Genetic psych testing
GeneSight DNA Test for Psychiatric & Depression Medication
GeneSight® Tests: Psychotropic and MTHFR
The GeneSight Psychotropic Test
The GeneSight Psychotropic test analyzes how your genes may affect your outcomes with medications commonly prescribed to treat depression, anxiety, ADHD, and other mental health conditions. The GeneSight Psychotropic test provides your clinician with information about which medications may require dose adjustments, may be less likely to work for you or may have an increased risk of side effects based on your genetic makeup.
The GeneSight Psychotropic Test
The GeneSight Psychotropic test analyzes how your genes may affect your outcomes with medications commonly prescribed to treat depression, anxiety, ADHD, and other mental health conditions. The GeneSight Psychotropic test provides your clinician with information about which medications may require dose adjustments, may be less likely to work for you or may have an increased risk of side effects based on your genetic makeup.
Medications on the GeneSight Psychotropic Report
Genes on the GeneSight Psychotropic Report
PK
Pharmacokinetic Genes
Pharmacokinetic genes tell us what the body does to the medication. These genes provide information on how a patient may break down certain medications.
PD
Pharmacodynamic Genes
Pharmacodynamic genes tell us what the medication does to the body. These genes provide information on likelihood of response and/or risk of side effects for certain medications.
+
Additional Genotypes
These genotypes are included on the report for informational purposes only.
The GeneSight® MTHFR Test
MTHFR is an enzyme required to convert folic acid and dietary folate into its active form, which is called l-methylfolate. L-methylfolate plays an important role in making neurotransmitters, such as serotonin, dopamine, and norepinephrine, which help regulate mood. The GeneSight MTHFR test shows whether a person has variation in MTHFR, which would limit their ability to create l-methylfolate.
The GeneSight MTHFR test shows whether a person has variation in MTHFR, which would limit their ability to create l-methylfolate.
- GeneSight Psychotropic
-
The GeneSight Psychotropic Test
The GeneSight Psychotropic test analyzes how your genes may affect your outcomes with medications commonly prescribed to treat depression, anxiety, ADHD, and other mental health conditions. The GeneSight Psychotropic test provides your clinician with information about which medications may require dose adjustments, may be less likely to work for you or may have an increased risk of side effects based on your genetic makeup.
The GeneSight Psychotropic Test
The GeneSight Psychotropic test analyzes how your genes may affect your outcomes with medications commonly prescribed to treat depression, anxiety, ADHD, and other mental health conditions.
 The GeneSight Psychotropic test provides your clinician with information about which medications may require dose adjustments, may be less likely to work for you or may have an increased risk of side effects based on your genetic makeup.
The GeneSight Psychotropic test provides your clinician with information about which medications may require dose adjustments, may be less likely to work for you or may have an increased risk of side effects based on your genetic makeup.Medications on the GeneSight Psychotropic Report
Genes on the GeneSight Psychotropic Report
PK
Pharmacokinetic Genes
Pharmacokinetic genes tell us what the body does to the medication. These genes provide information on how a patient may break down certain medications.
PD
Pharmacodynamic Genes
Pharmacodynamic genes tell us what the medication does to the body. These genes provide information on likelihood of response and/or risk of side effects for certain medications.
+
Additional Genotypes
These genotypes are included on the report for informational purposes only.
- GeneSight MTHFR
-
The GeneSight® MTHFR Test
MTHFR is an enzyme required to convert folic acid and dietary folate into its active form, which is called l-methylfolate.
 L-methylfolate plays an important role in making neurotransmitters, such as serotonin, dopamine, and norepinephrine, which help regulate mood. The GeneSight MTHFR test shows whether a person has variation in MTHFR, which would limit their ability to create l-methylfolate.
L-methylfolate plays an important role in making neurotransmitters, such as serotonin, dopamine, and norepinephrine, which help regulate mood. The GeneSight MTHFR test shows whether a person has variation in MTHFR, which would limit their ability to create l-methylfolate.
How does it work?
The GeneSight test must be ordered by your doctor or nurse practitioner. The test is a simple cheek swab taken in your healthcare provider’s office or can be sent by your doctor to be taken in the convenience of your home.
Step 1
Your doctor collects a DNA sample by painlessly swabbing the inside of your cheek OR you can collect the sample at home using our patient collection kit.
Step 2
The sample is sent to our lab for analysis.
Step 3
After we receive your sample, your doctor will typically get test results in about 2 days.
Step 4
Your doctor can contact our Medical Affairs team for a consultation. Your doctor can then review the results with you on your next visit.
Your doctor can then review the results with you on your next visit.
How does it work?
The GeneSight test must be ordered by your doctor or nurse practitioner. The test is a simple cheek swab taken in your healthcare provider’s office or can be sent by your doctor to be taken in the convenience of your home.
Step 1
Your doctor collects a DNA sample by painlessly swabbing the inside of your cheek OR you can collect the sample at home using our patient collection kit.
Step 2
The sample is sent to our lab for analysis.
Step 3
After we receive your sample, your doctor will typically get test results about 2 days.
Step 4
Your doctor can contact our Medical Affairs team for a consultation. Your doctor can then review the results with you on your next visit.
Educational Resources
16
Understanding the GeneSight test algorithm The GeneSight test uses a unique combinatorial algorithm, which evaluates how variations in multiple genes may influence an individual’s outcomes with certain medications. The algorithm…
The algorithm…
Read More
It is more common than you might think for women to suffer from major depressive disorder. However, depression can and should be treated. Please view this infographic to learn more…
Read More
By identifying the presence of the gene variations in HLA-B*1502 and HLA-A*3101, the GeneSight® Psychotropic pharmacogenomic test can predict if a patient may be at an increased risk of severe…
Read More
Lamictal (Lamotrigine) Uses, Dosage, Side Effects and Drug Interactions
MEDICATIONS
INDICATION AND USES:
LAMICTAL is indicated for:
- Epilepsy—adjunctive therapy in patients aged 2 years and older:
- partial-onset seizures. primary generalized tonic-clonic seizures.
- generalized seizures of Lennox-Gastaut syndrome. (1.1)
- Epilepsy—monotherapy in patients aged 16 years and older: Conversion to monotherapy in patients with partial-onset seizures who are receiving treatment with carbamazepine, phenytoin, phenobarbital, primidone, or valproate as the single antiepileptic drug.
 (1.1)
(1.1) - Bipolar disorder: Maintenance treatment of bipolar I disorder to delay the time to occurrence of mood episodes in patients treated for acute mood episodes with standard therapy. (1.2)
Limitations of Use: Treatment of acute manic or mixed episodes is not recommended. Effectiveness of LAMICTAL in the acute treatment of mood episodes has not been established.
DOSAGE AND ADMINISTRATION
- Dosing is based on concomitant medications, indication, and patient age. (2.1, 2.2, 2.3, 2.4)
- To avoid an increased risk of rash, the recommended initial dose and subsequent dose escalations should not be exceeded. LAMICTAL Starter Kits and LAMICTAL ODT Patient Titration Kits are available for the first 5 weeks of treatment. (2.1, 16)
- Do not restart LAMICTAL in patients who discontinued due to rash unless the potential benefits clearly outweigh the risks. (2.1, 5.1)
- Adjustments to maintenance doses will be necessary in most patients starting or stopping estrogen-containing oral contraceptives.
 (2.1, 5.9)
(2.1, 5.9) - Discontinuation: Taper over a period of at least 2 weeks (approximately 50% dose reduction per week). (2.1, 5.10) Epilepsy:
- Adjunctive therapy—See Table 1 for patients older than 12 years and Tables 2 and 3 for patients aged 2 to 12 years. (2.2)
- Conversion to monotherapy—See Table 4. (2.3) Bipolar disorder: See Tables 5 and 6. (2.4)
SIDE EFFECTS:
Epilepsy: Most common adverse reactions (incidence ≥10%) in adults were dizziness, headache, diplopia, ataxia, nausea, blurred vision, somnolence, rhinitis, pharyngitis, and rash. Additional adverse reactions (incidence ≥10%) reported in children included vomiting, infection, fever, accidental injury, diarrhea, abdominal pain, and tremor. (6.1)
Bipolar disorder: Most common adverse reactions (incidence >5%) in adults were nausea, insomnia, somnolence, back pain, fatigue, rash, rhinitis, abdominal pain, and xerostomia. (6.1)
CONTRAINDICATIONS:
Hypersensitivity to the drug or its ingredients. (Boxed Warning, 4)
(Boxed Warning, 4)
WARNINGS AND PRECAUTIONS:
- Life-threatening serious rash and/or rash-related death: Discontinue at the first sign of rash, unless the rash is clearly not drug related. (Boxed Warning, 5.1)
- Hemophagocytic lymphohistiocytosis: Consider this diagnosis and evaluate patients immediately if they develop signs or symptoms of systemic inflammation. Discontinue LAMICTAL if an alternative etiology is not established. (5.2)
- Fatal or life-threatening hypersensitivity reaction: Multiorgan hypersensitivity reactions, also known as drug reaction with eosinophilia and systemic symptoms, may be fatal or life threatening. Early signs may include rash, fever, and lymphadenopathy. These reactions may be associated with other organ involvement, such as hepatitis, hepatic failure, blood dyscrasias, or acute multiorgan failure. LAMICTAL should be discontinued if alternate etiology for this reaction is not found. (5.3)
- Cardiac rhythm and conduction abnormalities: Avoid LAMICTAL in patients with certain underlying cardiac disorders or arrhythmias.
 (5.4)
(5.4) - Blood dyscrasias (e.g., neutropenia, thrombocytopenia, pancytopenia): May occur, either with or without an associated hypersensitivity syndrome. Monitor for signs of anemia, unexpected infection, or bleeding. (5.5)
- Suicidal behavior and ideation: Monitor for suicidal thoughts or behaviors. (5.6)
- Aseptic meningitis: Monitor for signs of meningitis. (5.7)
- Medication errors due to product name confusion: Strongly advise patients to visually inspect tablets to verify the received drug is correct. (5.8, 16, 17)
DRUG INTERACTIONS:
- Valproate increases lamotrigine concentrations more than 2-fold. (7, 12.3)
- Carbamazepine, phenytoin, phenobarbital, primidone, and rifampin decrease lamotrigine concentrations by approximately 40%. (7, 12.3)
- Estrogen-containing oral contraceptives decrease lamotrigine concentrations by approximately 50%. (7, 12.3)
- Protease inhibitors lopinavir/ritonavir and atazanavir/lopinavir decrease lamotrigine exposure by approximately 50% and 32%, respectively.
 (7, 12.3)
(7, 12.3) - Coadministration with organic cationic transporter 2 substrates with narrow therapeutic index is not recommended (7, 12.3)
OVERDOSE:
Overdoses involving quantities up to 15 g have been reported for LAMICTAL, some of which have been fatal. Overdose has resulted in ataxia, nystagmus, seizures (including tonic-clonic seizures), decreased level of consciousness, coma, and intraventricular conduction delay.
Management of Overdose: There are no specific antidotes for lamotrigine. Following a suspected overdose, hospitalization of the patient is advised. General supportive care is indicated, including frequent monitoring of vital signs and close observation of the patient. If indicated, emesis should be induced; usual precautions should be taken to protect the airway. It should be kept in mind that immediate-release lamotrigine is rapidly absorbed [see Clinical Pharmacology (12.3)]. It is uncertain whether hemodialysis is an effective means of removing lamotrigine from the blood. In 6 renal failure patients, about 20% of the amount of lamotrigine in the body was removed by hemodialysis during a 4-hour session. A Poison Control Center should be contacted for information on the management of overdosage of LAMICTAL.
In 6 renal failure patients, about 20% of the amount of lamotrigine in the body was removed by hemodialysis during a 4-hour session. A Poison Control Center should be contacted for information on the management of overdosage of LAMICTAL.
- Uses
-
INDICATION AND USES:
LAMICTAL is indicated for:
- Epilepsy—adjunctive therapy in patients aged 2 years and older:
- partial-onset seizures. primary generalized tonic-clonic seizures.
- generalized seizures of Lennox-Gastaut syndrome. (1.1)
- Epilepsy—monotherapy in patients aged 16 years and older: Conversion to monotherapy in patients with partial-onset seizures who are receiving treatment with carbamazepine, phenytoin, phenobarbital, primidone, or valproate as the single antiepileptic drug. (1.1)
- Bipolar disorder: Maintenance treatment of bipolar I disorder to delay the time to occurrence of mood episodes in patients treated for acute mood episodes with standard therapy.
 (1.2)
(1.2)
Limitations of Use: Treatment of acute manic or mixed episodes is not recommended. Effectiveness of LAMICTAL in the acute treatment of mood episodes has not been established.
DOSAGE AND ADMINISTRATION
- Dosing is based on concomitant medications, indication, and patient age. (2.1, 2.2, 2.3, 2.4)
- To avoid an increased risk of rash, the recommended initial dose and subsequent dose escalations should not be exceeded. LAMICTAL Starter Kits and LAMICTAL ODT Patient Titration Kits are available for the first 5 weeks of treatment. (2.1, 16)
- Do not restart LAMICTAL in patients who discontinued due to rash unless the potential benefits clearly outweigh the risks. (2.1, 5.1)
- Adjustments to maintenance doses will be necessary in most patients starting or stopping estrogen-containing oral contraceptives. (2.1, 5.9)
- Discontinuation: Taper over a period of at least 2 weeks (approximately 50% dose reduction per week).
 (2.1, 5.10) Epilepsy:
(2.1, 5.10) Epilepsy: - Adjunctive therapy—See Table 1 for patients older than 12 years and Tables 2 and 3 for patients aged 2 to 12 years. (2.2)
- Conversion to monotherapy—See Table 4. (2.3) Bipolar disorder: See Tables 5 and 6. (2.4)
- Side Effects
-
SIDE EFFECTS:
Epilepsy: Most common adverse reactions (incidence ≥10%) in adults were dizziness, headache, diplopia, ataxia, nausea, blurred vision, somnolence, rhinitis, pharyngitis, and rash. Additional adverse reactions (incidence ≥10%) reported in children included vomiting, infection, fever, accidental injury, diarrhea, abdominal pain, and tremor. (6.1)
Bipolar disorder: Most common adverse reactions (incidence >5%) in adults were nausea, insomnia, somnolence, back pain, fatigue, rash, rhinitis, abdominal pain, and xerostomia.
 (6.1)
(6.1) - Precautions
-
CONTRAINDICATIONS:
Hypersensitivity to the drug or its ingredients. (Boxed Warning, 4)
WARNINGS AND PRECAUTIONS:
- Life-threatening serious rash and/or rash-related death: Discontinue at the first sign of rash, unless the rash is clearly not drug related. (Boxed Warning, 5.1)
- Hemophagocytic lymphohistiocytosis: Consider this diagnosis and evaluate patients immediately if they develop signs or symptoms of systemic inflammation. Discontinue LAMICTAL if an alternative etiology is not established. (5.2)
- Fatal or life-threatening hypersensitivity reaction: Multiorgan hypersensitivity reactions, also known as drug reaction with eosinophilia and systemic symptoms, may be fatal or life threatening. Early signs may include rash, fever, and lymphadenopathy.
 These reactions may be associated with other organ involvement, such as hepatitis, hepatic failure, blood dyscrasias, or acute multiorgan failure. LAMICTAL should be discontinued if alternate etiology for this reaction is not found. (5.3)
These reactions may be associated with other organ involvement, such as hepatitis, hepatic failure, blood dyscrasias, or acute multiorgan failure. LAMICTAL should be discontinued if alternate etiology for this reaction is not found. (5.3) - Cardiac rhythm and conduction abnormalities: Avoid LAMICTAL in patients with certain underlying cardiac disorders or arrhythmias. (5.4)
- Blood dyscrasias (e.g., neutropenia, thrombocytopenia, pancytopenia): May occur, either with or without an associated hypersensitivity syndrome. Monitor for signs of anemia, unexpected infection, or bleeding. (5.5)
- Suicidal behavior and ideation: Monitor for suicidal thoughts or behaviors. (5.6)
- Aseptic meningitis: Monitor for signs of meningitis. (5.7)
- Medication errors due to product name confusion: Strongly advise patients to visually inspect tablets to verify the received drug is correct. (5.8, 16, 17)
- Interactions
-
DRUG INTERACTIONS:
- Valproate increases lamotrigine concentrations more than 2-fold.
 (7, 12.3)
(7, 12.3) - Carbamazepine, phenytoin, phenobarbital, primidone, and rifampin decrease lamotrigine concentrations by approximately 40%. (7, 12.3)
- Estrogen-containing oral contraceptives decrease lamotrigine concentrations by approximately 50%. (7, 12.3)
- Protease inhibitors lopinavir/ritonavir and atazanavir/lopinavir decrease lamotrigine exposure by approximately 50% and 32%, respectively. (7, 12.3)
- Coadministration with organic cationic transporter 2 substrates with narrow therapeutic index is not recommended (7, 12.3)
- Valproate increases lamotrigine concentrations more than 2-fold.
- Overdose
-
OVERDOSE:
Overdoses involving quantities up to 15 g have been reported for LAMICTAL, some of which have been fatal. Overdose has resulted in ataxia, nystagmus, seizures (including tonic-clonic seizures), decreased level of consciousness, coma, and intraventricular conduction delay.

Management of Overdose: There are no specific antidotes for lamotrigine. Following a suspected overdose, hospitalization of the patient is advised. General supportive care is indicated, including frequent monitoring of vital signs and close observation of the patient. If indicated, emesis should be induced; usual precautions should be taken to protect the airway. It should be kept in mind that immediate-release lamotrigine is rapidly absorbed [see Clinical Pharmacology (12.3)]. It is uncertain whether hemodialysis is an effective means of removing lamotrigine from the blood. In 6 renal failure patients, about 20% of the amount of lamotrigine in the body was removed by hemodialysis during a 4-hour session. A Poison Control Center should be contacted for information on the management of overdosage of LAMICTAL.
Interpreting the GeneSight® Test:
Gene-Drug Interaction Chart
Patient Stories
What Other Doctors Think
Costs
Who Do I Talk To?
Find A Provider
Genes and madness: genetic testing in psychiatry
Genes and madness: genetic testing in psychiatryContents
Contents
- Origin of abnormality
- Compatibility check
- Many knowledge - many sorrows? nine0008
August 25, 2017
Popular science competition "Bio/mol/text" -2017
Overview
Genes are the foundation on which our entire organism is built. Changes in the foundation, its defects can lead to serious consequences, for example, to mental disorders.
Changes in the foundation, its defects can lead to serious consequences, for example, to mental disorders.
The genetics of consciousness
-
Author
- Viktor Lebedev
-
Editors
- Vera Bashmakova
- Andrey Panov
Topics
- "Bio/mol/text"-2017
- Genetics nine0009
- Medicine
- Psychogenetics
Bio/mol/text contest entry: Psychiatry has been aloof from all major branches of medicine for many years. While traumatologists took x-rays and therapists studied blood tests, psychiatrists simply talked to their patients and watched them. Now genetics with its modern technologies comes to the aid of psychiatrists. nine0003
While traumatologists took x-rays and therapists studied blood tests, psychiatrists simply talked to their patients and watched them. Now genetics with its modern technologies comes to the aid of psychiatrists. nine0003
This work was published in the nomination "Biomedicine today and tomorrow" of the competition "bio/mol/text"-2017.
The general sponsor of the competition is the Diaem company: the largest supplier of equipment, reagents and consumables for biological research and production.
The sponsor of the audience award and the partner of the nomination "Biomedicine Today and Tomorrow" was the company "Invitro".
"Book" sponsor of the competition - "Alpina non-fiction"
Psychiatry has always lacked objectivity. A few decades ago, a patient might have had an electroencephalogram or pneumoventriculography to rule out a neurological disorder. And if it was confirmed, then the patient passed into the hands of neurosurgeons or neurologists. Psychiatrists continued to work with those patients in whom nothing significant could be found.
Psychiatrists continued to work with those patients in whom nothing significant could be found.
With the increase and complexity of the arsenal of medical research, psychiatry seems to have begun to claim its use on a regular basis, but in reality this is not so. For example, we know that the progression of Alzheimer's disease [1] is accompanied by a decrease in the volume of the hippocampus, the brain regions associated with memory [2]. It is also known that treatment with anti-dementia drugs can slow down the loss of hippocampal substance [3]. The question arises: how often does a patient with dementia undergo an MRI of the brain with the calculation of the volume of the hippocampus? The answer lies on the surface: almost never. nine0003
Mental illness is not taken from scratch. It is often possible to identify a provoking social factor in the development of a disorder, but one should not forget about biological factors. Each of us has genes on the basis of which the complex life of our cells, including neurons, is built. In order to understand how applicable to reality genetic testing in psychiatry can be, it is necessary to evaluate its effectiveness and usefulness before its introduction into widespread practice. We need answers to a few questions. Their approximate list might look like this:
In order to understand how applicable to reality genetic testing in psychiatry can be, it is necessary to evaluate its effectiveness and usefulness before its introduction into widespread practice. We need answers to a few questions. Their approximate list might look like this:
- Do genetic factors influence the development of mental disorders? Psychiatric disorders is a large group of diseases that includes affective pathologies (depression, bipolar affective disorder [BAD], anxiety disorders), diseases with psychotic symptoms (schizophrenia, confusional states) and cognitive impairment (mental retardation, dementia). Obviously, for each disease, the genetic contribution will be different. For this reason, it is necessary to understand under what pathologies it will be maximum. nine0009
- Can these factors be inherited, that is, pass from generation to generation? Through genetic research, we can understand the origin of genetic disorders in mental disorders.
 Were they passed on from parents, grandparents? Or did the observed changes occur in the patient himself (mutations de novo )? Only extensive fundamental research will help us find answers to these questions.
Were they passed on from parents, grandparents? Or did the observed changes occur in the patient himself (mutations de novo )? Only extensive fundamental research will help us find answers to these questions. - Is it possible to single out a specific gene or group of genes that have a noticeable effect on the development of pathology? nine0025 The search for scientists leads to different results. They can find a specific gene responsible for the development of a disease, or they can find several genes that affect the disease itself or individual symptoms.
- Can we find some genetic factors that determine the effect of antipsychotics, antidepressants and other drugs in mental disorders? Pharmacogenetic testing is the determination of genetic factors associated with the characteristics of drug metabolism, the development of side effects when taking it. Pharmacogenetic testing can be useful in predicting side effects and patient response to a drug.
 nine0009
nine0009 - Is it ethically reasonable to conduct genetic testing for mental disorders? The data obtained by scientists can be interesting, and the way they are obtained is extremely exciting, but it is important for us to evaluate the usefulness and applicability of this information. We cannot do research just for the sake of knowledge; it is important for us that they are cost-effective and do not harm the patient and his family.
The list can be supplemented depending on the circumstances, but the general vector of reflection is clear. The proposed study must be informative, and its application must be economically justified and morally acceptable. If we can combine these factors together, then genetic testing for psychiatric disorders will make sense. nine0003
The origin of the abnormality
Basic genetic research in mental disorders can be of considerable benefit. Molecular methods will help in the classification of mental disorders, in clarifying their relationships, just as they have been useful in determining and clarifying the degree of relatedness in plants, animals and microorganisms. The cost of genetic research is gradually decreasing [4], and their availability for the average user and the healthcare system as a whole is growing (Fig. 1). This means that extensive genetic research will become more and more part of the daily practice of researchers and physicians. nine0003
The cost of genetic research is gradually decreasing [4], and their availability for the average user and the healthcare system as a whole is growing (Fig. 1). This means that extensive genetic research will become more and more part of the daily practice of researchers and physicians. nine0003
Figure 1. The cost of genome research has dropped significantly over the past 15 years, outstripping even the pace of Moore's Law.
Diagnosis of mental disorders is based on the patient's complaints and the results of the examination, and not on the data of instrumental studies. The RDoC project ( Research Domain Criteria ) is currently being implemented in the United States, which aims to identify links between specific genetic variants and features of the functioning of a normal brain and a brain affected by a mental disorder [5]. The accumulation of data on this project may lead to a change in the classification of mental disorders, approaches to their diagnosis and treatment.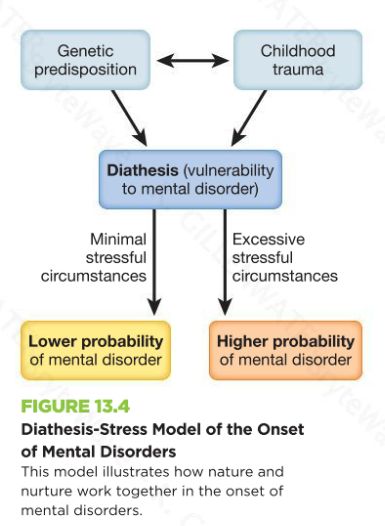 nine0003
nine0003
Currently, genetic testing methods for psychiatric disorders are mainly limited to looking for chromosomal abnormalities (such as Down's syndrome) or identifying monogenic diseases (such as gangliosidosis) (Fig. 2).
Figure 2. Karyotype of a patient with Down syndrome. Circled in red is an additional 21st chromosome (trisomy on the 21st chromosome).
site pinterest.com
These disorders in the DNA structure have been well known for decades, and their detection has become part of the usual medical practice. The problem with mental disorders is that for the vast majority of them, it is impossible to find a specific gene responsible for the development of the disease. Mental disorders are polygenic diseases, the development of which is associated with a violation of the function of several genes at once, as well as changes in the network of their interaction. In addition, a significant part of the cases of the disease, for example, in schizophrenia, is associated with the occurrence of mutations de novo , which are not so easy to determine [6].
This leads to the fact that in the field of genetic research, new methods appear that allow a fresh look at this component of pathogenesis [7]:
- part of DNA that codes for proteins. Since only 1% of the entire nuclear DNA sequence is used to encode proteins, this approach is faster and cheaper than whole genome sequencing. nine0009
- Whole genome sequencing ( whole genome sequencing ) studies not only the coding sequence of nuclear DNA, but also promoter regions, enhancers, and mitochondrial DNA. This method provides a huge amount of information, but its usefulness in each case is evaluated differently.
- RNA sequencing ( RNA-seq ) evaluates the structure of messenger RNA, which is not a direct copy of the coding DNA. This is the advantage of the method: it is able to evaluate not the genetic sequence itself, but how it is embodied in the course of the cell. nine0009
In addition to these methods, it is possible to study proteins that function inside nerve cells and their interactions. Transcriptome analysis is promising for studying the genetics of mental disorders. A transcriptome is the totality of all RNA that is produced in a cell. Thanks to their study, we will find out which proteins, in what variants and in what quantity are produced by the cell. Alternative splicing occurs in the brain more often than in other organs [8], so the DNA sequence itself is not able to give us enough information about which proteins are synthesized based on it. nine0003
Transcriptome analysis is promising for studying the genetics of mental disorders. A transcriptome is the totality of all RNA that is produced in a cell. Thanks to their study, we will find out which proteins, in what variants and in what quantity are produced by the cell. Alternative splicing occurs in the brain more often than in other organs [8], so the DNA sequence itself is not able to give us enough information about which proteins are synthesized based on it. nine0003
In turn, the sum of genetic disorders can give more than each of them separately. Such network interactions are already known in schizophrenia [9] and late-onset Alzheimer's disease [10]. An extensive study in 2014 found about 4,000 genes associated with the occurrence of autism spectrum disorders, attention deficit hyperactivity disorder (ADHD), schizophrenia, and X-linked intellectual development disorders [11]. From a number of these genes, 435 of the most significant were identified, which contained a total of 789nonsynonymous single nucleotide substitutions (SNPs). As further analysis showed, the detected genetic variants could affect a number of important processes inside the nerve cell (Fig. 3). Similar "overlaps" have been found in other studies. For example, a number of identical genes are involved in the development of borderline personality disorder and bipolar affective disorder, for example, DPYD and PKP4 [12]. In addition, when calculating the polygenic risk of developing some mental disorders, their genetic proximity was found (Fig. 4). nine0003
As further analysis showed, the detected genetic variants could affect a number of important processes inside the nerve cell (Fig. 3). Similar "overlaps" have been found in other studies. For example, a number of identical genes are involved in the development of borderline personality disorder and bipolar affective disorder, for example, DPYD and PKP4 [12]. In addition, when calculating the polygenic risk of developing some mental disorders, their genetic proximity was found (Fig. 4). nine0003
Figure 3. A variety of mental disorders have common molecular bases at the protein level. Presents 13 protein modules involved in key processes within neurons. Modules with significant differences in the frequency of primary candidate genes are indicated with an asterisk. Lines with numbers represent protein interactions between modules. Legend: ASD - Autism Spectrum Disorder, ADHD - Attention Deficit Hyperactivity Disorder, SZ - schizophrenia, XLID - X-linked disorders of intellectual development.
To see the picture in full size, click on it.
[11], drawing adapted
Figure 4. When calculating the polygenic risk of bipolar affective disorder, schizophrenia and depression, it was found that some of the genes responsible for the development of one disease are involved in the pathogenesis of other mental disorders. Legend: Mean standardized PRS - average standardized polygenic risk score, BOR - borderline personality disorder, BIP - bipolar affective disorder, SCZ - schizophrenia, MDD - depression.
Departure from the search for specific genes leads to the search for links between endophenotypes in schizophrenia and changes in large areas of the genome [13]. An endophenotype is a set of behavioral or physiological traits that is stable and stably associated with specific changes in genetic data. At the same time, the signs themselves do not reach the level of a symptom. Most likely, the term "feature" fits them. To endophenotypes, for example, scientists include impaired recognition of emotions and problems with how the patient controls his movements. Problems with recognizing emotions turned out to be associated with changes in the region of chromosome 1p36, where the gene encoding the serotonin type 6 receptor is located. This receptor is a target for typical and atypical antipsychotics, drugs that show high efficacy in the treatment of schizophrenia. nine0003
In general, the situation with genetic research in the origin of psychiatric pathology is disappointing. Too many genes influence the development of mental disorders. At the same time, they have too weak effects that require new mathematical methods for their analysis. Too complex studies are required to determine these weak links: they are not yet widely available in wide practice.
Compatibility testing
Genetic research in mental disorders is not limited to finding the causes of the disease and their differences. Now pharmacogenetic testing is gaining more and more popularity - the detection of features of enzymes that are involved in the metabolism of drugs. There are amazing workers in our body - a family of enzymes called "cytochrome p450". This family includes more than 50 enzymes, 6 of which are involved in the metabolism of about 90% of all medicines [14]. Here are the strikers of the metabolic front: CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP3A4 and CYP3A5. CYP2C19 and CYP2D6 are of great importance for the metabolism of psychotropic drugs.
For example, 85% of antidepressants and 40% of antipsychotics are metabolized by the CYP2D6 enzyme [15]. This is reflected in the frequency of development of specific side effects when using psychotropic drugs. Patients with high CYP2D6 activity receiving antipsychotic therapy are more prone to the development of tardive (tardive) dyskinesia than those in whom this enzyme is less active [16]. Tardive dyskinesia is a specific syndrome caused by long-term use of neuroleptics and persisting after their withdrawal. With its development, the patient develops violent, repetitive movements of the tongue and lips. In severe forms, other muscle groups are involved: the patient experiences violent movements of the torso and limbs. These problems can be combined with restlessness, tremors, and drug-induced parkinsonism. Correcting tardive dyskinesia with medication is a difficult task. For this reason, efforts are usually made to prevent it. There is evidence that indicates that insufficient activity of CYP2D6 can lead to neuroleptic malignant syndrome [17]. After taking antipsychotics, the patient begins to complain about a rise in temperature. He has a pronounced increase in muscle tone, pronounced changes in pulse rate and blood pressure, as well as impaired consciousness of varying degrees. This is one of those rare conditions in psychiatry that by itself can lead to the death of the patient. nine0003
Existing pharmacogenetic data in psychiatry are associated with the work of CYP2C19 and CYP2D6 enzymes [18]. Genetic testing can determine the rate at which enzymes work, depending on which allele of a gene is present in a person and in how many copies. Functional variants of CYP2D6 include variants of CYP2D6*1, CYP2D6*2 in any combination with other alleles. If this gene has additional copies, then the enzyme works too actively, which puts its owner into the group of "ultrafast" metabolizers. "Intermediate" and "slow" CYP2D6 metabolizers may have an increased risk of side effects, and therefore require lower doses of drugs in the treatment of mental disorders. By CYP2C19 enzyme activityhumans can also be classified into "ultra-fast", "extensive", "intermediate", and "slow" metabolisers. The prevalence of different alleles varies depending on the race to which the patient belongs.
The enzymes CYP2C19 and CYP2D6 play a key role in the metabolism of tricyclic antidepressants, among which amitriptyline must be mentioned. It is widely used by psychiatrists, neurologists and therapists for a wide variety of diseases. In the course of metabolism, amitriptyline undergoes transformations leading to a change in its effect on the mental state (Fig. 5) [18]. Amitriptyline as a tertiary amine has a pronounced effect on the serotonin system. Through the action of CYP2C19, it turns into nortriptyline, which actively interferes with the work of norepinephrine transmission. The more active the enzyme works, the weaker the “serotonin” component of the effect of amitriptyline and the stronger the norepinephrine one. Since CYP2D6 is involved in the metabolism of tricyclic antidepressants, its activity affects the ability of drugs to affect the patient's condition. In "ultra-rapid" CYP2D6 metabolizers, it is recommended to start therapy not with this class of drugs. If a patient with such metabolic features receives tricyclic therapy, then it is necessary to regularly evaluate the concentration of the drug in plasma. For "slow" metabolizers, the recommendations are the same. If they have to take tricyclic antidepressants, then the initial dose should be 50% of the recommended starting dose.
Similar recommendations exist for CYP2C19[eighteen]. At the same time, one should not think that genetic testing of the enzymes under discussion is some kind of exotic. In 2005, the FDA approved the AmpliChip CYP450 system, which provides data on the genetics of these enzymes. Separate studies of the CYP2C19 and CYP2D6 genes are also available in our country.
Figure 5. In humans, amitriptyline is converted by CYP2C19 to nortriptyline, the active metabolite of amitriptyline. CYP2D6 is involved in the conversion of both molecules to an inactive form. nine0003
Another example of already existing pharmacogenetic testing aimed at preventing rare but dangerous side effects is screening for the HLA-B*1502 marker in people of Asian descent. Carbamazepine therapy in patients with this gene increases the risk of developing Stevens-Johnson syndrome, a potentially fatal skin lesion in which epidermal cells separate from the dermis [19]. The FDA recommends testing the HLA-B*1502 marker before initiating carbamazepine therapy. nine0003
Many knowledge - many sorrows?
Whenever it comes to the introduction and use of a diagnostic method in medical practice, it is necessary to evaluate its usefulness. If we start doing genetic tests on patients with mental disorders, will it be useful for them? Will we get any meaningful information for the diagnosis and treatment of this group of diseases?
At the current stage of development of the genetics of mental disorders, their usefulness is doubtful. There are too many uncertain and poorly applicable results in studies even with a large sample. The main reason for this is the fundamental difference between mental disorders and monogenic diseases. In the classic case of a monogenic disease (for example, Huntington's disease), it is enough to analyze the structure of one gene to understand whether the patient has this disorder or not. With the same certainty, it will work to predict the development of Huntington's disease in a potential carrier of the gene. One can recall the Thirteenth from the TV series House M.D., which found out by one analysis whether she would develop Huntington's disease or not [20]. nine0003
Mental disorders have a different genetic basis. These are polygenic diseases, the development of which is associated with a change in the work of many genes at the same time. The identification of each of these genes will not bring important diagnostic information for the doctor, at least at the current stage of development of this field of knowledge. There is also little point now in predicting the risk of developing a mental disorder based on genetic studies in each person and relatives of already known patients. In the development of mental disorders, environmental factors play an important role - socio-economic status, serious upheavals in life, place of residence of a person. The vague information that a person who does not suffer from a mental disorder will receive will lead to an increase in his anxiety about his health, and this excessive anxiety can provoke the onset of his illness ("I was worried that I would go crazy, and in the end I went crazy") . The other side of identifying such genetic risks in a person is a negative attitude towards him from others (“He has the genes for schizophrenia, which means that he can become a schizophrenic at any moment”). This will significantly complicate the life of a person. Although the risk itself may be insignificant, all the words and decisions of a person can be perceived through the prism of his potential insanity. A person with a calculated risk of a mental disorder can be recognized as sick without the disease itself. The usefulness here, of course, is doubtful. nine0003
This problem is well illustrated by studies of the 5-HTTLPR (serotonin transporter) gene, which is often associated with the risk of antisocial behavior (aggression, crimes against property). A short version of the gene with a small number of repeats in its structure makes a person vulnerable to external manifestations of threatening situations and provokes increased activity of the hypothalamic-pituitary-adrenal system [21]. As a result, a teenager with a short version of the 5-HTTLPR gene will be more likely to exhibit antisocial behavior than someone with a long version of this gene. So far, everything is clear: let's take all teenagers and test them for this gene. Then we will form a risk group and keep a close watch on it in order to prevent crimes and these young people from going to prison. As they say, it was smooth on paper, but they forgot about the ravines. The "ravine" in this case is the environmental factors, in particular, the socio-economic conditions in which the teenager grows up. If we are talking about disadvantaged areas, then in them economic and social factors (unemployment, level of education) have a predominant influence on antisocial behavior [22]. This means that in order to prevent crime, interventions are needed at the level of the entire locality, measures that improve the social climate as a whole. The influence of 5-HTTLPR gene variants becomes noticeable under favorable socioeconomic conditions.
It turns out that "genetic" hooligans should be looked for not in slums and ghettos, but among the representatives of the middle class and wealthy citizens, which is somewhat discouraging. nine0003
Development of genetic research in the field of mental disorders will continue. Thanks to the research, we have data on pharmacogenetics that allow us to choose the treatment wisely in order to avoid side effects and achieve a good result of therapy. The calculation of the risks of developing the disease and the diagnosis of mental disorders still remain a difficult and unattainable task in practice. Let's hope this changes over time.
- In the ruins of memory: the present and future of Alzheimer's disease; nine0009
- Jack C.R. Jr., Petersen R.C., Xu Y., O'Brien P.C., Smith G.E., Ivnik R.J. et al. (2000). Rates of hippocampal atrophy correlate with change in clinical status in aging and AD. Neurology . 55 , 484–89;
- Mamoru Hashimoto, Hiroaki Kazui, Keiji Matsumoto, Yoko Nakano, Minoru Yasuda, Etsuro Mori.
(2005). Does Donepezil Treatment Slow the Progression of Hippocampal Atrophy in Patients With Alzheimer's Disease?. AJP . 162 , 676-682;
- DNA sequencing costs: data. (2016). National Human Genome Research Institute ;
- Research Domain Criteria (RDoC). National Institute of Mental Health ;
- Hui Liu, Simon C. Heath, Christina Sobin, J. Louw Roos, Brandi L. Galke, et. al. (2002). Genetic variation at the 22q11PRODh3/DGCR6locus presents an unusual pattern and increases susceptibility to schizophrenia. PNAS . 99 , 3717-3722;
- U Demkow, T Wolańczyk. (2017). Genetic tests in major psychiatric disorders—integrating molecular medicine with clinical psychiatry—why is it so difficult?. Transl Psychiatry . 7 , e1151;
- Qun Pan, Ofer Shai, Leo J Lee, Brendan J Frey, Benjamin J Blencowe.
(2008). Deep surveying of alternative splicing complexity in the human transcriptome by high-throughput sequencing. Nat Genet . 40 , 1413-1415;
- C Chen, L Cheng, K Grennan, F Pibiri, C Zhang, et. al. (2013). Two gene co-expression modules differentiate psychotics and controls. Mol Psychiatry . 18 , 1308-1314;
- Bin Zhang, Chris Gaiteri, Liviu-Gabriel Bodea, Zhi Wang, Joshua McElwee, et. al. (2013). Integrated Systems Approach Identifies Genetic Nodes and Networks in Late-Onset Alzheimer's Disease. Cell . nine0024 153 , 707-720;
- A S Cristino, S M Williams, Z Hawi, J-Y An, M A Bellgrove, et. al. (2014). Neurodevelopmental and neuropsychiatric disorders represent an interconnected molecular system. Mol Psychiatry . 19 , 294-301;
- S H Witt, F Streit, M Jungkunz, J Frank, S Awasthi, et.
al. (2017). Genome-wide association study of borderline personality disorder reveals genetic overlap with bipolar disorder, major depression and schizophrenia. nine0241 Transl Psychiatry . 7 , e1155;
- Tiffany A. Greenwood, Neal R. Swerdlow, Raquel E. Gur, Kristin S. Cadenhead, Monica E. Calkins, et. al. (2013). Genome-Wide Linkage Analyzes of 12 Endophenotypes for Schizophrenia From the Consortium on the Genetics of Schizophrenia. AJP . 170 , 521-532;
- Lynch T. and Price A. (2007). The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. nine0064 Am. fam. Physician . 76 , 391–396;
- Needham D., Teed N., Pippins J. (2011). CYP2D6 and CYP2C19 genetic testing for psychiatric drug response. Personalized Medicine Portal ;
- Maju M Koola, Evangelia M Tsapakis, Padraig Wright, Shubulade Smith, Robert W Kerwin (RIP), et.
al. (2014). Association of tardive dyskinesia with variation in CYP2D6: Is there a role for active metabolites?. J Psychopharmacol . 28 , 665-670;
- Agnieszka Butwicka, Szymańska Krystyna, Włodzimierz Retka, Tomasz Wolańczyk. (2014). Neuroleptic malignant syndrome in an adolescent with CYP2D6 deficiency. Eur J Pediatr . 173 , 1639-1642;
- J K Hicks, J J Swen, C F Thorn, K Sangkuhl, E D Kharasch, et. al. (2013). Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Tricyclic Antidepressants. nine0241 Clin Pharmacol Ther . 93 , 402-408;
- P Brent Ferrell, Howard L McLeod. (2008). Carbamazepine,HLA-B*1502and risk of Stevens–Johnson syndrome and toxic epidermal necrolysis: US FDA recommendations. Pharmacogenomics . 9 , 1543-1546;
- How to save the Thirteenth? (Prospects for the treatment of Huntington's disease);
- Jorim J.
Tielbeek, Richard Karlsson Linnér, Koko Beers, Danielle Posthuma, Arne Popma, Tinca J. C. Polderman. (2016). Meta-analysis of the serotonin transporter promoter variant (5-HTTLPR) in relation to adverse environment and antisocial behavior. nine0241 Am. J. Med. Genet. . 171 , 748-760;
- Catherine Tuvblad, Martin Grann, Paul Lichtenstein. (2006). Heritability for adolescent antisocial behavior differs with socioeconomic status: gene-environment interaction. J Child Psychol & Psychiat . 47 , 734-743.
Comments
Genetic test | Testing | Career guidance
Genetic-test | Testing | career guidance nine0002 Passtesting Test your
baby now
Take the test To learn more
In what
profession Will your child be
successful?
Take the test To learn more
What
sport Is
suitable for your child? nine0003
Take the test To learn more
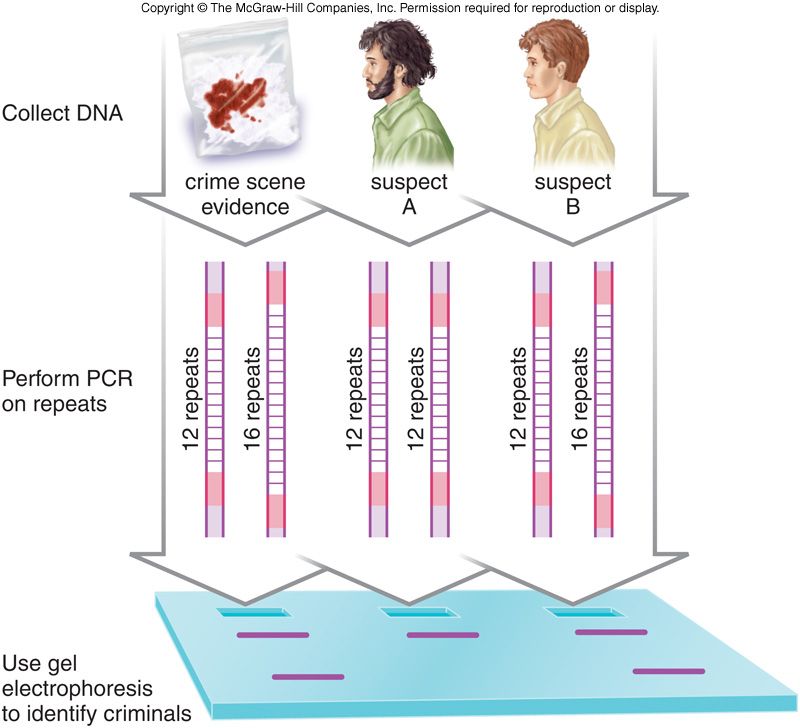
. 01 A large group of people underwent psychological testing to determine the type of nervous system.
.02 Among them were singled out people [A] with a strong nervous system and [B] with a weak nervous system
.03 According to the results of the statistical analysis of fingerprints, the predominant types of patterns in each group were identified. nine0003
.04 It turned out that people with a strong nervous system are dominated by complex patterns. And in people with a weak nervous system - simple.
.05 Thus, the hypothesis about the existence of a direct relationship between the type of the nervous system and the complexity of the type of pattern was confirmed.
How is testing
The biometric testing process is very
is simple and takes no more than 15 minutes.
STEP ONE Defining Pattern Types To generate a biometric report, you need a finger formula: types of patterns on all fingers. It is determined by the operator using a scanner, or by a specialist in the downloaded forms when testing online.
STEP TWO Data processing The formula is processed by algorithms written on the basis of research data in the field of dermatoglyphics. Processing of the finger formula takes from a few minutes (for the GT Standard report) to three days (for the GT-X and GT-S reports). nine0003
STEP THREE Report is ready As soon as we finish processing, your report will appear in your personal account. Each block of the report contains graphics and detailed comments. You can return to the report at any time.
About the company The unique biometric testing program Genetic-test was created by us on the basis of a large number of scientific studies in the field of dermatoglyphics
Dermatoglyphics How it works? nine0003
Our expert, Dr. Tamara Abramova talks about sports dermatoglyphics
Watch video
Genetic-test uses the experience of dermatoglyphics to determine the characteristics of a person's character and psychotype. Testing is not a DNA analysis, the results are for informational purposes only. The report helps to understand oneself, reveal one's potential, discover talent and prioritize development. Take the testLearn more
nine0002 Genetic-test report types:GT-X + GT-S report at a special price!
Unleashing the Potential:
Experience for yourself what Genetic-test is. The best offer for those who want to get maximum information! nine0003
GT-X Gift Set With the self-test kit, you can take the Genetic-test wherever you are and receive an extended 35-page report. The set includes: blank for prints, special inks, detailed instructions and activation code for the testing service
Sample report
PDF 0.4 MB nine0003
News
- June 20, 2017 Genetic-test entered the Golden Hundred Franchises of Russia Genetic-test entered the TOP 100 best franchises according to the independent rating of the business portal Beeboss!
- March 31, 2017 Genetic-test told "House-2" how to build love The participants of "House-2" learned how to obtain important information about a person using biometric testing and, based on this, you can build strong relationships.
nine0009
- December 30, 2016 Happy New Year! The Genetic-test team wishes everyone a Happy New Year and happy holidays!
all news
Question answer
- What is a genetic test? Genetic-test is a biometric test that allows you to quickly get a personal report on your natural potential. The information obtained will help to achieve maximum results in studies and sports, personal and professional development. nine0009
- What is testing? First, the specialist determines the types of fingerprint patterns. The formula is then processed by algorithms written on the basis of research data in the field of dermatoglyphics.
Processing of the finger formula takes from a few minutes (for the GT Standard report) to three days (for the GT-X and GT-S reports).
- I have a test kit, what should I do with it? Activate the code that is inside the box on the go.genetic-test.ru page, then follow the instructions. nine0009
- How to get tested? This can be done in two ways:
- At the testing point at the official representative.
- Online. After selecting the type of report you need, you can download the fingerprint form and fill it out following the detailed instructions. When placing an order, you need to upload a photo or scan of the form. You will be able to track the status of your application and receive an email notification as soon as the report is ready. nine0177 Regardless of how you pass the test, your report will always be available in your account on our website. - How long does it take? It takes 10 minutes to get a short GT Standard report from a company representative. For the generation of extended reports GT-X and GT-S, it takes 1-3 days for the questionnaire to be processed by the specialists of the central office. nine0007 What does the report include? There are various reporting options. The simplest one includes 16 pages of general information about your potential in such areas as education, professional activity, sports, health, personal relationships. The full 31-page report reflects in more detail the areas related to training, professional and personal growth. There is also a special version of the Genetic-test Sport, which describes the physiological and psychological characteristics of a person with recommendations for choosing a sport, role in team sports, as well as for choosing the optimal length of the distance.
- Can different people have the same reports? The microstructure of fingerprints is different for everyone. However, in relatives, due to the similarity of genes, the types of patterns on the phalanges of the fingers often have a high similarity. In addition, there are combinations of finger formulas that occur in the population in 3-5% of cases. People with the same finger formulas will have a similar type of nervous system and they will have the same reports. nine0009
- Who needs it? Parents: learn about the peculiarities of the nervous system and the hidden abilities of the child, decide on the choice of a circle or sports section, increase interest in learning and academic performance, help communicate with peers, build effective education tactics for the future, find a common language with the child.
Schoolchildren: decide on the choice of profession and university, find out their strengths, effectively prepare for exams and easily pass them, achieve success in sports, understand and love themselves.
nine0003
For students: to prepare effectively for exams and pass them easily, to determine the direction of development of their strengths, to understand where to go after university, to find out what qualities will help in personal and professional growth.
Adults: don't waste time on trial and error, find or change jobs, be guided by knowledge of your strengths and weaknesses in making decisions, choose a sport that will bring you pleasure, discover new directions for development, remember childhood dreams and gain courage embody them. nine0003
Coaches: take into account individual characteristics when drawing up a training program and forming teams.
Teachers: understand and take into account the characteristics of the nervous system of students, form an individual approach to learning, increase student motivation, help students develop their strengths and achieve the desired result, involve parents in the educational process.
Psychologists: it is easy to get acquainted with the client, to get an additional method for the initial assessment of the client, to take into account the natural features and abilities when working.
nine0003
- At what age can you get tested? The minimum age is determined by the ability to consider the types of patterns. The youngest owners of the Genetic-test report are 9-10 months old. There is no upper limit for passing the test, and adults also often learn something new from their reports. nine0007 Do you keep my data? Will my information be passed on to the police? Fingerprint images are not saved and are not processed in the program when testing with a Genetic-test representative. The fingerprint scanner is used to display the image on the computer screen, after which the operator determines the pattern type and enters the pattern type into the program. Identification of a person only by the type of pattern is not possible.
- How can physical or psychological features be determined by a fingerprint? Fingerprints and the nervous system are formed simultaneously at the 13th week of pregnancy from the germ layers of the ectoderm and are under the control of the same embryonic growth factors. This causes an inextricable causal relationship between the properties of the central nervous system and dermatoglyphic features. You can learn more about this in the section "Dermatoglyphics". nine0009
- How many people were tested in order to get the statistics? Each section of the report is based on the results of studies in which 100 to 2500 people participated, depending on the indicator, which satisfies the criteria for statistical significance.
- How long has this technique existed? In Russia, researchers have been engaged in dermatoglyphics for over 40 years. Genetic-test entered the market in 2011 with a software and hardware system that allows for quick testing. You can read more about the history of dermatoglyphics in a special section. nine0009
- Do you have a patent for the testing technique? The Genetic-test program has a certificate of state registration with Rospatent.
- How can DNA analysis be done using fingerprints? Genetic-test is not genetic testing, but biometric, do not confuse it with DNA analysis. nine0007 Does a Genetic-test representative need to have a special education to conduct testing? Data processing and report generation take place on the side of the company, so it is enough for the representative to have a partner certificate and a certificate confirming the successful completion of training in determining the types of patterns.
When testing online questionnaires with fingerprints are processed anonymously by operators (without reference to human data).