations, cataplexy of awakening and falling asleep (sleep paralysis), as well as disruption of nocturnal sleep are characteristic. But these symptoms are extremely rare at the same time. nine0003
But these symptoms are extremely rare at the same time. nine0003
In addition to the described manifestations in narcolepsy, obesity, depression, anxiety, and phobias are more common than in the general population [8]. The frequency of autonomic disorders is also increased (impaired pupillary reactions, hypotension, syncope, tachycardia, thermoregulation disorder, frequent urination, etc.), which occur in 80–100% of cases [9].
To confirm the diagnosis of narcolepsy, a polysomnographic study and a multiple sleep latency test are performed, during which a decrease in sleep latency is detected - the time required for the onset of sleep (normally at least 15 minutes), as well as premature onset of the sleep phase with rapid eye movement ( normal after 70-90 min from the start of sleep).
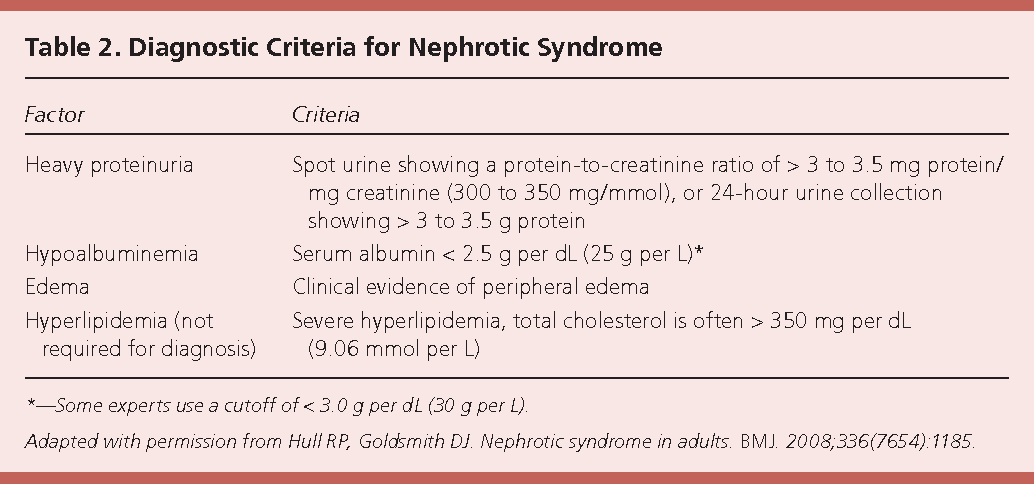
In connection with the above, in order to make a diagnosis of type 1 narcolepsy, in addition to patient complaints about episodes of an irresistible need for daytime sleep (which disturb daily for 3 months or more), it is necessary to have cataplexy attacks, a decrease in sleep latency (usually less than 8 minutes) , premature onset of rapid eye movement sleep (less than 15 min on at least 2 episodes) and/or cerebrospinal fluid (CSF) hypocretin levels of 110 pg/mL or less [10]. Narcolepsy of the second type is characterized by the same complaints (however, expressed to a greater extent) and a similar violation of the sleep architecture. At the same time, there are no attacks of cataplexy (if they develop at a later stage of the disease, then the diagnosis is formulated as type 1 narcolepsy), the normal level of hypocretin in the CSF is maintained [10]. nine0003
Narcolepsy of the second type is characterized by the same complaints (however, expressed to a greater extent) and a similar violation of the sleep architecture. At the same time, there are no attacks of cataplexy (if they develop at a later stage of the disease, then the diagnosis is formulated as type 1 narcolepsy), the normal level of hypocretin in the CSF is maintained [10]. nine0003
There are various approaches to the treatment of narcolepsy, including hypocretin replacement therapy [11] and administration of immunoglobulins [12]. However, in general, the treatment of this disease is only symptomatic. In 2015, recommendations for the care of patients with narcolepsy were published [10]. According to the recommendations, the goal of treatment is to correct daytime sleepiness to optimize the patient's daily activities, as well as to reduce nighttime sleep disturbances and other symptoms of narcolepsy, if present, if they bother the patient. The psychostimulant modafinil and its enantiomer, armodafinil, are recognized as effective means for reducing the severity of daytime sleepiness. Sodium hydroxybutyrate has also been recommended, which is also used to treat cataplexy, hypnagogic hallucinations, and sleep paralysis. Amphetamine, methamphetamine, dexamphetamine, and methylphenidate are effective in treating daytime sleepiness. Despite the proven effectiveness, the use of psychostimulants in medical practice is limited, in some countries it is prohibited [2]. Selegiline (a monoamine oxidase inhibitor) and ritanserin (a selective serotonin C2 receptor antagonist) may be effective. In addition, the method of "planned falling asleep" is effectively used. Tricyclic antidepressants, selective serotonin reuptake inhibitors, and venlafaxine are also used to treat cataplexy, sleep paralysis, and hypnagogic hallucinations. It has been noted that effective treatment of daytime sleepiness significantly improves the functional state of the patient, as well as the quality of life [10]. nine0003
Sodium hydroxybutyrate has also been recommended, which is also used to treat cataplexy, hypnagogic hallucinations, and sleep paralysis. Amphetamine, methamphetamine, dexamphetamine, and methylphenidate are effective in treating daytime sleepiness. Despite the proven effectiveness, the use of psychostimulants in medical practice is limited, in some countries it is prohibited [2]. Selegiline (a monoamine oxidase inhibitor) and ritanserin (a selective serotonin C2 receptor antagonist) may be effective. In addition, the method of "planned falling asleep" is effectively used. Tricyclic antidepressants, selective serotonin reuptake inhibitors, and venlafaxine are also used to treat cataplexy, sleep paralysis, and hypnagogic hallucinations. It has been noted that effective treatment of daytime sleepiness significantly improves the functional state of the patient, as well as the quality of life [10]. nine0003
The authors have their own experience in the diagnosis and treatment of patients with narcolepsy, based on the observation of 4 patients in the Sleep Laboratory of the Republican Clinical Medical Center of the Office of the President of the Republic of Belarus.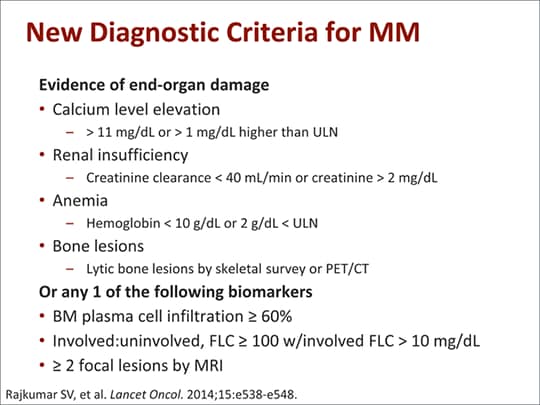
The studied group of patients included 1 man and 3 women aged 19 to 28 years (mean age 22.3 years). The average body mass index (BMI) of the patients was 21.1 kg/m 2 . Concomitant diseases included neurocirculatory dystonia, minor heart anomalies, and somatoform disorders. nine0003
The main complaint of the patients was increased daytime sleepiness, frequent bouts of falling asleep. Upon detailed questioning, non-specific complaints prevailed: short-term headaches mainly as a reaction to overwork or excitement, dizziness of a non-systemic nature, increased irritability, tearfulness in women, absent-mindedness, decreased performance, fatigue and exhaustion when performing usual work, emotional lability. This subjective symptomatology worsened during hard work, overwork, after excitement. Some improvement occurred after a short sleep, rest, or the use of medications. nine0003
In all patients, when describing daytime sleep, complaints of sudden frequent falling asleep, daytime sleepiness, weakness, and increased fatigue prevailed. During nocturnal sleep, restless sleep with dreams was noted. Nocturnal awakenings were accompanied by chills, palpitations, feelings of anxiety and fear. Morning awakenings were accompanied by a headache, a feeling of "heaviness", "brokenness" with a feeling of lack of proper sleep.
During nocturnal sleep, restless sleep with dreams was noted. Nocturnal awakenings were accompanied by chills, palpitations, feelings of anxiety and fear. Morning awakenings were accompanied by a headache, a feeling of "heaviness", "brokenness" with a feeling of lack of proper sleep.
The clinical symptom complex included a decrease in mental and physical activity. On examination, the neurological status showed a slight revival of tendon reflexes, inconsistent mounting nystagmus, staggering in the Romberg test is inconsistent. Neuropsychological examination revealed no cognitive impairments, memory remained normal in the presence of a decrease in concentration. Magnetic resonance imaging (MRI) and MRI angiography of the brain revealed no pathology. All patients underwent a polysomnographic study of sleep, and a multiple sleep latency test was performed. When examining patients, the SOMNOlab V 2.19 system was used.("Weinmann", Germany). Visual processing was subjected to each 30-second interval polysomnogram.
Here is a clinical case of narcolepsy.
Patient Sh. , born in 1999. She was under examination at the Sleep Laboratory on the basis of the neurological department of the above-mentioned Republican Clinical Medical Center from 10/08/18.
At admission, she complained of disturbed night sleep, morning headache, increased daytime sleepiness, attacks of sudden falling asleep during the daytime, general weakness, "weakness" in the daytime, decreased mood, deterioration in performance. Night sleep was described as intermittent with awakenings, anxious, unrefreshing. She noted deterioration in the background of psycho-emotional stress. I occasionally took phenibut, soothing herbal preparations. She has a history of traumatic brain injury at the age of five, after which headaches appeared. Attacks of drowsiness have been disturbing since September 2016, occur involuntarily, last 5–30 minutes. Recently, attacks of drowsiness during the day have become more frequent, sleep has become longer during the day and at night. The patient points to a conflict in the family, which began shortly before the onset of the first symptoms of the disease. In order to avoid communication with her mother, in protest, she tried to retire to her room and fell asleep. nine0003
The patient points to a conflict in the family, which began shortly before the onset of the first symptoms of the disease. In order to avoid communication with her mother, in protest, she tried to retire to her room and fell asleep. nine0003
Somatic status: skin clean, normal color. Peripheral lymph nodes are not palpable. In the lungs - vesicular breathing, percussion - pulmonary sound. Respiration rate 16 per minute. Heart sounds are rhythmic, muffled. Heart rate (HR) 84 beats / min. Blood pressure (BP) 100/70 mm Hg. The tongue is moist and clean. The abdomen is soft and painless. The liver is not palpable. Urination free, painless. There are no peripheral edema.
nine0002 Neurological status: correctly oriented. There is sweating, bright red dermographism, slight tremor of the fingers, aggravated by talking, excitement. Fixed in your feelings. Emotionally labile, mannered. The mood background is reduced, anxious. Nystagmus and oculomotor disorders were not detected. The face is symmetrical. Tongue in the midline. Swallowing is not disturbed. The strength in the limbs is sufficient. Tendon-periosteal reflexes of normal liveliness are equal. There are no root violations. Pathological foot and meningeal symptoms are not defined. Sensitivity is not broken. Muscle tone is not changed. The walk is confident. It is stable in the Romberg test. Performs coordination tests confidently on both sides with slight intentional tremor. nine0003
Tongue in the midline. Swallowing is not disturbed. The strength in the limbs is sufficient. Tendon-periosteal reflexes of normal liveliness are equal. There are no root violations. Pathological foot and meningeal symptoms are not defined. Sensitivity is not broken. Muscle tone is not changed. The walk is confident. It is stable in the Romberg test. Performs coordination tests confidently on both sides with slight intentional tremor. nine0003 Brain MRI showed no structural pathology. On MRI of the cranial arteries, the internal carotid arteries are symmetrically located, of normal course and caliber. MR venography showed no filling defects and areas of lack of signal from the blood flow in all visualized venous segments.
Ultrasound examination (ultrasound) of the thyroid gland and internal organs showed no pathology. ECG shows sinus rhythm. Normal position of the EOS. Holter monitoring of blood pressure: variability of blood pressure during the day 110/70-120/80 mm Hg. Ultrasound of the brachiocephalic vessels: tortuosity of the external carotid arteries, slight thickening of the intima-media complex. nine0003
Ultrasound of the brachiocephalic vessels: tortuosity of the external carotid arteries, slight thickening of the intima-media complex. nine0003
When performing a comprehensive test for the detection of sleep disorders (developed at the Somnological Center of the Central Clinical Hospital of the Medical Center of the Administration of the President of the Russian Federation), the patient scored 47 points, which indicates a poor quality of sleep; sleep. Sheehan score (to determine the level of anxiety) - 35 points, which corresponds to a significant level of anxiety, according to the Beck Depression Scale - 21 points (moderate depressive state). nine0003
A preliminary diagnosis of somatoform autonomic dysfunction with insomnia was established. To clarify the nature of insomnia, a polysomnographic study was performed (Fig. 1). 1. Fragment of the hypnogram of the patient Sh. with the presence of all phases of sleep. Here and in fig. 3-5: D - motor phase; B - wakefulness; 1-4 correspond to sleep phases S1-S4. Sleep phases are presented in full in the correct percentage. during which it was revealed: the architecture of sleep is not disturbed, all phases of sleep are presented in full in the correct percentage. However, a decrease in the time to fall asleep is revealed: the latency of falling asleep is 00:05:30 min. During a night's sleep, the latency to fall asleep is 00:05:00. Total sleep time (TOS) was 08:55:00 min, REM sleep 15.3%, activation responses in micro-awakening sleep 11.0%. REM sleep latency 00:49:30 minutes. REM sleep start time is 00:07:30. The duration of NREM sleep is increased - 73.5%. There are no respiratory disorders (Fig. 2): Fig. Fig. 2. A fragment of the polysomnogram of patient Sh. The upper segment shows episodes accompanied by changes in the electroencephalogram (1st and 2nd recording channels), electrooculogram (3rd and 4th recording channels), which are combined with episodes of muscle contractions on the electromyogram (5th channel). The lower segment shows the curve (fourth) with normal saturation values.
Sleep phases are presented in full in the correct percentage. during which it was revealed: the architecture of sleep is not disturbed, all phases of sleep are presented in full in the correct percentage. However, a decrease in the time to fall asleep is revealed: the latency of falling asleep is 00:05:30 min. During a night's sleep, the latency to fall asleep is 00:05:00. Total sleep time (TOS) was 08:55:00 min, REM sleep 15.3%, activation responses in micro-awakening sleep 11.0%. REM sleep latency 00:49:30 minutes. REM sleep start time is 00:07:30. The duration of NREM sleep is increased - 73.5%. There are no respiratory disorders (Fig. 2): Fig. Fig. 2. A fragment of the polysomnogram of patient Sh. The upper segment shows episodes accompanied by changes in the electroencephalogram (1st and 2nd recording channels), electrooculogram (3rd and 4th recording channels), which are combined with episodes of muscle contractions on the electromyogram (5th channel). The lower segment shows the curve (fourth) with normal saturation values. obstructive sleep apnea 1, mixed 1, central 7, total 9, duration 158 s. Desaturation index 0.0, average saturation (SpO2) 97.4%, minimum - 95%; proportion of snoring 0%; apnea-hypopnea index (AHI) REM 3.0, AHI NREM 0.6, AHI (AHI) 0.9. No heart rhythm disturbances were detected during sleep: heart rate variability 16; average heart rate 70 beats / min. In the polysomnogram, attention is drawn to the presence of characteristic episodes, in combination with normal saturation (see Fig. 2).
obstructive sleep apnea 1, mixed 1, central 7, total 9, duration 158 s. Desaturation index 0.0, average saturation (SpO2) 97.4%, minimum - 95%; proportion of snoring 0%; apnea-hypopnea index (AHI) REM 3.0, AHI NREM 0.6, AHI (AHI) 0.9. No heart rhythm disturbances were detected during sleep: heart rate variability 16; average heart rate 70 beats / min. In the polysomnogram, attention is drawn to the presence of characteristic episodes, in combination with normal saturation (see Fig. 2).
The patient underwent a multiple sleep latency test three times. According to the results of the first (Fig. 3) Fig. 3. Fragment of the hypnogram of patient Sh. during the multiple sleep latency test (first test). The complete absence of REM sleep, sleep is mainly represented by the NREM phase. the following changes were revealed: latency of falling asleep 00:00:24 s, complete absence of REM sleep, sleep mainly represented by the NREM phase — 96.9%, RVR was 49 min. During the second test (Fig. 4) Fig. 4. Fragment of the hypnogram of patient Sh. Results of the second sleep latency test. Complete absence of REM sleep, predominantly NREM sleep. revealed: sleep latency 00:00:22 s, complete absence of REM sleep, predominantly NREM sleep — 88.7%, RVR 25:48 min. At the third (Fig. 5) Fig. Fig. 5. Fragment of the hypnogram of patient Sh. Results of the third sleep latency test. Mostly REM sleep. — sleep latency was 00:03:30 min, predominantly REM sleep — 35.2%, RWS 33:00 min. nine0003
4) Fig. 4. Fragment of the hypnogram of patient Sh. Results of the second sleep latency test. Complete absence of REM sleep, predominantly NREM sleep. revealed: sleep latency 00:00:22 s, complete absence of REM sleep, predominantly NREM sleep — 88.7%, RVR 25:48 min. At the third (Fig. 5) Fig. Fig. 5. Fragment of the hypnogram of patient Sh. Results of the third sleep latency test. Mostly REM sleep. — sleep latency was 00:03:30 min, predominantly REM sleep — 35.2%, RWS 33:00 min. nine0003
The patient was also consulted by a psychiatrist who diagnosed her with narcolepsy. Somatoform autonomic dysfunction. Spitomin (buspirone, a non-benzodiazepine tranquilizer with antidepressant action) was prescribed at a dose of 10 mg per day.
Based on complaints (sleep attacks during the daytime and disturbed night sleep for more than 2 years), medical history (traumatic brain injury in childhood), physical examination (no other pathology that could explain the symptoms was identified), neurological status (presence of autonomic reactions) and the results of the examination (sleep latency from 22 s to 3 min 30 s and the onset of REM sleep 7 min 30 s), the diagnosis was clarified: “type 2 narcolepsy. Somatoform autonomic dysfunction. nine0003
Somatoform autonomic dysfunction. nine0003
The patient was recommended to be monitored by a neurologist and a psychiatrist to rule out type 1 narcolepsy, to continue taking Spitomin, and to observe the regime of work and rest. The features of the clinical picture and current world trends in the treatment of this disease were explained, but the information provided on the use of psychostimulants was perceived negatively.
The case of narcolepsy considered by us is of interest, since it was probably provoked by a conflict situation, in addition, there are indications in the anamnesis of the presence of a traumatic brain injury in childhood, which, possibly, over time led to the development of a symptom complex typical of the disease, which was confirmed during an in-depth examination. Also, the patient has abnormalities when testing on scales of anxiety and depression. nine0003
As mentioned above, there is currently no pathogenetic treatment for this disease. In recent years, a pitolizant, a drug that has a stimulating effect on the histaminergic neurons of the brain, has been recommended as an effective remedy for combating daytime sleepiness and cataplexy in narcolepsy (the drug has been tested on humans and is recommended in Europe for the treatment of both types 1 and 2 narcolepsy) [one].
In conclusion, it can be emphasized once again that despite the fact that the study of narcolepsy has almost a century and a half history, interest in it does not weaken, since this problem has not only medical, but also social aspects. According to M.M. Ohayon et al. [13], the mortality of patients with narcolepsy was 1.5 times higher than in the general population, which may be due to the pathology associated with narcolepsy. There are certain difficulties in making a diagnosis, since it usually takes about 7-10 years [13] before a diagnosis is made. Therefore, physicians should have a certain vigilance regarding the timely detection of this pathology in order to ensure dynamic observation, the appointment of symptomatic therapy, the prevention of anxiety and depressive conditions associated with the disease, as well as to form a behavioral algorithm in the patient and his relatives in the changed conditions in order to maximize social and household adaptation. nine0003
The authors declare no conflict of interest.
The authors declare no conflicts of interest.
Credits
Likhachev S.A. . — https://orcid.org/0000-0002-6019-042X
Chechik N.M. - https://orcid.org/0000-0002-3692-3961
Galievskaya O.V . — e-mail: [email protected]; https://orcid.org/0000-0001-9040-5535
Rushkevich Yu.N . — https://orcid.org/0000-0002-2529-8005
How to quote:
Likhachev S.A., Chechik N.M., Galievskaya O.V., Rushkevich Yu.N. Psychogenically induced narcolepsy. Journal of Neurology and Psychiatry. S.S. Korsakov. 2019;119(9):99-104. https://doi.org/10.17116/jnevro201911909199
Corresponding author: Galievskaya Olga Vasilievna — e-mail: [email protected]
what is it, symptoms, treatment, causes of daytime sleepiness
Font size Color scheme Images
x
Make an appointment
Name* Phone* Adult Child (under 18)x
Sign up for analysis
Name* Phone* ☆ st. Malaya Balkanskaya, 23 (m. Kupchino)
Malaya Balkanskaya, 23 (m. Kupchino)
Dunaisky ave., 47 (m. Dunaiskaya)
Udarnikov ave., 19 (m. Ladozhskaya)
st. Marshala Zakharova, 20 (metro station Leninskiy pr-t)
Vyborgskoe highway, 17 (metro Prospect of Prosveshcheniya)
- Call
435 55 55 -
Make an appointment
This disease is treated by Somnologist
The information provided on this page should not be used for self-treatment or self-diagnosis. If you suspect a disease, you should seek help from a qualified specialist. Only your doctor can diagnose and prescribe treatment.
Article content:
- Causes
- Symptoms of narcolepsy
- Diagnostics
- Narcolepsy treatment
- Prognosis and prevention
What is narcolepsy?
Narcolepsy is a pathological condition characterized by an inability to control sleep and wakefulness. Sudden onset of excessive daytime sleepiness and other symptoms of narcolepsy can occur at any time, even in situations that require extreme concentration, such as driving. The risk group for the development of narcolepsy is men, the frequency of cases is 1 in 2 thousand people. But there is an opinion that the prevalence is higher due to the fact that not all patients do not seek medical help and treatment. Narcolepsy Source:
Sudden onset of excessive daytime sleepiness and other symptoms of narcolepsy can occur at any time, even in situations that require extreme concentration, such as driving. The risk group for the development of narcolepsy is men, the frequency of cases is 1 in 2 thousand people. But there is an opinion that the prevalence is higher due to the fact that not all patients do not seek medical help and treatment. Narcolepsy Source:
description of the clinical observation. Remizevich R.S., Kurasov E.S. Bulletin of the National Medical and Surgical Center. N. I. Pirogova, Volume 8, No. 4, 2013. pp. 141-145 - not a fatal pathology, but accidents still happen during attacks.
Causes
The exact causes of narcolepsy are unknown, although it has been established that heredity plays a role, as well as a lack of the neurotransmitter orexin, which is responsible for wakefulness.
REM sleep literally invades the periods of wakefulness and the transition to sleep. Symptoms of narcolepsy are associated with a sharp loss of muscle tone, the appearance of vivid visions, which are just characteristic of the phase of REM sleep. nine0003
Symptoms of narcolepsy are associated with a sharp loss of muscle tone, the appearance of vivid visions, which are just characteristic of the phase of REM sleep. nine0003
It was not possible to determine the exact reasons for the decrease in the production of the neurotransmitter, but the predisposing factors for the development of the pathology were identified:
- serious craniocerebral injuries and their consequences;
- infectious diseases affecting the nervous system Source:
Autonomic disorders in narcolepsy (review of foreign literature). Golokov V.A., Nikolaeva T.Ya., Schneider N.A., Kantimirova E.A. Medical Almanac No. 5(45), 2016. pp. 165-168; - pronounced hormonal changes;
- autoimmune diseases;
- chronic stress and severe emotional upheavals;
- nervous and physical exhaustion.
As a rule, the combined action of several factors is necessary for the development of a disease. Great importance in the mechanism of the development of the state is given to the work of immunity. An immune response is triggered, as a result of which its own cells are mistakenly destroyed, which leads to the onset of symptoms. nine0003
An immune response is triggered, as a result of which its own cells are mistakenly destroyed, which leads to the onset of symptoms. nine0003
Symptoms of narcolepsy
The most common symptom is excessive daytime sleepiness, as well as persistent sleep disturbances at night. This creates inconvenience, spoils the quality of life, affects success in work and social relations.
Over time, the clinical picture changes, other signs join:
- The first and most common symptom is sudden falling asleep during the day. Drowsiness is severe, patients fall asleep against their will, even in unsuitable surroundings. But after waking up, they feel a surge of strength, there is no drowsiness. This state can be deceptive - after a short time they fall asleep again. At the same time, waking up the patient is no more difficult than during normal sleep. nine0131
- Cataplexy Source:
Narcolepsy with prepubertal onset cataplexy. Gromova D.O., Zinovieva O.E. , Rogovina E.G., Poluektov M.G. Neurological journal No. 4, 2012. pp. 22-27 - sudden muscle weakness after strong emotional outbursts. The resulting weakness can be explained by a sharp loss of muscle tone, which often ends in injuries associated with a fall. The duration of the attack varies and lasts up to several minutes, followed by falling asleep. nine0131
, Rogovina E.G., Poluektov M.G. Neurological journal No. 4, 2012. pp. 22-27 - sudden muscle weakness after strong emotional outbursts. The resulting weakness can be explained by a sharp loss of muscle tone, which often ends in injuries associated with a fall. The duration of the attack varies and lasts up to several minutes, followed by falling asleep. nine0131 - Hallucinations on falling asleep and waking up. They are characterized as vivid acoustic or visual visions that correspond to REM sleep. This state is sometimes called "waking sleep", and the patient himself does not realize that he is sleeping and dreaming. This is a dangerous condition that creates confusion between reality and dream.
- Sleep paralysis is a condition characterized by the inability to move after waking up, but the ability to breathe and blink remains. The patient is conscious, understands where he is. Most often, sleep paralysis is formed in the morning, less often in the evening and at night. Sleep paralysis is aggravated by hallucinations without the ability to move.
 The condition goes away after a few minutes. nine0131
The condition goes away after a few minutes. nine0131
Only 10% of patients present with all symptoms at once. Usually first appear in young people, with no previous diseases. Although they can be associated with strong emotional upheavals or chronic stress. After the first onset of symptoms, narcolepsy is permanent, but does not affect life expectancy.
In clinical practice, it is customary to distinguish 2 types of narcolepsy:
- the first occurs due to orexin deficiency, the appearance of cataplexy is characteristic Source:
Narcolepsy-cataplexy. Vasilchenko T.S., Gabdrakipova A.A. Bulletin of Science and Education No. 24(78), 2020. pp. 53-55; - the second is characterized by a normal level of the neurotransmitter and cataplexy does not occur.
Diagnostics
The main thing is to detect pathology in time to prevent risks to the patient's physical health and harm to others. The patient cannot control narcolepsy, attacks occur even at the time of hard work and maximum concentration of attention, as well as performing tasks that involve risks to health and even life. nine0003
nine0003
When visiting a doctor, the symptoms that characterize the diagnosis are studied in detail. The doctor is interested in:
- the patient's complaints, when the attack first occurred and how long it lasted, what symptoms are present;
- neurological examination data, some tests;
- results of additional examination methods to confirm the diagnosis.
These include polysomnography. Source:
Problems in the differential diagnosis of epileptic seizures and narcolepsy (clinical observation). Dmitrenko D.V., Alekseeva O.V., Sapronova M.R., Usoltseva A.A., Areshkina I.G. Bulletin of the North-Eastern Federal University. M. K. Ammosova. Series: Medical Sciences No. 4(13), 2018. pp. 44-51 with EEG data. This method of examination allows you to objectively assess the activity of the brain and sleep phases. The survey continues throughout the night. Electrodes are placed on the patient's head, which fix the indicators and give them out in the form of curves - the doctor analyzes the data.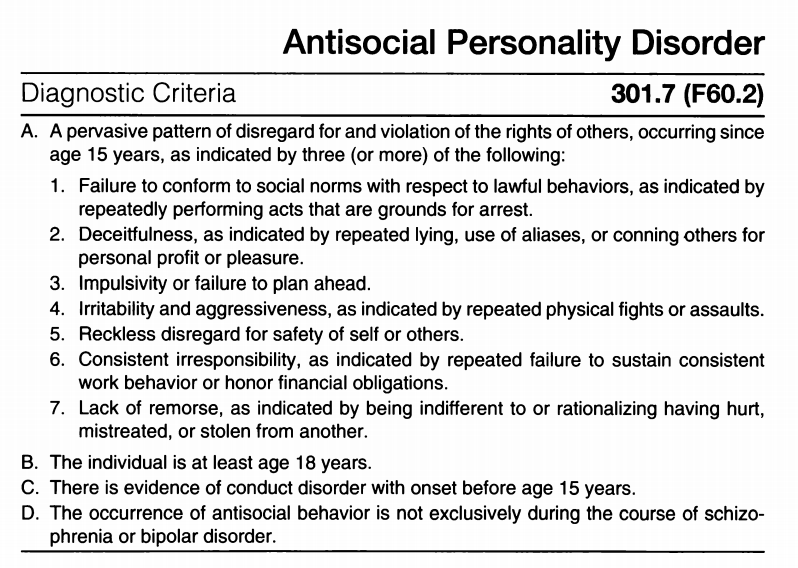 nine0003
nine0003
Additionally, CT and MRI are recommended to assess brain function and condition. In some cases, it may be necessary to analyze the cerebrospinal fluid, which is aimed at determining the concentration of orexin.
Treatment tactics are determined by the data obtained during the examination. This takes into account the severity of concomitant pathology, acquired diseases.
Treatment of narcolepsy
Drug treatment prescribed by specialists is constant, but the number of drugs depends on the clinical picture and the characteristics of the manifestation of the disease. Doctors usually prescribe:
- stimulants;
- sleeping pills to help normalize night sleep;
- antidepressants;
- means to combat daytime sleepiness.
Other recommendations are added to medications - lifestyle changes that help control symptoms. Patients with narcolepsy are recommended to:
- strictly observe the daily routine: go to bed and get up at the same time, regardless of holidays and weekends; nine0131
- give up alcohol completely and stop smoking;
- minimize your intake of coffee, soft drinks, energy drinks, and junk food;
- introduce short naps into your schedule;
- lead an active lifestyle, play sports, for example, exercise therapy, yoga.
Prognosis and prevention
Unfortunately, there is no cure for narcolepsy. All treatment is aimed at controlling and maximizing symptom relief. After the course of treatment, the patient returns to his usual way of life, although there are still some restrictions. nine0003
There are some prohibitions for all narcolepsy patients. They are forbidden to drive a car, as well as to occupy positions related to hazardous industries, for example, to work with machine tools, in large factories, etc. After all, an attack can happen at any moment, regardless of what a person is doing.
- Narcolepsy-cataplexy. Vasilchenko T.S., Gabdrakipova A.A. Bulletin of Science and Education No. 24(78), 2020. p.53-55
- Narcolepsy with cataplexy with onset in prepubertal age. Gromova D.O., Zinovieva O.E., Rogovina E.G., Poluektov M.G. Neurological journal №4, 2012. pp.22-27
- Modern ideas about narcolepsy with a description of clinical observation.
 Remizevich R.S., Kurasov E.S. Bulletin of the National Medical and Surgical Center. N. I. Pirogova, Volume 8, No. 4, 2013. pp. 141-145
Remizevich R.S., Kurasov E.S. Bulletin of the National Medical and Surgical Center. N. I. Pirogova, Volume 8, No. 4, 2013. pp. 141-145 - Autonomic disorders in narcolepsy (review of foreign literature). Golokov V.A., Nikolaeva T.Ya., Schneider N.A., Kantimirova E.A. Medical Almanac No. 5(45), 2016. p.165-168
- Problems of differential diagnosis of epileptic seizures and narcolepsy (clinical observation). Dmitrenko D.V., Alekseeva O.V., Sapronova M.R., Usoltseva A.A., Areshkina I.G. Bulletin of the North-Eastern Federal University. M. K. Ammosova. Series: Medical Sciences No. 4(13), 2018. p.44-51
Article published : 31/05/2017
Last updated : 30/11/2022
See also
Nightmares
Sleep disorders
Snoring treatment
Licenses
Medicom LLC
(Udarnikov Avenue)
Medicom LLC
(Vyborgskoye Highway)
Medi Len LLC
(Marshal Zakharov St.)
Medi30 LLC (Dunaisky) 901 avenue)
Medi Prof LLC
(Malaya Balkanskaya St.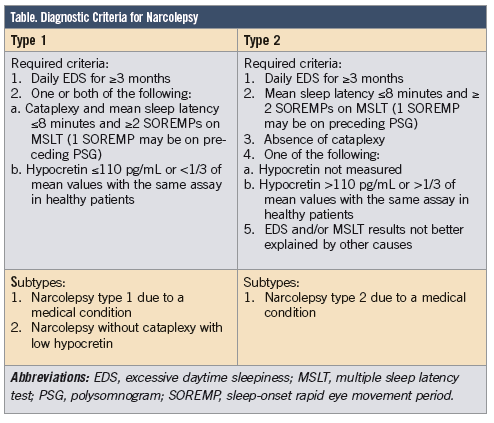 )
)
Go to the license section Go to the legal information section
record from website DISCOUNT 10%
Enrollment is only possible through the contact center.
To register, fill out the form below and you will be contacted.
By clicking on the button, you consent to the processing of your personal data by
nine0003
You are enrolling:
Clinic: {{department}}
Specialty: {{specialty}}
Doctor: {{doctor}}
Date and time: {{form.date | setTime(form.time) | dateTimeFormatted}}
Date of birth: {{age | dateFormatted}}
{{appointmentReply}}
By clicking "Sign up", I accept the terms of the user agreement, the provisions on the protection of personal data and give my consent to the processing of personal data.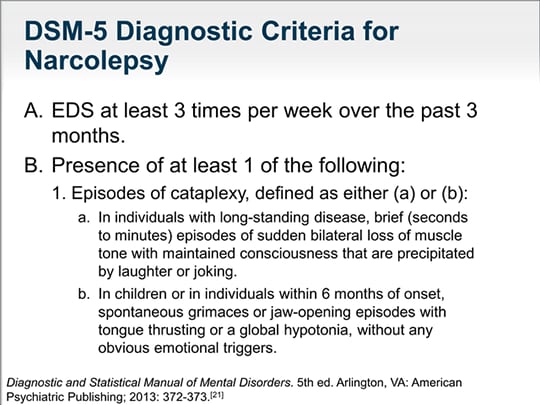 nine0003
nine0003
In order to pass the mandatory registration, you must come to the registration desk 10 minutes before your appointment with your passport.
If the patient is a minor (children under 18), it is mandatory to be accompanied by one of the parents with the presentation of his passport and birth certificate of the child.
Relatives and third parties accompanying a minor must have a notarized consent of the parents or legal representatives.
If you have booked an appointment with a coloproctologist, please read the information about preparing for an appointment
The price of the consultation includes:
History taking, preliminary diagnosis and examination appointment. All additional doctor's manipulations at the appointment are paid according to the price list.
If you change your mind, please unsubscribe from the appointment by phone +7 (812) 435-55-55
The price of the consultation includes:
History taking, preliminary diagnosis and examination appointment.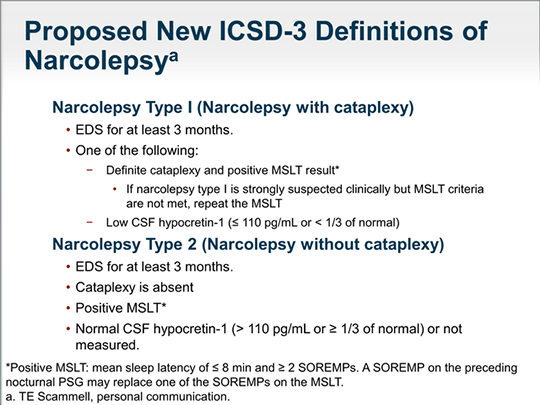 All additional doctor's manipulations at the appointment are paid according to the price list. nine0003
All additional doctor's manipulations at the appointment are paid according to the price list. nine0003
If you change your mind, please unsubscribe from the appointment using your Personal Account or by phone +7 (812) 435-55-55.
Are you sure you want to stop recording?
If you have any questions, call us at +7 (812) 435-55-55
Are you sure you want to change the current entry?
If you have any questions, call us at +7 (812) 435-55-55
You are subject to some restrictions on online booking. nine0003
Appointment possible via contact center.
You can sign up by phone +7 (812) 435-55-55
The specialist does not see patients of the specified age. To register please fill out the form below and you will be contacted.
Make an appointment
Do you want us to call you
?
Name Phone
By clicking on the button, you consent
to process your personal data
You will be contacted to confirm your application.
Making an appointment
Preliminary appointment through the site
Our employee will contact you to confirm the appointment with a specialist
By clicking on the button, you consent to the processing of your personal data by
Learn more about quality assurance of medical services
Would you like us to call you
?
By clicking on the button, you consent to the processing of your personal data by
Leave a request and our specialist
will select a convenient time for a communication session with a doctor
By clicking on the button, you consent to the processing of your personal data by
Screenshot of a review from Yandex.Maps*
By clicking on the button, you consent to the processing of your personal data by
Sign up
for a consultation
Choose a clinic 1st.