Effexor in pregnancy
Is it safe to take Effexor during pregnancy?
When you’re pregnant, you want to do everything you can to make sure the baby is safe and healthy. At the same time, you want to keep yourself healthy, too. Many women take medications during pregnancy to treat ongoing health conditions, but how do you know if they’re safe?
According to a CDC report, the number of American adults taking antidepressants is on the rise, especially among women. Nearly 18% of women say they’ve taken an antidepressant in the past month compared to just over 8% of men.
Effexor (venlafaxine) is an antidepressant that’s part of a group of drugs called serotonin and norepinephrine reuptake inhibitors (SNRIs). It alters brain chemicals that may be unbalanced in people with depression. It’s also commonly prescribed in extended-release formulation, called Effexor XR. Besides depression, Effexor is also taken to treat anxiety and repeated panic attacks. If you’re taking Effexor and you are pregnant or planning to become pregnant, you may be wondering whether it’s safe to take Effexor, or Effexor XR, during pregnancy.
Can taking Effexor make it harder to get or stay pregnant?
There are no studies currently examining if Effexor can cause infertility in men or women or increases the time it takes to get pregnant. Most research studies have not shown a link between Effexor and a higher chance of miscarriage, but one study found that women taking Effexor were more likely to miscarry. There is an increased risk of miscarriage in women with untreated depression.
Is Effexor safe during early pregnancy?
“As a psychiatrist, I evaluate many depressed and anxious women who are pregnant and breastfeeding,” says Leela Magavi, MD, psychiatrist and regional medical director of Community Psychiatry in Southern California. “Venlafaxine or Effexor may be a safe antidepressant to target mood and anxiety symptoms during pregnancy.”
Research is mixed about whether Effexor raises the chance of birth defects or other health issues. Dr. Magavi says, in general, all pregnant women have a 3% to 5% chance of having a baby with a birth defect. Research on more than 700 women who took Effexor while pregnant shows that their risk was around the same range: 3% to 5%.
Research on more than 700 women who took Effexor while pregnant shows that their risk was around the same range: 3% to 5%.
Some research shows that Effexor is safe to take during the first trimester. But, a study published in JAMA Psychiatry links taking Effexor during early pregnancy with more birth defects than other antidepressants, including defects of the:
- Heart
- Brain
- Spine
- Penis (hypospadias)
- Abdominal wall (gastroschisis)
- Lip and roof of the mouth (cleft lip and cleft palate)
The study’s authors acknowledge that more research is needed.
Is Effexor safe in late pregnancy and while breastfeeding?
Women who take Effexor throughout their pregnancy, including the third trimester, and while breastfeeding may have babies with toxic symptoms, withdrawal, and even serotonin syndrome, such as:
- Jitteriness
- Irritability
- Muscle tone conditions (hypotonia or hypertonia)
- Tremors
- Seizures
- Trouble breathing and blue skin due to lack of oxygen
- Vomiting
- Low blood sugar
- Trouble eating and sleeping
- Constant crying
- Abnormal sleep patterns
These symptoms may require prolonged hospitalizations, and other measures such as tube feeding and breathing support.
Which antidepressants are safe to take while pregnant and nursing?
Pregnant women can use most antidepressants safely during pregnancy. But, Effexor is “generally not the first choice when initiating antidepressant therapy during pregnancy,” says Leslie Southard, Pharm.D., founder of The Lactation Pharmacist.
Dr. Southard and Dr. Magavi agree that Zoloft (sertraline) is preferred. It’s considered one of the safest antidepressants for pregnant women since it’s been on the market for 30 years and has the most data behind it. Though, Zoloft may also come with complications. Be sure to discuss it with your healthcare provider.
RELATED: Is it safe to take Zoloft during pregnancy?
Your healthcare provider can help you decide which medication and dosage will work best based on your needs and overall physical and mental health.
Do not start or stop an antidepressant before first talking to your healthcare provider. Suddenly stopping an antidepressant may actually cause more harm than taking it. “This could potentially lead to worsening mood and anxiety symptoms, which could adversely affect both mom and baby,” Dr. Magavi says.
“This could potentially lead to worsening mood and anxiety symptoms, which could adversely affect both mom and baby,” Dr. Magavi says.
If you decide to stop taking your antidepressant during pregnancy, your healthcare provider will gradually decrease the dose over time. They’ll also discuss other ways to manage your mental health conditions.
Pregnancy, breastfeeding and fertility while taking venlafaxine
Venlafaxine and pregnancy
There’s no good evidence that taking venlafaxine in early pregnancy will affect your baby’s development.
When venlafaxine is taken in the weeks before delivery it can sometimes cause short-term withdrawal symptoms and, very rarely, breathing problems in the baby. Your baby will be checked after birth and given additional care if needed.
Taking venlafaxine in the last month of pregnancy may slightly increase your risk of bleeding after delivery. However, because this side-effect is rare, it's not a reason to stop taking venlafaxine for most pregnant women.
However, because this side-effect is rare, it's not a reason to stop taking venlafaxine for most pregnant women.
It’s important that your mental health is treated since this can impact on yours and your baby’s wellbeing. Depression and anxiety can sometimes get worse during pregnancy and after your baby has been born.
Speak to your doctor if you become pregnant. They will talk through the risks and benefits so you can decide on the best treatment for you and your baby.
Venlafaxine and breastfeeding
If your doctor or health visitor says your baby is healthy, you can take venlafaxine while breastfeeding.
Venlafaxine passes into breast milk in small amounts and has been linked with side effects in very few breastfed babies. It has been used by many breastfeeding mothers without any problems.
It's important you keep taking venlafaxine to keep you well. Breastfeeding will also benefit both you and your baby.
Breastfeeding will also benefit both you and your baby.
If you notice that your baby seems unusually sleepy, is not feeding as well as usual, seems irritable, or if you have any other concerns about your baby, then talk to your health visitor, midwife, doctor or pharmacist as soon as possible.
Venlafaxine and fertility
There's no clear evidence to suggest that taking venlafaxine reduces fertility in men, but it may affect the menstrual cycle in women.
Speak to a pharmacist or your doctor if you're trying to get pregnant. They may want to review your treatment.
Non-urgent advice: Tell your doctor if you're:
- trying to get pregnant
- pregnant
- breastfeeding
For more information about how venlafaxine can affect you and your baby during pregnancy, visit the Best Use of Medicines in Pregnancy (BUMPS) website.
Page last reviewed: 10 February 2022
Next review due: 10 February 2025
Preeclampsia and pregnancy | Ida-Tallinna Keskhaigla
The purpose of this leaflet is to provide the patient with information about the nature, occurrence, risk factors, symptoms and treatment of preeclampsia.
What is preeclampsia?
Pre-eclampsia is a disease that occurs during pregnancy and is characterized by high blood pressure and protein in the urine. Preeclampsia is one of the most common complications of pregnancy. Epilepsy-like seizures occur in severe preeclampsia and are life-threatening.
What symptoms may indicate the development of preeclampsia?
High blood pressure - blood pressure values are 140/90 mmHg. Art. or higher. If systolic (upper) or diastolic (lower) blood pressure rises by 30 mm Hg. Art. or more, then such an increase cannot be ignored.
Art. or higher. If systolic (upper) or diastolic (lower) blood pressure rises by 30 mm Hg. Art. or more, then such an increase cannot be ignored.
Protein in urine - 300 mg in urine collected over 24 hours, or +1 value on a rapid test.
Swelling of the arms, legs or face , especially under the eyes or if the swelling leaves a depression in the skin when pressed. Edema can occur in all pregnant women and is generally harmless, but rapidly developing edema should be taken into account.
Headache that does not improve after taking pain medication.
Visual disturbances - double vision or blurred vision, dots or flashes before the eyes, auras.
Nausea or pain in the upper abdomen - These symptoms are often mistaken for indigestion or gallbladder pain. Nausea in the second half of pregnancy is not normal.
Nausea in the second half of pregnancy is not normal.
Sudden weight gain - 2 kg or more per week.
As a rule, there is a mild course of the disease that occurs at the end of pregnancy and has a good prognosis. Sometimes, preeclampsia can worsen quickly and be dangerous to both mother and fetus. In such cases, rapid diagnosis and careful monitoring of the mother and child are of paramount importance.
Unfortunately, most women show symptoms in the final stages of the disease. If you experience any of the above symptoms, you should contact your midwife, gynecologist, or the Women's Clinic emergency department.
Is preeclampsia called toxemia of pregnancy?
Previously, pre-eclampsia was really called toxicosis, or toxemia, since it was believed that the cause of the disease was toxins, that is, poisons in the blood of a pregnant woman.
What is the difference between preeclampsia and gestational hypertension?
Pregnancy hypertension is an increase in blood pressure above normal after the 20th week of pregnancy. With hypertension of pregnant women, protein in the urine is not observed.
What is HELLP syndrome?
HELLP syndrome is one of the most severe forms of preeclampsia. HELLP syndrome is rare and sometimes develops before symptoms of preeclampsia appear. Sometimes the syndrome is difficult to diagnose, as the symptoms resemble gallbladder colic or a cold.
When does preeclampsia occur?
Preeclampsia usually occurs after the 20th week of pregnancy. As a rule, preeclampsia goes away after delivery, but complications can occur up to six weeks after delivery, during which careful monitoring of the condition is necessary. If by the sixth week after birth, blood pressure does not return to normal, then you need to contact a cardiologist, who will begin treatment against hypertension.
If by the sixth week after birth, blood pressure does not return to normal, then you need to contact a cardiologist, who will begin treatment against hypertension.
What is the cause of preeclampsia?
The causes of the disease are still not clear, there are only unproven hypotheses.
How does the disease affect pregnant women and pregnancy?
Most preeclamptic pregnancies have a favorable outcome and a healthy baby is born. However, the disease is very serious and is one of the most common causes of death of the child and mother. Preeclampsia affects a woman's kidneys, liver, and other vital organs, and if left untreated, it can cause seizures (eclampsia), cerebral hemorrhage, multiple organ failure, and death.
How does the disease affect the fetus?
In preeclampsia, the fetus does not receive enough oxygen and nutrients to grow, and intrauterine growth retardation may occur.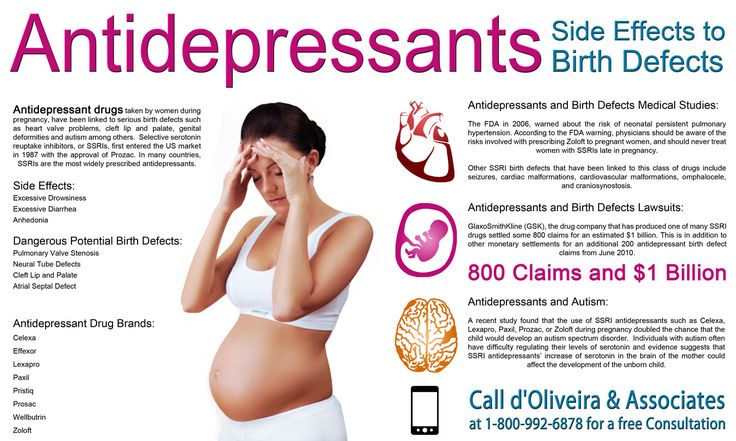 In addition, the placenta may separate from the uterine wall before the baby is born. Since the only treatment for preeclampsia is childbirth, sometimes a pregnancy has to be terminated prematurely. Until the 34th week of pregnancy, the lungs of the fetus have not yet matured, and steroid hormones are administered intravenously to the pregnant woman to prepare her lungs. In addition to the immaturity of the lungs, the health of a premature baby is threatened by many other diseases.
In addition, the placenta may separate from the uterine wall before the baby is born. Since the only treatment for preeclampsia is childbirth, sometimes a pregnancy has to be terminated prematurely. Until the 34th week of pregnancy, the lungs of the fetus have not yet matured, and steroid hormones are administered intravenously to the pregnant woman to prepare her lungs. In addition to the immaturity of the lungs, the health of a premature baby is threatened by many other diseases.
Who is at risk of developing preeclampsia?
Preeclampsia occurs in approximately 8% of pregnant women, many of whom have no known risk factors.
What are the risk factors for preeclampsia?
Patient-related risk factors
-
First pregnancy
-
Pre-eclampsia during a previous pregnancy
-
Age over 40 or under 18
-
High blood pressure before pregnancy
-
Diabetes before or during pregnancy
-
Multiple pregnancy
-
Overweight (BMI> 30)
-
Systemic lupus erythematosus or other autoimmune disease
-
Polycystic ovary syndrome
-
Long interval between two pregnancies
Risk factors associated with the patient's family
What is the prevention and treatment of preeclampsia
During the first trimester screening, or Oscar test, in addition to the most common chromosomal diseases, the risk of preeclampsia is also calculated. In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%.
In case of high risk, pregnant women are advised to take aspirin (acetylsalicylic acid) at a dose of 150 mg in the evenings until the 36th week of pregnancy. This helps reduce the chance of preeclampsia by the 34th week of pregnancy by up to 80%.
Childbirth is the only treatment for preeclampsia. Sometimes a child can be born naturally, but sometimes, if the disease is very acute, an emergency caesarean section is necessary. The best time to have a baby is after the 37th week of pregnancy. Bed rest, medications, and, if necessary, hospitalization can sometimes help bring the condition under control and prolong the pregnancy. Often, a doctor will refer a woman with preeclampsia to the hospital for observation, as the condition of the fetus and pregnant woman may suddenly worsen.
Does bed rest help?
Sometimes bed rest is enough to bring mild preeclampsia under control. In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
In this case, the patient often visits a doctor who measures blood pressure, does blood and urine tests, and monitors the course of the disease. The condition of the fetus is also often examined using a cardiotocogram (CTG) and ultrasound.
Are drugs used to treat preeclampsia?
High blood pressure sometimes requires medication. The medications used have few side effects, the drugs prescribed do not have much effect on the fetus, but are very important in the treatment of maternal high blood pressure.
Seizures are a rare but very serious complication of preeclampsia. Magnesium sulfate is sometimes given intravenously to prevent seizures in a pregnant woman with preeclampsia both during and after childbirth. It is safe for the fetus, but the mother may experience side effects such as hot flashes, sweating, thirst, visual disturbances, mild confusion, muscle weakness, and shortness of breath. All these side effects disappear when the drug is discontinued.
All these side effects disappear when the drug is discontinued.
Can preeclampsia recur?
Preeclampsia does not necessarily recur in the next pregnancy, but the main risk factor for preeclampsia is the presence of preeclampsia in a previous pregnancy(s). Risk factors for relapse include the severity of the previous case and the woman's overall health during pregnancy. A woman who has previously had preeclampsia should consult a gynecologist during a new pregnancy or when planning a pregnancy.
ITK1013
The information material was approved by the Health Services Quality Committee of East-Tallinn Central Hospital on 27.01.2021 (Minutes No. 2-21).
Signs, symptoms and causes of hemorrhoids in pregnant women - NEARMEDIC network of clinics
The main causes of hemorrhoids in pregnant women can be as follows:
- Chronic constipation.
 In this case, the stretching and tension of the walls of the rectum increases during defecation, which leads to the formation of hemorrhoids. In pregnant women, constipation occurs much more often due to a decrease in intestinal tone.
In this case, the stretching and tension of the walls of the rectum increases during defecation, which leads to the formation of hemorrhoids. In pregnant women, constipation occurs much more often due to a decrease in intestinal tone. - Inactive lifestyle. With hypodynamia, blood stagnation occurs in the venous plexus of the rectum, which eventually leads to vein thrombosis and the formation of hemorrhoids. Features of the condition do not always allow pregnant women to be mobile, therefore they have a high risk of developing this disease.
- Impaired blood circulation in the lower half of the body. During pregnancy, the uterus grows and compresses the inferior vena cava. This leads to stagnation of blood in the veins of the legs and rectum. During childbirth, a woman's intra-abdominal pressure rises greatly - this can cause hemorrhoids after pregnancy.
Signs of hemorrhoids in pregnant women
The longer the period, the higher the likelihood of developing the disease. Most often, hemorrhoids appear in the 3rd trimester or after childbirth.
Most often, hemorrhoids appear in the 3rd trimester or after childbirth.
The blood vessels of the hemorrhoidal plexus of the rectum gradually dilate. Over longer periods, the stretching of the veins becomes even stronger. With the expansion of the walls of the veins of the rectum, they lose their elasticity. This provokes protrusion of the veins under the mucous membrane.
If hemorrhoids protrude only into the lumen of the rectum and do not come out of the anus, then we are talking about the treatment of hemorrhoids of the 1st stage. The farther, the larger the knots become and the more they sag from the anus. In the second stage of hemorrhoids, the nodes sag from the anus, but are easily set back on their own. The third stage occurs when the nodes can no longer cope back.
Symptoms of the disease depend on its stage.
- Internal hemorrhoids. Symptoms are mild, there is no sagging of hemorrhoids from the anus. At this stage, women may experience pain during bowel movements, slight bleeding or fresh blood in the stool, and itching and discomfort in the anus.

- External hemorrhoids. The main symptom is the sagging of one or more purple-red nodes from the anus. This manifestation is the main sign of what is required, and not of another disease, such as anal fissure. Walking, sitting and defecation in this case become extremely painful.
Urgent medical attention is required in case of infringement of the hemorrhoid - a pregnant woman experiences very severe pain in the anus with fever.
Treatment of hemorrhoids during pregnancy
If a woman already has any symptoms of hemorrhoids - itching, pain in the anus, bleeding from the anus, etc. - professional treatment is required.
In NEARMEDIC, the first stage of treatment is the preventive measures described above, which stop the progression of the disease. Then the woman is prescribed drugs, both local and systemic. But due to pregnancy, local therapy is preferable, as this reduces the risk of side effects, increases the effectiveness of treatment and reduces the negative effects of drugs on the child. In any case, the medicine is prescribed only by the attending physician who observes the woman during pregnancy.
In any case, the medicine is prescribed only by the attending physician who observes the woman during pregnancy.
In the case when a woman already has prolapsed nodes that cannot be set, an operation is prescribed. Other indications for surgical intervention are infringement or necrosis of the hemorrhoid, as well as acute inflammation. Most often, in NEARMEDIC surgery is postponed until the postpartum period, and during pregnancy they are limited to conservative treatment.
Prevention of hemorrhoids during pregnancy
Due to the fact that all pregnant women are at high risk of developing hemorrhoids, NEARMEDIC doctors strongly recommend that preventive measures be taken throughout pregnancy, without waiting for symptoms to appear.
- Relief of constipation. To do this, you need to adjust your diet: eat more foods that contain coarse vegetable fiber - vegetables, fruits, cereals, cereals, prunes. Dairy products also have a beneficial effect on digestion.