Examples of bipolar delusions
Bipolar Delusions: Grandeur, Treatment, and More
Delusions are beliefs that aren’t based on reality. During a delusion, you might believe that you’re close friends with a famous musician you’ve never met or that you’re leading the country’s space program.
Having delusions can be a condition of its own, called delusional disorder. They also can occur during the manic or depressive episodes of bipolar disorder. Sometimes, delusions happen together with hallucinations.
Believing in things that aren’t true can distance you from the real world and leave you feeling distressed. The inability to let go of an untrue belief could affect your work, relationships, and other parts of your life. However, there are effective treatments available.
There are several different types of delusions. Grandiose and paranoid delusions are the most common in bipolar disorder. Guilt is more common during depressive bipolar episodes.
GrandiosePeople with grandiose delusions believe that they’re more powerful, rich, smart, or talented than they really are. They think that they have accomplished greater things than they have done. Sometimes grandiose delusions involve religious beliefs.
Someone with paranoid or persecutory delusions thinks that other people are trying to hurt them, despite having no proof that this is happening. They may feel so threatened that they repeatedly call the police seeking help.
JealousyA person with this type of delusion believes that their romantic partner is cheating on them. In reality, there’s no evidence that their partner is being unfaithful.
GuiltThis is when someone believes they’re responsible for committing a crime or causing a terrible event, such as a natural disaster. Again, there’s no evidence that they had involvement in the event.
ErotomanicThis type of delusion causes a person to believe that someone is in love with them who isn’t. Often the object of their affection is someone famous.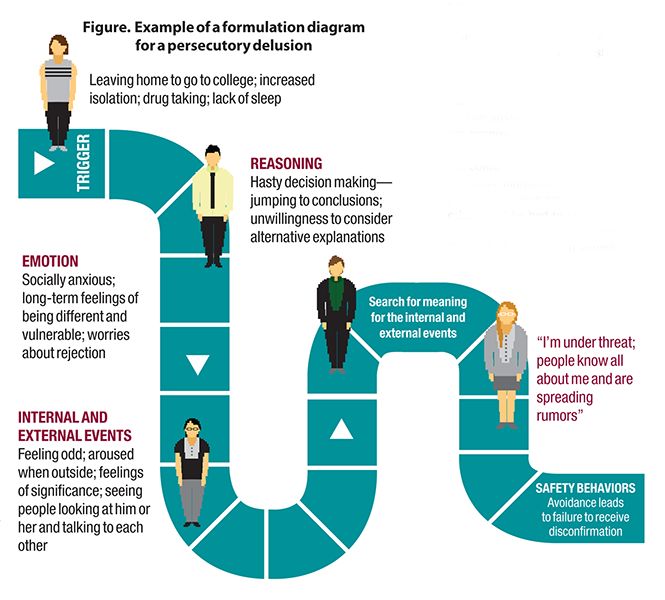
Someone with a somatic delusion believes that there’s something wrong with their body. For example, they believe that they have cancer or another disease, when they’re actually healthy.
MixedA person with mixed delusions has two or more of the delusions listed above.
Below are a few examples of what someone might say or believe with each type of delusion. In every case, there’s no evidence to back up their claims.
Grandiose
“I’ve discovered the cure for cancer.”
“I have millions of dollars in the bank.”
“I’m the new Pope.”
Paranoid or persecutory
“The government has planted a chip in my brain, and now they’re monitoring my every move.”
“The person in the car parked outside my home has been following me and is trying to kidnap me.”
“My co-worker puts poison in my coffee every morning. They want to kill me.”
Jealousy
“I need to check my partner’s emails every day to see who they’ve been talking to.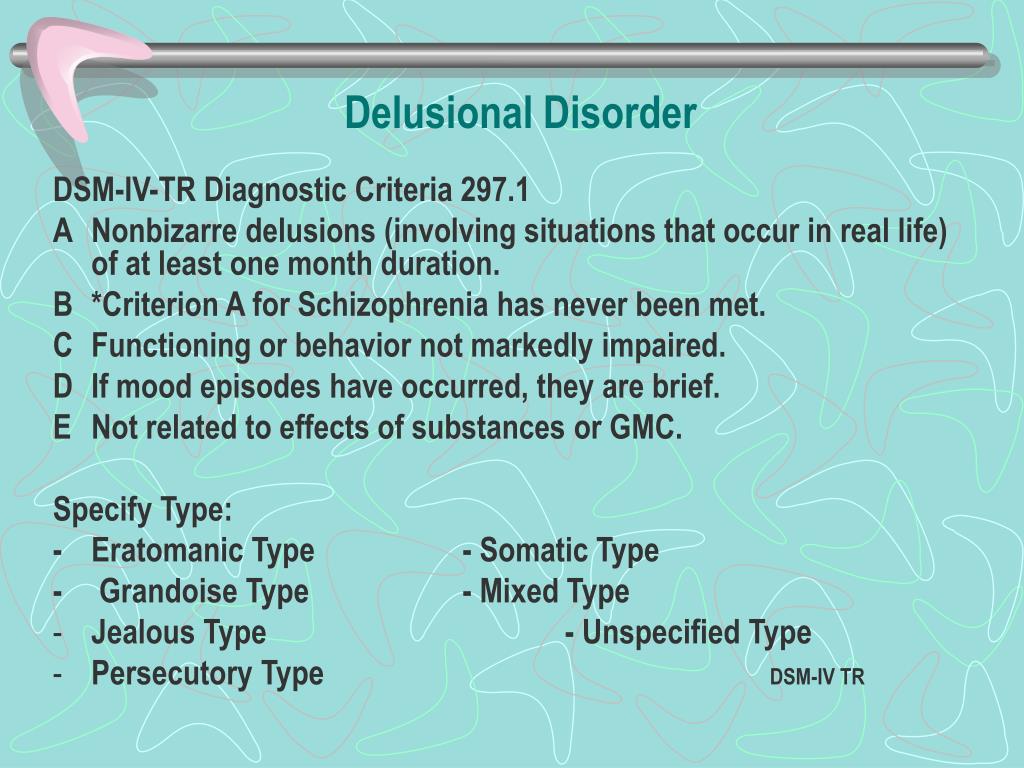 ”
”
“My spouse was 5 minutes late tonight. They must be cheating on me.”
“I waited outside my partner’s office for 2 hours to see where they went and who they were with.”
Guilt
“I gave my roommate a cup of tea, and she died of cancer. I’m responsible for her death, and I must be punished.”
“I wished for rain so that I wouldn’t have to go to work. The hurricane that blew through my city was my fault.”
Erotomanic
“The anchor on the evening news is sending secret messages straight into my brain.”
“I’ve written hundreds of letters to J. Lo. I wait for her in her hotel lobby after every concert.”
“My congressman is in love with me. The restraining order he filed against me is proof of his love.”
Somatic
“Parasites have crawled into my skin and are laying their eggs inside my intestines.”
“The left side of my face looks different than the right side. I’m disfigured and ugly.”
“I’ve been to 20 different doctors, but none of them will admit that something is wrong with me.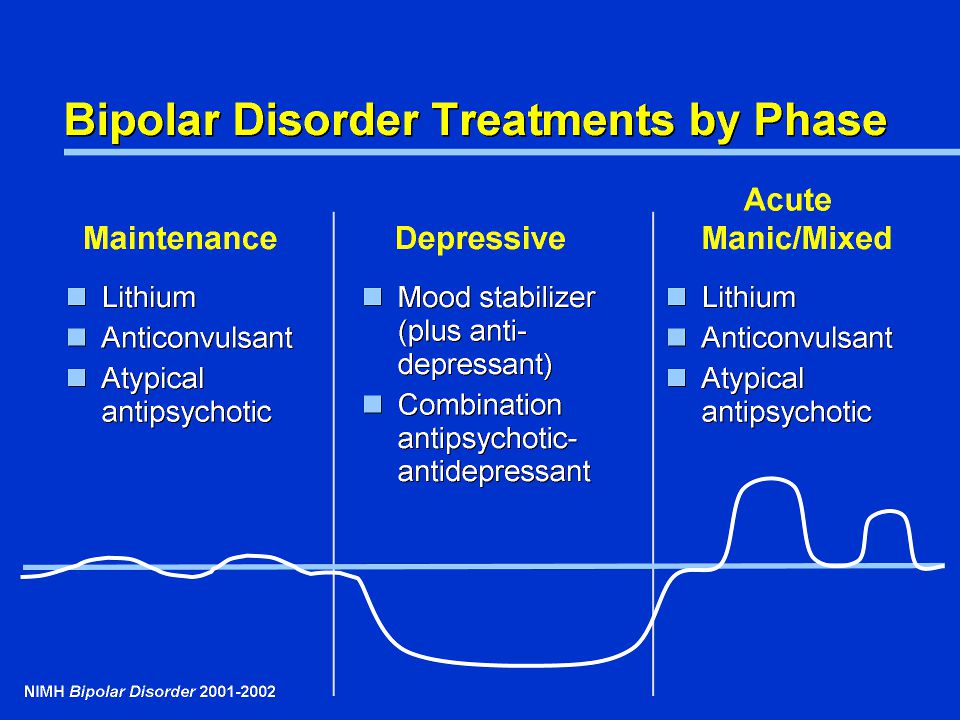 ”
”
Doctors don’t know exactly why some people develop delusions. These false beliefs are a feature of psychotic episodes in some people with bipolar disorder.
Genes may be at least partly responsible for delusions. You’re more likely to have them if one or more of your family members do, too.
Delusions may have something to do with brain chemicals called neurotransmitters, which send messages from one nerve cell to another. An imbalance in these chemicals can prevent the correct messages from getting through.
A few other factors cause people with bipolar disorder to have delusions. These include:
- stress
- drug and alcohol use
- poor vision and hearing
- loneliness
Your doctor will evaluate your symptoms to figure out which treatment might work best for you. If your doctor determines that you’re a danger to yourself or to others, you may need to stay in a hospital for a period of time.
Treatment for bipolar delusions often combines medication with talk therapy.
Talk therapy can help you identify and work through the thoughts that have become distorted. You can meet one on one with the therapist or together with your partner or other family members.
Antipsychotic drugs are the most common medications used to treat delusions. These drugs block the effects of the chemical dopamine in your brain. Dopamine is involved in triggering delusions.
When someone is having delusions, you instinct may be to reason with them or challenge the false belief. But the more you try to talk them out of it, the more difficult it will become to dissuade them.
Instead, try these strategies:
- Listen calmly as your loved one talks about their concern.
- Assure them that they’re safe and that you’ll help protect them from any harm.
- Offer other possible reasons for what is happening. For example, you might say, “I understand that you think the car parked outside your home is the CIA monitoring your movements. Why are they following you? Is it possible that the person who owns the car is simply visiting one of your neighbors?”
- Try to distract the person or direct them to another activity.
If your friends and family often tell you that your beliefs are untrue, see a mental healthcare provider. An exam can help pinpoint the reasons for your delusions. Your doctor will suggest treatments to help you manage false beliefs.
Delusions can be a symptom of both manic and depressive episodes in people with bipolar disorder. These false beliefs can be very distressing to anyone who experiences them.
If you’re concerned about delusions in yourself or a loved one, seek help from your primary care provider, a psychologist, or a psychiatrist. They can help you diagnose the condition and set up a treatment plan.
Bipolar Delusions: Grandeur, Treatment, and More
Delusions are beliefs that aren’t based on reality. During a delusion, you might believe that you’re close friends with a famous musician you’ve never met or that you’re leading the country’s space program.
Having delusions can be a condition of its own, called delusional disorder. They also can occur during the manic or depressive episodes of bipolar disorder. Sometimes, delusions happen together with hallucinations.
Sometimes, delusions happen together with hallucinations.
Believing in things that aren’t true can distance you from the real world and leave you feeling distressed. The inability to let go of an untrue belief could affect your work, relationships, and other parts of your life. However, there are effective treatments available.
There are several different types of delusions. Grandiose and paranoid delusions are the most common in bipolar disorder. Guilt is more common during depressive bipolar episodes.
GrandiosePeople with grandiose delusions believe that they’re more powerful, rich, smart, or talented than they really are. They think that they have accomplished greater things than they have done. Sometimes grandiose delusions involve religious beliefs.
Paranoid or persecutorySomeone with paranoid or persecutory delusions thinks that other people are trying to hurt them, despite having no proof that this is happening. They may feel so threatened that they repeatedly call the police seeking help.
They may feel so threatened that they repeatedly call the police seeking help.
A person with this type of delusion believes that their romantic partner is cheating on them. In reality, there’s no evidence that their partner is being unfaithful.
GuiltThis is when someone believes they’re responsible for committing a crime or causing a terrible event, such as a natural disaster. Again, there’s no evidence that they had involvement in the event.
ErotomanicThis type of delusion causes a person to believe that someone is in love with them who isn’t. Often the object of their affection is someone famous.
SomaticSomeone with a somatic delusion believes that there’s something wrong with their body. For example, they believe that they have cancer or another disease, when they’re actually healthy.
MixedA person with mixed delusions has two or more of the delusions listed above.
Below are a few examples of what someone might say or believe with each type of delusion. In every case, there’s no evidence to back up their claims.
Grandiose
“I’ve discovered the cure for cancer.”
“I have millions of dollars in the bank.”
“I’m the new Pope.”
Paranoid or persecutory
“The government has planted a chip in my brain, and now they’re monitoring my every move.”
“The person in the car parked outside my home has been following me and is trying to kidnap me.”
“My co-worker puts poison in my coffee every morning. They want to kill me.”
Jealousy
“I need to check my partner’s emails every day to see who they’ve been talking to.”
“My spouse was 5 minutes late tonight. They must be cheating on me.”
“I waited outside my partner’s office for 2 hours to see where they went and who they were with.”
Guilt
“I gave my roommate a cup of tea, and she died of cancer. I’m responsible for her death, and I must be punished. ”
”
“I wished for rain so that I wouldn’t have to go to work. The hurricane that blew through my city was my fault.”
Erotomanic
“The anchor on the evening news is sending secret messages straight into my brain.”
“I’ve written hundreds of letters to J. Lo. I wait for her in her hotel lobby after every concert.”
“My congressman is in love with me. The restraining order he filed against me is proof of his love.”
Somatic
“Parasites have crawled into my skin and are laying their eggs inside my intestines.”
“The left side of my face looks different than the right side. I’m disfigured and ugly.”
“I’ve been to 20 different doctors, but none of them will admit that something is wrong with me.”
Doctors don’t know exactly why some people develop delusions. These false beliefs are a feature of psychotic episodes in some people with bipolar disorder.
Genes may be at least partly responsible for delusions. You’re more likely to have them if one or more of your family members do, too.
Delusions may have something to do with brain chemicals called neurotransmitters, which send messages from one nerve cell to another. An imbalance in these chemicals can prevent the correct messages from getting through.
A few other factors cause people with bipolar disorder to have delusions. These include:
- stress
- drug and alcohol use
- poor vision and hearing
- loneliness
Your doctor will evaluate your symptoms to figure out which treatment might work best for you. If your doctor determines that you’re a danger to yourself or to others, you may need to stay in a hospital for a period of time.
Treatment for bipolar delusions often combines medication with talk therapy.
Talk therapy can help you identify and work through the thoughts that have become distorted. You can meet one on one with the therapist or together with your partner or other family members.
Antipsychotic drugs are the most common medications used to treat delusions.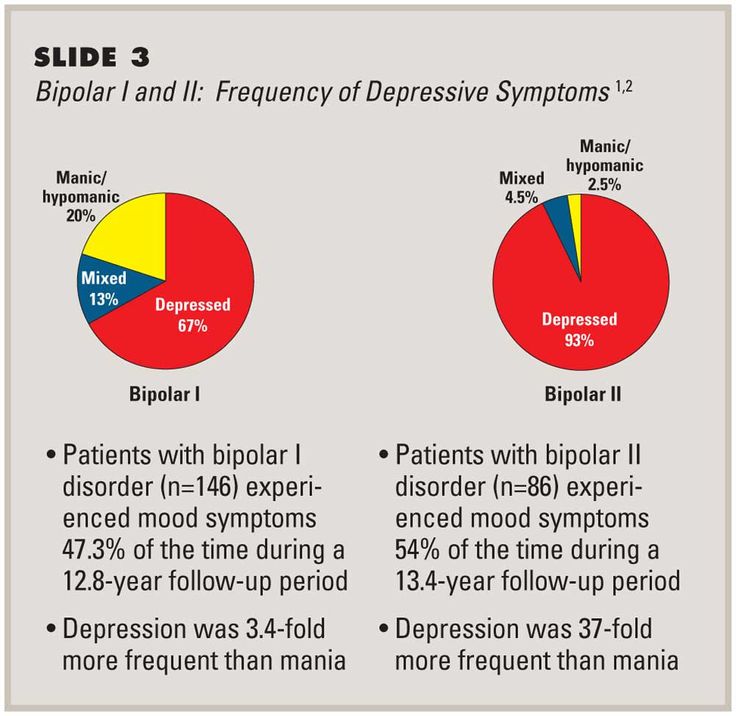 These drugs block the effects of the chemical dopamine in your brain. Dopamine is involved in triggering delusions.
These drugs block the effects of the chemical dopamine in your brain. Dopamine is involved in triggering delusions.
When someone is having delusions, you instinct may be to reason with them or challenge the false belief. But the more you try to talk them out of it, the more difficult it will become to dissuade them.
Instead, try these strategies:
- Listen calmly as your loved one talks about their concern.
- Assure them that they’re safe and that you’ll help protect them from any harm.
- Offer other possible reasons for what is happening. For example, you might say, “I understand that you think the car parked outside your home is the CIA monitoring your movements. Why are they following you? Is it possible that the person who owns the car is simply visiting one of your neighbors?”
- Try to distract the person or direct them to another activity.
If your friends and family often tell you that your beliefs are untrue, see a mental healthcare provider. An exam can help pinpoint the reasons for your delusions. Your doctor will suggest treatments to help you manage false beliefs.
An exam can help pinpoint the reasons for your delusions. Your doctor will suggest treatments to help you manage false beliefs.
Delusions can be a symptom of both manic and depressive episodes in people with bipolar disorder. These false beliefs can be very distressing to anyone who experiences them.
If you’re concerned about delusions in yourself or a loved one, seek help from your primary care provider, a psychologist, or a psychiatrist. They can help you diagnose the condition and set up a treatment plan.
Bipolar affective disorder (BAD), its signs, types and methods of treatment
Manifestations of various emotions, a change in a person's mood, manifestations of both sadness and joy are normal and depend on many factors - from temperament and character to ongoing events that influence from the outside. However, when these changes are excessive, often unexpected and for no apparent reason, emotions get out of control, or a person remains in a radically positive or negative mood for a long time, it is very likely that bipolar disorder can be diagnosed. This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease. The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease. The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
TABLE OF CONTENTS
- 1. Bipolar Personality Disorder - Overview
- 2. Symptoms and signs
- 3. Types of bipolar disorder
- 4. Phases of Bipolar Disorder
- 5. Bipolar disorder in women
- 6. Treatment of Bipolar Personality Disorder
It is not uncommon for women to be treated with a combination of drug therapy and cognitive behavioral or interpersonal therapy with a psychotherapist.
Bipolar personality disorder - general information
According to statistics, bipolar disorder affects people between 14 and 44 years of age. Unlike adults, children and adolescents experience more frequent mood swings from mania to depression, sometimes several times a day. 90% of young people make their debut precisely from the phase of depression or melancholy. Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Unlike adults, children and adolescents experience more frequent mood swings from mania to depression, sometimes several times a day. 90% of young people make their debut precisely from the phase of depression or melancholy. Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Most often, bipolar disorder is diagnosed in people whose immediate family members have had a similar problem. The causes of this disease are unknown, but stress, overstrain, and various diseases can provoke the manifestation of its symptoms. However, having fenced off a person from the influence of these factors, it is impossible to get rid of the problem, you need to seek help from a psychotherapist.
Bipolar disorder is a disease that cannot be completely cured. But with properly selected medication and psychotherapy, the quality of life is significantly improved and the periods between phases are lengthened. The person remains socialized and able to work.
The person remains socialized and able to work.
Symptoms and signs
From the name it is clear that we are talking about two different poles of affective manifestations, that is, mood manifestations. One of these conditions is depression. Depression in bipolar disorder is pronounced, with vivid symptoms. It can last up to a year and is manifested not only by low mood, lack of ability to enjoy and interest in ongoing events, but also by psychosis, when ideas of self-accusation arise, the patient feels inferior, unnecessary, poisoning the life of others. There are also nihilistic thoughts about suffering from some kind of severe illness, despite medical evidence to the contrary. There may be delusional thoughts, as well as suicidal thoughts and even attempts.
The other pole of bipolar disorder is a hypomanic state or hypomania, the characteristic features of which are an increased euphoric emotional background, the patient is constantly on the move, hyperactive, and is distinguished by very fast, associative speech. The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
Hypomania is often followed by a manic bipolar state with psychotic manifestations. The patient develops convictions in his own greatness, he believes that he is capable of anything, feels that he has a special calling in this world or that he is a descendant of great people. In extended manic episodes of mania with psychotic manifestations, anger, irritability, and direct aggression often occur. This condition leads the patient into extremely unpleasant and sometimes dangerous situations.
In addition to the typical symptoms of the disease, there are a large number of comorbid mental disorders. Comorbid mental disorders are those that accompany the underlying disease. The most common disorder of this kind is anxiety, which is manifested, among other things, by nonspecific autonomic symptoms, including sweating, palpitations, tremors of the limbs, various disorders of the gastrointestinal tract, dizziness, headaches, suffocation, and many others. In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
Types of Bipolar Disorder
Bipolar disorder can be Ι and ΙΙ types.
Bipolar I disorder is a condition in which the patient has persistent manias, i.e. overexcitation, enthusiastic inappropriate behavior, manic psychosis, as well as severe depressions. Symptoms of this type are more severe, so hospitalization is indicated in most cases.
Bipolar I disorder is characterized by short periods of hypomania followed by periods of deep depression. Hypomania is a pre-manic state with less active manifestations. Hypomania lasts a very short period of time - from several days to several hours, so sometimes patients do not even notice them and do not inform the doctor about it. Only careful, painstaking work with the patient makes it possible to identify hypomania, make the correct diagnosis and prescribe treatment.
Phases of bipolar disorder
There are several phases of bipolar personality disorder:
- Depressive (unipolar depression).
 People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.
People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.
Depersonalization and derealization may occur at the peak of bipolar depressive disorder. The boundaries of their own "I" and the world around them become blurred, patients experience difficulties in perceiving what is happening. Familiar places seem new, the colors of the surrounding world change, the patient constantly experiences a feeling of "déjà vu". Sounds become muffled, even if someone is talking very close, it seems to the patient that the voice is coming from afar.
- Manic (hypomanic). In this state, patients are full of energy, overly happy or optimistic, euphoric, and have extremely high self-esteem. At first glance, these are positive signs, but when a person experiences large-scale manic episodes, these symptoms and such an emotional state can reach dangerous extremes.
 A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another. These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another. These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
In the development of the manic phase, the following stages of development can be distinguished:
- Hypomania - increased excitement, emotional upsurge.
- Mania - all signs are more pronounced, aggression, irritability, irascibility and rage are possible.
- Phase peak. The patient constantly experiences nervous excitement, he cannot relax. All his emotions are "heated" to the limit, coordination of movements is disturbed, thoughts are illogical and abrupt, in speech he constantly jumps from one sentence to another.
- Relief of symptoms. The patient gradually calms down.
 Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged.
Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged. - Return to normal.
- Mixed. Sometimes people have complaints that are characteristic of both depression and mania at the same time. They may also experience frequent phasing—4 or more episodes in one year.
In the intervals between depressive and manic phases in bipolar disorder, there is a light period during which the general background of mood becomes relatively stable, the person continues to adequately respond to certain events, the emotional sphere is under his control. This is the main criterion for remission of bipolar disease.
Bipolar disorder in women
According to statistics, bipolar Ι disorder occurs with the same frequency in men and women, and type ΙΙ disease is more often diagnosed in women. It is also known that the female course of the disease is characterized by rapid cycles and mixed episodes. Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
For women, a special technique is being developed to alleviate this disorder, since from adolescence to menopause there are specific changes in hormonal levels that must be taken into account. In addition, psychotropic substances, which are supposed to stabilize the condition, can adversely affect the intrauterine development of the fetus if the woman is in position. It is noted that in the first trimester of pregnancy this disorder is milder, but after childbirth they often have to deal with postpartum depression. Thus, at each stage of the development of the female body, a competent doctor must review and adjust the treatment regimen. Often in the treatment of women, a complex method is used that combines drug therapy and cognitive-behavioral or interpersonal therapy with a psychotherapist. This approach gives the fastest results.
This approach gives the fastest results.
Treatment for bipolar disorder
Attempts to get rid of bipolar disorder on your own do not bring the desired result and, ultimately, lead to an aggravation of the situation, including the development of drug or alcohol dependence. In the diagnosis of the disease, keeping a mood diary can help, where the patient records all his thoughts, emotions, feelings, changes in mood. Such records will help the doctor to assess the mental state in detail and make the correct diagnosis. If you suspect bipolar disorder, you should consult a doctor, and the sooner a person realizes that he has a disease and comes to the clinic for help, the sooner professional help will be provided to him and painful symptoms will be replaced by a stable condition. It is impossible to get rid of the disease on your own, since a person cannot fully adequately assess not only his actions, but also the alternation of the phases of the disease.
Bipolar disorder is one of the few mental disorders in which medication is indicated in 100% of cases, and psychotherapy is an auxiliary tool. This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment. If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment. If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
If you have a disease, it is recommended to exclude coffee, strong tea, alcoholic and energy drinks from your diet in order not to provoke an overexcited state. If possible, you should stop smoking and in no case should you take even soft drugs. It is also very important to establish a sleep pattern, sleep at least 8 hours a day and try to go to bed at about the same time. You should learn to recognize mood swings and notice the early manifestations of new episodes.![]()
If you suspect that you have bipolar personality disorder, there is no need to panic, only a doctor can diagnose the disease, so you need to make an appointment with a psychotherapist with extensive experience in managing such patients at our MedAstrum clinic. If the diagnosis is confirmed, the doctor will make the necessary medication, if necessary, prescribe psychotherapeutic sessions and give recommendations for further lifestyle adjustments. You can make an appointment yourself on the website or by contacting our administrators.
You might be interested
Fall DepressionDon't Go Crazy: How Treatment Partners Help People with Bipolar Disorder
Initiated by community organizations of scientists, doctors and activists, World Bipolar Day is celebrated every March 30th. The date chosen was the birthday of Vincent van Gogh, an artist who, according to researchers, was the embodiment of a "bipolar genius."
With bipolar disorder, a person lives either in a state of high emotional uplift and excitement (mania), or in depression. According to world statistics, about 2% of people suffer from bipolar disorder in various forms. This means that in Russia there are at least three million bipolar people - this is about half of St. Petersburg.
According to world statistics, about 2% of people suffer from bipolar disorder in various forms. This means that in Russia there are at least three million bipolar people - this is about half of St. Petersburg.
In most cases, this condition responds well to medication. But, unfortunately, many do not seek help or do not know how to find it. Without treatment, the disease progresses and ultimately leads to sad consequences: loss of family, job, disability in general, and in almost every seventh case, suicide.
These consequences can be avoided. The peculiarity of bipolar disorder is that the onset of remission depends not only on the doctor and medications, but also on the behavior of the patient himself. Very often, bipolar people provoke seizures "with their own hands." The mood of people with BAD (bipolar affective disorder. - Note ed. ) is very unstable, the balance is fragile, and mania or depression can be “started” in dozens of ways: the psyche is easily shaken by psychoactive substances, alcohol, lack of sleep, too intense work, travel and even love. So, a short time after the next course of treatment with powerful drugs, the person again ends up in the hospital. And each new attack reduces the chances of a long remission, affects social status, and even more painfully - self-esteem.
So, a short time after the next course of treatment with powerful drugs, the person again ends up in the hospital. And each new attack reduces the chances of a long remission, affects social status, and even more painfully - self-esteem.
The experience of people with mental disorders around the world has proven that you are much more likely to cope with difficulties when you are supported by people who understand your problems and condition, but do not look at you as a patient. As practice shows, such a person can be not only a partner or close relative. An old friend, and even a person with whom you have never met in person, can help you get through the darkest times. Masha Pushkina, especially for Afisha Daily, spoke with several bipolar people about those in whom they found their support. The result is a story not about illness, but about friendship and trust, which can defeat even madness.
Yana, 31 years old
Housewife, collects books and enjoys confectionery
Purposefully, I didn't find out about the ways of support anywhere, everything turned out quite naturally. I have been sick for 15 years. The first person who looked after me was my best friend, and now it's my husband.
I have been sick for 15 years. The first person who looked after me was my best friend, and now it's my husband.
When my hypomania (a mild degree of mania, which is characterized by a constantly high mood. - Approx. ed. ) accelerated into a full-fledged mania (this state is also characterized by a one-sided attraction to some topic, sometimes accompanied by delirium. - Note ed. ), it became clear that I needed to be looked after. A friend began to pay attention to repetitive patterns of behavior in one phase or another, and we decided together to find out what helps in such cases. I think my friend was afraid to take responsibility for my condition, but she turned out to be generous and selfless. When I got married, a friend passed this knowledge on to her husband, and he already supplemented it, based on his own experience. The husband initially knew with whom he connects his life. He says it didn't scare him.
I have obsessions during my manic episodes. My husband does not argue with me at this time, but he also does not feed them, trying to redirect my stormy energy in a different direction. You can’t argue, because the result will be the opposite: I will finally get stuck on the idea, I will consider that I must prove it at all costs, even if the whole world is against me, and there are enemies and conspiracies around. If this does not help, the husband agrees to discuss all these things, but at the same time tries to slow down their implementation by offering to draw up a specific and detailed plan. Sometimes it takes me a long time.
My husband does not argue with me at this time, but he also does not feed them, trying to redirect my stormy energy in a different direction. You can’t argue, because the result will be the opposite: I will finally get stuck on the idea, I will consider that I must prove it at all costs, even if the whole world is against me, and there are enemies and conspiracies around. If this does not help, the husband agrees to discuss all these things, but at the same time tries to slow down their implementation by offering to draw up a specific and detailed plan. Sometimes it takes me a long time.
For example, I always want to move somewhere. Right now, and why aren't we packing our things yet? My husband tries to make me write down what are the pros and cons of different cities, what attracts us to them. As a result, I sit for hours on different forums, make lists, think about how we will arrange our life, calculate the budget for different countries of the world. There is also a manic passion for travel, but after preparation, we usually implement these plans. And many years ago, in a fit of mania, I bought an apartment - with a mortgage, with hellish payments. Then it took a long time to resolve this situation, but, fortunately, everything worked out well.
And many years ago, in a fit of mania, I bought an apartment - with a mortgage, with hellish payments. Then it took a long time to resolve this situation, but, fortunately, everything worked out well.
My husband began to chart my mood. I also manage it, and we check the results so that they are objective. Quarrels due to the fact that the husband takes on the role of the elder often arise in the manic phase (never in depression). Then I become very suspicious, any attempts at control cause rage. But now the husband has learned from experience, so he does not react to attempts to unleash a conflict. With obvious attacks of rage and auto-aggression, he uses holding therapy (long strong hugs. - Note ed. ). We have seen this in autistic children, this is how their parents influence them.
When I'm depressed, he doesn't comfort me because it's pointless, but he tries to give reasonable arguments that this period has always ended and this time will also pass soon.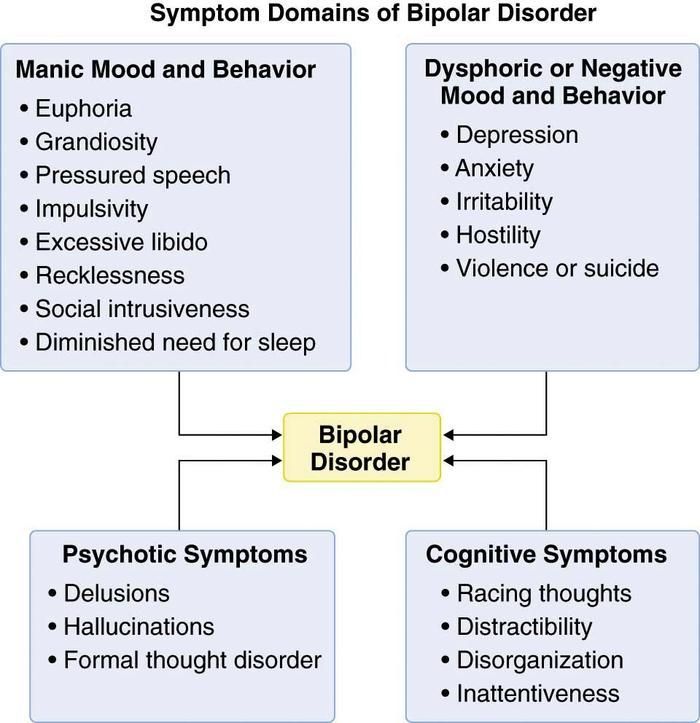 We look at mood charts for the past months, discuss the duration of the attacks: two weeks have already passed and, judging by past experience, it should get better in a couple of weeks.
We look at mood charts for the past months, discuss the duration of the attacks: two weeks have already passed and, judging by past experience, it should get better in a couple of weeks.
Such support from the husband helps in many ways. When I was being treated by two doctors, taking all the medicines, I didn’t have such support, everything was very bad. Over time, I stopped disappearing from home in a manic state and inflicting serious injuries on myself. All my super-ideas remain on paper in the form of graphs and tables, I don’t even have time to start putting them into practice, so that later I don’t have to deal with the consequences with the whole family.
Alice, 27 years old
Biologist
To be honest, I don't always find understanding from my healthy environment, I often faced condemnation, devaluation of problems. But from a person who has a similar experience, you won’t hear “don’t invent”, “you can’t feel so bad”, “take a walk and it will pass”.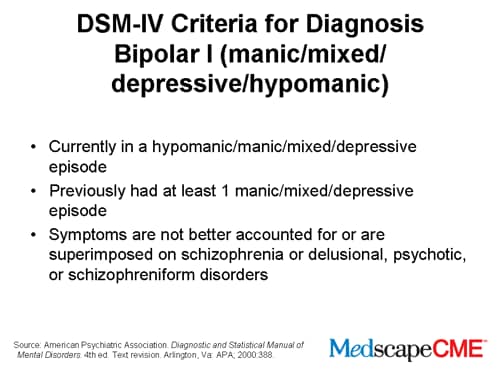
It just so happens that my best friend also suffers from bipolar disorder. I did not look for support in specialized communities where patients communicate, we met by chance. My friend is much older, he has much more life experience, and he was able to become a real mentor for me. Not once did his actions worsen my condition - I hope that he can say the same about me.
When I'm on the rise, I feel uncomfortable when he tries to slow me down and reduce my passions. But as soon as this state passes and I again take a sober look at the situation, each time I thank him for trying to stop the revelry and disgrace. My friend himself is currently not being treated, but he never imposed his position on me, and when I turn to doctors, he supports me in this.
I told the doctor about this source of support - he is all for it. Before meeting a friend, I had suicidal attempts, but during the entire time of our communication I never tried to say goodbye to life. When you know that there is a person who will understand everything and share warmth (while even my own family repels me), that there is a place where you can come in any condition and where they will accept me without unnecessary questions and teachings, this is a source of great strength. and hope.
and hope.
When I was expecting my second child, I was depressed. My husband did not yet fully understand the features of the disease and did not want to admit obvious things - this added problems, and my emotional state became extremely difficult. It seems that only thanks to the participation of my friend, I did not do anything to myself and successfully endured the pregnancy. The child was named after him.
Sergey, 49 years old
Freelancer
At the height of the depression, I was looking for any available support and ended up in an online group of anonymous debtors (people who have taken on large loans). One of the participants drew attention to my condition and said that I urgently need medical help. Despite the fact that she lives in the USA, we began to communicate regularly via Skype. Olga literally brought me to the hospital and helped me prepare for the treatment.
Americans are a pragmatic people, many young and healthy people have folders with wills and instructions in case of their death.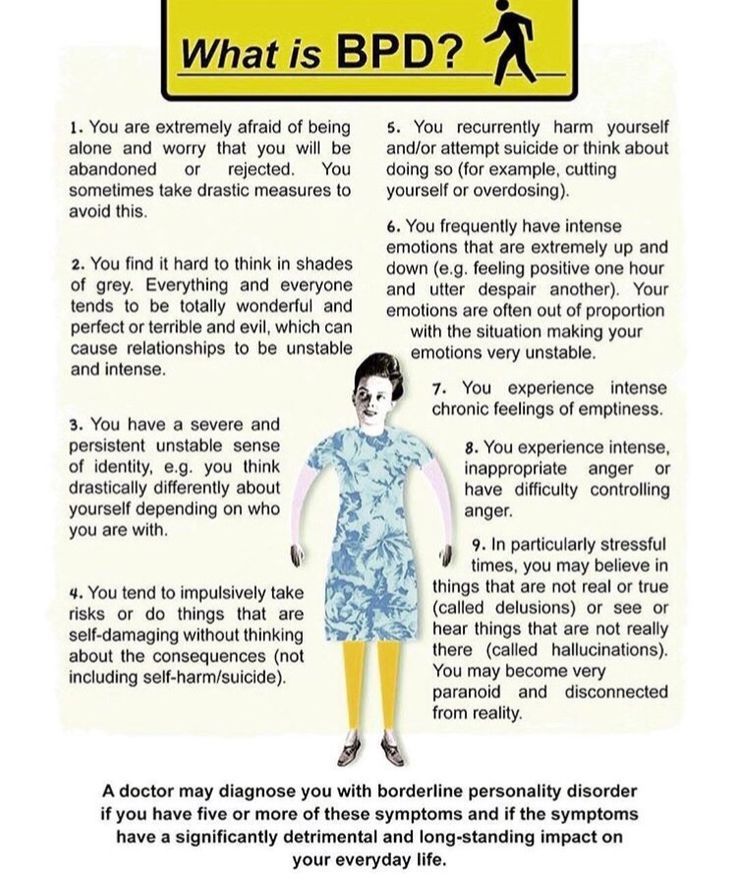 They also approach mental difficulties calmly and thoroughly. It is common practice for the patient to draw up detailed instructions in advance. In the United States, there is a practice of issuing Treatment Agreements for people with mental illness (Treatment Contract). This document is needed so that family, friends and doctors recognize the symptoms of deterioration in time and take into account your experience and wishes in the treatment. Typically, such a document contains: a list of trusted people; signs of a normal state; signs of an approaching episode; symptoms of mania and depression; actions that trusted people should take to help a person get better and keep him from destructive acts; plan of action in case of an emergency (for example, a suicide attempt). who and what will be done in case of his hospitalization, so that he can be treated without anxiety for household chores.
They also approach mental difficulties calmly and thoroughly. It is common practice for the patient to draw up detailed instructions in advance. In the United States, there is a practice of issuing Treatment Agreements for people with mental illness (Treatment Contract). This document is needed so that family, friends and doctors recognize the symptoms of deterioration in time and take into account your experience and wishes in the treatment. Typically, such a document contains: a list of trusted people; signs of a normal state; signs of an approaching episode; symptoms of mania and depression; actions that trusted people should take to help a person get better and keep him from destructive acts; plan of action in case of an emergency (for example, a suicide attempt). who and what will be done in case of his hospitalization, so that he can be treated without anxiety for household chores.
In a period of severe depression, there is a struggle inside a person between the craving for death and the desire to live - and many external things can outweigh in one direction or another.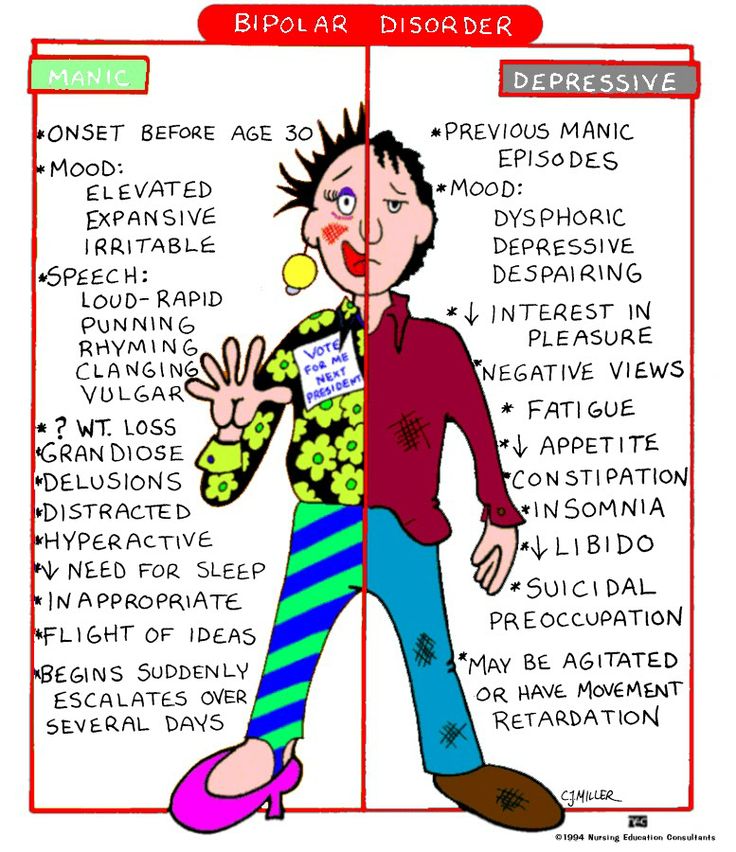 Every clue is important to help you get out. It is very difficult for one to cope with all this.
Every clue is important to help you get out. It is very difficult for one to cope with all this.
I madly didn’t want to go to the hospital and wouldn’t have made up my mind myself, until the last I hoped that somehow everything would go away on its own. But under the supervision of a friend, I drew up a preparation plan: warn the customer at work, arrange to look after my cats. Reported to her about every step. But then he could no longer simply “escape” [from hospitalization], because he felt obliged to both her and the doctor. During depression, one's own life has no value, but the people dear to me, the promises made to them, do.
At the most difficult moment, Olga became my “outer brain”, which told me what to do when I didn’t understand anything myself. After I was discharged from the hospital, I turned to four friends for support. Usually we call each other once a week, I tell what my condition is. It is important not only to chat online, but also to hear the voice, you can understand a lot from it. Friends immediately pay attention, if I suddenly disappear and stop calling, then something is wrong.
Friends immediately pay attention, if I suddenly disappear and stop calling, then something is wrong.
I think it is possible to find such a person if you set yourself such a goal. Take a closer look at people in support groups, religious or other communities - those who understand what compassion and mutual assistance are. This must be an internally mature person, ready to take responsibility for you in a difficult situation. If this person has similar problems, then he will better understand your experiences. For this reason, relatives are far from always suitable: they themselves can panic, seeing how bad you feel, choke you with their anxiety, overprotection.
It is necessary to establish the frequency of communication and observe it. And of course, in no case should you parasitize on someone else's kindness. The support system works when you yourself take responsibility for your life, and do not outweigh it completely on another.
Anna and Valeria, 21
Students
Anna: After a major depressive episode four years ago that almost ended in a suicide attempt, I started looking for information on [support]. I managed to find a guide in English for relatives and friends on how to behave with such a person. I have sent this list to all my friends so that they have an idea of what is happening to me. For the past few years, Lera has been monitoring my emotional state on a daily basis, and if, in her opinion, it goes beyond the norm, she tells me about it. Lera just asks every day how I'm doing, and if she sees that I'm reacting strangely, she wonders if something happened. At first, it was very difficult, because, in principle, I did not like to regularly share personal experiences. But by regularly receiving feedback, I can imagine the dynamics: do the pills help, how long do the side effects last, does the depressive phase go into a moderate and severe degree, do I lose my critical thinking during hypomania.
I managed to find a guide in English for relatives and friends on how to behave with such a person. I have sent this list to all my friends so that they have an idea of what is happening to me. For the past few years, Lera has been monitoring my emotional state on a daily basis, and if, in her opinion, it goes beyond the norm, she tells me about it. Lera just asks every day how I'm doing, and if she sees that I'm reacting strangely, she wonders if something happened. At first, it was very difficult, because, in principle, I did not like to regularly share personal experiences. But by regularly receiving feedback, I can imagine the dynamics: do the pills help, how long do the side effects last, does the depressive phase go into a moderate and severe degree, do I lose my critical thinking during hypomania.
Valeria: We gradually established a very trusting relationship. Anya studied the topic of bipolar disorder up and down, and I read the articles that she sent me. The diagnosis did not change anything for me, because it remained the same. After that, we already discussed some formalities (for example, who to call in case of an emergency).
The diagnosis did not change anything for me, because it remained the same. After that, we already discussed some formalities (for example, who to call in case of an emergency).
Anna: I asked Lera to watch for hypomanic manifestations in which I lose an adequate assessment of my actions: impulsive night walks, alcohol begin.
Valeria: My friend is a very responsible and conscious girl who takes care of herself, her health and her wallet. Before buying something expensive, she asks for my advice - and then we are already sorting out the situation. We can entrust accounts to each other and not worry. I also know where and to whom to run in cases of exacerbation.
Anna: I react badly to prohibitions and reminders of illness. Yes, I periodically have to turn to relatives for help, change treatment or take long breaks, but I expect mutual respect so that they don’t look at me through the prism of the disease.
When the mood is unstable, harsh phrases like “the disease speaks in you”, “these are not your real emotions” cause persistent rejection, even when they are true.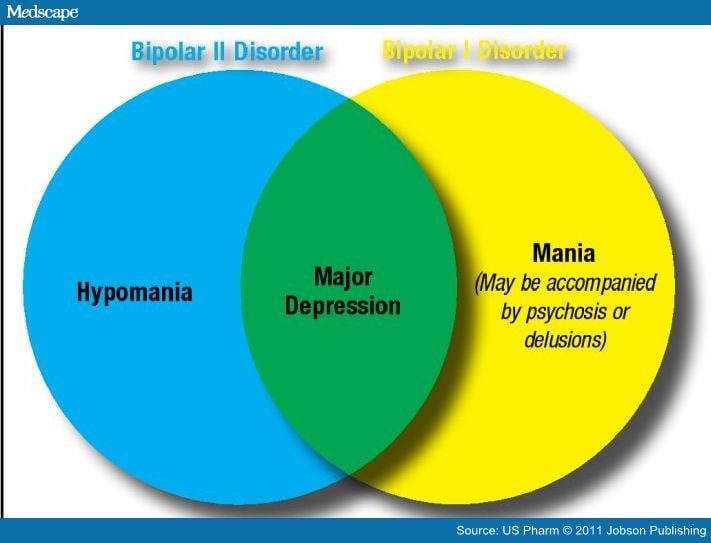 The line between accepting a loved one's illness and identifying him with a diagnosis for healthy people is extremely thin. Therefore, those who were able to grope it deserve great respect.
The line between accepting a loved one's illness and identifying him with a diagnosis for healthy people is extremely thin. Therefore, those who were able to grope it deserve great respect.
Anna: In the last year, I go to see the doctor with my parents. When the doctor notices that I may not be able to do it alone, she duplicates the instructions and advice for them. I, in turn, am a friend. The doctor has repeatedly emphasized that the change of episodes is more noticeable from the outside.
Valeria: We don't have any kind of hierarchy in relationships, so there is no pressure when one makes decisions for another. This is not eating each other's emotional resources, but complementing and supporting.
Anna: The main danger in a relationship with a person with a serious illness is to fall into codependency. This format is equally bad for both the "controller" and the "subordinate". Unfortunately, I have been in such relationships before. It is worth maintaining mutual respect and treating each other as equals. Illness should not dominate a relationship. In difficult episodes, it temporarily comes to the fore, but you should always remember that you are not a disease.
It is worth maintaining mutual respect and treating each other as equals. Illness should not dominate a relationship. In difficult episodes, it temporarily comes to the fore, but you should always remember that you are not a disease.
Anna: I have memory problems: I don't remember some episodes. In such cases, I can ask Lera for help. If you remember the last weeks, then these are regular reminders to call the doctor. In mixed episodes, this becomes an acute problem, because I can suddenly change my mind or forget. Against the backdrop of a severe episode, I may develop psychosis, and this is the most dangerous thing in the disease. Thanks to our format, I manage to avoid such exacerbations almost always.
The advantages of observation from a loved one are an early response and the fact that he knows the patient's usual behavior very well and can notice even small changes. The main disadvantage is that normal friendly communication risks turning into constant monitoring of symptoms. Not every mentally healthy person is able to remain within the boundaries of reason.
Not every mentally healthy person is able to remain within the boundaries of reason.
It is important to agree in advance, before an attack, what is an undoubted sign of a worsening condition (for example, persistent insomnia), and what you do not need to pay special attention to (for example, loud indignation at something that you do not like). In a difficult situation, often a loved one begins to behave not as an equal, but as a “healthy” and “knowledgeable”. Not all relationships stand this test.
There is also a variant of "buddy" (when two people with mental disorders look after each other. - Note ed. ) - it is good precisely because it is the true request of the patient and more equal relations without mixing roles. But I don't know the buddy support system.
To choose a person you can rely on in a critical situation, take a closer look at your surroundings. Above all, a high level of trust is needed. Your assistant should be open to nonjudgmental and open dialogue and at the same time emotionally stable and resistant to stress.
Support is essential for every person - very often we as mental health professionals need it. And with bipolar disorder, this problem is especially acute. At the initial stages, those closest to you often ignore the presence of the disease, and friends advise you to either "pull yourself together" or, conversely, "relax", sometimes with the help of alcohol. When it becomes obvious to everyone that the “condition” will not go away on its own, urgent hospitalization is already required. The saved patient receives the "stigma".
Psychiatrists then make it the responsibility of the uninitiated next of kin (parent or spouse) to monitor any changes in the patient, and they really try to do so. At the level of "laughing out loud - hypomania has begun, upset - depression." As a result, psychiatrists begin to treat quite normal human emotions based on complaints from relatives... and the circle closes.
For this to change, mental health literacy must play a major role. Relatives, in order to be able to help, need to understand well what is happening with a loved one.