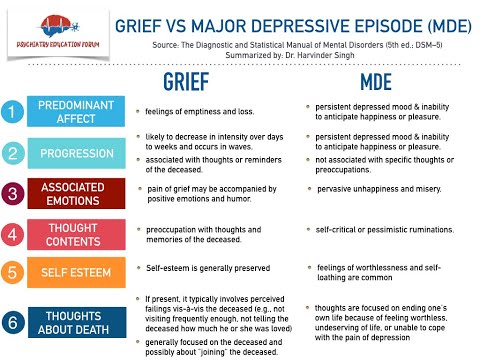
Depression vs depressive episode
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.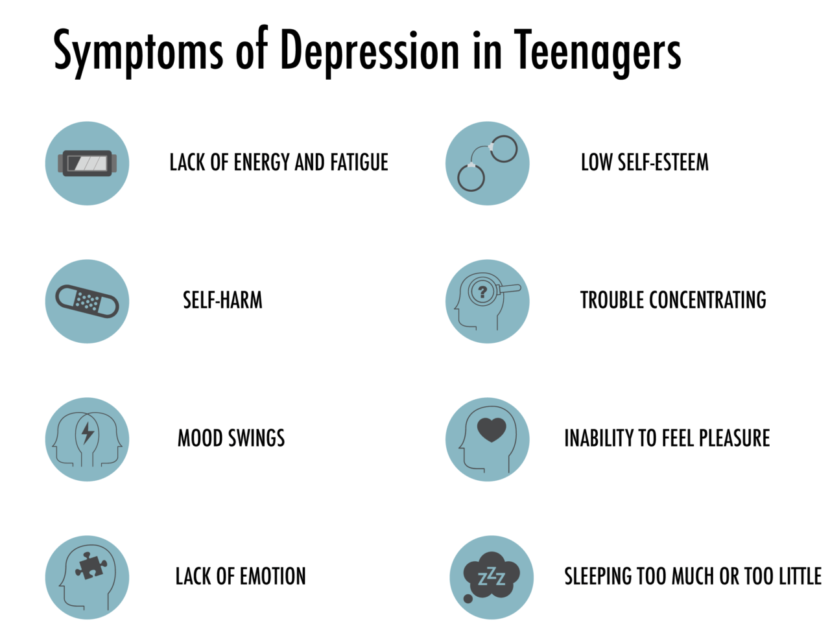
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.
-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly.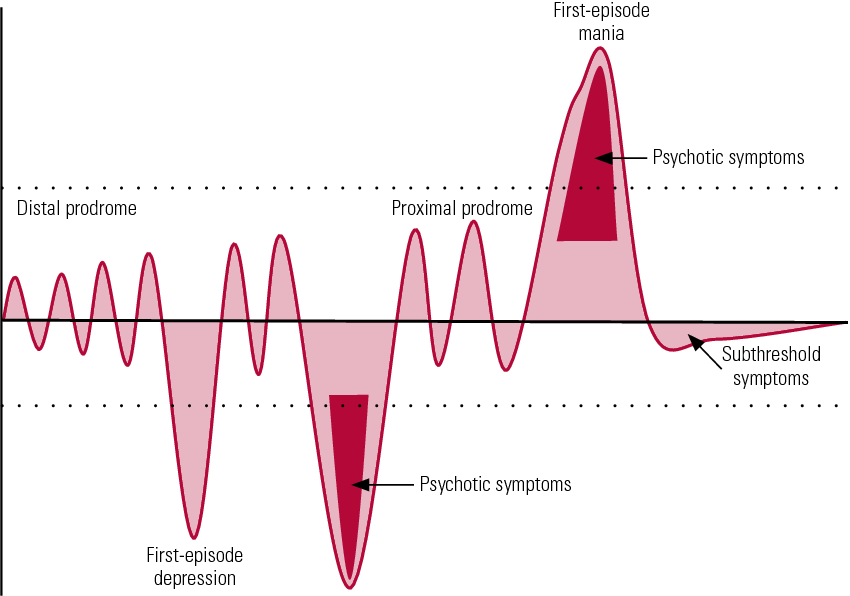 Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Depressive episode | Rehab Family Clinic
In modern society, depression has become one of the most common and serious diseases. A depressive episode is an affective disorder characterized by cognitive, emotional and somatic disturbances. This manifests itself in the form of poor health, apathy, loss of interest in life, loss of energy, fatigue and a generally bleak mood.
The patient does not want to do anything, and any activity quickly bothers him. Also, such episodes are accompanied by a decrease in concentration and concentration, low self-esteem, loss of confidence, gloomy mood, insomnia and decreased appetite.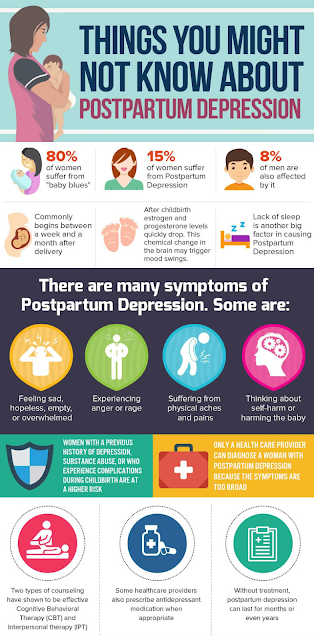 Often, such transitions lead to thoughts of suicide. nine0003
Often, such transitions lead to thoughts of suicide. nine0003
Mild, moderate or severe typical cases are accompanied by low mood, weakness, lack of energy, decreased activity. The patient ceases to be interested in life, he does not enjoy any activities, and fatigue appears even after minimal effort. As a rule, this is also accompanied by insomnia and decreased appetite.
Self-esteem in a person is reduced even in a mild depressive episode. Decreased mood does not depend on circumstances and is accompanied by somatic disorders - loss of interest in life, apathy, morning depression, decreased appetite. A depressive episode is classified into mild, moderate, and severe, depending on the number of symptoms and their severity. nine0003
Symptoms of a depressive episode
Symptoms of this disease in a patient differ depending on the severity of his condition. So, among the main symptoms are the following:
- lack of concentration;
- low academic and work performance;
- decreased physical activity;
- irritability, aggression;
- anxiety state;
- insecurity, low self-esteem; nine0018
- manifestation of self-flagellation, self-humiliation;
- violation of the daily routine;
- insomnia at night and inability to get up in the morning;
- loss of appetite;
- a person is lost in time, ceases to follow the appearance;
- slow speech.

At a doctor's appointment, a patient with a depressive episode can be identified by the following factors:
- The patient does not look into the eyes of the doctor, looks away to the window. nine0018
- Hands clasped to chest.
- Anxious manifestations are accompanied by a desire to touch the throat.
- The man sits in a pose of submission.
- Dropped corners of the mouth.
- Low, quiet voice.
- There are long pauses between words.
Among the indirect signs of a depressive episode are the following:
- The patient has enlarged pupils.
- Decreased skin turgor.
- Heart palpitations. nine0018
- Increased fragility of hair and nails.
- The process of urination is disturbed.
- There is pain in the chest area.
- In some cases, the functions of the gastrointestinal tract are disturbed.
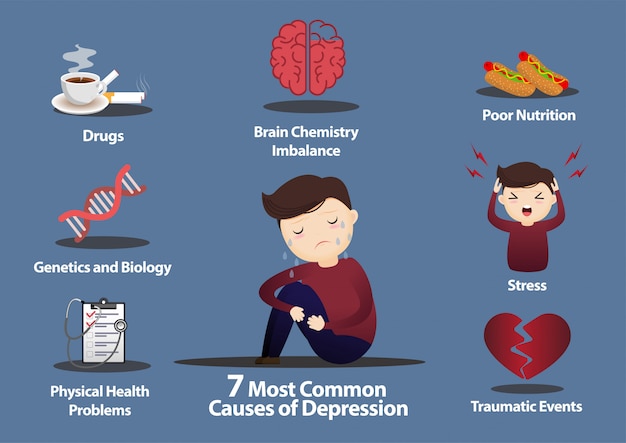
Causes of a depressive episode
There are 3 main causes of a depressive episode:
- Genetic. Associated with abnormalities in chromosome 11.
- Biochemical. When the activity of neurotransmitter exchanges is disturbed and, as a result, there is a lack of serotonin and catecholamine. nine0018
- Neuroendocrine. Expressed in violation of the functioning of the epiphysis, limbic and hypothalamic-pituitary systems. This, in turn, impairs the release of releasing hormones and melatonin.
The main risk group includes people from 20 to 40 years old. Other factors that contribute to the onset of a depressive episode include:
- People with low social status.
- People who have experienced the loss of a loved one.
- Those who have experienced suicide in the family.
 nine0018
nine0018 - People prone to experiences from scratch.
- Persons of unconventional orientation.
- In women, episodes are often associated with the postpartum period.
- Persons who are in a stressful situation for a long time.
Depressive episode pathogenesis
Scientists concluded that the disease has a biochemical origin due to the fact that different areas of the brain of patients have different activity. The hereditary factor is more difficult to recognize. Depression is also associated with disturbances in the circadian rhythm and biological clock. So, for example, the phase of REM sleep, during which people dream, in depressed patients passes much more rapidly. This phase depends on how low the level of serotonin in the brain is, and the use of antidepressants significantly disrupts its work and increases serotonergic tone. He, in turn, is more active during the day when a person is awake. Insomnia activates serotonergic neurons, leading to the same result as the use of antidepressants. nine0003
nine0003
Depressed patients, on the contrary, feel much better after a sleepless night. The effect of antidepressants depends on an increase in central serotonergic neurotransmission, the very system that influences sleep and wake cycles. In the treatment of major depression, specialists use light therapy, sleep deprivation and displacement. An increase or decrease in the duration of sleep is one of the factors in the onset of depression.
It is not uncommon for patients with this disease to have a mixture of various diurnal or seasonal symptoms of depression, even out of season. Mood improvement throughout the day depends on the activity of dorsal neural networks. According to one version, depression is the result of a phase shift. nine0003
According to other studies, depression persists in patients at rest and reveals itself only in the environment. Without denying the biological factor of their occurrence, it is believed that a stressful event and a person's reaction to it cause a depressive episode. Patients with a similar disease show social communication, avoid all kinds of positive activities, and perform inappropriate actions.
Patients with a similar disease show social communication, avoid all kinds of positive activities, and perform inappropriate actions.
One of the factors in the occurrence of a depressive episode is the lack of communication skills in society and the lack of interaction with various social groups. Over time, this leads to isolation from society and, as a result, a decrease in self-esteem and an increase in the feeling of uselessness. nine0003
According to another theory, depression occurs due to inadequate rewards for the patient's positive behavior. The latter completely ceases to show such actions. The loss of action reinforcement can be associated with various events. The loss of such reinforcement leads the patient to think about the futility of his actions and their meaninglessness. As a result, there is a feeling of loss of control over the result, regardless of the actions taken.
Depressive episode duration
As a rule, the development of a depressive episode occurs slowly and very imperceptibly, both for the patient himself and for his relatives. Initially, there is irritability, emotional discomfort. A person tries to find an explanation for his behavior, to deal with the root cause of his suffering. Then comes the realization that he is sick, however, what kind of disease the person does not understand. Typically, a depressive disorder lasts a couple of weeks, and a prolonged depressive episode lasts at least 2 years. Without proper treatment, an episode can pass in a year, however, its symptoms remain forever in 25% of patients. nine0003
Initially, there is irritability, emotional discomfort. A person tries to find an explanation for his behavior, to deal with the root cause of his suffering. Then comes the realization that he is sick, however, what kind of disease the person does not understand. Typically, a depressive disorder lasts a couple of weeks, and a prolonged depressive episode lasts at least 2 years. Without proper treatment, an episode can pass in a year, however, its symptoms remain forever in 25% of patients. nine0003
Short-term depressive spectrum disorders include some forms of depression:
- Depression after childbirth. Lasts from 1 week to 2 months.
- Disorders before the menstrual cycle. A similar phenomenon occurs in 5% of women and lasts about 2 weeks before the cycle.
In 15% of patients, a depressive episode becomes chronic. Depression, in most cases, returns, sometimes with exacerbations and tends to be chronic. In 6% of the population, it lasts more than 2 years, in 13% - more than five years, and patients with chronic depression make up 28% of the total number of patients with a depressive episode. Relapses tend to occur in patients who have had it for the first time before the age of 20. nine0003
Before antibiotics are started, episodes can last up to 1 year. Timely treatment will help get rid of it in six months.
Depressive episode severity
There are several degrees of a depressive episode. Among them:
- mild depressive episode. It usually begins with somatic disorders. A person experiences a headache, fatigue, quickly gets tired. Mood changes, concentration of attention decreases, difficulties with thinking appear. The patient feels unwell in the morning, and in the evening it improves markedly. nine0078 As the disease develops, insomnia, an increase or decrease in appetite, a feeling of anxiety and sadness appear. Without proper treatment, the symptoms get worse. The patient becomes whiny, irritable, apathetic.
- Depressive episode of moderate severity. Characterized by low mood, pessimism, dreary mood. It becomes difficult to do work, sleep, appetite are disturbed, weight changes.
The patient hates his condition. From the outside, he looks tired, depressed and not energetic. There is a somatic character, anxiety, in some cases there are no emotions at all. nine0018 - Severe degree. It is characterized by a constant painful feeling. The patient experiences heaviness in the chest area, there are no fluctuations in mood, the ability to communicate in society is completely lost.
At this stage, the patient often spends all the time in bed, walks slowly, there is no facial expression. Speech becomes slurred and inaudible. There is no activity. The patient has suicidal thoughts. In some cases, hallucinations and delusions are observed. nine0158 - Daily low mood lasting more than 2 weeks.
- Decreased concentration.
- Fast fatiguability.
- Lack of focus.
- Low self-esteem.
- Insomnia.
- Appetite problems. nine0041
- Heightened emotional response to external events.
- Increased appetite and drowsiness.
- Somatic disorders, expressed in headache, shortness of breath, pain in the chest, nausea, diarrhea, etc.
- Hamilton Depression Scale.

- Symptom questionnaire.
- Questioning on a scale of severity of suicidal thoughts.
- Interview to assess the classification of the disease.
- psychotherapy;
- drug treatment;
- electroconvulsive therapy. nine0018
- Smulevich A. B. "Depression in somatic and mental illness."
- Smulevich A.B. ‹‹Depression in General Medicine: A Guide for Physicians
- Tarakanova Elena Alexandrovna, Ivanchuk Elvira Gustavovna, Rostovshchikov Vitaly Vladimirovich - Problems of depressive insomnia nine0018
- Soldatos K.
 , Teleritis X - Improving the sleep-wake cycle to achieve therapeutic remission in depression
, Teleritis X - Improving the sleep-wake cycle to achieve therapeutic remission in depression
Depressive episode classification
The main criteria for a depressive episode by which this disease can be recognized are:
One form of depressive disorder is an atypical depressive episode. In addition to the features characteristic of a depressive episode, it also has others:
As a rule, atypical depression manifests itself sluggishly and has a chronic character. A person considers himself ill with an incurable disease and ceases to live a normal life. At the same time, he often turns to alternative medicine, magicians, clairvoyants instead of observation and treatment by experienced specialists. nine0003
A mild depressive episode is another form of depression that manifests itself in a change in the patient's behavior and his constant complaints. This leads to a decrease in the level of social activity and prevents the realization of a person in all aspects.
The patient experiences all of the symptoms of a depressive episode, plus several of the common criteria for depression, such as negative thoughts, low self-esteem, self-judgment, and suicidal thoughts. This episode lasts for several weeks. nine0003
A manic depressive episode or bipolar disorder is accompanied by affective disturbances with alternating mania and depression.
Irritability, psychomotor agitation can be added to the main symptoms of a manic disorder, in some cases delusions or hallucinations appear. During a depressive episode, the patient experiences the opposite feelings: slow speech and movement, decreased appetite and weight, lack of sexual desire. nine0003
A recurrent depressive episode is a recurrent depressive episode. This form of depression excludes individual episodes of elevated mood or hyperactivity from the anamnesis. As a rule, it begins after 20 years and without proper treatment can last several years.
Complications of a depressive episode
Lack of treatment in some cases can lead to negative consequences for the patient himself. He can harm himself, lose his social status - family, work. There is a high probability of developing chronic diseases - metabolic syndrome, sexual dysfunction, cardiovascular diseases. According to statistics, life expectancy in patients with a depressive episode is much lower, partly due to suicide (in 50%). nine0003
He can harm himself, lose his social status - family, work. There is a high probability of developing chronic diseases - metabolic syndrome, sexual dysfunction, cardiovascular diseases. According to statistics, life expectancy in patients with a depressive episode is much lower, partly due to suicide (in 50%). nine0003
Depression should definitely be treated by a psychiatrist who will help diagnose, assess the severity and prescribe appropriate treatment. It is necessary to consult a doctor after a prolonged decline in mood for at least 2 weeks, sleep disturbance and appetite.
Diagnosis of a depressive episode
To make the correct diagnosis of a depressive episode, the doctor uses clinical, psychopathological and experimental psychological methods. Among them are questionnaires and diagnostics on the Barratt impulsivity scale, dynamic observation, personality questionnaires of different levels. nine0003
Among clinometric diagnostics:
Treatment of a depressive episode
The most effective treatments for a depressive episode are:
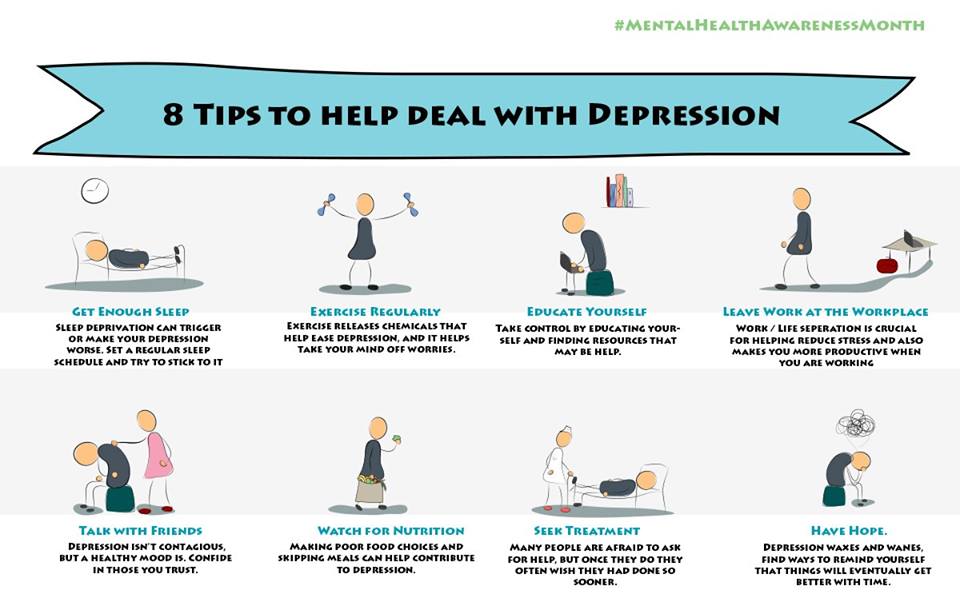
For the treatment of mild depression in its initial stage, the use of antidepressants is not recommended. They should only be used with the psychosocial correction method and for at least 6 months. Also, for the treatment of the disease at its onset, it is important to engage in physical exercises, which significantly reduce the symptoms of a depressive episode.
For more complex depressive episodes, a combination of drugs and psychotherapy is used. Such therapy is effective in the treatment of depression in the older generation. Cognitive behavioral therapy is used to treat children and adolescents. nine0003
nine0003
+7 (495) 121-48-31
Prevention of a depressive episode
According to studies, most patients experience this again after their first depressive episode. 20% of them have a chronic relapse. It is possible if all symptoms are not eliminated during treatment. Therefore, it is important not to stop taking antidepressants prescribed by your doctor. Their use reduces the likelihood of an episode by 80%. In some cases, the use of drugs lasts much longer or a lifetime. nine0003
Clinical recommendations for a depressive episode include interpersonal and cognitive-behavioral therapy and regular follow-up with a psychiatrist.
References:
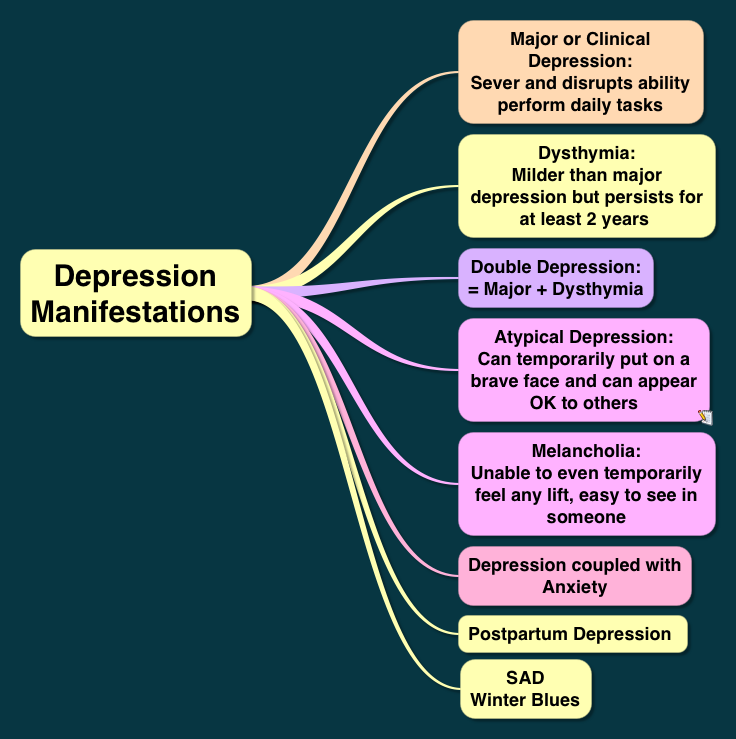
Types of depression - iFightDepression [EN]
There are different types of depression, which are different.
Signs and symptoms vary in number, time, severity and frequency, but are generally very similar. Because different types of depression are treated differently, it is important to pinpoint the type of depression. Depending on gender, age and cultural characteristics, people have different symptoms and severity of depression. nine0003
Neurotic, reactive (minor) depression is treated with psychotherapy.
Somatic and psychotic - medication. These terms are used by psychiatrists.
Studies have shown that depression has a phasic course. Periods of normal mood alternate with depressive episodes. Sometimes, instead of a depressive phase,
there may be a manic phase, which is manifested by irritability and high mood. If so, then it is not depression, but bipolar disorder (a more serious illness). nine0003
nine0003
1. Depressive episode
The most common and typical form of depression is the depressive episode. An episode lasts from a few weeks to a year, but is always longer than 2 weeks. A single depressive episode is called a unipolar episode. Approximately one third of affected people experience only one episode, or "phase", during their lifetime. However, if a person does not receive appropriate treatment for depression, there is a risk of recurrent depressive episodes in the future. Depressive episodes always affect a person's performance to one degree or another. nine0003
2. Intermittent (recurrent) depressive disorder
When a depressive episode recurs, it is recurrent depressive disorder or major depressive disorder, which usually begins in adolescence or early adulthood. With this kind of depression, depressive phases, which can last from several months to several years, alternate with phases of normal mood. This type of depressive disorder can seriously affect performance and is unipolar in nature (no manic or hypomanic phase). This is the so-called "classic" or "clinical" depression. nine0003
This is the so-called "classic" or "clinical" depression. nine0003
3. Dysthymia
Dysthymia presents with milder and less severe symptoms than a depressive episode or recurrent depression. However, the disorder is permanent, with symptoms lasting much longer, at least 2 years, sometimes decades, which is why it is called "chronic depression". This disorder is unipolar and also affects performance. This type of depression sometimes develops into a more severe form (major depressive episode) and if this happens it is called double depression. nine0003
4. Bipolar depression, type I
This is the type of depression in bipolar disorder, formerly called manic-depressive illness, and is less common than unipolar depression. It consists of alternating depressive phases, phases of normal mood and so-called manic phases.
Manic phases are characterized by excessively high mood associated with hyperactivity, anxiety, and decreased need for sleep.
Mania affects thinking, judgment and social behavior causing serious problems and difficulties. When a person is in a manic phase, he makes frequent casual unsafe sex, makes unwise financial decisions. After a manic episode, such people often experience depression. nine0003
When a person is in a manic phase, he makes frequent casual unsafe sex, makes unwise financial decisions. After a manic episode, such people often experience depression. nine0003
The best way to describe these "emotional upheavals" is "to be on top of the world and fall into the depths of despair".
Symptoms of the phases of depression in bipolar disorder are sometimes difficult to distinguish from unipolar depression.
5. Bipolar depression type II
More like recurrent depressive disorder than bipolar disorder. In this disorder, multiple depressive phases alternate with phases of mania, but with less pronounced euphoria. During these phases, family and loved ones may even mistakenly assume that the person is doing well. nine0003
6. Mixed anxiety-depressive disorder
In anxiety-depressive disorder, the clinical picture is very similar to depression, however, in depression, depressive syndromes always come first. In this case, both anxious and depressive symptoms are evenly combined.
7. Depressive psychotic episode
A special form of depressive episode is psychotic or delusional depression. Psychosis is a condition in which people see or hear things that do not exist (hallucinations) and/or have false ideas or beliefs (delusions). There are various types of delusions such as self-accusation for no reason (delusion of guilt), financial ruin (delusions of poverty), feeling of an incomprehensible illness (hypochondriac delusions). People with delusional depression almost always require inpatient psychiatric treatment. Psychotic episodes can be either unipolar or bipolar. nine0003
8. Atypical depression
This type of depression is characterized by hypersensitivity and mood swings, overeating and drowsiness, panic attacks. This type of depression is mild and can be bipolar.
9. Seasonal depressive disorder
This type of depression is similar to atypical depression and comes on seasonally with climate change, usually in autumn or winter.