Level one autism spectrum disorder
Understanding Level 1 of Autism Spectrum Disorder
Your child is the most important person in your life, and you want the best outcomes for their future. You may notice, however, that while your child is able to focus on a task and is highly intelligent, they may have difficulties holding a proper conversation or understanding social cues.
There is a chance that your child may have a mild form of autism known as Autism Level 1. But, what exactly does that mean?
What Is Autism-Level 1?
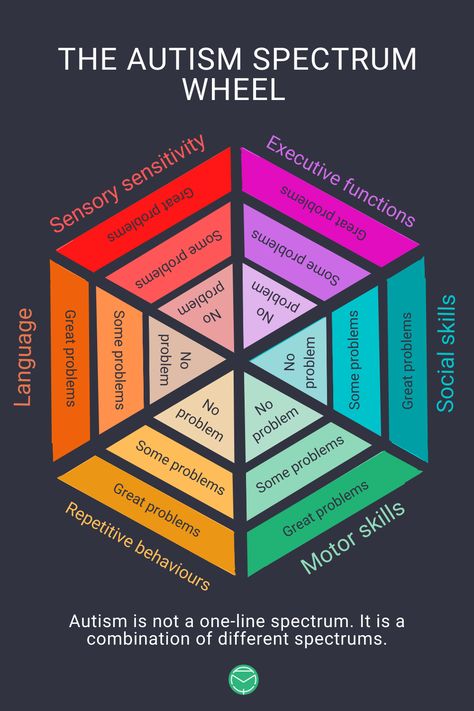
Autism is generally defined as a broad range of conditions characterized by challenges with social skills, repetitive behaviors, speech, and nonverbal autism communication. According to the Centers for Disease Control, autism affects an estimated one in fifty-four children in the U.S. today.
Additionally, there are several types of autism. The American Psychiatric Association (APA) combines all autism-related conditions under one umbrella term, known as autism spectrum disorders (ASD).
Today, ASD is divided into three levels that reflect severity:
- Level 1: Level 1 is the mildest form of ASD, but children in this category still require support. Generally, children at this level have more mild symptoms, but still have a hard time communicating appropriately or engaging with others. For example, they may not say the right thing at the right time or have difficulty reading social cues and body language. This is what most people previously referred to when they used the terms “Asperger’s syndrome” or “high-functioning autism”.
- Level 2: Children at this level require substantial support as there are typically more obvious problems with verbal and social communication compared to those diagnosed with Level 1 autism. Children with Level 2 tend to have very narrow interests and engage in repetitive behaviors that can make it difficult for them to function or participate in certain situations.
- Level 3: This is the most severe form of ASD.
 Children in this category tend to have many of the same difficulties or behaviors as those with Levels 1 and 2, but to a heightened degree. Children at this level have severe deficits in verbal and nonverbal social communication skills that cause severe impairments in functioning, very limited initiation of social interactions, and minimal response to social overtures from others. People at this level require the most support, which can include full-time aides.
Children in this category tend to have many of the same difficulties or behaviors as those with Levels 1 and 2, but to a heightened degree. Children at this level have severe deficits in verbal and nonverbal social communication skills that cause severe impairments in functioning, very limited initiation of social interactions, and minimal response to social overtures from others. People at this level require the most support, which can include full-time aides.
Autism (Level 1) Symptoms
Autism symptoms differ for each child. However, generally speaking, there are common symptoms for children with Autism-Level 1. Some of these symptoms may be viewed as strengths, while other symptoms can be considered challenges.
Strengths can include:
- Remarkable focus and persistence
- Aptitude for recognizing patterns
- Attention to detail
Challenges can include:
- Hypersensitivities to lights, sounds, or other stimuli
- Difficulty maintaining a typical conversation
- Difficulty with nonverbal conversation skills, such as distance, loudness, or tone during conversations
- Uncoordinated movements or clumsiness
If you believe that your child may be demonstrating Autism-Level 1 symptoms, Ascend Autism is ready to answer your questions about how to best support your child.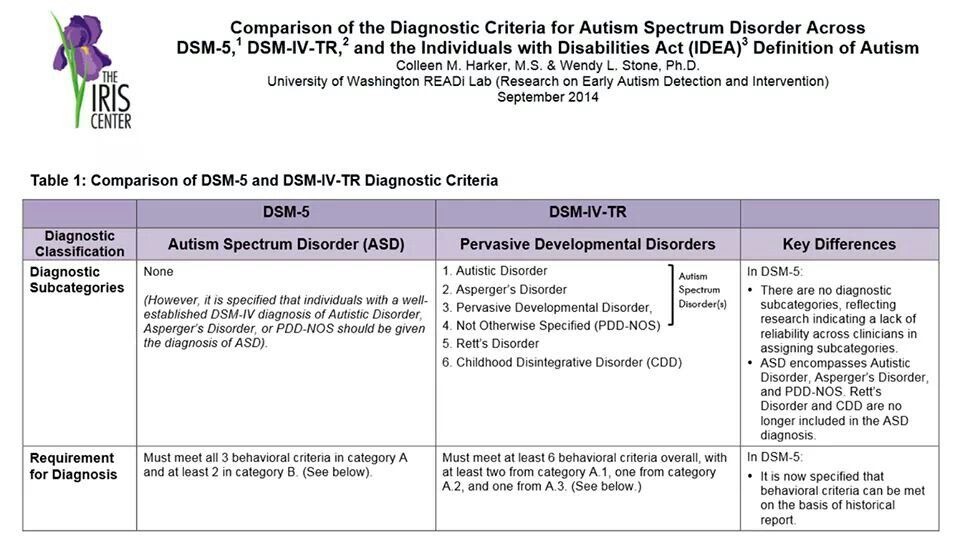
Related Reading:
- Early Signs of Autism
- Signs of Autism in Boys
- Signs of Autism in Girls
- Life Before an ASD Diagnosis: Pre-Testing or Screening
About Ascend Autism
Ascend Autism is a valuable resource for children with high-functioning autism and their families. Over a decade ago, Ascend Autism was founded by a highly qualified team of healthcare operators and Board Certified Behavior Analysts (BCBA).
Ascend Autism provides interventions using evidence-based practices (EBPs) for children with high-functioning autism symptoms. EBPs are therapies and treatments that have gone through rigorous research and review and have been found to be effective for treating children with high-functioning autism. Children with high-functioning autism symptoms who have participated in EBPs have shown positive results and better outcomes.
Along with our treatment programs, we provide a safe environment for children with high-functioning autism so that they feel secure and relaxed. When children with high-functioning autism are comfortable in their setting, they are free to achieve their treatment goals.
When children with high-functioning autism are comfortable in their setting, they are free to achieve their treatment goals.
Autism Therapy Programs at Ascend Autism
At Ascend Autism, we offer autism spectrum treatment programs for our students, including:
- Early intervention program
- Targeted intervention program
- Social skills work
- Parental services
Find Out How Ascend Autism Can Help Your Child with High-Functioning Autism
Our Ascend Autism team is ready to help children with high-functioning autism. We have treatment programs that are based on methods that are scientifically proven to be effective.
Learn more about Ascend Autism and our track record of success for children with high-functioning autism. Contact us today by calling us or completing our secure online form for more information.
Level 1 Autism Spectrum Disorder (formerly known as Asperger's Syndrome)
- Typical Academic Accommodations
- Resources
- References
Since the mid-2000’s, there has been a steady increase in the number of students with Autism Spectrum Disorder (ASD) registered at the Paul Menton Centre, consistent with the finding that Ottawa has the second-highest concentration of such students in Ontario (Alcorn-MacKay, 2010).
While still in use, the term Asperger’s Syndrome does not appear in the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM; American Psychiatric Association, 2013), and is now subsumed under the broad category of Autism Spectrum Disorder (ASD). Those diagnosed in the past with Asperger’s would now be identified as having Level 1 ASD (requiring minimal supports). A neurodevelopmental disorder usually identified in childhood, ASD is diagnosed and described based on two symptom dimensions: (1) Deficits in social communication/social interaction, and (2) Restricted, repetitive patterns of behaviour, interests or activities.
Carleton students with ASD typically have many strengths. They are usually highly articulate, in speech and in writing. They tend to be attentive to detail, with strengths in rote memory and a systematic, logical approach to problem solving. They may have intense interests around a general theme (for example, mechanics or history) with more specific, related interests having varied since childhood (Stoddart, Burke and King, 2012), which can be highly motivating if they are in a related program.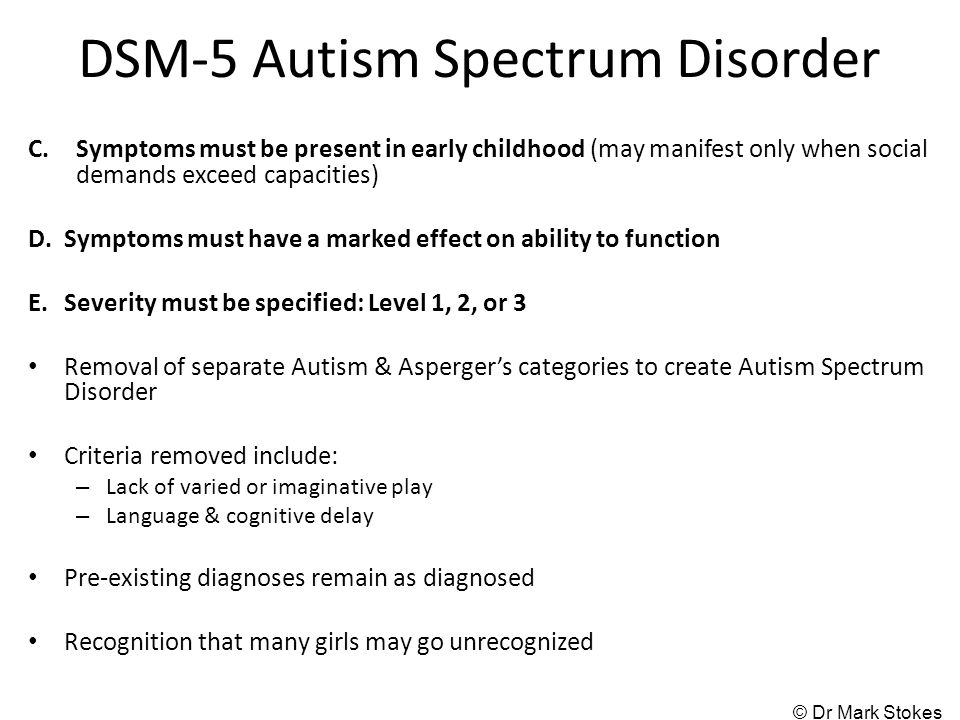 They are also likely to be straightforward, loyal and honest (McMahon-Coleman, 2016).
They are also likely to be straightforward, loyal and honest (McMahon-Coleman, 2016).
In addition to the two DSM-V symptom dimensions, students with ASD may experience excessive anxiety associated with everyday events. Many are hypersensitive to environmental stimuli, such as noise, harsh lighting and crowds. They may exhibit rigid, inflexible, rule-bound behaviour, and can experience profound anxiety in response to unfamiliar settings, unclear expectations, and (seemingly minor) changes (e.g. last-minute changes to course syllabus). Other observed areas of difficulty include time management and organization, concentration, fine motor skills (messy, effortful handwriting) and processing speed.
Many students with ASD struggle to participate in class discussions, presentations and group work. Grades may suffer because they do not intuitively grasp “the hidden curriculum” like their peers. To illustrate, some may lack awareness of the various types of postsecondary settings – like lectures, labs, and discussion groups – with distinct formats for teaching and learning and expectations for behaviour. They may generalize from the familiar, predominately reproductive learning culture of high school (memorise this and give it back) and be unprepared when required to analyse, critique, or apply knowledge. They may need to be taught explicitly that different academic fields apply different writing conventions, which vary further across assignment types (book report versus persuasive essay, for example), and benefit from access to models, scaffolded assignments (McMahon-Coleman, 2016) and clear written instructions.
They may generalize from the familiar, predominately reproductive learning culture of high school (memorise this and give it back) and be unprepared when required to analyse, critique, or apply knowledge. They may need to be taught explicitly that different academic fields apply different writing conventions, which vary further across assignment types (book report versus persuasive essay, for example), and benefit from access to models, scaffolded assignments (McMahon-Coleman, 2016) and clear written instructions.
Symptoms and characteristics of ASD may lead to false impressions; as a result, many students struggle to establish and maintain friendships. Some speak in a relatively monotone voice with limited eye contact and avoid social interactions. Such individuals may be perceived as aloof, uninterested “loners”. Others speak too loudly and out of context, with intense eye contact and a propensity to talk extensively about their own interests, giving the impression that they are insensitive and self-centered. They may be unaware of “unwritten” social rules (e.g. personal space), or interpret language in a highly literal fashion (cannot detect sarcasm or “read between the lines”). Most can’t “do small talk”; nor do they readily interpret and express non-verbal social cues (facial expressions, tone of voice, gestures).
They may be unaware of “unwritten” social rules (e.g. personal space), or interpret language in a highly literal fashion (cannot detect sarcasm or “read between the lines”). Most can’t “do small talk”; nor do they readily interpret and express non-verbal social cues (facial expressions, tone of voice, gestures).
Typical Academic Accommodations
- Extra time and a smaller location for tests and exams
- Access to a word processor for written tests and exams
- Recording software or recording pen for lectures
- Access to volunteer notetaking services
- Consideration for group work, presentations or participation1.
In some cases, a PMC Coordinator will encourage students with ASD to send their instructors a personalised Letter of Introduction explaining the impact of their disability and related strengths and challenges.
1 Students with ASD are expected to work to develop their skills in these areas, but individualized accommodations may be negotiated with instructors to allow them to perform to the best of their ability.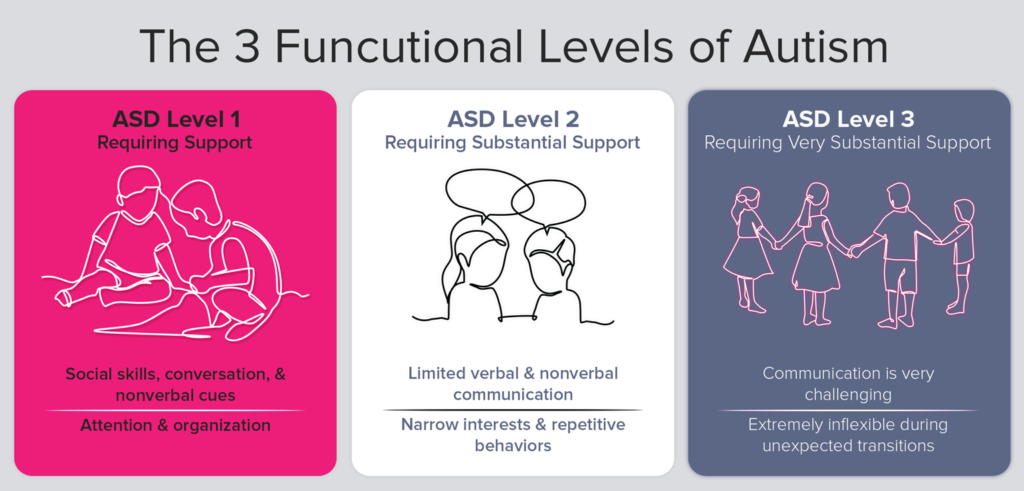
Resources
Gobbo, K. and Shmulsky, S. (2014) Faculty Experience With College Students With Autism Spectrum Disorders: A Qualitative Study of Challenges and Solutions. Focus on Autism and other Developmental Disabilities, 29(1), 13-22
McKeon, B., Alpern, C. S., & Zager, D. (2013). Promoting academic engagement for college students with Autism Spectrum Disorder. Journal of Postsecondary Education and Disability, 26(4), 353-366.
Burgstahler, S. & Russo-Gleicher, R.J. (2015). Applying universal design to address the needs of postsecondary students on the autism spectrum. Journal of Postsecondary Education and Disability, 29, 199-212.
https://www.facultyfocus.com/articles/effective-classroom-management/teachingcollege-students-with-autism-spectrum-disorders/
https://www.facultyfocus.com/articles/course-design-ideas/why-some-students-strugglewith-group-work/
References
Alcorn Mackay, S.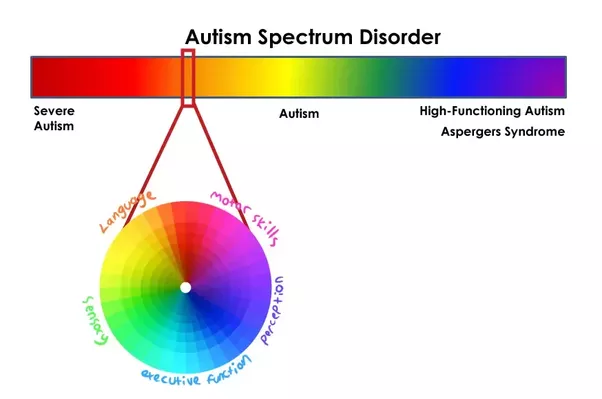 (2010). Identifying Trends and Supports for Students with Autism Spectrum Disorder Transitioning into Postsecondary. Toronto: Higher Education Quality Council Ontario.
(2010). Identifying Trends and Supports for Students with Autism Spectrum Disorder Transitioning into Postsecondary. Toronto: Higher Education Quality Council Ontario.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Stoddart, K. P., Burke, L., and King, R. (2012). Asperger Syndrome in Adulthood: A Comprehensive Guide for Clinicians. New York: W.W. Norton & Company, Inc.
Baron-Cohen, S., Leslie, A. and Frith, U. (1985). Does the autistic child have a “theory of mind”? Cognition, 21(1), 37-46
Share: Twitter, Facebook
Short URL: https://carleton.ca/pmc/?p=499
Autism spectrum disorders in children
home
Articles
Diseases
Alpatsky Dmitry Aleksandrovich Neurologist, epileptologist, EEG doctor
07.12.2015
Often, mothers come to the doctor with complaints of delayed speech development in a child. But in some children, with a close look, the specialist, in addition, sees the features of the child's behavior that differ from the norm and are alarming .
But in some children, with a close look, the specialist, in addition, sees the features of the child's behavior that differ from the norm and are alarming .
Consider a clinical example:
Boy S. Age 2 years 9 months. According to the mother, the child's vocabulary is no more than 20 separate words, consisting of two or three syllables. There are no phrases. Mom says that the child often has tantrums, is restless, it is difficult to fall asleep. The child's mother has no other complaints. On examination, the doctor notices that the child does not look into the eyes, is constantly in motion, reacts with a cry if something is not given or forbidden to him. You can calm the child only by giving him a mobile phone or tablet. Shows interest not in children's toys, but more in shiny pieces of furniture and interior. Starting to play something, quickly loses interest and switches to something else. Asking the mother, it turns out that the child is very selective in food. Not accustomed to the potty, defecation only in a diaper in a standing position. Difficulty falling asleep and waking up during sleep. The child underwent Electroencephalography and consultations with a clinical psychologist and a speech therapist. Based on the results of the diagnosis and the clinical picture, the diagnosis was made - Autism Spectrum Disorder. nine0026
Not accustomed to the potty, defecation only in a diaper in a standing position. Difficulty falling asleep and waking up during sleep. The child underwent Electroencephalography and consultations with a clinical psychologist and a speech therapist. Based on the results of the diagnosis and the clinical picture, the diagnosis was made - Autism Spectrum Disorder. nine0026
Autism Spectrum Disorders (ASD) are complex disorders of mental development that are characterized by social maladaptation and inability to social interaction, communication and behavioral stereotypy (multiple repetitions of monotonous actions).
Back in the middle of the last century, autism was a fairly rare disease. But over time, more and more children suffering from this disorder began to appear. Statistics show that the incidence of ASD in children over the past 30-40 years in countries where such statistics are carried out has risen from 4-5 people per 10,000 children to 50-116 cases per 10,000 children. At the same time, boys are more susceptible to this disease than girls (approximately 4:1 ratio). nine0003
At the same time, boys are more susceptible to this disease than girls (approximately 4:1 ratio). nine0003
Causes of RAS.
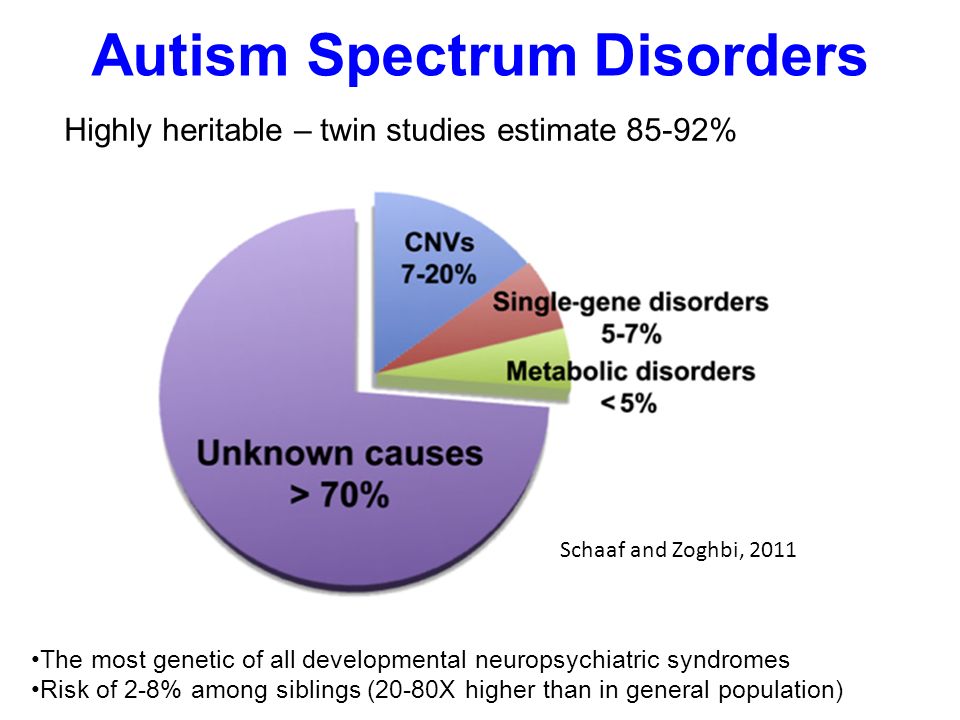
All over the world, until today, scientists studying the causes of autism have not come to a consensus. Many assumptions are put forward. Among the possible factors for the appearance of this disorder in children are some hypotheses:
- genetic predisposition hypothesis
- a hypothesis based on disorders of the development of the nervous system (autism is considered as a disease caused by disorders of brain development in the early stages of a child's growth). nine0003
- hypotheses about the influence of external factors: infections, chemical effects on the mother's body during pregnancy, birth trauma, congenital metabolic disorders, the influence of certain drugs, industrial toxins.
But whether these factors really can lead to the appearance of autism in children has not yet been clarified.
Features of the mental development of children with ASD.
To understand and recognize the presence of autism in a child, parents need to carefully monitor the behavior of the child, notice unusual signs that are not characteristic of the age norm. Most often, these signs can be detected in children under the age of 3 years. nine0003
Childhood autism is considered as a developmental disorder that affects all areas of the child's psyche: intellectual, emotional, sensitivity, motor sphere, attention, thinking, memory, speech.
Disorders of speech development : absent or weak cooing and babbling may be noted at an early age. After a year, it becomes noticeable that the child does not use speech to communicate with adults, does not respond to a name, and does not follow verbal instructions. By the age of 2, children have a very small vocabulary. By the age of 3 they do not build phrases or sentences. At the same time, children often stereotypically repeat words (often incomprehensible to others) in the form of an echo. Some children have a lack of speech development. For others, speech continues to develop, but there are still communication impairments. Children do not use pronouns, address, speak about themselves in the third person. In some cases, there is a regression of previously acquired speech skills. nine0003
Some children have a lack of speech development. For others, speech continues to develop, but there are still communication impairments. Children do not use pronouns, address, speak about themselves in the third person. In some cases, there is a regression of previously acquired speech skills. nine0003
Difficulties in communication and lack of emotional contact with others: Such children shy away from tactile contact, eye contact is almost completely absent, there are inadequate facial reactions and difficulties in using gestures. Children most often do not smile, do not reach out to their parents and resist attempts by adults to take them in their arms. Children with autism lack the ability to express their emotions, as well as to recognize them in the people around them. There is a lack of empathy for other people. The child, along with the adult, does not focus on one activity. Children with autism do not make contact with other children or avoid it, they find it difficult to cooperate with other children, most often they tend to retire (difficulties in adapting to the environment). nine0003
nine0003
H violation of exploratory behavior: children are not attracted by the novelty of the situation, are not interested in the environment, are not interested in toys. Therefore, children with autism most often use toys in an unusual way, for example, a child may not roll the whole car, but turn one of its wheels monotonously for hours. Or not understanding the purpose of the toy to use it for other purposes.
Eating disorders : a child with autism can be extremely selective in the products offered, food can cause the child to be disgusted, dangerous, often children begin to sniff food. But along with this, children may try to eat an inedible thing. nine0003
Violation of self-preservation behavior: due to a large number of fears, the child often finds himself in a situation that is dangerous for himself. The cause can be any external stimulus that causes an inadequate reaction in the child. For example, a sudden noise may cause a child to run in a random direction.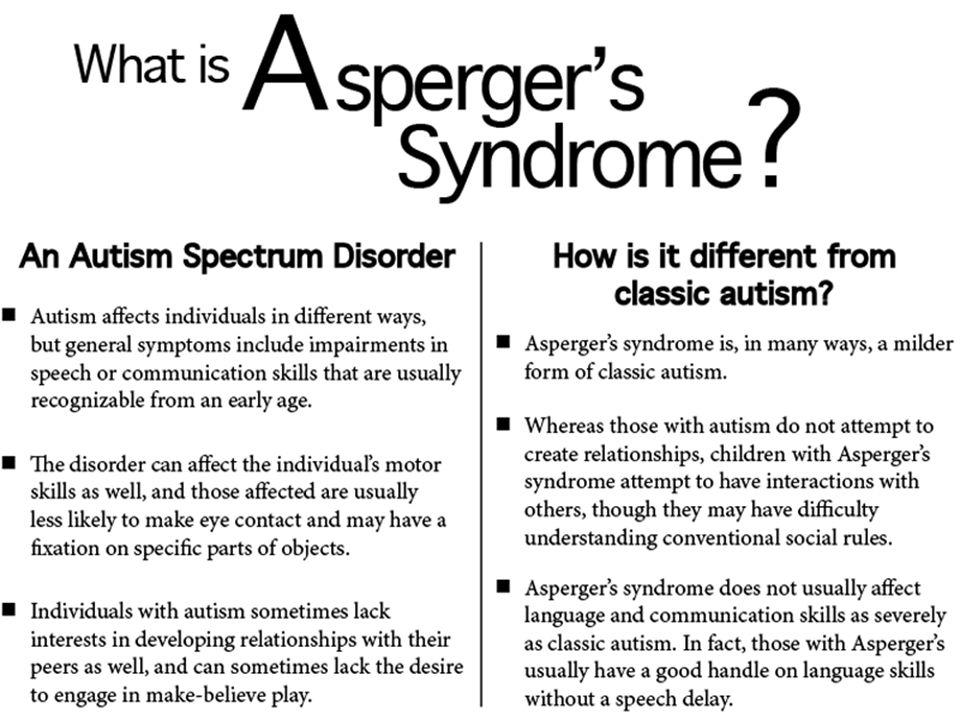 Also, the reason is ignoring real threats to life: a child can climb very high, play with sharp objects, cross the road without looking. nine0003
Also, the reason is ignoring real threats to life: a child can climb very high, play with sharp objects, cross the road without looking. nine0003
Disturbance of motor development: as soon as the child begins to walk, he is noted for clumsiness. Also, some children with autism are inherent in walking on their toes, a very noticeable violation of the coordination of hands and feet. It is very difficult for such children to teach everyday actions, it is rather difficult for them to imitate. Instead, they develop stereotypical movements (performing the same actions for a long time, running in circles, swinging, flapping “like wings” and circular movements with their arms), as well as stereotypical manipulations with objects (tweaking small details, lining them up). Children with autism have significant difficulty in learning self-care skills. Pronounced motor awkwardness. nine0003
Perception disorders: difficulties in orientation in space, fragmentation in the perception of the environment, distortion of a holistic picture of the objective world.
Difficulty in concentrating: children have difficulty concentrating on one thing, there is high impulsivity and restlessness.
Poor memory: Often, both parents and professionals notice that children with autism are good at remembering things that are meaningful to them (this may cause them pleasure or fear). Such children remember their fear for a long time, even if it happened a very long time ago. nine0003
Features of thinking: experts note difficulties in arbitrary learning. Also, children with autism do not focus on understanding the cause-and-effect relationships in what is happening, there are difficulties in transferring the acquired skills to a new situation, the concreteness of thinking. It is difficult for a child to understand the sequence of events and the logic of another person.
Behavioral problems: negativism (refusal to listen to the adult's instructions, to perform joint activities with him, avoiding the learning situation). Often accompanied by resistance, screams, aggressive outbursts. A huge problem is the fears of such children. Usually they are incomprehensible to others, because often children cannot explain them. The child may be frightened by sharp sounds, some specific actions. Another behavioral disorder is aggression. Any disorder, violation of a stereotype, interference of the outside world in a child's life can provoke aggressive (hysteria or physical attack) and auto-aggressive outbursts (damage to oneself). nine0003
Often accompanied by resistance, screams, aggressive outbursts. A huge problem is the fears of such children. Usually they are incomprehensible to others, because often children cannot explain them. The child may be frightened by sharp sounds, some specific actions. Another behavioral disorder is aggression. Any disorder, violation of a stereotype, interference of the outside world in a child's life can provoke aggressive (hysteria or physical attack) and auto-aggressive outbursts (damage to oneself). nine0003
Each case of the disease is very individual: autism can have most of the listed signs in an extreme degree of manifestation, and it can manifest itself only in some barely noticeable features.
Diagnosis of Autism Spectrum Disorders
To diagnose autism, specialists use the criteria of 2 international classifications: ICD-10 and DSM-5.
But the main three criteria (“triad” of violations) that can be distinguished are: nine0003
- violation of social adaptation
- violations in the communication sphere
- stereotypical behavior
The main diagnostic steps include:
- examination of the child by a psychiatrist, neurologist, psychologist
- observation of the child and filling out the "Autism Rating Scale", which can be used to determine the severity of the disorder
- conversation with parents nine0003
- filling in questionnaires by parents - "Questionnaire for the diagnosis of autism"
Species PAC
There are several existing classifications of ASD, and the separation often occurs on completely different grounds, which, of course, can bring some inconvenience to a person who is initially little familiar with medicine or psychology; therefore, the most basic and frequently encountered types of ASD will be highlighted below: - Kanner's syndrome (Early childhood autism) - characterized by a "triad" of the main violations: difficulty in establishing contacts with the outside world, stereotypical behavior, as well as a delay or violation of the communicative functions of speech development . It is also necessary to note the condition of the early onset of these symptoms (up to about 2.5 years) nine0003
It is also necessary to note the condition of the early onset of these symptoms (up to about 2.5 years) nine0003
It manifests itself in children in 4 forms, depending on the degree of fencing off from the outside world:
Complete detachment from what is happening. This group is characterized by the absence of speech and the inability to organize the child (to establish eye contact, to achieve the implementation of instructions and assignments). When trying to interact with the child, he shows the greatest discomfort and impaired activity.
Active rejection. It is characterized by more active contact with the environment than the first group. There is no such detachment, but there is rejection of a part of the world that is unacceptable to the child. The child shows selective behavior (in communication with people, in food, in clothes) nine0003
Preoccupation with autistic interests. It is characterized by the formation of overvalued addictions (for years a child can talk on the same topic, draw the same plot).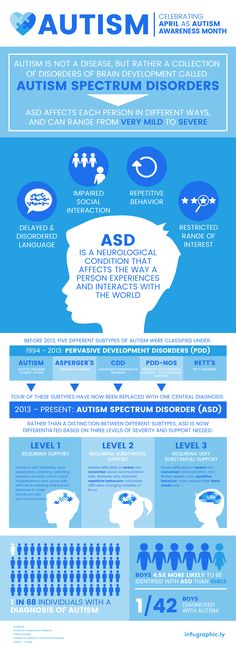 The gaze of such children is directed at the face of a person, but they look "through" this person. Such children enjoy the stereotyped reproduction of individual impressions.
The gaze of such children is directed at the face of a person, but they look "through" this person. Such children enjoy the stereotyped reproduction of individual impressions.
Extreme difficulty in organizing communication and interaction. Autism at its mildest. Children are characterized by increased vulnerability, contact with the world stops at the slightest sensation of obstacles. These children can make eye contact. nine0003
- Asperger's Syndrome. Formed from birth. Children have an early onset of speech development, a rich vocabulary, developed logical thinking, and there are no disorders in mental development. But at the same time, the communicative side of speech suffers: such children do not know how to establish contact with other people, do not listen to them, can talk to themselves, do not keep a distance in communication, and do not know how to empathize with other people.
- Rett syndrome. Its peculiarity lies in the fact that the development of a child up to 1-1.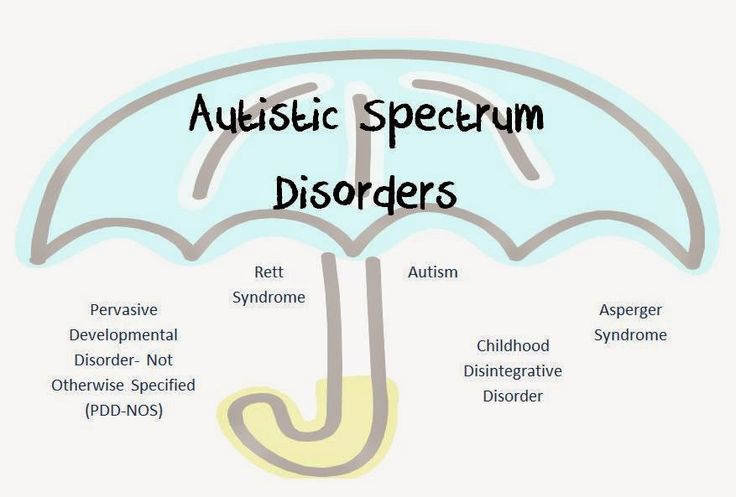 5 years proceeds normally, but then the newly acquired speech, motor and subject-role skills begin to disintegrate. Characteristic for this condition are stereotypical, monotonous movements of the hands, rubbing, wringing, while not carrying a purposeful character. The rarest of the presented diseases, occurring almost always only in girls. nine0003
5 years proceeds normally, but then the newly acquired speech, motor and subject-role skills begin to disintegrate. Characteristic for this condition are stereotypical, monotonous movements of the hands, rubbing, wringing, while not carrying a purposeful character. The rarest of the presented diseases, occurring almost always only in girls. nine0003
- Childhood psychosis. The first manifestation of symptoms before 3 years of age. It is characterized by violations of social behavior, communication disorders. There are stereotypes in behavior (children run in a monotonous circle, sway while standing and sitting, fingering their fingers, shaking their hands). These children have eating disorders: they can swallow food without chewing. Their unclear speech can sometimes be an incoherent collection of words. There are times when children freeze in place, like dolls. nine0003
- Atypical autism. It differs from autism in terms of age manifestation and the absence of one criterion from the “triad” of major disorders.
Correction of patients with ASD
One of the most important sections of habilitation for children with ASD is undoubtedly the provision of psycho-correctional and social rehabilitation assistance, with the formation of social interaction and adaptation skills. Comprehensive psycho-correctional work, which includes all sections and types of rehabilitation assistance, which will be described below, is, along with drug therapy, an effective means of stopping the negative symptoms of ASD, and also contributes to the normal inclusion of the child in society. Types of RAS correction: nine0003
1) Psychological correction - the most common and well-known type; It is characterized by a fairly wide range of methods, of which the TEACCH and ABA-therapy programs are most widely used and recognized in the world.
The first program is based on the following principles:
- The characteristics of each individual child are interpreted on the basis of observations of him, and not from theoretical ideas;
- increasing adaptation is carried out both by learning new skills and by adapting existing ones to the environment; nine0003
- Creation of an individual training program for each child; use of structured learning; holistic approach to intervention.
The second program is largely based on learning, which depends on the consequences that have arisen after the behavior. Consequences can be in the form of punishment or reward. In this model, it is necessary to highlight the main methods, such as the procedure for creating a contour and reinforcing behavior similar to the target; method of teaching chains of behavior; method of teaching discrimination of stimuli. nine0003
2) Neuropsychological correction - this type includes a set of exercises consisting of stretching, breathing, oculomotor, facial and other exercises for the development of the communicative and cognitive sphere, and the exercises themselves differ markedly in time and quantity.
3) Work with the child's family and environment - first of all, this type of correction is aimed at alleviating emotional tension and anxiety among family members, since parents of children with ASD often also need help, including psychotherapeutic support and training programs (such programs are mainly aimed at developing feelings of understanding of the problem, the reality of its solution and the meaningfulness of behavior in the current family situation).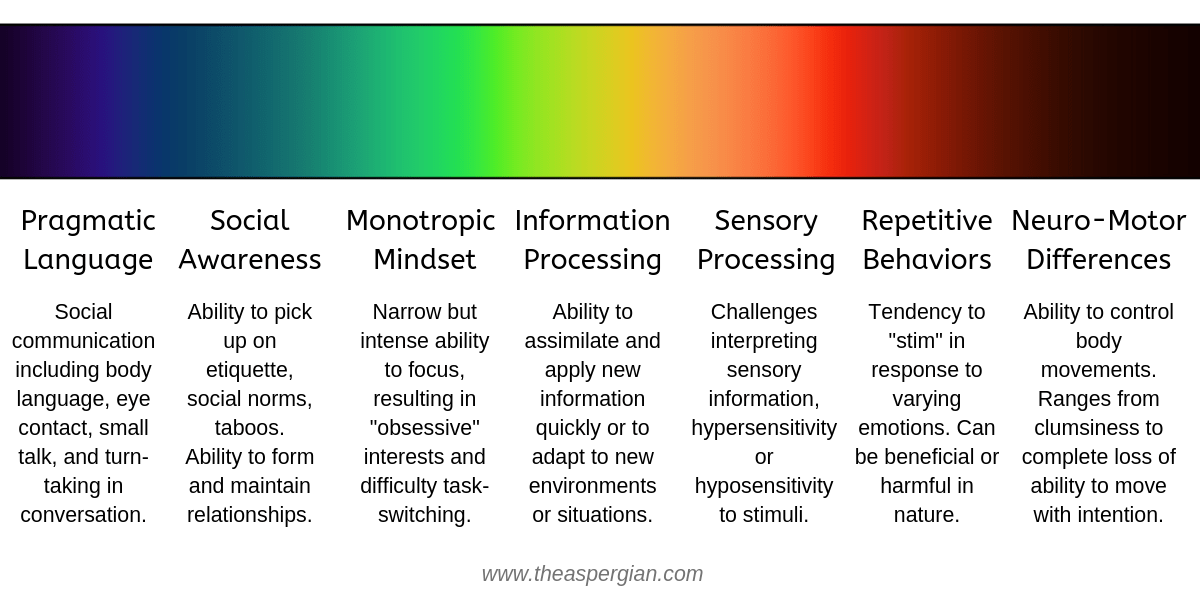 nine0003
nine0003
4) Psychosocial therapy - in fact, work with the child himself to form the cognitive, emotional and motivational-volitional resources of the individual for the possibility of further social adaptation, the need for which becomes more pronounced as the child with ASD grows older.
5) Logopedic correction - given the fact that speech development disorder is one of the cardinal manifestations of ASD, this type of work with a child will be an integral part of the correction program. It is characterized by a focus on the formation of vocabulary, the development of auditory attention, as well as phonetic and speech hearing. nine0003
6) Medical correction of RAS. In some forms of autism, medication is needed for the child. For example, to improve concentration and perseverance, a doctor may prescribe vitamins and nootropic drugs that improve thinking processes and stimulate speech development. And with high impulsivity, aggression, negativism, pronounced signs of "withdrawal into oneself", psychotropic drugs can help. In some cases, autism is combined with epileptic seizures. In such cases, anti-seizure medications are needed. Many mothers are afraid of drugs. But drugs are prescribed for a certain period, and not forever. Adverse drug reactions are rare. And the result of the effect in most cases is worth the courage of the parents. In each case, it is necessary to individually decide what kind of therapy is needed. And the doctor should be able to clearly explain to parents all questions regarding medications. nine0003
In some cases, autism is combined with epileptic seizures. In such cases, anti-seizure medications are needed. Many mothers are afraid of drugs. But drugs are prescribed for a certain period, and not forever. Adverse drug reactions are rare. And the result of the effect in most cases is worth the courage of the parents. In each case, it is necessary to individually decide what kind of therapy is needed. And the doctor should be able to clearly explain to parents all questions regarding medications. nine0003
The Children's Diagnostic Center in Domodedovo has all the facilities for diagnosing Autism Spectrum Disorders. Such as: examination by a child neurologist, clinical psychologist, speech therapist, examination - electroencephalography and video EEG monitoring. As well as correction techniques, such as ABA therapy.
Alpatsky D.A. (chief physician, neurologist of DDC), Litvinova E.V. (psychologist DDC)
Applied Behavior Analysis (ABA)
- 0 Popular Topics
- Air pollution
- Coronavirus disease (COVID-19)
- Hepatitis
- Data and statistics »
- Newsletter
- The facts are clear
- Publications
- E
- Yu
- I
- WHO in countries »
- Reporting
- Regions »
- Africa
- America
- Southeast Asia
- Europe
- Eastern Mediterranean
- Western Pacific
- Media Center
- Press releases
- Statements
- Media messages nine0202 Comments
- Reporting
- Online Q&A
- Developments
- Photo reports
- Questions and answers
- Latest information
- Emergencies "
- News "
- Disease Outbreak News
- WHO data »
- Dashboards »
- COVID-19 Monitoring Dashboard
- Highlights "
- About WHO »
- General director
- About WHO
- WHO activities
- Where does WHO work?
- Governing Bodies »
- World Health Assembly
- Executive committee
- Main page/
- Media Center/ nine0202 Newsletters/
- Read more/
- Autism
Key Facts
- Autism, also called autism spectrum disorder, is a diverse group of pathological conditions caused by the development of the brain.
- Signs of autism can be detected in early childhood, but it is often not diagnosed until later in life.
- Approximately 1 in 100 children have autism.
- The abilities and needs of people with autism can vary and change over time. Some people with autism are able to lead independent and productive lives, while others become severely disabled and require lifelong care and support.
- Evidence-based psychosocial interventions lead to improved communication skills and social behavior that positively impact the well-being and quality of life of people with autism and their caregivers. nine0488
- Care for people with autism must be accompanied by local and community action to make physical and social environments and relationships more accessible, inclusive and supportive.
Introduction
Autism Spectrum Disorders (ASD) are a group of different conditions. All of them are characterized by certain difficulties with social interaction and communication. Other features include atypical patterns of action and behaviors, such as difficulty moving from one activity to another, focus on details, and unusual responses to external stimuli. nine0003
All of them are characterized by certain difficulties with social interaction and communication. Other features include atypical patterns of action and behaviors, such as difficulty moving from one activity to another, focus on details, and unusual responses to external stimuli. nine0003
The abilities and needs of people with autism can vary and change over time. Some people with autism are able to live independent and productive lives, while others become severely disabled and require lifelong care and support. Autism often negatively affects educational or employment opportunities. In addition, for family members of people with autism, care and support responsibilities can often be a source of significant stress. Community attitudes and the level of support from local and national governments are important determinants of the quality of life of people with autism. nine0003
Signs of autism can be identified in early childhood, but the condition is often diagnosed at much later stages.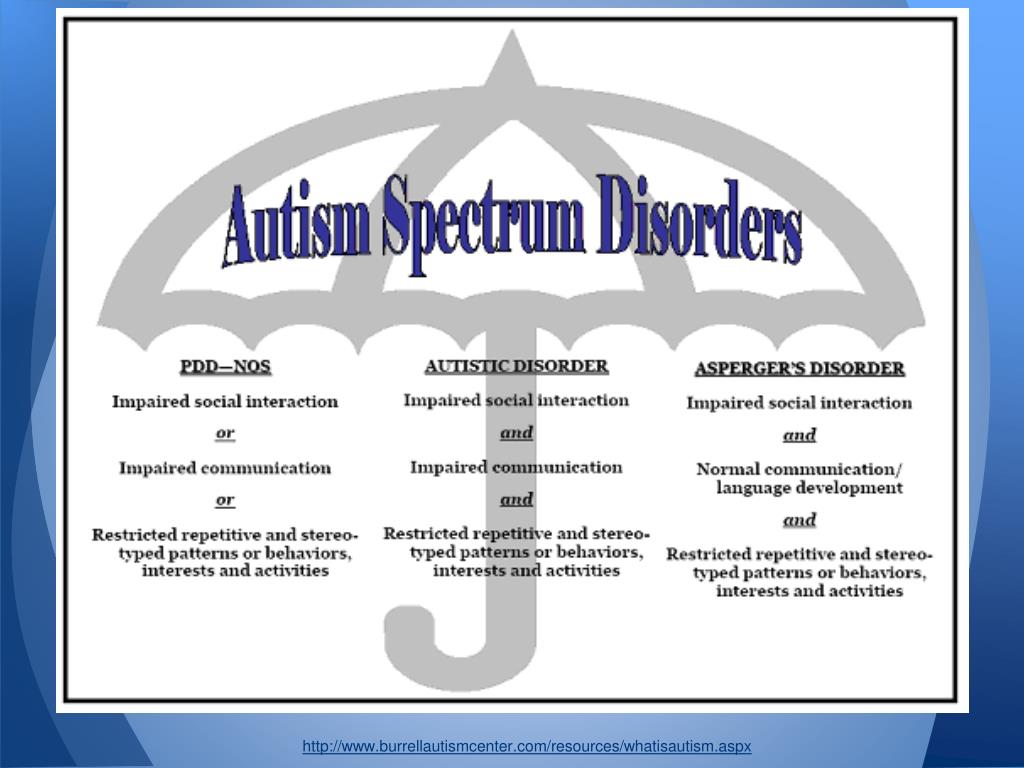
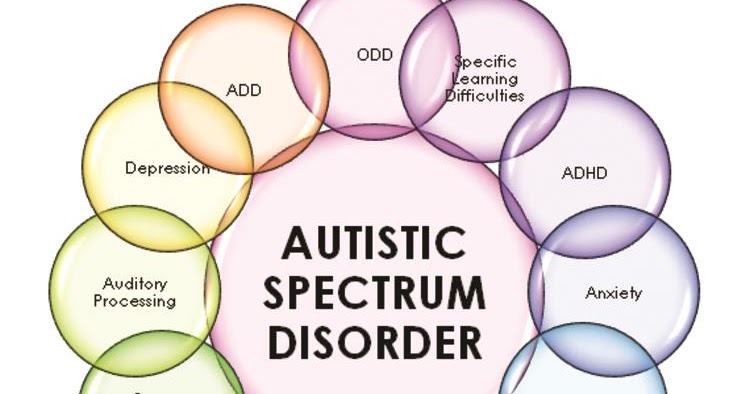
People with autism often have comorbid conditions and illnesses, including epilepsy, depression, anxiety, and attention deficit hyperactivity disorder, as well as behavioral problems such as sleep disturbances or self-harm. The level of intellectual abilities of people with autism varies in a wide range from severe cognitive impairment to a high level of intelligence. nine0003
Epidemiology
It is estimated that autism affects about 1 in 100 children worldwide (1). At the same time, we are talking about an average indicator, and the prevalence rates of autism recorded according to different studies vary widely. Nevertheless, according to some reputable controlled studies, the real numbers are much higher. The prevalence of autism in many low- and middle-income countries is unknown.
Causes
Available scientific evidence indicates many factors that may increase the likelihood of children developing autism, including environmental and genetic factors.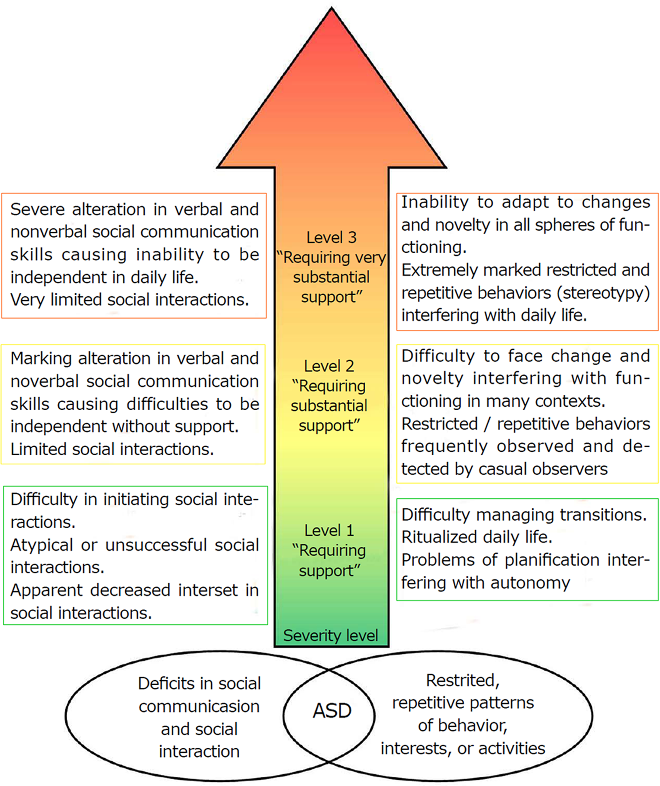
Available epidemiological data do not support a causal relationship between autism and measles, mumps and rubella vaccination. Past studies suggesting such a causal relationship have been many methodological problems were found (2), (3). nine0003
Similarly, there is no evidence that any childhood vaccine can increase the risk of developing autism. Evidence reviews on a potential association between the preservative thiomersal and aluminum adjuvants contained in inactivated vaccines and the risk of developing autism strongly suggest that vaccines do not lead to an increase in this risk.
Needs Assessment and Care Management
A range of interventions, from early childhood and throughout life, can contribute to the optimal development, well-being and quality of life of people with autism. Timely evidence-based psychosocial interventions at an early age can improve the ability of children with autism to communicate and interact effectively with others.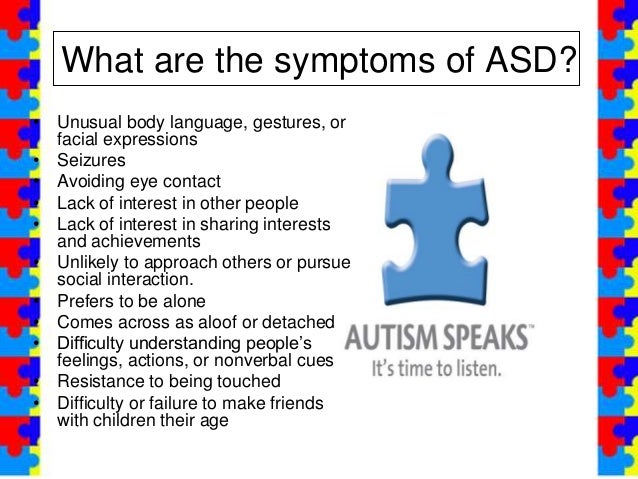 It is recommended to monitor the development of children as part of the planned provision of medical care to mothers and children. nine0003
It is recommended to monitor the development of children as part of the planned provision of medical care to mothers and children. nine0003
It is important that immediately after diagnosis, children, adolescents and adults diagnosed with autism and their caregivers have access to relevant information, referrals and practical support tailored to their individual needs. constantly changing needs and preferences.
The health care needs of people with autism are complex, requiring them to provide comprehensive services, including health promotion, care and rehabilitation services. Therefore, it is important to ensure cooperation with other sectors, in particular with the education system, employment and the social sector. nine0003
Interventions to help people with autism and other developmental disabilities should be planned and implemented with the participation of people with these conditions themselves. Caring for people with autism should be accompanied by local action. and at the level of society as a whole, in order to make the physical and social environment and relationships more accessible, inclusive and supportive.
and at the level of society as a whole, in order to make the physical and social environment and relationships more accessible, inclusive and supportive.
Human rights
All people, including those with autism, have the right to the highest attainable standard of physical and mental health. nine0003
Yet people with autism often face stigma and discrimination: their health care and education rights are unfairly denied, and their opportunities to participate in society are limited.
People with autism may experience the same health problems as the rest of the population. In addition, they may have special health care needs related to autism and other related conditions. They can be are more vulnerable to chronic noncommunicable diseases associated with behavioral risk factors such as physical inactivity and poor diet, and are at greater risk of violence, injury and abuse. nine0003
People with autism, like the rest of the population, need affordable health services to meet general health needs, including health promotion and prevention services, as well as acute and chronic care.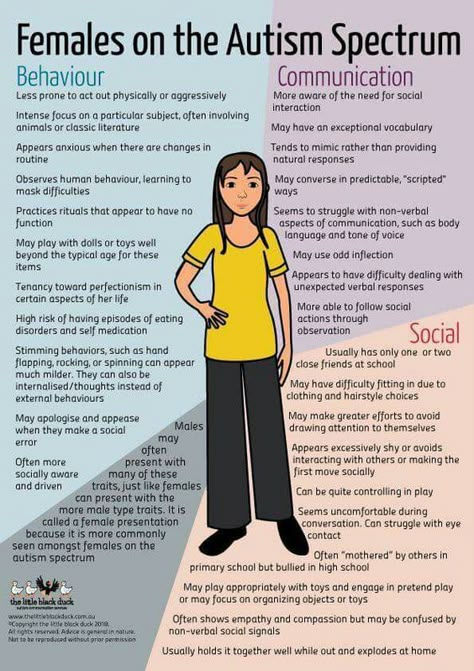 However less than in the general population, the level of satisfaction of the medical needs of people with autism is at a lower level. These people are also more vulnerable in humanitarian emergencies. One of the common barriers is the insufficient level of knowledge and understanding of the specifics of autism by medical professionals. nine0003
However less than in the general population, the level of satisfaction of the medical needs of people with autism is at a lower level. These people are also more vulnerable in humanitarian emergencies. One of the common barriers is the insufficient level of knowledge and understanding of the specifics of autism by medical professionals. nine0003
WHO Resolution on Autism Spectrum Disorders
In May 2014, the Sixty-seventh World Health Assembly adopted a resolution on "Comprehensive and concerted efforts for the management of autism spectrum disorders", supported by over 60 countries.
The resolution calls on WHO to work with Member States and partner agencies to strengthen national capacity to address ASD and other developmental disabilities. nine0003
WHO activities
WHO and its partners recognize the need to strengthen the capacity of countries to promote the optimal health and well-being of all people with autism.
The main activities of WHO in this regard are:
- promoting targeted action by national governments to improve the quality of life of people with autism;
- develop recommendations for policies and action plans to address autism in the broader context of physical, mental, brain health and care for people with disabilities; nine0203
- help empower healthcare professionals to provide appropriate and effective care for people with autism and achieve optimal health and well-being; and
- Promoting an inclusive and supportive environment for people with autism and other developmental disabilities and providing support to their caregivers.
WHO Comprehensive Mental Health Action Plan 2013–2030 and World Health Assembly Resolution WHA73.10 "Global action against epilepsy and other neurological disorders" contain calling on countries to address significant gaps in the early detection, care, treatment and rehabilitation of people with mental and neurodevelopmental disorders, including and autism. The resolution also calls on countries to take action to meet the social, economic, educational and other needs of people living with mental and neurological disorders and their families, and to develop surveillance and related research activities. nine0003
References
(1) Global prevalence of autism: A systematic review update. Zeidan J et al. Autism Research 2022 March.
(2) Wakefield's affair: 12 years of uncertainty whereas no link between autism and MMR vaccine has been proven. Maisonneuve H, Floret D. Presse Med. 2012 Sep; French https://pubmed.