Low self esteem mental illness
Low Self-Esteem and Its Association With Anxiety, Depression, and Suicidal Ideation in Vietnamese Secondary School Students: A Cross-Sectional Study
Introduction
It is well recognised that adolescence is one of the most rapid phases of human development (1). It is characterised by a rapid physical, social, and cognitive growth, as well as changes in self-esteem. Self-esteem is reported to have a significant impact on important life outcomes including health and social outcomes during adolescence and adulthood. For example, there is a clear connection between higher self-esteem and positive outcomes, such as occupational success, better social relationships, a sense of well-being, and positive perceptions by peers, academic achievement, and good coping skills (2, 3). Low self-esteem is causally related to depression, substance abuse, antisocial behaviour, and suicide (4–6). The literature demonstrates that social functioning, such as acceptance by peers, is lower in children with low self-esteem (7).
Extensive research has explored risk and protective factors related to low self-esteem development during adolescence. Reported risk factors include being a girl (6, 8, 9), the family’s low socioeconomic status (10), parents’ education level, family eligibility for public assistance, eligibility for free or reduced-cost school meals, the parents’ employment status (11), and school performance and grades (6, 12), as well as obesity (13).
Academic achievement is known to be affected by self-esteem, while self-esteem may also influence academic achievement (7). High self-esteem is reported as an important predictive factor for students’ academic achievement (14). Another study found that while high self-esteem resulted in many positive outcomes and benefits, it did not necessarily lead to good school performance (15). On the other hand, adolescents with poor academic results did not always have low general self-esteem (16).
There is an association between low self-esteem and negative outcomes for young people’s behavioural and mental health problems, including health-compromising behaviours such as substance abuse, early sexual activity, and eating problems (17). A longitudinal study among a large sample of young New Zealanders found, however, that while low self-esteem significantly predicted adolescent eating and other health-compromising behaviours, it was not related to substance abuse and early sexual activity (18). With regard to mental health, a correlation has been detected between low self-esteem and depression (19, 20), anxiety (10, 21), and adolescents’ suicidal ideation and attempts (18, 22).
A longitudinal study among a large sample of young New Zealanders found, however, that while low self-esteem significantly predicted adolescent eating and other health-compromising behaviours, it was not related to substance abuse and early sexual activity (18). With regard to mental health, a correlation has been detected between low self-esteem and depression (19, 20), anxiety (10, 21), and adolescents’ suicidal ideation and attempts (18, 22).
Reports during the past few years indicate that there is a strong relationship between academic pressure and stress, depression, anxiety, low self-esteem, and suicidal ideation among students in secondary or high school and in young adults (23–25). A study describing perceptions about mental illness in Hue in Vietnam noted that “studying or thinking too much” is a cause of mental health problems (26). In Vietnamese culture, the pressure from parents and schools might be expected to have an unintended effect, leading to lower self-esteem and associated outcomes seen elsewhere among high school students. There are as yet no reports of systematic studies on this issue in Vietnam, and there are few reports of descriptive or analytical research into adolescent self-esteem.
There are as yet no reports of systematic studies on this issue in Vietnam, and there are few reports of descriptive or analytical research into adolescent self-esteem.
This is particularly relevant since we found high levels of depression, anxiety, and suicidal ideation among secondary school students in Vietnam [Nguyen, D. T., Dedding, C., Pham, T. T., Wright, P., & Bunders, J. (25)]. This article reports on a study that aimed to determine (1) the prevalence of low self-esteem; (2) the characteristics associated with low self-esteem; and (3) the relationships among self-esteem and anxiety, depression, educational stress, and suicidal ideation in secondary school students. We hypothesised that low self-esteem would be associated with a greater risk of poor mental health status.
Materials and Methods
Study Design and Participants
A cross-sectional study design was used to recruit 1,260 students at three secondary schools in urban and suburban areas in Cantho City in Vietnam. All data were collected during the first academic semester, from September to December 2011. A more detailed description of the sampling and its participants can be found elsewhere (25).
All data were collected during the first academic semester, from September to December 2011. A more detailed description of the sampling and its participants can be found elsewhere (25).
Measures
All participants were invited to provide information by self-reporting using a questionnaire. This was done after class or at home anonymously to minimise potential reporting bias and to keep information confidential. The detailed components of the questionnaire have been described elsewhere (25).
The 10-item Rosenberg Self-esteem Scale (21, 27) was used to assess global self-esteem, with higher scores indicating more positive self-regard. Each item asked for response using a 4-point Likert scale ranging from 1 (strongly agree) to 4 (strongly disagree). The scale is generally reliable, with test–retest correlations value between 0.82 and 0.88 (21). The Cronbach α of the scale in the present study was 0.77. The scale ranges from 0 to 30: a score greater than 25 suggests high self-esteem; scores between 15 and 25 are considered to be within normal range, whereas scores less than 15 suggest low self-esteem (Morris Rosenberg).
A more detailed method description on employing the Center for Epidemiology Studies Depression (CES-D), the anxiety scale, and the Educational Stress Scale for Adolescents for this study is available (25).
To address the issue of suicidal ideation, additional questions on whether the student had ever seriously considered suicide or made a suicide plan used a 3-point scale (never, sometimes, and often). A yes/no question was also used to identify students who had attempted suicide.
To define risks and protective factors, we explore the variables listed in Table 1, including mother’s education, physical and emotional abuse by parents or other adults in the household or school, academic performance in the last semester, educational stress, attendance at a supplementary class, and use of personal tutor. The data collected using the questionnaire is available in the Supplementary Data File.
Table 1 Frequencies and percentages (%) of sociodemographic variables of participants by self-esteem status.
Data Analysis
Demographic data were analysed descriptively to determine basic characteristics of the sample population and presented as means ± standard deviations (SD). The χ2 test was used to assess the significance of differences in the distribution of participants by selected sociodemographic characteristics, risk factors, and outcome variables. Associations between low self-esteem and family characteristics, educational stress, and academic achievement were explored by logistic regression analysis. Univariate independent predictors of low self-esteem with p < 0.10 were entered in a multivariate logistic regression model, and the backward Wald method was applied to study their influence on the presence of low self-esteem. Univariate logistical analyses were also applied to determine the relationships among low self-esteem and anxiety, depression, and suicidal ideation, and Pearson correlation coefficients were used to measure the correlations among these. All analyses were carried out using a significance level of 5%, and all tests were 2-sided. The 95% confidence intervals (CIs) of odds ratios (ORs) were also calculated. All analyses were analysed by using SPSS Inc, Chicago, the United States of America version 16.0.
All analyses were carried out using a significance level of 5%, and all tests were 2-sided. The 95% confidence intervals (CIs) of odds ratios (ORs) were also calculated. All analyses were analysed by using SPSS Inc, Chicago, the United States of America version 16.0.
Results
Demographics
Of the 1,260 students invited to participate, 111 (7.3%) were excluded from analysis because they did not adequately complete the questionnaire; for example, they did not provide answers to five or more items in the CES-D. The final sample comprised 1,149 senior high school students with a mean age of 16.1 years. Participating students were fairly evenly distributed in terms of sex: 36.5% males and 63.5% females (Table 1). This proportion also reflects the proportion of males and females enrolled in the classes studied. Students’ participation from each grade (10–12) did not significantly differ, at around 33% each. Ninety-five percent of students were ethnically Kinh; other ethnic groups included Hoa and Khmer. This sample was in line with the school population in this area.
This sample was in line with the school population in this area.
Prevalence of Low Self-Esteem and Characteristics Associated With Self-Esteem
The mean self-esteem score was 17.56 on a scale of 0 to 30. The scores for boys and girls were similar (17.83 vs. 17.40; t = 1.720; p = 0.086). Based on all scores, nearly a fifth (19.4%) of the respondents reported low self-esteem according to Rosenberg’s criteria, with scores below 15 (Table 1). Based on univariate logistic regression analysis, among six investigated variables, two variables “having a personal tutor” and “attendance at supplementary class” were negatively associated with the risk of low self-esteem, while the other variables were positively correlated to low self-esteem (Table 2). Students were likely to show lower self-esteem, when their mother’s education was at primary level or below, when they were often physically or emotionally abused at home or at school, when they had below average/very poor academic performance in the last semester, or when they reported experiencing high educational stress.
Table 2 Factors associated with low self-esteem: multivariate logistic regression analyses.
In the multivariate regression analysis (with the backward Wald method), not accounting for effect modification, four variables remained correlated to low self-esteem, either in a negative or positive direction. Having a personal tutor and academic performance in the last semester were no longer a significant association, but attending supplementary classes still remained a protective factor for low self-esteem (reduced OR of 43% compared with students not attending) (Table 2).Study results that were considerably positively associated to low self-esteem were medium and high educational stress (ORs = 2.25 and 4.02, respectively).
Relationships Between Self-Esteem and Anxiety, Depression, and Educational Stress, and Suicidal Ideation
As shown in Table 3, four variables—self-esteem, anxiety, depression, and educational stress—were related to each other. Self-esteem was negatively correlated to anxiety, depression, and educational stress, while educational stress was positively correlated to anxiety and depression.
Table 3 Pearson correlations between self-esteem, anxiety, depression, and educational stress.
One of the purposes of the study was to identify the impact of self-esteem on mental health problems. The results of univariate logistics indicate that low self-esteem contributed significantly to anxiety, depression, and suicide among adolescents. Compared to students who reported normal self-esteem, the students who reported low self-esteem had twice the odds of having anxiety symptoms [20.3% (187/921) vs. 34.2% (76/222)] (OR = 2.04; 95% CI OR = 1.48–2.82,
p < 0.001), nearly six times the odds of being at risk of depression (CES-D score of ≥16) (74.0% vs. 33.2%), (OR = 5.72; 95% CI OR = 4.11–7.59), four times the odds of having depressive symptoms (CES-D scores of > 21) (50.7% vs. 19.8%) (OR = 4.16; 95% CI OR = 3.06–5.66), and nearly five times the odds of having depression (CES-D score of > 25) (41.7% vs. 13.0%), (OR = 4.79; 95% CI OR = 3.45 – 6. 65). Students with low self-esteem also were significantly more likely to have considered or attempted suicide (Table 4).
65). Students with low self-esteem also were significantly more likely to have considered or attempted suicide (Table 4).
Table 4 Associations between self-esteem and suicidal ideation.
Discussion
We investigated the prevalence of low self-esteem among secondary school students, the characteristics associated with low self-esteem, and the relationships among self-esteem and anxiety, depression, and suicide. Nearly 20% of the students had low self-esteem, with no difference between girls and boys. These results are in line with some previous studies (12, 28), but inconsistent with others (6, 12). Cultural and social differences in the study populations could explain some of the differences.
Reasons for Having a Higher Prevalence of Low Self-Esteem Among Females
The results of this study cannot provide precise reasons for the higher prevalence of lower self-esteem among females; however, a number of possible causes for the gender differences are worth discussing. Although gender equality has improved in recent years in Vietnam and is clearly legislated, gender issues within the family and society remain a challenge for most Vietnamese, who are strongly influenced by traditional culture and custom (29). There is an association between female gender and emotionally unstable personality (30, 31). As a result, women are more prone to develop emotionally unstable personality (e.g. borderline personality) (32). Thus, females’ self-esteem may be more likely to fluctuate, depending on how they themselves or others, especially their parents, evaluate their achievements.
Although gender equality has improved in recent years in Vietnam and is clearly legislated, gender issues within the family and society remain a challenge for most Vietnamese, who are strongly influenced by traditional culture and custom (29). There is an association between female gender and emotionally unstable personality (30, 31). As a result, women are more prone to develop emotionally unstable personality (e.g. borderline personality) (32). Thus, females’ self-esteem may be more likely to fluctuate, depending on how they themselves or others, especially their parents, evaluate their achievements.
A high prevalence of low self-esteem among the secondary school students should be considered as an important mental health problem not only by parents, school teachers, and principals but also by policy makers in the education and health sectors in Vietnam. In fact, health care related to psychological disorders has not received adequate consideration yet in Vietnam (33). Therefore, it is important to take mental health care into account when developing a policy framework to improve general school health services, such as directive no. 23/2006/CT-TTg on having well-equipped and professionally qualified health officers in schools (34), and Decision No. 401/2009/QD-TTg, which approved the program “Preventing and combatting diseases in educational establishments belonging to the national education system” (35).
23/2006/CT-TTg on having well-equipped and professionally qualified health officers in schools (34), and Decision No. 401/2009/QD-TTg, which approved the program “Preventing and combatting diseases in educational establishments belonging to the national education system” (35).
Our results confirm the findings of previous studies (6, 10, 25, 36), namely, that family characteristics, including mother’s low educational level and physical and emotional abuse by parents or other adults in the household, were associated with low levels of self-esteem. In addition, educational characteristics such as the school environment, academic performance, and high educational stress were strongly associated with self-esteem. These findings are consistent with results of other studies, for example, by Pullmann & Allik (16), which found that parents have a great deal of influence on their children’s psychological development, including on the relationships outside the family environment (6, 10). Students who attended one or more supplementary classes appeared to be at lower risk of having poor self-esteem. In Vietnam, these students are usually from a family with a higher socioeconomic status. Attending supplementary class may reduce the stress of workload and academic pressure for those students. It would be useful to confirm this with further studies in the Vietnamese context, but this kind of support is unlikely to be available to families who cannot pay for it.
Students who attended one or more supplementary classes appeared to be at lower risk of having poor self-esteem. In Vietnam, these students are usually from a family with a higher socioeconomic status. Attending supplementary class may reduce the stress of workload and academic pressure for those students. It would be useful to confirm this with further studies in the Vietnamese context, but this kind of support is unlikely to be available to families who cannot pay for it.
Low self-esteem in the adolescents in Cantho City was associated with poor academic performance. Aryana (14) reported that high self-esteem among preuniversity students was an important factor in predicting high academic achievement. Our finding also highlights that self-esteem plays an important role in predicting academic achievement, although a cross-sectional study design is unable to demonstrate causality; a prospective study to identify causality of the low self-esteem would be appropriate in future research.
With regard to mental health, the results of Pearson correlation analysis showed that self-esteem was negatively correlated to anxiety, depression, and educational stress, while the results of univariate logistic regression illustrated that low self-esteem contributed to a high risk of anxiety, depression, and suicidal ideation. These results are comparable to others showing that low self-esteem was associated with depression (19, 20, 37) and identifying a relationship between self-esteem and anxiety (10, 21), as well as a relationship between low self-esteem and suicidal ideation and suicide attempts among adolescents (18, 22). Screening for low self-esteem in adolescents is a possible strategy to help identify secondary school students at risk of anxiety, depression, and suicide. In addition, our previous study (25) showed an association between mental health problems and academic pressure, resulting from an overloaded curriculum and pressure from teachers and parents to succeed. There is clearly a need to reduce mental health problems among today’s secondary school students in Vietnam. The development of a website to provide psychoeducation designed to meet the needs of young Vietnamese and of school-based counselling services for students, possibly by collaborating with volunteers from the Youth Union, the largest sociopolitical Vietnamese youth organization, at local universities, teachers, and parents, will be explored as one of the solutions (36). Around 66.3% of young Vietnamese downloaded the mobile health applications for disease prevention (38). Nevertheless, one of the challenges to using a digital health intervention is that young Vietnamese with a higher perceived stress level were significantly less likely to use such interventions (39).
There is clearly a need to reduce mental health problems among today’s secondary school students in Vietnam. The development of a website to provide psychoeducation designed to meet the needs of young Vietnamese and of school-based counselling services for students, possibly by collaborating with volunteers from the Youth Union, the largest sociopolitical Vietnamese youth organization, at local universities, teachers, and parents, will be explored as one of the solutions (36). Around 66.3% of young Vietnamese downloaded the mobile health applications for disease prevention (38). Nevertheless, one of the challenges to using a digital health intervention is that young Vietnamese with a higher perceived stress level were significantly less likely to use such interventions (39).
Study Limitations
One limitation of this study relates to the sample and its generalizability. Although the distribution of girls and boys reflected the true/current situation in the classes selected, the sample was from only three schools in urban and suburban Cantho. Another limitation concerns the study design, which specified collection of data from adolescents by self-reporting using standardised questionnaires. The respondents’ personality and identity development are still incomplete, which could result in fluctuating self-perceptions (9) and thus unreliable reporting. Also, the exploration of potential causes of low self-esteem as self-reported by subjects was not included in the survey. Another limitation is that the cross-sectional study design does not permit detection of links between covariates; longitudinal studies on this topic are still needed. Finally, the self-esteem, anxiety, and CES-D scales, like other screening instruments, cannot be viewed as diagnostic tools, but only as screening tests to identify members of groups at risk for these conditions. The results tell us how the students perceive their health but are not in themselves evidence of medical concerns. Moreover, there is no assessment of stress coping and stress levels, obesity (40), and chronic medical illness (e.
Another limitation concerns the study design, which specified collection of data from adolescents by self-reporting using standardised questionnaires. The respondents’ personality and identity development are still incomplete, which could result in fluctuating self-perceptions (9) and thus unreliable reporting. Also, the exploration of potential causes of low self-esteem as self-reported by subjects was not included in the survey. Another limitation is that the cross-sectional study design does not permit detection of links between covariates; longitudinal studies on this topic are still needed. Finally, the self-esteem, anxiety, and CES-D scales, like other screening instruments, cannot be viewed as diagnostic tools, but only as screening tests to identify members of groups at risk for these conditions. The results tell us how the students perceive their health but are not in themselves evidence of medical concerns. Moreover, there is no assessment of stress coping and stress levels, obesity (40), and chronic medical illness (e. g. asthma) (41), which may confound and influence anxiety, depression, and suicidal ideations. Finally, in a cross-sectional study, the cause–effect relationship cannot be measured; that requires a longitudinal cohort or a randomised controlled study.
g. asthma) (41), which may confound and influence anxiety, depression, and suicidal ideations. Finally, in a cross-sectional study, the cause–effect relationship cannot be measured; that requires a longitudinal cohort or a randomised controlled study.
Conclusions
Our research suggested that self-esteem is correlated to anxiety, depression, and academic stress, which significantly affects students’ quality of life and is linked to suicidal ideation. The results therefore suggest the need for a school-based or web-based provision of information or services aimed at proactively increasing students’ self-esteem and skills for dealing with academic stress.
Ethics Statement
The study was approved by the Scientific and Training Committees of Cantho University of Medicine and Pharmacy. Written informed consent for participation was obtained from students’ parents or legal guardians before data collection.
Author Contributions
A first draft of the manuscript was prepared by DN under the guidance of CD. All authors contributed to the final manuscript version. DN, JB, and CD jointly generated the research idea and the study design. DN, CD, TP, and EW contributed to the survey tools. DN and TP coordinated the surveys and data collection in the field. DN, TP, CD, and EW carried out data analysis.
All authors contributed to the final manuscript version. DN, JB, and CD jointly generated the research idea and the study design. DN, CD, TP, and EW contributed to the survey tools. DN and TP coordinated the surveys and data collection in the field. DN, TP, CD, and EW carried out data analysis.
Funding
The study has been supported by a scholarship from the “Strengthening teaching and research capacity of preventive medicine staffs to meet the challenges of emerging infections and new environmental hazards to health” Project, collaboration between Hanoi University, NUFFIC, and the Dutch Government.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Special thanks to all the students who participated in the study. We would also like to thank Hanoi University of Medicine and Cantho University of Medicine and Pharmacy as the Coordinating Board of the project in Vietnam and Professor Pham Van Linh, Rector of Cantho University of Medicine and Pharmacy, for their kind support for this work. Our appreciation also goes to Professor Wim Brandsma and Professor Wim van Brakel for their kind advice on the data analysis.
Our appreciation also goes to Professor Wim Brandsma and Professor Wim van Brakel for their kind advice on the data analysis.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00698/full#supplementary-material
References
1. World Health Organization. Maternal, newborn, child and adolescent health: adolescent development. Retrieved 29/07, 2019, from https://www.who.int/maternal_child_adolescent/topics/adolescence/development/en/.
Google Scholar
2. Boden JM, Fergusson DM, Horwood LJ. Does adolescent self-esteem predict later life outcomes? A test of the causal role of self-esteem. Dev Psychopathol (2008) 20(1):319–39. doi: 10.1017/S0954579408000151
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Trzesniewski KH, Donnellan MB, Robins RW. Stability of self-esteem across the life span. J Pers Soc Psychol (2003) 84(1):205–20. doi: 10.1037//0022-3514.84.1.205
doi: 10.1037//0022-3514.84.1.205
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Choo CC, Harris KM, Chew PKH, Ho RC. What predicts medical lethality of suicide attempts in Asian youths? Asian J Psychiatr (2017) 29: 136–41. doi: 10.1016/j.ajp.2017.05.008
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Crocker J, Wolfe CT. Contingencies of self-worth. Psychol Rev (2001) 108(3):593–623. doi: 10.1037//0033-295X.108.3.593
PubMed Abstract | CrossRef Full Text | Google Scholar
6. McClure AC, Tanski SE, Kingsbury J, Gerrard M, Sargent JD. Characteristics associated with low self-esteem among US adolescents. Acad Pediatr (2010) 10:238–44. doi: 10.1016/j.acap.2010.03.007
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Bos AER, Muris P, Mulkens S, Schaalma HP. Changing self-esteem in children and adolescents: a roadmap for future interventions. Netherlands J Psychol (2006) 62:26–33. doi: 10. 1007/BF03061048
1007/BF03061048
CrossRef Full Text | Google Scholar
8. Kling KC, Hyde JS, Showers CJ, Buswell BN. Gender differences in self-esteem: a meta-analysis. Psychol Bull (1999) 125(4):470–500. doi: 10.1037//0033-2909.125.4.470
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Schraml K, Perski A, Grossi G, Simonsson-Sarnecki M. Stress symptoms among adolescents: the role of subjective psychosocial conditions, lifestyle, and self-esteem. J Adolesc (2011) 34:987–96. doi: 10.1016/j.adolescence.2010.11.010
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Veselska Z, Geckova AM, Gajdosova B, Orosova O, Dijk JPV, Reijneveld SA. Socio-economic differences in self-esteem of adolescents influenced by personality, mental health and social support. Eur J Public Health (2009) 20(6):647–52. doi: 10.1093/eurpub/ckp210
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Berg PVD, Mond J, Eisenberg M, Ackard D, Neumark-Sztainer D. The link between body dissatisfaction and self-esteem in adolescents: similarities across gender, age, weight status, race/ethnicity, and socioeconomic status. J Adolesc Health (2010) 47:290–6. doi: 10.1016/j.jadohealth.2010.02.004
The link between body dissatisfaction and self-esteem in adolescents: similarities across gender, age, weight status, race/ethnicity, and socioeconomic status. J Adolesc Health (2010) 47:290–6. doi: 10.1016/j.jadohealth.2010.02.004
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Birndorf S, Ryan S, Auinger P, Aten M. High self-esteem among adolescents: longitudinal trends, sex differences, and protective factors. J Adolesc Health (2005) 37(3):194–201. doi: 10.1016/j.jadohealth.2004.08.012
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Mak KK, Pang JS, Lai CM, Ho RC. Body esteem in Chinese adolescents: effect of gender, age, and weight. J Health Psychol (2013) 18(1):46–54. doi: 10.1177/1359105312437264
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Aryana M. Relationship between self-esteem and academic achievement amongst pre-university students. J Appl Sci (2010) 10(20): 2474–7. doi: 10.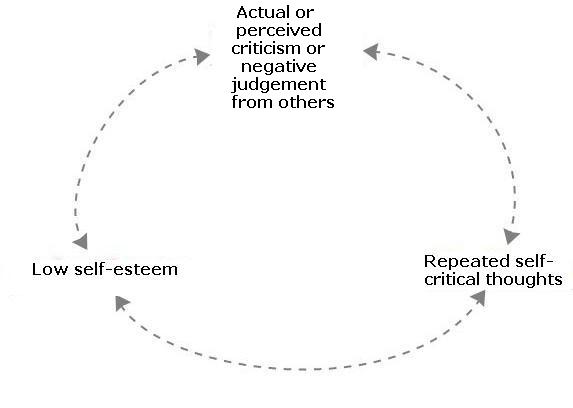 3923/jas.2010.2474.2477
3923/jas.2010.2474.2477
CrossRef Full Text | Google Scholar
15. Baumeister RF, Campbell JD, Krueger JI, Vohs KD. Does high self-esteem cause better performance, interpersonal success, happiness, or health lifestyles? Psychol Sci Public Interest (2003) 4(1):1–44. doi: 10.1111/1529-1006.01431
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Pullmann H, Allik J. Relations of academic and general self-esteem to school achievement. Pers Individual Diff (2008) 45:559–64. doi: 10.1016/j.paid.2008.06.017
CrossRef Full Text | Google Scholar
17. Keane L, Loades M. Review: low self-esteem and internalizing disorders in young people—a systematic review. Child Adolesc Mental Health (2017) 22(1):4–15. doi: 10.1111/camh.12204
CrossRef Full Text | Google Scholar
18. McGee R, Williams S. Does low self-esteem predict health compromising behaviours among adolescents? J Adolesc (2000) 23:569–82. doi: 10.1006/jado.2000. 0344
0344
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Millings A, Buck R, Montgomery A, Spears M, Stallard P. School connectedness, peer attachment, and self-esteem as predictors of adolescent depression. J Adolesc (2012) 35:1061–7. doi: 10.1016/j.adolescence.2012.02.015
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Weber S, Puskar KR, Puskar KR. Relationships between depressive symptoms and perceived social support, self-esteem, & optimism in a sample of rural adolescents. Issues Mental Health Nursing (2010) 31:584–8. doi: 10.3109/01612841003775061
CrossRef Full Text | Google Scholar
21. Rosenberg M, Schooler C, Schoenbach C, Rosenberg F. Global self-esteem and specific self-esteem: different concepts, different outcomes. Am Sociol Rev (1995) 60(1):141–56. doi: 10.2307/2096350
CrossRef Full Text | Google Scholar
22. Wild LG, Flisher AJ, Lombard C. Suicidal ideation and attempts in adolescents: associations with depression and six domains of self-esteem. J Adolesc (2004) 27:611–24. doi: 10.1016/j.adolescence.2004.03.001
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Ghatol SD. Academic stress among higher secondary school students: a review. Int J Adv Res Educ Technol (IJARET) (2017) 4(1):38–41.
Google Scholar
24. Kumari R, Gartia R. Relationship between stress and academic achievement of senior secondary school students. Asian J Multidimension Res (2012) 1(3):153–60.
Google Scholar
25. Nguyen DT, Dedding C, Pham TT, Wright P, Bunders J. Depression, anxiety, and suicidal ideation among Vietnamese secondary school students and proposed solutions: a cross-sectional study. BMC Public Health (2013b) 13(1195). doi: 10.1186/1471-2458-13-1195
CrossRef Full Text | Google Scholar
26. van der Ham L, Wright P, Van TV, Doan VD, Broerse JE. Perceptions of mental health and help-seeking behavior in an urban community in Vietnam: an explorative study. Community Ment Health J (2011) 47(5):574–82. doi: 10.1007/s10597-011-9393-x
doi: 10.1007/s10597-011-9393-x
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Rosenberg M. Society and the adolescent self-image. Revised edition. Middletown, CT: Wesleyan University Press (1989).
Google Scholar
28. Heinonen K, Räikkönen K, Keltikangas-Järvinen L. Self-esteem in early and late adolescence predicts dispositional optimism–pessimism in adulthood: a 21-year longitudinal study. Pers Individual Diff (2005) 39:511–21. doi: 10.1016/j.paid.2005.01.026
CrossRef Full Text | Google Scholar
29. UNICEF Viet Nam. (2010). An analysis of the situation of children in Vietnam 2010. Retrieved 21/9, 2018, from https://www.unicef.org/sitan/files/SitAn-Viet_Nam_2010_Eng.pdf.
Google Scholar
30. Dedovic K, Wadiwalla M, Engert V, Pruessner JC. The role of sex and gender socialization in stress reactivity. Dev Psychol (2009) 45(1):45–55. doi: 10.1037/a0014433
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Rudolph KD. Gender differences in emotional responses to interpersonal stress during adolescence. J Adolesc Health (2002) 30(4 Suppl):3–13. doi: 10.1016/S1054-139X(01)00383-4
Rudolph KD. Gender differences in emotional responses to interpersonal stress during adolescence. J Adolesc Health (2002) 30(4 Suppl):3–13. doi: 10.1016/S1054-139X(01)00383-4
CrossRef Full Text | Google Scholar
32. Keng SL, Lee Y, Drabu S, Hong RY, Chee CYI, Ho CSH, et al. Construct validity of the McLean Screening Instrument for Borderline Personality Disorder in two Singaporean samples. J Pers Disord (2018), 30 (44):450-569. doi: 10.1521/pedi_2018_32_352
CrossRef Full Text | Google Scholar
33. Communist Party of Vietnam. (2017). No. 20-NQ/TW: resolution of the sixth plenary session the 12th Party Central Committee on the protection, care and improvement of people’s health in the new situation. Retrieved March 29th, 2019, from http://unaids.org.vn/wp-content/uploads/2017/12/RESOLUTION.-En.pdf.
Google Scholar
34. Prime Minister of Vietnam. (2006). Directive 23/2006/CT-TTg: directive on strengthening health care at school (Chỉ th về việc tăng cường công tác y tế trong các trường hc). Retrieved August 12, 2017, from https://thuvienphapluat.vn/van-ban/Giao-duc/Chi-thi-23-2006-CT-TTg-tang-cuong-cong-tac-y-te-truong-hoc-13022.aspx.
Retrieved August 12, 2017, from https://thuvienphapluat.vn/van-ban/Giao-duc/Chi-thi-23-2006-CT-TTg-tang-cuong-cong-tac-y-te-truong-hoc-13022.aspx.
Google Scholar
35. Prime Minister of Vietnam. (2009). Decision 401/QĐ-TTg: decision on approving the program on prevention and control of diseases in educational institutions belonging to the public education system (Quyết đnh về việc phê duyệt chương trình phòng, chống bệnh, tật trong các cơ sở giáo dc thuộc hệ thống giáo dc quốc dân). Retrieved August 12, 2017, from https://thuvienphapluat.vn/van-ban/Giao-duc/Quyet-dinh-401-QD-TTg-phe-duyet-chuong-trinh-phong-chong-benh-tat-trong-cac-co-so-giao-duc-thuoc-he-thong-giao-duc-quoc-dan-86772.aspx.
Google Scholar
36. Nguyen DT, Dedding C, Pham TT, Bunders J. Perspectives of pupils, parents, and teachers on mental health problems among Vietnamese secondary school pupils. BMC Public Health (2013a) 13(1046). doi: 10.1186/1471-2458-13-1046
CrossRef Full Text | Google Scholar
37. Yaacob SN, Juhari R, Talib MA, Uba I. Loneliness, stress, self esteem and depression among Malaysian adolescents. Jurnal Kemanusiaan Bil (2009) 14.
Yaacob SN, Juhari R, Talib MA, Uba I. Loneliness, stress, self esteem and depression among Malaysian adolescents. Jurnal Kemanusiaan Bil (2009) 14.
Google Scholar
38. Do TTT, Le MD, Van Nguyen T, Tran BX, Le HT, Nguyen HD, et al. Receptiveness and preferences of health-related smartphone applications among Vietnamese youth and young adults. BMC Public Health (2018) 18(1):764. doi: 10.1186/s12889-018-5641-0
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Tran BX, Zhang MW, Le HT, Nguyen HD, Nguyen LH, Nguyen QLT, et al. What drives young Vietnamese to use mobile health innovations? Implications for health communication and behavioral interventions. JMIR Mhealth Uhealth (2018) 6(11):e194. doi: 10.2196/mhealth.6490
PubMed Abstract | CrossRef Full Text | Google Scholar
40. Quek YH, Tam WWS, Zhang MWB, Ho RCM. Exploring the association between childhood and adolescent obesity and depression: a meta-analysis. Obes Rev (2017) 18(7): 742–54. doi: 10.1111/obr.12535
doi: 10.1111/obr.12535
PubMed Abstract | CrossRef Full Text | Google Scholar
41. Lu Y, Mak KK, van Bever HP, Ng TP, Mak A, Ho RC. Prevalence of anxiety and depressive symptoms in adolescents with asthma: a meta-analysis and meta-regression. Pediatr Allergy Immunol (2012) 23(8):707–15. doi: 10.1111/pai.12000
PubMed Abstract | CrossRef Full Text | Google Scholar
Why Self-Esteem Is Important for Mental Health
JUL. 12, 2016
By Anne Gold
Although low self-esteem is not categorized as a mental health condition in itself, there are clear links between the way we feel about ourselves and our overall mental and emotional wellbeing. U.K.-based charity, Teenage Minds, defines self-esteem as “how a person feels about themselves and what they do.” So a person with high self-esteem believes they are a good person; they can recognize their good qualities and will generally strive for a happy and successful life. Someone with low self-esteem has negative feelings about themselves, believing that they are not worthy of love, happiness or success.
Someone with low self-esteem has negative feelings about themselves, believing that they are not worthy of love, happiness or success.
With research linking low self-esteem to mental health issues and poor quality-of-life, this is a potentially dangerous way to live. Here are just a few ways that low self-esteem can affect mental health and how you can try and improve yours:
- Poor Relationships. As humans, we strive to interact with others and the relationships we have with those closest to us help define us as people. So negative relationships ultimately equal negative feelings and a negative perception of ourselves.
- Addiction. Psychological studies indicate that low self-esteem in childhood and early adulthood can be a predisposition to addiction in later life. Many addicts use substances such as drugs or alcohol to help ease the negative feelings they have about themselves. But over time this method of escapism develops into an addiction and of course this has detrimental effects on their already depleted self-esteem levels.

- Depression and anxiety. Low self-esteem tends to work in a vicious cycle with other mental health conditions like depression and anxiety. It's hard to say which comes first, only that the combination is both common and troublesome. Someone who already lives with a mental illness may find that low self-esteem develops due to the social stigma surrounding mental illness. Stigma can perpetuate the feeling that they have somehow failed.
Building Self-Esteem
Building self-esteem is crucial. When we learn to love ourselves, we strive for a better life—a happier relationship, a more fulfilling career or recovery from addiction. But changing the deep-rooted feelings we have about ourselves isn't easy and often experts recommend some form of therapy (usually Cognitive Behavioral Therapy) to get to the underlying reasons behind our negative thoughts about ourselves.
The key then is to challenge and adjust these negative thoughts into more positive ones. Learning to value and care for your mind and body through a healthy lifestyle is also important. Good diet, exercise and meditation can be the first stepping stones in reclaiming physical and emotional confidence. Fully engaging with those we love is important. Feeling loved and supported (and being able to offer love and support in return) is a wonderful way to start increasing self-esteem. If you don't have any immediate friends or family then consider joining a support group or even volunteering. Helping others is a great way to help yourself.
Learning to value and care for your mind and body through a healthy lifestyle is also important. Good diet, exercise and meditation can be the first stepping stones in reclaiming physical and emotional confidence. Fully engaging with those we love is important. Feeling loved and supported (and being able to offer love and support in return) is a wonderful way to start increasing self-esteem. If you don't have any immediate friends or family then consider joining a support group or even volunteering. Helping others is a great way to help yourself.
Now a writer, Anne Gold worked previously in the mental health sector. She's someone who has battled her own problems with depression and anxiety and firmly believes that to be able to help others, you have to help yourself. Now that she's a mother, she's more acutely aware of staying well and promoting good mental health to others.
We’re always accepting submissions to the NAMI Blog! We feature the latest research, stories of recovery, ways to end stigma and strategies for living well with mental illness. Most importantly: We feature your voices.
Most importantly: We feature your voices.
Check out our Submission Guidelines for more information.
LEARN MORE
high or low in psychology
What is self-esteem? Its main functions. How are self-esteem and self-awareness related? Levels of self-esteem and their signs. How do people's ideas about themselves compare with the opinions of others about them? What is the danger of inadequate self-esteem and how to deal with it? We touched on all these issues in an interview with the Chief Physician of the Harmony Zdorovya Medical Center, psychiatrist, psychiatrist-narcologist and psychotherapist Vladislav Sipovich.
Self-assessment - what is it and what are its main functions?
Self-assessment is a person's ideas about his own personality, its importance to others, the results of his activities, his professional, creative and intellectual abilities, moral qualities, shortcomings and merits. In fact, self-esteem is an assessment of oneself, and all these evaluative ideas about one's personality are based on the individual's value system. The individual in the process of self-observation determines his own personal significance and value in general and its individual aspects. This process is also influenced by external factors, namely:
The individual in the process of self-observation determines his own personal significance and value in general and its individual aspects. This process is also influenced by external factors, namely:
• opinion of the socio-cultural environment, both positive and negative;
• real successes or, conversely, failures;
• the reaction of society to the actions, behavior and psychological qualities of the individual;
• miscalculations in education, etc.
The main functions of self-assessment are as follows:
1. Regulatory , which allows you to make decisions and select targets, ultimately leading to the desire to change yourself for the better, develop and improve your abilities. Varieties of the regulatory function depending on the stage of a particular activity are:
• A predictive function that is important at the initial stage of solving a problem.
• Corrective, or controlling, regulating the process of doing work.
• Retrospective, related to the evaluation of the results of its activities at its final stage.
• Terminal, which ensures the interruption of one's own activities in the event of grounds for self-criticism and a negative assessment of its results. An example is the rejection of unconfirmed hypotheses and options.
2. Protective responsible for the stability of the individual's psyche and its relative independence from the opinions of others.
3. Developing and motivational , providing the individual with the opportunity to develop through the desire for self-improvement and obtaining approval from society.
4. Emotional , which allows you to get moral satisfaction from your qualities, performance results and approving characteristics, which is extremely important for maintaining human dignity.
5. Adaptive providing the best adaptive opportunities in society.
Self-esteem is a natural property of a person and the main component of self-consciousness (knowledge of oneself). Without it, it is impossible to determine one's place in life, set realistic goals, weigh all the pros and cons, adequately correlate one's desires and opportunities, and correctly interpret their compliance with society's requirements.
Without it, it is impossible to determine one's place in life, set realistic goals, weigh all the pros and cons, adequately correlate one's desires and opportunities, and correctly interpret their compliance with society's requirements.
In psychology, self-esteem is given special attention as the central core of the personality and the main component of the self-concept.
What are the types of self-assessment and how is it formed?
In psychology, 3 levels of self-esteem are differentiated, namely:
• Low self-esteem , the psychology of which manifests itself in shyness, lack of self-confidence, lack of a real assessment of one's role and capabilities, difficulties in making decisions, etc.
• Adequate self-esteem is the basis of a reasonable attitude towards oneself, a real correlation of one's desires with needs, abilities with ambitions, opportunities with the tasks set for oneself. Adequacy in self-esteem ensures the harmony of the inner spiritual world of a person, his organic functioning in society and the achievement of success in life.
• Inflated self-esteem is primarily arrogance, peremptoryness, lack of self-criticism, disdain for the opinions of others, boasting and arrogance.
The level of self-esteem in psychology is determined by the formula: the level of claims / the level of opportunities. Moreover, claims include desires, goals, requirements for oneself and others, opportunities - abilities, talent, education and intelligence, social status, upbringing, willpower, physical condition, etc.
The formation of one or another level of self-esteem is significantly influenced by the opinions of others and their attention to the individual and his actions. For the sake of this attention, a person is sometimes ready to take the most inappropriate actions, including crime and even suicide. In addition, it should be remembered that the development of self-esteem begins in childhood, so it largely depends on competent family education. Self-esteem is not a constant formation of the human personality. It varies depending on the stage of personality formation, its self-awareness and level of development.
It varies depending on the stage of personality formation, its self-awareness and level of development.
The following points are important for the formation of self-esteem:
• The fundamental influence of the experience of interaction with the outside world on the formation of the psyche, including the self-esteem of the individual. In psychology, this phenomenon is called internalization and denotes the development of the basic mental functions of a person in the process of growing up and social adaptation with the transition of external interaction into internal mental activity.
• The real success of a person in various fields of activity. The greater the achievement, the higher the self-esteem of the individual.
• Comparability of the real I with the ideal I, i.e. of what a person really is with the way he would like to be. A significant coincidence of the real and ideal self indicates mental health. The smaller the distance between them, the more adequate self-esteem.
Proceeding from this, it can be argued that self-esteem is a rather subjective mental formation, which may not always coincide with the objective assessment of a person by his environment. The adequacy and consistency of self-assessment are tested by real achievements, specific actions and trends in the behavior of the individual in society.
What are the main problems with self-esteem that you can name, how does low self-esteem manifest itself?
I have already talked about the levels of self-esteem, which can be adequate and inadequate. Problems arise when a person evaluates himself inadequately - either with an increase in self-esteem, or with its underestimation. It's hard to say which one is the worst. Both inadequate self-assessments are dangerous both for the person himself and for his environment, because such people endanger themselves and others with their actions that do not correspond to the real state of affairs, or vice versa, inaction.
Let's deal with low self-esteem first. Why is she dangerous? First, a person who underestimates himself is not confident in himself, in his decisions and actions. Secondly, he is inclined to consider even his real successes as pure accident, does not draw conclusions from them and does not include them in his positive experience. Thirdly, it dooms itself to underestimation of others, tk. people are impressed by strong personalities, self-confident and soberly assessing their capabilities.
Why is she dangerous? First, a person who underestimates himself is not confident in himself, in his decisions and actions. Secondly, he is inclined to consider even his real successes as pure accident, does not draw conclusions from them and does not include them in his positive experience. Thirdly, it dooms itself to underestimation of others, tk. people are impressed by strong personalities, self-confident and soberly assessing their capabilities.
A person with low self-esteem is constantly in an atmosphere of doubt and anxiety, which clearly does not contribute to the achievement of goals and adaptation in society. He is primarily concerned with questions about what neighbors, relatives, acquaintances, work colleagues and other representatives of his society will think of him. And this limits the field of his activity and the number of behavioral acts that are necessary to solve problems, but raise doubts in the assessment of others. For example, “Can I smoke in my own apartment, what if cigarette smoke gets through the ventilation to the neighbors, and they will be unhappy”, “What should I do so that my colleague does not think that I am a careerist and set him up?” and so on.
Even in a normal checkout line, a person with low self-esteem always tends to give in, skip, and not resent. In order for him to claim his rights, the injustice must be too obvious. The inability to evaluate oneself adequately leads to an exaggerated dependence on external evaluations of the type: “What will people think and say about me”, and it doesn’t matter that most of them cannot influence his life in any way and whom he may never meet again. Moreover, such assessments are generally not objective and are often the result of a bad mood of the interlocutor. Moreover, a subject with low self-esteem simply thinks out negative conclusions about the opinions of others, evaluating himself as if through the eyes of outsiders and “reading” their thoughts. Even a look that reflects the negative thoughts of another person about his personal situation is attributed to a person with low self-esteem.
Excessive dependence on someone else's opinion leads to the fact that a person constantly experiences strong emotional stress, is in a state of increased anxiety and fear of condemnation. His self-image remains insufficiently formed and is based not so much on real personal characteristics, but on compliance with a set of rules of behavior and relations with the outside world, as well as generally accepted moral and ethical standards. For example, a person tries to help everyone, give up his place in transport and queues for the elderly, pregnant women and people with small children. All this, of course, is not bad, if it does not reach the point of absurdity, when, for example, a pensioner gives way to another similar pensioner, who, in the opinion of the former, is even worse or who is several years older. Such constant humiliation does not pass without a trace and has a destructive effect on the psyche. Sooner or later, it can cause a nervous breakdown (more on neurosis) and violent indignation at the fact that others do not comply with a set of unspoken laws. In fact, the underlying reason for such passions is ordinary envy of those who can afford to break the rules or act according to the situation, regardless of the appropriateness of actions.
His self-image remains insufficiently formed and is based not so much on real personal characteristics, but on compliance with a set of rules of behavior and relations with the outside world, as well as generally accepted moral and ethical standards. For example, a person tries to help everyone, give up his place in transport and queues for the elderly, pregnant women and people with small children. All this, of course, is not bad, if it does not reach the point of absurdity, when, for example, a pensioner gives way to another similar pensioner, who, in the opinion of the former, is even worse or who is several years older. Such constant humiliation does not pass without a trace and has a destructive effect on the psyche. Sooner or later, it can cause a nervous breakdown (more on neurosis) and violent indignation at the fact that others do not comply with a set of unspoken laws. In fact, the underlying reason for such passions is ordinary envy of those who can afford to break the rules or act according to the situation, regardless of the appropriateness of actions.
A person with low self-esteem is not independent in making decisions, he is dependent on the advice and promptings of his environment - family, neighbors, colleagues, friends and even just acquaintances. Although more than once he could make sure that, acting according to his personal motives, he could achieve more tangible results.
Low self-esteem is characterized by excessive self-criticism. A person actually engages in self-discipline when he internally negatively relates to all his actions. And this forms a complex of incompetence and defeatism. Low self-esteem is especially pronounced in public speaking, regardless of the size of the audience. This may be an answer at the blackboard in front of the class, a toast, an entry into a discussion, etc. The fear of becoming a laughingstock literally paralyzes such a person; he cannot clearly state his position and defend his own opinion. The only thing that can help in this case is raising self-esteem with the help of a psychotherapist, who will help to transfer the critical assessment level of the Parent, characteristic of low self-esteem, to the level of an Adult who treats his own person objectively and with self-respect.
Summing up the information about low self-esteem, let me remind you once again of its main features. These are such as:
• Uncertainty in oneself, one's actions and statements.
• Lack of independence and persistent dependence on the opinions and attention of other people.
• Stereotypical actions and behavioral responses.
• Showiness of plausible deeds, helpfulness, desire to please everyone and always.
• Fear of socializing with large numbers of people and fear of public speaking.
• The constant presence of anxiety and obsessive thoughts about their failure.
How does inflated self-esteem manifest itself and how can it harm?
With overestimated self-esteem, an individual tends to overestimate his capabilities and, accordingly, has an increased level of claims. He is self-confident, takes on the most difficult cases, even exceeding his real capabilities, peremptory in his assessments and donkey-like in his statements. It is almost impossible to convince him, he does not take into account the opinions of others, and tends to idealize his own person.
The main signs of inflated self-esteem are the following manifestations:
• Arrogance and arrogance.
• Lack of self-criticism and painful perception of criticism from others.
• Boundless self-confidence, lack of authority, ignoring the opinions of others.
• Leadership ambitions, the desire to always and everywhere be the first, envy and hostility towards more successful people.
• In case of failure of projects, non-admission of one's guilt and incompetence, manifestation of aggression towards competitors, shifting responsibility to others.
• Imposing your opinion, advice and experience, even if no one was interested in them.
• The prevalence of one's own I in any conversation, which he will in any case translate into a discussion of his beloved and ordinary bragging.
• A person with inflated self-esteem often becomes toxic, because he is more likely to bring his environment to a nervous breakdown than himself, because. he is independent of other people's opinions and is not at all worried about this.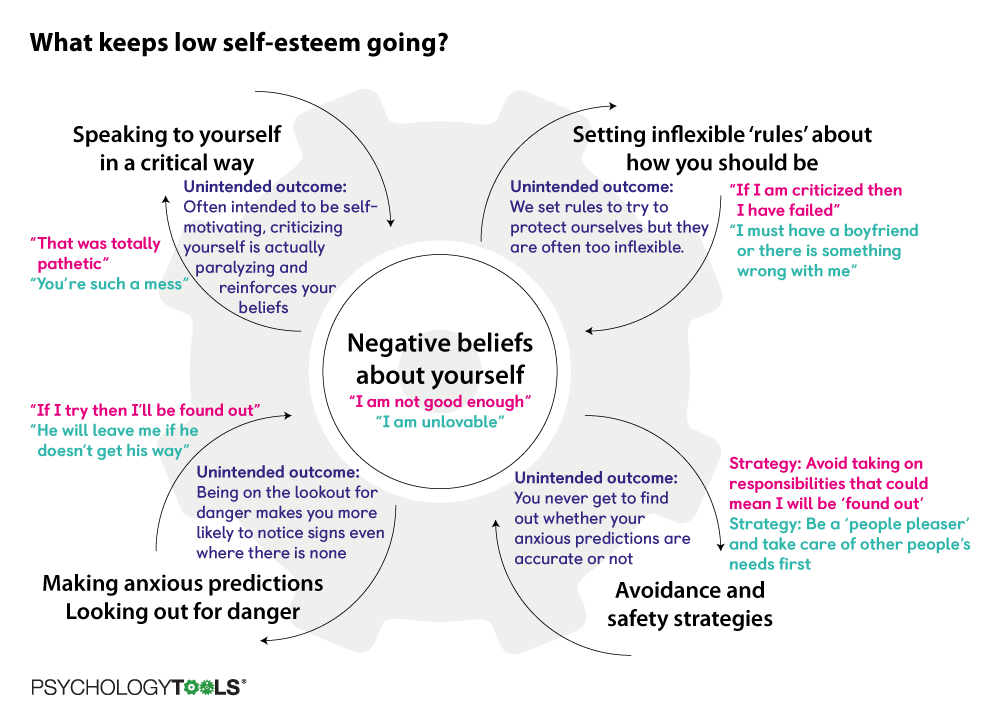 Learn more about toxic relationships.
Learn more about toxic relationships.
Most often, the origins of overly high self-esteem lie in childhood, when a spoiled child is used to being in the epicenter of adult attention and always getting what he wants. The little family idol, whom everyone admires, indulges all his whims and fulfills his desires, begins to believe in his exclusivity and enters adulthood with such convictions. By the way, overestimation of self-esteem can also form in adulthood in the presence of exceptional circumstances. For example, when a girl turns out to be the only representative of the weaker sex in a purely male team or is distinguished by outstanding external data that attracts everyone's attention to her.
How to deal with inadequate self-esteem?
It is quite difficult and problematic to independently change one's self-esteem towards greater adequacy, because people with inadequate self-esteem have practically no ability to control themselves and willpower. With low self-esteem, it is difficult to rely on the willpower of an ever-doubting person, and with an overestimated one, self-control is impossible due to the complete absence of self-criticism. Therefore, if inadequate self-esteem prevents you from living, establishing relationships in the family and the team, achieving professional and creative success, and you are aware of all this, then you cannot do without the help of a psychotherapist. Perhaps he will refer you to courses to improve self-esteem, training and coaching for decision making, assertive behavior, and perhaps develop an individual program for cognitive behavioral therapy, gestalt therapy, etc. But in any case, he will establish and explain the root cause of the patient's inadequate assessment of himself, and this is already the first significant step towards its correction and, if necessary, a deeper change.
Therefore, if inadequate self-esteem prevents you from living, establishing relationships in the family and the team, achieving professional and creative success, and you are aware of all this, then you cannot do without the help of a psychotherapist. Perhaps he will refer you to courses to improve self-esteem, training and coaching for decision making, assertive behavior, and perhaps develop an individual program for cognitive behavioral therapy, gestalt therapy, etc. But in any case, he will establish and explain the root cause of the patient's inadequate assessment of himself, and this is already the first significant step towards its correction and, if necessary, a deeper change.
Where does low self-esteem really come from and how can it be corrected?
Health
Low self-esteem (which is formed due to childhood traumas, biological characteristics and bad life experiences) can be fought. The scientific director of the psychological center "Quality of Life", a specialist in the field of cognitive-behavioral psychotherapy Alexander Erichev told Sobaka. Ru what steps will help to do this.
Ru what steps will help to do this.
Reasons for low self-esteem
People with low self-esteem always have negative core beliefs about themselves. They appear in the process of life experience - including if a person has faced a large number of punishments, prohibitions, insults, neglect. The first group of such beliefs is associated with defectiveness ("I'm somehow not like that"), the second - with helplessness ("I'm weak") and the third - with the lack of love ("they don't like me").
Negative beliefs often arise when childhood is not satisfied basic needs. First of all, the need for love and acceptance. For example, at the time of the birth of a child, maternal feelings did not awaken at the mother, and the father generally disappeared in an unknown direction. Another situation is emotional deprivation from parents. For example, they were not used to expressing warm feelings, were less emotional than other families.
Quite often people suffer from low self-esteem, who seemed to have quite good support in the family, but got into a situation of prolonged bullying. For example, at school, such a situation can seriously change the perception of oneself. The man, remembering the time of persecution, says that he felt fear and helplessness. He was in a state of chronic stress for a very long time, and this negative experience stuck with him.
When a person's self-esteem is distorted, he finds even more evidence in events that he is bad
There are also biological preconditions for low self-esteem to become fixed in a person . For example, a dandelion baby and an orchid baby can be born in the same family. "Dandelion" will grow through the asphalt and will be less sensitive to environmental factors. Such a child will more easily cope with the same bullying. And the orchid child, who, for biological reasons, is more vulnerable and shy, will not be able to resolve this situation, perhaps he will not even seek support from his parents. We must not forget that we all have different types of nervous system. We are different from each other even at birth, and then life also leaves its serious imprint. The production of hormones changes, stress reactions are fixed.
We must not forget that we all have different types of nervous system. We are different from each other even at birth, and then life also leaves its serious imprint. The production of hormones changes, stress reactions are fixed.
Distortions in personal thinking play a huge role in our self-esteem. We all perceive the same situation differently. Recent studies show that even our memories should not be trusted, because they are seriously distorted, including under the influence of our emotions. So, if a person has a distorted personal self-esteem, and he feels weak, helpless, defective and lazy, then he will also perceive all the events that happen to him in a distorted way. And find more and more evidence that he is bad.
One person with low self-esteem will avoid contact with the opposite sex out of fear, another, on the contrary, will have a huge number of casual relationships
What bad thoughts about ourselves lead to
in addition, the person himself tries to protect himself from them by a set of rules. That is, he seeks to prevent the confirmation of his fears and fears. For example, if he thinks that he is unloved, then what strategies of behavior will he demonstrate? They can be completely opposite. One will avoid contact with the opposite sex for fear of being rejected anyway. The other will choose a different behavior: on the contrary, he will have a huge number of casual connections, and he will perceive each acquaintance as a trophy. In appearance, he will seem confident and impudent, but in fact, behind this behavior, hide his negative attitudes towards himself. Such rules that a person has created for himself can be different. For example, a person decides that he must always be polite. Or if he is criticized, it immediately means that he is bad. And if he doesn't try his best, he won't achieve anything.
That is, he seeks to prevent the confirmation of his fears and fears. For example, if he thinks that he is unloved, then what strategies of behavior will he demonstrate? They can be completely opposite. One will avoid contact with the opposite sex for fear of being rejected anyway. The other will choose a different behavior: on the contrary, he will have a huge number of casual connections, and he will perceive each acquaintance as a trophy. In appearance, he will seem confident and impudent, but in fact, behind this behavior, hide his negative attitudes towards himself. Such rules that a person has created for himself can be different. For example, a person decides that he must always be polite. Or if he is criticized, it immediately means that he is bad. And if he doesn't try his best, he won't achieve anything.
A person with low self-esteem attributes all failures to himself, and success to chance
To assess your self-esteem, ask yourself a series of questions. Has your life experience taught you to value yourself for who you are? Do you have a good opinion of yourself? Do you take good care of yourself and take care of yourself? Do you like yourself? Do you value both your strengths and weaknesses equally? Are you quite satisfied? Do you feel entitled to other people's attention and time? Do you judge yourself the same way you judge others – no more, no less? Are you more inclined to encourage yourself than engage in self-criticism?
Has your life experience taught you to value yourself for who you are? Do you have a good opinion of yourself? Do you take good care of yourself and take care of yourself? Do you like yourself? Do you value both your strengths and weaknesses equally? Are you quite satisfied? Do you feel entitled to other people's attention and time? Do you judge yourself the same way you judge others – no more, no less? Are you more inclined to encourage yourself than engage in self-criticism?
When working on self-esteem, one should not strive for it to become inflated and fly away into space. This is also not good. When we deliberately make unrealistic demands of ourselves and declare something like “I am the king of the world,” the more often reality tells us that something is wrong with our beliefs about ourselves. High self-esteem is often unstable, so external circumstances can easily unsettle a person. And you need to strive first of all for stability and learn to support yourself.
A person is more likely to conditionally “get” depression or an anxiety disorder if he attributes all failures to himself, and attributes all positive things to chance. Namely, this is usually done by a person with low self-esteem.
It is easy to track and stop unjustified criticism of yourself
What to do? Stop criticizing yourself, punish yourself
Psychotherapists identify several modes, that is, emotional states, which we enter from time to time. One of the unhealthy is the regime of a critical or punishing parent. In it, we force ourselves to experience feelings of inferiority and guilt, point out that we owe something. At the same time, we criticize for such trifles for which we would never scold others. And we punish in those moments when we really need help.
You can easily see how this mode turns on. It additionally supports low self-esteem or even lowers it even more. For example, when you say to yourself: “Could have done better”, “Why is this not so good?”, “Is that all you did?”, “Others can, and you can”. You also present the results of your work as some kind of nonsense. Others praise you, but you think: “No, it seemed to them, I just got lucky.”
You also present the results of your work as some kind of nonsense. Others praise you, but you think: “No, it seemed to them, I just got lucky.”
Learn to turn off your inner critic mode and be more supportive of yourself
The good news is that we can easily detect and stop unreasonable self-criticism and depreciation in ourselves. This skill is quite possible to develop even without the help of a psychotherapist. Although it can take a decent amount of time. Try to observe your critical parent for at least a week. You will most likely notice that he appears even when you shouldn't be scolding yourself.
Try to translate self-criticism into self-compassion. Instead of the desire to punish and condemn yourself, you should switch to the desire to correct the situation and achieve a better result. Instead of looking to the past, look to the future and try to figure out what can be done now. Shift the focus from your mistakes to your strengths and resources, and instead of frustration, anger, and anxiety, try to be supportive of yourself.
Learn to express emotions, both negative and positive
Stand up for your boundaries and rights
Develop assertiveness - the ability to stand up for your boundaries and rights so as not to destroy someone else's personal space. It is believed that assertive behavior quite clearly correlates with adequate self-esteem. What does it include? Open and sincere expression of positive emotions, as well as open (but adequate) expression of negative ones. We need to learn how to properly express our negative emotions - this is very important. Assertiveness also includes the ability to self-defense and the ability to say “no”. Quite often, when we feel anxious and helpless inside, we agree to things that are obviously unpleasant for us. And then we begin to blame ourselves: “How could you, you definitely had to refuse, why didn’t you refuse, you could pull yourself together!” Assertiveness also includes initiative, the ability to offer, ask, respect one’s own dignity - now this is beautifully called such a term as “proactivity”.
Often we can't say "no" to a person and end up blaming ourselves for it even more
Practice assertive behavior other than "You're a rag, come on!" , but in the style of "You're worried, but let's try to take a small step now." It is also worth praising yourself for trying, even if it has not yet been successful. For example, you failed to deny, although you tried to do so. Or you said “no” but the other person insisted that you say “yes”. But this is already a reason to tell yourself that you have practically succeeded, although not yet completely.
Take care of your needs
Learn to take care of yourself and your needs (again, without overstepping other people's boundaries). This is probably the most difficult advice, because it requires a fairly good level of awareness. You can learn this slowly - you feel that you want to drink water and drink it. Try to listen to more ambiguous needs and feel your desires.
Imagine praising yourself as your favorite child
Learn self-efficacy
Self-efficacy is how we perceive our ability to cope with certain circumstances. If we feel that the world is so inexplicable and cruel that we cannot do anything, then naturally we will evaluate ourselves worse. If we perceive our ability to act, this gives us significant help and support. For me, a good example of self-efficacy is independent travel. At first you are scared, and then you get the feeling that the world around you is quite friendly, that you can easily deal with the transport network and find yourself a place to sleep.
Support yourself and celebrate your achievements
It is important that support and praise in your address does not turn into something like: "I'm so cool." Think about what you can support yourself for today? What good did you do during the day? Imagine that you yourself, as your beloved child, say good words. At the same time, praise can be not only for certain successful actions. For example, I survived a difficult situation, I coped with it - this is also a reason for praise. It will be good if it becomes your tradition to notice your achievements.
At the same time, praise can be not only for certain successful actions. For example, I survived a difficult situation, I coped with it - this is also a reason for praise. It will be good if it becomes your tradition to notice your achievements.
Build goals in accordance with personal values
To reinforce an adequate and stable self-esteem, you need to learn to look for your values. Note that values are not goals. For example, buying a car is a goal. And what could be the value here? Freedom of movement, travel. The goal can be achieved and after that it will not be. And the value is unattainable, this is a certain stage of the path. It is very important to understand what your values are and, if possible, build your life in this direction. But do not turn it into a radical search for "one's destiny." This is a dangerous and wrong situation.
Some of our values may conflict with each other. For example, it is important for you to travel and develop, while you dream of children.