Mild intellectual disability iq
Mild, Moderate, Severe Intellectual Disability Differences
Samantha Gluck
Experts divide the types of cognitive impairment into four categories: mild intellectual disability, moderate intellectual disability, severe intellectual disability, and profound intellectual disability. The degree of impairment from an intellectual disability varies widely. DSM-V places less emphasis on the degree of impairment (i.e. IQ scores) and more on the amount and type of intervention needed.
While IQ scores are still relevant and important in assessing the level of intellectual disability, the new DSM-V adds another layer of diagnostic criteria (Intellectual Disability: Causes and Characteristics). Mental health professionals must consider the person's ability or impairment across three skill areas: conceptual, social, and practical life skill.
The category details are as follows:
Mild intellectual disability
- IQ 50 to 70
- Slower than typical in all developmental areas
- No unusual physical characteristics
- Able to learn practical life skills
- Attains reading and math skills up to grade levels 3 to 6
- Able to blend in socially
- Functions in daily life
About 85 percent of people with intellectual disabilities fall into the mild category and many even achieve academic success. A person who can read, but has difficulty comprehending what he or she reads represents one example of someone with mild intellectual disability.
Moderate intellectual disability
- IQ 35 to 49
- Noticeable developmental delays (i.e. speech, motor skills)
- May have physical signs of impairment (i.e. thick tongue)
- Can communicate in basic, simple ways
- Able to learn basic health and safety skills
- Can complete self-care activities
- Can travel alone to nearby, familiar places
People with moderate intellectual disability have fair communication skills, but cannot typically communicate on complex levels. They may have difficulty in social situations and problems with social cues and judgment. These people can care for themselves, but might need more instruction and support than the typical person. Many can live in independent situations, but some still need the support of a group home. About 10 percent of those with intellectual disabilities fall into the moderate category.
Severe intellectual disability
- IQ 20 to 34
- Considerable delays in development
- Understands speech, but little ability to communicate
- Able to learn daily routines
- May learn very simple self-care
- Needs direct supervision in social situations
Only about 3 or 4 percent of those diagnosed with intellectual disability fall into the severe category. These people can only communicate on the most basic levels. They cannot perform all self-care activities independently and need daily supervision and support. Most people in this category cannot successfully live an independent life and will need to live in a group home setting.
Profound intellectual disability
- IQ less than 20
- Significant developmental delays in all areas
- Obvious physical and congenital abnormalities
- Requires close supervision
- Requires attendant to help in self-care activities
- May respond to physical and social activities
- Not capable of independent living
People with profound intellectual disability require round-the-clock support and care. They depend on others for all aspects of day-to-day life and have extremely limited communication ability. Frequently, people in this category have other physical limitations as well. About 1 to 2 percent of people with intellectual disabilities fall into this category.
They depend on others for all aspects of day-to-day life and have extremely limited communication ability. Frequently, people in this category have other physical limitations as well. About 1 to 2 percent of people with intellectual disabilities fall into this category.
According to the new DSM-V, though, someone with severe social impairment (so severe they would fall into the moderate category, for example) may be placed in the mild category because they have an IQ of 80 or 85. So the changes in the DSM-V require mental health professionals to assess the level of impairment by weighing the IQ score against the person's ability to perform day-to-day life skills and activities. (Read about the types of intellectual disabilities.)
article references
APA Reference
Gluck, S. (2022, January 10). Mild, Moderate, Severe Intellectual Disability Differences, HealthyPlace. Retrieved on 2023, January 9 from https://www.healthyplace.com/neurodevelopmental-disorders/intellectual-disability/mild-moderate-severe-intellectual-disability-differences
Last Updated: January 16, 2022
Medically reviewed by Harry Croft, MD
More Info
Intellectual Disability: Causes and Characteristics
What is an Intellectual Disability?
Stuttering Treatment: How to Stop Stuttering
Stuttering Causes: Why Do People Stutter?
What is Stuttering aka Childhood-Onset Fluency Disorder?
Treatment for Autism Spectrum Disorder: Therapy, Resources
What are Motor Disorders? Signs, Symptoms, Causes, Treatments
Intellectual Disability: Levels, Causes, and Outlook
Overview
If your child has an intellectual disability (ID), their brain hasn’t developed properly or has been injured in some way. Their brain may also not function within the normal range of both intellectual and adaptive functioning. In the past, medical professionals called this condition “mental retardation.”
Their brain may also not function within the normal range of both intellectual and adaptive functioning. In the past, medical professionals called this condition “mental retardation.”
There are four levels of ID:
- mild
- moderate
- severe
- profound
Sometimes, ID may be classified as:
- “other”
- “unspecified”
ID involves both a low IQ and problems adjusting to everyday life. There may also be learning, speech, social, and physical disabilities.
Severe cases of ID may be diagnosed soon after birth. However, you might not realize your child has a milder form of ID until they fail to meet common developmental goals. Almost all cases of ID are diagnosed by the time a child reaches 18 years of age.
Symptoms of ID will vary based on your child’s level of disability and may include:
- failure to meet intellectual milestones
- sitting, crawling, or walking later than other children
- problems learning to talk or trouble speaking clearly
- memory problems
- inability to understand the consequences of actions
- inability to think logically
- childish behavior inconsistent with the child’s age
- lack of curiosity
- learning difficulties
- IQ below 70
- inability to lead a fully independent life due to challenges communicating, taking care of themselves, or interacting with others
If your child has ID, they may experience some of the following behavioral issues:
- aggression
- dependency
- withdrawal from social activities
- attention-seeking behavior
- depression during adolescent and teen years
- lack of impulse control
- passivity
- tendency toward self-injury
- stubbornness
- low self-esteem
- low tolerance for frustration
- psychotic disorders
- difficulty paying attention
Some people with ID may also have specific physical characteristics. These can include having a short stature or facial abnormalities.
These can include having a short stature or facial abnormalities.
ID is divided into four levels, based on your child’s IQ and degree of social adjustment.
Mild intellectual disability
Some of the symptoms of mild intellectual disability include:
- taking longer to learn to talk, but communicating well once they know how
- being fully independent in self-care when they get older
- having problems with reading and writing
- social immaturity
- increased difficulty with the responsibilities of marriage or parenting
- benefiting from specialized education plans
- having an IQ range of 50 to 69
Moderate intellectual disability
If your child has moderate ID, they may exhibit some of the following symptoms:
- are slow in understanding and using language
- may have some difficulties with communication
- can learn basic reading, writing, and counting skills
- are generally unable to live alone
- can often get around on their own to familiar places
- can take part in various types of social activities
- generally having an IQ range of 35 to 49
Severe intellectual disability
Symptoms of severe ID include:
- noticeable motor impairment
- severe damage to, or abnormal development of, their central nervous system
- generally having an IQ range of 20 to 34
Profound intellectual disability
Symptoms of profound ID include:
- inability to understand or comply with requests or instructions
- possible immobility
- incontinence
- very basic nonverbal communication
- inability to care for their own needs independently
- the need of constant help and supervision
- having an IQ of less than 20
Other intellectual disability
People in this category are often physically impaired, have hearing loss, are nonverbal, or have a physical disability. These factors may prevent your child’s doctor from conducting screening tests.
These factors may prevent your child’s doctor from conducting screening tests.
Unspecified intellectual disability
If your child has an unspecified ID, they will show symptoms of ID, but their doctor doesn’t have enough information to determine their level of disability.
Doctors can’t always identify a specific cause of ID, but causes of ID can include:
- trauma before birth, such as an infection or exposure to alcohol, drugs, or other toxins
- trauma during birth, such as oxygen deprivation or premature delivery
- inherited disorders, such as phenylketonuria (PKU) or Tay-Sachs disease
- chromosome abnormalities, such as Down syndrome
- lead or mercury poisoning
- severe malnutrition or other dietary issues
- severe cases of early childhood illness, such as whooping cough, measles, or meningitis
- brain injury
To be diagnosed with ID, your child must have below-average intellectual and adaptive skills. Your child’s doctor will perform a three-part evaluation that includes:
- interviews with you
- observations of your child
- standard tests
Your child will be given standard intelligence tests, such as the Stanford-Binet Intelligence Test.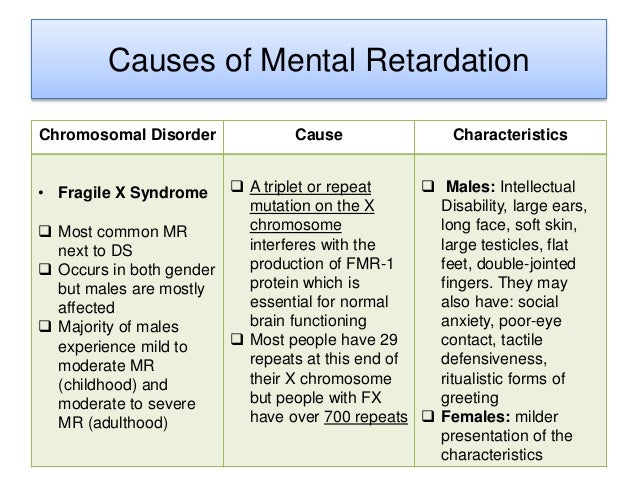 This will help the doctor determine your child’s IQ.
This will help the doctor determine your child’s IQ.
The doctor may also administer other tests such as the Vineland Adaptive Behavior Scales. This test provides an assessment of your child’s daily living skills and social abilities, compared to other children in the same age group.
It’s important to remember that children from different cultures and socioeconomic statuses may perform differently on these tests. To form a diagnosis, your child’s doctor will consider the test results, interviews with you, and observations of your child.
Your child’s evaluation process might include visits to specialists, who may include a:
- psychologist
- speech pathologist
- social worker
- pediatric neurologist
- developmental pediatrician
- physical therapist
Laboratory and imaging tests may also be performed. These can help your child’s doctor detect metabolic and genetic disorders, as well as structural problems with your child’s brain.
Other conditions, such as hearing loss, learning disorders, neurological disorders, and emotional problems can also cause delayed development. Your child’s doctor should rule these conditions out before diagnosing your child with ID.
You, your child’s school, and your doctor will use the results of these tests and evaluations to develop a treatment and education plan for your child.
Your child will probably need ongoing counseling to help them cope with their disability.
You will get a family service plan that describes your child’s needs. The plan will also detail the services that your child will need to help them with normal development. Your family needs will also be addressed in the plan.
When your child is ready to attend school, an Individualized Education Program (IEP) will be put in place to help them with their educational needs. All children with ID benefit from special education.
The federal Individuals with Disabilities Act (IDEA) requires that public schools provide free and appropriate education to children with ID and other developmental disabilities.
The main goal of treatment is to help your child reach their full potential in terms of:
- education
- social skills
- life skills
Treatment may include:
- behavior therapy
- occupational therapy
- counseling
- medication, in some cases
When ID occurs with other serious physical problems, your child may have a below-average life expectancy. However, if your child has mild to moderate ID, they will probably have a fairly normal life expectancy.
When your child grows up, they may be able to work a job that complements their level of ID, live independently, and support themselves.
Support services are available to help adults with ID live independent and fulfilling lives.
MENTAL DISABILITY | Encyclopedia Around the World
Contents of the article- Degrees of mental retardation.
- Clinical forms.
- Reasons.
- Treatment.
- Medications.
- Psychotherapy.

MENTAL retardation, underdevelopment of intelligence or, in a broader sense, the lower part of the spectrum of the distribution of intelligence in a population. Mental retardation is not a separate disease or special condition, but rather a common name for many abnormalities, varying in nature and severity. In practice, for example, when hospitalized in a psychiatric hospital or solving legal problems, a mentally retarded person is considered to be a person who, due to a congenital or early age decrease in intelligence, is not capable of an independent existence and needs outside help. Mental retardation should be distinguished from intellectual disabilities that occur in old age, as well as as a result of mental or neurological diseases. In such cases, the intellect is reduced from the previous higher level, while in mental retardation it never reaches the normal level. The two types of intellectual impairments also differ in the nature of the defect and in the presence or absence of concomitant emotional disorders. It is most difficult to differentiate them in childhood. Mental retardation is sometimes misattributed to children with psychotic disorders. nine0019
It is most difficult to differentiate them in childhood. Mental retardation is sometimes misattributed to children with psychotic disorders. nine0019
To diagnose mental retardation, standardized tests are often used to calculate the so-called. intelligence quotient (IQ). An indicator of mental retardation is considered to be IQ below 70. However, this psychometric criterion must be supplemented with data on the social maturity of children, i.e. about their everyday skills, the ability to act independently, as well as information about mental development, the presence of physical diseases, and the ability to learn. Mentally retarded children usually have impaired speech development as well, making it even more difficult to both learn and assess their intelligence. Data on the prevalence of mental retardation vary widely, but the most thorough studies show that the incidence of this condition in the population is as high as 2%. The inconsistency of the data is due to differences in the criteria (psychometric, social, etc. ), in the choice of the boundaries of normal development and mental retardation, as well as the specifics of the studied regions and other factors. Some severe forms of mental retardation are associated with reduced life expectancy, so screening of children usually reveals a higher prevalence of mental retardation than screening of adults. nine0019
), in the choice of the boundaries of normal development and mental retardation, as well as the specifics of the studied regions and other factors. Some severe forms of mental retardation are associated with reduced life expectancy, so screening of children usually reveals a higher prevalence of mental retardation than screening of adults. nine0019
Degrees of mental retardation.
In the general population there are individuals with different levels of intelligence, from low to high, and there is no clear natural boundary between normal and low intelligence. Borderline cases, when IQ ranges from 65 to 85, depending on certain circumstances, can be attributed both to the norm and to mental retardation. The traditional division of backwardness into degrees, which is of great practical importance, is also conditional. In accordance with the most common classification, three levels or degrees of retardation are distinguished: mild (IQ 50–69), moderate (IQ 20-49), severe (IQ below 20). This division is approximate and depends on the tests used to assess intelligence. The American Association for the Study of Mental Disability has proposed another classification with five levels of retardation, from borderline to profound.
This division is approximate and depends on the tests used to assess intelligence. The American Association for the Study of Mental Disability has proposed another classification with five levels of retardation, from borderline to profound.
Although the degree of mental retardation is conditionally determined by the IQ value, in each case, other characteristics must be taken into account, in particular social competence. Thus, according to English law, persons who are unable to take care of the safety of their bodies are considered severely retarded, those who are unable to maintain their existence are moderately retarded, and those who are incapable of planning and arranging their lives and are in need of guardianship are considered mildly retarded. nine0019
Since the 1950s, more and more attention has been paid to the education of mentally retarded children. In this regard, it became necessary to differentiate such children into learners and those who are only capable of acquiring certain skills.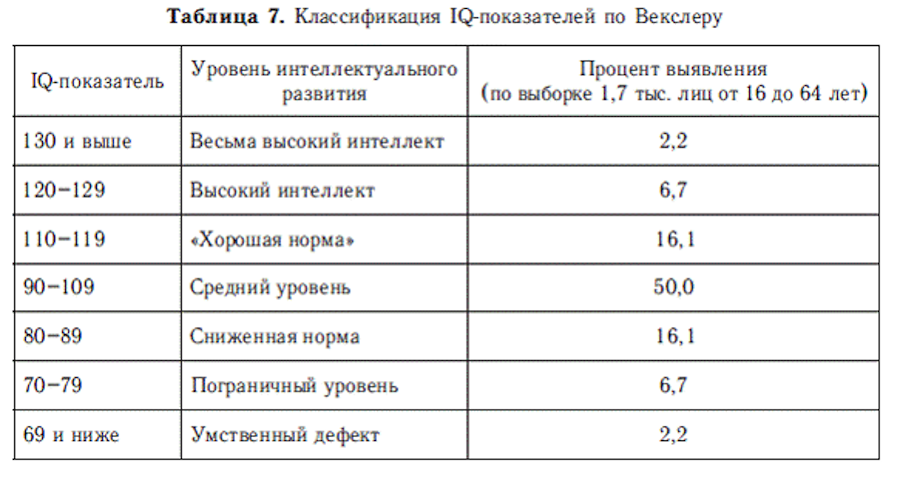 The former can learn a simple curriculum in special classes, while the latter can only develop household, motor and, to a very limited extent, speech skills with the help of special classes (training). It is believed that it is useful for children of both the first and second groups to attend classes at school while living at home. The IQ boundaries of both groups overlap markedly, but those who are able to learn have an average IQ of 50, while those who are only capable of acquiring skills are about 30. In more severe cases, when patients are not amenable to learning during group classes, only care and supervision. nine0019
The former can learn a simple curriculum in special classes, while the latter can only develop household, motor and, to a very limited extent, speech skills with the help of special classes (training). It is believed that it is useful for children of both the first and second groups to attend classes at school while living at home. The IQ boundaries of both groups overlap markedly, but those who are able to learn have an average IQ of 50, while those who are only capable of acquiring skills are about 30. In more severe cases, when patients are not amenable to learning during group classes, only care and supervision. nine0019
Clinical forms.
Depending on the accompanying syndromes, mental retardation can be classified into separate clinical forms. These forms are varied, but few of them are so common as to be of general interest. One of the most common forms is Down's syndrome, which is found in more than 10% of mentally retarded people hospitalized in psychiatric institutions. Patients with this syndrome are usually physically underdeveloped, undersized, they have a small rounded head, characteristic anomalies of the face and hands, narrow slanting eyes, giving the patient an outward resemblance to the faces of the Mongoloid race. Hence the original name of the disease - Mongolism. This name is erroneous, since Down syndrome occurs in representatives of all races. Approximately with the same frequency, mental retardation associated with cerebral palsy is detected ( see also DOWN SYNDROME; CEREBRAL PALSY).
Patients with this syndrome are usually physically underdeveloped, undersized, they have a small rounded head, characteristic anomalies of the face and hands, narrow slanting eyes, giving the patient an outward resemblance to the faces of the Mongoloid race. Hence the original name of the disease - Mongolism. This name is erroneous, since Down syndrome occurs in representatives of all races. Approximately with the same frequency, mental retardation associated with cerebral palsy is detected ( see also DOWN SYNDROME; CEREBRAL PALSY).
Other forms of mental retardation are relatively rare: they occur in no more than 1% of persons admitted to psychiatric hospitals. Microcephaly is characterized by a small, wedge-shaped skull with a sloping forehead. With hydrocephalus, there is an accumulation of cerebrospinal fluid in the ventricles of the brain due to a violation of its absorption or blockade of the outflow tract; as a result, the brain is stretched, its convolutions are smoothed out, and the size of the skull is increased. In case of insufficiency of thyroid hormones, cretinism develops, which is easy to diagnose by signs such as a flattened, broad face, rough thick skin, short crooked legs, short stature. With the so-called. in congenital ectodermoses (phakomatoses), mental retardation is combined with tumors of the nervous system and skin changes. Phenylketonuria leads to mental retardation due to hereditary metabolic disorders ( see also Phenylketonuria). Another example of a hereditary metabolic disease is Tay-Sachs disease, characterized by progressive blindness, thin limbs, and mental retardation.
In case of insufficiency of thyroid hormones, cretinism develops, which is easy to diagnose by signs such as a flattened, broad face, rough thick skin, short crooked legs, short stature. With the so-called. in congenital ectodermoses (phakomatoses), mental retardation is combined with tumors of the nervous system and skin changes. Phenylketonuria leads to mental retardation due to hereditary metabolic disorders ( see also Phenylketonuria). Another example of a hereditary metabolic disease is Tay-Sachs disease, characterized by progressive blindness, thin limbs, and mental retardation.
However, the most significant part of the mentally retarded are those who do not show signs of any specific clinical form and who are outwardly indistinguishable from healthy people. This form is called simple, or subclinical. The decrease in intelligence in such individuals is usually mild or borderline between moderate and mild mental retardation. At the same time, patients with specific clinical forms are more likely to have a severe or moderate decrease in intelligence.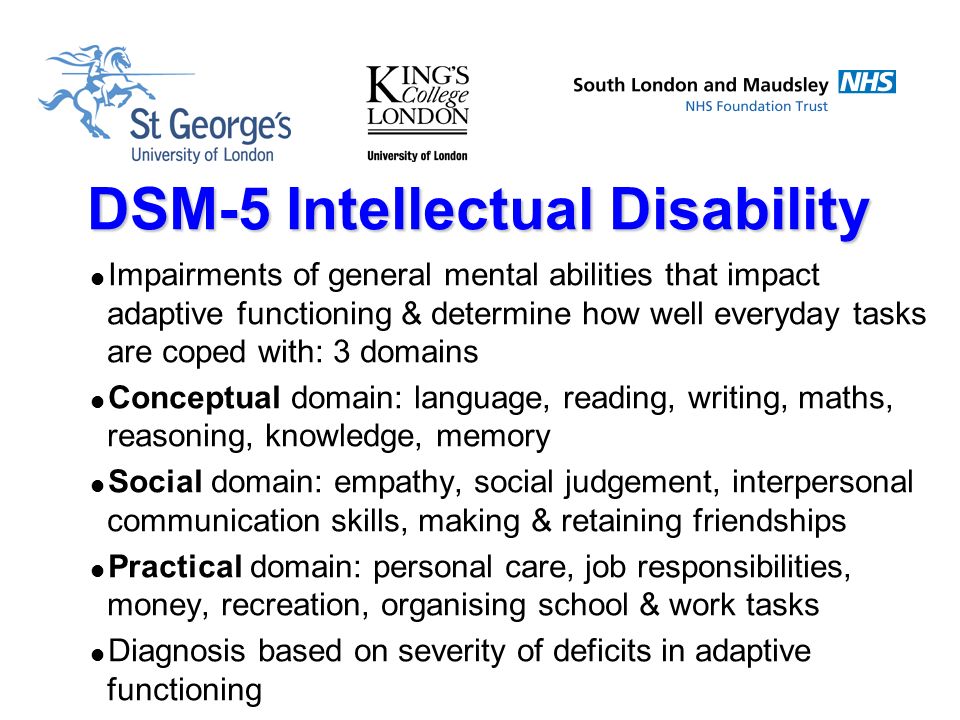 nine0019
nine0019
Reasons.
The causes of mental retardation are mainly those damaging factors that act in utero (prenatal factors), during childbirth (perinatal) and immediately after childbirth (early postnatal). Prenatal factors include malnutrition, endocrine disorders, intoxication, radiation exposure, and infections that the mother had during pregnancy (for example, rubella). Perinatal factors include cerebral hemorrhage, anoxia (oxygen starvation), mechanical damage to the brain during childbirth. The most common postnatal causes are severe infectious diseases of newborns, mainly meningitis and encephalitis, accompanied by inflammation of the brain. It should be noted that not all patients who have been exposed to these factors develop mental retardation. In addition, its development depends more on the time when the factor acted than on its nature. In other words, any of a number of completely different factors, acting at a certain period of individual development, can lead to the development of the same form of mental retardation, and the same factor, acting at different periods, can cause its various forms. nine0019
nine0019
It is possible that Rh-conflict between mother and fetus is also among the causes of mental retardation. Since during pregnancy a certain amount of the mother's blood plasma enters the fetus's body, if the Rh factor or other blood factors are incompatible, massive destruction of its blood cells (erythrocytes) can occur with serious consequences for the developing organism. It is believed that even in the absence of obvious signs of pathology, damage to blood cells can be severe enough to disrupt brain development and cause subsequent mental retardation. A number of studies have found that among persons with a simple form of it, Rh-positive children born from Rh-negative mothers are more common than among healthy or patients with specific forms of mental retardation. At the same time, these data have not been confirmed by other studies, so a final conclusion cannot yet be made. nine0019
Heredity is now considered to be a less common cause of retardation than previously thought. Hereditary include such rare forms as, for example, phenylketonuria and Tay-Sachs disease. They are associated with metabolic disorders, which are based on a single recessive gene. It is believed that some cases of microcephaly are due to a genetic defect. Down syndrome, although caused by a chromosomal abnormality, is not inherited; its cause is an error (non-disjunction of one of the pairs of chromosomes) that occurs during the formation of germ cells in the mother and leads to the fact that the child receives additional chromosomal material, usually in the form of the third 21st chromosome (normally there should be only two). nine0019
Hereditary include such rare forms as, for example, phenylketonuria and Tay-Sachs disease. They are associated with metabolic disorders, which are based on a single recessive gene. It is believed that some cases of microcephaly are due to a genetic defect. Down syndrome, although caused by a chromosomal abnormality, is not inherited; its cause is an error (non-disjunction of one of the pairs of chromosomes) that occurs during the formation of germ cells in the mother and leads to the fact that the child receives additional chromosomal material, usually in the form of the third 21st chromosome (normally there should be only two). nine0019
There is still debate about the role of heredity and organic pathology in the development of a simple form of mental retardation. Some researchers propose to divide this form into exogenous and endogenous, depending on whether organic brain damage is detected or not. The existence of these two variants is supported by case histories and psychological studies. The exogenous variant is more clearly associated with external factors, while in the endogenous variant, apparently unknown hereditary factors play a decisive role. In favor of the latter assumption, in particular, the results of pathoanatomical studies, which often reveal signs of a general underdevelopment of the nervous system, testify. On the other hand, there is evidence of a possible role of family conditions, at least in some cases. Unlike patients with specific forms of mental retardation, people with a simple form are more likely to be brought up in poor socio-economic conditions or dysfunctional families. Therefore, more and more attention is now being paid to parenting methods and other family factors that can contribute to the development of mental retardation in children without organic pathology. nine0019
The exogenous variant is more clearly associated with external factors, while in the endogenous variant, apparently unknown hereditary factors play a decisive role. In favor of the latter assumption, in particular, the results of pathoanatomical studies, which often reveal signs of a general underdevelopment of the nervous system, testify. On the other hand, there is evidence of a possible role of family conditions, at least in some cases. Unlike patients with specific forms of mental retardation, people with a simple form are more likely to be brought up in poor socio-economic conditions or dysfunctional families. Therefore, more and more attention is now being paid to parenting methods and other family factors that can contribute to the development of mental retardation in children without organic pathology. nine0019
Treatment.
Medications.
The possibilities of drug therapy in the prevention or treatment of mental retardation are very limited. The effectiveness of thyroid hormones in cretinism has been well studied: their administration at an early age usually prevents the development of both physical anomalies and intellectual impairment.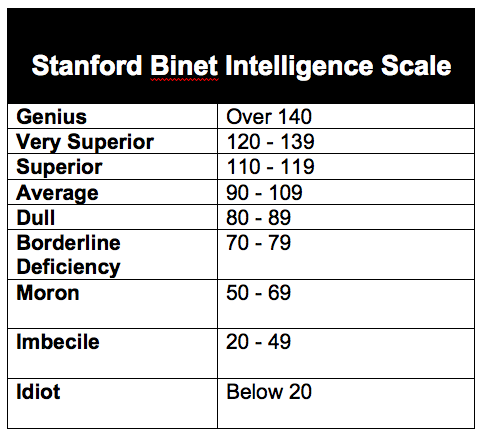 According to some reports, thyroid hormones have a beneficial effect in Down syndrome. Other options for hormone therapy are currently being researched, but all are under development. In phenylketonuria, some improvement can be achieved by long-term adherence to a diet based on the exclusion of phenylalanine. Ongoing biochemical studies open up ever greater possibilities for preventing the consequences of such metabolic disorders, for example, by timely administration of substances that are not synthesized in the body due to a genetic defect. nine0019
According to some reports, thyroid hormones have a beneficial effect in Down syndrome. Other options for hormone therapy are currently being researched, but all are under development. In phenylketonuria, some improvement can be achieved by long-term adherence to a diet based on the exclusion of phenylalanine. Ongoing biochemical studies open up ever greater possibilities for preventing the consequences of such metabolic disorders, for example, by timely administration of substances that are not synthesized in the body due to a genetic defect. nine0019
Trials of a glutamic acid preparation proposed for the treatment of children with mental retardation were carried out. It is believed that this acid, one of the essential amino acids that make up proteins, can improve intellectual functions by affecting brain metabolism. Some experimenters have noted a significant increase in the average IQ of mentally retarded children who took glutamic acid for a long time. However, other researchers do not confirm these results. But even with a positive result, it is not clear whether it is associated with a specific biochemical effect of glutamic acid on the brain or with a non-specific effect of the general improvement of the body and an increase in the activity of children. A significant long-term effect can be obtained by preventing the development of nutritional deficiencies in the prenatal period. In one study, mothers who were chronically malnourished for socioeconomic reasons were given thiamine and other vitamins during pregnancy and lactation. This improved the intellectual development of their children: at the age of three and four, they had a significantly higher Stanford-Binet IQ than children of mothers who did not receive vitamins. nine0019
But even with a positive result, it is not clear whether it is associated with a specific biochemical effect of glutamic acid on the brain or with a non-specific effect of the general improvement of the body and an increase in the activity of children. A significant long-term effect can be obtained by preventing the development of nutritional deficiencies in the prenatal period. In one study, mothers who were chronically malnourished for socioeconomic reasons were given thiamine and other vitamins during pregnancy and lactation. This improved the intellectual development of their children: at the age of three and four, they had a significantly higher Stanford-Binet IQ than children of mothers who did not receive vitamins. nine0019
Training (learning) is an important part of the mentally retarded treatment programs and its importance is constantly growing. Teaching can be carried out in psychiatric institutions, specialized schools, at home - under the supervision of specially trained teachers. With severe mental retardation, the child is taught the ability to serve himself, coordinate movements, recognize external stimuli, as well as other simple skills necessary in everyday life. In view of the frequent speech disorders, much attention is paid to speech education in such programs. In less severe cases, children are taught elementary knowledge and work skills. Some specialized schools have pre-school departments to prepare mentally retarded children for admission to a regular or specialized school. nine0019
With severe mental retardation, the child is taught the ability to serve himself, coordinate movements, recognize external stimuli, as well as other simple skills necessary in everyday life. In view of the frequent speech disorders, much attention is paid to speech education in such programs. In less severe cases, children are taught elementary knowledge and work skills. Some specialized schools have pre-school departments to prepare mentally retarded children for admission to a regular or specialized school. nine0019
Long-term follow-up of mentally retarded persons who received education in specialized schools or underwent rehabilitation in psychiatric institutions reveals good results: most of these persons are professionally and socially adapted to life; many acquire domestic independence and find stable work; repeated tests show a significant increase in IQ compared to the original value. In addition, according to the survey, children of such individuals showed a spread of IQ results about the same as among the rest of the population, and the average value was only slightly below 100.
Psychotherapy.
The possibilities of psychotherapy for mentally retarded people are attracting more and more attention. Although this retardation is not in itself associated with neurosis or psychosis, those who suffer from it are subject to psychological disorders no less than healthy people. Moreover, in some patients, the frustration associated with their disability gives rise to anxiety and aggressive behavior. Attempts to use some form of psychotherapy in mentally retarded hospitals have shown encouraging results. Given the poor language development of most mentally retarded individuals, non-verbal communication methods, including finger painting (washable paint) and modelling, may be helpful. Occupational therapy is a mandatory part of educational programs. Group psychotherapy with role-playing and discussion of problems also finds some use in stationary settings. nine0033 See also INT.
Mental retardation
Mental retardation is a congenital or acquired (by a child under the age of 3 years) decrease in intelligence. At the same time, the ability for abstract thinking is mainly reduced (it is this that is the basis of mathematical abilities, logic, and even creativity). At the same time, the emotional sphere practically does not suffer - i.e. patients with mental retardation feel sympathy and dislike, joy and grief, sadness and fun, perhaps the emotions of mentally retarded people are not as multifaceted and complex as those of people with normal intelligence. It is important to note that mental retardation does not tend to progress - i.e. the level of underdevelopment of the intellect is stable, and sometimes the intellect even increases with time under the influence of training and upbringing. nine0019
At the same time, the ability for abstract thinking is mainly reduced (it is this that is the basis of mathematical abilities, logic, and even creativity). At the same time, the emotional sphere practically does not suffer - i.e. patients with mental retardation feel sympathy and dislike, joy and grief, sadness and fun, perhaps the emotions of mentally retarded people are not as multifaceted and complex as those of people with normal intelligence. It is important to note that mental retardation does not tend to progress - i.e. the level of underdevelopment of the intellect is stable, and sometimes the intellect even increases with time under the influence of training and upbringing. nine0019
The terms "debility", "imbecile" and "idiocy", used in the traditional classification, are completely excluded from the ICD-10. This was done due to the fact that they went beyond a purely medical framework, they began to play a social (negative) connotation. Instead, it is proposed to use exclusively neutral terms that quantitatively reflect the degree of mental retardation.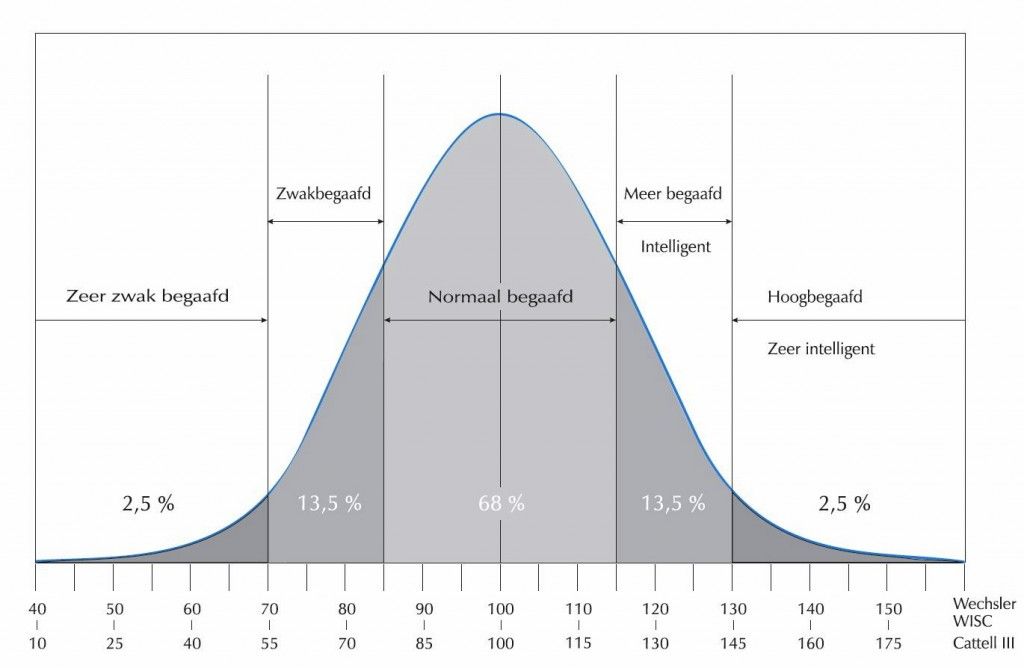 To date, there are 4 degrees:
To date, there are 4 degrees:
1. Easy - corresponds to the traditional concept of "debility", IQ 50-69.
2. Moderate - imbecility, IQ 35-49.
3. Severe - imbecility, IQ 20-34.
4. Deep - idiocy, IQ < 20.
Mild mental retardation
Outwardly, such people may not differ at all from healthy people. They usually experience learning difficulties due to a reduced ability to concentrate. At the same time, their memory is quite good. Often people with a mild degree of mental retardation are dependent on parents or caregivers, they are afraid of a change of scenery. Sometimes such people become withdrawn (because they do not recognize other people's emotions well, therefore they experience difficulties in communication). And sometimes, on the contrary, they try to attract attention to themselves with various bright actions, usually ridiculous. Almost everyone is aware of their difference from healthy people and seeks to hide their disease. The vast majority of them also achieve complete independence in personal care and in practical and domestic skills, even if development is much slower than normal. The main difficulties are usually observed in the field of school performance and many have special problems in reading and writing. nine0019
The main difficulties are usually observed in the field of school performance and many have special problems in reading and writing. nine0019
Moderate mental retardation
People with this diagnosis are able to experience affection, distinguish between praise and punishment, they can be taught basic self-care skills, and sometimes even reading, writing, and simple arithmetic. Individuals in this category slowly develop understanding and use of speech, and the final development in this area is limited. School success is limited, but some patients master the basic skills necessary for reading, writing and counting. In adulthood, persons with moderate mental retardation are usually capable of simple practical work with careful construction of tasks and the provision of qualified support. Completely independent living is rarely achieved. However, such people are generally fully mobile and physically active, and most of them show signs of social development, which is the ability to establish contacts, communicate with other people and participate in basic social activities. nine0019
nine0019
Severe mental retardation
People with this diagnosis can partially master speech and acquire basic skills to serve themselves. Vocabulary is very poor, sometimes it does not exceed ten or twenty words. Almost all of them are needed to communicate their own desires and needs, their thinking is very concrete, chaotic and unsystematic. Phenomena and objects that are not familiar to children may not cause any response. Satisfactorily distinguished are those objects that are well and long familiar, which are constantly before the eyes. On rare occasions, some may master the counting of visible objects, or group real things together, such as furniture or clothing. There are also movement disorders - the gait is slow and clumsy, the movements of the arms and legs are late and do not have amplitude. nine0019
Profound mental retardation
In people with deep brain damage, the structures of internal organs are very often disturbed. Speech is completely absent, they emit either separate syllables or inarticulate sounds, repeating them endlessly.