Intermittent explosive disorder icd 10
2023 ICD-10-CM Diagnosis Code F63.81: Intermittent explosive disorder
- ICD-10-CM Codes ›
- F01-F99 ›
- F60-F69 ›
- F63- ›
- 2023 ICD-10-CM Diagnosis Code F63.81
Intermittent explosive disorder
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
- F63.81 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
- The 2023 edition of ICD-10-CM F63.81 became effective on October 1, 2022.
- This is the American ICD-10-CM version of F63.81 - other international versions of ICD-10 F63.81 may differ.
The following code(s) above F63. 81 contain annotation back-references
Annotation Back-References
In this context, annotation back-references refer to codes that contain:
- Applicable To annotations, or
- Code Also annotations, or
- Code First annotations, or
- Excludes1 annotations, or
- Excludes2 annotations, or
- Includes annotations, or
- Note annotations, or
- Use Additional annotations
that may be applicable to F63.81:
- F01-F99
2023 ICD-10-CM Range F01-F99
Mental, Behavioral and Neurodevelopmental disorders
Includes
- disorders of psychological development
Type 2 Excludes
- symptoms, signs and abnormal clinical laboratory findings, not elsewhere classified (R00-R99)
- F63
ICD-10-CM Diagnosis Code F63
Impulse disorders
- 2016 2017 2018 2019 2020 2021 2022 2023 Non-Billable/Non-Specific Code
Type 2 Excludes
- habitual excessive use of alcohol or psychoactive substances (F10-F19)
- impulse disorders involving sexual behavior (F65.
 -)
-)
Approximate Synonyms
- Explosive disorder, intermittent
- Explosive disorder, isolated
- Isolated explosive disorder
Clinical Information
- A disorder characterized by recurrent episodes of serious assaultive acts or destruction of property due to a failure to resist aggressive impulses; the degree of aggression during these episodes is grossly out of proportion to any psychosocial provocation. The aggressive episodes are not etiologically linked to another mental disorder, a general medical condition, or substance use.
ICD-10-CM F63.81 is grouped within Diagnostic Related Group(s) (MS-DRG v40.0):
- 883 Disorders of personality and impulse control
Convert F63. 81 to ICD-9-CM
81 to ICD-9-CM
Code History
- 2016 (effective 10/1/2015): New code (first year of non-draft ICD-10-CM)
- 2017 (effective 10/1/2016): No change
- 2018 (effective 10/1/2017): No change
- 2019 (effective 10/1/2018): No change
- 2020 (effective 10/1/2019): No change
- 2021 (effective 10/1/2020): No change
- 2022 (effective 10/1/2021): No change
- 2023 (effective 10/1/2022): No change
Diagnosis Index entries containing back-references to F63.81:
- Disorder (of) - see also Disease
- intermittent explosive F63.81
ICD-10-CM Codes Adjacent To F63. 81
81
F60.8 Other specific personality disorders
F60.81 Narcissistic personality disorder
F60.89 Other specific personality disorders
F60.9 Personality disorder, unspecified
F63 Impulse disorders
F63. 0 Pathological gambling
0 Pathological gambling
F63.1 Pyromania
F63.2 Kleptomania
F63.3 Trichotillomania
F63.8 Other impulse disorders
F63.81 Intermittent explosive disorder
F63. 89 Other impulse disorders
89 Other impulse disorders
F63.9 Impulse disorder, unspecified
F64 Gender identity disorders
F64.0 Transsexualism
F64.1 Dual role transvestism
F64.2 Gender identity disorder of childhood
F64. 8 Other gender identity disorders
8 Other gender identity disorders
F64.9 Gender identity disorder, unspecified
F65 Paraphilias
F65.0 Fetishism
Reimbursement claims with a date of service on or after October 1, 2015 require the use of ICD-10-CM codes.
ICD-9-CM Diagnosis Code 312.34 : Intermittent explosive disorder
Home > 2015 ICD-9-CM Diagnosis Codes > Mental Disorders 290-319 > Neurotic Disorders, Personality Disorders, And Other Nonpsychotic Mental Disorders 300-316 > Disturbance of conduct not elsewhere classified 312-
2015 ICD-9-CM Diagnosis Code 312. 34
34
Intermittent explosive disorder
- 2015
- Billable Thru Sept 30/2015
- Non-Billable On/After Oct 1/2015
- ICD-9-CM 312.34 is a billable medical code that can be used to indicate a diagnosis on a reimbursement claim, however, 312.34 should only be used for claims with a date of service on or before September 30, 2015. For claims with a date of service on or after October 1, 2015, use an equivalent ICD-10-CM code (or codes).
Convert to ICD-10-CM: 312.34 converts approximately to:
- 2015/16 ICD-10-CM F63.81 Intermittent explosive disorder
Approximate Synonyms
- Explosive disorder, intermittent
Clinical Information
- A disorder characterized by recurrent episodes of serious assaultive acts or destruction of property due to a failure to resist aggressive impulses; the degree of aggression during these episodes is grossly out of proportion to any psychosocial provocation.
 The aggressive episodes are not etiologically linked to another mental disorder, a general medical condition, or substance use
The aggressive episodes are not etiologically linked to another mental disorder, a general medical condition, or substance use
ICD-9-CM Volume 2 Index entries containing back-references to 312.34:
- Disorder - see also Disease
- explosive
- intermittent 312.34
- isolated 312.35
- intermittent explosive 312.34
- explosive
- Disturbance - see also Disease
- conduct 312.9
- adjustment reaction 309.3
- adolescent onset type 312.82
- childhood onset type 312.81
- compulsive 312.30
- intermittent explosive disorder 312.34
- isolated explosive disorder 312.35
- kleptomania 312.32
- pathological gambling 312.31
- pyromania 312.33
- hyperkinetic 314.2
- intermittent explosive 312.34
- isolated explosive 312.35
- mixed with emotions 312.4
- socialized (type) 312.20
- aggressive 312.23
- unaggressive 312.
 21
21
- specified type NEC 312.89
- undersocialized, unsocialized
- aggressive (type) 312.0
- unaggressive (type) 312.1
- conduct 312.9
| 312.33 | ICD9Data.com | 312.35 |
- 2015/Index · 2014/Index · 2013/Index
- 2012/Index · 2011/Index · 2010/Index
- 2009/Index · 2008/Index · 2007/Index
- About · Privacy Policy · Disclaimer
- 2016 ICD-10-CM Diagnosis Codes · Index
- Convert ICD-9-CM <-> 2016 ICD-10-CM
- 2016 ICD-10-PCS Procedure Codes
- 2016 · 2015 · 2014 · 2013 · 2012
- 2011 · 2010 · 2009 · 2008
Intermittent Explosive Disorder - frwiki.wiki
Intermittent temper disorder ( TEI ) is a behavioral disorder characterized by extreme expressions of anger, often to the point of violence, disproportionate to what is happening (see also Seb Buje's definition). It is currently classified in the Diagnostic and Statistical Manual of Mental Disorders as habit and impulse disorder. TEI belongs to axis I of the habit and impulse disorders listed in the DSM-IV-TR, which include kleptomania, pyromania, pathological gambling, and others. Impulsive aggression is not intentional and is defined by a disproportionate response to every perceived response. Some people report physiological changes (eg, tension, depression).
It is currently classified in the Diagnostic and Statistical Manual of Mental Disorders as habit and impulse disorder. TEI belongs to axis I of the habit and impulse disorders listed in the DSM-IV-TR, which include kleptomania, pyromania, pathological gambling, and others. Impulsive aggression is not intentional and is defined by a disproportionate response to every perceived response. Some people report physiological changes (eg, tension, depression).
A 2006 study shows that the prevalence is much higher than previously thought.
Prevalence is higher in men than in women. The disorder itself is not easily characterized and often comorbid with other mood disorders, especially bipolar disorder. People diagnosed with TEI report that their temper tantrums are short-lived (lasting an hour or less) and are accompanied by a variety of symptoms (sweating, heart palpitations). Violent acts are often reported accompanied by a sense of relief or even in some cases pleasure, but subsequently accompanied by remorse. Then the person is in a phase of complete loss of control. Moments of extreme anger followed a hidden headache, severe chest pain (sharp burning) and eye pain (or even red eyes). Which sometimes leads to death.
Then the person is in a phase of complete loss of control. Moments of extreme anger followed a hidden headache, severe chest pain (sharp burning) and eye pain (or even red eyes). Which sometimes leads to death.
CV
- 1 Diagnosis
- 2 Treatment
- 3 links
- 4 External link
Diagnostic
Diagnostic criteria for DSM-IV include: inability to resist aggressive urges, level of aggression expressed during a highly disproportionate episode in the face of a provocation or source of psychosocial stress, and, as previously explained, a diagnosis is made when other mental disorders that may be harmful (eg, antisocial personality disorder, borderline personality). At a distance, acts of aggression cannot be caused by a common disease, for example. head injuries, Alzheimer's disease, etc. as a result of long-term drug use or drug abuse. The diagnosis is made when the emotional and behavioral symptoms meet the criteria specified in the DSM-IV.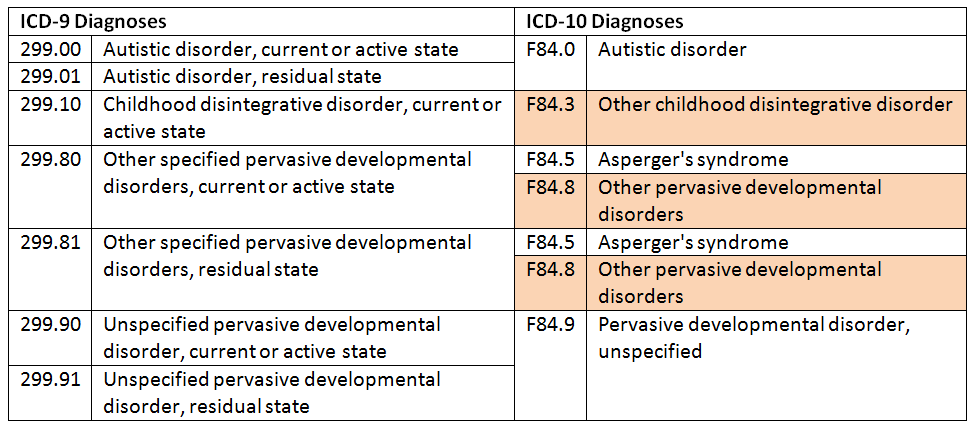
The DSM-IV-TR is very selective in its definitions of intermittent explosive disorder, which essentially defines the exclusion of other conditions. Diagnosis requires:
- Several episodes of impulsive behavior that could result in very serious damage to another person or property.
- The level of aggression is grossly disproportionate to the circumstances or the provocation.
- Episodic violence cannot be caused by another physical or mental illness.
Care
Treatment, which requires, inter alia, cognitive behavioral therapy and psychotropic drugs, has shown temporary success. Therapy can help the patient recognize their impulsivity and control it. Patients with TEI are prescribed several drugs.
Of the tricyclic antidepressants and selective serotonin reuptake inhibitors such as fluoxetine, fluvoxamine and sertraline appear to relieve some psychopathological symptoms.
Recommendations
- ↑ Diagnostic and Statistical Manual of Mental Disorders: DSM-IV , Washington, DC, American Psychiatric Association , 943 p.
 (ISBN 0-89042-025-4) , 663–7
(ISBN 0-89042-025-4) , 663–7 - ↑ (in) McElroy S. L., Recognition and treatment of intermittent explosive disorder DSM-IV , theft. 60 Appendix 15, , 12–6 p. (PMID 10418808)
- ↑ (in) Boyd, Mary Ann, The Psychiatric Nurse: Modern Practice , Philadelphia, Wolters Kluwer Health / Lippincott Williams & Wilkins, , 820–1 pp. (ISBN 0-7817-9169-3)
- ↑ a b and c (ru) McElroy SL, Soutullo CA, Beckman DA, Taylor P, Keck PE, DSM-IV intermittent explosive disorder: report of 27 cases , T.
 59, , 203–10; quiz 211 p. (PMID 95
59, , 203–10; quiz 211 p. (PMID 95- , DOI 10.4088 / JCP.v59n0411)
- ↑ (in) McCloskey, MS, Noblett, KL, Deffenbacher, JL Gollan, JK Coccaro, EF (2008) Cognitive behavioral therapy for intermittent explosive disorder: a pilot randomized clinical trial. 76(5), 876-886.
External link
- (en) « Impulsive Disorder Management Clinic at the University of Minnesota » ( Archive • Wikiwix • Archive.is • Google • What to do? )
| Mental and behavioral disorders (ICD-10: F00-F99) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||
| |||||||||||||
| |||||||||||||
| |||||||||||||
| |||||||||||||
| |||||||||||||
| |||||||||||||
| |||||||||||||

Traumatology and orthopedic department №10
8 (3522) 45-33-57, 45-43-06
Block B, 2nd floor ensure the transition of a patient with an axial skeletal pathology, i.e. diseases of the spine, spinal cord, deformities of the chest and pelvis to a qualitatively higher level of support and movement.
History and background of creation:
Traumatology and orthopedic department No. 10 was organized in 2015 on the basis of the department of vertebrology and neurosurgery.
Scientific group and department of vertebrology and neurosurgery was organized in 1993. Khudyaev Alexander Timofeevich headed the department and clinical group. Under the leadership of A.T. Khudyaev, the use of an external transpedicular fixation apparatus was started in the treatment of patients with traumatic injuries of the spine, scoliotic and kyphotic deformities, and spondylolisthesis.
The first experimental work on the spine refers to the end of 1974. In 1978-1979. A.M. Markhashov under the direction of G.A. Ilizarov created a pin apparatus for fixing the vertebrae of dogs and began the development of an apparatus for fixing the human spine.
In 1978-1979. A.M. Markhashov under the direction of G.A. Ilizarov created a pin apparatus for fixing the vertebrae of dogs and began the development of an apparatus for fixing the human spine.
The studies were carried out from 1983 to 1985 and included many aspects. Researchers were: A.M. Markhashov, K.P. Kirsanov, Yu.A. Mushtaeva, G.D. Safonova, P.I. Kovalenko, L.O. Marchenkova, I.A. Menshchikov. The work opened a new page in spinal surgery.
External transpedicular fixation of the spine has become an innovative method for the treatment of patients with spinal pathology. Controlled dosed controlled extrafocal impact on the spine was based on the philosophy of the method of G.A. Ilizarov and was its continuation. This method of correcting spinal deformities of various etiologies with the possibility of creating conditions for spinal fusion was a pioneering alternative direction for existing fixation devices.
January 1993 a scientific group and a department of vertebrology and neurosurgery have been organized at the RRC VTO./imgs/2018/04/24/07/2145384/d11f8ff1e9138af1ff3e97a83f223157d6fe943d.jpg) The head of the department and the head of the clinical group was appointed Ph.D. Khudyaev Alexander Timofeevich. Under the leadership of A.T. Khudyaev, the use of an external transpedicular fixation apparatus was started in the treatment of patients with traumatic injuries of the spine, scoliotic and kyphotic deformities, and spondylolisthesis. In the years when modern submersible implants were not available in Russia, the external transpedicular fixation apparatus became the main tool in the treatment of patients with acute spinal cord and spinal cord injury, patients with the consequences of trauma, for the correction of scoliotic and kyphotic spinal deformities and spondylolisthesis.
The head of the department and the head of the clinical group was appointed Ph.D. Khudyaev Alexander Timofeevich. Under the leadership of A.T. Khudyaev, the use of an external transpedicular fixation apparatus was started in the treatment of patients with traumatic injuries of the spine, scoliotic and kyphotic deformities, and spondylolisthesis. In the years when modern submersible implants were not available in Russia, the external transpedicular fixation apparatus became the main tool in the treatment of patients with acute spinal cord and spinal cord injury, patients with the consequences of trauma, for the correction of scoliotic and kyphotic spinal deformities and spondylolisthesis.
In the future, the range of surgical interventions and applied methods of treating patients was constantly expanding. The main activities of the department were: the treatment of patients with spinal deformities of various etiologies, degenerative-dystrophic diseases and the use of neuromodulation techniques in patients with the consequences of damage to the spinal cord and peripheral nerves. Since January 2015, on the basis of the neurosurgical department, the traumatology and orthopedic department No. 10 has been formed.
Since January 2015, on the basis of the neurosurgical department, the traumatology and orthopedic department No. 10 has been formed.
Currently, the main clinical and scientific direction of the department's activity is the surgical treatment of adult patients with spinal deformities of various origins, degenerative diseases, spinal injuries, consequences of injuries and previous surgical interventions. For this, modern diagnostic tools, the latest treatment technologies and medical equipment are used.
The main concept of treatment
is not only surgical treatment of spinal pathology, but orthopedic, neurological and functional rehabilitation in general for patients with severe spinal pathology to improve the quality and life expectancy.
Employees
| Prudnikova Oksana Germanovna Head of the traumatological and orthopedic department No. 10. Doctor of Medical Sciences, neurosurgeon of the highest category, orthopedist-traumatologist, vertebrologist. Summary Download https://www.researchgate.net/profile/Oxana_Prudnikova?ev=prf_highl Contacts: (3522) 45 33 57, [email protected] | |
| Evsyukov Alexey Vladimirovich Candidate of Medical Sciences, neurosurgeon. Head of the Clinic for Spinal Pathology and Rare Diseases of the Ilizarov Center | |
| Khomchenkov Maxim Viktorovich Orthopedist-traumatologist, vertebrologist Junior Researcher, Scientific Clinical Experimental Laboratory of Axial Skeleton Pathology and Neurosurgery Resume download | |
| Kotelnikov Alexander Olegovich Traumatologist-orthopedist | |
| Garipov Ilgiz Ildarovich Orthopedist-traumatologist, PhD student | |
| Volynsky Alexey Leonidovich Neurosurgeon | |
| Kuzmenko Elmira Ismailovna Senior Nurse, Highest qualification category. Work experience at the Center since 2011. Diploma in the specialty "Medicine", qualification of a paramedic 1996.
| |
| Khlystova Yulia Alexandrovna Specialist LLP No. 10 Operating since 2006 Education: Higher pedagogical education |