Mixed state symptoms
Mixed Bipolar Disorder Symptoms, Causes, and Treatments
Written by Matthew Hoffman, MD
In this Article
- What Are Mixed Episodes in Bipolar Disorder?
- Who Gets Mixed Bipolar Episodes?
- What Are the Symptoms of a Mixed Features Episode?
- What Are the Risks of Mixed Features During Mood Episodes of Bipolar Disorder?
- What Are the Treatments for Mood Episodes With Mixed Features in Bipolar Disorder?
What Are Mixed Episodes in Bipolar Disorder?
Mixed features refers to the presence of high and low symptoms occurring at the same time, or as part of a single episode, in people experiencing an episode of mania or depression. In most forms of bipolar disorder, moods alternate between elevated and depressed over time. A person with mixed features experiences symptoms of both mood "poles" -- mania and depression -- simultaneously or in rapid sequence.
Who Gets Mixed Bipolar Episodes?
Virtually anyone can develop bipolar disorder. About 2.5% of the U.S. population -- nearly 6 million people -- has some form of bipolar disorder.
Mixed episodes are common in people with bipolar disorder -- half or more of people with bipolar disorder have at least some mania symptoms during a full episode of depression. Those who develop bipolar disorder at a younger age, particularly in adolescence, may be more likely to have mixed episodes. People who develop episodes with mixed features may also develop "pure" depressed or "pure" manic or hypomanic phases of bipolar illness. People who have episodes of major depression but not full episodes of mania or hypomania also can sometimes have low-grade mania symptoms. These are symptoms that are not severe or extensive enough to be classified as bipolar disorder. This is referred to as an episode of "mixed depression" or a unipolar (major) depressive episode with mixed features.
Most people are in their teens or early 20s when symptoms from bipolar disorder first start. It is rare for bipolar disorder to develop for the first time after age 50. People who have an immediate family member with bipolar are at higher risk.
It is rare for bipolar disorder to develop for the first time after age 50. People who have an immediate family member with bipolar are at higher risk.
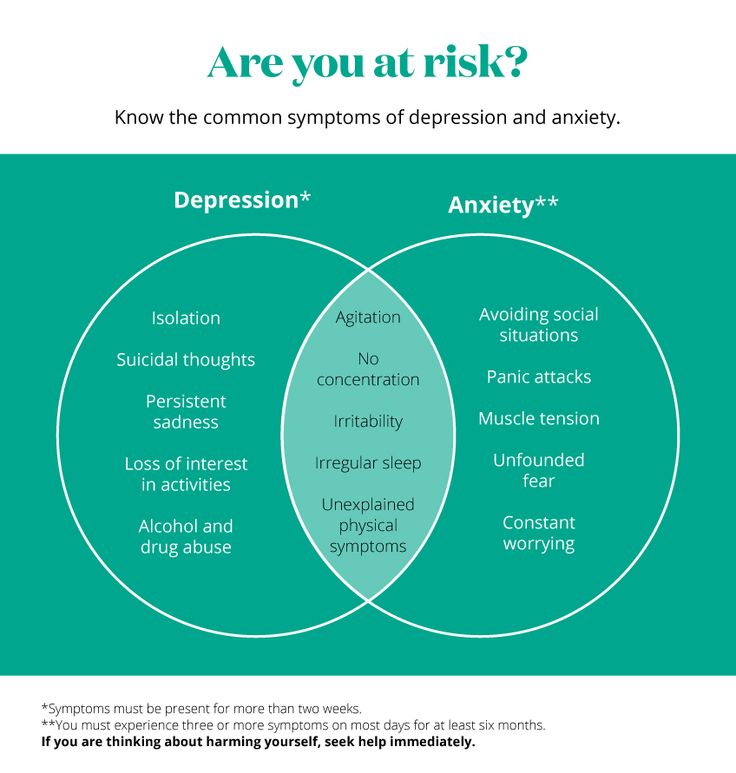
What Are the Symptoms of a Mixed Features Episode?
Mixed episodes are defined by symptoms of mania and depression that occur at the same time or in rapid sequence without recovery in between..
- Mania with mixed features usually involves irritability, high energy, racing thoughts and speech, and overactivity or agitation.
- Depression during episodes with mixed features involves the same symptoms as in "regular" depression, with feelings of sadness, loss of interest in activities, low energy, feelings of guilt and worthlessness, and thoughts of suicide.
This may seem impossible. How can someone be manic and depressed at the same time? The high energy of mania with the despair of depression are not mutually exclusive symptoms, and their co-occurrence may be much more common than people realize.
For example, a person in an episode with mixed features could be crying uncontrollably while announcing they have never felt better in their life. Or they could be exuberantly happy, only to suddenly collapse in misery. A short while later they might suddenly return to an ecstatic state.
Mood episodes with mixed features can last from days to weeks or sometimes months if untreated. They may recur ,and recovery can be slower than during episodes of "pure" bipolar depression or "pure" mania or hypomania.
What Are the Risks of Mixed Features During Mood Episodes of Bipolar Disorder?
The most serious risk of mixed features during a manic or depressive episode is suicide. People with bipolar disorder are 10 to 20 times more likely to commit suicide than people without bipolar disorder. Tragically, as many as 10% to 15% of people with bipolar disorder eventually lose their lives to suicide.
Evidence shows that during episodes with mixed features, people may be at even higher risk for suicide than people in episodes of bipolar depression.
Treatment reduces the likelihood of serious depression and suicide. Lithium (Eskalith, Lithobid) in particular, taken long term, may help to reduce the risk of suicide.
People with bipolar disorder are also at higher risk for substance abuse. Nearly 60% of people with bipolar disorder abuse drugs or alcohol. Substance abuse is associated with more severe or poorly controlled bipolar disorder.
What Are the Treatments for Mood Episodes With Mixed Features in Bipolar Disorder?
Manic or depressive episodes with mixed features generally require treatment with medication. Unfortunately, such episodes are more difficult to control than an episode of pure mania or depression. The main drugs used to treat episodes with mixed features are mood stabilizers and antipsychotics.
Mood Stabilizers
While lithium is often considered a gold standard treatment for mania, it may be less effective when mania and depression occur simultaneously, as in a manic episode with mixed features. Lithium has been used for more than 60 years to treat bipolar disorder. It can take weeks to work fully, making it better for maintenance treatment than for acute manic episodes. Blood levels of lithium and other lab test results must be monitored to avoid side effects.
Lithium has been used for more than 60 years to treat bipolar disorder. It can take weeks to work fully, making it better for maintenance treatment than for acute manic episodes. Blood levels of lithium and other lab test results must be monitored to avoid side effects.
Valproic acid (Depakote) is an antiseizure medication that also levels out moods in bipolar disorder. It has a more rapid onset of action, and in some studies has been shown to be more effective than lithium for the treatment of manic episodes with mixed features.
Some other antiseizure drugs, such as and carbamazepine (Tegretol) and lamotrigine (Lamictal), are also effective mood stabilizers.
Antipsychotics
Many atypical antipsychotic drugs are effective FDA-approved treatments for manic episodes with mixed features. These includearipiprazole (Abilify), asenapine (Saphris), cariprazine (Vraylar), olanzapine (Zyprexa), quetiapine (Seroquel), risperidone (Risperdal), and ziprasidone (Geodon). Antipsychotic drugs are also sometimes used alone or in combination with mood stabilizers for preventive treatment.
Antipsychotic drugs are also sometimes used alone or in combination with mood stabilizers for preventive treatment.
Electroconvulsive Therapy (ECT)
Despite its frightening reputation, electroconvulsive therapy (ECT) is an effective treatment for any phase of bipolar disorder, including manic episodes with mixed features. ECT can be helpful if medication fails or can't be used.
Treatment for Depression in Mixed Bipolar Disorder
Common antidepressants such as fluoxetine (Prozac, Sarafem), paroxetine (Paxil), and sertraline (Zoloft) have been shown to worsen mania symptoms without necessarily improving depressive symptoms when depressive and manic symptoms occur together. Most experts therefore advise against using antidepressants during episodes with mixed features. Mood stabilizers (particularly Depakote), as well as atypical antipsychotic drugs, are considered the first-line treatments for mood episodes with mixed features.
Bipolar disorder usually involves recurrences of mixed, manic, or depressed phases of illness. Therefore, it is usually recommended that medications be continued in an ongoing fashion after an acute episode resolves in order to prevent relapses. This is sometimes called maintenance treatment.
Therefore, it is usually recommended that medications be continued in an ongoing fashion after an acute episode resolves in order to prevent relapses. This is sometimes called maintenance treatment.
Bipolar Disorder Guide
- Overview
- Symptoms & Types
- Treatment & Prevention
- Living & Support
Understanding Bipolar Disorder with Mixed Features (Mixed State)
Bipolar disorder is often thought of as a condition with alternating periods of depression and mania. While some people do experience distinct periods of each, many people with bipolar disorder may experience symptoms of both depression and mania at the same time.
This is now called bipolar disorder with mixed features, but it was previously known as mixed state bipolar disorder.
Bipolar disorder with mixed features is thought to affect one-third to half of people with bipolar disorder. Knowing more about this condition can help you make informed decisions about your treatment plan.
Knowing more about this condition can help you make informed decisions about your treatment plan.
“Mixed state bipolar” or “bipolar with mixed states” are outdated terms previously used as a specifier for bipolar disorder. A specifier is a term used to describe characteristics of mental health conditions like mood disorders.
When the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) was released in 2013, the specifier became “mixed features” rather than “mixed state.”
If you have bipolar disorder with mixed features, you experience symptoms of both manic and depressive episodes.
This means you can have a depressive episode with mixed features, where the main symptoms are depressive but subclinical manic symptoms are also present. For example, you may feel depressed and also experience racing thoughts or rapid speech.
Or you can have a manic episode with mixed features, where the main symptoms are those of a manic episode but depressive symptoms are also present. For example, you may be doing several high-energy activities, but you also feel depressed.
For example, you may be doing several high-energy activities, but you also feel depressed.
Symptoms of bipolar disorder with mixed features may vary, depending on the mood episode in question. They can include:
- feeling a mixture of elevated and low moods
- doing pleasurable activities but still having depressive symptoms
- experiencing low mood with rapid speech
- experiencing elevated mood with suicidal ideation
- experiencing severely disturbed sleep
- having a severe disruption of appetite
It’s important to note that how well an individual functions in their everyday life can vary, depending on their exact diagnosis and symptoms.
For bipolar disorder with mixed features, the diagnostic criteria in the DSM-5 include the following, according to a 2017 review:
- three or more manic or hypomanic symptoms during a major depressive episode
- three or more depressive symptoms during a manic or hypomanic episode
Once bipolar disorder is diagnosed, a clinician may add a specifier like “with mixed features,” depending on the reported mood episodes and symptoms.
There’s no specific known cause of bipolar with mixed features, but experts have some insights about potential causes.
Researchers suspect one factor is a change in the functioning of a part of the brain called the hypothalamus. These changes may contribute to sleep problems many people with bipolar disorder report. Sleep problems, difficulty falling asleep or staying asleep, may also affect the ability to regulate moods. Both sleep disturbances and variable moods seem to follow seasonal patterns and may be associated with changes in the intensity of available natural light.
In addition, people with bipolar disorder may also experience changing hormone levels which have been found to be related to functions of the hypothalamus as well.
Every person with bipolar disorder shows manic and depressive symptoms to some extent. But different factors trigger mood changes differently for each person. Some people switch or cycle between often extreme mood states rapidly, others more slowly.
More research needs to be done on potential triggers in order to find out the exact causes of these mood changes.
Sometimes people with bipolar depression may switch into manic or hypomanic states if they’re taking certain antidepressants called tricyclic antidepressants.
Mixed episodes are more likely to happen in these cases. In fact, long-term treatment with tricyclic antidepressants has been associated with mood changes in up to 70 percent of people taking them.
The antidepressant bupropion has also been associated with mood changes, even when a person is taking mood stabilizers at the same time.
So, looking at what medications a person is taking may give some insight into mood changes. There may also be genetic changes, but more research is needed.
Certain risk factors do exist for bipolar disorder, but specific risk factors for bipolar disorder with mixed episodes are not known.
According to a 2008 review, children may have greater chances of developing later bipolar disorder if they have a first-degree relative who has bipolar disorder and:
- a subsyndromal form of bipolar disorder
- a major depressive episode with manic symptoms
- possibly, ADHD with mood fluctuation
No single neurobiological risk factor has been found for bipolar disorder, but others may include:
- a stressful event or major life change
- drug misuse
- certain elements of brain structure and development, such as the prefrontal cortex, hippocampus, and hypothalamus
Finding care for bipolar disorder
Finding care for bipolar disorder can be challenging and confusing. Sometimes it’s hard to figure out where to start. Here are some suggestions:
Sometimes it’s hard to figure out where to start. Here are some suggestions:
- National Alliance on Mental Illness HelpLine
- Substance Abuse and Mental Health Services Administration Mental Illness Treatment Locator
There’s no known way to prevent bipolar disorder. However, if you experience a mixed episode during treatment, your care team can work on figuring out what might have caused it, then adjust any necessary medication or work with you on lifestyle behaviors.
Managing episodes with mixed features is part of the treatment for bipolar disorder.
Episodes with mixed features typically indicate a more serious condition, as well as poor response to treatment, according to the 2017 review mentioned earlier.
No single medication is indicated for use in treating mixed features. Usually, a mental health professional will prescribe a combination of two or more medications, depending on your individual circumstances. Using one antidepressant for therapy isn’t recommended, according to a 2014 review.
Combination therapy for bipolar disorder with mixed states may include:
- atypical antipsychotics (one or more)
- mood stabilizers, including newer anticonvulsants
- electroconvulsive therapy (ECT)
In severe cases where medication is not effective, ECT may be effective very quickly and resolve symptoms.
Atypical antipsychotics can include:
- risperidone
- olanzapine
- quetiapine
- ziprasidone
- asenapine
- lurasidone
- aripiprazole
Mood stabilizers can include:
- lithium
- divalproex sodium
- carbamazepine/oxcarbazepine/eslicarbazepine
- lamotrigine
- topiramate
- gabapentin/pregabalin
While there’s no cure for bipolar disorder with mixed features, there is treatment to help you manage it.
Mixed episodes can be especially serious because of the risk of suicide — the depression is there, as well as the energy to carry it out. That’s why symptom management and supportive treatment are extremely important.
Suicide prevention
If you or someone you know is considering suicide, you’re not alone. Help is available right now:
- Call a crisis hotline, such as the National Suicide Prevention Lifeline at 800-273-8255.
- Not in the U.S.? Find a helpline in your country with Befrienders Worldwide or the International Association for Suicide Prevention.
- Go to the nearest emergency room.
Here are many more resources to help you find assistance.
A mental health professional can help you better manage symptoms and can alter your treatment plan to help stabilize moods and reduce subsequent mood shifts.
If there’s an underlying cause to the mixed features, like medications, your care team can recommend other medication options to help stabilize your moods.
While more research is necessary to determine the underlying causes of mixed states and triggers, there are ways to manage the mixed episodes. If you’re experiencing symptoms of bipolar disorder with mixed features, reach out to a mental health professional.
Bipolar disorder - Official website of the FGBUZ KB No. 85 FMBA of Russia
General brief information
Bipolar disorder, also known as bipolar affective disorder (BAD) and formerly as manic-depressive psychosis (PMD). It is a set of mood disorders characterized by marked fluctuations in mood, thinking, behaviour, energy and ability to perform daily activities.
A person suffering from this disorder alternates his state of mind between mania or hypomania - a phase of joy, exaltation, euphoria and grandiosity and depression, with sadness, inhibition and ideas of death.
Four types of bipolar disorder were defined by severity and alternation of moods over time:
- Bipolar I disorder
- Bipolar disorder type II
- Cyclothymia
- Non-specific bipolar disorder
Because bipolar disorder occurs in young people, it has a high social cost. It is the second leading cause of disability worldwide. In addition, those who suffer from it pose a higher risk than the general population of deaths from suicide, homicide, accidents, and natural causes such as cardiovascular disease.
In addition, those who suffer from it pose a higher risk than the general population of deaths from suicide, homicide, accidents, and natural causes such as cardiovascular disease.
In type 1, the person alternates between depressive episodes with full manic episodes, and in type 2, he alternates between depressive episodes and hypomanic (less severe) episodes.
The symptoms of this disorder are severe, different from the normal highs and lows of mood. These symptoms can lead to relationship problems, work, school, or even suicide.
During the depression phase a person may experience:
- Negative perception of life.
- Inability to feel the pleasure of life.
- No energy
- Self-criticism.
- In extreme cases, suicide.
During a manic phase a person may experience:
- Denial that there is a problem.
- Sudden change of mood.
- Irrational financial decisions.
- Feeling of great enthusiasm
- Don't think about the consequences of your actions.
- Lack of sleep
Although childhood onset occurs, the normal age of onset for type 1 is 18 years and for type 2 is 22 years.
About 10% of bipolar 2 cases develop into type 1.
Although the causes are unclear, genetic and environmental factors (stress, childhood abuse) play a role.
Treatment usually includes psychotherapy, medication, sometimes electroconvulsive therapy may be helpful.
Symptoms
Signs and symptoms of the depressive phase of bipolar disorder include:
- Persistent sadness
- Lack of interest in engaging in pleasurable activities.
- Apathy or indifference.
- Anxiety or social anxiety.
- Chronic pain or irritability.
- Lack of motivation
- Guilt, hopelessness, social isolation.
- Lack of sleep or appetite.
- Suicidal thoughts
- In extreme cases, there may be psychotic symptoms: delusions or hallucinations are usually unpleasant.
Manic symptoms
Mania can occur in varying degrees:
Hypomania
This is the least severe degree of mania and lasts at least 4 days. This does not result in a noticeable decrease in a person's ability to work, communicate, or adapt.
He also does not require hospitalization and does not have psychotic characteristics.
In fact, overall functioning may improve during a hypomanic episode and is considered a natural anti-depression mechanism.
If an event of hypomania is not accompanied by or precedes depressive episodes, it is not considered a problem if the state of mind is uncontrollable.
Symptoms may last from several weeks to several months.
It is characterized by:
- Great energy and activity.
- Some people may be more creative, while others may be more irritable.
- A person may feel so good that he denies that he is experiencing a state of hypomania.
Mania
Mania is a period of euphoria and high mood for at least 7 days. If left untreated, a manic episode can last 3 to 6 months.
If left untreated, a manic episode can last 3 to 6 months.
It is characterized by displaying three or more of the following behaviors:
- Talk quickly and smoothly.
- Accelerated thoughts.
- Agitation.
- Light condition.
- Impulsive and risky behavior.
- Excessive cash expenses
- Hypersexuality.
- A person with mania may also experience lack of sleep and inadequate judgment.
- On the other hand, maniacs may have problems with alcohol or other substance abuse.
In extreme cases, they may experience psychosis, so that contact with reality is broken, having a high state of mind.
It is common for a manic person to feel incomparable or indestructible and to feel chosen to realize a goal.
Approximately 50% of people with bipolar disorder experience hallucinations or delusions, which can lead to violent behavior or admission to a psychiatric hospital.
Mixed episodes
In bipolar disorder, a mixed episode is a condition in which mania and depression occur simultaneously.
People who experience this condition may have thoughts of grandiosity while having depressive symptoms such as suicidal thoughts or feelings of guilt.
People who are in this state are at high risk of committing suicide because they confuse depressive emotions with mood swings or difficulty controlling impulsivity.
Causes
The exact causes of bipolar disorder are unclear, although they are thought to be largely genetic and environmental.
Genetic factors
It is believed that 60-70% of the risk of developing bipolarity depends on genetic factors.
Several studies have shown that certain genes and chromosomal regions are associated with susceptibility to develop the disorder, with each gene being more or less important.
The risk of bipolar disorder in people with family members with the same diagnosis is 10 times higher than in the general population.
Studies indicate heterogeneity, meaning that different genes are involved in different families.
Environmental factors
Research shows that environmental factors play an important role in the development of bipolar disorder, and psychosocial variables may interact with genetic dispositions.
Recent life events and interpersonal relationships contribute to manic and depressive episodes.
30-50% of adults diagnosed with bipolar disorder have been found to report abuse or trauma in childhood, which is associated with an earlier onset of the disorder and more suicide attempts.
Evolutionary factors
From evolutionary theory, one might think that the negative effects that bipolar disorder can have on adaptability cause genes not to be selected by natural selection.
However, there is still a high incidence of BD in many populations, so there may be some evolutionary benefit.
Doctors of evolutionary medicine suggest that high rates of BR throughout history suggest that the change between depressive and manic states suggested some evolutionary advantage in ancestral humans.
In highly stressed individuals, depressed mood can serve as a defense strategy to escape external stress, store energy, and increase sleep hours.
Mania could benefit from her relationship with creativity, confidence, high energy levels and greater productivity.
Physiological, neurological and neuroendocrine factors
Brain imaging studies have shown differences in the volume of various brain areas between patients with bipolar disorder and healthy patients.
An increase in the volume of the lateral ventricles and an increase in the rate of white matter hyperintensity were found.
Magnetic resonance studies have shown that there is an abnormal modulation between the abdominal prefrontal region and the limbic regions, especially the amygdala. This will contribute to poor emotional regulation and mood-related symptoms.
On the other hand, there is evidence of an association between early stressful experiences and dysfunction of the hypothalamic-pituitary-adrenal axis, leading to hyperactivation.
Less common bipolar disorder can result from trauma or a neurological condition: brain injury, stroke, HIV, multiple sclerosis, porphyria, and temporal lobe epilepsy.
The neurotransmitter responsible for regulating mood, dopamine, has been found to increase its transmission during the manic phase and decrease during the depressive phase.
Glutamate increases in the left dorsolateral prefrontal cortex during the manic phase.
Diagnosis
A patient must have at least two episodes of affective disorder to be diagnosed with bipolar disorder. At the same time, at least one of them must be either manic or mixed. For the correct diagnosis, the psychiatrist must take into account the characteristics of the patient's history, information received from his relatives. Currently, it is believed that the symptoms of bipolar disorder are characteristic of 1% of people, and in 30% of them the disease becomes a severe psychotic form. Determination of the severity of depression is carried out using special scales. The manic phase of bipolar disorder must be differentiated from arousal caused by the use of psychoactive substances, lack of sleep, or other causes, and the depressive phase from psychogenic depression. Psychopathy, neurosis, schizophrenia, as well as affective disorders and other psychoses due to somatic or nervous diseases should be excluded.
The manic phase of bipolar disorder must be differentiated from arousal caused by the use of psychoactive substances, lack of sleep, or other causes, and the depressive phase from psychogenic depression. Psychopathy, neurosis, schizophrenia, as well as affective disorders and other psychoses due to somatic or nervous diseases should be excluded.
Methods of treatment
The main goal of the treatment of bipolar disorder is to normalize the mental state and mood of the patient, to achieve long-term remission. In severe cases of the disease, patients are hospitalized in the psychiatric department. Mild forms of the disorder can be treated on an outpatient basis. Antidepressants are used to relieve a depressive episode. The choice of a specific drug, its dosage and frequency of administration in each case is determined by a psychiatrist, taking into account the age of the patient, the severity of depression, and the possibility of its transition to mania. If necessary, the appointment of antidepressants is supplemented with mood stabilizers or antipsychotics. Antidepressants help to stop depressive states in bipolar disorder. Drug treatment of bipolar disorder in the stage of mania is carried out by normotimics, and in severe cases of the disease, antipsychotics are additionally prescribed. In the stage of remission, psychotherapy (group, family and individual) is shown.
Antidepressants help to stop depressive states in bipolar disorder. Drug treatment of bipolar disorder in the stage of mania is carried out by normotimics, and in severe cases of the disease, antipsychotics are additionally prescribed. In the stage of remission, psychotherapy (group, family and individual) is shown.
The evolution of the concept of mixed states in the clinic of bipolar affective disorder
Mixed states are a controversial area of psychopathology. Along with mania and depression, they act as an independent phase of manic-depressive disorder [47], forming a family of separate forms of affective syndromes. Characterized by the introduction of depressive features into mania/hypomania or, conversely, manic into depression, mixed states are often not recognized by clinicians due to the polymorphism of symptoms and the lack of adequate diagnostic criteria.
The history of the concept of mixed states had four stages: the stage of creating the Kraepelinian concept of mixed states, which generalized all earlier indications of their existence; relative oblivion of the concept of mixed states; introduction into practice of their criteria within the framework of modern classifications of mental disorders; scientific search for new diagnostic criteria. For a deeper understanding of the essence of mixed states, one should consider each of them in more detail, prefixing them with a description of the stage of prototypes of mixed states.
For a deeper understanding of the essence of mixed states, one should consider each of them in more detail, prefixing them with a description of the stage of prototypes of mixed states.
Mixed states prototype stage. As pointed out by A. Koukopoulos and A. Koukopoulos [54], the first mention of conditions that could essentially be called mixed are found in Lorry, Boissier de Sauvages and Cullen in descriptions of individual variants of melancholia ( melancholia moria, melancholia enthusiastica and etc.).
In the classification of mental disorders proposed by J. Heinroth [51], states of exaltation and excitation (hyperthymia), depressed states (asthenia), mixed states of excitation and weakness (hypoasthenia) were distinguished. The last diagnostic category included "mixed emotional disorders" ( animi morbi complicati ), "mixed mental disorders" ( morbi mentis mixti ) and "mixed impulse disorders" ( morbi voluntatis mixti, athymia ). The first two groups correspond to modern definitions of mixed affective and schizoaffective disorders. The French psychiatrist J. Guislain [49] classified “grumpy depression”, “grumpy exaltation”, “depression with exaltation and recklessness”, and “depression with anxiety” as mixed states, while noting the long duration of episodes characteristic of the first type and an unfavorable prognosis. . In his opinion, "gloomy insanity precedes frenzy", and the transition from one state to another can be accomplished through numerous steps, representing a "mixture of mental disorders" in various combinations. Similar descriptions can be found in J. Baillarger [25]. F. Richarz [72] used the term " melancholia agitans ". W. Griesinger [48] noted that depressive ideas and ideas of grandeur "do not necessarily exclude" each other, but can be observed simultaneously during the transition from one state to another, representing a "conglomerate of manic and depressive symptoms." The same opinion was shared by J.
The first two groups correspond to modern definitions of mixed affective and schizoaffective disorders. The French psychiatrist J. Guislain [49] classified “grumpy depression”, “grumpy exaltation”, “depression with exaltation and recklessness”, and “depression with anxiety” as mixed states, while noting the long duration of episodes characteristic of the first type and an unfavorable prognosis. . In his opinion, "gloomy insanity precedes frenzy", and the transition from one state to another can be accomplished through numerous steps, representing a "mixture of mental disorders" in various combinations. Similar descriptions can be found in J. Baillarger [25]. F. Richarz [72] used the term " melancholia agitans ". W. Griesinger [48] noted that depressive ideas and ideas of grandeur "do not necessarily exclude" each other, but can be observed simultaneously during the transition from one state to another, representing a "conglomerate of manic and depressive symptoms." The same opinion was shared by J. Falret [42], describing the period of “transition from excitation to depression” with the onset of a hard-to-characterize state formed by weakened excitation and beginning depression. Studying circular psychosis, R. Kraft-Ebing [57] singled out the phase of “indefinite symptoms, when excitement follows depression and vice versa”: in the transitional period, these states “merge” and one can observe the phenomenon when “temporary symptoms” appear in a depressive or manic picture. opposite state." In the group of "combined" psychoses, C. Wernicke [86] described "agitated melancholia" with characteristic features: intense anxiety, speech pressure and a jump in ideas. According to him, "agitated melancholy" combined elements of depression and melancholy.
Falret [42], describing the period of “transition from excitation to depression” with the onset of a hard-to-characterize state formed by weakened excitation and beginning depression. Studying circular psychosis, R. Kraft-Ebing [57] singled out the phase of “indefinite symptoms, when excitement follows depression and vice versa”: in the transitional period, these states “merge” and one can observe the phenomenon when “temporary symptoms” appear in a depressive or manic picture. opposite state." In the group of "combined" psychoses, C. Wernicke [86] described "agitated melancholia" with characteristic features: intense anxiety, speech pressure and a jump in ideas. According to him, "agitated melancholy" combined elements of depression and melancholy.
Thus, already in the 19th century, most well-known psychiatrists noted the existence of mixed states, denoting in their first prototypical descriptions fundamentally different positions, considering these states as an independent form or as a stage of transition between opposite affective phases.
The period of conceptualization of mixed states. By the beginning of the 20th century, numerous indications of the existence of mixed states needed to be generalized and were conceptualized by E. Kraepelin and his student W. Weygandt [87]. The latter, working under the guidance of E. Kraepelin in the psychiatric clinic of the University of Hedelberg, drew attention to the frequency of the simultaneous appearance of symptoms of different poles of manic-depressive psychosis (in 20% of the “circular” patients he observed). In his first monograph on mixed states in psychiatric literature - "On mixed states in manic-depressive insanity" ("Uber die Mischzustande des Manisch-depressiven Irreseins") - he outlined the fundamental approaches to their diagnosis - a different combination of opposite manic and depressive symptoms from triads: elated mood, psychomotor agitation and a jump in ideas, on the one hand, and low mood, psychomotor and ideator retardation, on the other. According to the author, instability of mood, motility and thinking is a characteristic feature of manic-depressive (circular) psychosis. He also noted that in some cases, mixed symptoms determine the clinical picture of the entire episode, contributing to a more protracted course (weeks, months, and even years) than in pure manic or depressive states. W. Weygandt believed that with various combinations of symptoms of the manic and depressive triad, at least six variants of mixed states can occur for a short time. Avoiding speculativeness, he attached practical importance to only three of their types, which are more common in clinical practice and have the longest duration - "manic stupor", "agitated depression" and "unproductive mania".
According to the author, instability of mood, motility and thinking is a characteristic feature of manic-depressive (circular) psychosis. He also noted that in some cases, mixed symptoms determine the clinical picture of the entire episode, contributing to a more protracted course (weeks, months, and even years) than in pure manic or depressive states. W. Weygandt believed that with various combinations of symptoms of the manic and depressive triad, at least six variants of mixed states can occur for a short time. Avoiding speculativeness, he attached practical importance to only three of their types, which are more common in clinical practice and have the longest duration - "manic stupor", "agitated depression" and "unproductive mania".
According to P. Salvatore [75], the works of W. Weygandt were a powerful impetus to the creation of Kraepelin's concept of manic-depressive psychosis, which was finally published in the 8th edition of his manual [55]. In this work, E. Kraepelin developed the concept of mixed states (Mischzustande) with a circular form of periodic insanity, pointing to the “internal relationship of seemingly opposite states”, in which there is a multidirectionality of the three components of an affective state - thinking, motor activity and mood itself. Singling out six mixed states (see table) , he believed that depressive or anxious mania (depressive oder ängsliche Manie), excited depression (erregte Depression), mania with scarcity of thoughts (ideenarme Manie) are based on three fundamental symptoms of mania (high euphoric mood, jump ideas, hyperactivity), while manic stupor (manischer Stupor), depression with a flight of thoughts (ideenfluchtige Depression), inhibited mania (gehemmte Manie) - on the fundamental symptomatology of depression ("ideational weakness", "depressed mood", "decreased motivation "). Analyzing the stereotype of the development of mixed states, E. Kraepelin singled out the transient form as a stage of transition from depression to mania or vice versa and an independent form characterized by a tendency to a protracted course.
Singling out six mixed states (see table) , he believed that depressive or anxious mania (depressive oder ängsliche Manie), excited depression (erregte Depression), mania with scarcity of thoughts (ideenarme Manie) are based on three fundamental symptoms of mania (high euphoric mood, jump ideas, hyperactivity), while manic stupor (manischer Stupor), depression with a flight of thoughts (ideenfluchtige Depression), inhibited mania (gehemmte Manie) - on the fundamental symptomatology of depression ("ideational weakness", "depressed mood", "decreased motivation "). Analyzing the stereotype of the development of mixed states, E. Kraepelin singled out the transient form as a stage of transition from depression to mania or vice versa and an independent form characterized by a tendency to a protracted course.
E. Kraepelin's concept had many supporters.
E. Bleuler [36] emphasized the importance of "such a quality of manic-depressive psychosis as confusion", reflecting, in his opinion, the possibility of a diverse combination of symptoms. K. Leonhard [59] believed that the allocation of mixed states indicates the potential properties of manic-depressive psychosis "to involve the characteristics of the opposite affective pole." However, other opinions were also expressed.
K. Leonhard [59] believed that the allocation of mixed states indicates the potential properties of manic-depressive psychosis "to involve the characteristics of the opposite affective pole." However, other opinions were also expressed.
In particular, K. Jaspers [52] and K. Schneider [77], questioning the independent significance of mixed states, considered it unlawful to “break” manic-depressive disorders into affective, intellectual and cognitive components. In their opinion, mixed states are nothing more than a change from a manic state to a depressive state and vice versa.
In parallel with E. Kraepelin, other researchers also worked on the issue of mixed states. O. Rehm [71], using the term "mixed affect" and separating "speech" and "general motor skills" from the psychomotor component of the affective state, proposed a more complex typification of mixed states. A different classification principle was proposed by E. Stransky [81], who divided mixed states depending on the nature of the predominant affect (manic and depressive types of mixed states), as well as taking into account the mechanisms of their formation (simultaneous and successive variants). At the same time, simultaneous mixed states were characterized by the simultaneous coexistence of individual signs of an affect of different polarity, and successive ones were characterized by a successive change of individual components of different polarity in the structure of one phase.
At the same time, simultaneous mixed states were characterized by the simultaneous coexistence of individual signs of an affect of different polarity, and successive ones were characterized by a successive change of individual components of different polarity in the structure of one phase.
In domestic psychiatry of the beginning of the 20th century, works devoted to mixed states are relatively few in number. Mixed states were mentioned by P.B. Gannushkin, S.A. Sukhanov [3], V.P. Serbian [11, 12], A.N. Bernstein [1], Yu.V. Kannabih [6], E.S. Lokshin [8]. A particularly detailed study of mixed states was carried out by S.A. Sukhanov [13]. The author noted that mixed states appear at more distant stages of the disease as a "further evolution of manic-depressive psychosis" after the stage of alternation of typical manic and depressive phases.
The middle of the 20th century became a period of relative oblivion for mixed states . Nevertheless, in a few publications of foreign psychiatrists (K. Kleist [56], G. Ewald [41], J. Rouart [74], M. Fischetti [44], J. Lange [58], J. Campbell [37] ) you can find indications of the importance of identifying mixed conditions, which, combining the symptoms of different affective poles, thereby reflect the commonality of a single cyclothymic process with the possibility of developing any of these forms in a particular patient.
Kleist [56], G. Ewald [41], J. Rouart [74], M. Fischetti [44], J. Lange [58], J. Campbell [37] ) you can find indications of the importance of identifying mixed conditions, which, combining the symptoms of different affective poles, thereby reflect the commonality of a single cyclothymic process with the possibility of developing any of these forms in a particular patient.
During this period, in domestic psychiatry, with some delay, active disputes continued about the validity of E. Kraepelin's ideas in relation to these conditions. One of the followers of the Kraepelinian model of mixed states in the Russian psychiatric school, V.A. Gilyarovsky [4] pointed out that "in addition to pure states of excitation or depression, mixed patterns are observed, characterized by a longer course and an unfavorable prognosis." The author believed that out of nine theoretically possible combinations of excitation and oppression in three areas of mental activity (emotional, intellectual and volitional), the real value among mixed states with an emphasis on the manic component is angry mania, with an emphasis on the depressive - agitated melancholia. Opposite views were expressed by V.M. Bekhterev [2], pointing out the inconclusive evidence for the existence of mixed or transient manic-melancholic states.
Opposite views were expressed by V.M. Bekhterev [2], pointing out the inconclusive evidence for the existence of mixed or transient manic-melancholic states.
The stage of introduction of criteria within the framework of modern classifications of mental disorders. Subsequently, in the wake of the consequences of the psychopharmacological "revolution" in the works of a number of researchers [22, 68, 88], a revival of interest in mixed states began, which was characterized by two features: on the one hand, confirmation of the previously formulated provisions regarding this concept, on the other hand, dissatisfaction with the accumulated by that time, ideas about the structure of mixed states as a simple combination of polar symptoms. Deepening knowledge about the dependence of the psychopathological structure of mixed affective syndromes on syndromokinesis, S. Mentzos [66] proposed to distinguish between stable and unstable mixed states. The clinical picture of stable mixed states is represented by a synchronous combination of symptoms of depression and mania and is characterized by the replacement of one or more elements of mania (hypomania) by signs of depression and vice versa (for example, agitation in depression or lethargy in a manic state). So, during the period of the greatest severity of affective disorders, anxiety can be accompanied by motor restlessness (patients are tense, cannot find a place for themselves, can neither sit nor lie down) and speech excitation with groans, lamentations, anxious verbigeration - repeated monotonous repetition of monotonous short phrases and expressions ( agitated depression). Unstable mixed states are formed during the rapid change of polar affective phases within the "short cycle". At the same time, depressive and manic manifestations overlap in various, sometimes very chaotic combinations. Their psychopathological structure, in contrast to "pure" depression and hypomania, is determined by a large polymorphism; the variety of manifestations is associated both with the formation of general symptoms (irritability, anxiety, ideomotor restlessness, internal tension, impaired concentration, insomnia), and the addition of psychopathological disorders of other registers (obsessive-compulsive, panic attacks, depersonalization).
So, during the period of the greatest severity of affective disorders, anxiety can be accompanied by motor restlessness (patients are tense, cannot find a place for themselves, can neither sit nor lie down) and speech excitation with groans, lamentations, anxious verbigeration - repeated monotonous repetition of monotonous short phrases and expressions ( agitated depression). Unstable mixed states are formed during the rapid change of polar affective phases within the "short cycle". At the same time, depressive and manic manifestations overlap in various, sometimes very chaotic combinations. Their psychopathological structure, in contrast to "pure" depression and hypomania, is determined by a large polymorphism; the variety of manifestations is associated both with the formation of general symptoms (irritability, anxiety, ideomotor restlessness, internal tension, impaired concentration, insomnia), and the addition of psychopathological disorders of other registers (obsessive-compulsive, panic attacks, depersonalization). Such unstable mixed states were described in the domestic literature [7] under the term “atypical”, often associated with the consequences of the use of antidepressants.
Such unstable mixed states were described in the domestic literature [7] under the term “atypical”, often associated with the consequences of the use of antidepressants.
T.F. put another meaning into the term "atypical mixed states". Papadopoulos [10]. Noting the relative clarity in terms of the psychopathological structure of the periods of "mixed affect" during the transition from one phase to another, he singled out true mixed states that require special analysis within the atypical phases of not only circular, but also affective psychoses in a broader sense. The author suggested considering the "atypia" of individual phases of manic-depressive psychosis, taking into account the premorbid personality and age of patients.
Yu.L. Nuller and I.N. Mikhalenko [9] to the assumption that the typology of mixed states proposed by E. Kraepelin is limited.
Uniformity in the diagnosis of mixed states began with the creation in the 80s of unified criteria for assessing mental disorders - Research Diagnostic Criteria (RDC) [78, 79] and the DSM-III-R classification [20].
In the RDC, two variants of mixed states were distinguished: when depressive and manic syndromes were presented simultaneously during one episode and when they followed one after the other without interruption. RDC criteria were partly incorporated into the DSM-III-R classification, which provided a rather vague description of the category "bipolar disorder - mixed". Its diagnosis required the presence of a complete symptomatological picture of a manic and major depressive episode, coexisting simultaneously or rapidly replacing each other every few days. At the same time, depressive symptoms had to be sufficiently pronounced and persist at least throughout the day. The advent of the DSM-III-R did not add clarity to the diagnosis of mixed conditions. As noted by G. Perugi et al. [69], such criteria ruled out the possibility of the presence of individual competing symptoms of opposite polarity, which led to an underdiagnosis of mixed conditions.
A more specific definition of a "mixed episode" was given in DSM-IV [21].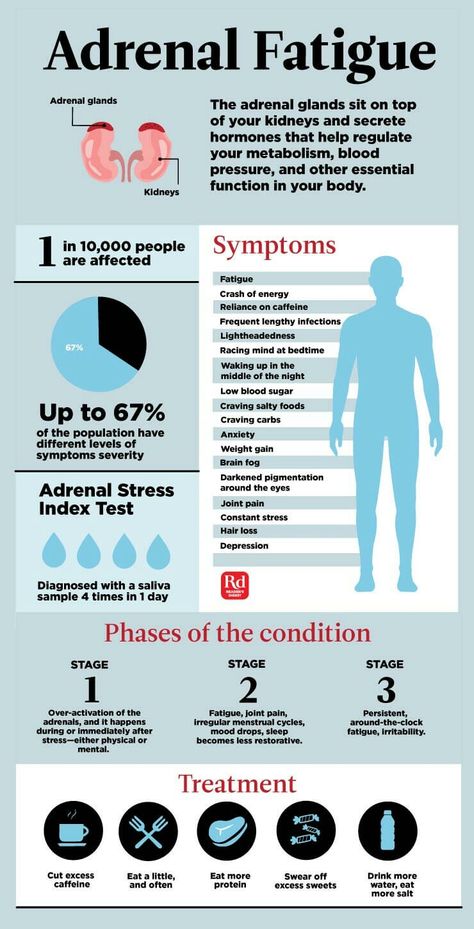 Its diagnosis required meeting the criteria for both manic and major depressive episodes almost every day for at least 1 week. Thus, the category of mixed episodes did not include unstable forms characterized by a successive change of manic and depressive symptoms, which were classified under the heading specifier “rapid cyclicity”.
Its diagnosis required meeting the criteria for both manic and major depressive episodes almost every day for at least 1 week. Thus, the category of mixed episodes did not include unstable forms characterized by a successive change of manic and depressive symptoms, which were classified under the heading specifier “rapid cyclicity”.
In this regard, the criteria of the modern American classification correspond only to stable forms of mixed conditions.
The DSM-IV criteria for mixed states have also been criticized as narrow, restrictive, and inconsistent with clinical reality [17, 26, 65, 69, 83], primarily due to the high prevalence of non-syndromic symptoms of the opposite polarity. Thus, F. Benazzi [27] cites data that the formation of complete syndromic hypomania in patients with a major depressive episode was observed in 2.8% of cases, while in the presence of individual hypomanic symptoms - in 28.5%.
In accordance with the results of the study by F. Benazzi, H. Akiskal [29], 48.7% of patients with major depression as part of bipolar affective disorder type II (BAD II) had three or more competing hypomanic symptoms coexisting.
Benazzi, H. Akiskal [29], 48.7% of patients with major depression as part of bipolar affective disorder type II (BAD II) had three or more competing hypomanic symptoms coexisting.
The ICD-10 [89] defines a mixed episode as “an affective episode lasting at least 2 weeks and characterized by either a mixture or a rapid alternation (often within hours) of hypomanic, manic and depressive symptoms.” Both sets of symptoms must be "significantly pronounced during most of the current episode of the disease." It further clarifies that "depressive mood is often accompanied for days or weeks by hyperactivity and the pressure of speech, and a manic state with grandiosity - agitation and loss of energy and libido." Thus, the ICD-10, compared to DSM-IV, offers less restrictive criteria for mixed states, requiring only "pronounced" manic or hypomanic and depressive symptoms, but not full syndromes, and explicitly embraces ultradian cyclicity. Moreover, unlike the DSM-IV, the description of the ICD-10 recognizes the existence of mixed depression and mania.
Search for new diagnostic criteria. In recent decades, the concept of mixed states has received increasing attention in light of the increasing interest in the problem of bipolar disorders (especially type II). Research is directed, on the one hand, to the search for new, more realistic diagnostic criteria, and, on the other hand, to clarify the phenomenology of mixed states.
During the search for new diagnostic criteria for a mixed state, evidence has been accumulated for the sufficiency of verification of several competing contrapolar symptoms for the diagnosis of subsyndromal depression in the structure of syndromic mania [63, 69] or subsyndromal mania in the structure of syndromic depression [15, 53, 69]. At the same time, the discussions concerned the question of the number of these contrapolar symptoms that are optimally sufficient for the diagnosis of a mixed state: S. McElroy et al. [63] proposed in this vein to consider more than three depressive symptoms in the structure of mania, H. Akiskal et al. [17] - more than two, and A. Swann et al. [83] - more than one, which predetermined the expansion of the concept of mixed states.
Akiskal et al. [17] - more than two, and A. Swann et al. [83] - more than one, which predetermined the expansion of the concept of mixed states.
Alternative criteria of mixed states proposed at that time (three of the best known - Cincinnati [63], Vienna [32-34], Pisan [69]) were not sufficiently valid and did not provide the same diagnostic accuracy when compared with each other and with DSM-IV-TR and ICD-10 diagnostic criteria [50]. Thus, mixed mania, detected by clinical assessment in 23.2% of patients with BAD I, could be diagnosed using Cincinnati criteria in 16.7% of cases, and DSM-IV-TR and ICD-10 criteria - only in 12.9 and 9% of cases, respectively [85].
H. Akiskal [14-16, 18] expanded the interpretation of mixed states by including signs that appear as part of the manifestation of an affective episode based on temperament of the opposite polarity (hyperthymic, depressive, cyclothymic, irritable and anxious).
The concept of the bipolar spectrum, which has numerous supporters, also has a certain influence on the formation of new views on mixed states.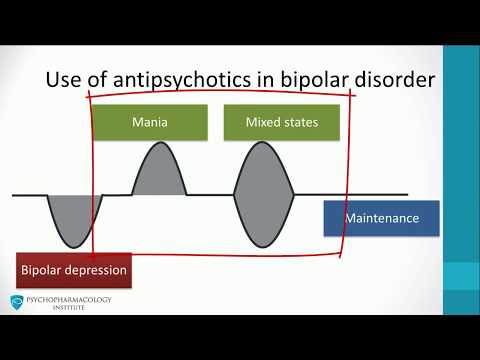 S. McElroy [65], considering mixed bipolar episodes in relation to their belonging to the bipolar spectrum, indicates the possibility of countless variants of combinations of different severity of manic and depressive symptoms. In its extreme form, the dimensional approach was presented by A. Swann et al. [82], who proposed to consider mixed states in the form of a continuum of various combinations of manic and depressive manifestations, including not only Kraepelinian subtypes, but also many of their transitional forms.
S. McElroy [65], considering mixed bipolar episodes in relation to their belonging to the bipolar spectrum, indicates the possibility of countless variants of combinations of different severity of manic and depressive symptoms. In its extreme form, the dimensional approach was presented by A. Swann et al. [82], who proposed to consider mixed states in the form of a continuum of various combinations of manic and depressive manifestations, including not only Kraepelinian subtypes, but also many of their transitional forms.
Recent research is moving away from categorical positions towards a dimensional study of the individual symptoms of mania and depression involved in the formation of mixed states in order to identify underlying symptomatic clusters that determine response to therapy and prognosis.
The need to develop a modern phenomenology of mixed states forced researchers to turn again to the Kraepelin typology when describing the most common variants of mixed states - dysphoric mania [49, 63, 70] and agitated depression [15, 30, 31, 53, 61]. F. Cassidy [38] and T. Sato [76] confirm the validity of the subtype of mania with severe symptoms of dysphoria, corresponding to Kraepelin's "anxiety-depressive mania". N. Akiskal and F. Benazzi [19], considering mixed depression as a combination of a complete depressive syndrome and three competing hypomanic symptoms, also indicate the existence of two subtypes corresponding to Kraepelin's "depression with a leap of ideas" and "agitated depression".
F. Cassidy [38] and T. Sato [76] confirm the validity of the subtype of mania with severe symptoms of dysphoria, corresponding to Kraepelin's "anxiety-depressive mania". N. Akiskal and F. Benazzi [19], considering mixed depression as a combination of a complete depressive syndrome and three competing hypomanic symptoms, also indicate the existence of two subtypes corresponding to Kraepelin's "depression with a leap of ideas" and "agitated depression".
To the most common manic symptoms in the structure of a depressive episode in BAD I and II J. Goldberg et al. [46] refer to distractibility, ideational acceleration, agitation, and C. Pae et al. [67] - jump of ideas, increased distractibility, irritability, of which the latter, according to the authors, seems to be the main predictor of response to antipsychotic therapy. Symptoms of anxiety and dysphoria, which are related to the nuclear symptoms of mixed mania [35, 40], are attracting more and more attention from researchers. At the same time, dysphoria is considered as a special component of the affective syndrome, which correlates with irritability, increased sensitivity to external physical influences, impulsivity, and a sense of internal tension. F. Cassidy [40], based on the results of a factor analysis of a large sample of bipolar patients with mania, indicates that anxiety is an extremely common symptom of states corresponding to Kraepelin's "anxiety-depressive mania", and proposes to include it in the criteria for mixed states. A comparable level of anxiety in a comparative study of agitated depression and mixed mania by A. Swann [82] also confirms its inherent belonging to a mixed bipolar phenomenology.
At the same time, dysphoria is considered as a special component of the affective syndrome, which correlates with irritability, increased sensitivity to external physical influences, impulsivity, and a sense of internal tension. F. Cassidy [40], based on the results of a factor analysis of a large sample of bipolar patients with mania, indicates that anxiety is an extremely common symptom of states corresponding to Kraepelin's "anxiety-depressive mania", and proposes to include it in the criteria for mixed states. A comparable level of anxiety in a comparative study of agitated depression and mixed mania by A. Swann [82] also confirms its inherent belonging to a mixed bipolar phenomenology.
Factor analysis of individual symptoms of a mixed state showed that the predominance of manic or depressive symptoms in them already leads to heterogeneity in terms of subsequent dynamics, response to treatment and prognosis. Thus, according to the observations of J. Azorin [24], mixed states with a predominance of depressive symptoms are characterized by a lower probability of relapses compared with mixed states with a predominance of manic symptoms; the former often turn into depression, the latter into mania.
Further prospects. The proposed DSM-V classification criteria published to date demonstrate the intention of its developers to bring the controversies of recent years to a common denominator and continue the clearly emerging trend towards expanding the criteria for mixed conditions by reducing the number of symptoms of the opposite affect, sufficient for its diagnosis. Presumably, the DSM-V will be different from the DSM-IV: the category "mixed episode" will disappear altogether and instead the specifier "with mixed features" will be introduced, applicable to the diagnosis of both depression and mania in case at least three symptoms are present. opposite polarity. The latter comes from the already mentioned data confirming that distinct differences between "pure" and "mixed" mania/hypomania or major depression appear when the number of contrapolar symptoms reaches at least three (cited in [84]). The list of counterpolar symptoms will be excluded from those occurring in both mania and depression: psychomotor agitation, irritability, insomnia (to be distinguished from a decrease in the need for sleep), increased distractibility and loss of appetite.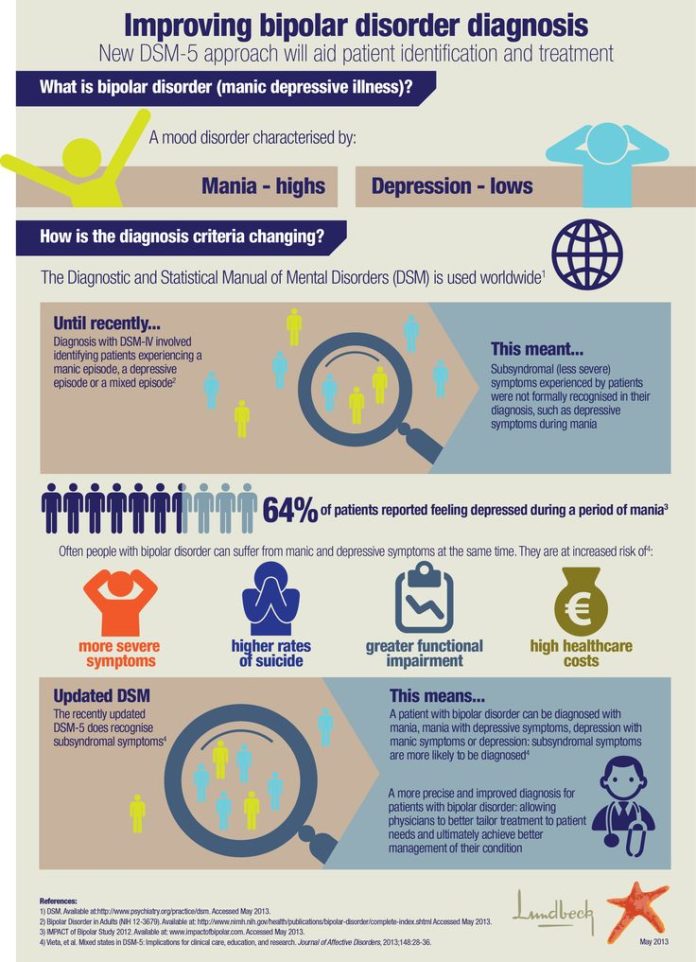
Thus, the proposed definition of mania/hypomania "with features of confusion" in the DSM-V requires that the criteria for a manic or hypomanic episode be fully met and that at least three of the following symptoms be present almost every day during the episode: severe dysphoria or depressed mood, decreased interest or pleasure in almost all activities, psychomotor retardation, fatigue or loss of energy, feelings of inadequacy and excessive or unjustified guilt, recurring thoughts of death or a suicide attempt or suicide planning. The proposed definition of a major depressive episode "with features of confusion" requires meeting the criteria for a major depressive episode and the presence of at least three of the following symptoms observed almost every day during the episode: high or expansive mood, high self-esteem, or grandiosity, unusual talkativeness, or verbal rush, racing of ideas, or subjective feeling of speeding up thoughts, increased energy, purposeful activity, involvement in activities with a high risk of unpleasant consequences, reduced need for sleep.
In addition, the use of the specifier “with mixed traits” for manic, hypomanic and depressive episodes would mean that mixed states are included not only in the circle of BAD I and II, but also in the depressive episode. Thus, the application of this criterion will mean that the diagnosis of major depression "with features of confusion" will not indicate the phenomena of bipolarity. Thus, a patient with three typical manic competing symptoms (eg, high spirits, high self-esteem or grandiosity, excessive involvement in activities with a high risk of adverse consequences) in the structure of a major depressive episode can be classified as unipolar.
The definition of mania/hypomania “with features of confusion” is consistent with available research data and operational criteria reported earlier in the literature [65] and is not likely to change. On the contrary, the definition of major depression "with features of mixed depression" is likely to be debatable, since it includes typical manic symptoms, such as elation and grandiosity, which are rare in patients with mixed depressions, while among the excluded symptoms are those often observed in them. - irritability, psychomotor agitation and distractibility [46, 60]. It is important to note that the putative criteria for the "mixed-feature" specifier in DSM-V, like the criteria for "mixed episode" in DSM-IV, do not include ultradian cyclicity, which may be the subject of further research.
- irritability, psychomotor agitation and distractibility [46, 60]. It is important to note that the putative criteria for the "mixed-feature" specifier in DSM-V, like the criteria for "mixed episode" in DSM-IV, do not include ultradian cyclicity, which may be the subject of further research.
As for the forthcoming edition of ICD-11, the same difficulties may arise before its creators. If the data on insufficient effectiveness and an increased risk of affect reversal against the background of the use of antidepressants in mixed depression are not generally recognized as sufficiently convincing [43], then all researchers emphasize a higher suicidal risk among patients with mixed states [45, 73, 80]. Moreover, mixed states belong to those clarifying diagnostic categories that significantly affect the choice of therapeutic tactics, requiring the use of specific approaches.
From the point of view of the practical orientation of modern classifications, all this justifies the need to use new criteria for the diagnosis of mixed conditions.