Mdd with anxious distress
What Is Major Depression With Anxious Distress?
It's no secret that anxiety conditions and depression co-occur. In fact, most researchers agree they co-occur at least 60 percent of the time. They're so interrelated that most antidepressants are also often effective for anxiety; both conditions are highly associated with decreased serotonin. With these facts in mind, it's no surprise that some people, when they experience a Major Depressive Disorder (MDD) episode, there is an onset of some specific anxiety that is congruent to the depression.
Source: Gert Altmann/Pixabay
The presentation:
MDD patients with Anxious Distress are not only down and out. They're tormented by inner restlessness and anticipating worst-case scenarios that compound the negative thinking already present from the depression. Unfortunately, it seems like anxious distress is more common than meets the eye. Researchers like Zimmerman et al. (2018) have noted that, in a sample of 260 people with MDD, 75 percent met the criteria for the specifier; this was after controlling for co-occurring anxiety disorders.
Imagine the compounded misery of patients, like Liz:
The case of Liz:
Liz, a 26-year-old part-time college student, was no stranger to anxiety. She struggled with Social Anxiety Disorder (SAD) throughout her teens and 20's. It was tough for her to get through college, but she was gaining on it. Nonetheless, like many suffering from SAD, Liz was prone to MDD. For Liz, the episodes would come on when she began dwelling on how stalled her life was from SAD. Many peers were already in careers and had a family, and she wondered if she'd ever make it. Liz made an appointment with Dr. H, her long-term psychologist, because the depression felt different this time. In her voicemail to Dr. H, she said, "Doc, I've dealt with being depressed, I've dealt with getting through socially anxious situations, but I'm not handling well whatever is happening to me this time."
At her appointment, Dr. H noticed Liz not only going to that dark place again, but she also appeared to have a tense jaw and was prone to hand wringing; she looked very uneasy on top of being depressed.
Liz confessed that the past couple of weeks she was increasingly dreading that she will never get out from under this psychological roller coaster. "I'm so stuck!" she lamented, noting she worries about the depression never ending and being alone forever. "It seems so futile, I may as well give up," Liz mumbled through tears.
Courtesy of page 184 in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), the criteria for With Anxious Distress (which must be present more days than not during the current Major Depressive episode) are:
- Poor concentration due to worry
- Feeling tense
- Restlessness
- The feeling something bad will happen
- The feeling of losing control.
Critical thinking about what qualifies as an Anxious Distress specifier:
Though Liz experienced an anxiety disorder at baseline, Social Anxiety, it does not make the fact she experienced an anxiety disorder and a depressive episode together as "with anxious distress.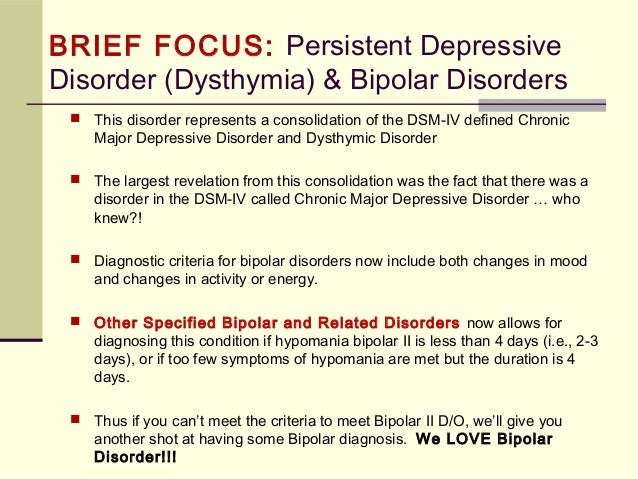 " These would be considered independent, co-occurring diagnoses. The anxiety symptoms that arose with the MDD episode were a direct consequence of her mood; "owned by the depression," if you will, and therefore meet the criteria for With Anxious Distress specifier. Interested readers are directed to Yang et al. (2014) who explores this in detail.
" These would be considered independent, co-occurring diagnoses. The anxiety symptoms that arose with the MDD episode were a direct consequence of her mood; "owned by the depression," if you will, and therefore meet the criteria for With Anxious Distress specifier. Interested readers are directed to Yang et al. (2014) who explores this in detail.
You may be asking yourself, "What about if the person develops panic attacks from being so overwhelmed by the depression?" Panic is "special" in that any condition can have a "with panic" specifier. Just because someone experiences a panic attack or occasional attacks, also doesn't mean they have Panic Disorder.
There must also be significant fear of future attacks and or maladaptive behaviors to try to keep future attacks at bay, like avoiding exercise and sex because the exertion can lead to feelings that are reminiscent of panic symptoms and there is fear it may evolve into an attack. Of course, someone may have MDD and Panic Disorder if full criteria for the latter are also met. Readers are directed to page 214 of the DSM-5 for more information on this nuance.
Readers are directed to page 214 of the DSM-5 for more information on this nuance.
Though uncomfortable, panic is often sporadic and fleeting, while the symptoms of With Anxious Distress must be specifically noted because they are chronic and gnawing, adding torment to the person's condition. Imagine suffering the low feeling of serious depression, coupled with a feeling that you can't gain control, feeling physically tense, and worrying it will never end. This is quite a problem in that, as seen with Liz, the depression encourages the anxiety, and that added anxiety encourages intensifying depression.
Treatment implications:
This additional insult of anxiety on the MDD episode can induce so much havoc that Barlow and Durand (2015) note, "The presence of anxiety [in depressive episodes] makes a more severe condition, makes suicidal thoughts and completed suicide more likely, and predicts a poorer outcome."
Research is not clear if Anxious Distress tends to be a trend in every episode for people prone to it, or if it may vary. Regardless, given the gravity of the matter, clinicians must be vigilant to the possibility of arising Anxious Distress amid their patients' MDD episodes, and evaluate accordingly. Patients may not be as forthcoming and obvious as Liz. Perhaps it is more of an inner tension they are experiencing, and the patient assumes worrying their life will never get on track is just part of being depressed. Directly asking depressed patients if they've begun to develop muscle tension, worry, and feeling they're losing control takes mere minutes and can have big clinical payoffs. Assuaging the anxiety will help in managing the MDD.
Regardless, given the gravity of the matter, clinicians must be vigilant to the possibility of arising Anxious Distress amid their patients' MDD episodes, and evaluate accordingly. Patients may not be as forthcoming and obvious as Liz. Perhaps it is more of an inner tension they are experiencing, and the patient assumes worrying their life will never get on track is just part of being depressed. Directly asking depressed patients if they've begun to develop muscle tension, worry, and feeling they're losing control takes mere minutes and can have big clinical payoffs. Assuaging the anxiety will help in managing the MDD.
Source: Cottonbro/Pexels
Clinical considerations if Anxious Distress is suspected:
- Suicide prevention: Suicide attempts may be more prevalent with anxious distress, evaluating for risk is even more important.
- Be sure to consult with the person's prescriber if you are concerned about Anxious Distress. They should be aware because some medications could exacerbate the anxiety, and there is always the possibility the anxiety will not get reported or noticed in the prescriber's office.

- Evaluate if the person's lifestyle may be exacerbating the anxious distress. Namely, are they caffeine consumers, eat a lot of junk food or sugar, and get no exercise? It's no surprise that caffeine and sugar can make things worse. Exercising, if they are capable, can help "burn off" some anxiety; it can also provide further structure and occupation rather than being 100 percent stuck inside their mind. The old saying is particularly true for sufferers of depression and anxiety: "idle mind = devil's playground." The positive effects of exercise on anxiety and depression are well-documented. If the person does not already exercise, of course suggest they consult their doctor before initiating a regimen.
- Once beginning to stabilize, the job of a therapist is to not only help the episode to continue to remit but continue to evaluate for any return of the Anxious Distress. In the long run, prevention is the best option. If we know a patient is prone to Anxious Distress, it is of utmost importance to have a plan in place to immediately return to treatment if they or friends and loved ones recognize the onset of a depressive episode.
 Keeping the MDD at bay likely will help keep the Anxious Distress away.
Keeping the MDD at bay likely will help keep the Anxious Distress away.
Stay tuned for the next post on Monday, October 11, for a tour of Melancholic Features, perhaps the "darkest flavor" of Major Depressive Disorder.
References
Barlow, D.H. and Durand, V.M. (2015). Abnormal psychology: an integrative approach. Cengage.
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association, 2013.
Yang, M.J., Kim, B.N., Lee, E.H., Lee, D., Yu, B.H., Jeon, H.J., & Kim, J.H. (2014). Diagnostic utility of worry and rumination: a comparison between generalized anxiety disorder and major depressive disorder. Psychiatry and Clinical Neurosciences (68), 712–720 doi:10.1111/pcn.12193
Zimmerman, M., Martin, J., McGonigal, P., Harris, L., Kerr, S., Balling, C., Keifer, R., Stanton, K., & Dalrymple, K. (2018). Validity of the dsm-5 anxious distress specifier for major depressive disorder. Depression and Anxiety (36) 1, 31-38. https://doi.org/10.1002/da.22837
Depression and Anxiety (36) 1, 31-38. https://doi.org/10.1002/da.22837
Anxious distress and major depressive disorder: Recognition, assessment and treatment
Anxious distress in depressive disorders
Globally, major depressive disorder (MDD) is one of the leading causes of disability.1 Within the category of depressive disorders, in DSM 5, anxious distress includes patients who experience episodes of at least two of the following: feeling keyed up/tense; feeling unusually restless; feeling difficulty concentrating due to worry; fear that something awful may happen; feeling loss of control.2
Many patients with MDD also experience anxious distress
Anxious distress may occur in the majority of people with MDD;3 however, Professor Hopwood discussed, patients may not be able to recall if anxious distress preceded onset of MDD and anxious depression may be hard to distinguish from an anxiety disorder. 4
4
It is important to recognise anxious distress, stressed Professor Hopwood, as when it is present with MDD, longer times to remission5 have been shown and patients report poorer functioning and coping abilities than those without anxious distress.6 With these in mind, he concluded, recognition and treatment of anxious distress is key in people with MDD.
Pharmacotherapy for anxiety symptoms in MDD
According to Professor Stein, there are several ways a person can meet diagnostic criteria for MDD. Domains that need to be assessed include not only symptom profile and current stressors, but also early trauma and family history, personality traits, neurocognition, resilience, comorbidities, functioning, severity/staging and clinical subtype. Assessment also needs to take in factors such as social and material resources, occupation, family, abilities and intimate relationships and be culturally congruent.7
Within the diagnosis of MDD, anxious depression is associated with greater neuropathological findings, worse outcomes, greater MDD severity and increased suicidality. According to Professor Stein, taking these factors into account means treatment should be tailored accordingly.8
According to Professor Stein, taking these factors into account means treatment should be tailored accordingly.8
Anxious depresssion is associated with greater severity and worse outcomes in MDD
A large meta-analysis found that no one antidepressant medication stands out as being more efficacious or better tolerated for such.9 Analysis of studies of combination treatment of medication plus psychotherapy found this more effective than either psychotherapy (relative rate [RR] 1.27, 95% confidence interval [CI] 1.14, 1.39) or pharmacotherapy (RR 1.25, 95% CI 1.14, 1.37) alone. Combined treatment was also more acceptable.10
The Taiwan Tailor Survey of what patients want in MDD treatment
Within this symposium, Professor Chang presented results from a Taiwan Tailor Survey that investigated experience, preferences and stigmatized attitudes toward depression and antidepressants. This survey included 340 patients with MDD who were taking at least one antidepressant for at least a month and had no major comorbid psychiatric disorder, neurological condition or substance use disorder.
Respondents were mainly female (73.2%) and aged 21−50 (84.4%). Results showed that 37.1% had not sought help at their first episode of depression (mean age 32.8), predominantly because they didn’t know they were experiencing this or didn’t know where to get treatment. When they did seek help, most patients went to a psychiatrist or a counsellor. Regarding their current episode, reasons for seeking help included emotional, physical or life disturbances, insomnia and suicidal ideation.
The survey also revealed that treatment for depression was most often the decision of healthcare professionals and that patients prefered a combination of pharmacotherapy and psychotherapy over either treatment alone.
Reasons for medication non-adherence include both symptom recovery and adverse events
When patients were asked about medication adherence, 50.3% reported that they had been nonadherent to an antidepressant, with the main reasons cited being because they felt better, they experienced adverse events or the medication was not effective.
Concerns about adverse events included that antidepressants might cause withdrawal effects, sleep disturbances, weight gain, anhedonia and sexual dysfunction.
A final question on the survey was with regard to stigma, with higher ratings for what participants thought other people may believe regarding depression, such as that a person could snap out of it or that it was a sign of personal weakness, than they themselves believed.
causes, symptoms, diagnosis, treatment, therapy and drugs
Anastasia Somova
worries a lot
Author profile
I suffered from increased anxiety since childhood, and at the age of 22 a psychiatrist diagnosed me with generalized anxiety disorder.
I am now 24 years old and have had severe anxiety since I was 15. I was treated for vascular dystonia, headaches, sleep problems, low blood pressure.
In the eleventh grade, at the peak of preparation for the Unified State Examination, I fainted at school and ended up in the hospital - in the children's neurological department. There, too, no one suspected a psychiatric diagnosis and problems with mental health. But they prescribed a whole list of non-working drugs - nootropics and the like. At that moment, I myself did not know anything about mental disorders.
There, too, no one suspected a psychiatric diagnosis and problems with mental health. But they prescribed a whole list of non-working drugs - nootropics and the like. At that moment, I myself did not know anything about mental disorders.
Explain how I got the correct diagnosis and how I live with Generalized Anxiety Disorder.
Go see a doctor
Our articles are written with love for evidence-based medicine. We refer to authoritative sources and go to doctors with a good reputation for comments. But remember: the responsibility for your health lies with you and your doctor. We don't write prescriptions, we make recommendations. Relying on our point of view or not is up to you.
What is Generalized Anxiety Disorder
The International Classification of Diseases has an entire section on anxiety and fear-related disorders.
Generalized Anxiety Disorder in Adults - Uptodate
Generalized Anxiety Disorder in Adults: Management - Uptodate
Generalized Anxiety Disorder is the most common of these. In addition, this disease is generally one of the most common mental disorders.
In addition, this disease is generally one of the most common mental disorders.
Why Generalized Anxiety Disorder develops is not yet known. Perhaps this is due to a disruption in the production of a number of neurotransmitters, that is, connections due to which brain neurons communicate with each other, or to a change in metabolism in some parts of the brain. There is also a link between increased anxiety and a large number of traumatic situations, especially in childhood.
Generalized Anxiety Disorder - NHS
Generalized anxiety disorder can begin at any age. For no reason, a strong anxiety appears that prevents a person from living and working normally. Anxiety attacks can be accompanied by bodily manifestations: a feeling of lack of air, a strong heartbeat, numbness of the limbs, and others.
The disease does not pass without a trace, not only for the psyche. According to some data, increased anxiety increases the risk of coronary heart disease and hypertension, and also increases the risk of death from cardiovascular diseases in general.
I believe that my disorder began to manifest itself in childhood. I grew up with a constant feeling of anxiety, which became stronger with age. My father is a very specific person. He could at one point just stop talking to me and mom. I collected my things and "moved" to another room - the apartment was big enough. I don’t know why I, a small child, fell under this “torture by silence”. Colliding in the corridor or at the front door, we did not say hello.
I also had constant headaches from the age of six. I was examined, but the reasons were not found. Neurologists prescribed glycine, physiotherapy and pain relief according to the situation.
/migraine-kids/
How to Treat Migraines in Children and Adolescents
Now, after going through therapy and many hours of soul-searching, I understand that almost every interaction with my father went through anxiety.
For example, with a good family income, you had to beg for clothes, choosing the time when he was in a good mood. Trips - no matter to the country or abroad - have always been nervous and stressful.
Trips - no matter to the country or abroad - have always been nervous and stressful.
I wasn't taught to recognize emotions, so I didn't know it was anxiety. I felt it as a restless state in which everyone lives in one way or another - that's how it seemed to me then.
Headaches, by the way, disappeared with the start of taking antidepressants. The psychiatrist said that most likely they were one of the symptoms of the disorder.
Symptoms of generalized anxiety disorder
Kirill Sychev
psychiatrist, psychotherapist
The main difference between generalized anxiety disorder and other disorders is that anxiety in it is not limited to specific situations. That is, anxiety lasts for a long time - a month or more, for at least two weeks, and does not depend on what the person does.
The main signs of pathological anxiety are intense, constant, almost uncontrollable, and appear without clear causes. A person with an anxiety disorder usually feels fear, distress, and impending danger most of the time.
Anxiety becomes a constant companion: a person wakes up in anxiety, worries all day for a million different reasons and without, falls asleep for a long time and sleeps badly because of anxiety. At the same time, he cannot cope with this feeling on his own.
Life before diagnosis
Anxiety did not recede during adolescence, and then it only got worse. After school, I entered St. Petersburg State University, where I really wanted to go. However, as a result, I was expelled at the end of the third year - I did not even pass the session to get an incomplete higher education.
Six months before that, there was a period of constant unreasonable anxiety, absolute impotence, inability to sleep and unwillingness to get out of bed. Most of the time I didn't go to university. The people around attributed everything to laziness, but in fact, sometimes I physically could not force myself to get out of bed and go to study. In fact, I did everything to be expelled: I didn’t have the strength to reach the administration and refuse to study myself. And the alarm would not even allow me to enter the faculty building.
And the alarm would not even allow me to enter the faculty building.
It was not customary in my environment to talk about problems with mental health. Perhaps if I had come across a person, video or text with recommendations to go to a psychiatrist with my symptoms, I would not have been expelled and life would have turned out differently.
After leaving the university for two years, I lived in a state of anxiety. I had a constant headache, ten painkillers were enough for a week. I went to a neurologist - he prescribed muscle relaxants and nootropics, and advised melatonin for sleep problems.
/guide/nootropics/
Nootropics: do they really improve brain function
My body has never been relaxed. Every little muscle was tense every second. Massage trips always took place with the requests of the master to relax. I didn’t sleep well, I could wake up at night and lie awake for several hours.
Anxiety arose even because of everyday trifles and was incommensurable with the problem. For example, dirty dishes in the sink in the morning, which the boyfriend had to wash, became the cause of terrible anxiety for the whole day. Even fixing the problem - washing dishes - did not change the state.
For example, dirty dishes in the sink in the morning, which the boyfriend had to wash, became the cause of terrible anxiety for the whole day. Even fixing the problem - washing dishes - did not change the state.
I think it comes from childhood - my father constantly scolded me for what I thought was a mess. It seemed to me that the dirty dishes in the sink meant that I was useless, you couldn’t love me, you had to leave me as soon as possible. In those moments, I did not recognize such thoughts as strange and illogical.
There was a similar situation with spending money: I bought something expensive, spent the money, so you can’t love me, you have to leave me alone. At the same time, my boyfriend and I have been together for a long time and have never quarreled over expenses that fit into the budget.
Community 08/24/21
How to get rid of the idea that there is not enough money?
In general, I had a clear set of anxiety triggers. These are dirty dishes and the floor, spending money on something relatively expensive, buying coffee to go, talking with your father. And if before the trigger, anxiety was background, then after it began to grow to the size of an entire planet.
These are dirty dishes and the floor, spending money on something relatively expensive, buying coffee to go, talking with your father. And if before the trigger, anxiety was background, then after it began to grow to the size of an entire planet.
At this time, popular science books came into my life. In the summer I bought a book by Daria Varlamova and Anton Zainiev “Go crazy! A Guide to Mental Disorders for a Big City Resident. One of the chapters is devoted to anxiety disorders - and it was about me, and so precisely that it became scary. At the same time, I learned about the Beck test for determining the level of anxiety, passed it and got almost the maximum score.
Beck's Anxiety Scale in Russian
However, I still didn't think about the urgent need for a psychiatrist. To go to the doctor, I had to make an effort and admit that I have a problem. I didn’t want to do this - I was afraid to be unnecessary and unloved again. After all, you cannot love a person with mental problems. My logic, of course, was wonderful.
My logic, of course, was wonderful.
First visit to a psychotherapist and diagnosis
One day I went to the market where I bought Uzbek tomatoes for 800 R per kilo. They were insanely delicious, fit into the budget, that is, the purchase should not have caused me discomfort. However, anxiety didn't think so. She covered me as soon as I left the market building.
The anxiety was so strong that I did not remember either the way to the house or how I spent the evening. I was shaking, at home I locked myself in the toilet and sobbed sobbing. I was suffocating, I was terribly out of breath. The night did not sleep, every second I thought about the price of tomatoes. One obsessive phrase was spinning in my head: "Tomatoes cost 800 R per kilogram."
/psychotherapy-search/
How to choose a psychotherapist
In the morning I began to google a psychotherapist. At that moment, I did not know about psychiatry according to compulsory medical insurance, as well as about the division of doctors into psychiatrists, psychotherapists and psychologists.
At that moment, I did not know about psychiatry according to compulsory medical insurance, as well as about the division of doctors into psychiatrists, psychotherapists and psychologists.
Can a psychologist work with anxiety disorders
Anna Shilova
psychologist
For a psychologist, the first meeting with a client is a diagnostic one. On it, we find out whether it is necessary to connect a psychiatrist. I ask questions about the quality of sleep, the level of libido, eating habits and appetite, chronic and current diseases, fatigue, somatic manifestations of anxiety, if any.
When I complain about anxiety, regardless of the data that I collected during the first meeting, after it I send a diagnostic questionnaire - it allows you to determine the likelihood of a diagnosis.
As a psychologist, I have no right to make diagnoses - this is beyond my competence. This part of the work is done by a psychiatrist. If, according to the results of the questionnaire and the collection of information, there are symptoms of a disorder, I send the person for a psychiatric consultation. I do this even with the slightest suspicion, because only a doctor can comment on whether it is necessary to connect medication to psychotherapy.
I do this even with the slightest suspicion, because only a doctor can comment on whether it is necessary to connect medication to psychotherapy.
I chose my first psychotherapist based on reviews and the ability to see me on the same day. The appointment then cost 3500 R. At the clinic, I was met by a pleasant doctor, led to the office, where he asked me to tell me what was bothering me. I told him about the tomatoes, the inability to sleep well, and my relationship with my father.
3500 Р
cost one appointment with a private psychotherapist
Before the appointment, I made a checklist for myself, where I wrote down the main causes of anxiety. It helped me a lot - due to the large flow of emotions at the reception, it was difficult to focus on my thoughts. The psychotherapist asked me questions, led me to reasoning, as a result, he diagnosed me with generalized anxiety disorder, and prescribed treatment.
Diagnosis of generalized anxiety disorder
Kirill Sychev
psychiatrist, psychotherapist
For a doctor to make a diagnosis, a person must have the following manifestations:
 Sometimes even headaches due to this tension;
Sometimes even headaches due to this tension; The American DSM-5 Diagnostic Manual also emphasizes that a person must have at least three of the following symptoms: feeling “on edge”, easy fatigue, difficulty concentrating, irritability, muscle tension, or sleep disturbance.
Treatment of generalized anxiety disorder
Anxiety disorder is treated with psychotherapy, particularly cognitive behavioral therapy, and medications, most commonly antidepressants. Psychotherapy can sometimes be used as the main method of treatment - it depends on the severity of anxiety and the patient's capabilities, since not everyone can regularly visit a psychotherapist.
Pharmacotherapy for Generalized Anxiety Disorder in Adults - Uptodate
Generalized Anxiety Disorder in Adults: Cognitive Behavioral Therapy and Other Therapies - Uptodate
My doctor recommended antidepressants at my first consultation.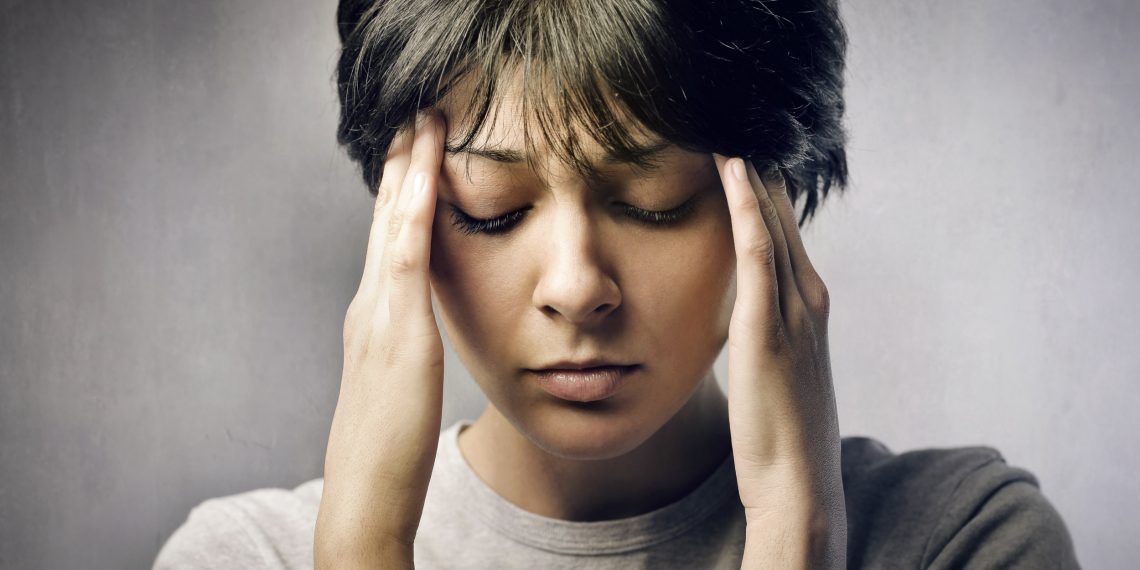 He told about their work and how to properly start a reception.
He told about their work and how to properly start a reception.
I really liked the metaphor about crutches and broken legs. Crutches are antidepressants. They will not help the leg grow together, but they will make life easier and make it possible to walk while the leg in the cast grows together. Gypsum, on the other hand, is therapy and its own work. You can walk on crutches for a long time without a cast, but nothing good will come of it.
With a psychotherapist, we also went through therapy. Then I didn’t know about different methods and schools of psychotherapy, so I can’t say exactly what technique he used. Most likely, it was one of the variations of cognitive behavioral therapy.
I was prescribed an antidepressant from the group of selective serotonin reuptake inhibitors, or SSRIs. Simply put, these drugs increase the concentration of serotonin in the brain, which improves mood and relieves anxiety. However, in the first weeks of taking such medications, they can cause the opposite side effect - increased anxiety. Therefore, in addition, I was prescribed a tranquilizer. He also helped to sleep well.
Therefore, in addition, I was prescribed a tranquilizer. He also helped to sleep well.
/list/antidepressant-myths/
8 myths about antidepressants
When I first handed the prescription to the pharmacist, I felt like I was buying something forbidden and scary. In the countries of the former CIS, antidepressants, it seems to me, do not have a good reputation, but in fact there is nothing wrong with such pills, let alone prohibited.
Tranquilizer relieves symptoms almost immediately. For a long time I lived with the feeling that someone stepped on my chest and I couldn’t breathe normally. The feeling of relaxation and calmness that I got after the first use of the medicines is hard to forget. It's like taking off uncomfortable shoes after a hard day's work or unzipping your jeans after a heavy meal - only ten times better.
Taking an antidepressant was easy enough for me. A month later, I again went to a psychotherapist and received a prescription for six months. In addition, I was also prescribed one of the neuroleptics for sleep. It took about 900 R per month for pills. We also discussed the issues that worried me again, they mainly concerned behavior patterns.
In addition, I was also prescribed one of the neuroleptics for sleep. It took about 900 R per month for pills. We also discussed the issues that worried me again, they mainly concerned behavior patterns.
900 R
on average I spent monthly on pills
Summer and early autumn after the first dose were among the best for me in several years. I lived the life of an ordinary person, I had enough strength to work, go to the gym, take long walks. If earlier I started shaking at the sight of a dirty plate in the sink in the morning, now it worried me much less.
My prescriptions for drugsHow generalized anxiety disorder is treated
Kirill Sychev
psychiatrist, psychotherapist
Treatment of generalized anxiety disorder usually begins with cognitive behavioral therapy, if the person agrees to it and is ready to do it. If it does not help or this option is not suitable for a person, we use pharmacological treatment.
Antidepressants, selective serotonin reuptake inhibitors and selective serotonin and norepinephrine reuptake inhibitors, i.e. SSRIs and SSRIs, are usually prescribed first.
Antidepressants are well-researched and effective drugs. This is the same adequate treatment for mental disorders as insulin for a person with diabetes or a painkiller for a fracture. They restore the correct functioning of the brain and thinking, give the patient the necessary resource to fight the disease.
Antidepressants are not addictive. From a medical point of view, addiction is a craving for use, accompanied by a constant increase in the dose of the substance taken. When taking antidepressants, there is no such craving. The patient does not need to constantly increase the dose. However, at the stage of selecting the drug, the doctor can increase it.
There are concepts of the minimum and maximum therapeutic dose - the first is not always enough, but it is never raised above the maximum. And then the patient drinks the medicine in the required amount until the end of the course.
And then the patient drinks the medicine in the required amount until the end of the course.
In the treatment of depression and anxiety disorders, antidepressants should be taken for at least a year from the moment the condition noticeably improved. So the risk of relapse is lower.
The first unsuccessful attempt to get to the doctor under OMI
In the autumn, a few months after the start of treatment, I decided to go to the psychotherapist again. The anxiety went away, but the dream began to go astray, there were questions that I would like to solve in therapy: I still transferred the patterns from the relationship with my father to the relationship with my boyfriend. At that moment, the price of seeing a paid psychotherapist increased to 5,000 R. I could not afford it and for the first time decided on CHI therapy.
At that time, a list with numbers of free psychological help roamed the Internet. There was also a number of a free psychotherapist in St. Petersburg, where I lived. Everything turned out to be not so simple: at first, I called the reception desk of one of the PNDs for about an hour, and they told me to call another phone number. By the second number they gave me another number. As a result, after a couple of hours, I got through and made an appointment. They asked me for my name and age, gave me the address and name of the doctor.
Petersburg, where I lived. Everything turned out to be not so simple: at first, I called the reception desk of one of the PNDs for about an hour, and they told me to call another phone number. By the second number they gave me another number. As a result, after a couple of hours, I got through and made an appointment. They asked me for my name and age, gave me the address and name of the doctor.
/psychotherapy/
How psychotherapy works
The office was in one of the clinics in my neighborhood. I arrived for the session at nine in the morning. At the registry, which was separate for a psychotherapist, they took my address of residence, passport number, compulsory medical insurance and SNILS, then I went to the doctor.
The first question the therapist asked me was if I was working. At that moment, I had problems with this, I honestly answered that I didn’t, and my boyfriend helps me with money. Here he began to scold me. He said that I had no right to apply for help under compulsory medical insurance, that I had to go to a paid doctor, that I was a parasitic and all that. And also that I can’t come to him, because this is an office not in my place of residence. After that, I didn’t want to open up to the person, I shrunk in my chair and almost cried. But I needed to extend the prescription - this is the only thing that kept me from escaping.
And also that I can’t come to him, because this is an office not in my place of residence. After that, I didn’t want to open up to the person, I shrunk in my chair and almost cried. But I needed to extend the prescription - this is the only thing that kept me from escaping.
After somehow telling what I was taking and what my diagnosis was, I asked for a prescription. He shook his head and began to tell me that I needed to leave Russia and there was nothing for me to do here. Then he recommended taking Phenibut, a drug that is available by prescription, but does not have proven effectiveness.
/healthcare/
9 problems of free healthcare in Russia
I left the office in shock. Fortunately, this did not affect my psyche - from the very beginning I managed to build an armor between me and this pseudo-psychotherapist. By the way, in the end he wrote out the prescriptions I needed. However, the experience was unsuccessful, so until the next year I was afraid to even think about psychotherapy.
| Minor work helped me get rid of obsessive thoughts during the treatment process. For the first time in my life, I picked up a hook and began to knit a string bag. Then it had to be dissolved, but these are trifles | But I nevertheless knitted a blanket made of special yarn - still one of my favorite things |
Treatment by a psychiatrist at the district dispensary according to compulsory medical insurance
In winter, I went into remission - this means that I felt like a healthy person for a long time on the therapeutic dosage of the medicine. Then I decided to reduce the dosage. A paid psychotherapist told me about the correct exit from treatment in one of the first sessions, so it seemed to me that I understood how to do it.
Back then, I was actively sitting on a mental health forum where people share their stories of illness and treatment. You can also consult a psychiatrist there. Such a consultation will not replace treatment and face-to-face sessions, but it can help in situations where you need an answer to a small question, but you don’t want to pay 5000 R for a session.
/list/psihiatr/
12 important questions to psychiatrist Kirill Sychev
I asked a question on the forum about the abolition of pills and received general recommendations. The dosage of the antidepressant was reduced very slowly, reaching 1/8 tablet. It was hard, because out of ignorance I did not take anything to alleviate the symptoms.
Of course, stopping antidepressants on my own was a big mistake. When taking any medication, you do not need self-activity and advice from the Internet. I decided to stop taking the pills too early - I had to take antidepressants for at least a year from the improvement in my condition, best under the supervision of a doctor.
Why you can’t stop drugs or change the dosage yourself
Kirill Sychev
psychiatrist, psychotherapist
You can’t stop psychiatric drugs on your own, because there is a high probability that side effects or a withdrawal syndrome will occur.
It is best to be in touch with your doctor during dose changes or withdrawals. So you can choose the right withdrawal tactics, add other drugs for this period that will remove side effects, change the rate of withdrawal, taking into account the reaction of the body.
In the spring of 2020, the COVID-19 pandemic struck, and I again developed severe anxiety. The social and medical problems associated with the coronavirus bypassed me, there were no objective reasons to worry. And I was worried.
And it happened all of a sudden. I could do yoga and in the middle of the practice lie on the floor with a rapid heartbeat due to sudden unreasonable anxiety or suddenly cry. It feels like a sudden wave: it covers your head, you can’t run away from it anywhere.
About two months have passed since the end of taking the pills. I tried to cope with anxiety non-drug - meditation, dynamic relaxation according to Jacobson, freewriting about experiences. It did not help. The prices for therapy at that moment rose again, and I needed, if not psychotherapy, then definitely crutches in the form of pills.
/shizofreniya/
How much does it cost to support a relative with a mental disorder? To do this, I found the address of the district PND in the issuance of a search engine, called the registry office and found out what was needed for admission. Everything turned out to be simple:
- You need to come to the PND, apply to the reception. There, give your passport, policy and SNILS, give the actual address of residence. At the reception, they will issue a card and call the office number.
- People go to the office in a queue. Each section has its own psychiatrist. You cannot sign up for a specific time, as it happens in a regular clinic.
 It is better to come early, then you will get there faster. Arriving 15-20 minutes before the doctor started the appointment, on average I was third or fourth in line.
It is better to come early, then you will get there faster. Arriving 15-20 minutes before the doctor started the appointment, on average I was third or fourth in line.
At the appointment, the psychiatrist asked what was bothering me. I told my story, he offered me several antidepressants to choose from, talking about the pros and cons of each. He also prescribed a tranquilizer to remove the primary side effects.
The antidepressant was from the same group as the first time, but different. The packaging cost me 800 R, in total I bought two of them. I was told to come back in three or four weeks. This is necessary to understand whether the medicine suits me or not, whether the dosage needs to be adjusted. The diagnosis remained the same - generalized anxiety disorder.
A month later I came back to PND. At that moment, another doctor saw me, because my district police officer fell ill. During my visit to the dispensary, I talked with four different psychiatrists - and I had no problems with any of them. No one humiliated me, everyone spoke politely and professionally, they really tried to help.
No one humiliated me, everyone spoke politely and professionally, they really tried to help.
The pills did not help me this time, so the psychiatrist suggested trying to be treated in a hospital. With a residence permit in St. Petersburg, I could be hospitalized in a neurosis clinic. However, there was no registration, so they could only offer me a day hospital at the hospital named after. Kashchenko.
You can get to the hospital only by direction from the PND. The doctor appoints a day, issues a referral with which you need to come to the hospital. They make a card there, and then send it to the primary appointment with the doctor.
/spravka/
How to get a certificate from the PND
Treatment in a hospital according to compulsory medical insurance
In total, I was treated in a day hospital twice. I don't have a single negative memory associated with it, I liked this place, I liked the people there.
Treatment is quite simple. After an initial conversation with a psychiatrist, medications are selected. You also need to consult with a clinical psychologist, make a cardiogram, if necessary, visit other doctors - for example, a cardiologist or endocrinologist. This can be done either in the hospital itself, or in the clinic in the direction.
After an initial conversation with a psychiatrist, medications are selected. You also need to consult with a clinical psychologist, make a cardiogram, if necessary, visit other doctors - for example, a cardiologist or endocrinologist. This can be done either in the hospital itself, or in the clinic in the direction.
Clinical psychologist gives tests for attentiveness and memory. Together with him, we also filled out several questionnaires - for the level of anxiety and the presence of depression.
Community 11/23/21
What is depression?
There is a psychotherapist in the hospital, and a psychiatrist also makes appointments with him. Usually these are one-hour sessions once or twice a week. You can also go to a theater or art studio, to bibliotherapy, dance therapy, adaptive yoga. All this is free.
Studio teachers really want to help patients. People in the hospital are different, with different diseases, different states of mind, but it was very comfortable to work with everyone.
| Neat and pleasant day care unit | In the head nurse's office, before admission, you need to fill out documents with basic information: height, weight, pressure, place of work. For the duration of treatment, they give sick leave, if necessary |
| The day hospital has a small ward with beds. There are patients who are put on drips. And I was lying down there after taking blood - I always do not tolerate the procedure | There were many flowers in the hospital. I then became interested in plants, so this mini-garden was very pleasing |
 There were a lot of flowers in the hospital. I then became interested in plants, so this mini-garden made me very happy. The hospital is located in the city center, not far from Sennaya Square. During the pandemic, I went there by taxi and returned on foot. I called it a “healing walk” because it helped me get distracted
There were a lot of flowers in the hospital. I then became interested in plants, so this mini-garden made me very happy. The hospital is located in the city center, not far from Sennaya Square. During the pandemic, I went there by taxi and returned on foot. I called it a “healing walk” because it helped me get distracted I went to psychotherapy twice a week, every other day I went to the psychiatrist. I wanted to go to yoga several times, but it was early in the morning, I woke up every time.
The way psychotherapy sessions go depends on the methodology that the therapist uses. I wanted to do cognitive behavioral therapy, one of the techniques supported by evidence-based medicine. This was not the case at the hospital, but my doctor offered to help me find a good private therapist working in this direction if I wanted to.
Tablets prescribed by a doctor were distributed by nurses in a special room. You need to go to the hospital often - at first every day, then every other day, at the end at least twice a week. The drugs are given in the amount they are needed for the time while the patient is not in the hospital. The nurses are sympathetic and sweet, they call everyone by diminutive names, they remember them in just a couple of days.
The drugs are given in the amount they are needed for the time while the patient is not in the hospital. The nurses are sympathetic and sweet, they call everyone by diminutive names, they remember them in just a couple of days.
In the hospital they provide food, you can have breakfast and lunch. The food is ordinary hospital food, but I liked it: I love simple food, especially all sorts of stews.
/bye-depression/
“It was like a strict regime sanatorium”: how much I spent on treating depression
During the pandemic, consultations with psychotherapists were moved to Skype, and visits to a psychiatrist were once or twice a week, sometimes more, depending on the state.
Due to frequent visits, any changes in the condition are easily monitored and the dosage of drugs is quickly adjusted. For example, once I was unsuccessfully prescribed a drug. The next day, I told about it at the meeting - and it was canceled for me.
Treatment in the hospital continues until a stable condition is reached. For example, in my case it was the disappearance of constant anxiety for at least a few weeks.
Both times I left the hospital myself because I got tired of visiting it so often. But before that, the doctors selected a treatment for me, and it worked. I had to try several schemes. As a result, we came to my very first medicine, only at a dosage 2.5 times higher. I still take it.
My experience only describes a particular hospital. The system of psychiatry in Russia is imperfect, it is difficult, but possible, to find a competent doctor for CHI. The biggest problem in this situation is not to run into a specialist who will only make things worse. However, incompetent specialists are also found in the commercial system.
Even then, I began to actively buy books about anxiety and mental disorders. It helped keep me going
It helped keep me going How I currently live with Generalized Anxiety Disorder
I am still undergoing compulsory medical insurance. It will soon be a year since I follow the latest version of the therapeutic regimen. Once every three or four months I go to a paid psychologist, a consultation costs 3500 R, but now I don’t need regular therapy.
Increased anxiety is still in my life, but it does not immobilize me, does not deprive me of freedom. I still have problems sleeping, and the crowd is filled with terrible anxiety and lack of air. Mostly somatic manifestations remained: muscle tension in trigger situations, a feeling of lack of air and headaches if I am very nervous.
On the other hand, I learned a lot during the treatment period: talk about problems, look for solutions, work with anxiety, and even relax. Both psychotherapy and antidepressants helped me with this.
/psychotherapy-pros-cons/
Pros and cons: is it worth spending money on a psychotherapist
I spend 28,250 R per year on the treatment of anxiety disorder
| Spending | Cost | Total for the year |
|---|---|---|
| Psychotherapist appointment | From 3500 R per visit | 14 000 R |
| Antidepressants - pack of 100 tablets, enough for me for 40 days | 1200 R per pack | 10 950 Р |
| Antipsychotic - pack of 60 tablets, enough for me for 120 days | 1100 R per pack | 3300 R |
Psychotherapist appointment
Cost
From 3500 R per visit
Total for the year
14 000 R
Antidepressants - in a pack of 100 tablets, I have enough for 40 days
Cost
1200 r per pack
Total for the year
9000 10Neuroleptic - neuroleptic - In a pack of 60 tablets, I have enough for 120 days
Cost
1100 R per pack
Total for the year
3300 R
What helps me to work with anxiety
I will talk about books, applications and other things that are helped me before and help me now, but do not replace therapy and taking pills:
- Mental health diary application.
 It is built on the principles of cognitive behavioral therapy. Helps to recognize automatic thoughts and rationalize them, makes it possible to become more conscious. The application has a diary of automatic thoughts, where you can write daily what worries you. My favorite feature is the destruction of negativity, try it.
It is built on the principles of cognitive behavioral therapy. Helps to recognize automatic thoughts and rationalize them, makes it possible to become more conscious. The application has a diary of automatic thoughts, where you can write daily what worries you. My favorite feature is the destruction of negativity, try it. - Robert Leahy, "Freedom from Anxiety". A must have book for all anxious people. The author is a doctor of psychology, adheres to the methods of cognitive therapy. You can read in order, or you can only read the chapters of interest. It will not replace therapy, but it will help to understand where the anxiety manifestations come from, teach you how to work with the disorder.
- Forum "Mental Balance". As in any other forum, the audience there is different, so the information needs to be filtered. However, it was there that they supported me when I was very ill. Here you can also consult with psychiatrists, read useful articles and case histories of other people.

- TED Talks about psychological first aid and emotional hygiene.
- Lindsey K. Gibson, Adult Children of Emotionally Immature Parents. One of my favorite books that helped me understand and let go of my relationship with my father. The book has interactive tasks to help work through the questions.
- Muscle relaxation according to Jacobson. I like a particular video, but there are many options on the Internet.
- Application for meditation Insight Timer and meditation by Valery Veryaskin. I tried a thousand and one meditations, but only Valery's audio helps me relax and fall asleep in the evening. My favorite is The Practice of Relaxation.
Remember
- If you feel that anxiety interferes with your life, you should go to a psychiatrist. For self-examination, you can take the Beck test.
- It is better to ask for help - to the doctor, relatives, friends, people on the forum. Anxious thoughts are much easier to deal with if you speak them out.

- Taking antidepressants, antipsychotics and tranquilizers as prescribed by a doctor is normal and not a shame.
- You should definitely share your problems with those with whom you live. For people who are unfamiliar with mental disorders, many of the actions of anxious people will seem strange. In the most difficult moments, I slept for days, simply because anxiety takes a lot of strength. From the outside, it looks incomprehensible, and therefore it is worth talking about the problem.
- Anxiety is treated, after a while it will be possible to return to normal life.
Did you also have an illness that affected your lifestyle or attitude? Share your story.
Tell
Therapy of anxiety disorders: a modern view on the problem
Summary. The International Classification of Diseases-10 group of anxiety disorders includes generalized anxiety disorder, panic disorder, specific phobias, and social anxiety disorder (F40 and F41). Anxiety disorders are very common in the general population and occur in every 5th inhabitant of developed countries throughout life. One of the most difficult to treat in this group is Generalized Anxiety Disorder, characterized by excessive worrying about various events or activities, resulting in significant distress and disruption of social, work, and daily functioning. The use of antidepressants is ineffective in about ⅓ of these patients. In modern clinical guidelines, other groups of drugs are indicated in first and second line therapy - anticonvulsants, atypical antipsychotics. Among them, an important place is occupied by pregabalin, a drug of the anticonvulsant group, which is also used for chronic pain syndrome. The article considers the current state of the problem of treating anxiety disorders and (using pregabalin as an example) the feasibility of using alternative drugs to antidepressants.
Anxiety disorders are very common in the general population and occur in every 5th inhabitant of developed countries throughout life. One of the most difficult to treat in this group is Generalized Anxiety Disorder, characterized by excessive worrying about various events or activities, resulting in significant distress and disruption of social, work, and daily functioning. The use of antidepressants is ineffective in about ⅓ of these patients. In modern clinical guidelines, other groups of drugs are indicated in first and second line therapy - anticonvulsants, atypical antipsychotics. Among them, an important place is occupied by pregabalin, a drug of the anticonvulsant group, which is also used for chronic pain syndrome. The article considers the current state of the problem of treating anxiety disorders and (using pregabalin as an example) the feasibility of using alternative drugs to antidepressants.
Urgency
Anxiety disorders are among the most common mental health problems in the world. In addition, among all medical problems, anxiety also occupies a leading position in terms of prevalence. Within the framework of epidemiological studies, it is customary to talk about two variants of the prevalence of any condition - annual, that is, an assessment of this indicator in a small time slice (12-month prevalence), and lifelong - the proportion of people who have experienced this condition at least once. For the entire group of anxiety disorders, research has shown a 12-month prevalence of >15% and a lifetime prevalence of >20%.
In addition, among all medical problems, anxiety also occupies a leading position in terms of prevalence. Within the framework of epidemiological studies, it is customary to talk about two variants of the prevalence of any condition - annual, that is, an assessment of this indicator in a small time slice (12-month prevalence), and lifelong - the proportion of people who have experienced this condition at least once. For the entire group of anxiety disorders, research has shown a 12-month prevalence of >15% and a lifetime prevalence of >20%.
As a clear demonstration of the relevance of the problem, we present the results of a large-scale study on the assessment of the mental and somatic health of US residents "National Comorbidity Survey". Along with Framingham, this is one of the largest observational studies, the results of which are often used to evaluate epidemiological data and the relationship between various factors that affect health. According to him, the 12-month prevalence of anxiety disorders is 17. 2%, which means that every 6th person in the United States develops an anxiety disorder within one year. The lifetime prevalence is 24.9%; this means that every 4th person during his life at least once encounters an anxiety disorder (Kessler R.C. et al., 1994). These data are approximately the same for both Caucasians and African Americans. Thus, with a sufficiently high degree of accuracy, they can be extrapolated to the Ukrainian population.
2%, which means that every 6th person in the United States develops an anxiety disorder within one year. The lifetime prevalence is 24.9%; this means that every 4th person during his life at least once encounters an anxiety disorder (Kessler R.C. et al., 1994). These data are approximately the same for both Caucasians and African Americans. Thus, with a sufficiently high degree of accuracy, they can be extrapolated to the Ukrainian population.
Analysis of World Health Organization data suggests that this group of mental health problems is the 6th most common cause of disability in both high-income, middle- and low-income countries, including Ukraine. For every 100 thousand inhabitants of the Earth, anxiety disorders account for 390 years of disability. Among women, anxiety disorders are responsible for 65% of all years of life lost (disabled) from all causes (Baxter A.J. et al., 2014).
Among anxiety disorders, a special place is occupied by generalized anxiety disorder, which is characterized by excessive anxiety and feelings in relation to a large number of events or activities (for example, work), accompanied by severe anxiety, fatigue, irritability, difficulty concentrating, muscle tension and impaired sleep. This state of affairs leads to significant distress and difficulties in social, work or even normal daily functioning. For example, anxiety significantly complicates the performance of work duties, which can lead to job loss or provoke conflict in the family.
This state of affairs leads to significant distress and difficulties in social, work or even normal daily functioning. For example, anxiety significantly complicates the performance of work duties, which can lead to job loss or provoke conflict in the family.
The sleep disturbance that often accompanies anxiety can be a serious problem in itself, as anxiety-induced insomnia is usually long-term and thus poorly controlled by benzodiazepines or their derivatives, as they are not recommended for long-term use. Another serious problem that deserves attention is a significant decrease in the quality of life of patients with anxiety. Given the gradual transition to patient-centered care, it is also recommended to use this indicator as a marker of the severity of the condition, in addition to standard diagnostic measures (clinical scales for assessing anxiety).
Studies have shown that anxiety is associated with a significant reduction in quality of life, especially when taking into account the widely used SF-36 quality of life scale. To a greater extent, the deterioration relates to the psychological and some characteristics of the somatic component of the quality of life. Thus, anxiety is associated with a deterioration in indicators on such a somatic scale as pain intensity. This may be due to the fact that patients with anxiety are often diagnosed with conditions associated with pain, such as chronic tension headache, nonspecific back pain, and a number of others. As an example, let's cite the results of a large-scale multinational survey, which also included Ukraine. According to the data obtained in our country, chronic pain has been noted in 19 patients over the past 12 months..7% of patients with anxiety or depression (Tsang A. et al., 2008). Thus, every 5th patient with an anxiety disorder also needs therapy aimed at eliminating pain.
To a greater extent, the deterioration relates to the psychological and some characteristics of the somatic component of the quality of life. Thus, anxiety is associated with a deterioration in indicators on such a somatic scale as pain intensity. This may be due to the fact that patients with anxiety are often diagnosed with conditions associated with pain, such as chronic tension headache, nonspecific back pain, and a number of others. As an example, let's cite the results of a large-scale multinational survey, which also included Ukraine. According to the data obtained in our country, chronic pain has been noted in 19 patients over the past 12 months..7% of patients with anxiety or depression (Tsang A. et al., 2008). Thus, every 5th patient with an anxiety disorder also needs therapy aimed at eliminating pain.
Evidence-based therapy
A rational approach to patient care includes both an individualized approach, taking into account the characteristics of each individual case, and reliance on the existing evidence base, including clinical guidelines, meta-analyses and the results of recent randomized controlled clinical trials.
The National Institute for Health and Care Excellence (NICE), UK, is one of the well-known and leading providers of evidence-based clinical guidelines. In the latest guidelines on the quality standard of care for anxiety, a team of leading experts note that benzodiazepines and antipsychotics should be avoided in routine practice in patients with anxiety disorders (NICE, 2014). These recommendations are explained by the fact that taking the former is associated with the development of tolerance and dependence, and the latter with a relatively high risk of side effects. The authors recommend taking this into account, and if prescribed, then a short course in cases of exacerbation of symptoms, when other methods of treatment do not demonstrate sufficient effectiveness. Thus, antidepressants and/or cognitive-behavioral therapy are recommended as first-line therapy. For the pharmacological treatment of anxiety, in particular generalized anxiety disorder, NICE recommends selective serotonin reuptake inhibitors (SSRIs), selective serotonin and norepinephrine reuptake inhibitors (SNRIs), and pregabalin. The authors of the guidelines note that one should also be aware of the possible withdrawal syndrome when using SSRIs and SNRIs, especially paroxetine and venlafaxine.
The authors of the guidelines note that one should also be aware of the possible withdrawal syndrome when using SSRIs and SNRIs, especially paroxetine and venlafaxine.
The American Academy of Family Physicians (AAFP) and the American Psychiatric Association (APA) are other well-known organizations that compile guidelines for the treatment of mental disorders and offer the same psychological and pharmacological treatments. We are talking, in particular, about the guidelines for the diagnosis and management of generalized anxiety and panic disorder (AAFP, 2015) and the APA clinical guidelines (2009) only for panic disorder, which practically duplicate the above, however, the regimens for prescribing drugs and psychological methods of treatment are prescribed in more detail. The list of recommended drugs is presented in the table.
Table AAFP recommended drugs for first and second line therapy
for generalized and panic disorder
| Drug | Recommendations |
|---|---|
| SSRI | |
| Escitalopram | Generalized anxiety disorder, panic disorder |
| Fluvoxamine | Panic disorder |
| Fluoxetine | Generalized anxiety disorder, panic disorder |
| Paroxetine | Generalized anxiety disorder, panic disorder |
| Sertraline | Generalized anxiety disorder, panic disorder |
| SNRI | |
| Duloxetine | Generalized anxiety disorder |
| Venlafaxine | Generalized anxiety disorder, panic disorder |
| Azaperone | |
| Buspirone | Generalized anxiety disorder |
| Tricyclic antidepressants | |
| Amitriptyline | Generalized anxiety disorder, panic disorder |
| Imipramine | Generalized anxiety disorder, panic disorder |
| Nortriptyline | Generalized anxiety disorder, panic disorder |
| Antiepileptic drugs | |
| Pregabalin | Generalized anxiety disorder |
| Antipsychotics | |
| Quetiapine | Generalized Anxiety Disorder |
In addition to the medical communities of Great Britain and the USA, we also note the World Federation of Biological Psychiatry, which brings together specialists from different countries. In 2012, based on a review of the evidence base, this organization also published clinical guidelines for the treatment of anxiety disorders. The authors separately identified for panic, generalized disorder and social anxiety drugs included in first-line therapy:
In 2012, based on a review of the evidence base, this organization also published clinical guidelines for the treatment of anxiety disorders. The authors separately identified for panic, generalized disorder and social anxiety drugs included in first-line therapy:
- for social anxiety: escitalopram, fluvoxamine, paroxetine, sertraline, venlafaxine;
- for panic disorder: same drugs + citalopram and fluoxetine;
- for generalized disorder: escitalopram, paroxetine, sertraline, venlafaxine, quetiapine, and pregabalin.
Particular attention in this list should be given to pregabalin, which belongs to the group of antiepileptic drugs. It should be noted that for a long time in the medical and pharmacological communities there has been a discussion of changing the existing approach to the classification of psychotropic drugs. Often the name of a group of drugs, such as antidepressants, antipsychotics (neuroleptics), or anticonvulsants (antiepileptic drugs), does not correspond to the diagnosis for which they are prescribed. So, antidepressants can be prescribed for anxiety, bulimia; antipsychotics - for anxiety, depression; anticonvulsants - for the same anxiety or bipolar affective disorder. Assigning a prescribed drug to any of these groups often confuses patients, which can be a cause for additional concern or reduced compliance. Discussion of the transition from the old classification model based on symptoms to the new one was one of the main topics of one of the largest annual world conferences on psychiatry and psychopharmacology "ECNP Congress" in 2014, 2015 and 2016, and it is possible that in the near future this new model will be implemented.
So, antidepressants can be prescribed for anxiety, bulimia; antipsychotics - for anxiety, depression; anticonvulsants - for the same anxiety or bipolar affective disorder. Assigning a prescribed drug to any of these groups often confuses patients, which can be a cause for additional concern or reduced compliance. Discussion of the transition from the old classification model based on symptoms to the new one was one of the main topics of one of the largest annual world conferences on psychiatry and psychopharmacology "ECNP Congress" in 2014, 2015 and 2016, and it is possible that in the near future this new model will be implemented.
Pregabalin differs in its chemical structure and mechanism of action from SSRIs and SNRIs, while remaining highly effective in generalized anxiety disorder, as evidenced by its inclusion as first-line therapy in various management guidelines for these patients. Pregabalin is a γ-aminobutyric acid derivative and was originally used and approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of epilepsy and various types of chronic pain syndrome, including diabetic peripheral neuropathy, postherpetic neuralgia, and fibromyalgia. Later evidence began to emerge for its effectiveness in anxiety disorders, especially generalized anxiety disorder and, to a lesser extent, social phobia.
Later evidence began to emerge for its effectiveness in anxiety disorders, especially generalized anxiety disorder and, to a lesser extent, social phobia.
Recently, this drug has increasingly become the subject of study specifically in the context of anxiety treatment as an alternative to SSRIs. The problem of the widespread use of the latter is mainly due to the relatively slow onset of action, the risk of withdrawal syndrome and the lack of a significant effect in relation to such often comorbid conditions as chronic pain syndrome of various origins. In addition, in about ⅓ of patients, the use of SSRIs and SNRIs does not lead to the desired effect and there is a need to look for another therapy with a different mechanism of action.
This was reflected in a systematic review of scientific studies conducted by the staff of the Villa San Benedetto Menni clinics in Rome, Maastricht University and the University of Miami. Summarizing the available evidence base for all drugs used in anxiety disorders, the researchers concluded that pregabalin is highly effective in generalized anxiety disorder. At the same time, as the authors note, the drug showed a low risk of adverse effects with long-term use and did not have a negative effect on cognitive or psychomotor functioning (Perna G. et al., 2016).
At the same time, as the authors note, the drug showed a low risk of adverse effects with long-term use and did not have a negative effect on cognitive or psychomotor functioning (Perna G. et al., 2016).
Also published this year are the results of an analysis of several randomized clinical trials that evaluated the effectiveness of pregabalin in the context of pain reduction and improvement in various areas of functioning. The authors note that taking pregabalin led to a significant reduction in pain, improved sleep quality and physical functioning. The analysis also assessed symptoms of anxiety and depression using the Hospital Anxiety and Depression Scale (HADS). On the one hand, no significant differences were found with the control group (placebo), on the other hand, the study sample consisted of individuals with a low initial level of anxiety and depression, which did not reach the level of clinical significance (6 points each on the HADS anxiety and depression subscales at the threshold level ≥8 points and clinically significant ≥11 points) (Sadosky A. et al., 2016).
et al., 2016).
The problem of anxiety is also relevant for patients undergoing surgical treatment. This disorder often accompanies these patients both in the pre- and postoperative period. In addition, anxiety about the upcoming operation and pain has a negative effect on surgery and anesthesia. A new clinical trial conducted in 2016 demonstrated the effectiveness of pregabalin adjunctive therapy for bone surgery. In this study, patients of the experimental group were premedicated with pregabalin in different dosages before blockade of peripheral nerves. The control group did not receive any additional therapy. According to the results, the use of pregabalin significantly contributed to the maintenance of hemodynamic parameters during the intervention at a normal level and greater patient satisfaction with the quality of anesthesia. When using pregabalin at a dose of 150 and 300 mg, a significantly shorter duration of surgical intervention was also noted compared with the control (76. 5; 68.0 and 83.3 minutes, respectively).
5; 68.0 and 83.3 minutes, respectively).
Conclusions
Anxiety disorders are a common problem of our time, one of the main characteristics of which is a high comorbidity with both somatic and other mental disorders. The gradual discovery of new drugs and the study of additional properties of already long-term use has replaced benzodiazepines from the first-line therapy recommended in current guidelines for patients with anxiety disorders. Highly effective drugs are not limited to the SSRI and SNRI group; Today, there are other effective medicines classified as anticonvulsants and atypical antipsychotics. In particular, the study of the additional properties of pregabalin has demonstrated its high efficacy in generalized anxiety disorder, which is reflected in the most significant clinical guidelines and recommendations of the European Medical Agency. Experts conclude that pregabalin can be used as a first-line therapy for this disorder, and it may also be the best pharmacological alternative to SSRIs when they are ineffective or poorly tolerated.