How many people suffer from schizophrenia
Schizophrenia
Schizophrenia- All topics »
- A
- B
- C
- D
- E
- F
- G
- H
- I
- J
- K
- L
- M
- N
- O
- P
- Q
- R
- S
- T
- U
- V
- W
- X
- Y
- Z
- Resources »
- Fact sheets
- Facts in pictures
- Multimedia
- Publications
- Questions & answers
- Tools and toolkits
- Popular »
- Air pollution
- Coronavirus disease (COVID-19)
- Hepatitis
- Monkeypox
- All countries »
- A
- B
- C
- D
- E
- F
- G
- H
- I
- J
- K
- L
- M
- N
- O
- P
- Q
- R
- S
- T
- U
- V
- W
- X
- Y
- Z
- Regions »
- Africa
- Americas
- South-East Asia
- Europe
- Eastern Mediterranean
- Western Pacific
- WHO in countries »
- Statistics
- Cooperation strategies
- Ukraine emergency
- All news »
- News releases
- Statements
- Campaigns
- Commentaries
- Events
- Feature stories
- Speeches
- Spotlights
- Newsletters
- Photo library
- Media distribution list
- Headlines »
- Focus on »
- Afghanistan crisis
- COVID-19 pandemic
- Northern Ethiopia crisis
- Syria crisis
- Ukraine emergency
- Monkeypox outbreak
- Greater Horn of Africa crisis
- Latest »
- Disease Outbreak News
- Travel advice
- Situation reports
- Weekly Epidemiological Record
- WHO in emergencies »
- Surveillance
- Research
- Funding
- Partners
- Operations
- Independent Oversight and Advisory Committee
- WHO's Health Emergency Appeal 2023
- Data at WHO »
- Global Health Estimates
- Health SDGs
- Mortality Database
- Data collections
- Dashboards »
- COVID-19 Dashboard
- Triple Billion Dashboard
- Health Inequality Monitor
- Highlights »
- Global Health Observatory
- SCORE
- Insights and visualizations
- Data collection tools
- Reports »
- World Health Statistics 2022
- COVID excess deaths
- DDI IN FOCUS: 2022
- About WHO »
- People
- Teams
- Structure
- Partnerships and collaboration
- Collaborating centres
- Networks, committees and advisory groups
- Transformation
- Our Work »
- General Programme of Work
- WHO Academy
- Activities
- Initiatives
- Funding »
- Investment case
- WHO Foundation
- Accountability »
- Audit
- Programme Budget
- Financial statements
- Programme Budget Portal
- Results Report
- Governance »
- World Health Assembly
- Executive Board
- Election of Director-General
- Governing Bodies website
- Member States Portal
- Home/
- Newsroom/
- Fact sheets/
- Detail/
- Schizophrenia
Key facts
- Schizophrenia causes psychosis and is associated with considerable disability and may affect all areas of life including personal, family, social, educational, and occupational functioning.
- Stigma, discrimination, and violation of human rights of people with schizophrenia are common.
- More than two out of three people with psychosis in the world do not receive specialist mental health care.
- A range of effective care options for people with schizophrenia exist and at least one in three people with schizophrenia will be able to fully recover.
Schizophrenia is characterised by significant impairments in the way reality is perceived and changes in behaviour related to:
- persistent delusions: the person has fixed beliefs that something is true, despite evidence to the contrary;
- persistent hallucinations: the person may hear, smell, see, touch, or feel things that are not there;
- experiences of influence, control or passivity: the experience that one’s feelings, impulses, actions, or thoughts are not generated by oneself, are being placed in one’s mind or withdrawn from one’s mind by others, or that one’s thoughts are being broadcast to others;
- disorganized thinking, which is often observed as jumbled or irrelevant speech;
- highly disorganised behaviour e.
 g. the person does things that appear bizarre or purposeless, or the person has unpredictable or inappropriate emotional responses that interfere with their ability to organise their behaviour;
g. the person does things that appear bizarre or purposeless, or the person has unpredictable or inappropriate emotional responses that interfere with their ability to organise their behaviour; - “negative symptoms” such as very limited speech, restricted experience and expression of emotions, inability to experience interest or pleasure, and social withdrawal; and/or
- extreme agitation or slowing of movements, maintenance of unusual postures.
People with schizophrenia often also experience persistent difficulties with their cognitive or thinking skills, such as memory, attention, and problem-solving.
At least one third of people with schizophrenia experiences complete remission of symptoms (1). Some people with schizophrenia experience worsening and remission of symptoms periodically throughout their lives, others a gradual worsening of symptoms over time.
Magnitude and impact
Schizophrenia affects approximately 24 million people or 1 in 300 people (0. 32%) worldwide. This rate is 1 in 222 people (0.45%) among adults (2). It is not as common as many other mental disorders. Onset is most often during late adolescence and the twenties, and onset tends to happen earlier among men than among women.
32%) worldwide. This rate is 1 in 222 people (0.45%) among adults (2). It is not as common as many other mental disorders. Onset is most often during late adolescence and the twenties, and onset tends to happen earlier among men than among women.
Schizophrenia is frequently associated with significant distress and impairment in personal, family, social, educational, occupational, and other important areas of life.
People with schizophrenia are 2 to 3 times more likely to die early than the general population (3). This is often due to physical illnesses, such as cardiovascular, metabolic, and infectious diseases.
People with schizophrenia often experience human rights violations both inside mental health institutions and in community settings. Stigma against people with this condition is intense and widespread, causing social exclusion, and impacting their relationships with others, including family and friends. This contributes to discrimination, which in turn can limit access to general health care, education, housing, and employment.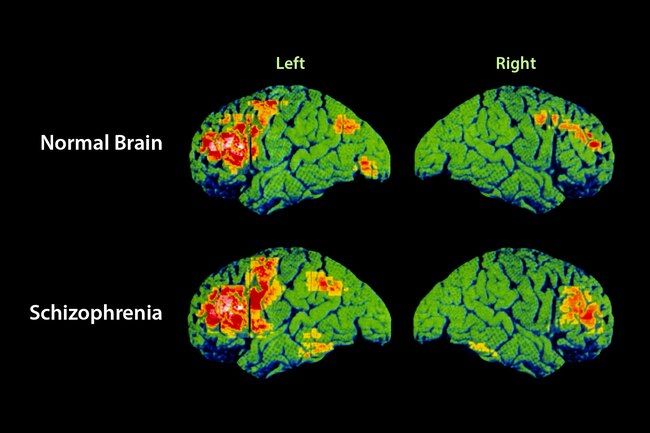
During humanitarian and public health emergencies, extreme stress and fear, breakdown of social supports, isolation and disruption of health-care services and supply of medication can occur. These changes can have an impact on the lives of people with schizophrenia, such as exacerbation of existing symptoms. During emergencies, people with schizophrenia are more vulnerable than others to various human rights violations, including neglect, abandonment, homelessness, abuse and exclusion.
Causes of schizophreniaResearch has not identified one single cause of schizophrenia. It is thought that an interaction between genes and a range of environmental factors may cause schizophrenia. Psychosocial factors may also affect the onset and course of schizophrenia. Heavy use of cannabis is associated with an elevated risk of the disorder.
ServicesCurrently, the vast majority of people with schizophrenia around the world are not receiving mental health care. Approximately 50% of people in mental hospitals have a schizophrenia diagnosis (4). Only 31.3% of people with psychosis receive specialist mental health care (5). Most resources for mental health services are inefficiently spent on care within mental hospitals.
Approximately 50% of people in mental hospitals have a schizophrenia diagnosis (4). Only 31.3% of people with psychosis receive specialist mental health care (5). Most resources for mental health services are inefficiently spent on care within mental hospitals.
There is clear evidence that mental hospitals are not effective in providing the care that people with mental health conditions need and, regularly, violate the basic human rights of persons with schizophrenia. Efforts to transfer care from mental health institutions to the community need to be expanded and accelerated. Such efforts start with the development of a range of quality community-based mental health services. Options for community-based mental health care include integration in primary health and general hospital care, community mental health centres, day centres, supported housing, and outreach services for home-based support. The engagement of the person with schizophrenia, family members and the wider community in providing support is important.
A range of effective care options for people with schizophrenia exist, and these include medication, psychoeducation, family interventions, cognitive-behavioural therapy and psychosocial rehabilitation (e.g., life skills training). Facilitated assisted living, supported housing and supported employment are essential care options that should be available for people with schizophrenia. A recovery-oriented approach – giving people agency in treatment decisions – is essential for people with schizophrenia and for their families and/or caregivers as well.
WHO responseWHO’s Comprehensive Mental Health Action Plan 2013-2030 highlights the steps required to provide appropriate services for people with mental disorders including schizophrenia. A key recommendation of the Action Plan is to shift services from institutions to the community. The WHO Special Initiative for Mental Health aims to further progress towards objectives of the Comprehensive Mental Health Action Plan 2013-2030 by ensuring 100 million more people have access to quality and affordable care for mental health conditions.
WHO's Mental Health Gap Action Programme (mhGAP) uses evidence-based technical guidance, tools and training packages to expand service in countries, especially in resource-poor settings. It focuses on a prioritized set of conditions, including psychosis, directing capacity building towards non-specialized health-care providers in an integrated approach that promotes mental health at all levels of care. Currently mhGAP is being implemented in more than 100 WHO Member States.
The WHO QualityRights Project involves improving the quality of care and human rights conditions in mental health and social care facilities and to empower organizations to advocate for the health of people with mental health conditions and psychosocial disabilities.
The WHO guidance on community mental health services and person-centred and rights-based approaches provides information and support to all stakeholders who wish to develop or transform their mental health system and services to align with international human rights standards including the UN Convention on the Rights of Persons with Disabilities.
(1) Harrison G, Hopper K, Craig T, Laska E, Siegel C, Wanderling J. Recovery from psychotic illness: a 15- and 25-year international follow-up study. Br J Psychiatry 2001;178:506-17.
(2) Institute of health Metrics and Evaluation (IHME). Global Health Data Exchange (GHDx). http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/27a7644e8ad28e739382d31e77589dd7 (Accessed 25 September 2021)
(3) Laursen TM, Nordentoft M, Mortensen PB. Excess early mortality in schizophrenia. Annual Review of Clinical Psychology, 2014;10, 425-438.
(4) WHO. Mental health systems in selected low- and middle-income countries: a WHO-AIMS cross-national analysis. WHO: Geneva, 2009
(5) Jaeschke K et al. Global estimates of service coverage for severe mental disorders: findings from the WHO Mental Health Atlas 2017 Glob Ment Health 2021;8:e27.
WHO’s Comprehensive Mental Health Action Plan 2013-2030
WHO Special Initiative for Mental Health
WHO's Mental Health Gap Action Programme (mhGAP)
WHO QualityRights Project
WHO guidance on community mental health services and person-centred and rights-based approaches
More on mental health
Schizophrenia – Fact Sheet - Treatment Advocacy Center
(January 2022) Schizophrenia is a chronic and severe brain disorder that interferes with a person’s ability to think clearly, manage emotions, make decisions and relate to others. Although it affects barely 1% of the population, it is one of the most disabling diseases affecting humankind.
Although it affects barely 1% of the population, it is one of the most disabling diseases affecting humankind.
Schizophrenia is a chronic and severe neurological brain disorder estimated in 2020 to affect 1.1 percent of the population or approximately 2.8 million adults in the United States aged 18 or older. An estimated 40 percent of individuals with the condition are untreated in any given year. Abnormalities that characterize schizophrenia include:
- delusions and hallucinations;
- alterations of the senses;
- an inability to sort and interpret incoming sensations, and an inability therefore to respond appropriately;
- an altered sense of self; and
- changes in emotions, movements and behavior.
Psychotic disorders nearly always emerge in late adolescence or early adulthood, with onset peaking between the ages of 18 and 25. The reasons for its appearance in this age range have not been identified. Some consensus already has emerged around the concept that psychotic breaks are not, as they may seem, abrupt but rather are the climax of a long buildup. In this model, they are rooted in molecular changes in the brain that begin as much as a decade before symptoms occur and progress to an end-stage psychosis in which reality surrenders to delusion, paranoia, hallucinations or other forms of disordered thinking.
In this model, they are rooted in molecular changes in the brain that begin as much as a decade before symptoms occur and progress to an end-stage psychosis in which reality surrenders to delusion, paranoia, hallucinations or other forms of disordered thinking.
For decades, research on the causes of schizophrenia has been dominated by theories related genetics and neurotransmitters. In the mid-2010s, a third theory–the infectious/inflammatory theory—became a major new addition to schizophrenia study.
Symptoms of Schizophrenia
In healthy people, the brain functions in such a way that incoming stimuli are sorted and interpreted, followed by a logical response (e.g., saying "thank you" after a gift is given, realizing the potential outcome of arriving late to work, etc.). Conversely, the inability of patients with schizophrenia to sort and interpret stimuli and select appropriate responses is one of the hallmarks of the disease.
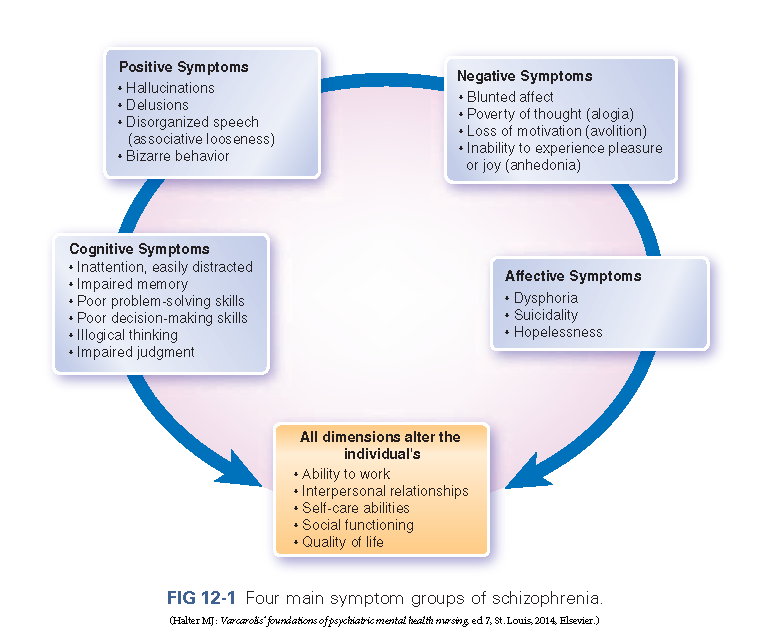
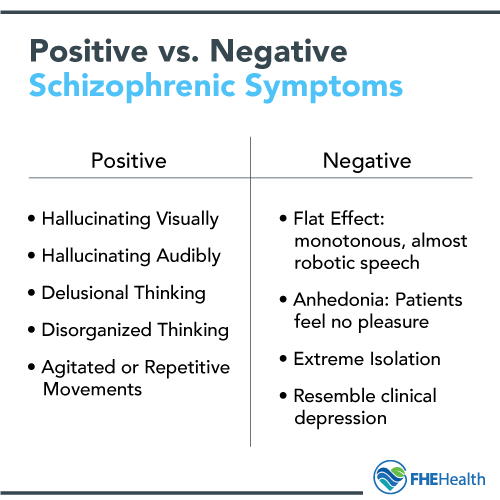
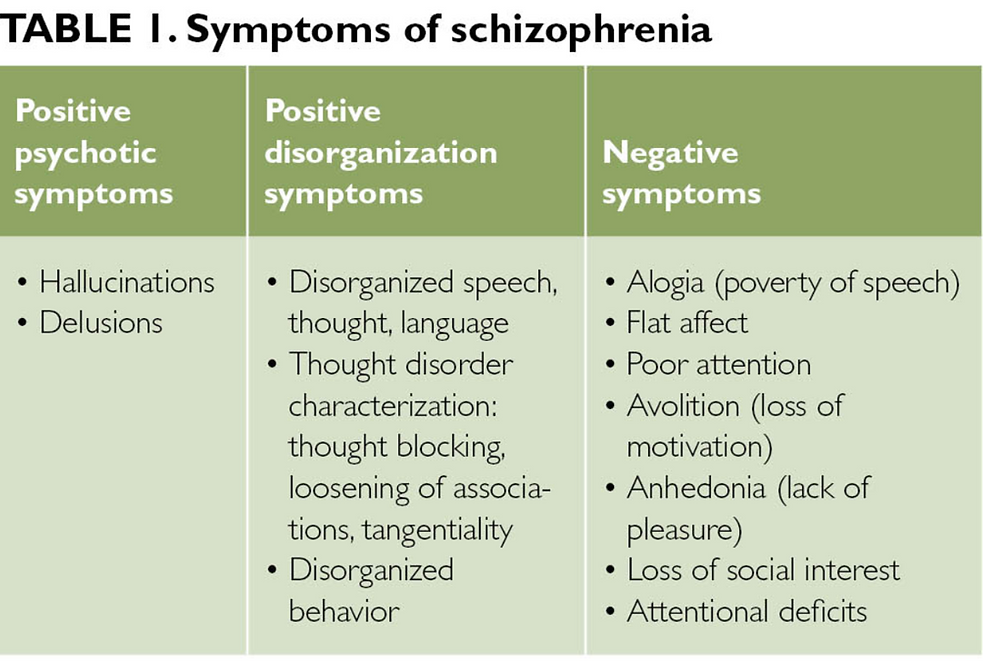
The symptoms of schizophrenia are generally divided into three categories: positive, negative and cognitive. The National Institute of Mental Illness (NIMH) publishes the following about the three categories of symptoms:
The National Institute of Mental Illness (NIMH) publishes the following about the three categories of symptoms:
Positive symptoms: “Positive” symptoms are psychotic behaviors not generally seen in healthy people. People with positive symptoms may “lose touch” with some aspects of reality. Symptoms include:
- Hallucinations
- Delusions
- Thought disorders
- Movement disorders (agitated body movements)
Negative symptoms: “Negative” symptoms are associated with disruptions to normal emotions and behaviors. Symptoms include:
- “Flat affect” (reduced expression of emotions via facial expression or voice tone)
- Reduced feelings of pleasure in everyday life
- Difficulty beginning and sustaining activities Reduced speaking
Cognitive symptoms: For some patients, the cognitive symptoms of schizophrenia are subtle, but for others, they are more severe and patients may notice changes in their memory or other aspects of thinking. Symptoms include:
Symptoms include:
- Poor “executive functioning” (the ability to understand information and use it to make decisions)
- Trouble focusing or paying attention
- Problems with “working memory” (the ability to use information immediately after learning it)
Diagnosing Schizophrenia
Although there are numerous abnormalities in the brain structure and function of individuals with schizophrenia, there is no single condition that can be tested or measured to produce a definitive diagnosis. Without such measures, the disease is diagnosed by its symptoms.
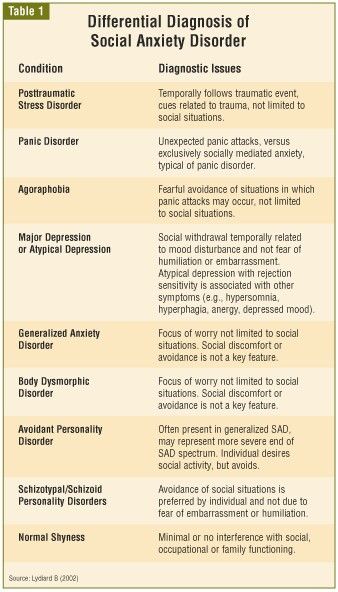
Prior to a medical diagnosis, it is critically important that a doctor rule out other problems that may mimic schizophrenia, such as psychotic symptoms caused by the use of drugs or other medical illnesses; major depressive episode or manic episode with psychotic features; delusional disorder (no hallucinations, disorganized speech or thought or "flattened" emotions) and autistic disorder or personality disorders (especially schizotypal, schizoid, or paranoid personality disorders). Schizoaffective disorder is a diagnosis used to indicate that the person has an illness with a mix of symptoms of both schizophrenia and bipolar disorder.
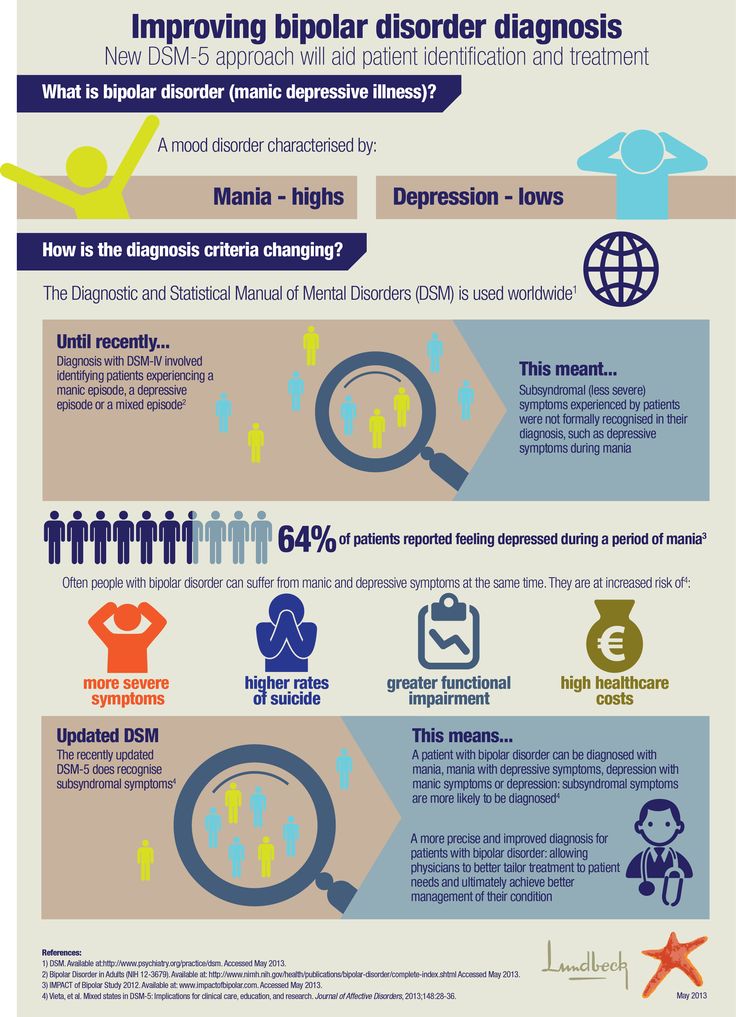
Schizoaffective disorder is a diagnosis used to indicate that the person has an illness with a mix of symptoms of both schizophrenia and bipolar disorder.
“Although there is no single symptom that is found only in schizophrenia, there are several that are found very uncommonly in diseases other than schizophrenia,” Dr. Torrey writes in Surviving Schizophrenia, now in its sixth edition as the authoritative book on the subject. “When they are present they should elevate the index of suspicion considerably….”
Precise diagnosis is of “utmost importance,” he writes. “It both determines the appropriate treatment for the patient and provides the patient and family with an informed prognosis. It also makes research on the disease easier because it allows researchers to be certain they are talking about the same thing.” It is important to diagnose and treat schizophrenia as early as possible to help people avoid or reduce frequent relapses and re-hospitalizations. Several promising, large-scale studies suggest early intervention may forestall the worst long-term outcomes of this devastating brain disorder.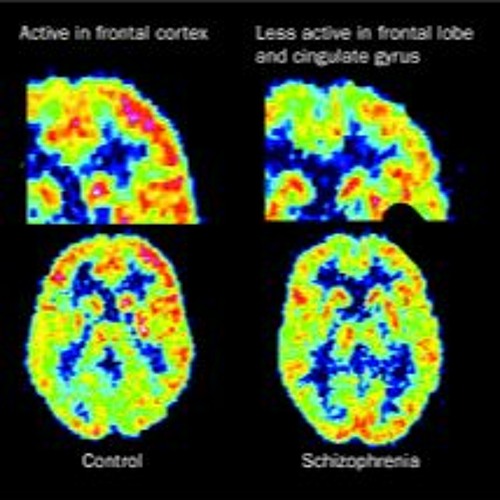
Treatments and Therapies
While there is no cure for schizophrenia, it is a highly treatable disorder. In fact, according to the National Advisory Mental Health Council, the treatment success rate for schizophrenia is comparable to the treatment success rate for heart disease. People who experience acute symptoms of schizophrenia may require intensive treatment, sometimes including hospitalization, to treat severe delusions or hallucinations, serious suicidal inclinations, inability to care for oneself or severe problems with drugs or alcohol.
It is critical that people with schizophrenia stay in treatment even after recovering from an acute episode. About 80 percent of those who stop taking their medications after an acute episode will have a relapse within one year, whereas only 30 percent of those who continue their medications will experience a relapse in the same time period. Because the causes of schizophrenia are still unknown, treatments focus on eliminating the symptoms of the disease. Antipsychotic drugs typically are used in the treatment of schizophrenia because they help relieve the positive symptoms. No treatments exist for negative symptoms of the disease.
Antipsychotic drugs typically are used in the treatment of schizophrenia because they help relieve the positive symptoms. No treatments exist for negative symptoms of the disease.
The NIMH publishes the following on treatments and therapies for schizophrenia:
- Antipsychotic medications: Antipsychotic medications are usually taken daily in pill or liquid form. Some antipsychotics are injections that are given once or twice a month. Some people have side effects when they start taking medications, but most side effects go away after a few days. Doctors and patients can work together to find the best medication or medication combination, and the right dose. Up-to-date information on medication use and side effects can be found on the U.S. Food and Drug Administration (FDA) website, including the latest information on warnings, patient medication guides, or newly approved medications.
- Psychosocial treatments: These treatments are helpful after patients and their doctor find a medication that works.
 Learning and using coping skills to address the everyday challenges of schizophrenia helps people to pursue their life goals, such as attending school or work. Individuals who participate in regular psychosocial treatment are less likely to have relapses or be hospitalized. For more information on psychosocial treatments, see the Psychotherapies webpage on the NIMH website.
Learning and using coping skills to address the everyday challenges of schizophrenia helps people to pursue their life goals, such as attending school or work. Individuals who participate in regular psychosocial treatment are less likely to have relapses or be hospitalized. For more information on psychosocial treatments, see the Psychotherapies webpage on the NIMH website. - Coordinated specialty care (CSC): This treatment model integrates medication, psychosocial therapies, case management, family involvement and supported education and employment services, all aimed at reducing symptoms and improving quality of life. The NIMH Recovery After an Initial Schizophrenia Episode (RAISE) research project seeks to fundamentally change the trajectory and prognosis of schizophrenia through coordinated specialty care treatment in the earliest stages of the disorder. RAISE is designed to reduce the likelihood of long-term disability that people with schizophrenia often experience and help them lead productive, independent lives.
Schizophrenia and Mortality
Individuals with schizophrenia die at a younger age than do healthy people. Males have a 5.1 greater than expected early mortality rate than the general population, and females have a 5.6 greater risk of early death. Suicide is the single largest contributor to this excess mortality rate, which is 10 to 13 percent higher in schizophrenia than the general population.
Suicide is in fact the number one cause of premature death among people with schizophrenia, with an estimated 10 percent to 13 percent killing themselves. The extreme depression and psychoses that can result due to lack of treatment are the usual culprits in these sad cases. These suicides rates can be compared to the general population, which is somewhere around 0.01%. Other contributors to excess mortality include:
- Accidents: Although individuals with schizophrenia do not drive as much as other people, studies have shown that they have double the rate of motor vehicle accidents per mile driven.
 A significant but unknown number of individuals with schizophrenia also are killed as pedestrians by motor vehicles.
A significant but unknown number of individuals with schizophrenia also are killed as pedestrians by motor vehicles. - Diseases: There is some evidence that individuals with schizophrenia have more infections, heart disease, type II (adult onset) diabetes, and female breast cancer, all of which might increase their mortality rate. Individuals with schizophrenia who become sick are less able to explain their symptoms to medical personnel, and medical personnel are more likely to disregard their complaints and assume that they are simply part of the illness. There also is evidence that some persons with schizophrenia have an elevated pain threshold so they may not complain of symptoms until the disease has progressed too far to be treatable.
- Homelessness: Although it has not been well studied to date, it appears that homelessness increases the mortality rate of individuals with schizophrenia by making them even more susceptible to accidents and diseases.
Additional information about schizophrenia is available from the following resources:
- Torrey, E.
 Fuller. (2013). Surviving Schizophrenia: A Family Manual (sixth edition). New York: Harper Perennial.
Fuller. (2013). Surviving Schizophrenia: A Family Manual (sixth edition). New York: Harper Perennial. - National Institute of Mental Illness (NIMH): Schizophrenia overview
- Treatment Advocacy Center. (2015). Clozapine for Treating Schizophrenia: A Comparison of the States
Schizophrenia
Schizophrenia- Healthcare issues »
- A
- B
- B
- G
- D
- E
- and
- 9000 About
- P
- P
- With
- T
- U
- F
- x
- S
- B
- E
- S
- I
005
- Popular Topics
- Air pollution
- Coronavirus disease (COVID-19)
- Hepatitis
- Data and statistics »
- News bulletin
- The facts are clear
- Publications
- Find country »
- A
- B
- C
- g
- D
- E
- and
- th
- K
- L
- 9000 N
- 9000
- in
- f
- x
- C
- hours
- Sh
- Sh.
- 9000 WHO in countries »
- Reporting
- Regions »
- Africa
- America
- Southeast Asia
- Europe
- Eastern Mediterranean
- Western Pacific
- Media Center
- Press releases
- Statements
- Media messages
- Comments
- Reporting
- Online Q&A
- Events
- Photo reports
- case studies
- Questions and answers
- Speeches
- Update
- Emergencies "
- News "
- Disease Outbreak News
- WHO data »
- Dashboards »
- COVID-19 Monitoring Dashboard
- Basic moments "
- About WHO »
- CEO
- About WHO
- WHO activities
- Where does WHO work?
- Governing Bodies »
- World Health Assembly
- Executive committee
- Main page/
- Media Center /
- Newsletters/
- Read more/
- Schizophrenia
Key Facts
- Schizophrenia is a severe mental disorder that affects approximately 24 million people, or 1 in 300 people worldwide.

- Schizophrenia causes psychosis, is associated with severe disability, and can negatively affect all areas of life, including personal, family, social, academic and work life.
- People with schizophrenia are often subject to stigma, discrimination and human rights violations.
- Worldwide, more than two thirds of people with psychosis do not receive specialized mental health care.
- There are a number of effective options for helping patients with schizophrenia, which can lead to a complete recovery of at least one in three patients.
Symptoms
Schizophrenia is characterized by significant disturbances in the perception of reality and behavioral changes, such as:
People with schizophrenia often also experience persistent cognitive or thinking problems that affect memory, attention, or problem-solving skills.
At least one third of patients with schizophrenia experience complete remission of symptoms (1). In some, periods of remission and exacerbation of symptoms follow each other throughout life, in others there is a gradual increase in symptoms.
Scope and impact
Schizophrenia affects approximately 24 million people, or 1 in 300 people (0.32%) worldwide. Among adults, the rate is 1 in 222 (0.45%) (2). Schizophrenia is less common than many other mental disorders. Onset is most common in late adolescence and between the ages of 20 and 30; while women tend to have a later onset of the disease.
Schizophrenia is often accompanied by significant stress and difficulties in personal relationships, family life, social contacts, studies, work or other important areas of life.
People with schizophrenia are 2-3 times more likely to die early than the population average (2). It is often associated with physical illnesses such as cardiovascular disease, metabolic disease, and infectious disease.
It is often associated with physical illnesses such as cardiovascular disease, metabolic disease, and infectious disease.
Patients with schizophrenia often become the object of human rights violations both within the walls of psychiatric institutions and in everyday life. Significant stigmatization of people with this disease is a widespread phenomenon that leads to their social isolation and has a negative impact on their relationships with others, including family and friends. This creates grounds for discrimination, which in turn limits access to health services in general, education, housing and employment.
Humanitarian emergencies and health crises can cause intense stress and fear, disrupt social support mechanisms, lead to isolation and disruption of health services and supply of medicines. All these shocks can have a negative impact on the lives of people with schizophrenia, in particular by exacerbating existing symptoms of the disease. People with schizophrenia are more vulnerable during emergencies to various human rights violations and, in particular, face neglect, abandonment, homelessness, abuse and social exclusion.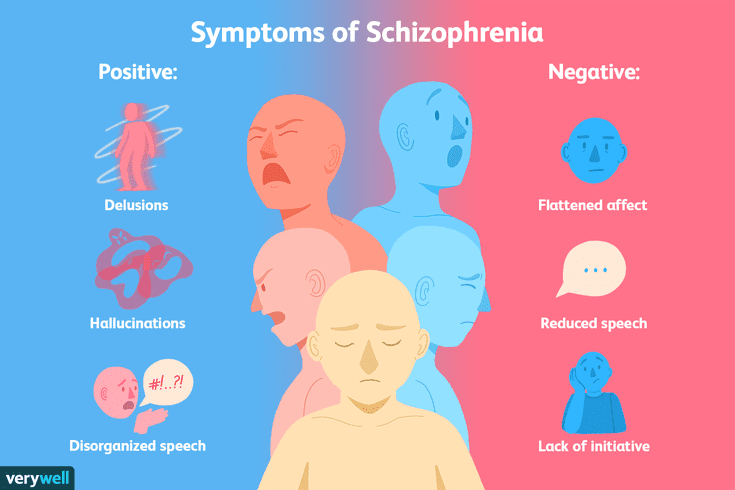
Causes of schizophrenia
Science has not established any single cause of the disease. It is believed that schizophrenia may be the result of the interaction of a number of genetic and environmental factors. Psychosocial factors may also influence the onset and course of schizophrenia. In particular, heavy marijuana abuse is associated with an increased risk of this mental disorder.
Assistance services
At present, the vast majority of people with schizophrenia do not receive mental health care worldwide. Approximately 50% of patients in psychiatric hospitals are diagnosed with schizophrenia (4). Only 31.3% of people with psychosis get specialized mental health care (5). Much of the resources allocated to mental health services are inefficiently spent on the care of patients admitted to psychiatric hospitals.
Available scientific evidence clearly indicates that hospitalization in psychiatric hospitals is not an effective way of providing care for mental disorders and is regularly associated with the violation of the fundamental rights of patients with schizophrenia. Therefore, it is necessary to ensure the expansion and acceleration of work on the transfer of functions in the field of mental health care from psychiatric institutions to the level of local communities. Such work should begin with the organization of the provision a wide range of quality community-based mental health services. Options for community-based mental health care include integrating this type of care into primary health care and hospital care. general care, setting up community mental health centres, outpatient care centres, social housing with nursing care and social home care services. Involvement in the care process is important the patient with schizophrenia, his family members and members of local communities.
Therefore, it is necessary to ensure the expansion and acceleration of work on the transfer of functions in the field of mental health care from psychiatric institutions to the level of local communities. Such work should begin with the organization of the provision a wide range of quality community-based mental health services. Options for community-based mental health care include integrating this type of care into primary health care and hospital care. general care, setting up community mental health centres, outpatient care centres, social housing with nursing care and social home care services. Involvement in the care process is important the patient with schizophrenia, his family members and members of local communities.
Schizophrenia management and care
There are a number of effective approaches to treating people with schizophrenia, including medication, psychoeducation, family therapy, cognitive behavioral therapy, and psychosocial rehabilitation (eg, life skills education). The most important interventions for helping people with schizophrenia are assisted living, special housing and employment assistance. It is extremely important for people with schizophrenia and their families and/or caregivers to a recovery-centered approach that empowers people to participate in decisions about their care.
The most important interventions for helping people with schizophrenia are assisted living, special housing and employment assistance. It is extremely important for people with schizophrenia and their families and/or caregivers to a recovery-centered approach that empowers people to participate in decisions about their care.
WHO action
steps are in place to ensure that appropriate services are provided to people with mental disorders, including schizophrenia. One of the key recommendations The action plan is to transfer the function of providing assistance from institutions to local communities. WHO Special Mental Health Initiative aims to further progress towards the goals of the Comprehensive Plan mental health action 2013–2030 by ensuring that 100 million more people have access to quality and affordable mental health care.
The WHO Mental Health Gap Action Program (mhGAP) is working to develop evidence-based technical guidelines, tools and training packages to scale up services in countries, especially in low-resource settings. The program focuses on a priority list of mental health disorders, including psychosis, and aims to strengthen the capacity of non-specialized health workers in as part of an integrated approach to mental health care at all levels of care. To date, the mhGAP Program has been implemented in more than 100 WHO Member States.
The program focuses on a priority list of mental health disorders, including psychosis, and aims to strengthen the capacity of non-specialized health workers in as part of an integrated approach to mental health care at all levels of care. To date, the mhGAP Program has been implemented in more than 100 WHO Member States.
The WHO QualityRights project aims to improve the quality of care and better protect human rights in mental health and social care settings and to expand opportunities of various organizations and associations to defend the rights of persons with mental disorders and psychosocial disabilities.
The WHO guidelines on community mental health services and human rights-based approaches provide information for all stakeholders who intend to develop or transform mental health systems and services. health in accordance with international human rights standards, including the UN Convention on the Rights of Persons with Disabilities.
Bibliography
(1) Harrison G, Hopper K, Craig T, Laska E, Siegel C, Wanderling J.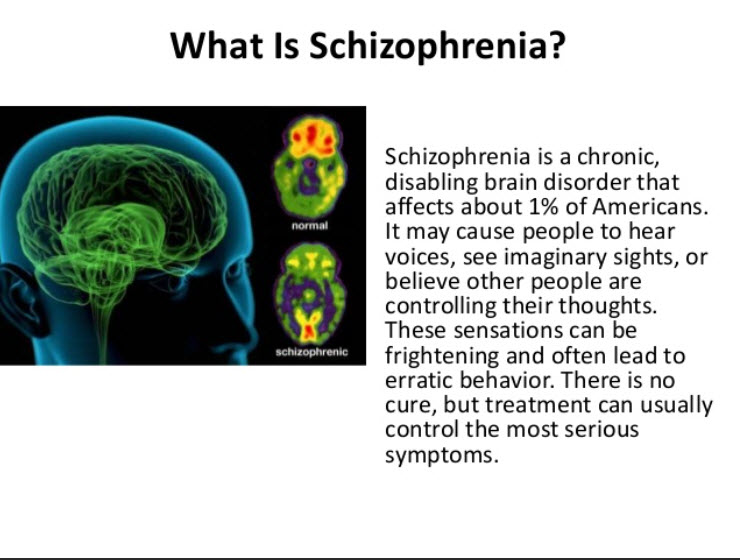 Recovery from psychotic illness: a 15- and 25-year international follow-up study. Br J Psychiatry 2001;178:506-17.
Recovery from psychotic illness: a 15- and 25-year international follow-up study. Br J Psychiatry 2001;178:506-17.
(2) Institute of Health Metrics and Evaluation (IHME). Global Health Data Exchange (GHDx). http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/27a7644e8ad28e739382d31e77589dd7 (accessed 25 September 2021)
(3) LaursenTM, Nordentoft M, Mortensen PB. Excess early mortality in schizophrenia. Annual Review of Clinical Psychology , 2014;10, 425-438.
(4) WHO. Mental health systems in selected low- and middle-income countries: a WHO-AIMS cross-national analysis. WHO: Geneva, 2009
(5) Jaeschke K et al. Global estimates of service coverage for severe mental disorders: findings from the WHO Mental Health Atlas 2017 Glob Ment Health 2021;8:e27.
The brain of a person suffering from schizophrenia: how the disease manifests itself and how scientists fight it
The brain of a person suffering from schizophrenia: how the disease manifests itself and how scientists fight it
Even if there are no people suffering from schizophrenia among your acquaintances, most likely, you have an idea about its symptoms.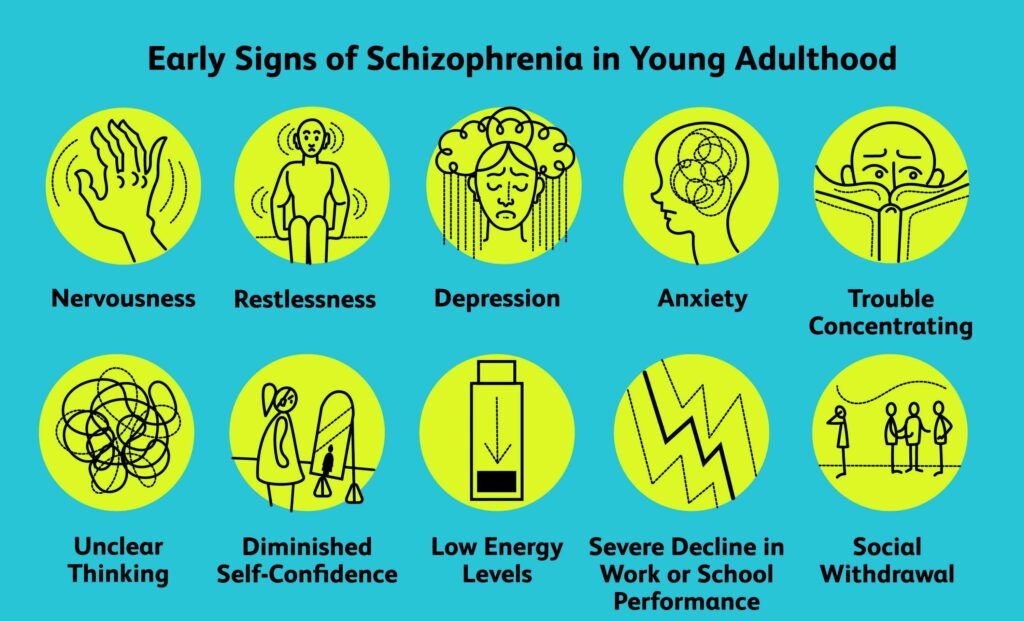
The disorder can manifest as hallucinations, delusions, and paranoia, as well as difficulty concentrating, organizing thoughts, and performing basic daily tasks.
For many years doctors knew little about this disease, except for the symptoms reported by the patients themselves. The causes of schizophrenia and how it affects the brain have for the most part remained a mystery due to the extreme difficulty scientists have had in trying to understand the most complex—and least accessible—organ in the human body.
But today, thanks to new technologies, the veil of secrecy is beginning to be covered.
“Over the past few years, we have seen tremendous advances in the understanding and treatment of schizophrenia,” says MD Husseini Manji, MD, Global Head of Neurology Therapeutics at Janssen. “This area of medicine is going through an exciting period.”
The possibility of developing new treatments for people with schizophrenia was one of the reasons that attracted Dr. Manji to the company. Then, in 2008, he was director of the National Institute of Mental Health and director of the Mood and Anxiety Disorders Program.
Manji to the company. Then, in 2008, he was director of the National Institute of Mental Health and director of the Mood and Anxiety Disorders Program.
“Several drug companies tried to convince me to join them, but at Johnson & Johnson they were focusing on neuroscience just as many were moving away from the field,” he explains. “The science of mental illness has reached a point of maturity where existing knowledge can be translated into advanced treatments for illnesses like schizophrenia.”
The nearly 2.5 million people with schizophrenia—one percent of the US adult population—are looking forward to progress in understanding and treating this complex disease.
Dr. Husseini Manji,
Head of Global Therapeutics Neurology at Janssen
Schizophrenia is one of the most severe mental illnesses. It usually manifests itself in late adolescence or after 20 years of age. Its consequences can be catastrophic: people with schizophrenia are at increased risk of becoming unemployed, homeless and incarcerated. About a third of patients attempt to commit suicide, and about one in ten eventually succeeds.
About a third of patients attempt to commit suicide, and about one in ten eventually succeeds.
Researchers know that schizophrenia is largely hereditary, but they know less about the biological basis of the disease. However, thanks to advanced brain imaging technologies, scientists such as Dr. Manji are beginning to gain a clearer picture of the changes taking place in the brain of a person with schizophrenia. It turns out that these changes occur even before the onset of clinical symptoms.
Study of the brain of a patient with schizophrenia
Over the past decade, several brain imaging studies have provided evidence that structural abnormalities are present in the brains of patients with schizophrenia. This gave scientists clues to the biological causes of the disease and how it progresses.
In one 15-year study funded in part by Janssen and described in the American Psychiatric Journal ( American Journal of Psychiatry ), it was found that during the first attack of psychosis, patients had less brain tissue than healthy people.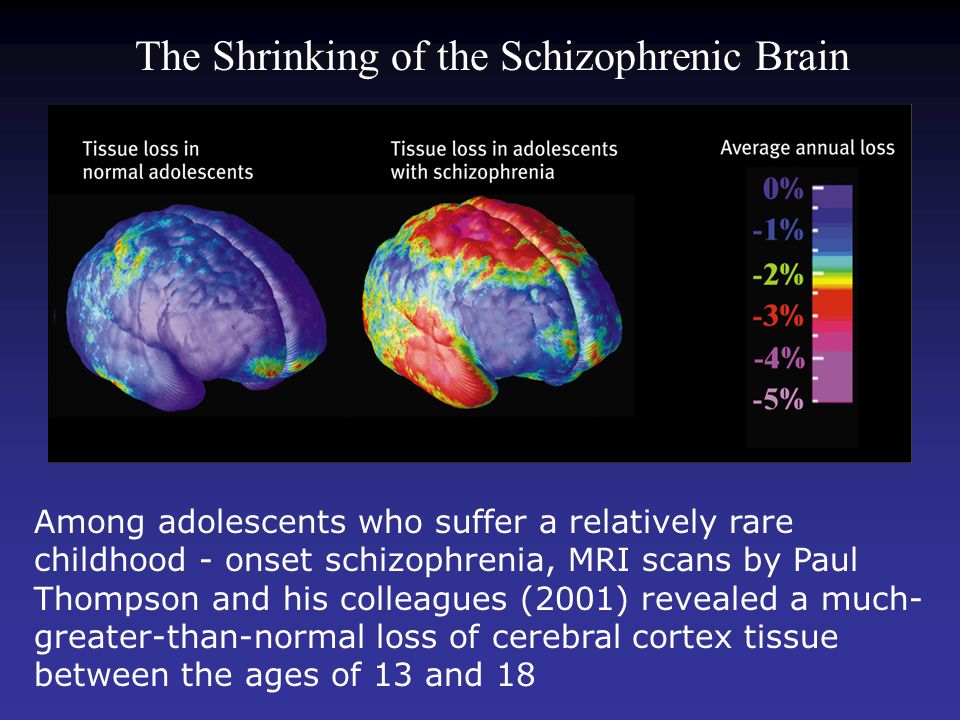 Although losses stabilized over time, long-term relapses of psychosis were associated with additional volume reductions.
Although losses stabilized over time, long-term relapses of psychosis were associated with additional volume reductions.
"We knew from earlier post-mortem studies on the brains of schizophrenic patients that they have fewer synapses and neural branches that allow neurons to communicate," explains MD Scott W. Woods, Professor of Psychiatry and Director of the Research Clinic prodromal period of psychosis PRIME at Yale University. “We think this explains the reduction in brain tissue seen on the scans.”
During adolescence, everyone experiences a normal loss of a certain amount of gray matter, which contains neurons and their short processes, but experts believe that in people at high risk of developing schizophrenia, this process may proceed too quickly or actively, causing psychosis.
Imaging studies indicate a lack of gray and white matter in the brains of people with schizophrenia. In adolescence, everyone experiences a normal loss of a certain amount of gray matter, which contains neurons and their short processes, but experts believe that in people at high risk of developing schizophrenia, this process may proceed too quickly or actively, causing psychosis.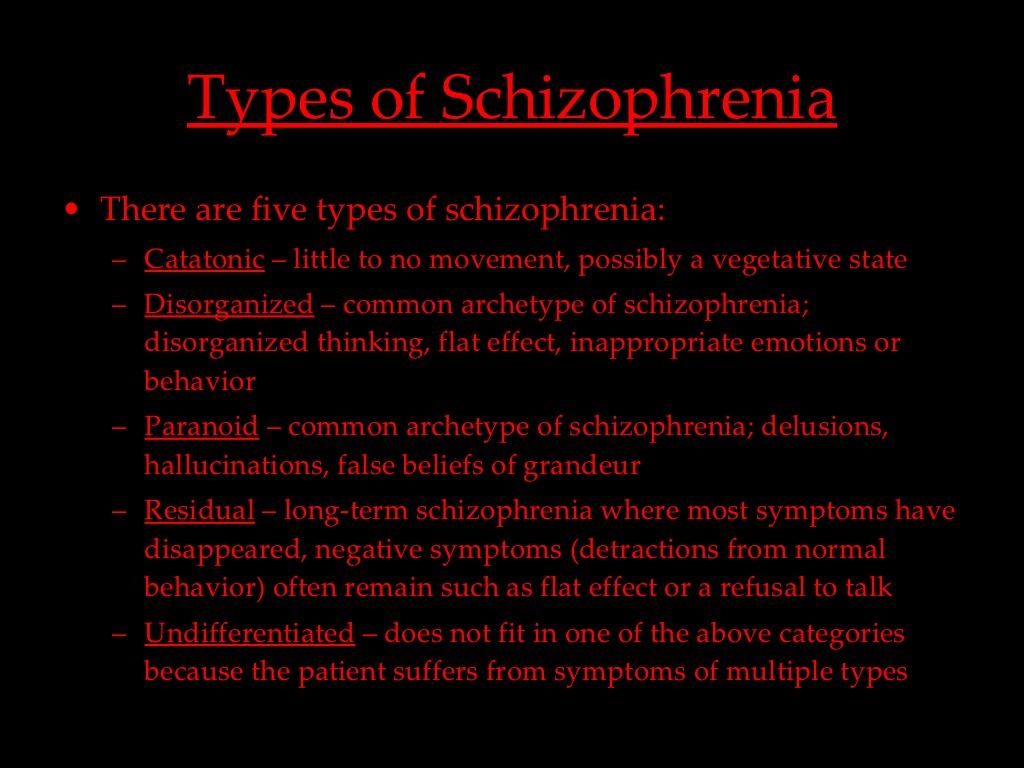
The abnormal development of the white matter, which contains long, myelinated nerve fibers that connect the four lobes of the brain, can also be a tipping point for some people who are predisposed to this disease. The authors of the study, published in the journal Clinical Neuroimaging ( NeuroImage: Clinical ), suggest that this may be related to cognitive symptoms in patients with schizophrenia, including cognitive and memory impairments, apathy, and low motivation.
What causes these losses is still unknown, but a common theory is that inflammation contributes to the progression of many diseases. Two years ago, British researchers discovered increased activity of immune cells in the brains of schizophrenic patients and people at risk. It is not clear what exactly can serve as a stimulus for the onset of the inflammatory process, but in the course of previous studies it was possible to establish a link between infections at an early age and cases of schizophrenia.
"Inflammation is one of the mechanisms leading to the destruction of synapses and neuronal branches in the brain, so severe inflammation could explain the loss," says Dr. Woods.
Advanced Brain Protection
By learning about these brain abnormalities, Janssen scientists understand the importance of treating people at the earliest stage of schizophrenia and discovering new ways to minimize the damage caused by multiple relapses.
One of Janssen's important areas of research is finding ways to improve treatment adherence. This problem is faced by any doctor who treats chronic diseases, but it is especially difficult when working with patients suffering from schizophrenia. Only about half of patients are taking prescribed medications. Failure to adhere to the regimen sets off a cycle of relapse and return of symptoms that is difficult to break and weakens the response to treatment.
“Unfortunately, the nature of schizophrenia limits patients' understanding of the disease,” says Dr. Manji. “In many cases, when they feel a little better, they stop taking the medication. However, unlike, for example, patients with diabetes, who feel the effects of missing a dose of insulin after only a few hours, patients with schizophrenia who stop taking antipsychotic drugs may not experience symptoms of relapse for several weeks.
Manji. “In many cases, when they feel a little better, they stop taking the medication. However, unlike, for example, patients with diabetes, who feel the effects of missing a dose of insulin after only a few hours, patients with schizophrenia who stop taking antipsychotic drugs may not experience symptoms of relapse for several weeks.
Janssen scientists have attempted to help reverse this severe cycle of relapse by developing long-acting injectable antipsychotics that are given to patients less frequently than other drugs.
To further protect patients from the damaging effects of multiple relapses, Janssen is exploring ways to identify patients at high risk of relapse using data collected from smartphones, medical trackers and body sensors.
Long-acting injectables are administered by physicians, so if a patient misses a dose, the attending physician will know and take action.
To further protect patients from the damaging effects of multiple relapses, Janssen is exploring ways to identify patients at high risk of relapse using data collected from smartphones, medical trackers and body sensors.
“We want to know if by tracking factors such as sleep, activity levels, interactions with other people and other biomarkers, we can provide doctors with early information about an impending relapse,” explains Dr. Manji. “This would give them the ability to identify patients who are deteriorating and get in touch with them, instead of waiting for them to come to the appointment themselves.”
Among other things, incorporating medical technology into a patient's treatment plan would help clinicians gain more objective data on how a person is actually feeling. Practice shows that when patients are asked about their well-being for several weeks, they remember only the last day or two. With more long-term, measurable data, clinicians could not only have a relatively clear picture of how a patient is feeling, but also be more constructive in their appointments.
“If patients are stable and you don't have to spend so much time just dealing with psychotic symptoms, you can focus on finding constructive ways to help them get back to normal,” says Dr. Manji.
Manji.
More than just symptom relief, it's a comprehensive treatment
To truly improve the lives of people with schizophrenia, scientists are not only developing new drugs, but also advancing the principles of integrative care. Dr. Manji said he was drawn to work at Johnson & Johnson because the company shares his belief that medicine must go beyond pills to provide the best possible outcome for patients with schizophrenia.
“We want people to understand that the best way to treat schizophrenia in the long term is through a more holistic, integrated model of care,” he explains. Mental illness has a big impact on every aspect of a person's life: their physical health, behavior and relationships. Patients require several types of correction, and not just medication.”
One of Janssen's research focuses on the vital role of carers and the challenges they face in treating and caring for people with schizophrenia. Patients are currently being recruited for a one-year clinical trial called Family Intervention in Recent Onset Schizophrenia Treatment (FIRST). The scientists plan to evaluate the overall impact that caregivers can have on patients by participating in a program of psychological education and training for caregivers. Perhaps such programs will help reduce the number of treatment failures, such as psychiatric hospitalization and suicide or attempted suicide.
The scientists plan to evaluate the overall impact that caregivers can have on patients by participating in a program of psychological education and training for caregivers. Perhaps such programs will help reduce the number of treatment failures, such as psychiatric hospitalization and suicide or attempted suicide.
The company's sincere commitment to improving the lives of patients is reflected in its projects in partnership with academia, government and the biotechnology industry. “This disease is so complex that we need to come together to make progress in research,” says Dr. Manji.
In 2015, Janssen Research & Development launched the Open Translational Science in Schizophrenia (OPTICS) project, a forum for collaborative analysis of Janssen clinical trial data and publicly available information on schizophrenia provided by the National Institutes of Health.
In addition, the company is an industry partner in a recently formed consortium led by the Johns Hopkins University School of Medicine and the Salk Institute for Biological Research.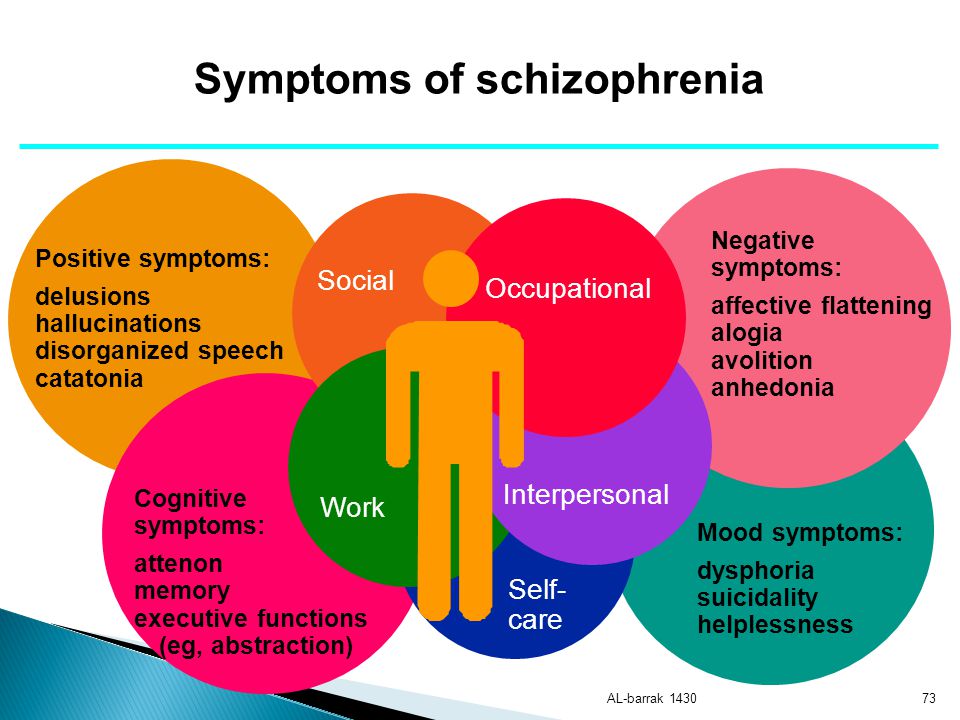 The consortium aims to improve the quality of induced pluripotent stem cell technology, a tool that allows scientists to harvest skin cells from mentally ill patients and convert them into neurons. By building a neural model of schizophrenia using patient cells, scientists hope to gain new insights into the underlying mechanisms of the disease in order to develop more targeted treatments.
The consortium aims to improve the quality of induced pluripotent stem cell technology, a tool that allows scientists to harvest skin cells from mentally ill patients and convert them into neurons. By building a neural model of schizophrenia using patient cells, scientists hope to gain new insights into the underlying mechanisms of the disease in order to develop more targeted treatments.
Dr. Manji believes that such innovative projects will not only lead to new treatments for schizophrenia, but also approaches to delay and possibly even prevent the disease.
“We now know that schizophrenia, like many other diseases, does not strike people overnight,” he explains. “It matures before a person develops full-blown psychosis, and the sooner treatment is started, the better the long-term prognosis will be.
If we learn to identify people at high risk of developing schizophrenia and learn what happens to them at the earliest stages, then in the long run we can change the entire trajectory of the disease.