Mmpi psychological evaluation
What Is the Minnesota Multiphasic Personality Inventory (MMPI)?
Does taking a personality test give you the jitters? Learn all about the MMPI and how it’s meant to help you.
The Minnesota Multiphasic Personality Inventory (MMPI) is one of the most commonly used psychological tests in the United States.
It contains a variety of true/false questions that are scored on a scale used to describe a person’s mental processes and how they manage stress.
Primarily, the MMPI is used to help mental health professionals assess and diagnose mental health conditions such as schizophrenia, depression, and anxiety.
Lawyers also use the MMPI as forensic evidence in criminal defense and custody disputes. According to the publisher of the MMPI, the University of Minnesota Press, employers sometimes use the test in job screenings for high risk public safety positions, such as:
- police officers
- nuclear power plant personnel
- firefighters
- pilots
- air-traffic controllers
The University of Minnesota first published the test by Starke R. Hathaway and J.C. McKinley in 1942 and currently owns the copyright.
The University of Minnesota Press licenses the test to Pearson Assessments and other companies for sales and distribution.
The MMPI is a protected psychological test. This means the test and its materials are not freely available to the public. You won’t find the test items online, except for a few examples.
Only professionals who can provide the required credentials can buy the test from Pearson Assessments.
Types of MMPI tests
There are a variety of versions of the MMPI in general use today:
- MMPI-2. This is the standard adult version of the assessment. It was first released in 1989. It contains 567 true/false questions and takes 60 to 90 minutes to complete. It’s been revised to reflect more culturally diverse values than the original 1942 version.
- MMPI-2-Retracted Form. This version, published in 2008, is a shorter version of the MMPI-2.
 It’s intended for adults and contains 338 true/false items. The MMPI-2-R F takes about half the time as the MMPI-2 to complete, about 40 to 50 minutes.
It’s intended for adults and contains 338 true/false items. The MMPI-2-R F takes about half the time as the MMPI-2 to complete, about 40 to 50 minutes. - MMPI-Adolescent. This is a version of the test released in 1992 for adolescents from 14 to 18 years old. The MMPI-A contains 478 items and takes about 60 minutes to complete.
- MMPI-A-RF. This short form of the test for adolescents was released in 2016. It contains 241 items and takes 25 to 45 minutes to complete.
- MMPI-3. This is the newest version of the MMPI. It was released in 2020. It has updated items, scales, and norms. It contains 335 items and takes 25 to 50 minutes to complete.
These versions of the test are based on different norms and clinical scales.
A norm is a statistic or set of statistics (such as average, standard deviations, and score ranges) that researchers compare an individual’s score against. This helps researchers determine the baseline “normal,” or typical, result.
A scale is a group of questions that measure a person’s tendency toward a certain mental health condition. They can also measure aspects of mental or social functioning that don’t necessarily indicate a disorder.
Each test version also contains varying content scales, clinical subscales, and supplementary scales.
Interpreting the MMPI is a complex process that is closely protected and monitored. This is because the complex scale requires specific training to accurately interpret the results — and misinterpreting the results can have harmful consequences, leading to unnecessary distress.
It’s important to know that the MMPI isn’t a standardized test in the usual sense. It doesn’t use percentile ranks that indicate how well you did on the test. It’s not a test you either pass or fail.
The test is part of a psychological evaluation your clinician will make. The results of the MMPI test will give your clinician a sense of what mental health conditions you might be experiencing.
The MMPI result will be just one factor in the diagnosis the clinician may make and the treatment they’ll recommend. Your mental health and medical history will be considered, along with your experiences.
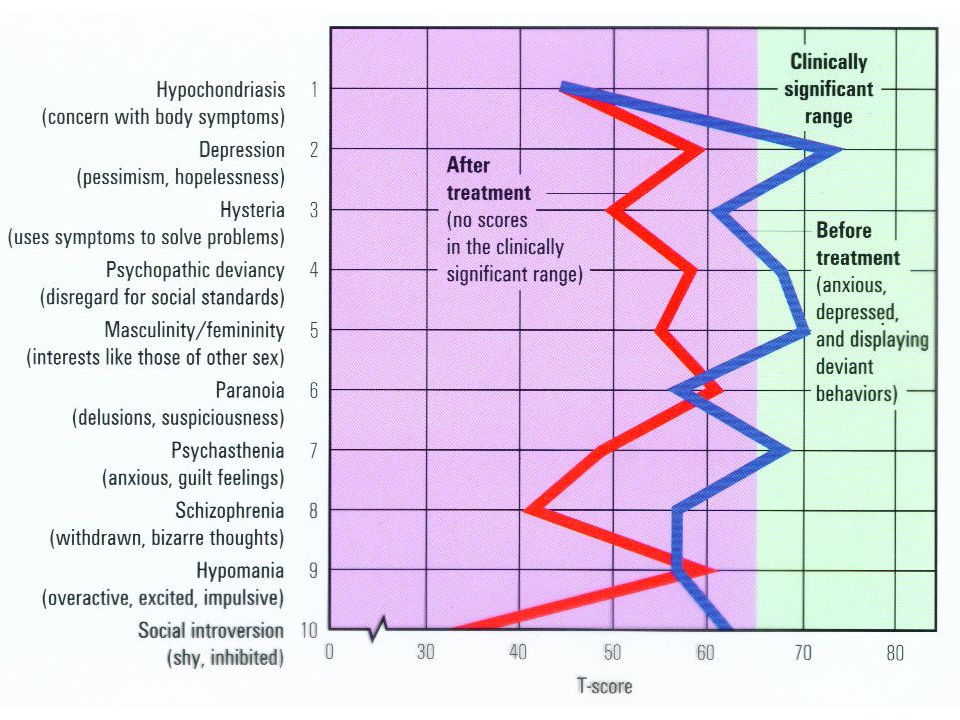
The MMPI has built-in clinical scales that describe a person’s psychological processes and how they respond to stress.
Each scale is made of a specific group of questions (unknown to the test taker), which the test developer’s field research says indicates a particular psychological condition.
The MMPI also has built-in validity scales designed to identify how a person approached the test, such as whether they attempted to present themselves differently from how they actually view themselves.
Here are the 10 clinical scales of the MMPI-2, which is still the most widely used version of the MMPI. These scales overlap, but generally, high scale scores point to a high risk of having a mental health disorder.
1. Hypochondriasis (Hs)
The hypochondriasis scale is designed to detect exaggerated concern over one’s health that is unsupported by medical authority.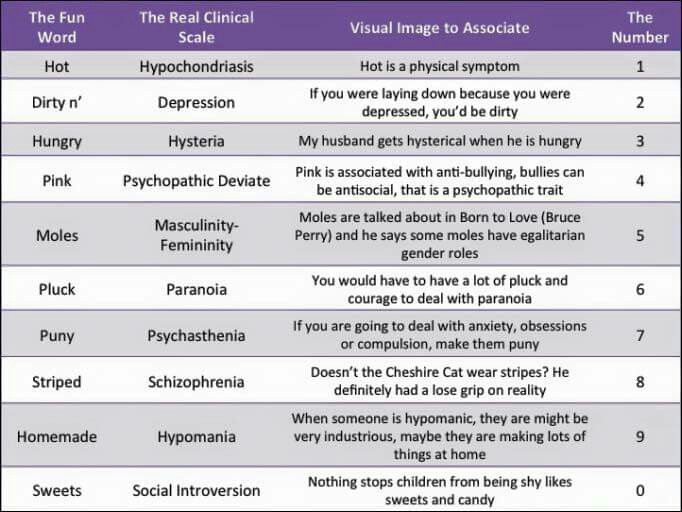 The concerns are usually vague and persist despite not being validated.
The concerns are usually vague and persist despite not being validated.
2. Depression (D)
The depression scale points to aspects related to clinical depression. The related questions concern low morale, overall dissatisfaction in life, and an absence of hope for the future.
3. Hysteria (Hy)
The hysteria scale tracks five aspects of a person:
- poor physical health
- shyness
- cynicism
- headaches
- neuroticism
A high score on this scale could point to a variety of mental health disorders, such as anxiety, paranoia, or dissociative disorders.
4. Psychopathic deviate (Pd)
This scale points to difficulty with family and authority figures.
It also gauges feelings of alienation from self and society as well as boredom.
5. Masculinity/femininity (Mf)
This scale measures how much a person abides by stereotypical masculine and feminine values and roles.
The questions deal with:
- activity interests
- aesthetic preferences
- personal sensitivities
6.
 Paranoia (Pa)
Paranoia (Pa)The paranoia scale identifies aspects of personality, such as grandiose thinking, suspicion toward other people, and rigid thinking.
It also includes items that might reflect delusions.
7. Psychasthenia (Pt)
This scale gauges a person’s ability to resist certain thoughts or behaviors.
This scale identifies abnormal fears, self-criticism, and concentration difficulty.
8. Schizophrenia (Sc)
This scale identifies tendencies toward bizarre thoughts and social alienation.
Its questions deal with:
- family relationships
- impulse control
- questions of self-worth
- sexual difficulties
9. Hypomania (Ma)
This scale identifies unhealthy overactivity expressed as excitement, elevated and unstable mood, and long strings of ideas.
Also included are feelings of grandiosity and egocentricity.
10. Social introversion (Si)
This scale gauges social introversion, which is the tendency to avoid social interactions or feel awkward and withdraw from them.
These items point to a lack of social skills and a preference to be among small groups or alone.
The validity scales attempt to identify deceptive or inconsistent test results. There are a variety of both intentional and unintentional reasons people might try to present themselves other than what they are.
Intentional deception has been known to occur in situations such as:
- employment screening
- attempts to get costly treatment
- disability evaluations
- personal injury lawsuits
- court-ordered evaluations
- competency hearings
- custody proceedings
- unwillingness to cooperate
Unintentional deception might occur for reasons such as:
- illness
- cultural misunderstanding
- test-taking difficulty
The validity scales vary among MMPI versions, but the MMPI-2 contains three general types of validity scales:
- non-responding or inconsistent responding (CNS, VRIN, TRIN)
- over-reporting, or exaggerating psychological symptoms, popularly called “faking bad” (F, Fb, Fp, FBS)
- under-reporting, or reducing psychological symptoms, popularly called “faking good” (L, K, S)
Here are the validity scales usually used in the MMPI-2 assessment. Some have been developed independently from the MMPI-2 test itself.
Some have been developed independently from the MMPI-2 test itself.
- CNS (cannot say). This is a measure of the number of “cannot say” responses.
- VRIN-r (variable response inconsistency). This identifies random responses made without consideration of the content.
- TRIN-r (true response inconsistency). This identifies fixed responding patterns.
- F scale (infrequent responses, 60 items). These are a collection of unlikely and contradictory responses.
- Fb (F back scale). This is the same as the F scale, except it only looks at responses to the second half of the test.
- FBS-r (symptom validity, 43 items). This scale is designed to identify the over-reporting of symptoms. It is popularly referred to as the “faking bad scale” scale.
- L-r (uncommon virtues, 15 items).
 This scale is also called the “lie scale.” It attempts to identify under-reporting of symptoms by test takers to appear in a better light than they actually are.
This scale is also called the “lie scale.” It attempts to identify under-reporting of symptoms by test takers to appear in a better light than they actually are. - K-r (adjustment validity, 30 items). This scale identifies under-reporting by test takers who may be tailoring answers to give the impression of healthy psychological adjustment. It’s also called the “faking good scale.”
- S (superlative self-presentation, 50 items). This scale identifies under-reporting by test takers who are defensive and intentionally distort their responses to try to look better in terms of certain human virtues.
People have always had concerns over the reliability and accuracy of the MMPI ever since it was first published in 1942.
The MMPI has been revised and updated various times to correct gender and racial bias, and to validate the test against new normative samples.
Studies of MMPI accuracy usually focus on specific uses. Reports often vary.
Reports often vary.
For example, a 2021 study concluded that the MMPI-2, when results were evaluated through machine learning, provided reliable accuracy in classifying and predicting suicidal ideation and past suicidal attempts.
Researchers recommended that clinicians could use the MMPI to help detect and treat groups with a high risk of suicide.
The MMPI will probably never receive total approval or total disapproval. It’s one tool within a large diagnostic toolbox, and it’s constantly being reviewed and revised.
It will continue to be tweaked and analyzed, and most likely always be a work in progress.
In the book “Of Psychometric Means: Starke R. Hathaway and the Popularization of the Minnesota Multiphasic Personality Inventory,” authors Rebecca Schilling and Stephen T. Casper conclude that the MMPI gives behavioral health professionals a starting point from which to build diagnoses and initiate treatment.
They point out that the MMPI can also help test takers to consider their mental health and better understand their own psychology.
Consider speaking with a doctor or a mental health professional to help you determine which type of MMPI test best aligns with your unique mental health experience.
If you’re going to take the MMPI test, there really is no way to prepare. The best you can do is to be well-rested for the test and answer the questions truthfully.
It’s also good to remember the test is designed to be a helping tool, one that can give both you and your mental health professionals a clearer vision of one precious and unique human personality.
What Is the Minnesota Multiphasic Personality Inventory (MMPI)?
Does taking a personality test give you the jitters? Learn all about the MMPI and how it’s meant to help you.
The Minnesota Multiphasic Personality Inventory (MMPI) is one of the most commonly used psychological tests in the United States.
It contains a variety of true/false questions that are scored on a scale used to describe a person’s mental processes and how they manage stress.
Primarily, the MMPI is used to help mental health professionals assess and diagnose mental health conditions such as schizophrenia, depression, and anxiety.
Lawyers also use the MMPI as forensic evidence in criminal defense and custody disputes. According to the publisher of the MMPI, the University of Minnesota Press, employers sometimes use the test in job screenings for high risk public safety positions, such as:
- police officers
- nuclear power plant personnel
- firefighters
- pilots
- air-traffic controllers
The University of Minnesota first published the test by Starke R. Hathaway and J.C. McKinley in 1942 and currently owns the copyright.
The University of Minnesota Press licenses the test to Pearson Assessments and other companies for sales and distribution.
The MMPI is a protected psychological test. This means the test and its materials are not freely available to the public. You won’t find the test items online, except for a few examples.
Only professionals who can provide the required credentials can buy the test from Pearson Assessments.
Types of MMPI tests
There are a variety of versions of the MMPI in general use today:
- MMPI-2. This is the standard adult version of the assessment. It was first released in 1989. It contains 567 true/false questions and takes 60 to 90 minutes to complete. It’s been revised to reflect more culturally diverse values than the original 1942 version.
- MMPI-2-Retracted Form. This version, published in 2008, is a shorter version of the MMPI-2. It’s intended for adults and contains 338 true/false items. The MMPI-2-R F takes about half the time as the MMPI-2 to complete, about 40 to 50 minutes.
- MMPI-Adolescent. This is a version of the test released in 1992 for adolescents from 14 to 18 years old. The MMPI-A contains 478 items and takes about 60 minutes to complete.
- MMPI-A-RF. This short form of the test for adolescents was released in 2016.
 It contains 241 items and takes 25 to 45 minutes to complete.
It contains 241 items and takes 25 to 45 minutes to complete. - MMPI-3. This is the newest version of the MMPI. It was released in 2020. It has updated items, scales, and norms. It contains 335 items and takes 25 to 50 minutes to complete.
These versions of the test are based on different norms and clinical scales.
A norm is a statistic or set of statistics (such as average, standard deviations, and score ranges) that researchers compare an individual’s score against. This helps researchers determine the baseline “normal,” or typical, result.
A scale is a group of questions that measure a person’s tendency toward a certain mental health condition. They can also measure aspects of mental or social functioning that don’t necessarily indicate a disorder.
Each test version also contains varying content scales, clinical subscales, and supplementary scales.
Interpreting the MMPI is a complex process that is closely protected and monitored. This is because the complex scale requires specific training to accurately interpret the results — and misinterpreting the results can have harmful consequences, leading to unnecessary distress.
This is because the complex scale requires specific training to accurately interpret the results — and misinterpreting the results can have harmful consequences, leading to unnecessary distress.
It’s important to know that the MMPI isn’t a standardized test in the usual sense. It doesn’t use percentile ranks that indicate how well you did on the test. It’s not a test you either pass or fail.
The test is part of a psychological evaluation your clinician will make. The results of the MMPI test will give your clinician a sense of what mental health conditions you might be experiencing.
The MMPI result will be just one factor in the diagnosis the clinician may make and the treatment they’ll recommend. Your mental health and medical history will be considered, along with your experiences.
The MMPI has built-in clinical scales that describe a person’s psychological processes and how they respond to stress.
Each scale is made of a specific group of questions (unknown to the test taker), which the test developer’s field research says indicates a particular psychological condition.
The MMPI also has built-in validity scales designed to identify how a person approached the test, such as whether they attempted to present themselves differently from how they actually view themselves.
Here are the 10 clinical scales of the MMPI-2, which is still the most widely used version of the MMPI. These scales overlap, but generally, high scale scores point to a high risk of having a mental health disorder.
1. Hypochondriasis (Hs)
The hypochondriasis scale is designed to detect exaggerated concern over one’s health that is unsupported by medical authority. The concerns are usually vague and persist despite not being validated.
2. Depression (D)
The depression scale points to aspects related to clinical depression. The related questions concern low morale, overall dissatisfaction in life, and an absence of hope for the future.
3. Hysteria (Hy)
The hysteria scale tracks five aspects of a person:
- poor physical health
- shyness
- cynicism
- headaches
- neuroticism
A high score on this scale could point to a variety of mental health disorders, such as anxiety, paranoia, or dissociative disorders.
4. Psychopathic deviate (Pd)
This scale points to difficulty with family and authority figures.
It also gauges feelings of alienation from self and society as well as boredom.
5. Masculinity/femininity (Mf)
This scale measures how much a person abides by stereotypical masculine and feminine values and roles.
The questions deal with:
- activity interests
- aesthetic preferences
- personal sensitivities
6. Paranoia (Pa)
The paranoia scale identifies aspects of personality, such as grandiose thinking, suspicion toward other people, and rigid thinking.
It also includes items that might reflect delusions.
7. Psychasthenia (Pt)
This scale gauges a person’s ability to resist certain thoughts or behaviors.
This scale identifies abnormal fears, self-criticism, and concentration difficulty.
8. Schizophrenia (Sc)
This scale identifies tendencies toward bizarre thoughts and social alienation.
Its questions deal with:
- family relationships
- impulse control
- questions of self-worth
- sexual difficulties
9. Hypomania (Ma)
This scale identifies unhealthy overactivity expressed as excitement, elevated and unstable mood, and long strings of ideas.
Also included are feelings of grandiosity and egocentricity.
10. Social introversion (Si)
This scale gauges social introversion, which is the tendency to avoid social interactions or feel awkward and withdraw from them.
These items point to a lack of social skills and a preference to be among small groups or alone.
The validity scales attempt to identify deceptive or inconsistent test results. There are a variety of both intentional and unintentional reasons people might try to present themselves other than what they are.
Intentional deception has been known to occur in situations such as:
- employment screening
- attempts to get costly treatment
- disability evaluations
- personal injury lawsuits
- court-ordered evaluations
- competency hearings
- custody proceedings
- unwillingness to cooperate
Unintentional deception might occur for reasons such as:
- illness
- cultural misunderstanding
- test-taking difficulty
The validity scales vary among MMPI versions, but the MMPI-2 contains three general types of validity scales:
- non-responding or inconsistent responding (CNS, VRIN, TRIN)
- over-reporting, or exaggerating psychological symptoms, popularly called “faking bad” (F, Fb, Fp, FBS)
- under-reporting, or reducing psychological symptoms, popularly called “faking good” (L, K, S)
Here are the validity scales usually used in the MMPI-2 assessment. Some have been developed independently from the MMPI-2 test itself.
- CNS (cannot say). This is a measure of the number of “cannot say” responses.
- VRIN-r (variable response inconsistency). This identifies random responses made without consideration of the content.
- TRIN-r (true response inconsistency). This identifies fixed responding patterns.
- F scale (infrequent responses, 60 items). These are a collection of unlikely and contradictory responses.
- Fb (F back scale). This is the same as the F scale, except it only looks at responses to the second half of the test.
- FBS-r (symptom validity, 43 items). This scale is designed to identify the over-reporting of symptoms. It is popularly referred to as the “faking bad scale” scale.
- L-r (uncommon virtues, 15 items).
This scale is also called the “lie scale.” It attempts to identify under-reporting of symptoms by test takers to appear in a better light than they actually are.
- K-r (adjustment validity, 30 items). This scale identifies under-reporting by test takers who may be tailoring answers to give the impression of healthy psychological adjustment. It’s also called the “faking good scale.”
- S (superlative self-presentation, 50 items). This scale identifies under-reporting by test takers who are defensive and intentionally distort their responses to try to look better in terms of certain human virtues.
People have always had concerns over the reliability and accuracy of the MMPI ever since it was first published in 1942.
The MMPI has been revised and updated various times to correct gender and racial bias, and to validate the test against new normative samples.
Studies of MMPI accuracy usually focus on specific uses. Reports often vary.
For example, a 2021 study concluded that the MMPI-2, when results were evaluated through machine learning, provided reliable accuracy in classifying and predicting suicidal ideation and past suicidal attempts.
Researchers recommended that clinicians could use the MMPI to help detect and treat groups with a high risk of suicide.
The MMPI will probably never receive total approval or total disapproval. It’s one tool within a large diagnostic toolbox, and it’s constantly being reviewed and revised.
It will continue to be tweaked and analyzed, and most likely always be a work in progress.
In the book “Of Psychometric Means: Starke R. Hathaway and the Popularization of the Minnesota Multiphasic Personality Inventory,” authors Rebecca Schilling and Stephen T. Casper conclude that the MMPI gives behavioral health professionals a starting point from which to build diagnoses and initiate treatment.
They point out that the MMPI can also help test takers to consider their mental health and better understand their own psychology.
Consider speaking with a doctor or a mental health professional to help you determine which type of MMPI test best aligns with your unique mental health experience.
If you’re going to take the MMPI test, there really is no way to prepare. The best you can do is to be well-rested for the test and answer the questions truthfully.
It’s also good to remember the test is designed to be a helping tool, one that can give both you and your mental health professionals a clearer vision of one precious and unique human personality.
Lie scale L of the MMPI method (SMIL)
Doctor Demkin's blog
Articles about psychology and psychodiagnostics
- Are you here:
- Home
- Blog
- Psychodiagnostics
- MMPI Lie L Scale (SMIL)
Psychodiagnostics
Lie scale L MMPI (SMIL, MMIL, SKLO, MLO)
Important! The “Lies” scale does not at all characterize the “truthfulness” or “falsehood” of a person. It is impossible to professionally judge the nature of the increase in indicators on a scale of L based solely on individual test results.
The Lie Scale was originally developed as a measure of overall honesty on the MMPI. Characteristics associated with higher L scores include defensive defensiveness, rigidity of mind, and a desire to put on a “good facade” (Butcher & Perry, 2008, p. 31). For example, people who feel unfairly accused or condemned, may show an understandable defensive reaction and try to present themselves as virtuous carriers of high moral standards, can be observed to increase on the scale. Indicators on the L scale are directly related to the level of education and occupation. For example, priests or deeply religious people who do have strong moral values may score high on the L scale.
Profiles with elevated values of the lie scale should be interpreted with caution, since the generalized reaction of an individual with claims to excessive virtue or denial of socially undesirable shortcomings, most likely, could distort the whole picture of personality reflected in the MMPI profile. High scores on the L scale, as a rule, correlate with distortion of answers to questions on clinical scales. This leads to a profile that underestimates the number and extent of problems a client or patient may have. In the setting of psychological care, a high L score is generally considered a negative indicator that indicates a person's unwillingness or inability to self-disclose.
The scale consists of statements whose content is very obvious. This is a description of relatively minor shortcomings that most people are willing to admit, such as: "I get angry sometimes. " However, when a deliberately false answer is given to most of these statements, it becomes obvious that the subject claims more virtue and presents himself more favorably than most other people.
Factors affecting the performance of the lie scale L
An increase in the L scale may be due to a number of reasons.
- People from lower socioeconomic backgrounds, with a lack of education, are likely to score slightly lower on the L scale than those with higher education and higher socioeconomic status.
- People with limited intelligence or lack of psychological sophistication may also score high L's in their attempts to look good.
- An individual may attempt to make a favorable impression in a recruiting or psychological assessment test situation in order to make a positive impression on the examiner.
- Some subcultural groups (eg, priests, monks, religious people), as well as some ethnic minorities, such as Hispanics (see Butcher, Cabiya, Lucio, and Garrido, 2007), may tend to display a more favorable image on psychological testing.
- Some patients with neurotic and psychosomatic disorders are prone to a general defensive reaction, which is reflected in an increase in the L scale.
- Personal characteristics: naivete, weak emotional intelligence, tendency to defensive reactions, psychological defense in the form of denial, "hysterical" thinking. They often have a rigid mindset and low adaptive capacity with a strong need to "put up a good facade" of their personality.
- L scores may be elevated by psychological pressure,
due to psychotic disorder with marked paranoid features
(Coyle & Heap, 1965; Fjordbak, 1985). - The L scale can also be increased in people who did not carefully delve into the content of the statements, but tried to "pass" the test.
Lie scale descriptors L
Complaints: subjective feeling of unfair treatment or condemnation, unfair criticism or accusation.
Thoughts: Judgmental, moralistic, lacking insight, inflexible, psychologically naive
Emotions: Self-control, denial, emotional stiffness Strengths : Good self-control, conscientiousness, willingness to conform, high standards, independence, autonomy
Lifestyle and parent-child relationships
Without additional interview, it is difficult for the researcher to understand whether a high score on the L scale is the result of a conscious defensive attitude or an unconscious rigidity of moral values and a lack of psychological sophistication. High L scores can be obtained from intelligent and educated people who have strict moral values. When identifying harsh and judgmental attitudes, the style of parenting should be assessed for a history of strict and uncompromising parental moral requirements. If high L values are due to the fear of being misjudged, and reflects a conscious
attempt to “pass” the test, it is recommended to explore fears about how the test results will be used.
Modifying scales
- When the K correction scale is also increased, the high L is probably associated with
conscious control of one's positive image. If other scales are within the normal range, then an increase in L may reflect a rigid style of thinking in black and white categories, reflecting a rigid and subjective personality style with values that do not allow for shades of gray. - When scale 6 is also elevated, the L score may indicate a fear of being judged
and criticized. This combination is not uncommon in forensic aspects of psychological examination and/or paranoid disorder.
High scores on the L scale
A good assessment of the reasons for the increase in the L scale requires that the demographic characteristics of the person be taken into account first of all. Thus, higher rates in people with higher education are not the norm, but may be normal for people from the lower class or people from the middle class without higher education or people in working occupations. which are workers. On the contrary, if a person with a higher education scores high on the L scale, it is necessary to find out if this can be explained by his occupation (for example, clergy or monasticism).
If the rating on the lie scale is high, this may indicate that the person describes himself in an overly favorable light. This can be the result of not only deliberate deception, but also an unrealistic view of oneself. Such subjects may be inflexible, unoriginal, and unaware of the impression they make on others by perceiving their world in a rigid, egocentric manner. As a result of their rigidity, they may have a low tolerance for stress. They will stubbornly deny any of their shortcomings, their understanding of themselves will be very difficult. Such people are poor candidates for psychotherapy. Extremely high scores indicate that the subjects are extremely rigid and will experience difficulties in relationships. This may be the case in paranoid disorders, in which patients place great importance on denying their personal shortcomings and projecting them onto others instead. Extremely high scores can also be the result of deliberate deception on the part of apparently anti-social individuals.
Low scores on L
Low scores indicate that subjects were frank and open about their responses. They are able to admit minor flaws in themselves and can also be articulate, relaxed, outgoing, open and confident. Low scores can also indicate clients who are somewhat sarcastic and cynical.
Subject feedback
It is important for the clinician to use client feedback statements to establish rapport and trust, to explore and determine the source of L-scale deviation from the norm: whether an increase in the L-scale reflects unconscious psychological rigidity, a conscious distortion of self-image, or some combination of these two factors.
In cases where the increase in the L scale is the result of emotional contraction, denial, lack of insight and a judgmental, critical personality structure, one should look for a history of parenting by disapproving, picky parents who instilled inflexible views on values.
If an increase in the L scale is associated with a defensive reaction, then the clinician needs to investigate whether this reflects a conscious form of control to simulate a positive impression of oneself (“built a facade”) or, less often, an unconscious defensive reaction.
As a rule, the higher the scores on the L scale, the lower the scores on the clinical scales. However, in some cases, an increase in the L scale is associated with an increase in clinical scales 1, 2 and 3, reflecting suppressed somatic depression. In such cases, an increase in L may reflect a conscious management of positive impressions, as well as a rigid, naive organization of the personality, congruent with increases in the hypochondria, depression, and hysteria (conversion) scales. The following statements for feedback with the subject will allow the clinician to establish a dialogue to clarify the reasons for the deviation of the L scale from the norm.
Normal range feedback ( T-scores from 50 to 65 - MMPI-2 and up to 70 - MMPI, SMIL, MMIL)
Your score on this scale is within the normal range. You have been able to strike a balance between honesty and the temptation to create an overly favorable impression of yourself. You confessed to ordinary human flaws, showing that you have good self-awareness and self-confidence. You were honest about your strengths and weaknesses.
Upscale feedback L ( T-scores > 65– MMPI-2 and above 70– MMPI, SMIL, MMIL)
Your profile suggests that you may feel vulnerable to judgment . You may have taken the test against your will, or you may think that the results will be used against you. You have answered a number of questions that indicate that you want the psychologist to know that you are a person who has high moral standards. People with your profile tend to have shared values and strong beliefs about the right and wrong way to do things. People may think of you as being too direct and uncomfortable with people who don't share your values.
Because you have high personal standards and such a strong sense of right and wrong behavior, others may think that you are somewhat judgmental or critical of them. People with your profile may be perceived as being too demanding on the morals and ethics of other people.
You work hard to follow the rules and do the right thing. You have responded to the statements in a way that suggests that you are in control of your emotions to ensure that your feelings and behavior are above moral reproach.
The way you answered the test questions indicates that you tend to see the world in a somewhat black and white color. Because of this, people may decide that you lack an understanding of normal human weaknesses. Because of your high moral standards, you may find yourself not knowing the shades of gray that is typical of most people's moral judgment.
It is possible that you answered the test carefully, trying to show only your best side, wanting to minimize the possibility of others judging or criticizing you. Perhaps you are the kind of person who walks through life cautiously, doing nothing that might cause others to pick on you.
People may perceive what you see as the right attitude to morality as
something rigid and inflexible. Your high standards can cause others to perceive you as a
perfectionist, often unreasonably critical of others. People may find it difficult to live up to your high standards and may want to argue with you or resist your values.
You may have grown up in an environment where parents or caregivers were overly critical and judgmental and moral standards were too difficult. Perhaps you follow a strict religious code of conduct that does not allow for shades of gray in morality. It's also possible that you're afraid of how the test results could be used against you, so you've been careful to only show your "better side".0019
Psychological help and therapeutic pitfalls
Reaffirming clients' desire to be above moral reproach would be the first important factor
in starting to build a therapeutic alliance. It is necessary to avoid developing in the client a feeling of condemnation from the therapist, which contributes to the development of countertransference due to a defensive and judgmental position. Teaching clients that people have different values, and that the rigidity of their own position can make other people around them become defensive, can help them become more flexible. It is also necessary to examine the early parental demands and strictness of parenting, and how the child tried to be "nice" and "pleasant" in order to avoid criticism.
People who score between 55 and 64 T-scores (up to 69 for MMPI, SMIL, MMIL, MLO) on the L scale engage in overly virtuous self-descriptions that can be counterproductive in therapy. A very principled, virtuous, and impeccable self-description should be a signal to the therapist that frank, direct, and open communication with the client is likely to be difficult. This difficulty in expressing oneself and one's feelings can be caused by a number of factors, including belonging to special subgroups of the population, such as the clergy, job seekers, who have a strong need to demonstrate their responsibility and honesty.
If the L scale is raised to 65 (70) or more T-scores, in the context of treatment evaluation, then therapy is unlikely to proceed well, progress will be insignificant, and premature discontinuation of therapy is very likely. People with unrealistically high claims to virtue are too rigid and "perfect" to change their sense of self much. They usually do not see the need to discuss their problems or change their behavior.
Client / patient advice
1. Talk to your therapist about using cognitive behavioral tools to change your black-and-white all-or-nothing mindset.
2. Work with your therapist to explore any early experiences where you
felt you should be above criticism. Once you identify these experiences, you and your therapist can use cognitive behavioral techniques to try to rethink and change these early childhood assumptions.
3. Because you tend to be a perfectionist, use “thought-stopping” techniques that can help you deal with negative thoughts about things you don’t do or others don’t do “good enough. ” Whenever you become aware of your critical thoughts, insistently tell yourself, “Stop.” Some people find it helpful to visualize a big red road sign at the same time. Some critical and negative thoughts tend to recur, so repeat the stopping technique until the negative thought is gone from your mind. You can then replace it with a more positive and constructive thought: for example, "I've felt this before and I know I can handle it" .
Andrey Demkin
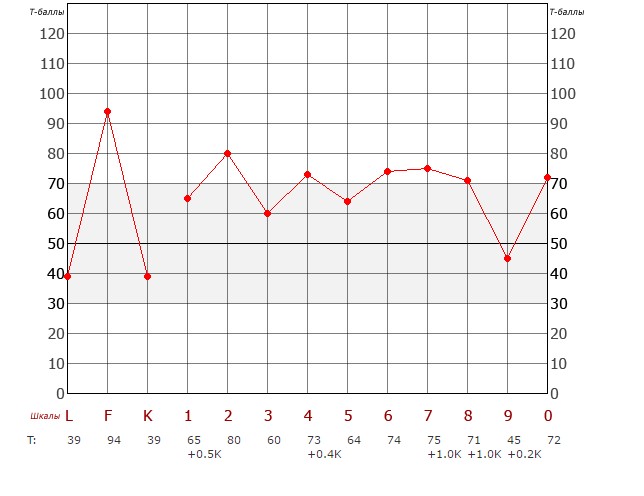
L - Lie F - Reliability K - Correction 1 - Hypochondria 2 - Depression 3 - Hysteria 4 - Psychopathy 6 - Paranoia 7 - Psychasthenia 8 - Schizophrenia 9 - Hypomania 0 - Introversion
- Back
- Forward
Related articles:
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Dr. Andrey Demkin
Professional psychological methods: MMPI, Szondi, Leary
- Material Information
- Psychodiagnostics
- Views: 8967
- Previous article Basic methods of psychology
- Next article Attention Research Methods (Luria)
Set font
- Size
- Style
- Reading mode
A great help to the practicing psychologist in diagnosing and establishing the personality traits of a patient is provided by standard testing methods developed and improved by leading experts throughout the twentieth century.
![]()
Psychodiagnostic testing is convenient because it makes it possible to create the most objective psychological portrait of the patient's personality, reveal his deeply hidden mental processes and inclinations, assess the quality of his relationships with other people and self-esteem. All this allows the most objective approach to identifying the problems that really exist and are felt by the patient, and therefore, to be able to help him. The most common methods of psychodiagnostic testing today include the following tests:
- MMPI (SMIL)
- Sondi test
- Leary test.
Russian-language versions of the methods with the possibility of online testing are available at http://www.psychol-ok.ru/. The MMPI questionnaire was created in the early 40s by American psychologists, translated into Russian and adapted for our country in the 60s. Subsequently, the test was repeatedly refined and improved, at the moment the most used option is the SMIL test, adapted by the psychologist L. N. Sobchik. It is considered the most reliable study of personality, giving an objective assessment of its individual psychological characteristics. The questionnaire consists of 566 statements, each of which the researcher must evaluate as true or false in relation to himself.
The MMPI test (SMIL) is now used not only in clinical psychology and psychiatry, but also in many other areas of human activity that require an assessment of personal characteristics. These are forensic psychological examination and the penitentiary system, education and sports, work with personnel, family counseling, assessment of professional suitability in a number of departments of the Ministry of Internal Affairs and the armed forces.
The Szondi test, named after its author, is a tool for identifying the mental processes of a person. It is based on an assessment of combinations of the patient's eight basic types of drives, the most pronounced of which correspond to his strongest needs or problems. The test is a set of 48 portraits of people with severe mental disorders, divided into series, in each of which the subject is asked to choose the most and least attractive faces for him. The test helps to reveal not only personality traits and motives of actions, realized by the patient himself, but also deeply hidden, unconscious tendencies of behavior. The Szondi test is used not only in clinical practice, but also in other areas: professional selection and training, methods of working with personnel, forensic psychological examination, etc.
The Leary test was developed in the middle of the twentieth century by a group of psychologists led by T. Leary, and is used to study the patient's self-esteem and his relationships with people based on two main factors: the degree of dominance and the degree of aggressiveness. Testing reveals the level of adaptability of the patient, i.e. his ability to change his behavior in order to achieve his goals and the ability to build relationships in a team.